Back to Journals » International Journal of Women's Health » Volume 14
COVID-19: A Cause of HELLP Syndrome? A Case Report
Authors Arslan E ![]()
Received 17 February 2022
Accepted for publication 21 April 2022
Published 26 April 2022 Volume 2022:14 Pages 617—623
DOI https://doi.org/10.2147/IJWH.S362877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Ebubekir Arslan
Mogadishu Somalia Turkish Training and Research Hospital, Mogadishu, 2526, Somalia
Correspondence: Ebubekir Arslan, Tel +905317936501, Email [email protected]
Purpose: There are still many unexplained points about how COVID-19 affects pregnant women and what kind of clinical and laboratory findings it reveals. These findings can become clinical conun drums when there is significant overlap with known and serious syndromes in pregnancy. The aim of this study is to report a case with a laboratory-proven diagnosis of COVID-19 and HELLP syndrome hypothesis.
Case Presentation: A 30-year-old multigravida (g3p2, repeated cesarean section) 32-week pregnant patient reported to the emergency service with complaints of chills, cough and shortness of breath that started 6 days ago. Following comprehensive screening tests for the differential diagnosis of lymphopenia, high liver enzymes, low platelets, abnormal coagulation panel, high D-dimer, high total bilirubin, high LDH and HELLP syndrome in the laboratory examinations of the patient, the patient’s laboratory findings were evaluated as compatible with HELLP syndrome. Emergency cesarean section was performed on the patient because of maternal hypoxemia. The finalization of the microbiological diagnosis of COVID-19 resulted to start conventional COVID-19 treatment. The fetus was also confirmed to be positive for COVID-19, and the newborn died on the 5th postnatal day. Unfortunately, our mother patient died on the 10th day of her hospitalization.
Conclusion: This report describes a case of multigravida, 30 years old, who presented with respiratory tract infection symptoms and hypothesized HELLP syndrome, who later tested positive for the novel coronavirus. The distinction between these two etiologies and onset times is extremely difficult. However, given the sequence of events in this case, it is reasonable to consider that COVID-19 may be an etiological factor associated with the pathophysiology of HELLP, despite the lack of conclusive evidence.
Keywords: COVID-19, pregnancy complication, HELLP, overlapping clinics, preeclampsia
Introduction
The coronavirus (CoV) pandemic still maintains a state of global urgency, and COVID-19 continues to remain a mystery with many still unknown features.1 There are reports of infectious diseases that mimicking hemolysis, elevated liver enzymes, and low platelet syndrome (HELLP) in pregnant patients.2,3 In this context, studies examining the effects of COVID-19 on pregnant women have also begun to be published.4 However, there are still many unexplained points about how COVID-19 affects pregnant women and what kind of clinical and laboratory findings it produces5. Furthermore, these findings can become clinical conundrums when they overlap significantly with known and serious syndromes in pregnancy. In this respect, sharing country experiences is of vital importance in learning lessons from mistakes, creating evidence and guides, and managing the process correctly.
HELLP syndrome occurs in 0.5–0.9% of all pregnancies, mostly in the last trimester (70%) and in multiparous women.6,7 It may present with nonspecific respiratory tract infection symptoms such as malaise, nausea, vomiting, abdominal pain and headache, as well as common pregnancy findings such as edema, proteinuria and hypertension. Although there is a close relationship between HELLP Syndrome and preeclampsia, hypertension may be mild in 16% of this syndrome and absent in 15%.8 In addition, in advanced cases, clinical manifestations such as impaired renal function, intracranial hemorrhage, intrahepatic hemorrhage, coagulopathy, and disseminated intravascular coagulation (DIC) may occur.9 Diagnostic criteria in the Tennessee classification are signs of microangiopathic hemolysis (abnormal peripheral smear, increased bilirubin level>1.2mg/dl, high LDH>600 IU/L), elevated liver enzymes (AST>70 IU/L), and low platelet count (<100k/dl). It is defined as mm3).10
Common laboratory abnormalities in COVID-19 patients include lymphopenia, elevated liver enzymes, and elevated C-reactive protein (CRP).11,12 In addition, studies in patients with severe disease showed laboratory abnormalities consistent with DIC and coagulopathy including thrombocytopenia,13 increased activated partial thromboplastin time (aPTT), prothrombin time (PT), D-dimer, interleukin-6 (IL-6), fibrin degradation products, and evidence of microangiopathic hemolytic anemia.11,14–20 It is possible that the pathology causing this clinical picture, defined as COVID-19-associated coagulopathy,16 may be the same and/or origin as the microangiopathy causing HELLP syndrome. For this reason, we would like to present a pregnant patient who has a positive new coronavirus test and has laboratory findings that match exactly with HELLP, and we want to create projections for further research in this direction.
Case Presentation
A 30-year-old multigravida (g3p2, repeated cesarean section) 32-weeks pregnant patient reported to the emergency service at 10 PM with complaints of chills, cough and shortness of breath that started 6 days ago. She had no medical history and her previous pregnancies had normal processes. There has never been a COVID-19 vaccine. Her respiratory rate was 26/min, blood pressure was 110/75 mm Hg, oxygen-free saturation was 84%, and body temperature was 38.8 °C. There was no uterine activity.
Initial laboratory examinations of the patient in the emergency room revealed lymphopenia, elevated liver enzymes, low platelets, increased Prothrombin Time (PT/INR) and activated Partial Thromboplastin Time (aPTT), high D-dimer, high total bilirubin, and high LDH; hemoglobin and kidney function tests were normal. The patient’s laboratory findings were evaluated as compatible with HELLP syndrome (Table 1). Gynecological examination by obstetrician (no uterine tenderness, no foul-smelling discharge, no amniotic discharge in speculum examination and ponding test), Ultrasound findings (head presentation, fetal heart rate: 145/min, amniotic fluid volume normal, biparietal diameter normal, placenta anterior) and NST findings (no reactive contraction) were normal. With these findings, the patient was admitted to the 3rd level intensive care unit reserved for COVID-19 patients, with preliminary diagnoses of COVID-19, sepsis and HELLP syndrome.
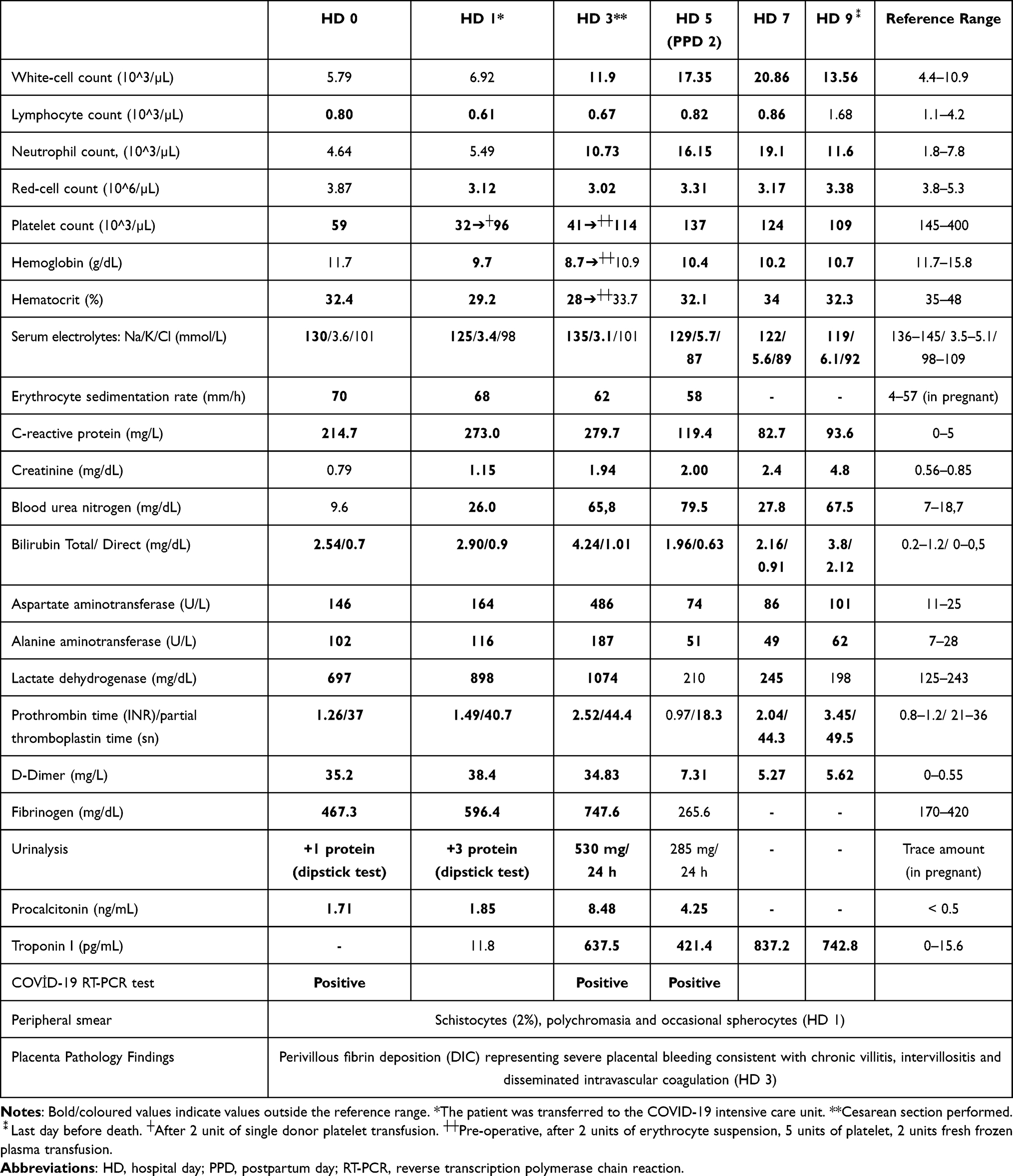 |
Table 1 Laboratory Findings of the Patient |
In the intensive care follow-up, the patient accepted the tomography recommendation, and bilateral diffuse ground glass areas, diffuse peripheral interstitial thickening and bilateral mild pleural effusion were found in the thorax CT examination, and these findings were reported to be compatible with viral pneumonia (COVID-19) (Figure 1). Immediately after this, the oropharyngeal swab sample obtained for the COVID-19 polymerase chain reaction (PCR) test was positive. Also, hepatitis markers studied and HIV test were negative. There was no growth in the blood and urine cultures taken on the first day. Serum electrolytes (Na, K, Cl, Ca, P, Mg) and cardiac markers (Troponin I, CKMB) were normal. Anti-Covid treatment (Lopinavir/Ritonavir, Hydroxychloroquine) was started upon the recommendation of the infection specialist, after obtaining the patient’s written consent.
 |
Figure 1 Chest tomography showing diffuse pulmonary involvement (hospital day 1). (A) Axial section. (B) Axial section. (C) Coronal section. |
The patient became hypertensive (blood pressure value ≥185/120 in consecutive measurements) at the end of the second day of hospitalization. Pregnant patient’s oxygen-free saturation dropped below 80% and a change in consciousness level developed. The patient was intubated in this condition. Obstetrician was consulted again to evaluate the possibility of termination of pregnancy, but they decided to operate the patient if hemodynamic stabilization was achieved. Our pregnant patient did not have risk factors for preeclampsia such as twin pregnancy and first pregnancy. However, hypertension developed. Therefore, the patient was started on antihypertensive treatment (sodium nitroprusside) and magnesium sulfate for seizure prophylaxis upon the recommendation of the obstetricians.
Haptoglobin studied on the 2nd day of hospitalization was 21 mg/dl, Reticulocyte Count was 98,109/L, Corrected Reticulocyte Percentage (Ret% ×HCT /45) was 2.93 and direct COOMBS test was negative. Abdominal USG was evaluated as normal (liver size, parenchyma echo was normal) and there was no acute fatty liver of pregnancy. In addition, Anti Ds DNA studied for differential diagnosis of HELLP Syndrome, IFT (5.88 IU/mL), Lupus anticoagulant/confirmation test (31.6 sec), Anti-nuclear Antibody (FANA) (IFA), Anti Cardiolipin IgG (5.6 GPL-U/ mL) was found to be negative on the 3rd day of hospitalization. In addition to these, thyroid function tests, vit-B, folic acid levels, Brucella Agglutination (Rose Bengal), lipase, urine microscopy and culture were also normal.
However, in the echocardiography performed on the 3rd day of the intensive care follow-up, segmental wall motion defects were detected and myocarditis was considered in the forefront by the cardiologist in the patient who developed concurrent troponin and CRP elevations. For the patient who was consulted again with the obstetrics and gynecology department on the same day (day three) (due to a progressive deterioration in maternal oxygen saturation, progressive deterioration in the blood picture despite platelet, FFP, fibrinogen replacement, a deterioration parallel to the pregnant’s baseline low in the NST follow-up of the fetus and in order to protect the fetus from hypoxic damage as much as possible), cesarean delivery was recommended. Thereupon, the patient was given preoperative two units of erythrocyte suspension, five units of platelet, two units of fresh frozen plasma transfusion with the recommendation of internal medicine physicians, and a singleton live baby boy via CS with Apgar scores of two and six was delivered on the third day of her hospitalization. Following delivery, the general condition and vital signs of the newborn deteriorated rapidly and he was intubated. Chest X-ray was normal, but the fetus was confirmed to be positive for COVID-19. Pancytopenia and renal failure developed on the 2nd day of intensive care hospitalization. The newborn died on the 5th postnatal day.
During the intensive care treatment, fluid, electrolyte, blood and blood products resuscitation, antihypertensive treatment, magnesium sulfate, antibiotherapy, hemodialysis due to anuria continued to be applied, however, the general condition of the patient gradually deteriorated. Brain MRI examination performed on the 9th day of her hospitalization revealed normal brain MRI findings. However, many attempts to extubate the patient were unsuccessful, and unfortunately the mother patient died on the 10th day of her hospitalization. This case belongs to a research proposal with ethical approval code of Mogadishu Somalia Recep Tayyip Erdogan Training and Research Hospital institutional Medical Ethics Committee (MSTH/8135).
Discussion
While the patient’s initial symptoms and clinical picture were suggestive of a respiratory infection, the diagnosis of HELLP syndrome seemed reasonable considering the laboratory findings. In the face of the mixed clinical picture at the beginning, the consultation reports of the relevant branches were only recommendations. The finalization of the microbiological diagnosis of COVID-19 caused us to start traditional COVID-19 treatment. In addition, we considered HELLP Syndrome as a highly probable diagnosis, as a result of microangiopathic hemolytic anemia characterized by schistocytes in peripheral smear and other findings supporting hemolysis, low platelet count and abnormal liver function tests, and extensive screening tests for differential diagnosis and exclusion of HELLP syndrome. Emergency cesarean section was applied to the patient due to the maternal hypoxemia and preeclampsia. On the 2nd day after cesarean section, liver enzymes decreased, platelet count increased, and this provided us with further evidence for the diagnosis of HELLP Syndrome, although not conclusive. This case is different from the cases previously presented in the literature.5,21,22 Because both diseases (COVID-19, HELLP) have a typical clinical course proven by laboratory findings and it is a case in which differential diagnostic diseases are ruled out with comprehensive screening.
The pathology of COVID-19 appears to be multifactorial, including thrombocytopenia, activation by aggregation and thrombosis, impaired bone marrow and megakaryocyte activity, and endothelial damage. In addition, it may cause platelet defragmentation due to changes in pulmonary capillary bed morphology.23,24 It is now a known fact that endothelial damage, platelet activation and thrombosis are also present in the physiopathology of HELLP syndrome and Preeclampsia.6–9 Despite the uncertainties based on this case, the synergism of these pathophysiological mechanisms (ie, causing HELLP syndrome in the most severe form of COVID-19, which is already a cause of thrombocytopenia) may have played an important role in reducing our patient’s already low platelet counts.
As in this case, there are already reports of elevated liver enzymes, thrombocytopenia, DIC, cardiomyopathy, acute renal failure, and ARDS in the general population infected with COVID-19.25–29 Pregnant patients infected with COVID-19 are likely to present with similar signs and symptoms, and most, if not all, of the same laboratory abnormalities, as in the general population.30,31 While the similarities between COVID-19 and HELLP are clear, it is essential to focus on some clinical criteria that can help the emergency physician or obstetrician differentiate between the two. The first is the presence or absence of high blood pressure. Depending on the severity of the disease, the elevated blood pressure seen in HELLP cases (seen in 20%) will be evident when compared to COVID-19 patients with normal or low blood pressure. The presence of proteinuria with hypertension will favor the diagnosis of HELLP syndrome, but normotensive and atypical HELLP syndrome cases without proteinuria should not be overlooked.32 Presence of fever, leukocytosis, respiratory distress and hypoxia will increase the suspicion of COVID-19. D-dimer is widely used as an initial screening parameter for COVID-19, but its sensitivity is known to be low in pregnancy.12 On the other hand, a chest X-ray or CT is helpful. Because the presence of “ground glass appearance” or “irregular infiltrates” can help differentiate COVID-19.33,34 Early chest imaging may also guide treatment in the acute phase when the COVID-19 PCR test may be negative. Also, early documentation of the respiratory infectious process can help avoid confusion when changes indicative of HELLP occur. On the other hand, while HELLP will begin to resolve 24 to 72 hours postpartum, it is likely that COVID-19 has nothing to do with timing of birth.
As a result, the distinction between these two etiologies and times of onset will be extremely difficult, as both diseases may cause similar laboratory findings and clinical presentations.5 In this respect, considering the current scenario in our case, the time of onset for respiratory infection symptoms and the sequence of events in this case, although there is no conclusive evidence, suggest that COVID-19 may be an etiological factor associated with HELLP physiopathology (hemolysis and thrombocytopenia) and it is reasonable to assume that it is a high risk for serious problems. However, the final clue will appear after microbiological diagnosis. In this context, our case report supports the early documentation of a positive COVID-19 test regardless of the severity of the disease and the early testing of pregnant women in centers where rapid viral tests are possible. Furthermore, it may help to encourage emergency physicians and obstetricians to gain insight into pregnant patients presenting to the clinic with findings similar to those presented in this case report, and to collaborate with a multidisciplinary team for the need for intensive care follow-up and possible preterm delivery.
Conclusion
This report describes a case of multigravida, 30 years old, who presented with respiratory tract infection symptoms and hypothesized HELLP syndrome, who later tested positive for the novel coronavirus. The distinction between these two etiologies and onset times is extremely difficult. However, given the sequence of events in this case and the extensive screening tests we performed for differential diagnosis of HELLP syndrome, it is reasonable to consider that COVID-19 may be an etiological factor associated with the pathophysiology of HELLP, despite the lack of conclusive evidence. However, the hypothesis that we have established in line with the clinical course of this case needs to be supported and proven by further studies to be conducted in this direction.
In this sense, we hypothesize that early documentation of a positive COVID-19 test when caring for pregnant women during the COVID-19 pandemic can help clinicians to avoid delays in early treatment and related complications of HELLP and COVID-19.
Institutional Review Board Statement
The ethics approval form was received from the ethics committee of Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital (approval number MSTH-8135).
Data Sharing Statement
Data are included in the manuscript.
Consent to Participate
Written informed consent has been obtained from the patient (the relatives of the patient) to publish this paper.
Funding
The author declares that this study has not received any funding resources.
Disclosure
The author declares no conflicts of interest associated with this publication.
References
1. Norooznezhad AH, Najafi F, Riahi P, Moradinazar M, Shakiba E, Mostafaei S. Primary symptoms, comorbidities, and outcomes of 431 hospitalized patients with confirmative RT-PCR results for COVID-19. Am J Trop Med Hyg. 2020;103(2):834–837. doi:10.4269/ajtmh.20-0512
2. White WM, Tran D, Garovic VD, Brost B. Acute interstitial nephritis proteinuria and herpes simplex virus hepatitis in pregnancy mimic HELLP syndrome (hemolysis, elevated liver enzymes, low platelets). AJP Rep. 2011;1(02):115–118. doi:10.1055/s-0031-1293513
3. Khangura RK, Williams N, Cooper S, Prabulos AM. Babesiosis in pregnancy: an imitator of HELLP syndrome. AJP Rep. 2019;9(02):e147–e152. doi:10.1055/s-0039-1687873
4. Allotey J, Stallings E, Bonet M, et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 2020;370:m3320. doi:10.1136/bmj.m3320
5. Futterman I, Toaff M, Navi L, Clare CA. COVID-19 and HELLP: overlapping Clinical Pictures in Two Gravid Patients. Am J Perinatol Rep. 2020;10(02):e179–e182. doi:10.1055/s-0040-1712978
6. Sibai BM, Ramadan MK, Usta I, Salama M, Mercer BM, Friedman SA. Maternal morbidity and mortality in 442 pregnancies with hemolysis, elevated liver enzymes and low platelets (HELLP syndrome). Am J Obstet Gynecol. 1993;169(4):1000–1006. doi:10.1016/0002-9378(93)90043-I
7. Mihu D, Costin N, Mihu CM, Seicean A, Ciortea R. HELLP syndrome - A multisystemic disorder. J Gastrointestin Liver Dis. 2007;16(4):419–424.
8. Saphier CJ, Repke JT. Hemolysis, elevated liver enzymes, and low platelets (HELLP) syndrome: a review of diagnosis and management. Semin Perinatol. 1998;22(2):118–133. doi:10.1016/S0146-0005(98)80044-X
9. Martin JJN, Rinehart BK, May WL, Magann EF, Terrone DA, Blake PG. The spectrum of severe preeclampsia: comparative analysis by HELLP (hemolysis, elevated liver enzyme levels, and low platelet count) syndrome classification. Am J Obstet Gynecol. 1999;180(6):1373–1384. doi:10.1016/S0002-9378(99)70022-0
10. Audibert F, Friedman SA, Frangieh AY, Sibai BM. Clinical utility of strict diagnostic criteria for the HELLP (hemolysis, elevated liver enzymes, and low platelets) syndrome. Am J Obstet Gynecol. 1996;175(2):460–464. doi:10.1016/S0002-9378(96)70162-X
11. Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med. 2020;20(02):124–127. doi:10.7861/clinmed.2019-coron
12. Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395(10226):809–815. doi:10.1016/S0140-6736(20)30360-3
13. Fan BE, Chong VCL, Chan SSW, et al. Hematologic parameters in patients with COVID-19 infection. Am J Hematol. 2020;1–4. doi:10.1002/ajh.25774
14. Nanshan C, Min Z, Xuan D, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
15. Dawei W, Bo H, Chang H, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
16. England JT, Abdulla A, Biggs CM, et al. Weathering the COVID-19 storm: lessons from hematologic cytokine syndromes. Blood Rev. 2020;45. doi:10.1016/j.blre.2020.100707
17. Engelmann B, Massberg S. Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol. 2013;13(1):34–45. doi:10.1038/nri3345
18. Chen G, Wu D, Guo W, et al. Clinical and Immunologic features in severe and moderate coronavirus disease 2019 [published online ahead of print 27 March 2020]. J Clin Invest. 2020. doi:10.1172/JCI137244
19. Levi M, Scully M. How I treat disseminated intravascular coagulation. Blood. 2018;131(8):845–854. doi:10.1182/blood-2017-10-804096
20. Ranucci M, Ballotta A, Di Dedda U, et al. The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome [published online ahead of print 17 April 2020]. J Thromb Haemost. 2020. doi:10.1111/jth.14854
21. Felipe L, Braga B, Sass N. Coronavirus 2019, thrombocytopenia and HELLP syndrome: association or coincidence? Rev Bras Ginecol Obstet. 2020;42(10):669–671. doi:10.1055/s-0040-1718437
22. Norooznezhad AH, Nurzadeh M, Darabi MH, Naemi M. Coronavirus disease 2019 (COVID-19) in a pregnant women with treatment resistance thrombocytopenic purpura with and suspicion to HELLP syndrome: a case report. BMC Pregnancy Childbirth. 2021;21(1):567. doi:10.1186/s12884-021-04030-x
23. Lippi G, Plebani M, Henry BM. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: a meta-analysis. Clin Chim Acta. 2020;506:145–148. doi:10.1016/j.cca.2020.03.022
24. Zulfiqar AA, Lorenzo-Villalba N, Hassler P, Andrès E. Immune thrombocytopenic purpura in a patient with Covid-19. N Engl J Med. 2020;382(18):e43. doi:10.1056/NEJMc2010472
25. Terpos E, Ntanasis-Stathopoulos I, Elalamy I, et al. Hematological findings and complications of COVID-19. Am J Hematol. 2020;95(7):834–847. doi:10.1002/ajh.25829
26. Lillicrap D. Disseminated intravascular coagulation in patients with 2019-nCoV pneumonia. J Thromb Haemost. 2020;18(4):786–787. doi:10.1111/jth.14781
27. Boettler T, Newsome PN, Mondelli MU, et al. Care of patients with liver disease during the COVID-19 pandemic: EASL-ESCMID position paper. JHEP Rep. 2020;2(03):100113. doi:10.1016/j.jhepr.2020.100113
28. Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811–818. doi:10.1001/jamacardio.2020.1017
29. Matthay MA, Aldrich JM, Gotts JE. Treatment for severe acute respiratory distress syndrome from COVID-19. Lancet Respir Med. 2020;8(5):433–434. doi:10.1016/S2213-2600(20)30127-2
30. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
31. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
32. Ronnje L, Länsberg J-K, Vikhareva O, Hansson SR, Herbst A, Zaigham M. Complicated COVID-19 in pregnancy: a case report with severe liver and coagulation dysfunction promptly improved by delivery. BMC Pregnancy Childbirth. 2020;20(1):511. doi:10.1186/s12884-020-03172-8
33. Yoon SH, Lee KH, Kim JY, et al. Chest radiographic and CT findings of the 2019 novel coronavirus disease (COVID-19): analysis of nine patients treated in Korea. Korean J Radiol. 2020;21(4):494–500. doi:10.3348/kjr.2020.0132
34. Mai C, Wang B, Chen R, et al. HELLP syndrome complicated by pulmonary edema: a case report. Open Med. 2018;13(1):509–511. doi:10.1515/med-2018-0075
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.