Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Costs and Clinical Consequences of Compliance with COPD GOLD Recommendations or National Guidelines Compared with Current Clinical Practice in Belgium, Germany, Sweden, and the United States
Authors Sethi S ![]() , Wright A, Hartgers-Gubbels ES
, Wright A, Hartgers-Gubbels ES ![]() , Hechtner M, Clark B
, Hechtner M, Clark B ![]() , Wright C, Langham S, Buhl R
, Wright C, Langham S, Buhl R
Received 4 May 2022
Accepted for publication 22 August 2022
Published 7 September 2022 Volume 2022:17 Pages 2149—2160
DOI https://doi.org/10.2147/COPD.S371440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Sanjay Sethi,1 Antony Wright,2 Elisabeth Sophia Hartgers-Gubbels,3 Marlene Hechtner,3 Brendan Clark,4 Ciara Wright,2 Sue Langham,2 Roland Buhl5
1Pulmonary/Critical Care/Sleep Medicine, University at Buffalo, State University of New York, Buffalo, NY, USA; 2Maverex Ltd., Newcastle Upon Tyne, NE6 2HL, UK; 3Boehringer Ingelheim GmbH, Ingelheim Am Rhein, Germany; 4Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA; 5Pulmonary Department, Mainz University Hospital, Mainz, Germany
Correspondence: Antony Wright, Maverex Ltd, Newcastle Upon Tyne, NE6 2HL, UK, Tel +44 (0) 161 4646838, Email [email protected]
Purpose: The objective of this study was to assess the clinical and cost benefits of treating patients with chronic obstructive pulmonary disease (COPD) according to global and national guidelines compared to real-life clinical practice in the United States and three European countries (Belgium, Germany, Sweden).
Patients and Methods: A cost-consequence model was developed to compare current prescribing patterns with two alternative scenarios, the first aligned with the Global Initiative for Chronic Obstructive Lung Disease (GOLD 2022) recommendations and the second with national guidelines. Costs and clinical outcomes were modeled for these alternative scenarios over a time horizon of one year, based on real-world evidence and health insurance data.
Results: Current clinical practice in each of the countries was inconsistent with published recommendations. A redistribution to prescribing patterns according to global and national recommendations led to a substantial decrease in the use of inhaled corticosteroid (ICS) containing therapies of more than 80% and 44%, respectively. There was a reduced incidence of up to 16% of mild-to-moderate pneumonia and up to 29% of severe pneumonia. Exacerbations decreased across all countries apart from Sweden, where a small increase in the rate of exacerbations was due to the redistribution of some patients currently undergoing inhaled triple therapy to non-ICS-containing therapies. Adapting treatment to recommendations could provide potential cost savings of up to 13% in estimated annual direct costs, resulting predominantly from the reduction in cost of healthcare resource use, including hospitalization associated with treating incident pneumonia, particularly severe pneumonia. Cost savings for prevalent adult patients with COPD on long-acting inhaler therapy ranged from € 31 to € 675 per patient per year.
Conclusion: Redistribution of COPD patients from current clinical practice to treatment according to published recommendations would provide clinical benefits and substantial cost savings.
Keywords: chronic obstructive pulmonary disease, guideline adherence, healthcare costs, maintenance inhaler therapy
Introduction
Chronic obstructive pulmonary disease (COPD) is chronic and progressive and is associated with significant societal and economic burden. It is underdiagnosed, preventable and treatable.1 Globally, age-standardized estimates of COPD prevalence are around 3.2% in males and 2.0% in females.2
The aim of treatment for COPD is to reduce symptoms, frequency and severity of exacerbations and complications and improve patients’ quality of life,3 using an individualized approach based on patient characteristics, particularly symptom burden and risk of exacerbations. In addition to global evidence-based strategy documents developed for the management of COPD,3 many countries produce national guidelines, for example, in Germany.4
There is often a divergence between treatment recommendations in COPD guidelines and real-life clinical practice.5 Real-world evidence suggests that prescribing patterns do not always follow evidence-based treatment strategies, in particular, inhaled corticosteroid (ICS)-based regimens. For example, triple therapy with ICS alongside a long-acting muscarinic antagonist (LAMA) bronchodilator and a long-acting β2 agonist (LABA) is prescribed frequently to patients outside of treatment recommendations.6–18 There are clinical and cost consequences of the divergence between recommendations and real-life clinical practice. Over-utilization of ICS-based regimens can increase the risk of pneumonia19 and other adverse effects associated with ICS use,20 thereby increasing healthcare resource use and associated costs.21
There are limited data evaluating the clinical and cost outcomes of treating COPD patients in line with Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations and national guidelines. We developed a cost-consequence model to estimate the clinical and cost benefits of prescribing according to global and national COPD recommendations compared to real-life clinical practice in the United States and three European countries (Belgium, Germany and Sweden).
Materials and Methods
Model Design
A cost-consequence analysis was conducted to estimate the difference in costs and clinical outcomes, over a one-year time horizon, between two alternative treatment scenarios: treatment according to current clinical practice based on real-world evidence (current treatment) and treatment according to either GOLD or national recommendations (proposed treatment). The model structure is outlined in Figure 1.
 |
Figure 1 Model structure. Abbreviations: COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; NICE, National Institute for Health and Care Excellence. Note: aTreatment distributions are broken down into four disease profiles based on exacerbation history and severity of symptoms. |
The impact of this redistribution of current treatment to an alternative recommendation-based treatment scenario was estimated for the International GOLD 20223 strategy recommendations in Belgium, Germany, Sweden and the United States and national guidelines in Belgium and Germany. National guidelines included the ABC approach defined in a 2017 consensus meeting of the committee for the evaluation of the medical practice regarding medicines in Belgium22 and the 2018 S2k guideline for the diagnosis and treatment of patients with COPD in Germany.4
Population
The model population in each country included adult patients with diagnosed COPD treated with maintenance long-acting bronchodilators. This population was estimated using country population estimates for adults ≥18 years, published COPD prevalence and the proportion of COPD patients using maintenance inhaler therapy (Supplementary Table 1). In the current treatment scenario, the population is distributed into four patient disease profiles for classification of symptom burden and risk of exacerbation and five classes of drug treatment, based on real-world evidence.
The four disease profiles are based on the profiles outlined in the GOLD ABCD assessment tool.3 GOLD A, patients with low exacerbation history (defined as ≤1 moderate exacerbations, not leading to hospitalization) and current low symptoms (defined as modified Medical Research Council [mMRC] 0–1 [dyspnea]; COPD Assessment Test [CAT] <10); GOLD B, patients with low exacerbation history and current high symptoms (defined as mMRC ≥2; CAT ≥10); GOLD C, patients with high exacerbation history (defined as ≥2 moderate exacerbations or ≥1 exacerbation leading to hospitalization) and current low symptoms; GOLD D, patients with high exacerbation history and current high symptoms.
The five treatment classes include monotherapy with LAMA or LABA; dual therapy with LAMA/LABA or LABA/ICS (fixed- or free-dose combination); or triple therapy consisting of LAMA with LABA and ICS (fixed-dose or free-dose combination). LABA monotherapy is infrequently prescribed in the United States, therefore this treatment option was not included in the United States adaptation of the model.
Treatment Distributions
The distribution of the prevalent COPD population into each of the four disease profiles and within these, into five treatment classes representing current treatment was carried out using observational data, which was country-specific where available (Supplementary Table 2). Real-world evidence included an ongoing, longitudinal, non-interventional study within the German COPD National Prospective Registry (DACCORD),23 a European Delphi online general practitioner and pulmonologist questionnaire,24 the Swedish National Airways Register,25 and an analysis of data in an administrative claims database in the United States.26
The GOLD 2022 strategy suggests that peripheral blood eosinophil counts could be used as a biomarker to guide the use of ICS therapy.3 Within each of the four disease profiles, the proportion of patients with high eosinophil levels (defined as a blood eosinophil count ≥300 cells/µL) was estimated from published evidence.27–30 The proportion of patients with high eosinophil levels was assumed to be equally distributed across all current treatment profiles in the United States (27% in each) and Sweden (27%) and distributed according to a UK database study in Belgium30 and based on the results of a large observational cohort study in Germany (14%).31
In order to estimate the change in clinical and economic outcomes resulting from prescribing according to guideline recommendations, the model hypothetically redistributed patients from current treatment to proposed treatment according to either GOLD or national recommendations (Figure 2).
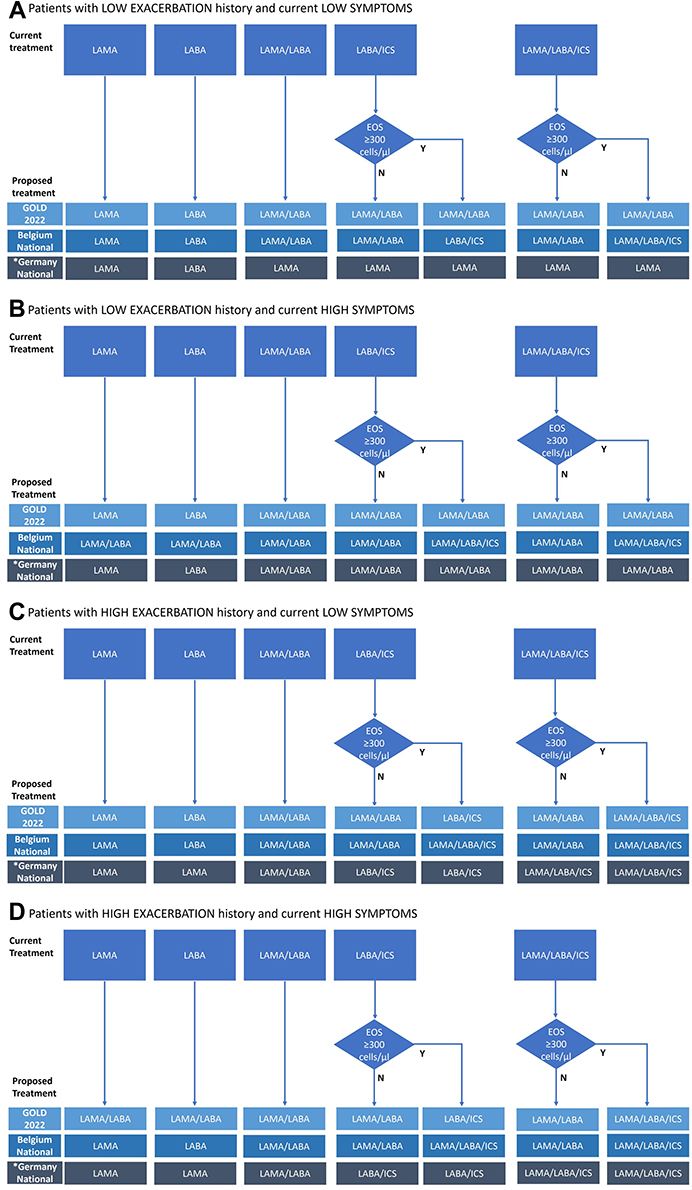 |
Figure 2 Treatment redistribution according to guideline recommendations. (A) Patients with LOW EXACERBATION history and current LOW SYMPTOMS. (B) Patients with LOW EXACERBATION history and current HIGH SYMPTOMS. (C) Patients with HIGH EXACERBATION history and current LOW SYMPTOMS, (D) Patients with HIGH EXACERBATION history and current HIGH SYMPTOMS. *German national guidelines do not consider blood eosinophil counts in treatment choice (for all disease profiles) and ICS is not recommended in patients with a low exacerbation history. Abbreviations: COPD, chronic obstructive pulmonary disease; EOS, eosinophils; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroids; LABA, long-acting β2 agonist; LAMA, long-acting muscarinic antagonist; N, no; Y, yes. Notes: The model includes a prevalent population of COPD patients. A large proportion of patients will have a previous treatment history and therefore be on maintenance/follow-up therapy (not initial therapy). Therefore, when redistributing, consideration was given to both initial treatment recommendations and follow-up treatment recommendations. LABA monotherapy is infrequently prescribed in the United States, therefore was not included in the calculations for that country. |
Clinical Outcomes
The impact on the annual rate of moderate and severe exacerbations and mild-to-moderate and severe pneumonia episodes resulting from a hypothetical redistribution of patients from current treatment to proposed treatment based on guideline recommendations was calculated.
The definition of moderate exacerbations used in this study included those that required treatment with antibiotics and/or systemic corticosteroids, prescribed in the primary care or outpatient hospital setting. Severe exacerbations included those that required inpatient hospital treatment.
The rate of moderate or severe exacerbations were calculated by establishing the baseline absolute risk of moderate or severe exacerbations in LAMA/LABA-treated patients with no history of exacerbations32 and then applying relative risks of other treatments compared to LAMA/LABA, without a constant for patients with no prior exacerbation history and with a constant for those with a prior exacerbation history.32,33 This constant was derived from risk estimates reported in patients who had experienced at least one exacerbation event subsequent to a year where no exacerbations were experienced34 (Supplementary Table 3).
The definitions of mild-to-moderate pneumonia were those that required treatment with antibiotics prescribed in the primary care setting and severe pneumonia were those that required inpatient hospital treatment. The relative risk between different drug classes was calculated by establishing the absolute pneumonia risk for LAMA/LABA and then applying the relative risk for other treatments35 (Supplementary Table 3).
Economic Outcomes
Direct costs of treatment, including drug cost and physician visits and hospitalization costs of moderate and severe exacerbations and mild-to-moderate and severe pneumonia events, were estimated for current treatment and proposed treatment, and the difference in total costs was calculated over a time horizon of one year. Annual costs were estimated from the perspective of a healthcare payer in the United States, statutory health insurance in Germany, the National Board of Health and Welfare in Sweden, and the payer perspective in Belgium with a 2020 cost year. Data sources included prescription data, national reference cost data based on the International Classification of Diseases revision 10 (ICD-10) or Diagnosis-Related Group (DRG) codes, and other published sources (Supplementary Table 4).
Results
Changes in Treatment Patterns, Costs and Outcomes
A change in treatment pattern is seen in each country when treatment is redistributed from current clinical practice to published recommendations (Table 1). In general, there is a substantial decrease in the use of ICS-containing dual or triple therapy with an increase in the use of LAMA/LABA, particularly in patients with low exacerbation history and current low symptoms and in patients with low exacerbation history and current high symptoms. Redistribution of patients from treatment according to current clinical practice to treatment according to GOLD recommendations led to a reduced incidence of pneumonia across all countries (Table 2 and Figure 3).
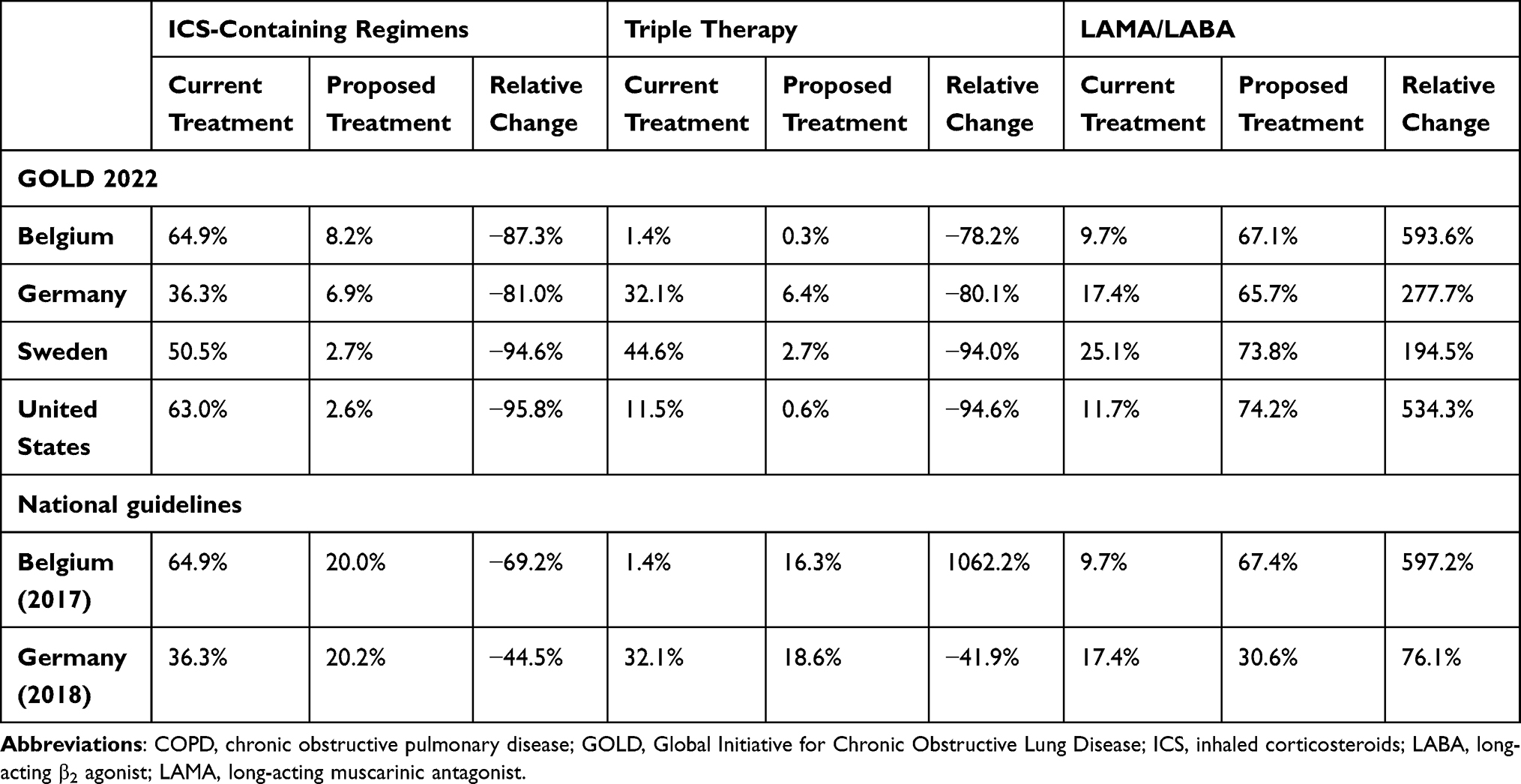 |
Table 1 Change in Proportion of Patients with COPD in Each Treatment Category Following Redistribution in Accordance with GOLD Recommendations and National Guidelines |
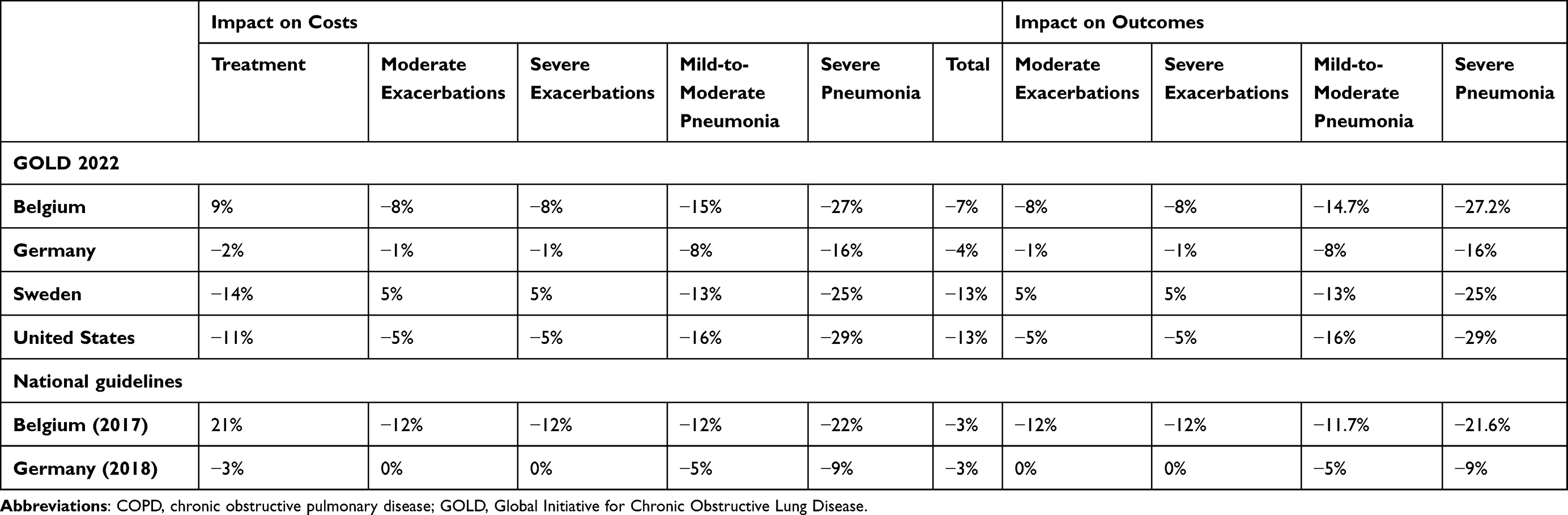 |
Table 2 Change in Annual Costs and Annual Clinical Events Following Redistribution in Accordance with GOLD Recommendations and National Guidelines |
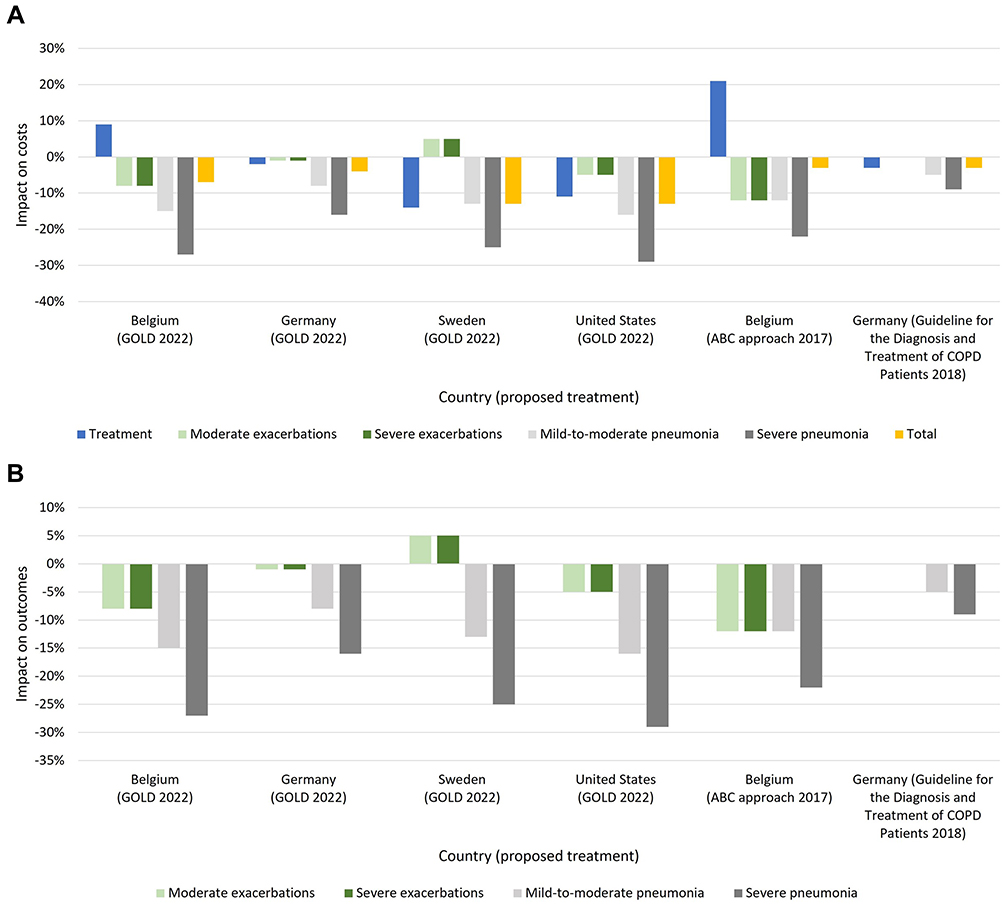 |
Figure 3 Percentage impact on (A) annual costs and (B) annual clinical events. Abbreviations: COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease. |
A reduction in the incidence of exacerbations was also seen in all countries except Sweden where there was a small increase (Table 2 and Figure 3), which was due to the high proportion of patients being redistributed from triple therapy to LABA/LAMA (Table 1).
Compared with current clinical practice, treating patients according to GOLD or national recommendations resulted in reductions of up to 13% in estimated annual direct costs (Table 2 and Figure 3). These cost savings resulted predominantly from reducing the cost of healthcare resource use, including hospitalization, associated with treating incident pneumonia, particularly severe pneumonia. Cost savings for prevalent adult patients with COPD on long-acting inhaler therapy ranged from €31 to €675 per patient per year (Table 3).
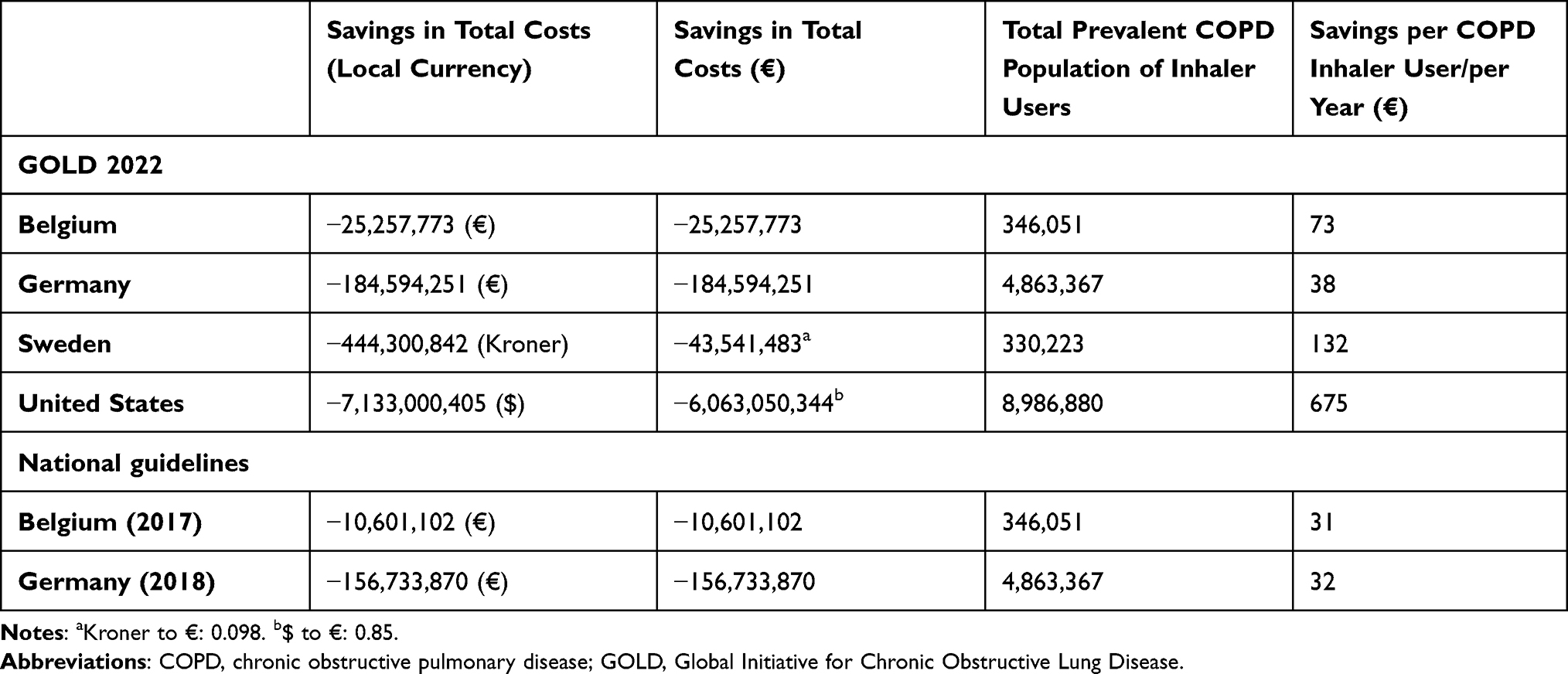 |
Table 3 Cost Savings Resulting from Prescribing According to Recommendations |
GOLD 2022 Strategy Country Variations
In the United States, 63% of patients with COPD who were being treated were prescribed ICS-containing regimens, based on real-world data. Treating this patient population in accordance with GOLD recommendations would reduce this proportion by 96% to 2.6%. The majority of these patients were a redistribution of patients on LABA/ICS in the current treatment scenario to LAMA/LABA in the proposed treatment scenario. This led to a large reduction in the incidence of mild-to-moderate pneumonia of 16% and severe pneumonia of 29%. There was also a small reduction in the rate of exacerbations due to the high proportion of patients being redistributed from LABA/ICS to LAMA/LABA. Cost savings amounted to around $7133 million, a reduction of 13%, with a corresponding saving of €675 per patient with COPD on maintenance inhalers per year. These savings resulted from the reduction in pneumonia events and also savings in treatment costs resulting from less triple therapy use.
In Sweden, 50% of COPD patients were being treated with ICS-containing regimens. A redistribution of patients with COPD from current practice to a proposed treatment scenario based on the GOLD strategy led to a reduction in the allocation of patients to ICS-containing regimens of 95%, all but a very small proportion of which was a redistribution of patients from LABA/ICS and triple therapy to LABA/LAMA. This led to a reduction in the incidence of mild-to-moderate pneumonia of 13% and severe pneumonia of 25%. There was a small increase in the rate of exacerbations of 5% arising from the redistribution of patients on ICS-containing therapy to LABA/LAMA. Cost savings amounted to around €43.5 million, a reduction of 13%, with a corresponding saving of €132 per patient with COPD per year. These savings resulted mainly from the reduction in pneumonia events and treatment costs. The annual costs of triple therapy are 35% higher than LABA/LAMA.
In Belgium, 65% of patients with COPD were being treated with ICS-containing regimens, based on real-world data. Treating this patient population according to GOLD recommendations would reduce this proportion by 87%, predominately due to a redistribution of patients on LABA/ICS to LAMA/LABA. This led to a large reduction in the incidence of mild-to-moderate pneumonia of 15% and severe pneumonia of 27%. There was also a small decrease in the rate of both moderate and severe exacerbations of 8% arising from the redistribution of patients on ICS-containing regimens to LAMA/LABA. Cost savings amounted to around €25.2 million, a reduction of 7%, with a corresponding saving of €73 per patient with COPD per year. Treatment costs increased resulting from the high proportion of patients redistributed from LABA/ICS (−88%) to LAMA/LABA (+606%).
In Germany 29% of patients were redistributed from ICS-containing regimens, the majority of which was LAMA/LABA/ICS (26%). This led to a reduction in the incidence of mild-to-moderate pneumonia of 8% and severe pneumonia of 16%. There was also a very small reduction in the rate of exacerbations. Cost savings amounted to around €184.6 million, a reduction of 4%, with a corresponding saving of €38 per patient with COPD per year. These savings resulted from the reduction in pneumonia events and treatment costs.
National Guidelines
In Belgium22 and Germany,4 where there are also national guidelines outlining treatment recommendations, redistribution of treatment patterns in line with these guidelines led to improved clinical and economic outcomes.
Overall, a reduction in the incidence and cost associated with treatment of exacerbations and pneumonia led to a projected reduction in the annual cost associated with treatment of COPD of 3% in Belgium and Germany, a saving of €31 and €32 per patient with COPD per year, respectively.
In Belgium, treatment according to national guidelines led to an increase in treatment costs of 21%. This was due to the very low use of triple therapy in current treatment practice and the recommendation in the Belgian national guidelines to use triple therapy in patients with historically high exacerbation risk and high blood eosinophils. The redistribution of patients from LABA/ICS to triple therapy resulting from adherence to the national guideline recommendations, increased use of triple therapy from a 1.4% share to 16.1%.
Discussion
Our cost-consequence model examined the economic and clinical impact of adapting the treatment of patients with COPD, profiled based on their exacerbation history and symptoms, from current clinical practice to treatment advised by published national and global recommendations. The results indicate that adherence to treatment guidelines would, in general, lead to a reduction in the prescription of ICS-containing regimens to patients with COPD of over 80% and 44% for global and national recommendations, respectively. The magnitude of this reduction for ICS-containing regimens overall and for triple therapy and LABA/ICS separately, is dependent on the clinical characteristics of the patient population, current prescribing patterns, and guideline recommendations.
Adapting treatment to recommendations could provide potential cost savings of up to 13% in estimated annual direct costs, resulting predominantly from decreased rates of pneumonia, with associated reductions in costs arising from antibiotic use and hospitalization. There was a reduced incidence of up to 16% of mild-to-moderate pneumonia and up to 29% of severe pneumonia. Exacerbations decreased across all countries, apart from Sweden where a small increase in the rate of exacerbations was due to the redistribution of certain patients currently undergoing triple inhaled therapy to non-ICS-containing therapies. Treatment cost savings were seen in some countries where there was a larger redistribution of patients from triple therapy to other treatment regimens. Cost savings for prevalent adult patients with COPD on long-acting inhaler therapy ranged from €31 to €675 per patient per year depending on country and guideline scenario.
Potential cost savings were higher for a redistribution to the GOLD strategy compared to national guidelines. GOLD recommendations led to a 4% (Germany) to 13% (the United States and Sweden) reduction in annual direct costs. In contrast, national guidelines led to a 3% reduction in Belgium and in Germany. Confirmation of these potential savings in well-controlled prospective observational studies is warranted.
Our results indicate that, overall, real-world adherence to recommendations is higher for national guidelines compared with the GOLD strategy. The main reason for this difference is that the GOLD strategy restricts the use of ICS to a limited number of high-risk patients. For example, guidelines recommend that triple therapy with LAMA/LABA/ICS should be reserved for patients who have a high symptom burden, a history of exacerbations, continue to experience persistent exacerbations while treated with LAMA/LABA and/or have evidence of high eosinophil levels.3 Restricting use to this high-risk population is based on clinical evidence suggesting that the balance of risks and benefits is favorable for this population but not in other lower-risk populations where patients would be exposed to unnecessary adverse events associated with ICS use.3
Previous studies have reported that treatments administered for patients with COPD do not always follow global or national guidelines. Patients with an unclear diagnosis or milder forms of the disease are frequently overtreated and, although less frequently, patients with more severe COPD may be undertreated.17,18,36,37 Evidence across Europe and the United States demonstrates that up to three-quarters of patients with less severe COPD, defined by exacerbation history and/or symptoms, are receiving ICS-based therapy, which is not in accordance with treatment strategies or guidelines.6–13,18,21 Another factor in the closer adherence to national guidelines may be that there are yearly updates to GOLD guidelines, while national guidelines are updated at much longer intervals. National guidelines are written by local experts in the local language, keeping national specifics and preferences in mind, facts which may also increase guideline adherence. The fact that international guidelines are written in English may still be a barrier for some physicians.
There are a number of limitations to this study. First, assumptions made in the development of this model include that a treatment distribution matrix is hypothesized to transfer patients from current treatment patterns to an alternate scenario aligned with GOLD 2022 or national guideline recommended maintenance inhaler therapy. The model does not represent switching patients to a new treatment. Second, model inputs and any other unspecified systemic and environmental factors (for example, population, treatment, market, and patient characteristics) remain unchanged over the time horizon. Third, while this framework was designed to represent real-world COPD care (for example, treatment patterns and adherence), the parameters were derived from multiple sources and may vary for different populations. In relation to adherence, no adjustment was made to account for treatment adherence when calculating annual treatment costs and, for efficacy and safety, adherence levels of the synthesized clinical trials used to derive outcome parameters were assumed. As adherence levels are likely to be lower in actual clinical practice this may have led to an overestimation of cost savings resulting from treatment according to clinical guideline recommendations, however the relative change in costs and outcomes would remain the same. Real-world data for fixed-dose combination triple therapy inhalers, approved in recent years, was limited in the United States. Data were not available on the distribution of high eosinophil levels between disease profiles in a number of countries and therefore an equal distribution was assumed. This assumption was based on available data demonstrating that the proportion of patients within each disease profile was similar.30 Indirect costs were not included. Country-specific data were used where available; however, in a small number of cases where this was not possible, data from other countries, in a similar geographical location and with similar healthcare systems were used.
It should be noted that individual patient or physician preference with regard to a decision to de-escalate or change treatment cannot be accounted for in the model. In specific cases, there may be a medical reason for deviating from the recommendations. Therefore, the results of this study should not be interpreted to mean that switching patients en masse is appropriate. Any proposed change to treatment should be discussed with the patient and should include a review of the diagnosis, management of comorbidities, symptoms and exacerbation history, inhaler technique, adherence to medication and any adverse events that may be associated with moving patients from one treatment to another. Finally, this model included patients diagnosed with COPD and prescribed inhaler treatment only. Studies conducted in North America and Europe have demonstrated that 10% to 12% of adults aged >40 years have evidence of persistent airflow limitation on spirometry, but only 20% to 30% of these subjects have been formally diagnosed with COPD.38
Conclusion
This study demonstrates that adherence to published research-based national or global guidelines for the treatment of COPD can lead to cost savings in four countries with distinct healthcare systems, by reducing healthcare resource use associated with the consequences of inappropriate treatment.
Data Sharing Statement
All data relevant to the study are included in the article or uploaded as Supplementary Tables.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by funding from Boehringer Ingelheim, Ingelheim am Rhein, Germany.
Disclosure
AW, SL, CW: received consulting fees from Boehringer Ingelheim and are affiliated with Maverex. BC, ESHG, MH: employees of Boehringer Ingelheim. SS reports consulting fees and/or honoraria from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Nuvaira, Pulmotect, Aerogen and Cornerstone, grants from Theravance, Regeneron and Sanofi all outside the submitted work. RB reports personal fees from AstraZeneca, Chiesi, Cipla, Sanofi, and Teva, as well as grants and personal fees from Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Roche, all outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18(1):163. doi:10.1186/s12890-018-0724-3
2. Soriano JB, Abajobir AA, Abate KH; GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet Respir Med. 2017;5(9):691–706.
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2022. Available from: https://goldcopd.org/2022-gold-reports-2/.
4. Vogelmeier C, Buhl R, Burghuber O, et al. Leitlinie zur Diagnostik und Therapie von Patienten mit chronisch obstruktiver Bronchitis und Lungenemphysem (COPD) herausgegeben von der Deutschen Gesellschaft für Pneumologie und Beatmungsmedizin e. V. und der Deutschen Atemwegsliga e. V., unter Beteiligung der Österreichischen Gesellschaft für Pneumologie. [Guideline for the diagnosis and treatment of COPD patients: issued by the German Respiratory Society and the German Respiratory League in co-operation with the Austrian Society of Pneumology]. Pneumologie. 2018;72(4):253–308. German. doi:10.1055/s-0043-125031
5. Bloom CI, Elkin SL, Quint JK. Changes in COPD inhaler prescriptions in the United Kingdom, 2000 to 2016. Int J Chron Obstruct Pulmon Dis. 2019;14:279–287. doi:10.2147/COPD.S190086
6. Adir Y, Horner A, de Vries GJ, et al. Treatment patterns in stable COPD patients – results from a large observational European study (SPACE). Eur Respir J. 2019;54(suppl 63):PA2509. doi:10.1183/13993003.congress-2019.PA2509
7. Chalmers JD, Poole C, Webster S, Tebboth A, Dickinson S, Gayle A. Assessing the healthcare resource use associated with inappropriate prescribing of inhaled corticosteroids for people with chronic obstructive pulmonary disease (COPD) in GOLD groups A or B: an observational study using the clinical practice research data. Respir Res. 2018;19(1):63. doi:10.1186/s12931-018-0767-2
8. Graf J, Jörres RA, Lucke T, Nowak D, Vogelmeier CF, Ficker JH. Medical treatment of COPD. Dtsch Arztebl Int. 2018;155(37):599–605. doi:10.3238/arztebl.2018.0599
9. Palmiotti GA, Lacedonia D, Liotino V, et al. Adherence to GOLD guidelines in real-life COPD management in the Puglia region of Italy. Int J Chron Obstruct Pulmon Dis. 2018;13:2455–2462. doi:10.2147/COPD.S157779
10. Lopez-Campos JL, Navarrete BA, Soriano JB, et al. Determinants of medical prescriptions for COPD care: an analysis of the EPOCONSUL clinical audit. Int J Chron Obstruct Pulmon Dis. 2018;13:2279–2288. doi:10.2147/COPD.S160842
11. Sundh J, Åberg J, Hasselgren M, et al. Factors influencing pharmacological treatment in COPD: a comparison of 2005 and 2014. Eur Clin Respir J. 2017;4(1):1409060. doi:10.1080/20018525.2017.1409060
12. Simeone JC, Luthra R, Kaila S, et al. Initiation of triple therapy maintenance treatment among patients with COPD in the US. Int J Chron Obstruct Pulmon Dis. 2017;12:73–83. doi:10.2147/COPD.S122013
13. Dhalwani N, Cabrera C, Booth A, Petrella R, Lambrelli D. Characteristics and treatment patterns of newly diagnosed COPD patients in Canada. Eur Respir J. 2019;54(Suppl 63):PA3385. doi:10.1183/13993003.congress-2019.PA3385
14. Reddel HK, Valenti L, Easton KL, Gordon J, Bayram C, Miller GC. Assessment and management of asthma and chronic obstructive pulmonary disease in Australian general practice. Aus Fam Physician. 2017;46(6):413–419.
15. Lane DC, Stemkowski S, Stanford RH, Tao Z. Initiation of triple therapy with multiple inhalers in chronic obstructive pulmonary disease: an analysis of treatment patterns from a U.S. retrospective database study. J Manag Care Spec Pharm. 2018;24(11):1165–1172. doi:10.18553/jmcp.2018.24.11.1165
16. Brusselle G, Price D, Gruffydd-Jones K, et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pathways in the UK. Int J Chron Obstruct Pulmon Dis. 2015;10(1):2207–2217. doi:10.2147/COPD.S91694
17. Barrecheguren M, Monteagudo M, Ferrer J, et al. Treatment patterns in COPD patients newly diagnosed in primary care. A population-based study. Respir Med. 2016;111:47–53. doi:10.1016/j.rmed.2015.12.004
18. Halpin DMG, de Jong HJI, Carter V, Skinner D, Price D. Distribution, temporal stability and appropriateness of therapy of patients with COPD in the UK in relation to GOLD 2019. EClinicalMedicine. 2019;14:32–41. doi:10.1016/j.eclinm.2019.07.003
19. Zheng Y, Zhu J, Liu Y, et al. Triple therapy in the management of chronic obstructive pulmonary disease: systematic review and meta-analysis. BMJ. 2018;363:k4388. doi:10.1136/bmj.k4388
20. Izquierdo JL, Cosio BG. The dose of inhaled corticosteroids in patients with COPD: when less is better. Int J Chron Obstruct Pulm Dis. 2018;13:3539–3547. doi:10.2147/COPD.S175047
21. Palli SR, Buikema AR, DuCharme M, Frazer M, Kaila S, Juday T. Costs, exacerbations and pneumonia after initiating combination tiotropium olodaterol versus triple therapy for chronic obstructive pulmonary disease. J Comp Eff Res. 2019;8(15):1299–1316. doi:10.2217/cer-2019-0101
22. de Cock J. Het rationeel gebruik van geneesmiddelen in de onderhoudsbehandeling van COPD en astma bij de volwassene. [The rational use of drugs in the maintenance treatment of COPD and asthma in adults]. Dutch; 2017. Available from: https://www.riziv.fgov.be/SiteCollectionDocuments/consensus_korte_tekst_20170511.pdf.
23. Worth H, Buhl R, Criée CP, Kardos P, Mailänder C, Vogelmeier C. The “real-life” COPD patient in Germany: the DACCORD study. Respir Med. 2016;111:64–71. doi:10.1016/j.rmed.2015.12.010
24. Ferreira AJ, Bakke P, Ekroos H, et al. Investigating the drivers for COPD treatment decisions. Eur Respir J. 2021;58(suppl 65):PA2413.
25. Swedish National Airways Register. Luftvägsregistret. [Swedish National Airways Register]. Swedish; 2020. Available from: https://lvr.registercentrum.se/nyheter?year=2020.
26. Palli SR, Zhou S, Shaikh A, Willey VJ. Effect of compliance with GOLD treatment recommendations on COPD health care resource utilization, cost, and exacerbations among patients with COPD on maintenance therapy. J Manag Care Spec Pharm. 2021;27(5):625–637. doi:10.18553/jmcp.2021.20390
27. Vogelmeier CF, Kostikas K, Fang J, et al. Evaluation of exacerbations and blood eosinophils in UK and US COPD populations. Respir Res. 2019;20(1):178. doi:10.1186/s12931-019-1130-y
28. Ellingsen J, Janson C, Bröms K, et al. Longitudinal measurements of blood eosinophils in relation to COPD outcomes. Eur Respir J. 2018;52(suppl 62):PA2015. doi:10.1183/13993003.congress-2018.PA2015
29. Sulku J, Janson C, Melhus H, et al. A cross-sectional study assessing appropriateness of inhaled corticosteroid treatment in primary and secondary care patients with COPD in Sweden. Int J Chron Obstruct Pulmon Dis. 2019;14:2451–2460. doi:10.2147/COPD.S218747
30. Gayle A, Dickinson S, Morris K, Poole C, Mathioudakis AG, Vestbo J. What is the impact of GOLD 2017 recommendations in primary care? – a descriptive study of patient classifications, treatment burden and costs. Int J Chron Obstruct Pulmon Dis. 2018;13:3485–3492. doi:10.2147/COPD.S173664
31. Greulich T, Mager S, Lucke T, et al. Longitudinal stability of blood eosinophil count strata in the COPD COSYCONET cohort. Int J Chron Obstruct Pulmon Dis. 2018;13:2999–3002. doi:10.2147/COPD.S165909
32. Oba Y, Keeney E, Ghatehorde N, Dias S. Dual combination therapy versus long-acting bronchodilators alone for chronic obstructive pulmonary disease (COPD): a systematic review and network meta-analysis. Cochrane Database Syst Rev. 2018;12(12):CD012620. doi:10.1002/14651858.CD012620.pub2
33. Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long-acting bronchodilator therapy in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Eur Respir J. 2018;52(6):1801586. doi:10.1183/13993003.01586-2018
34. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. New Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
35. Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219–229. doi:10.1001/archinternmed.2008.550
36. Grewe FA, Sievi NA, Bradicich M, et al. Compliance of pharmacotherapy with GOLD guidelines: a longitudinal study in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:627–635. doi:10.2147/COPD.S240444
37. Monteagudo M, Barrecheguren M, Solntseva I, et al. Clinical characteristics and factors associated with triple therapy use in newly diagnosed patients with COPD. NPJ Prim Care Respir Med. 2021;31(1):16. doi:10.1038/s41533-021-00227-x
38. Diab N, Gershon AS, Sin DD, et al. Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(9):1130–1139. doi:10.1164/RCCM.201804-0621CI
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patterns and Adherence to GOLD-Recommended Inhaled Therapy in Chronic Obstructive Pulmonary Disease (COPD) Patients with Acute Exacerbation History in Primary Care in China
Pei H, Su Y, Jing G, Su Q, Xu J, Jin X, Hao J, Xu J, Chen J, Li X, Ma J, Wang Y, Ye J, Yao M, Chi C
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:566724
Published Date: 14 February 2026