Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Cost-Effectiveness of Peptide Enhanced Bone Graft i-Factor versus Use of Local Autologous Bone in Anterior Cervical Discectomy and Fusion Surgery
Authors Thaci B, Yee R, Kim K, Vokshoor A, Johnson JP, Ament J
Received 4 May 2021
Accepted for publication 9 July 2021
Published 24 July 2021 Volume 2021:13 Pages 681—691
DOI https://doi.org/10.2147/CEOR.S318589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Bart Thaci,1 Randy Yee,2 Kee Kim,1 Amir Vokshoor,2– 4 J Patrick Johnson,5 Jared Ament2– 5
1University of California, Davis, Sacramento, CA, USA; 2Neuronomics LLC, Los Angeles, CA, USA; 3Neurosurgery & Spine Group, Los Angeles, CA, USA; 4Institute of Neuro Innovation, Santa Monica, CA, USA; 5Cedars Sinai Medical Center, Los Angeles, CA, USA
Correspondence: Jared Ament
Neuronomics LLC, 7320 Woodlake Ave, Suite 215, West Hills, CA, 91307, USA
Tel +1 800 899 0101
Fax +1 310 870 8677
Email [email protected]
Study Design: We conducted decision analytical modeling using a Markov model to determine the ICER of i-factor compared to autograft in ACDF surgery.
Objective: The efficacy and safety of traditional anterior cervical discectomy and fusion (ACDF) surgery has improved with the introduction of new implants and compounds. Cost-effectiveness of these innovations remains an often-overlooked aspect of this effort. To evaluate the cost-effectiveness of i-FACTOR compared to autograft for patients undergoing ACDF surgery.
Methods: The patient cohort was extracted from a prospective, multicenter randomized control trial (RCT) from twenty-two North American centers. Patients randomly received either autograft (N = 154) or i-Factor (N = 165). We analyzed various real-world scenarios, including inpatient and outpatient surgical settings as well as private versus public insurances. Two primary outcome measures were assessed: cost and utility. In the base-case analysis, both health and societal system costs were evaluated. Health-related utility outcome was expressed in quality-adjusted life years (QALYs). Cost-effectiveness was expressed as an incremental cost-effectiveness ratio (ICER).
Results: In all scenarios, i-FACTOR reduced costs within the first year by 1.4% to 2.1%. The savings proved to be incremental over time, increasing to 3.7% over an extrapolated 10 years. The ICER at 90 days was $13,333 per QALY and became negative (“dominated”) relative to the control group within one year and onwards. In a threshold sensitivity analysis, the cost of i-FACTOR could theoretically be increased 70-fold and still remain cost-effective.
Conclusion: The novel i-FACTOR is not only cost-effective compared to autograft in ACDF surgery but is the dominant economic strategy.
Keywords: cost-effectiveness, i-factor, spine fusion, spine allograft, cervical spondylosis, anterior cervical discectomy and fusion, cost analysis, decision analysis
Introduction
Cervical spondylosis is the most common cause of myelopathy and upper extremity radiculopathy. Anterior cervical discectomy and fusion (ACDF) interventions have doubled over the previous decades and this trend is likely to continue as the population ages.1 Current technological advances in biomaterials are shaping the future of surgical techniques. The ACDF procedure was first described by Cloward2 and Smith & Robinson3 six decades ago using autologous iliac crest bone graft (ICBG) and a lot has changed since. In the last two decades there has been increasing interest in biological grafts, the properties of natural and synthetic substitutes, and how alternatives to the traditional iliac crest autologous graft harvest can be safely used to accelerate healing and fusion. The debate comparing autologous bone, allografts, stem cells, and the highly cited and now debarred bone morphogenetic proteins (BMPs) for cervical spinal fusion4,5 is prevalent in the medical literature and omnipresent at national and international academic conferences. Efficacy and cost-effectiveness are the pillars on which we need to make our choices.
Recently, i-FACTOR® Peptide Enhanced Bone Graft, a novel anorganic bone matrix (ABM) containing a synthetic 15 amino acid cell-binding peptide (P-15 peptide) has been proposed as an alternative. Originally, this technology was approved by the FDA to promote bone formation in periodontal defects due to its properties to enhance cell proliferation, differentiation and osteogenesis.6–8 Notably, i-FACTOR, unlike bone morphogenetic protein, does not induce ossification in soft tissues. In a study, Arnold et al,9 demonstrated i-FACTOR to be comparable to local autologous bone for fusion rates and statistically superior in overall clinical success in patients undergoing ACDF surgery. Despite promising results, our healthcare system is constantly being taxed by a growing number of aging individuals and it remains critical that innovation be appropriately assessed for cost and sustainability.
Two approaches are commonly used to conduct a cost-effective analysis (CEA) in healthcare: simple incremental calculation or decision analytical modeling.10 A major drawback of the cost-accounting approach is its inability to describe relationships between clinical events, which impedes the prediction of how parameters change relative to one another. The purpose of this study was to perform a CEA via decision analytical modeling using a Markov method to evaluate the cost-effectiveness of i-FACTOR compared to autograft for patients receiving ACDF surgery.
Methods
Model Design
Patient informed consent and Institutional Review Board authorization was not required for this study since the patient cohort was extracted from a published prospective, multicenter randomized control trial (RCT).9,11 Included patients were randomized preoperatively to receive the ACDF structural graft either packed with local autologous bone (n=154) or with i-FACTOR (n=165). The additional device cost of i-FACTOR is assumed to be $750 compared to the $0 direct cost for autograft control. The primary time horizon used to estimate cost and health utility was two years. Additional post-operative periods examined in this analysis included 90 days, one year, six years, and 10 years.
The analysis was conducted to assess two principal outcome measures: cost and utility, in accordance with the Second Panel on Cost-Effectiveness Health and Medicine convened by the United States Public Health Service.12 For the former, we adopted two commonly employed perspectives - societal and health system - as our base case cost assessment. The health system perspective accounts for direct medical costs alone, whereas the societal perspective accounts for both direct and indirect costs. Indirect costs are often referred to as productivity loss. Direct medical costs included operating room time, hospital stay, post-operative medications, follow-up visits (scheduled and unscheduled), surgery-related complications, device-related complications, and subsequent surgeries following such complications. Productivity loss was defined as lost workdays. Productivity loss was not computed for retired patients. All cost items were adjusted for inflation to 2019 dollars per the US medical care Consumer Price Index (CPI) (https://www.bls.gov/news.release/pdf/wkyeng.pdf).
Health related utility outcome was expressed in quality-adjusted life years (QALYs). The base case analysis utilized SF-36 data from the RCT, transforming this into weighted utilities based on SF6D. Both cost and QALY outcomes were discounted at a yearly rate of 3% to reflect their present value. The cost-effectiveness outcome measure was calculated as the incremental cost-effectiveness ratio (ICER) for i-FACTOR compared to autograft. By definition, an ICER is the difference in cost divided by the difference in QALY for two interventions. A value under the commonly accepted US-based willingness-to-pay (WTP) threshold of $100,000 per QALY was considered cost-effective for i-FACTOR compared to autograft. Secondary thresholds, such as $50,000 per QALY and $150,000 per QALY were also examined.
Health States
To determine overall functional status of the RCT9,11 cohorts, five health states were constructed by regressing visual analog scale (VAS) on Neck disability index (NDI). Multiple VAS measurements were obtained in the original trial (ie shoulder, arm, neck). We used a mean VAS score for the analysis. The combined VAS score was found to have strong correlation (Pearson’s product-moment correlation: 0.797; p < 0.001) with NDI. The creation of health states is depicted in Supplementary Figure 1.
Markov Model Development
A cohort Markov model (Figure 1) was constructed to analyze peri-operative and post-operative costs and QALYs for both i-FACTOR and autologous bone cohorts. Each health state was associated with different costs and utilities. A sixth health state was created to represent “death”, accounting for US age-specific all-cause mortality (ie, an absorbing Markov state). Patients were redistributed across the six Markov states in each Markov cycle, attempting to parallel the post-operative course on a population level. The process of redistribution was controlled by two factors: (1) the preoperative distribution of health states; and, (2) the transition probabilities between the health states (Supplementary Tables 1 and 2).
 |
Figure 1 Markov model depicts patient’s health and work status at each follow-up period. Each node represents transition to health states associated with different costs and utility scores. |
Transition Probability Parameters
To better capture postoperative recovery, which is usually more dramatic and exponential in nature during the initial 6-weeks of follow-up compared to later periods, the model was designed with different cycle lengths. It began with 1.5-month cycles increasing to 3-month cycles after the 3-month follow-up visit; and then 6-month cycles from the 12-month follow-up visit onwards.
Work status was extracted from the RCT. Work status was categorized into “work with no restriction”, “work with few restrictions”, “work with many restrictions”, “unable to work”, and “not working for unrelated reasons” (ie unemployed, student, or retired).
Lastly, we considered four postoperative clinically pertinent events: 1) reoperations related to index surgery; 2) reoperations related to i-FACTOR failure; 3) reoperations related to subsequent surgery; and, (4) other types of complications. All complications have associated time-specific probabilities associated with level of severity (Table 1).
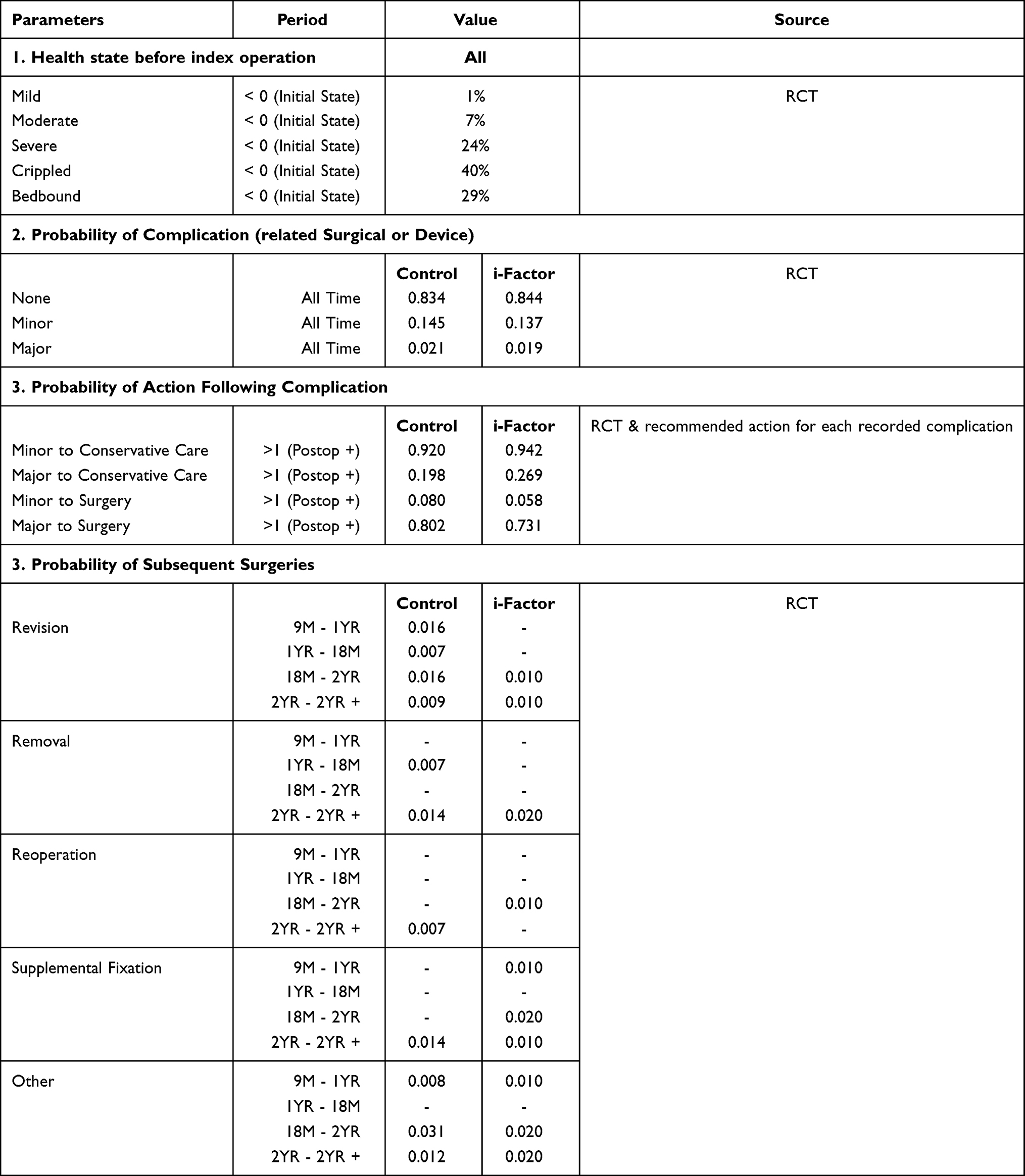 |
Table 1 Probability of Complications Depending on Preoperative Health Care Status |
Direct Costs
Direct surgical costs were taken from Medicare and private payer data. The base case model utilized a 50:50 split of Medicare and private payer rates to better reflect a realistic patient population. Supplemental procedures (office visits, physical therapy, etc.) were also considered in the model (Table 2).
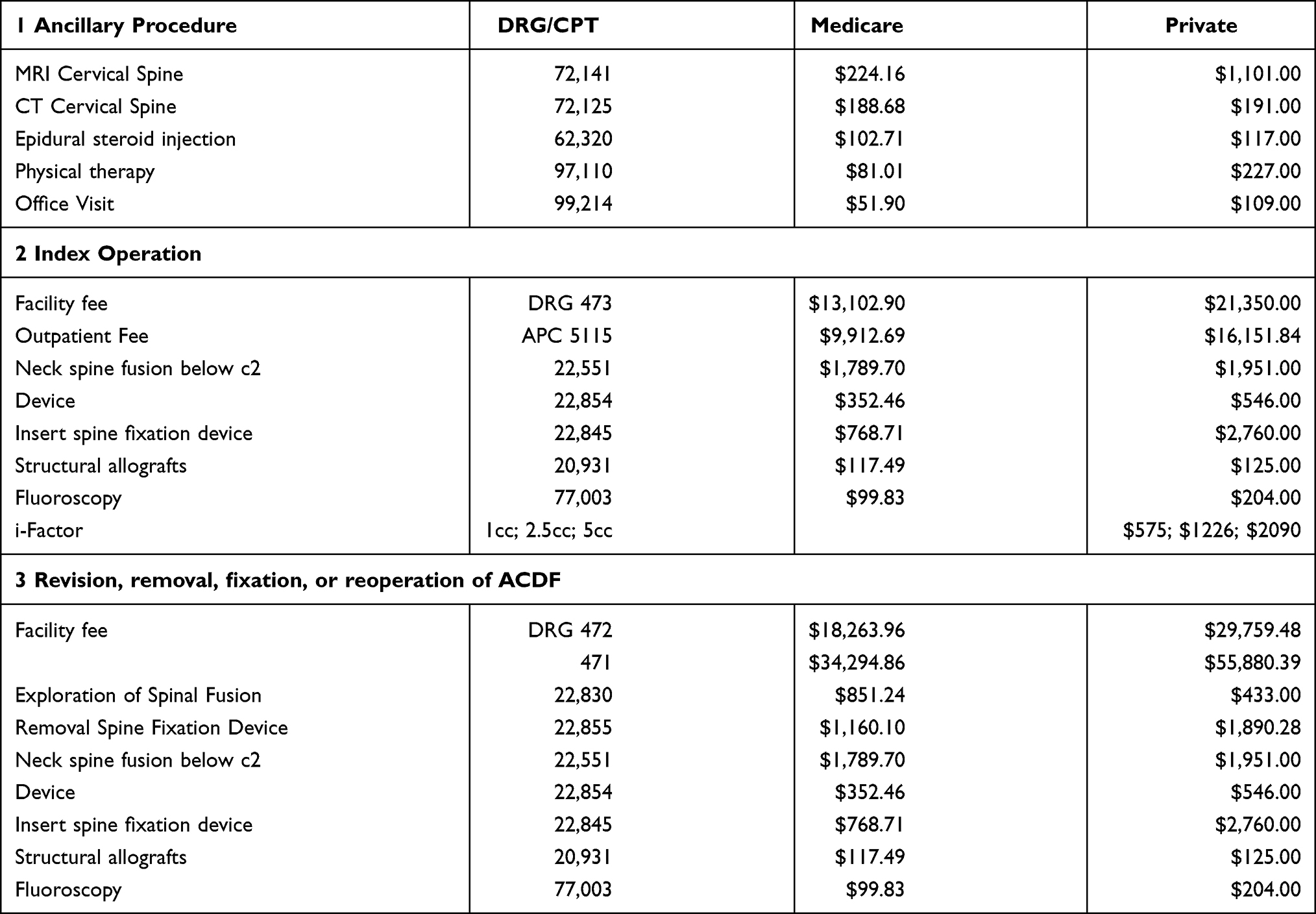 |
Table 2 Direct Surgical Costs |
Descriptive statistics for i-FACTOR found that amount of graft used per procedure was 1cc or less for 88.9%; 2cc for 8.6%; and 5cc for 2.5%. The base case model therefore assumed the 1cc price of $750. However, alternative scenarios were presented in the sensitivity analysis. Medication use were extracted from RCT data. We calculated average monthly medication costs for each health state (Supplementary Table 3). Prices were found for each medication using Micromedex’s RED BOOK.
Indirect Costs
Productivity loss is based on work status reported in the trial and was determined for each postoperative time point. In the Markov model, we translated work status into percentage of work time. The states: “work with no restriction”, “work with few restrictions”, “work with many restrictions”, and “unable to work” were associated with 100%, 70%, 30%, and 0% work time, respectively. We applied 2019 US national average annual wages to calculate productivity loss associated with health state transitions over time. Productivity loss is included in the scenarios analyzed from a societal perspective (Supplementary Table 4).
Base Case Scenario and Sensitivity Analysis
Quality of life estimates were converted from SF36 scores using Sheffield University’s SF-36/SF-6D scoring algorithm (Supplementary Table 5). We constructed the base case scenarios with a set of assumptions: 1) index surgery performed as inpatient with i-FACTOR cost was $750.00 greater than control (weighted with RCT distribution); 2) direct costs were calculated using a 50:50 mix of inpatient Medicare rates and private rates; and 3) horizon in which costs and benefits accrued was two years. Since the above assumptions can affect outcome, we also performed varying scenarios sensitivity analyses, assuming an entire inpatient or outpatient setting and complete Medicare versus private payer cohorts. One-way sensitivity analysis (OWSA) was used to identify the parameters associated with the greatest uncertainty and influence on our conclusions. Each parameter was varied by ±20% of its base case value. The OWSA was performed by varying each of the 52 input parameters individually (including initial surgery/complication/medication costs, complication probabilities, and utility values).
In the probabilistic sensitivity analysis (PSA), all input parameters (including 52 parameters tested in OWSA and 350 health state transition probabilities) were varied simultaneously to assess cost-effectiveness outcomes in response to collective parameter uncertainty. Probability and utility variables were randomly sampled based on 1) the statistics derived from the data; and, 2) cost variables, those variables that were not derived from the trials are sampled from Gamma distributions with standard deviations being 15.3% (~30%/1.96) of their base case values. Cost-effectiveness outcomes were calculated for each iteration of random sampling. The results presented were based on A 5,000 iteration Monte Carlo simulation.
Results
The majority of patients (92%) began with high NDI and VAS scores, thereby classifying them into the two worst health states (Table 1). There was a non-significant advantage in complication rates for the i-FACTOR group and also lower rates of return surgeries.
The direct health system costs perspective demonstrates that at 90 days, the i-FACTOR group costs were only marginally increased by $80 (0.25%) compared to the control group (Table 3). In contrast, within a year, the cost difference favored the i-FACTOR by $968 (2.1%). Notably, in the base case analysis, the ICER at 90 days was $13,333 per QALY and became negative (“dominated”) relative to the control group at one year and onwards.
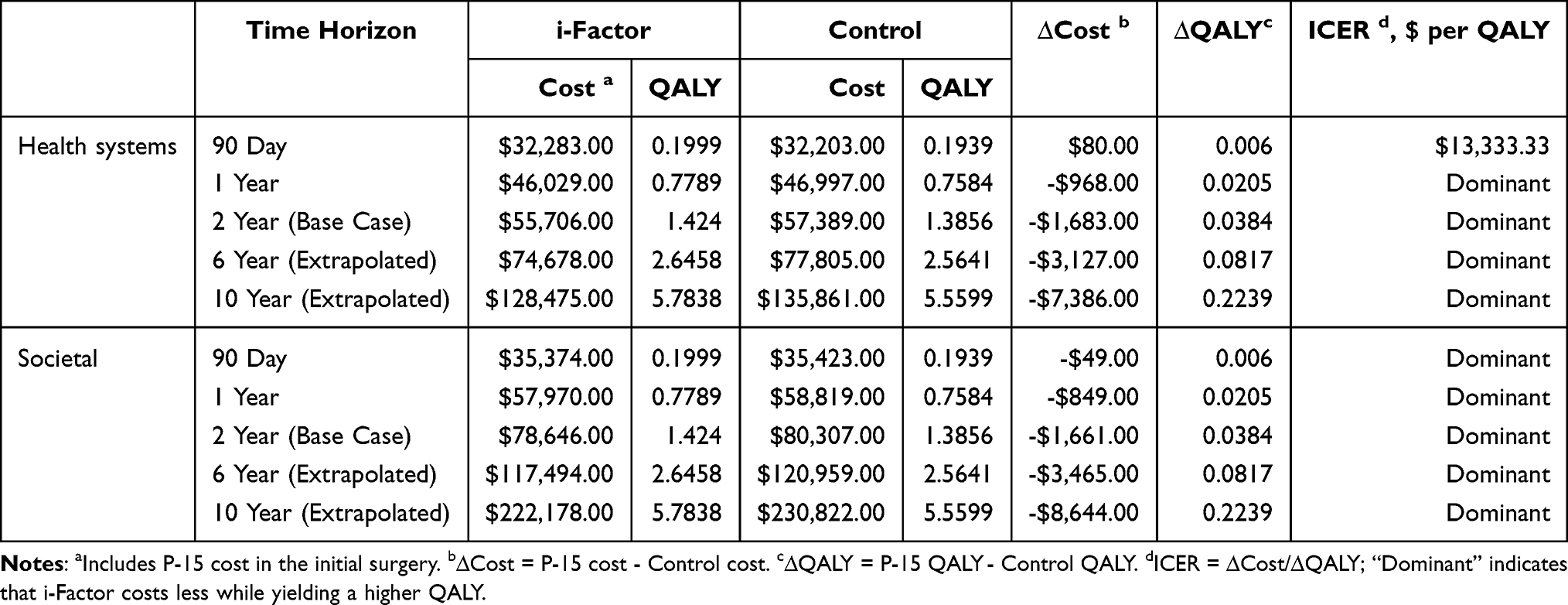 |
Table 3 Base Case Results with Medicare and Private Rates (Both Perspectives) |
In the societal perspective, i-FACTOR reduced costs by $49 in 90 days, suggesting economic dominance. The savings were incremental over time, reducing costs from 1.4% within the first year to 3.7% at an extrapolated 10-year interval (Table 3). Differences in work status between groups were minimal. At 2-years, 84.9% of patients in the i-FACTOR group had few or no limitation at work as compared to 83.5% in the control group (Supplementary Table 4). In all scenarios, the ICER for i-FACTOR was significantly lower than the US WTP threshold of $100,000 per QALY.
Net monetary benefit was also analyzed based on willingness-to-pay thresholds per unit of benefit (ie, QALY). At one year and a WTP threshold of $100,000/QALY, i-FACTOR saved $3,018 of direct cost and $2,899 of indirect cost (Supplementary Table 6). Complication rates based on the RCT data indicated a trend toward fewer complications in the i-FACTOR group as compared to control, 15.2% vs 16.2% respectively, at two years (Supplementary Table 7). As a result, there was a statistically non-significant greater requirement for subsequent surgical intervention in the control group at 90 days (2.81% versus 2.16%; Supplementary Table 8). This led to overall superior health states in the i-FACTOR group (Supplementary Table 9). A total of 63% of patients in the i-FACTOR group had “minimal deficits” at two years compared to 51.55% of the control cohort.
Sensitivity Analysis
The base case scenario assumed all procedures to be inpatient with a 50:50 distribution between Medicare and private insurance. This resulted in a $1,683 cost advantage for the i-FACTOR group (Table 4). Having a 50:50 distribution between inpatient and outpatient procedures did not alter the cost advantage for i-FACTOR (Panel 1, Table 4). This advantage remained even if all initial surgeries were outpatient. The i-FACTOR strategy dominated over the control in all the above scenarios, yielding an ICER of negative $43,828 per QALY.
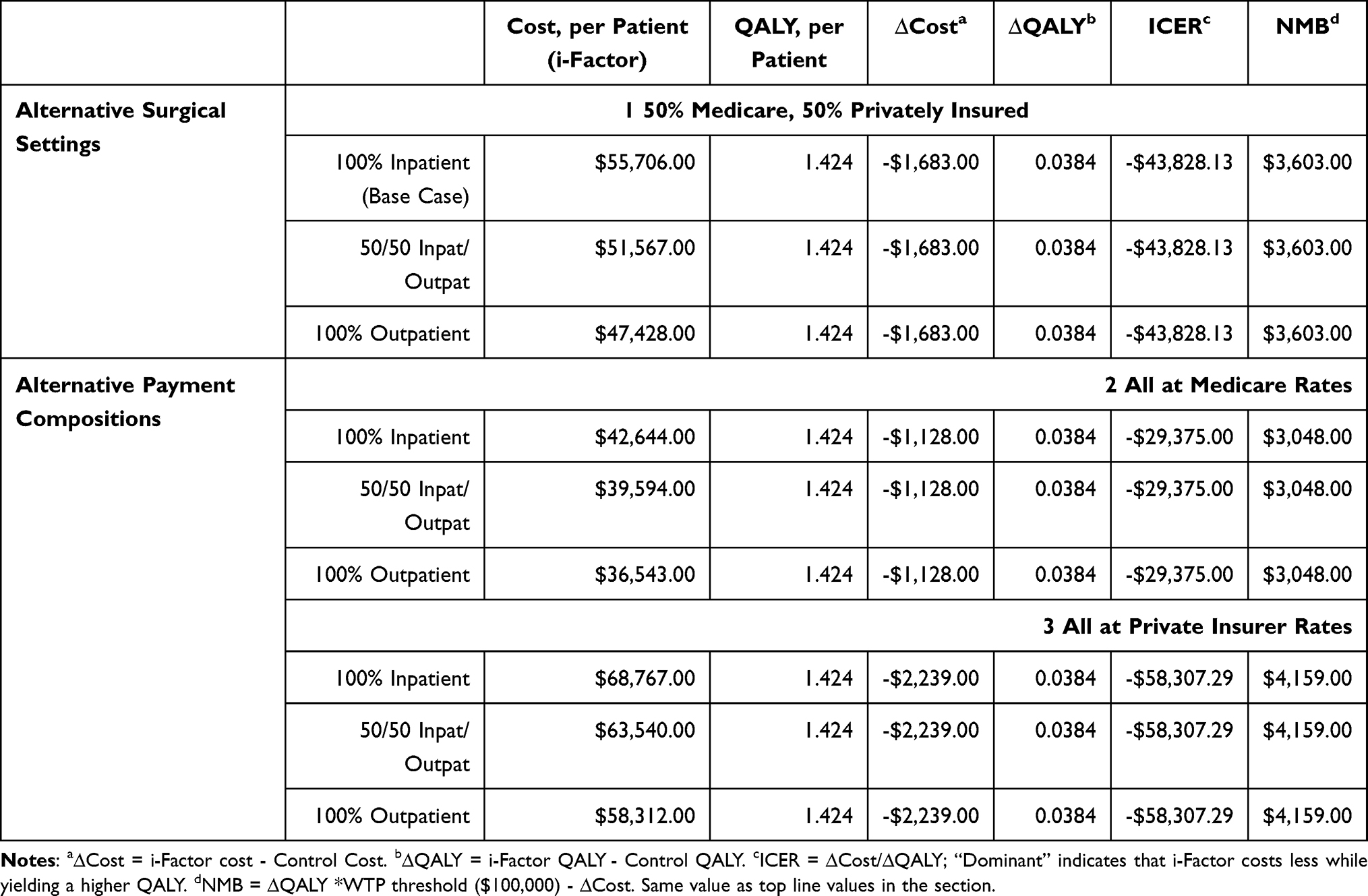 |
Table 4 Scenario Sensitivity Analyses: Cost-Effectiveness of P-15 vs Control in Alternative Scenarios |
Payer type scenarios were also examined (Panel 2, Table 4). In pure Medicare or private payer scenarios, i-FACTOR remained the dominant cost-effective strategy with ICERs of -$29,375 and -$58,307 per QALY, respectively.
Due to inherent uncertainties in the base case analysis, the OWSA results were presented in descending order of impact on cost-effectiveness (Supplementary Figure 2). The ICER consistently fell below the $100,000 WTP mark for most parameters. The greatest impact on the ICER and NMB were the “non-serious complication probabilities”. The PSA demonstrated i-FACTOR to be cost-effective in greater than two-thirds of the 5000 iterations (Figure 2A). As WTP increased from 50,000 to 100,000, favorable simulations increased from 66% to 75% (Figure 2B). Similarly, in the threshold analysis, the most conservative estimate limited the i-FACTOR price to $1,877 (in the “all privately insured; all hospital inpatient” scenario) at a WTP threshold of $50,000 per QALY. This represents a 250% increase in the current price. At a WTP threshold of $100,000 per QALY, assuming all procedures to be inpatient with a 50:50 distribution between Medicare and private insurance, the cost of i-FACTOR could theoretically be increased 70-fold while maintaining cost effectiveness (Supplementary Table 10).
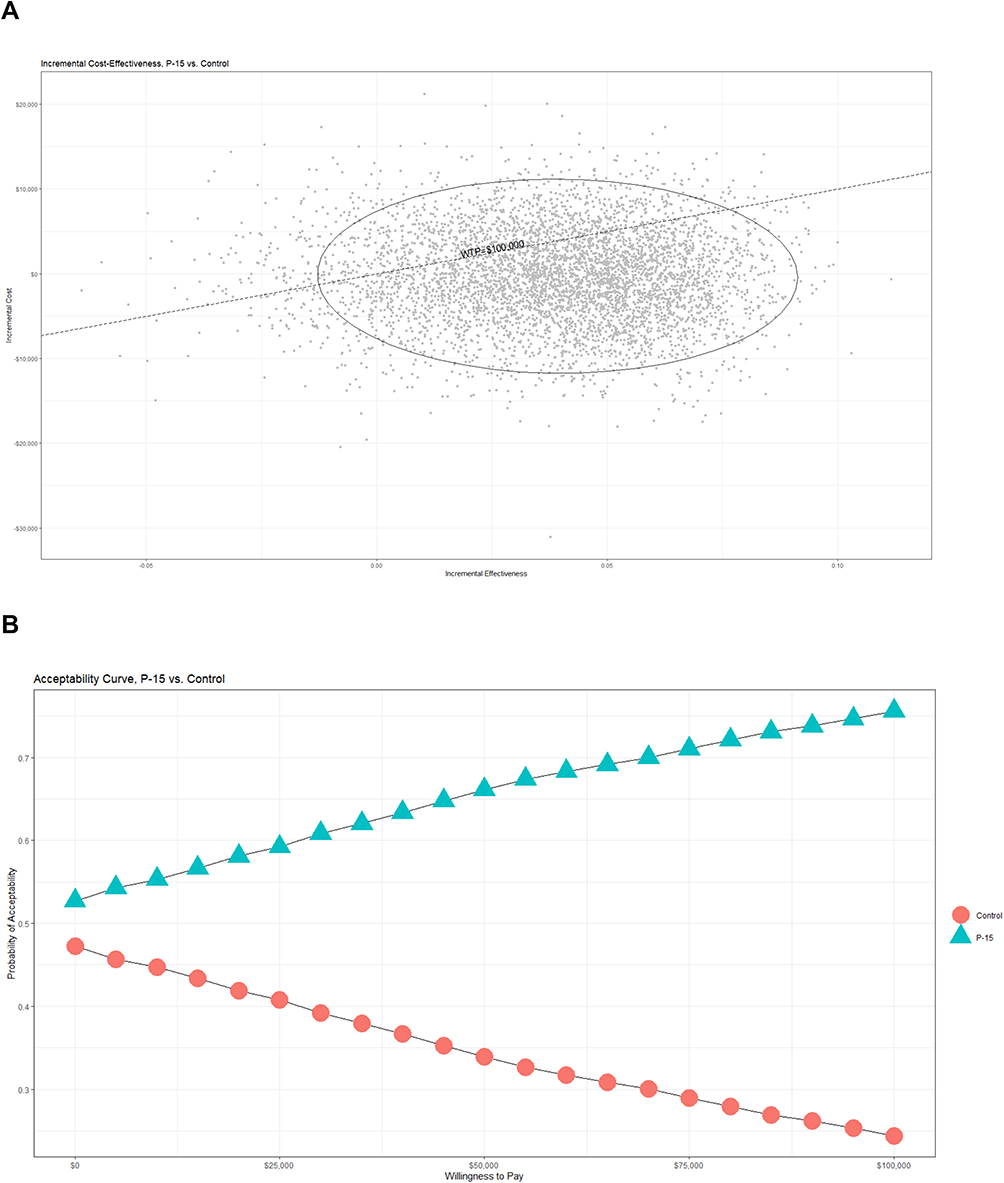 |
Figure 2 (A) Cost-effectiveness scatter plot representing 5,000 simulated iteration of input parameter variations. The resultant difference in increments of cost vs effectiveness is illustrated. Simulation points below the WTP line indicate cost-effectiveness. (B) Cost-effectiveness acceptability curves created based on the sensitivity analysis scatter plot. Percentages of iterations achieving cost-effectiveness are plotted for either group based on willingness-to-pay thresholds. Abbreviation: WTP, willingness-to-pay. |
Discussion
In this landmark study, i-FACTOR was clearly cost-effective compared to local autograft in ACDF surgery. Arguably, the choice of bone graft plays a critical role in ACDF surgery. This decision takes into consideration numerous variables, such as patient age, bone quality, smoking status, comorbidities, and number of levels. Understandably, local autograft has been the gold standard for decades. This sentiment, however, is largely based on expert opinion, a cursory understanding of pecuniary implications, short follow-up, and anecdotal data. Furthermore, there is frequently insufficient local bone to adequately fill an interbody cage, meaning a substitute or extender is often used. Randomized controlled trials have increasingly assisted surgeons, patients, and payers in deciding safety, efficacy, and cost-effectiveness.10 Despite this, highly detailed CEAs comparing novel technologies to presumed standards are limited. i-FACTOR has already demonstrated safety and improved outcomes compared to local autograft.11,13–15 This comprehensive cost-effective analysis was the critical next and necessary step, providing clear support for a better alternative to autograft.
The evolution of ACDF has been remarkable. Use of autologous iliac crest bone graft fell out of favor due to local pain and complications, but also due to increasing availability of alternative grafts believed to provide similar efficacy while reducing operative times. Prior research demonstrated that ACDF with allograft yielded a cost-utility benefit of $496 per QALYs over ACDF with autograft.16 In our model, i-FACTOR proved superior to autograft with an ICER of $13,333 per QALY at 90-days, well below the commonly accepted $100,000 per QALY WTP ceiling. The ICER became negative thereafter, suggesting economic dominance, a notion that greater benefit is afforded at less cost.
Despite numerous bone graft products available on the market today, until i-FACTOR, only bone morphogenetic protein (rhBMP2) had been supported by Level 1 clinical data.17–19 The benefits of rhBMP2 as a biologically superior conduit for new bone formation and fusion highlighted the potential in this space. In early studies, it was felt that the significant upfront cost of rhBMP2 were offset by lower rates of recurrent surgery.19 Unfortunately, over time, the increased risk of local hematoma, ectopic bone formation, seroma, and swelling, led to a decrease and virtual cessation of its use in cervical spine surgery.5 In contrast, the latest RCT data11 complemented by this CEA, suggests that i-FACTOR offers an optimal solution. As shown previously, both i-FACTOR and autograft groups were anticipated to have fusion rates of greater than 90% at two years.11 Similarly, the risks of minor complications were not significantly different despite the autograft group having more re-interventions (Supplementary Table 8). The averaged weighting of this complication difference is best illustrated in the ICER tornado diagram (Supplementary Figure 2). To ensure the robustness of the model, it was rigorously tested in different clinical and payer settings and all demonstrated cost-effectiveness and NMB gains, even at unrealistically low WTP-thresholds of $50,000 per QALY (Table 4 and Supplementary Table 6). To further support this conclusion, a threshold analysis suggested that i-FACTOR fell well below current pricing and societal tolerances (Supplementary Table 10). At its current price, i-FACTOR remains less than half the average cost for rhBMP2 while achieving similar fusion rates with fewer complications.19
It is critical that this analysis be considered in the context of its limitations. As with other complex statistical approaches, the Markov model is conditional on the present state alone; future and past events are independent. With disease processes, it is rarely plausible to assume that a patient’s transition to another health state was entirely independent of a previous health state. The model also assumed that surgical cohorts began in similar health states, which is likely acceptable because of the trial randomization and nonsignificant differences in baseline characteristics. We also recognize that some cost data were not ascertainable. As it is problematic to use hospital charge data to conduct a cost-effective analysis, we used Medicare and Humana DRG/APC rates as representations of public and private payers. As a result, differences in parameters (such as operating room time and length of stay) were not captured. Medication-related costs were estimated from the average wholesale price (0.85), as updated Medicare average sales prices are not publicly available. Although this estimate is considered appropriate, it is impossible to determine if it overestimated or underestimated costs for both groups. Productivity loss was also a significant contributor to cost, but this analysis was unable to include factors such as transportation costs, caregiver time/responsibilities, and educational days missed. Lastly, the authors have disclosed a conflict of interest since the analysis of the IDE RCT data that contributed to this study was funded by industry. The authors feel confident, however, that their analysis, interpretation of the data, and creation of this manuscript was independent of industry and that this ultimately mitigates bias and provides appropriate equipoise.
Despite these limitations, the data supporting i-FACTOR’s use in ACDF surgery appears compelling. This novel drug-device combination product (P-15 peptide and ABM) achieves fusion rates similar to autograft with a statistically significant increase in overall clinical success, thereby mitigating direct and indirect costs. A dominant economic strategy is a rarity in healthcare. The novel i-FACTOR is highly cost-effective early and quickly achieves economic dominance in almost all scenarios tested. In the emerging and rapidly expanding field of value-based medicine there will be an increased demand for these analyses, ensuring surgeons are empowered to make the best, most sustainable, solutions for their patients and for society.
Disclosure
Dr Amir Vokshoor reports Globus Spine Cervical Disc Implant royalties. The analysis of IDE trial data to conduct a cost-effectiveness evaluation of the i-factor product was funded by Cerapedics Inc. Cerapedics directly paid Dr. Ament’s healthcare economics think-tank, Neuronomics LLC. Cerapedics did not have input regarding the creation, critical revision, or fundamental production of this manuscript.
References
1. Passias PG, Marascalchi BJ, Boniello AJ, et al. Cervical spondylotic myelopathy: national trends in the treatment and peri-operative outcomes over 10 years. J Clin Neurosci. 2017;42:75–80. doi:10.1016/j.jocn.2017.04.017
2. Cloward RB. The anterior approach for removal of ruptured cervical disks. J Neurosurg. 1958;15(6):602–617. doi:10.3171/jns.1958.15.6.0602
3. Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958;40(3):607–624. doi:10.2106/00004623-195840030-00009
4. Buser Z, Brodke DS, Youssef JA, et al. Synthetic bone graft versus autograft or allograft for spinal fusion: a systematic review. J Neurosurg Spine. 2016;25(4):509–516. doi:10.3171/2016.1.SPINE151005
5. Carragee EJ, Hurwitz EL, Weiner BK. A critical review of recombinant human bone morphogenetic protein-2 trials in spinal surgery: emerging safety concerns and lessons learned. Spine J. 2011;11(6):471–491. doi:10.1016/j.spinee.2011.04.023
6. Bhatnagar RS, Qian JJ, Wedrychowska A, Sadeghi M, Wu YM, Smith N. Design of biomimetic habitats for tissue engineering with P-15, a synthetic peptide analogue of collagen. Tissue Eng. 1999;5(1):53–65. doi:10.1089/ten.1999.5.53
7. Qian JJ, Bhatnagar RS. Enhanced cell attachment to anorganic bone mineral in the presence of a synthetic peptide related to collagen. J Biomed Mater Res. 1996;31(4):545–554. doi:10.1002/(SICI)1097-4636(199608)31:4<545::AID-JBM15>3.0.CO;2-F
8. Fatima G, Shivamurthy R, Thakur S, Baseer MA. Evaluation of anorganic bovine-derived hydroxyapatite matrix/cell binding peptide as a bone graft material in the treatment of human periodontal infrabony defects: a clinico-radiographic study. J Indian Soc Periodontol. 2015;19(6):651–658. doi:10.4103/0972-124X.164766
9. Arnold PM, Sasso RC, Janssen ME, et al. Efficacy of i-factor bone graft versus autograft in anterior cervical discectomy and fusion: results of the prospective, randomized, single-blinded food and Drug Administration Investigational Device Exemption Study. Spine. 2016;41(13):1075–1083. doi:10.1097/BRS.0000000000001466
10. Ament JD, Kim KD. Standardizing cost-utility analysis in neurosurgery. Neurosurg Focus. 2012;33(1):E4. doi:10.3171/2012.4.FOCUS1288
11. Arnold PM, Sasso RC, Janssen ME, et al. i-factor bone graft vs autograft in anterior cervical discectomy and fusion: 2-year follow-up of the randomized single-blinded Food and Drug Administration Investigational Device Exemption Study. Neurosurgery. 2018;83(3):377–384. doi:10.1093/neuros/nyx432
12. Sanders GD, Neumann PJ, Basu A, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. 2016;316(10):1093–1103. doi:10.1001/jama.2016.12195
13. Lauweryns P, Raskin Y. Prospective analysis of a new bone graft in lumbar interbody fusion: results of a 2- year prospective clinical and radiological study. Int J Spine Surg. 2015;9. doi:10.14444/2002
14. Jacobsen MK, Andresen AK, Jespersen AB, et al. Randomized double blind clinical trial of ABM/P-15 versus allograft in noninstrumented lumbar fusion surgery. Spine J. 2020;20(5):677–684. doi:10.1016/j.spinee.2020.01.009
15. Mobbs RJ, Maharaj M, Rao PJ. Clinical outcomes and fusion rates following anterior lumbar interbody fusion with bone graft substitute i-FACTOR, an anorganic bone matrix/P-15 composite. J Neurosurg Spine. 2014;21(6):867–876. doi:10.3171/2014.9.SPINE131151
16. Angevine PD, Zivin JG, McCormick PC. Cost-effectiveness of single-level anterior cervical discectomy and fusion for cervical spondylosis. Spine. 2005;30(17):1989–1997. doi:10.1097/01.brs.0000176332.67849.ea
17. Baskin DS, Ryan P, Sonntag V, Westmark R, Widmayer MA. A prospective, randomized, controlled cervical fusion study using recombinant human bone morphogenetic protein-2 with the CORNERSTONE-SR allograft ring and the ATLANTIS anterior cervical plate. Spine. 2003;28(12):
18. Buttermann GR. Prospective nonrandomized comparison of an allograft with bone morphogenic protein versus an iliac-crest autograft in anterior cervical discectomy and fusion. Spine J. 2008;8(3):426–435. doi:10.1016/j.spinee.2006.12.006
19. Ackerman SJ, Mafilios MS, Polly DW
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.