Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Cost-Effectiveness of Blinatumomab Plus Chemotherapy vs Chemotherapy in Adults Newly Diagnosed with Philadelphia-Negative B-Cell Acute Lymphoblastic Leukemia in Italy
Authors Ghetti G ![]() , Castello L, Odonde LA, De Fazio S, Stella A, Bruno A, Marchionne E, Bonifacio M
, Castello L, Odonde LA, De Fazio S, Stella A, Bruno A, Marchionne E, Bonifacio M
Received 19 February 2026
Accepted for publication 20 May 2026
Published 12 June 2026 Volume 2026:18 599644
DOI https://doi.org/10.2147/CEOR.S599644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xing Lin Feng
Gianni Ghetti,1 Luca Castello,1 Linet Awino Odonde,1 Serena De Fazio,2 Andrea Stella,2 Angela Bruno,3 Emanuele Marchionne,3 Massimiliano Bonifacio4
1Department of Health Economics and Outcomes Research, AdRes, Turin, Italy; 2Department of Value & Access, Amgen Italy srl, Milan, Italy; 3Department of Medical Affairs, Amgen Italy srl, Milan, Italy; 4Department of Engineering for Innovation Medicine, University of Verona, Verona, Italy
Correspondence: Gianni Ghetti, Department of Health Economics and Outcomes Research, AdRes, Via Cervino 75, Turin, 10155, Italy, Tel +39 011 76 51 239, Email [email protected]
Background: While chemotherapy is the standard treatment for adults with newly diagnosed Philadelphia chromosome-negative (Ph-) B-cell precursor acute lymphoblastic leukemia (ALL), long-term remission remains difficult to achieve. Blinatumomab, an immunotherapy drug, has shown survival benefits when alternated with consolidation chemotherapy in patients with CD19-positive Ph- B-cell ALL, but its economic value had not been assessed in Italy.
Methods: This study evaluated the cost-effectiveness of alternating blinatumomab with standard consolidation chemotherapy compared with chemotherapy alone, using data from the ECOG-ACRIN E1910 Phase III trial. A model was developed to estimate lifetime health outcomes and costs from the perspective of the Italian National Health Service.
Results: Patients who received blinatumomab lived on average 5.06 years longer and gained 4.56 more quality-adjusted life years, but incurred higher healthcare costs, with an incremental cost of € 165,401 per patient, primarily due to drug acquisition. The incremental cost-effectiveness ratio (ICER) was € 36,261 per quality-adjusted life year gained, within the range of values typically considered acceptable in Italy. These results were confirmed in sensitivity analyses, with the ICER ranging from € 28,082 to € 49,034 under various assumptions.
Conclusion: The alternation of blinatumomab with chemotherapy provides a substantial clinical benefit at a cost that is likely acceptable to the Italian healthcare system. These findings support the value of blinatumomab in improving outcomes in adult patients newly diagnosed with Ph- CD19-positive B-cell ALL. Results were consistent across sensitivity analyses, supporting the robustness of the findings.
Keywords: consolidation phase, frontline therapy, CD19-positive, health economic evaluation, incremental cost-effectiveness ratio, QALY
Introduction
Acute lymphoblastic leukemia (ALL) is a blood cancer that affects the bone marrow, leading to the overproduction of lymphoblasts (immature white blood cells), also referred to as leukemia blasts.1 In Europe, approximately 1.3 per 100,000 adults are diagnosed with ALL each year, making it a rare condition among adults.2 Despite favorable responses to induction chemotherapy, long-term remission remains challenging in adults because of high rates of relapses.3 ALL is further classified into B-cell and T-cell categories, with B-cell ALL comprising up to 75% of cases in adults.4
Treatment of newly diagnosed ALL generally includes three phases: induction (including intensification), consolidation, and maintenance therapy. These regimens typically consist of a mixture of anti-neoplastic agents that aim to eradicate hyperproliferation of progenitor cells and restore hemopoiesis through synergistic mechanisms of action.5
Blinatumomab is a bispecific T-cell engager molecule that activates endogenous T-cells by connecting CD3 antigen in the T-cell receptor complex with CD19 on benign and malignant B-cells, leading to T-cell proliferation and B-cell apoptosis.6–8 The European Medicines Agency (EMA) has recently recommended extending the indications for blinatumomab to include its use as a consolidation therapy for patients with newly diagnosed Philadelphia chromosome-negative (Ph-) CD19-positive B-cell precursor ALL, regardless of minimal residual disease (MRD) status.8 This recommendation was supported by findings from the ECOG-ACRIN E1910 trial (ClinicalTrials.gov number: NCT02003222), a phase III clinical trial that included patients with newly diagnosed Ph- B-cell precursor ALL between 30 and 70 years old. In the E1910 trial, patients received two cycles of induction chemotherapy followed by one cycle of intensification. Patients were then assessed for complete remission and MRD response. Patients without MRD (MRD-) were then randomized to receive either consolidation with blinatumomab alternating with chemotherapy or chemotherapy alone. The trial showed superior overall survival (OS; hazard ratio for death, 0.41; 95% confidence interval [CI], 0.23 to 0.73) and relapse-free survival (RFS; hazard ratio for relapse or death, 0.53; 95% CI, 0.32 to 0.87) in the blinatumomab arm compared to chemotherapy alone.9
Although clinical evidence supports the benefit of blinatumomab in patients with newly diagnosed Ph- B-cell precursor ALL who are MRD-, little is known about its cost-effectiveness. In Italy, reimbursement and pricing decisions are increasingly informed by health economic evidence to support the efficient allocation of healthcare resources within the National Health Service (NHS). Therefore, country-specific cost-effectiveness analyses are essential to inform decision-making and ensure the sustainability of innovative therapies in clinical practice. To date, economic evaluations of blinatumomab have primarily focused on relapsed/refractory or pediatric populations, and evidence in the consolidation setting for newly diagnosed adult patients remains limited. To address this gap, we conducted a cost-effectiveness analysis in the Italian setting, comparing blinatumomab alternating with consolidation chemotherapy (blinatumomab + SoC) versus chemotherapy alone (SoC), using data from the E1910 trial (Amgen, Clinical Study Report, unpublished data, 2023).
Materials and Methods
Model Design
In line with the latest blinatumomab submission to National Institute for Health and Care Excellence (NICE),10 the cost-effectiveness model was designed as a three-state partitional survival model comprising three mutually exclusive health states: RFS, post-relapse survival (PRS), and death (Supplemental Figure 1).
All patients entered the model in the RFS state and could thereafter transition to either the PRS or death states. Patients in the PRS state were assumed to have relapsed and moved on to second-line (2L) treatment. Patients in the PRS state could either stay within the PRS state, or transition to the death state.
The three-state model was deemed appropriate to describe the clinical pathway as it allowed the direct use of the RFS and OS outcomes of the E1910 trial.
The consolidation chemotherapy regimen used in the trial was based on the UKALL XII/ECOG E2993 protocol, which reflects the US clinical practice. This differs in some aspects from the Italian approach, as described in the LAL1913 trial conducted by the Gruppo Italiano Malattie EMatologiche dell’adulto (GIMEMA).11 Despite the differences, the chemotherapy regimen from the E1910 trial was used in the analysis for three main reasons: (i) to ensure methodological and statistical consistency between the efficacy data and drug consumption; (ii) the reasonable assumption that cost differences between the two regimens are negligible, as both involve low-cost drugs included within the national Diagnosis-Related Group (DRG) tariffs, which cover both drug acquisition and administration; and (iii) the clinical equivalence of the two regimens, as recently demonstrated in a matching-adjusted indirect comparison (MAIC) analysis.12
While cure has not been formally defined in treatment guidelines, patients who remain in remission for around 3 to 5 years are perceived to have achieved a cure.13 To account for the possibility of deep clinical remission, survival was modelled using mixture cure models (MCMs). This approach aligns with the plateau observed in the E1910 trial Kaplan-Meier (KM) curves for RFS and OS of blinatumomab + SoC and SoC from 48 and 72 months onwards, respectively, suggesting that patients were cured and at a low risk of relapse and ALL-related death.
The analysis was conducted from the Italian NHS perspective over a lifetime, 50-year time horizon. A weekly model cycle length was considered to accommodate chemotherapy regimens with varying cycle durations. While treatment is administered over relatively short periods, the lifetime time horizon was adopted to capture the long-term impact of treatment on survival outcomes (RFS and OS), which extend well beyond the treatment duration. A half-cycle correction was applied, assuming that transitions between health states occur at mid-cycle. Both costs and effectiveness – life years (LYs) and quality-adjusted life years (QALYs) – were discounted at 3.0% annually, as per national guidance.14 This assumption was tested in the scenario analyses. All costs are presented as 2025 values. A summary of key model parameters is presented in Table 1.
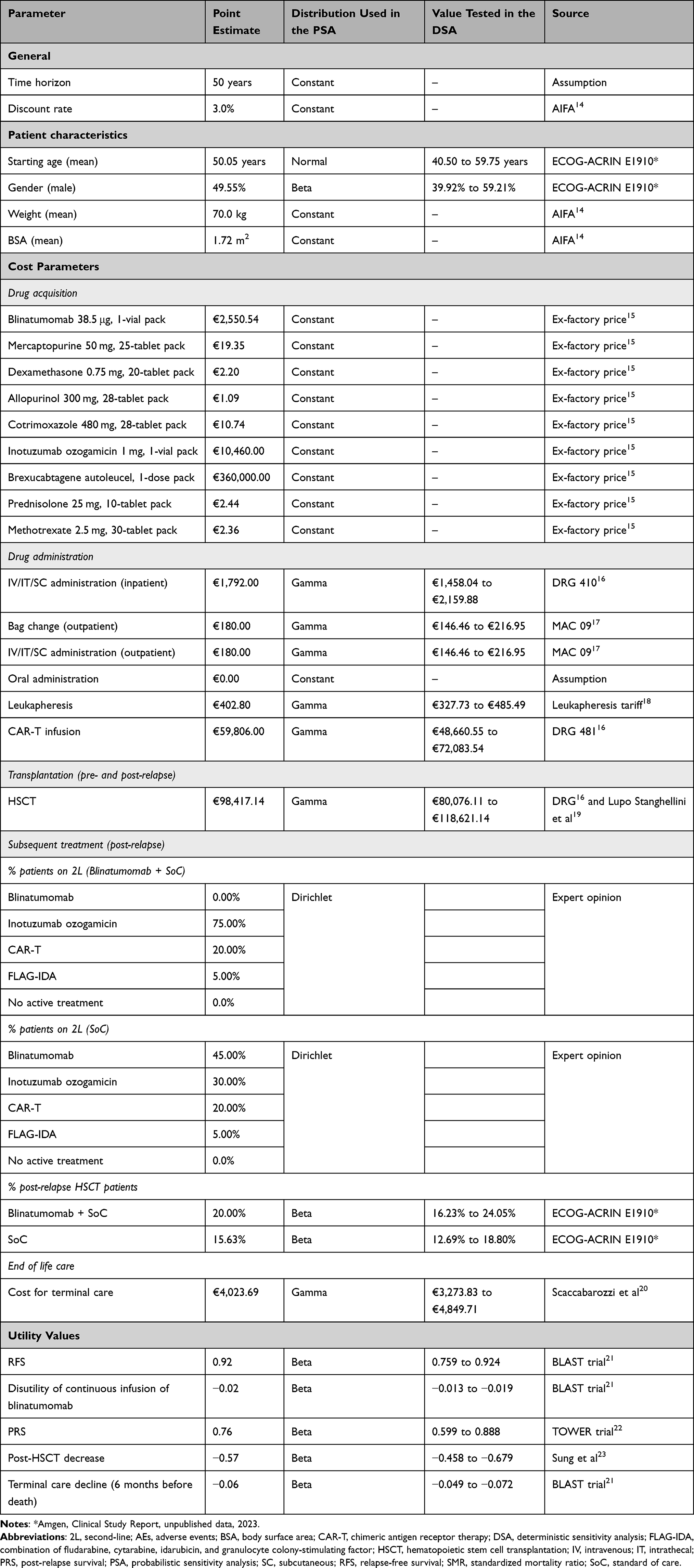 |
Table 1 Summary of Key Model Input Parameters |
Clinical Input
The model inputs were based on data from the phase III E1910 trial, which enrolled 488 patients in total, of whom 224 were randomized in the MRD- population to receive blinatumomab alternating with consolidation chemotherapy or chemotherapy alone.9 Survival inputs (RFS and OS) and drug consumption data used in the model were derived from this population.
Although the survival data from the E1910 trial were sufficiently long to inform short- to medium-term clinical outcomes, they did not provide information beyond the follow-up period. Therefore, extrapolation of survival beyond the trial period was necessary to estimate long-term survival. The trial data indicated that a group of patients achieved durable treatment remission. Consequently, MCMs were considered to inform long-term survival, in line with NICE recommendations.24
In MCMs, survival is modelled by estimating an implicit “cure fraction” (ie the proportion of patients “cured”). The survival of patients who are “cured” was then modelled assuming age- and gender-matched Italian population mortality,25 adjusted by a standardized mortality ratio (SMR) of 1.0926,27 to account for any potential lingering complications due to ALL disease or hematopoietic stem cell transplantation (HSCT). The impact of this assumption was further evaluated in the scenario analysis. The survival of non-cured patients was modelled using a parametric survival model. The “flexsurvcure” R package was used to fit MCMs.28,29
A range of criteria were used to select from the fitted RFS and OS distributions, including clinical plausibility, visual inspection, and goodness-of-fit, using the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). The same distribution was applied across both arms for the same endpoint for consistency in the assumption that different distributions make about the shape of the hazard rate. When assessing for proportional hazards, the proportional hazards assumption was not met, and therefore, the survival curves by treatment arm were fitted separately. The log-normal MCM and Weibull MCM were selected for modelling RFS and OS, respectively, in the base case, based on their good statistical and visual fits and clinical plausibility. The modelled RFS and OS curves for the base case are presented in Figure 1.
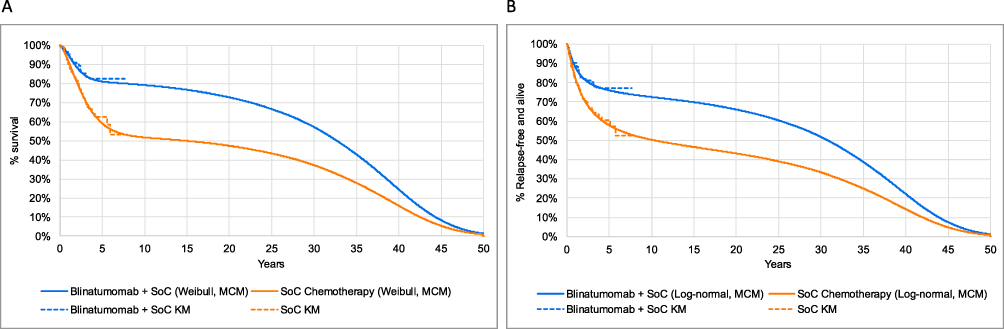 |
Figure 1 Long-term extrapolations. (A) Overall survival. (B) Relapse-free survival. Abbreviations: KM, Kaplan-Meier; MCM, mixture cure models; SoC, standard of care. |
Further details on distribution fitting and clinical input data are provided in Supplemental Table 1, Supplemental Tables 5–8 and Supplemental Figures 2–5.
Utilities
As health-related quality-of-life data were not collected in the E1910 trial, utility values were based on the BLAST trial, a Phase II study of blinatumomab in ALL adult patients with MRD, and estimated using Italian tariffs.30 A decrement of 0.016 was applied to patients on blinatumomab to account for any disutility due to continuous intravenous (IV) infusion and a terminal decrement of −0.060 was applied for patients within 6 months of death.
As post-relapse utility assessments were limited in the BLAST trial,21 utility values of patients who were receiving salvage chemotherapy in the TOWER trial,22 a phase III randomized trial of blinatumomab versus chemotherapy in relapsed/refractory Ph- B-cell ALL adult patients, were used instead. The utilities from BLAST and TOWER were assumed to reasonably represent the quality of life of the modelled population.
Considering the lifetime horizon of the model, the age- and sex-matched general population utilities31 were included to account for the deterioration in health-related quality of life as patients age. Additionally, patients were assumed to switch to general population utilities after five years, as they were considered clinically cured and thus no longer experiencing reduced utilities due to ALL disease. The impact of this assumption was further evaluated in the scenario analysis.
Furthermore, the analysis included the impact of adverse events (AEs) on quality of life by adjusting for utility decrements associated with these events and their duration. The data for utility decrements were primarily sourced from literature and previous submissions to NICE. Utility decrements were applied as a one-off reduction in the first cycle of the model. For further details, please refer to Supplemental Table 1.
Finally, patients who had received HSCT were assumed to incur utility decrements to reflect known AEs or complications associated with HSCT. A utility decrement of −0.57 was applied for one year, as reported in the literature23 and in line with previous NICE submissions.26,27 The HSCT-related disutility was applied as a one-off reduction in the first cycle of the model for the proportion of patients who received HSCT pre-relapse. For patients who received HSCT post-relapse, the HSCT-related disutility was applied as a one-off decrement at the time of relapse.
Cost Inputs
This analysis was conducted from the perspective of the Italian NHS, considering only direct healthcare costs, including drug acquisition and administration costs for consolidation and maintenance, HSCT, subsequent therapies, AE management, and terminal care. Patients remaining in remission for five years were considered clinically cured and therefore no longer incurred ALL-related costs from five years onwards.
Drug Acquisition and Administration
The ex-factory price net of mandatory discounts was used to determine drug acquisition costs.15 For chemotherapy drugs administered via IV, subcutaneous (SC), or intrathecal (IT) injection, the acquisition cost was assumed to be included in the administration tariff. This was estimated using the DRG 41027 tariff for inpatient infusion and the MAC 0917 tariff for outpatient delivery. The MAC 09 tariff was also used to value the cost of changing the blinatumomab bag. Finally, it was assumed that the administration costs for blinatumomab also included pump acquisition, maintenance, and consumable costs. In the event multiple drugs were administered on the same day, a single administration cost was applied. For drugs requiring oral administration, the administration cost was assumed to be zero.
For those drugs whose dosage depends on body surface area (BSA) or weight, an average BSA of 1.72 m2 and an average weight of 70 kg were considered, in line with national guidelines.14 The analysis also considered drug wastage for drugs administered intravenously (ie, no vial sharing was assumed).
For consolidation therapy, drug acquisition and administration costs were corrected by the observed proportion of patients starting each cycle of treatment in the E1910 trial, to ensure that the modelled costs matched actual drug consumption This observed treatment use already accounted for patients discontinuing due to relapse and therefore was modelled independently from RFS. To best reflect clinical practice, the model conservatively assumed one full vial of blinatumomab per administration. Given that opened vials can only be stored for a short period of time and the limited number of patients eligible for blinatumomab therapy in Italy, it is not expected that the content of opened vials would be reused by hospitals.
In line with the E1910 protocol, patients were assumed to receive blinatumomab infusion in an inpatient setting for the first three days during the first cycle and for the first two days of each subsequent cycle. In the remaining days of each cycle, patients were assumed to require one bag change every four days, in an outpatient setting. For consolidation chemotherapy cycles, patients treated with blinatumomab + SoC were assumed to require hospitalization for administration for the first two days of each chemotherapy cycle. The remaining chemotherapy drugs were administered in the outpatient setting. Patients treated with SoC alone were assumed to receive treatment in an inpatient setting for the first three days of the first consolidation cycle, and during the first two days of each subsequent cycle. Thereafter, all SoC drugs were administered in the outpatient setting.
Upon completion of consolidation therapy, patients in both treatment arms were assumed to go on to receive maintenance therapy for up to 2.5 years or until relapse. The dosing and administration schedule of maintenance chemotherapy used in the model followed the E1910 trial protocol. Maintenance chemotherapy was assumed to be administered exclusively in the outpatient setting.
Further details on the dosing and administration schedule are provided in Supplemental Table 2.
Hematopoietic Stem Cell Transplantation
In line with the E1910 trial (Amgen, Clinical Study Report, unpublished data, 2023), 22.3% of patients treated with blinatumomab + SoC and 25.0% treated with SoC were assumed to undergo HSCT in the RFS phase. The cost of HSCT was estimated using Italian tariffs16 and the literature.19 This cost was applied as a one-time cost in the first cycle of the model.
Subsequent Therapies
Upon relapse, patients were eligible to receive subsequent treatment with either blinatumomab, inotuzumab ozogamicin, chemotherapy, or chimeric antigen receptor (CAR)-T cell therapy. Further details on drug posology are provided in Supplemental Table 3. The proportion of patients receiving these therapies by treatment arm was based on clinician feedback.
In addition to the therapies described, the analysis assumed that patients may also receive HSCT. In line with the E1910 trial (Amgen, Clinical Study Report, unpublished data, 2023), it was assumed that 20.0% and 15.6% of patients received HSCT after blinatumomab + SoC and after SoC, respectively. As patients may potentially receive any of the subsequent therapies as a bridge to HSCT, HSCT costs were calculated in addition to the subsequent therapy costs. The cost of the post-relapse transplant was assumed equal to the pre-relapse cost.
All second-line treatment costs were applied as a one-off cost at the time of relapse to patients who relapsed at each model cycle.
Management of Adverse Events
The model included all AEs of Grade ≥3 that occurred in ≥5% of patients in either treatment arm, as events not meeting these criteria were considered to have a minimal impact on costs. While Grade ≥3 cytokine release syndrome (CRS) occurred in less than 5% of patients, it was included in the model as it was associated with high resource consumption. Safety data were obtained from the E1910 trial.
The mean per-patient cost for AE management was calculated by multiplying the frequency of each event by its corresponding management cost, derived from the relevant literature32,33 or national tariffs.16,18 For AE that did not require hospitalization, it was assumed that a specialist consultation would be sufficient. Further details on safety data and AE management costs are provided in Supplemental Table 1.
End of Life
All patients who died before the defined cure timepoint (five years) were assumed to incur a one-time terminal care cost, applied at the time of death. Given that patients who survive beyond this cure timepoint were considered long-term survivors, it was assumed that these patients would not incur the costs of terminal care, in line with a previous NICE submission.26 In the absence of Italian data on terminal care for adult patients with ALL, literature data20 were used.
Sensitivity Analyses
A deterministic sensitivity analysis (DSA) was conducted to examine the sensitivity of the model results to the lower and upper parameter estimates, in order to identify those with the greatest impact on the incremental cost-effectiveness ratio (ICER). Only inputs that could vary independently were included, and for this reason, survival parameters were not varied in the DSA. Where possible, CI was used to estimate the lower and upper parameter bounds. In the absence of data, the upper (97.5th percentile) and lower (2.5th percentile) bounds tested in the DSA were calculated assuming a standard error (SE) of 10% of the base case value. The DSA results are presented as a tornado diagram, where the top ten parameters with the greatest impact on the ICER are reported.
To assess the impact of the combined uncertainty of all parameters on the ICER, a probabilistic sensitivity analysis (PSA) was also conducted. In the PSA 1,000 iterations of the model were performed, each time varying the values of the parameters simultaneously and randomly according to their assigned probabilistic distributions and recalculating the results for each iteration. The PSA results are presented as scatter plots on the incremental cost-effectiveness plane displaying the distribution of outcomes, and on a cost-effectiveness acceptability curve (CEAC), which provides the probability that, for a given willingness-to-pay (WTP) threshold, the treatment is cost-effective.
Uncertainties around the assumptions in the cost-effectiveness model were examined through scenario analyses (Supplemental Table 4). Key model assumptions or parameters were modified for each analysis, and the corresponding results were tabulated.
Results
Base Case Analyses
In the base case, blinatumomab + SoC was associated with substantial clinical benefits, with gains of 5.06 LYs and 4.56 QALYs, at an incremental cost of €165,401 compared with SoC alone.
When considering a lifetime horizon, patients receiving blinatumomab + SoC were estimated to achieve 17.50 LYs and 15.22 QALYs, compared to 12.44 LYs and 10.66 QALYs for those receiving SoC alone (Table 2). The overall treatment costs associated with blinatumomab + SoC were estimated to be higher than those for SoC alone (€314,416 vs €149,014), primarily due to incremental drug acquisition costs. However, blinatumomab + SoC was also predicted to generate savings with respect to maintenance therapy, HSCT, subsequent therapies, and end of life. Notably, costs for subsequent therapies were reduced by more than 50%. The ICER for blinatumomab + SoC compared to SoC alone was estimated to be €36,261 per QALY gained.
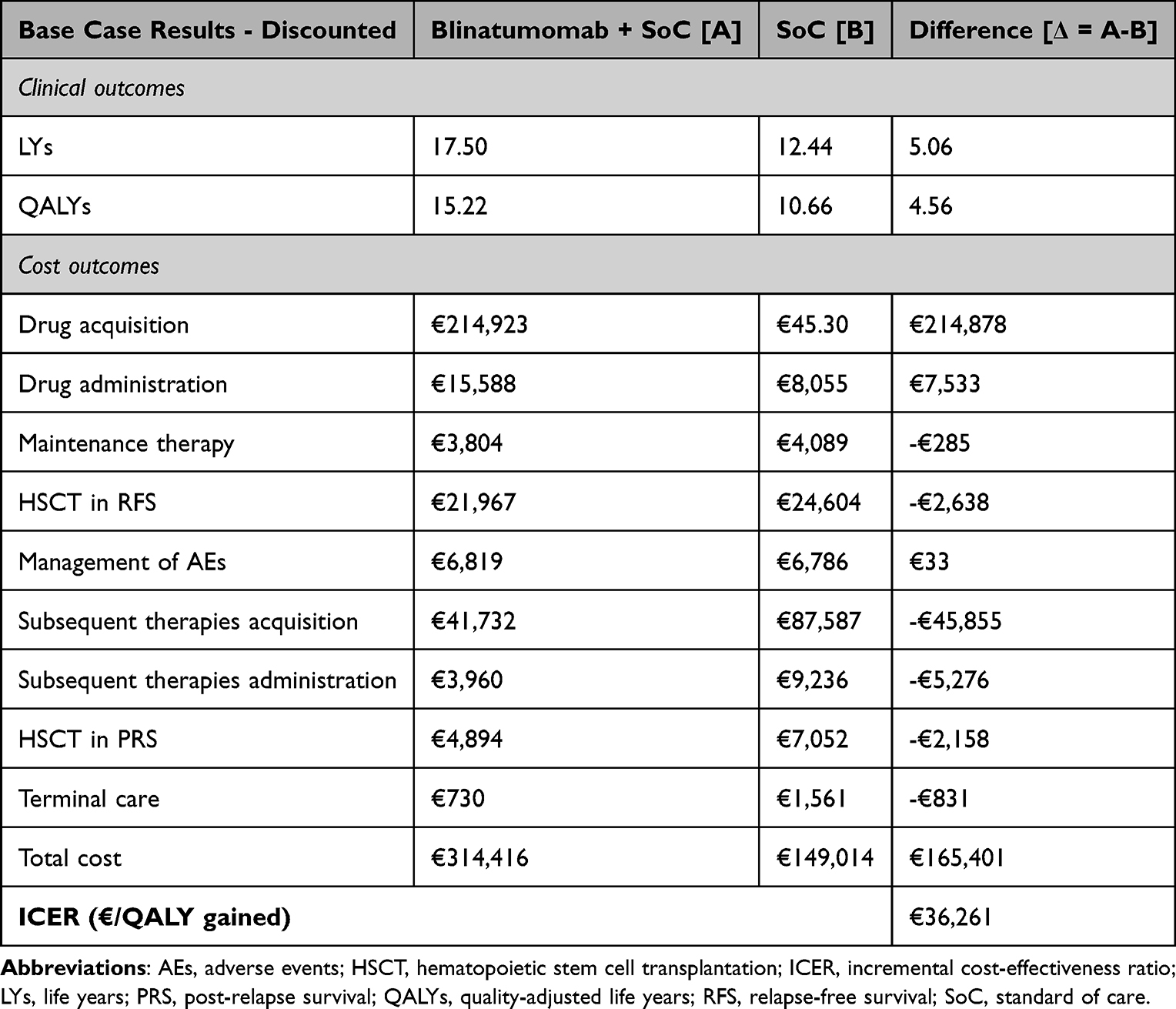 |
Table 2 Base Case Analysis results |
Sensitivity Analyses
Among the ten parameters with the greatest impact on the ICER in the DSA (Figure 2), patient age was the most influential parameter. This is because increasing/decreasing the age reduced/increased the estimated gains in LYs and, consequently, in QALYs, while costs remained largely unaffected. The overall effect was an increase/decrease in the estimated ICER.
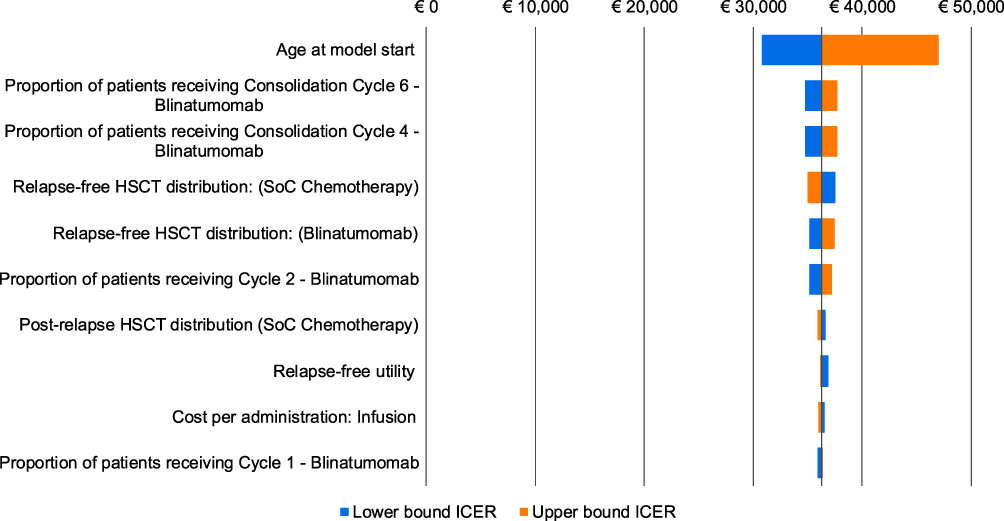 |
Figure 2 Deterministic sensitivity analysis results. Tornado diagram representing incremental cost-effectiveness ratio variations. Abbreviations: ICER, incremental cost-effectiveness ratio; SoC, standard of care. |
The mean ICER of €37,588 per QALY gained obtained from the PSA was very close to the base-case deterministic ICER and all (100%) simulations fell within the north-east quadrant, indicating that blinatumomab + SoC was more effective and more expensive than SoC alone (Figure 3A). The probability of blinatumomab + SoC being cost-effective compared to SoC alone was estimated to be 21.70%, 45.50%, and 63.30% at a WTP threshold of €30,000, €36,000, and €42,000 per QALY, respectively (Figure 3B). These thresholds are consistent with values reported in the Italian context for reimbursed medicines and reflect commonly used benchmarks for decision-making in the absence of an official national threshold.34
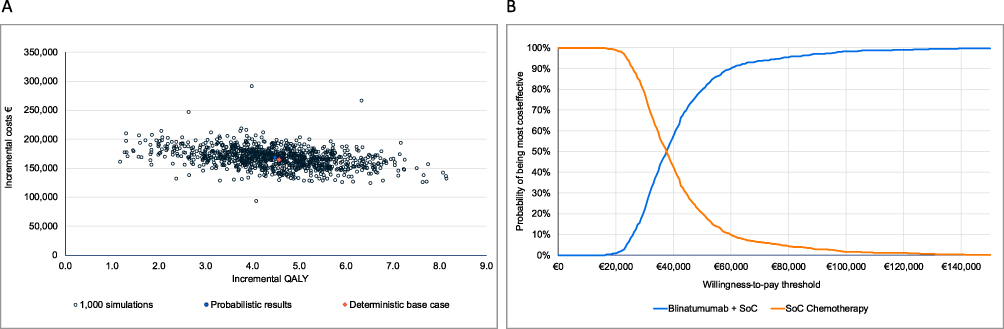 |
Figure 3 Probabilistic sensitivity analysis results. (A) Incremental cost-effectiveness plane. (B) Cost-effectiveness acceptability curve. Abbreviations: PSA, probabilistic sensitivity analysis; QALY, quality-adjusted life years; SoC, standard of care; WTP, willingness-to-pay. |
The investigated scenarios yielded ICERs ranging from €28,082 to €49,034 per QALY gained (Table 3). The lowest ICER value of €28,082 per QALY gained was obtained considering a 1.5% discount rate; with a 5% discount rate the ICER was €49,034 per QALY gained. Notably, the assumptions regarding the parametric distribution used to extrapolate efficacy data beyond the trial follow-up had minimal impact on the estimated ICER. These findings confirmed the base case results.
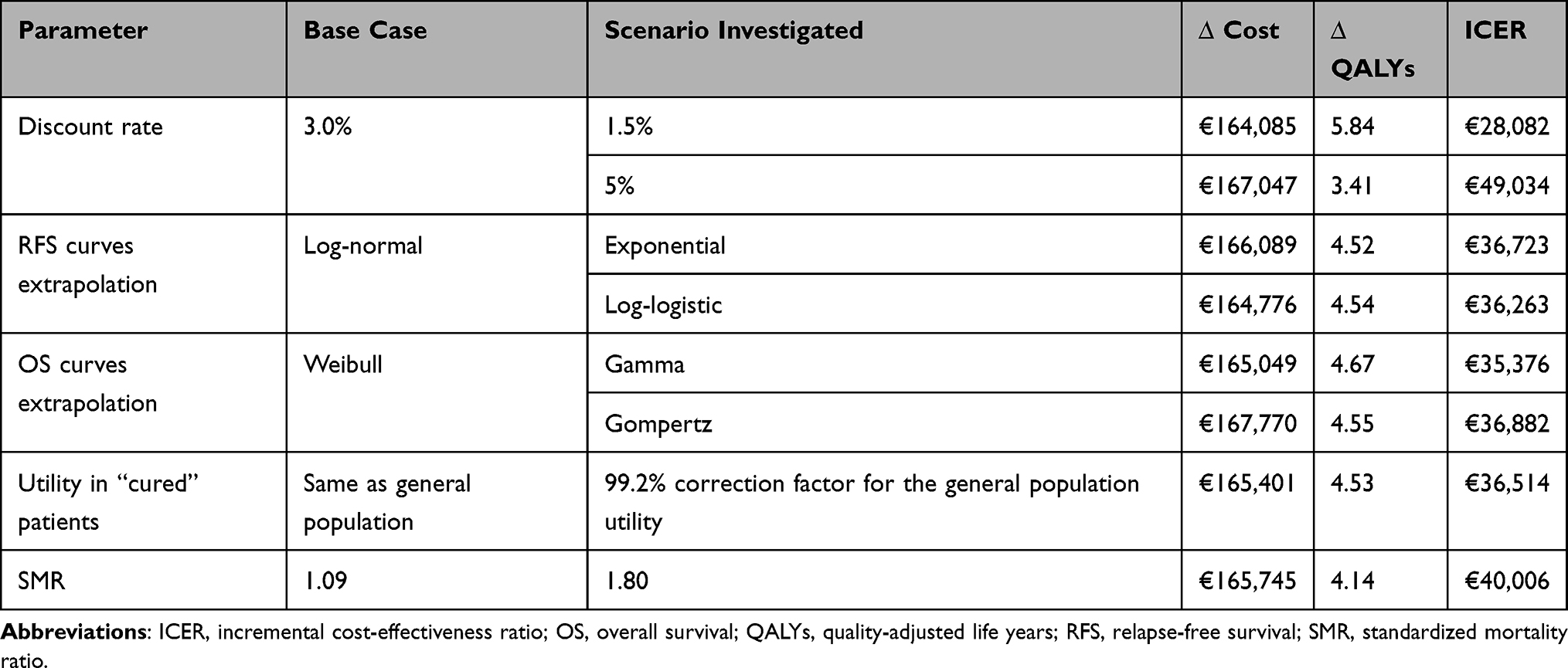 |
Table 3 Scenario Analysis Results |
Discussion
The E1910 trial, conducted in patients with newly diagnosed Ph- B-cell precursor ALL who are MRD-, demonstrated that blinatumomab alternating with chemotherapy prolonged OS and improved RFS compared to chemotherapy alone.9 To assess the long-term clinical and economic outcomes of blinatumomab + SoC versus SoC alone in this patient population, a cost-effectiveness analysis was conducted. The analysis was based on data from the E1910 trial and considered a lifetime horizon of 50 years. The evaluation was conducted from the perspective of the Italian NHS.
In the base case, blinatumomab + SoC was associated with incremental costs of €165,401, mainly attributable to increased drug acquisition costs. This increase was accompanied by substantial clinical benefits, with patients experiencing an additional 5.06 LYs and 4.56 QALYs. The resulting ICER was €36,261 per QALY gained. Although Italy lacks a formal WTP threshold, the estimated ICER is in line with a recent Italian study reporting an average ICER of €33,000 per QALY gained (range: €22,637 – €44,218 per QALY gained) across 48 reimbursed medicines.34 Sensitivity and scenario analyses confirmed the robustness of the base-case results.
The analysis considered chemotherapy consolidation as defined by the UKALL XII/ECOG E2993 protocol. Although variations exist across countries in the standard-of-care chemotherapy regimens for this patient population, a recent study demonstrated that the Italian GIMEMA LAL1913 protocol yielded comparable outcomes, supporting the clinical equivalence of the two regimens.12 In the E1910 trial, patients were stratified by intent to receive HSCT, yet the criteria for proceeding to HSCT may differ by country. For instance, in the Italian clinical practice, HSCT eligibility is determined by a risk model integrating clinical characteristics and post-induction MRD. As a result, the proportion and clinical profile of patients undergoing HSCT in Italian practice may not fully reflect those observed in the E1910 trial. Specifically, among B-cell ALL patients with MRD <10−4 at the end of induction/intensification (ie TP2) in the GIMEMA LAL1913 trial, those with baseline very high features were 22% (19 out of 85). An HSCT realization rate of approximately 50%, as observed in recent Italian trials,11,35 suggests that the number of MRD- patients actually undergoing transplant in Italy could be around 10 to 15%. These differences may potentially influence both clinical and economic outcomes of treatment strategies. In the analysis we used HSCT rates observed in the trial to preserve consistency with the clinical data and avoid introducing additional uncertainty.
To the best of our knowledge, this is the first published cost-effectiveness analysis of blinatumomab in the consolidation setting for newly diagnosed Ph- B-cell ALL who are MRD-. Previous economic evaluations have focused on relapsed/refractory or pediatric patients,36–41 and no further analyses were identified in the literature for this specific setting.
The analysis employed a model structure consistent with the recent submission to NICE. However, limitations should be considered when interpreting the results. First, the model relied on a partitioned survival approach, which – while widely used in oncology – does not explicitly model the interdependencies among clinical events such as response, relapse, and overall survival. As a result, it may not fully capture the dynamic and sequential nature of disease progression, potentially affecting the precision of long-term projections. Second, while the model incorporated long-term survival data from the E1910 trial, uncertainties remain around the extrapolation of survival beyond the observed follow-up. Survival extrapolation inherently involves assumptions about long-term outcomes, which – even when supported by expert opinion – may not fully reflect real-world experience. Finally, because health-related quality of life data was not collected in E1910, utility values were sourced from the BLAST and TOWER trials to inform pre- and post-relapse health states in the modelled population.
Despite these potential uncertainties, extensive sensitivity and scenario analyses were conducted to assess the impact of key parameters and assumptions. The results demonstrated limited variability in the ICER, which ranged from €28,082 to €49,034 per QALY gained in the scenarios investigated, supporting the robustness of the base-case analysis.
From a policy and reimbursement perspective, these findings provide evidence to support the inclusion of blinatumomab as a consolidation option for adult patients with newly diagnosed Ph− CD19-positive B-cell precursor ALL who are MRD- within the Italian NHS. The results are particularly noteworthy in the context of orphan medicines. Although Italy does not apply a formal cost-effectiveness threshold, the estimated ICER of €36,261 per QALY gained was consistent with the value of €37,157 per QALY gained reported for reimbursed orphan drugs in Italy.34 These results may therefore inform national and regional reimbursement assessments, formulary inclusion, and clinical pathway planning within the Italian NHS. Future real-world evidence and broader value assessments, including elements highlighted in the ISPOR Value Flower framework42 may further clarify the long-term economic and societal impact of blinatumomab in Italian clinical practice.
Conclusion
The analysis demonstrated that blinatumomab alternating with chemotherapy compared to chemotherapy alone offered significant clinical benefits in patients with newly diagnosed Ph- CD19-positive B-cell ALL who are MRD-, at an incremental cost consistent with acceptable thresholds in the Italian healthcare context. Reduced costs for subsequent therapies, along with substantial gains in life expectancy and quality-adjusted survival, support the value of blinatumomab in this patient population. Although Italy does not have an officially defined national willingness-to-pay threshold, the resulting ICER is consistent with WTP value reported in the literature for reimbursed orphan drugs in the Italian context,34 providing additional support for the economic viability of this treatment strategy in Italy. Sensitivity analyses confirmed the robustness of these findings. These findings should be interpreted in light of the modelling limitations, such as long-term survival extrapolation and the use of utility inputs derived from external sources. Future evaluations incorporating broader value elements, including societal and innovation impacts, could further elucidate the comprehensive benefits of blinatumomab.
Abbreviations
2L, Second-line treatment; AE, Adverse event; AIC, Akaike information criterion; AIFA, Italian Medicines Agency (Agenzia Italiana del Farmaco); ALL, Acute lymphoblastic leukemia; BIC, Bayesian information criterion; BSA, Body surface area; CAR-T, Chimeric antigen receptor T-cell; CEAC, Cost-effectiveness acceptability curve; CI, Confidence interval; CRS, Cytokine release syndrome; DRG, Diagnosis-related group; DSA, Deterministic sensitivity analysis; EMA, European Medicines Agency; GIMEMA, Gruppo Italiano Malattie EMatologiche dell’Adulto; HSCT, Hematopoietic stem cell transplantation; ICER, Incremental cost-effectiveness ratio; IT, Intrathecal; IV, Intravenous; KM, Kaplan–Meier; LYs, Life years; MAIC, Matching-adjusted indirect comparison; MCM, Mixture cure model; MRD, Minimal residual disease; NHS, National Health Service; NICE, National Institute for Health and Care Excellence; OS, Overall survival; Ph, Philadelphia chromosome; PRS, Post-relapse survival; PSA, Probabilistic sensitivity analysis; QALYs, Quality-adjusted life years; RFS, Relapse-free survival; SC, Subcutaneous; SE, Standard error; SMR, Standardized mortality ratio; SoC, Standard of care; WTP, Willingness-to-pay.
Data Sharing Statement
The data are available from the corresponding authors on a reasonable request.
Ethics
This study relied exclusively on previously collected data and did not involve the recruitment of patients. All clinical inputs used in the model were derived from the phase III ECOG-ACRIN E1910 study, which was conducted in accordance with the Declaration of Helsinki and approved by the relevant institutional review boards (ClinicalTrials.gov number: NCT02003222). Therefore, ethical committee approval was not required and both the Declaration of Helsinki and patient consent were not relevant for this work.
Acknowledgments
We would like to thank Flavia Giacalone, from SEEd srl, who provided journal styling services. Editorial services were funded by Amgen.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Study and medical writing assistance were funded by Amgen. The funder (Amgen Italy S.r.l.) had a role in the study design, modelling analysis, data interpretation, supervision of the manuscript development in accordance with the ICMJE criteria, and took part in the decision to publish findings in concertation with all authors. Publication of the study results was not contingent on the funder’s approval or censorship.
Disclosure
GG, LC, and LAO are employees of AdRes which has received project funding from Amgen. SDF, AS, AB, and EM are employees and stockholders of Amgen. MB has received advisory board fees from Amgen, Ascentage Pharma, Blueprint Medicines, Bristol Myers Squibb, Glaxo Smith Kline, Incyte, Novartis, Pfizer. LC reports project funding from Amgen SpA, during the conduct of the study; Project fundings from Roche SpA, Sanofi SpA, Novartis SpA, and Johnson and Johnson, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Leukaemia Foundation. Acute lymphoblastic leukaemia (ALL). Available from: https://www.leukaemia.org.au/blood-cancer/types-of-blood-cancer/leukaemia/acute-lymphoblastic-leukaemia/.
2. European Society for Medical Oncology. Clinical Practice Guideline: Acute Lymphoblastic Leukaemia | ESMO. Available from: https://www.esmo.org/guidelines/esmo-clinical-practice-guideline-acute-lymphoblastic-leukaemia.
3. Jabbour E, O’Brien S, Konopleva M, Kantarjian H. New insights into the pathophysiology and therapy of adult acute lymphoblastic leukemia. Cancer. 2015;121(15):2517–14. doi:10.1002/cncr.29383
4. Shilpa P, Hagop K, Jabbour EJ. Adult acute lymphoblastic leukemia. Available from: https://www.mayoclinicproceedings.org/article/S0025-6196(16)30584-5/pdf.
5. Malard F, Mohty M. Acute lymphoblastic leukaemia. Lancet Lond Engl. 2020;395(10230):1146–1162. doi:10.1016/S0140-6736(19)33018-1
6. Zhu M, Wu B, Brandl C, et al. Blinatumomab, a Bispecific T-cell Engager (BiTE(®)) for CD-19 targeted cancer immunotherapy: clinical pharmacology and its implications. Clin Pharmacokinet. 2016;55(10):1271–1288. doi:10.1007/s40262-016-0405-4
7. Jabbour E, Düll J, Yilmaz M, et al. Outcome of patients with relapsed/refractory acute lymphoblastic leukemia after blinatumomab failure: no change in the level of CD19 expression. Am J Hematol. 2018;93(3):371–374. doi:10.1002/ajh.24987
8. European Medicines Agency. Blincyto. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/blincyto.
9. Litzow MR, Sun Z, Mattison RJ, et al. Blinatumomab for MRD-Negative Acute Lymphoblastic Leukemia in Adults. N Engl J Med. 2024;391(4):320–333. doi:10.1056/NEJMoa2312948
10. National Institute for Health and Care Excellence. Blinatumomab with chemotherapy for consolidation treatment of Philadelphia-chromosome-negative CD19-positive minimal residual disease-negative B-cell precursor acute lymphoblastic leukaemia | guidance | TA1049. Available from: https://www.nice.org.uk/guidance/ta1049.
11. Bassan R, Chiaretti S, Della Starza I, et al. Pegaspargase-modified risk-oriented program for adult acute lymphoblastic leukemia: results of the GIMEMA LAL1913 trial. Blood Adv. 2023;7(16):4448–4461. doi:10.1182/bloodadvances.2022009596
12. Piciocchi A, Marsili G, Messina M, et al. Comparative efficacy of the GIMEMA LAL1913 standard chemotherapy protocol versus the standard arm of the E1910 trial in MRD-negative Ph-negative ALL: a MAIC analysis. Present EHA 2025. Available from: https://library.ehaweb.org/eha/2025/eha2025-congress/4160455/.
13. Gidman W, Shah S, Zhang L, et al. Clinicians’ perspectives on cure in adult patients with acute lymphoblastic leukemia with minimal residual disease: a Delphi Study. Adv Ther. 2019;36(11):3017–3029. doi:10.1007/s12325-019-01099-x
14. AIFA. Linee guida AIFA per la compilazione del dossier a supporto della domanda di rimborsabilità e prezzo di un medicinale.
15. Codifa - L’Informatore Farmaceutico. Available from: https://www.codifa.it/.
16. Ministero della salute. Remunerazione prestazioni di assistenza ospedaliera per acuti, assistenza ospedaliera di riabilitazione e di lungodegenza post acuzie e di assistenza specialistica ambulatoriale. Decreto 10/2012 pubblicato in GU Serie Generale n.23 del 28-1-2013. 2013.
17. Regione Lombardia. DELIBERAZIONE N° IX / 2946; 2012.
18. Ministero della Salute. Definizione delle tariffe relative all’assistenza specialistica ambulatoriale e protesica. Decreto 11/2024 pubblicato in GU Serie Generale n.302 del 27-12-2024; 2024.
19. Lupo Stanghellini M, Rossi A, Bianchi L, et al. Direct costs in 4-years post allogeneic transplant follow-up: a comparative analysis of 15 matched patients with and without GvHD. Blood. 2019;130(1):5488. doi:10.1182/blood.V130.Suppl_1.5488
20. Scaccabarozzi G, Limonta F, Amodio E. Hospital, local palliative care network and public health: how do they involve terminally ill patients? Eur J Public Health. 2016;ckw152. doi:10.1093/eurpub/ckw152
21. Gökbuget N, Dombret H, Bonifacio M, et al. Blinatumomab for minimal residual disease in adults with B-cell precursor acute lymphoblastic leukemia. Blood. 2018;131(14):1522–1531. doi:10.1182/blood-2017-08-798322
22. Kantarjian H, Stein A, Gökbuget N, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med. 2017;376(9):836–847. doi:10.1056/NEJMoa1609783
23. Sung L, Buckstein R, Doyle JJ, Crump M, Detsky AS. Treatment options for patients with acute myeloid leukemia with a matched sibling donor: a decision analysis. Cancer. 2003;97(3):592–600. doi:10.1002/cncr.11098
24. Rutherford MJ, Lambert PC, Sweeting MJ, et al. NICE DSU TECHNICAL SUPPORT DOCUMENT 21.
25. Italian National Institute of Statistics. Demographic Statistics in Italy. Available from: https://demo.istat.it/.
26. National Institute for Health and Care Excellence. Tisagenlecleucel for treating relapsed or refractory B-cell acute lymphoblastic leukaemia in people 25 years and under. Available from: https://www.nice.org.uk/guidance/ta975/chapter/1-Recommendations.
27. National Institute for Health and Care Excellence. Autologous anti-CD19-transduced CD3+ cells for treating relapsed or refractory B-cell acute lymphoblastic leukaemia in people 26 years and over. Available from: https://www.nice.org.uk/guidance/ta893/documents/129.
28. Latimer NR. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: inconsistencies, limitations, and a practical guide. Med Decis Mak Int J Soc Med Decis Mak. 2013;33(6):743–754. doi:10.1177/0272989X12472398
29. Jordan A. Flexsurvcure: flexible parametric cure models 2025. Available from: https://cran.r-project.org/web/packages/flexsurvcure/flexsurvcure.pdf.
30. Scalone L, Cortesi PA, Ciampichini R, et al. Italian population-based values of EQ-5D health states. Value Health. 2013;16(5):814–822. doi:10.1016/j.jval.2013.04.008
31. Scalone L, Cortesi PA, Ciampichini R, Cesana G, Mantovani LG. Health related quality of life norm data of the Italian general population: results using the EQ-5D-3L and EQ-5D-5L instruments. Epidemiol Biostat Public Health. 2022;12(3). doi:10.2427/11457
32. Lazzaro C, Bordonaro R, Cognetti F, et al. An Italian cost-effectiveness analysis of paclitaxel albumin (nab-paclitaxel) versus conventional paclitaxel for metastatic breast cancer patients: the COSTANza study. Clin Outcomes Res. 2013:125. doi:10.2147/CEOR.S41850
33. Mickisch G, Gore M, Escudier B, Procopio G, Walzer S, Nuijten M. Costs of managing adverse events in the treatment of first-line metastatic renal cell carcinoma: bevacizumab in combination with interferon-α2a compared with sunitinib. Br J Cancer. 2010;102(1):80–86. doi:10.1038/sj.bjc.6605417
34. Russo P, Zanuzzi M, Carletto A, Sammarco A, Romano F, Manca A. Role of Economic Evaluations on Pricing of Medicines Reimbursed by the Italian National Health Service. PharmacoEconomics. 2023;41(1):107–117. doi:10.1007/s40273-022-01215-w
35. Bassan R, Chiaretti S, Della Starza I, et al. Up-front blinatumomab improves MRD clearance and outcome in adult Ph- B-lineage ALL: the GIMEMA LAL2317 Phase 2 study. Blood. 2025;145(21):2447–2459. doi:10.1182/blood.2024027500
36. Delea TE, Amdahl J, Boyko D, et al. Cost-effectiveness of blinatumomab versus salvage chemotherapy in relapsed or refractory Philadelphia-chromosome-negative B-precursor acute lymphoblastic leukemia from a US payer perspective. J Med Econ. 2017;20(9):911–922. doi:10.1080/13696998.2017.1344127
37. Caillon M, Brethon B, van Beurden-Tan C, et al. Cost-effectiveness of blinatumomab in pediatric patients with high-risk first-relapse B-Cell precursor acute lymphoblastic leukemia in France. PharmacoEconomics - Open. 2023;7(4):639–653. doi:10.1007/s41669-023-00411-4
38. Diaz martinez JP, de Maraumont TA, Camacho LM, Garcia L. Cost-effectiveness of blinatumomab for the treatment of B‑precursor acute lymphoblastic leukemia pediatric patients with high‑risk first‑relapse in Mexico. Leuk Res. 2024;145:107560. doi:10.1016/j.leukres.2024.107560
39. Gye A, Goodall S, De Abreu Lourenco R. Cost-effectiveness analysis of tisagenlecleucel versus blinatumomab in children and young adults with acute lymphoblastic leukemia: partitioned survival model to assess the impact of an outcome-based payment arrangement. PharmacoEconomics. 2023;41(2):175–186. doi:10.1007/s40273-022-01188-w
40. Wakase S, Teshima T, Zhang J, et al. Cost-effectiveness analysis of tisagenlecleucel for the treatment of pediatric and young adult patients with relapsed or refractory B Cell acute lymphoblastic leukemia in Japan. Transplant Cell Ther. 2021;27(3):241.e1–241.e11. doi:10.1016/j.jtct.2020.12.023
41. Lin JK, Lerman BJ, Barnes JI, et al. Cost effectiveness of chimeric antigen receptor T-Cell therapy in relapsed or refractory pediatric B-Cell acute lymphoblastic leukemia. J Clin Oncol off J Am Soc Clin Oncol. 2018;36(32):3192–3202. doi:10.1200/JCO.2018.79.0642
42. Neumann PJ, Garrison LP, Willke RJ. The history and future of the “ISPOR value flower”: addressing limitations of conventional cost-effectiveness analysis. Value Health J Int Soc Pharmacoeconomics Outcomes Res. 2022;25(4):558–565. doi:10.1016/j.jval.2022.01.010
43. Maurer MJ, Ghesquières H, Jais JP, et al. Event-free survival at 24 months is a robust end point for disease-related outcome in diffuse large B-cell lymphoma treated with immunochemotherapy. J Clin Oncol off J Am Soc Clin Oncol. 2014;32(10):1066–1073. doi:10.1200/JCO.2013.51.5866
44. Swinburn P, Lloyd A, Nathan P, Choueiri TK, Cella D, Neary MP. Elicitation of health state utilities in metastatic renal cell carcinoma. Curr Med Res Opin. 2010;26(5):1091–1096. doi:10.1185/03007991003712258
45. Howell TA, Matza LS, Jun MP, Garcia J, Powers A, Maloney DG. Health state utilities for adverse events associated with chimeric antigen receptor T-Cell therapy in Large B-cell lymphoma. PharmacoEconomics - Open. 2022;6(3):367–376. doi:10.1007/s41669-021-00316-0
46. Nafees B, Stafford M, Gavriel S, Bhalla S, Watkins J. Health state utilities for non small cell lung cancer. Health Qual Life Outcomes. 2008;6:84. doi:10.1186/1477-7525-6-84
47. Lloyd A, Nafees B, Narewska J, Dewilde S, Watkins J. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683–690. doi:10.1038/sj.bjc.6603326
48. Sullivan PW, Slejko JF, Sculpher MJ, Ghushchyan V. Catalogue of EQ-5D scores for the United Kingdom. Med Decis Mak Int J Soc Med Decis Mak. 2011;31(6):800–804. doi:10.1177/0272989X11401031
49. National Institute for Health and Care Excellence. Daratumumab monotherapy for treating relapsed and refractory multiple myeloma. Technology appraisal guidance Reference number: TA510. Available from: https://www.nice.org.uk/guidance/ta510.
50. National Institute for Health and Care Excellence. Atezolizumab for treating locally advanced or metastatic non-small-cell lung cancer after chemotherapy. Technology appraisal guidance TA520. Available from: https://www.nice.org.uk/guidance/ta520.
51. National Institute for Health and Care Excellence. Osimertinib for treating locally advanced or metastatic EGFR T790M mutation-positive non-small-cell lung cancer. Technology appraisal guidance Reference number: TA416. Available from: https://www.nice.org.uk/guidance/ta416.
52. Tolley K, Goad C, Yi Y, Maroudas P, Haiderali A, Thompson G. Utility elicitation study in the UK general public for late-stage chronic lymphocytic leukaemia. Eur J Health Econ HEPAC Health Econ Prev Care. 2013;14(5):749–759. doi:10.1007/s10198-012-0419-2
53. National Institute for Health and Care Excellence. Gilteritinib for treating relapsed or refractory acute myeloid leukaemia. Technology appraisal guidance Reference number: TA642. Available from: https://www.nice.org.uk/guidance/ta642.
54. National Institute for Health and Care Excellence. Inotuzumab ozogamicin for treating relapsed or refractory B-cell acute lymphoblastic leukaemia. Technology appraisal guidance. Reference number: TA541. Available from: https://www.nice.org.uk/guidance/ta541.
55. Martin PJ, Counts GW, Appelbaum FR, et al. Life expectancy in patients surviving more than 5 years after hematopoietic cell transplantation. J Clin Oncol off J Am Soc Clin Oncol. 2010;28(6):1011–1016. doi:10.1200/JCO.2009.25.6693
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.