Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Cost-Effectiveness Analysis of Fracture Liaison Services Compared with Standard of Care in the Secondary Prevention of Fragility Fractures in Spain
Authors Naranjo A ![]() , Prieto-Alhambra D
, Prieto-Alhambra D ![]() , Sánchez-Martín J, Pérez-Mitru A, Brosa M
, Sánchez-Martín J, Pérez-Mitru A, Brosa M
Received 29 November 2021
Accepted for publication 5 April 2022
Published 22 April 2022 Volume 2022:14 Pages 249—264
DOI https://doi.org/10.2147/CEOR.S350790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Samer Hamidi
Antonio Naranjo,1 Daniel Prieto-Alhambra,2 Julián Sánchez-Martín,3 Alejandro Pérez-Mitru,3 Max Brosa3
1Department of Rheumatology, Hospital Universitario de Gran Canaria Dr. Negrín, Universidad de Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, 35011, Spain; 2NIHR Musculoskeletal Biomedical Research Unit, University of Oxford, Oxford, UK; 3Market Access Area, Pharmalex Spain, Barcelona, Spain
Correspondence: Alejandro Pérez-Mitru, Market Access Area, Pharmalex Spain, C/ Comte d’Urgell, 240, 2-D, Barcelona, 08036, Spain, Tel +34 932 521 377, Fax +34 937 379 984, Email [email protected]
Purpose: To assess the cost-effectiveness of a Fracture Liaison Service (FLS) compared with standard care for the secondary prevention of fragility fractures in Spain.
Methods: Patients with osteoporosis and an initial fragility fracture who were candidates to initiate osteoporosis treatment (mean age 65 years, 90.7% female) were included in the model. Disease progression was simulated with a Markov model through seven health states (with and without osteoporosis treatment, subsequent hip, vertebral, forearm and humerus fracture, and death). A time horizon of 10 years and a 6-month duration per cycle was set. Clinical, economic, and quality of life parameters were estimated from the literature and Spanish clinical practice. Resource use and treatment patterns were validated by an expert panel. The Spanish National Health System (SNS) perspective was adopted, taking direct costs (€; 2020) into account. Effectiveness was measured in life-years gained (LYG) and quality-adjusted life years gained (QALYs). A discount rate of 3% was applied to costs and outcomes. The uncertainty of the parameters was assessed using deterministic, scenario and probabilistic sensitivity analyses (1000 iterations).
Results: Setting up a FLS for the secondary prevention of fragility fractures in Spain would provide better osteoporosis treatment initiation and persistence. This would reduce subsequent fragility fractures, disutilities and deaths. FLS would have greater clinical benefits (0.008 and 0.082 LYG and QALY gained per patient, respectively) and higher costs (€ 563.69 per patient) compared with standard care, leading to an incremental cost-utility ratio of € 6855.23 per QALY gained over the 10 years horizon. The sensitivity analyses showed limited dispersion of the base case results, corroborating their robustness.
Conclusion: From the SNS perspective and considering Spanish willingness-to-pay thresholds, the introduction of FLS for the secondary prevention of fragility fractures would be a cost-effective strategy.
Keywords: economic evaluation, osteoporotic fracture prevention, fracture liaison service, Spain
Introduction
Fragility fractures are caused by a force which does not normally cause fractures, such as a fall from the height of the foot or lower.1 Patients with osteoporosis are likely to have more fragility fractures, given that osteoporosis promotes bone weakness and fragility.1
Fragility fractures and associated complications are a significant healthcare problem, especially considering the aging of the population and the increase in chronic diseases. In Spain, osteoporosis is estimated to affect 32% of women aged >50 years and 52% of those aged >70 years.2 An incidence rate of fragility fractures of 86.9/10,000 person-years in Spain is estimated.3 In 2017, up to 330,000 fragility fractures occurred in Spain, with an estimated associated cost of 4.2 billion euros.4
Subsequent fragility fractures account for a considerable number of hospitalizations and are, therefore, a significant public healthcare problem.5–8 They represent a significant direct healthcare cost attributable to surgeries and associated indirect costs, and may also lead to life-threatening events: 15.8% to 30.0% of patients with osteoporotic hip fracture are estimated to die during the following year due to associated complications.9–11 Fragility fractures are associated with high age- and gender-dependent mortality rates.12 Additionally, any fragility fracture doubles the risk of subsequent fractures.13,14
Fracture Liaison Services (FLS) aim to reduce the risk of new fragility fractures in patients aged ≥ 50 years with a history of fragility fractures,15 by correct identification of the fracture risk, proper pharmacological therapy, patient monitoring and clinical and educational activities whose objective is to increase therapeutic adherence, minimizing the appearance of medication-related errors and, ultimately, reducing the risk of new fragility fractures.
FLS have been shown to improve the management and secondary prevention of fragility fractures, improving bone densitometry (BMD) testing rates, therapeutic initiation and persistence, and significantly reducing the risk of refractures and deaths.16 Many studies have evaluated the efficiency of healthcare interventions aimed at addressing the risk of new fragility fractures. A systematic review of economic evaluations by Wu et al16 showed that FLS are cost-effective strategies for the secondary prevention of fragility fractures in patients with osteoporosis compared with usual clinical management, regardless of the intensity of the program and the geographical or healthcare setting. Therefore, evidence of favorable pharmacoeconomic arguments in terms of efficiency would encourage and support the application and implementation of FLS programs.17
However, no published economic assessments have been identified assessing the efficiency of FLS in Spain. Therefore, this study aimed to evaluate the efficiency of FLS compared with the standard of care (SOC) in the secondary prevention of fragility fractures in Spain.
Materials and Methods
Study Design
A structured literature review was conducted to identify pharmacoeconomic evaluations of FLS, the methodology used, and the main inputs required. A panel of two clinical experts (a rheumatologist and an epidemiologist, with wide experience in the implementation and evaluation of FLS programs and osteoporosis therapy persistence monitoring in Spanish clinical practice), participated in the design of the study, input selection, validation and interpretation of the structural assumptions, in addition to the validation and transferability of the results.
Population and Comparative Treatments
The study population consisted of a hypothetical cohort of patients aged ≥ 50 years with a history of fragility fracture who were either identified by an FLS or received SOC for the secondary prevention of fragility fracture. On one hand, to model the clinical and economic consequences of FLS, data from publications reporting the extensive experience of FLS implementation in the Gran Canaria North healthcare area was included.10,18–20 On the other hand, Spanish clinical data on the persistence of osteoporosis medication were considered to model the clinical and economic consequences of SOC.21,22
Therefore, the study population in both arms of the study was defined as a cohort of patients with fragility fracture who were candidates to initiate osteoporosis treatment, with a mean age of 65 years (range: 52–78 years) and who were 90.7% female (range: 72.5–100%). This was aligned with data from the study by Martín Merino et al, which described the evolution of the pharmacotherapeutic persistence of 95,057 patients who initiated osteoporosis treatment between 2001 and 2013, based on the Database for Pharmacoepidemiologic Research in Primary Care, which contained clinical information from six Spanish healthcare regions representing 8.9% of the Spanish population.22
FLS consisted of an active identification of patients with fragility fracture and, after agreeing to participate, patients are clinically assessed and followed-up. The evaluation included initial nurse and specialist visits to train patients how to manage their disease and medication, and to conduct initial BMD and biochemical tests. Subsequent presential and telematic nurse and specialist follow-up visits were also provided to patients included into FLS. Patients with standard management follow the usual pathway after a fracture, that is emergency department, orthopedics and, in some cases physical therapy. Usually less than 20% of patients initiate a treatment to prevent new fractures,23 are not systematically evaluated and are followed-up in an unstructured manner because usual care is highly dependent on each doctor and each patient.
All inputs considered in the current study were available from the literature and validated through an expert panel. Therefore, this study did not require ethical review board or committee approval neither to obtain patient consent.
Type of Analysis
A cost-effectiveness model was developed to compare the costs (monetary value) and effectiveness (health benefits) of FLS versus SOC in the secondary prevention of fragility fracture. The results were expressed as the incremental cost-effectiveness ratio (ICER), according to the following formula: ICER = (Cost FLS – Cost soc)/(Effectiveness FLS – Effectiveness SOC). Cost FLS and Cost SOC represent the cost associated with FLS and SOC, respectively. Effectiveness FLS and Effectiveness SOC represent the clinical consequences in terms of life years gained (LYG) and quality-adjusted life years (QALY) gained.
Cost-utility analysis was selected mainly because it permits comparisons using QALYs, a homogeneous result measure that unifies the quantity and quality of life gained. The analysis was carried out from the Spanish National Health System (SNS) perspective, considering only direct disease-related healthcare costs. In line with previous economic evaluations of FLS and due to the lack of differential information for each alternative compared, the social perspective was not included.16 In addition, direct healthcare costs have the greatest relevance from the SNS perspective.
Pharmacoeconomic Model
The economic evaluation consisted of two stages. Initially, a decision tree was established to compare treatment initiation and pharmacotherapeutic persistence in the cohort established, through FLS or SOC (Figure 1A). Afterwards, a Markov model estimated the clinical and economic consequences through seven mutually exclusive health states (“Treated with anti-osteoporotic medication”, “Without anti-osteoporotic medication”, “Subsequent hip fracture”, “Subsequent vertebral fracture”, “Subsequent forearm fracture”, “Subsequent humerus fracture” and “Death”), allowing disease progression modeling in terms of subsequent fractures and their respective economic consequences, morbidity, and mortality (Figure 1B).
 |
Figure 1 Model structure. (A) decision tree. (B) Markov model. Abbreviations: FLS, Fracture Liaison Service; Fx, fracture; SOC, standard of care. |
Patients initiated the Markov model in the health state “Treated with anti-osteoporotic medication” or “Without anti-osteoporotic medication” depending on whether they were included in an FLS or not. According to the persistence of pharmacological treatment in each cohort, a probability of subsequent fragility fractures was established. When patients presented subsequent fragility fractures, their transition to the health state “Treated with anti-osteoporotic medication” or “Without anti-osteoporotic medication” was established at the end of the subsequent fragility fracture cycle, depending on whether they were treated in an FLS. The health state “Death” is an absorbing state and transition to this state was estimated from the Spanish general population mortality rates, differentiated according to age and gender,24 and considering an increase in the standardized mortality ratio due to the main reported subsequent fragility fractures.25,26
Time Horizon and Cycle Length
The time horizon of the study was 10 years, aligned with previous FLS economic assessments.16,25–28 According to Spanish methodological recommendations for health technology assessments,29–31 sensitivity analyses were conducted across alternative time horizons. A cycle duration of 6 months was established to resemble the usual monitoring period of osteoporotic patients, which is aligned with specific methodological recommendations for economic evaluations of osteoporosis.32
Discount Rate
Aligned with Spanish recommendations for health technology assessment,29,30 a time-preference discount rate of 3% was applied to costs and health outcomes. According to Spanish methodological recommendations,29–31 sensitivity analyses were conducted through a range of variations in the discount rate.
Clinical Parameters
Effectiveness
The proportion of patients initiating treatment after the fragility fracture was considered differentially in the FLS and SOC groups. For the SOC group, we considered the percentage of antiresorptive treatment prescription at 6 months after the index fracture found in a retrospective study carried out at the University Hospital of Gran Canaria Doctor Negrín (HUGCDN), which included 167 patients treated in the emergency department in October 2012 with a diagnosis of fragility fracture.33 For the FLS group, the percentage was estimated from the degree of eligibility to initiate osteoporosis treatment in patients with fragility fracture according to the 2018 criteria of the Spanish Society of Rheumatology,34 and the degree of FLS acceptability of the HUGCDN.33
The effectiveness of the FLS after a mean follow-up of four years, defined as the relative increase in osteoporosis treatment persistence, was obtained from the study by Ojeda et al,20 which described the clinical benefits attributed to the implementation of a secondary prevention program of fragility fractures by the HUGCDN.
The risk of subsequent fragility fractures was taken from the study by García Renedo et al, in which a cohort of patients with a history of non-surgical fragility fracture was retrospectively assessed over a time horizon of 10 years.21 The risk is assumed to be dependent whether patient are persistent or not to their anti-osteoporotic treatment.
To capture the risk in terms of morbidity and mortality associated with subsequent fragility fractures, in line with previously published economic evaluations,25,26 an increase in the standardized mortality ratio due to the main subsequent fragility fractures described in the literature was established. The main clinical parameters evaluated were validated by the panel of experts (Table 1).
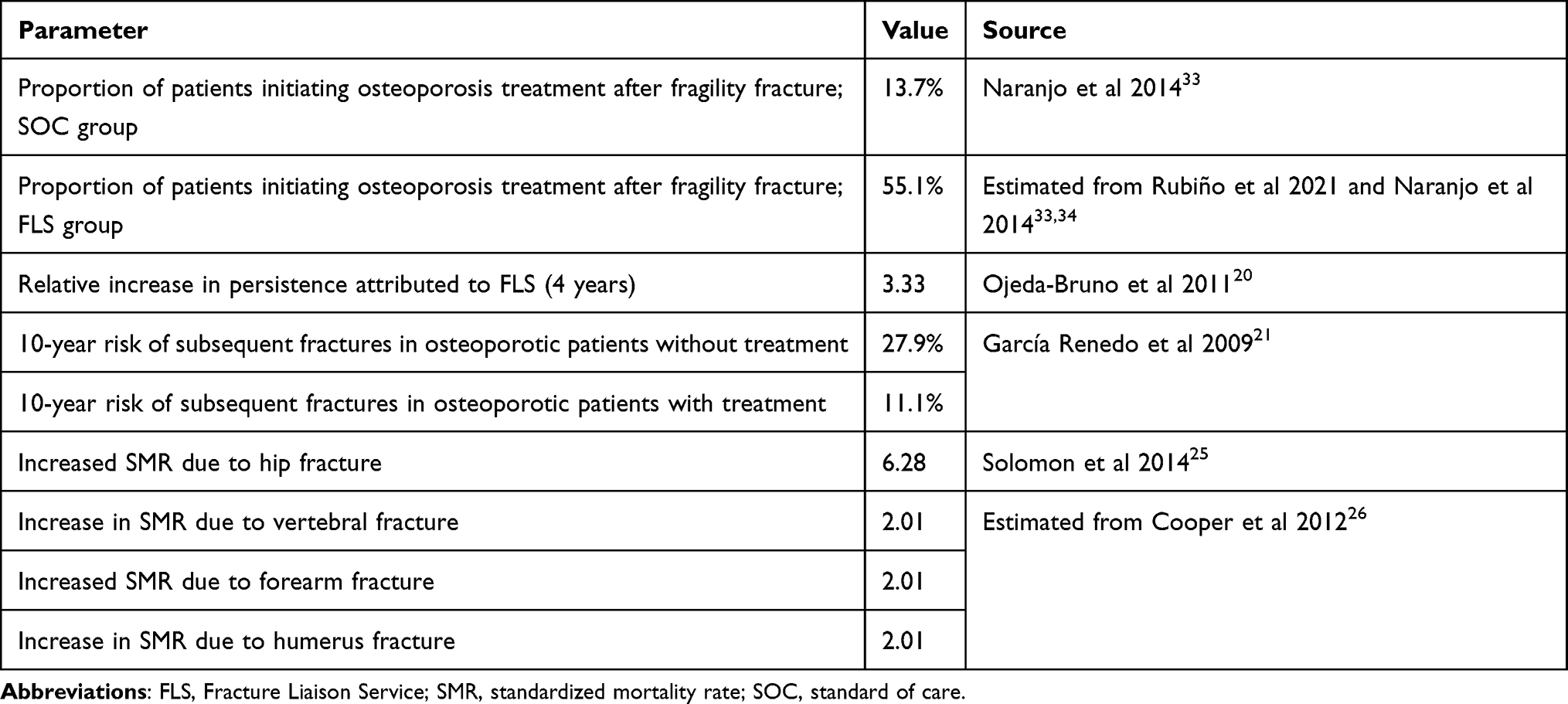 |
Table 1 Clinical Parameters Considered in the Base Case |
Quality of Life
The impact in terms of perceived quality of life was represented by using specific utility values for each health state evaluated on a scale of 0 (death) to 1 (perfect health).
The utility values for the general population were estimated according to the 2014 Spanish National Health Survey by the Spanish National Institute of Statistics.35 Given the lack of Spanish data on the disutilities attributed to the safety and tolerability profile of bisphosphonates, and of subsequent fragility fractures in patients with osteoporosis, these parameters were obtained from previous reports,25,36 and were validated by the expert panel (Table 2).
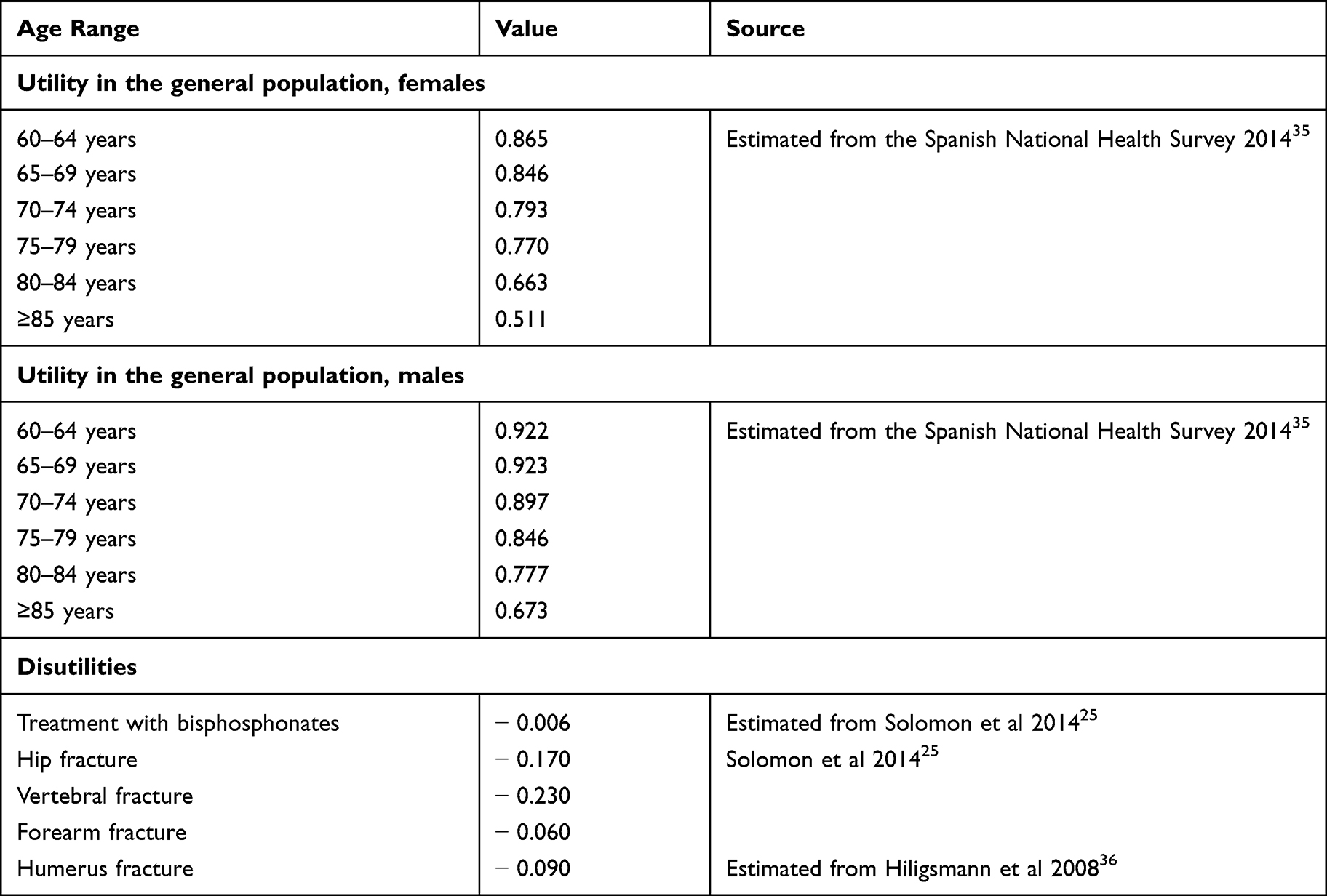 |
Table 2 Utilities and Disutilities Considered in the Base Case |
Resource Use and Costs
In line with Spanish methodological recommendations,29–31 the following categories of direct healthcare costs were considered: healthcare resource use and costs associated with the secondary prevention program of fragility fractures, pharmacological costs associated with osteoporosis therapy, costs attributed to subsequent fragility fractures and end-of-life costs. All costs were expressed in 2020 euros (Table 3).
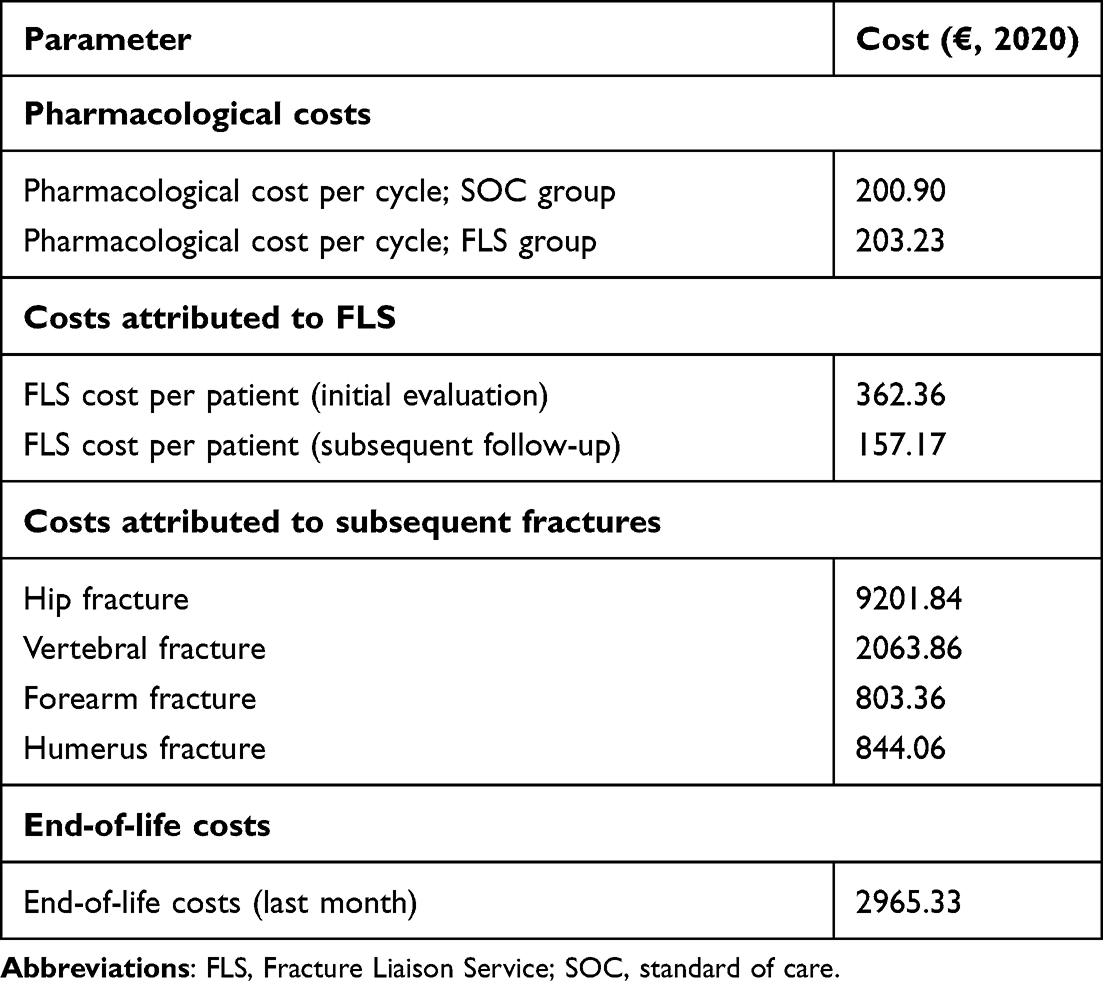 |
Table 3 Economic Parameters Considered in the Base Case |
In line with Spanish methodological recommendations,29–31 the cost of dispensing drugs through community pharmacies was estimated using the retail price,36 applying value added tax (VAT) and the deduction corresponding to Royal Decree Law (RDL) 08/2010.37 The dose was based on the recommendations of the respective Summary of Product Characteristics,37 and the distribution of the treatments was validated by the expert panel (Tables S1 and S2).
The resource use attributed to the FLS was obtained from publications describing the experience of the FLS implemented in the Gran Canaria North healthcare area for the secondary prevention of fragility fractures.10,18,20,38 The degree of real-word applicability of these healthcare resources was validated by the expert panel. Unit costs were identified in Spanish healthcare cost databases (Tables S1 and S2).39,40
The resource use associated with subsequent fragility fractures and the end-of-life were validated by the expert panel and were identified in Spanish healthcare cost databases (Tables S1 and S2).39,40
Sensitivity Analysis
The uncertainty associated with the study variables and the robustness of the results were evaluated using scenario analysis, deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA).
Scenario Analysis
To evaluate the uncertainty inherent in the discrete quantitative parameters, and the structural parameters of the current economic assessment, various scenario analyses were simulated (Table 4).
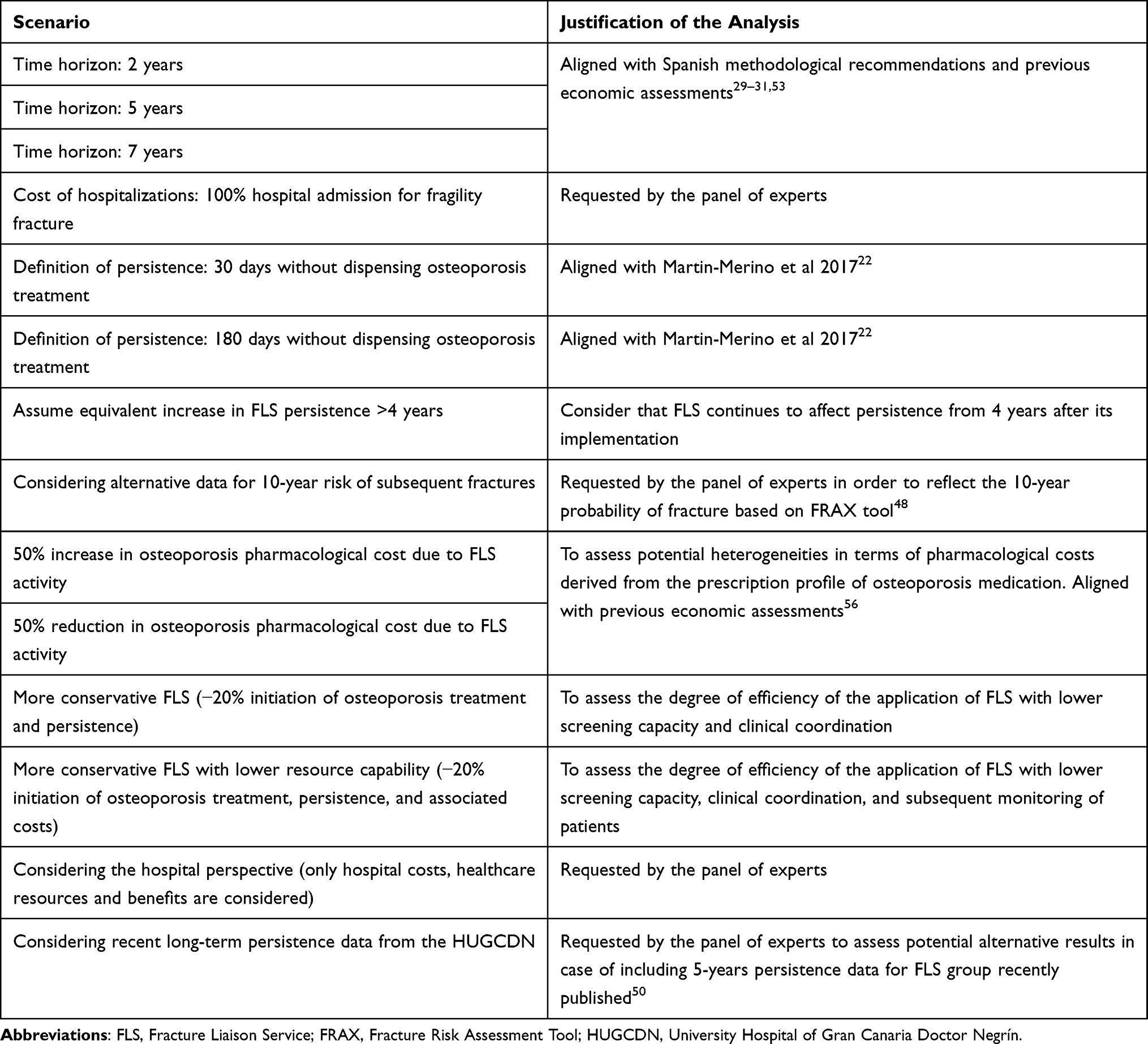 |
Table 4 Description of Scenario Analyses Evaluated |
Deterministic Sensitivity Analysis
The DSA were generated by applying a maximum univariate variation of ±20% to the continuous quantitative variables. Inputs and ranges of variability considered in DSA are detailed in the Supplementary Material (Tables S3 and S4). The results of the DSA are represented in tornado diagrams.
Probabilistic Sensitivity Analysis
A PSA was conducted to assess how the results of the base case would be modified due to the uncertainty inherent in the parameters considered. This was done using a Monte Carlo simulation, with 1000 random iterations across the confidence intervals of the continuous quantitative parameters. Inputs and ranges of variability considered in PSA are detailed in the Supplementary Material (Tables S5 and S6). The results are shown through an incremental cost-effectiveness plane.
Results
Base Case
Implementing FLS provides health benefits for osteoporotic patients. Due to the higher proportion of therapeutic initiation and persistence of patients managed by the FLS, an increase in LYG was observed in the state “Treated with anti-osteoporotic medication” (2.078 years) compared with a decrease in LYG in the states “Without anti-osteoporotic medication” (−1.983 years) and “Subsequent fractures” (−0.065 years). There was an increase in the cost of the “Treated with anti-osteoporotic medication” health state due to the FLS (€ 845.36) and savings in the “Subsequent fractures” (€ −561.51) and “Death” (€ −3.72) health states.
Over a time-horizon of 10 years, setting up FLS would generate an increase of 0.008 LYG and 0.082 additional QALYs per patient with limited incremental costs of € 563.69 per patient. This would result in an incremental cost-utility ratio (ICUR) of €6855.23 per QALY gained (Table 5). Therefore, from the SNS perspective, implementing an FLS would be a cost-effective strategy compared with SOC for the secondary prevention of fragility fractures according to the willingness-to-pay threshold commonly accepted in Spain (€20,000 to €30,000 per QALY gained).29,41,42
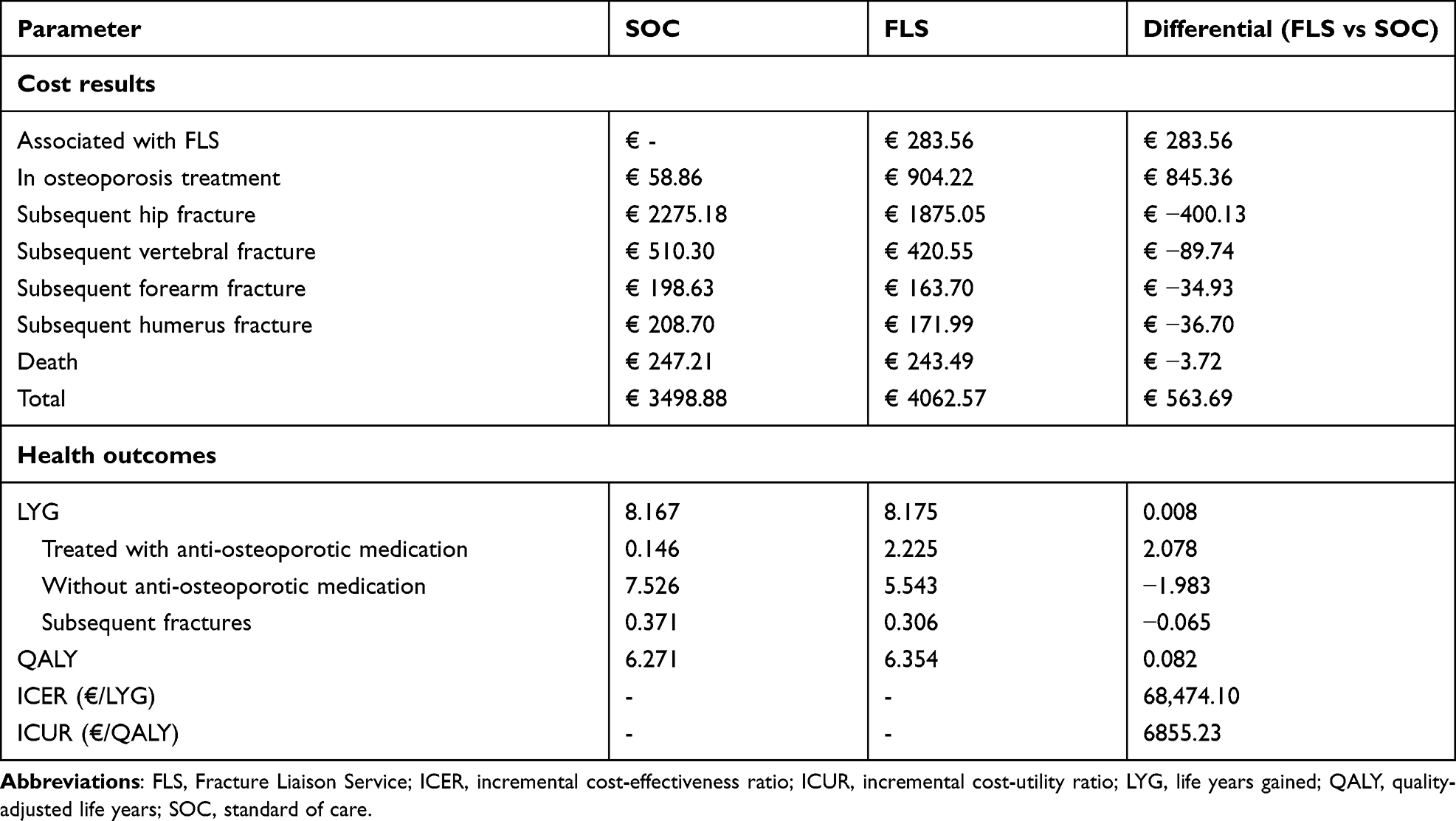 |
Table 5 Results of the Base Case |
Sensitivity Analysis
All scenario analyses indicated that FLS, compared with SOC, would provide increases of between 0.031 and 0.093 QALYs and an increase in direct healthcare costs from € 111.58 to € 1015.80, except for the scenario using the hospital perspective, which implied a cost reduction of € 281.48. The scenario analysis results showed an ICUR range of between € 1356.99 and € 14,457.18 per QALY gained, remaining below Spanish willingness-to-pay thresholds.29,41,42 In the hospital-perspective sensitivity analysis, the FLS was a dominant strategy over SOC by providing incremental clinical benefits along with economic savings (Table 6).
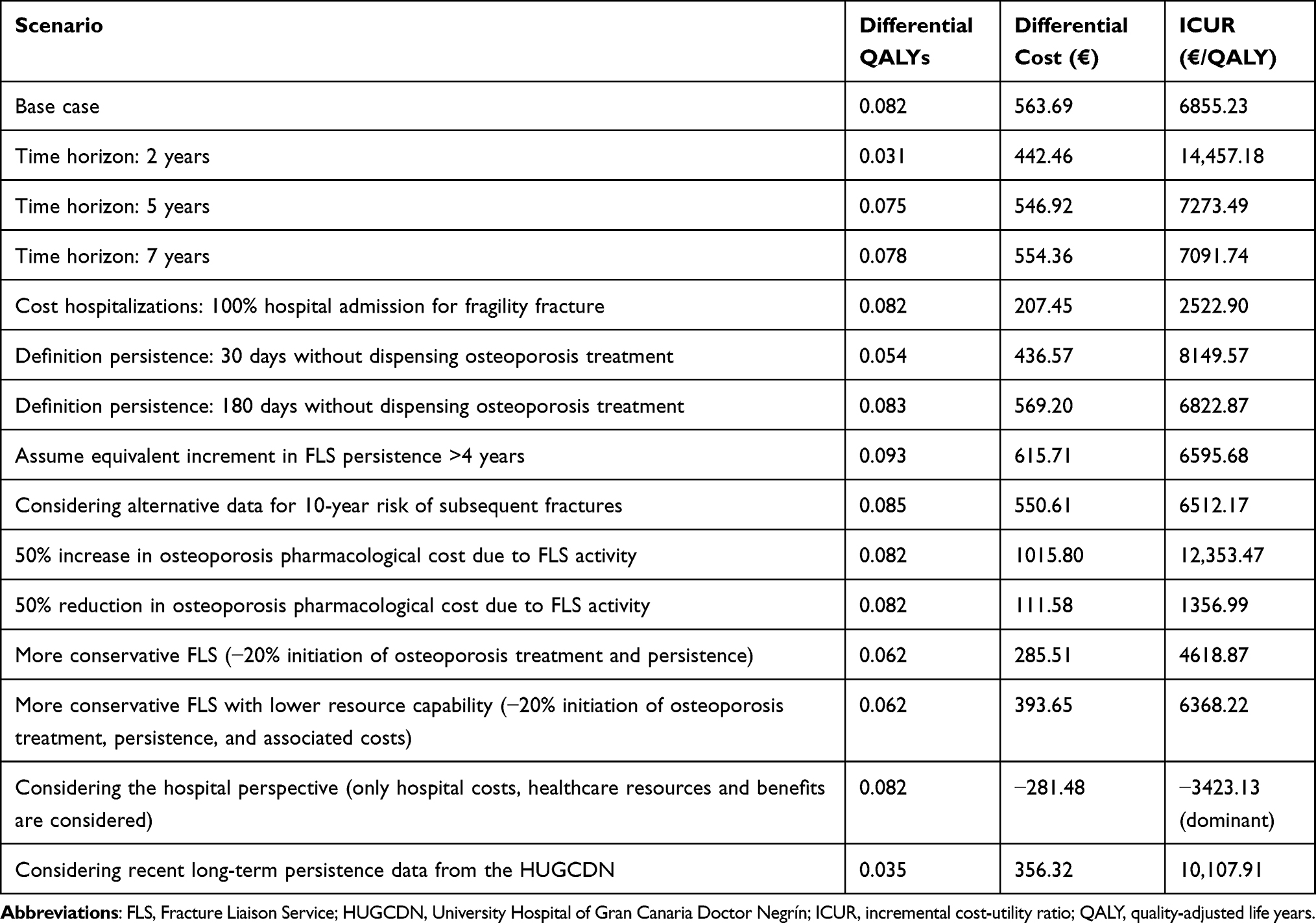 |
Table 6 Results of the Scenario Analysis |
The results of the DSA show the 16 parameters that generated the greatest variation in the ICUR obtained in the base case. Considering Spanish willingness-to-pay thresholds,29,41,42 in all results from the DSA, FLS were cost-effective strategies compared with SOC for secondary prevention of fragility fractures. The probability of subsequent fractures, the pharmacological cost associated with osteoporosis therapy, and the cost attributed to subsequent fractures, were the parameters which most conditioned the results of the base case. The variability of the ICUR resulting from the DSA showed a homogeneous trend (Figure 2).
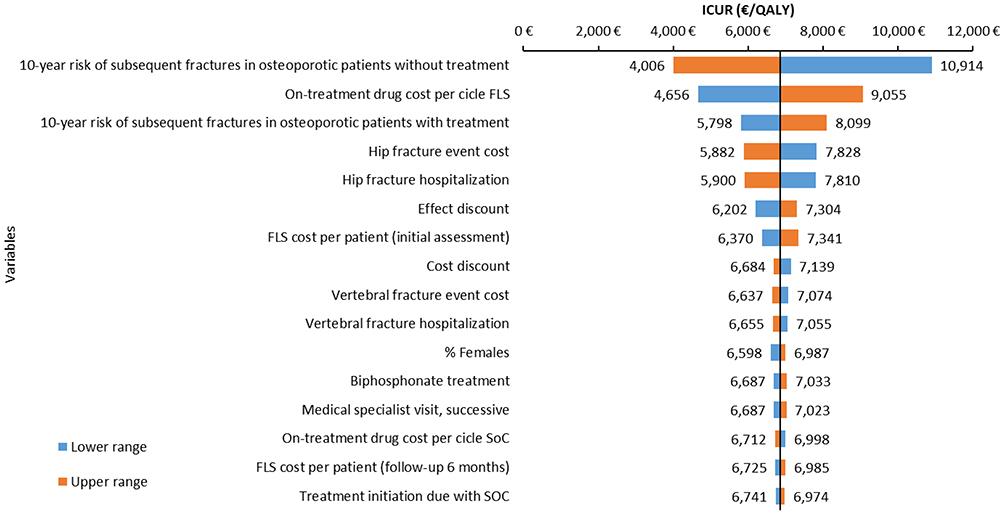 |
Figure 2 Tornado diagram. Abbreviations: ICUR, incremental cost-utility ratio; FLS, Fracture Liaison Service; SOC, standard of care; OP, osteoporosis. |
All PSA simulations indicated that FLS would provide QALY increases compared with SOC for the secondary prevention of fragility fractures. Between 97.1% and 99.6% of PSA simulations were below the Spanish willingness-to-pay thresholds,29,41,42 supporting the robustness of the results of the base case (Figure 3).
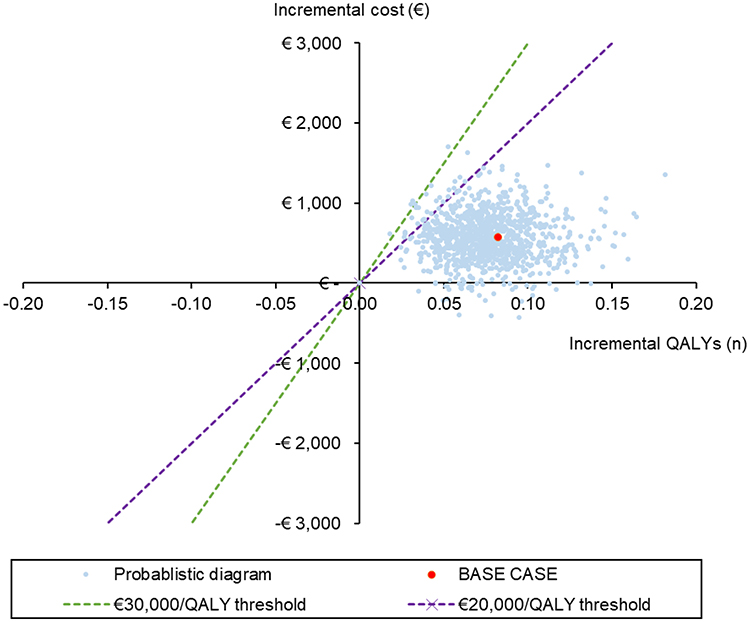 |
Figure 3 Incremental cost-effectiveness plane resulting from probabilistic sensitivity analysis. Abbreviation: QALY, quality-adjusted life years. |
Discussion
Fragility fractures and their associated complications are a growing healthcare problem. In 2017, costs related to fragility fractures in France, Germany, Italy, Spain, Sweden and the United Kingdom amounted to 37.5 billion euros and are expected to increase by 27% in 2030, reaching 47.4 billion euros.43
FLS are fracture coordination units that aim to reduce the risk of subsequent fragility fractures by identifying and systematically treating patients aged ≥ 50 years with fragility fractures.44
Many economic evaluations have analyzed the efficiency of FLS. The systematic review by Wu et al16 found that various healthcare interventions aimed at reducing the risk of subsequent fractures were cost-effective. However, there is a lack of published economic evaluations assessing the efficiency of implementing FLS in the Spanish setting. The present study represents, to our knowledge, the first economic assessment of FLS from the Spanish perspective.
The base case results show that introducing FLS programs in Spain would provide clinical benefits for the secondary prevention of fragility fractures, with 0.008 LYG and 0.082 QALY gained per patient along with a slight cost increase of €563.69 per patient over a 10-year time horizon. This would lead to an ICUR of € 6855.23 per QALY gained. Considering the Spanish commonly-accepted willingness-to-pay thresholds,29,41,42 FLS would be a cost-effective strategy compared with SOC for secondary prevention of fragility fractures. The results of the deterministic, probabilistic and scenario sensitivity analyses showed limited dispersion of the results, which corroborated the robustness of the base-case results.
The clinical results are attributable to higher percentage of patients who start anti-osteoporotic medication, a better adherence in anti-osteoporosis medication, but also to clinical and pedagogical recommendations on diet, exercise and balance provided by healthcare professionals to patients and relatives. Being part of a FLS also contributes to an increase in patients’ awareness regarding their disease and treatment, leading to a better monitoring of the disease, medication persistence and contributing to achieve better clinical results.
The efficacy of FLS in terms of fewer subsequent fractures and lower mortality is higher than expected only due to the effect of the medication,45 which suggests that non-pharmacological measures could be significantly influencing the results of FLS.
Patients with fragility fractures usually present an initial fracture with low morbidity and mortality, such as fractures of the forearm or humerus, while subsequent fractures, such as vertebral or hip fractures, have greater morbidity and mortality.46 Our results suggest that FLS produces savings in subsequent hip fractures (-€400.13), showing the importance of introducing FLS to prevent secondary fractures with higher morbidity and mortality and economic impact.
This study was carried using a simulated model and thus its theoretical nature is an inherent limitation because it may not reflect real clinical practice. Thus, the results should be interpreted with caution. To overcome this limitation, we tried to adopt premises and assumptions that provided clinical plausibility compatible with real clinical practice. Additionally, a large range of sensitivity analyses were carried out to confirm the conclusions of the analysis under different assumptions.
Given the lack of direct comparisons regarding the risk reduction of subsequent fractures due to Spanish FLS versus SOC, an indirect comparison generated from the evidence identified in the literature was necessary to carry out. Despite the intrinsic limitations of indirect comparisons, they provide useful information when there is no head-to-head clinical evidence.47 For this input, we used the risk of subsequent fractures with and without osteoporotic treatment reported by García-Renedo et al,21 refracture in 77 women with initial vertebral fracture with and without antiresorptive therapy was evaluated over a time horizon of 10 years. Due to the limited sample size, deterministic, probabilistic and scenario sensitivity analyses were performed to assess the potential inherent uncertainty of this input.
To determine the proportion of patients initiating osteoporosis treatment, an indirect comparison with data retrieved from the literature was made. For the SOC group, the prescription of antiresorptive treatment at 6 months post-fracture reported in a retrospective study conducted by the HUGCDN, which included 167 patients treated in the emergency department in October 2012 for fracture was considered.32 For the FLS group, it was estimated from the treatment initiation criteria of the Spanish Society of Rheumatology,34 and the degree of FLS acceptability described by the HUGCDN.33 Despite being an estimated value, it was aligned with FLS reported from other countries.16,44 This input was also subjected to deterministic, probabilistic and scenario sensitivity analyses.
Many studies have identified risk factors for fragility fractures, such as the FRAX index. Based on available data on the evolution of antiresorptive treatment persistence in patients with osteoporosis,22 we could not develop modelling exercises based on the risk of refracture indices. However, among the sensitivity scenarios included, we assessed the results of applying a 10-years probability of fracture based on FRAX tool developed by the University of Sheffield,48 using patients’ characteristics described by Martín-Merino et al study and the location of fragility fractures according to local clinical practice. The findings from this scenario were congruent and aligned with the results obtained in the base case.
Given the lack of specific Spanish data on the disutilities associated with subsequent fractures and treatment with bisphosphonates, these inputs were obtained from the literature.25,36 Their clinical suitability to the Spanish setting was validated by the expert panel. This limitation is common in economic assessments in our setting given the usual lack of this type of data.
Despite evidence showing that FLS do not increase total pharmacological expenditure associated with the management of osteoporosis,19 we conservatively included some modulation of prescribed osteoporosis medication in patients included in the FLS through a relative increase in the prescription of treatments with higher efficacy, tolerability and convenience profiles. This implies an increase in the estimated pharmacological cost for patients included in an FLS compared with SOC, which increases the cost per patient managed with FLS and, therefore, represents a conservative approach. In addition, as the distribution of treatments could present significant variations linked to Spanish clinical practice, deterministic, probabilistic and scenario sensitivity analyses were performed to address this input.
The study by Martín-Merino et al22 reported on the evolution of pharmacotherapeutic persistence in patients with osteoporosis according to the osteoporosis treatment initially prescribed. However, there is a lack of Spanish information on the increase in pharmacotherapeutic persistence due to the FLS according to the type of osteoporosis treatment used. Therefore, we were unable to construct models based on the pharmacological prescription profile. In this regard, the interpretation of such analyses should be considered with caution, given the difficulties in discerning between the factors associated with increases in osteoporosis pharmacotherapeutic persistence, ie, whether the increase in persistence can be attributed to patient monitoring, clinical and teaching activities linked to the FLS or to potential changes in the prescription profile.
An additional limitation, due to the lack of reliable data, are the benefits attributed to exercise and diet in reducing fractures. These recommendations are a fundamental part of FLS activity, including activities focused on fall prevention based on practicing and reinforcing balancing exercises.49 We could not assess the effectiveness of recommendations to reduce falls on the incidence of new fractures in the FLS arm, highlighting the conservative nature of current economic assessment.
Due to the nature of the FLS implemented in the HUGCDN, the results cannot be extrapolated for all current FLS activity in the SNS. To address uncertainty about the degree of efficiency of FLS with less experience, resource capability and clinical coordination, multiple scenario analyses were conducted. These sensitivity analyses showed that the introduction of more conservative FLS also would provide favorable efficiency results from the SNS perspective. As recent data on the evolution of persistence in FLS become available at Spanish level,50 a sensitivity scenario analysis was conducted supporting the results of the base case. Although the results of this scenario should be treated with caution due to differences in patient characteristics between studies, it also suggested that implementing an FLS program would provide clinical benefits to patients (0.003 LY and 0.035 QALY per patient) with limited incremental costs of € 356,32 per patient, resulting in an ICUR below the commonly accepted willingness-to-pay thresholds.29,41,42 A recent publication from an FLS of Virgen Macarena University Hospital showed adherence of 96% in the first year of the program,51 data aligned with the estimated persistence in the base case of this study.
Our results are aligned with most international studies assessing the efficiency of secondary prevention programs in patients with osteoporosis. In line with the reports by Inderjeeth et al,52 Yates et al,53 Cooper et al,26 Yong et al,54 Moriwaki et al55 and Majumdar et al,56 the introduction of FLS in Spain resulted a cost-effective strategy compared with SOC for the secondary prevention of fragility fractures. With a lower degree of agreement, the study by Majumdar et al57 presented results with a dominant cost-effectiveness ratio, meaning that FLS would increase the clinical benefits and economic savings in some healthcare settings. This study evaluated four main activities: patient education, organization and interpretation of bone densitometry, medication prescriptions and advice, and communication with primary care physicians. The analysis was conducted from the perspective of the Canadian healthcare system and included patients aged ≥74 years with hip fractures with a lifetime time horizon, suggesting that the longer the time horizon, the greater the clinical and economic benefits associated with FLS. Although our results are aligned with economic assessments conducted in other countries, the generalization and extrapolation of these results to other setting should be made with caution.
Likewise, the scenario analysis conducted from the hospital perspective found that the degree of efficiency of implementing FLS compared with SOC for secondary prevention of fragility fractures was a dominant strategy, as it provided incremental clinical benefits together with economic savings. In this analysis, the pharmacological costs associated with antiresorptive treatment occur mainly in the outpatient setting, and therefore are irrelevant from the hospital perspective. Thus, these costs would have been omitted from this scenario analysis, which justifies the estimated economic savings in the hospital setting after the implementation of the FLS.
The overall results of our study align with the conclusions of the main international pharmacoeconomic evidence on FLS, and similarities were observed in terms of clinical outcomes despite methodological, geographic, FLS clinical modality and patient profile differences. We found an incremental benefit compared with SOC of 0.082 QALYs per patient, which was in the range of the results identified in the literature (from 0.004 to 0.118 QALY gained per patient, according to the geographic setting, the FLS clinical modality and patient profile assessed).26,53–56
Conclusion
This cost-utility analysis found that the implementation in Spain of FLS, ie, structured programs for secondary prevention of fragility fractures, would be a cost-effective strategy compared with SOC, providing health benefits (0.082 additional QALYs over a time-horizon of 10 years) with a limited incremental cost (€ 563.69 per patient over a time-horizon of 10 years). This would result in an ICUR of € 6855.23 per QALY gained, markedly below the commonly accepted Spanish willingness-to-pay thresholds. The results of the base case were corroborated by a wide range of deterministic, probabilistic and scenario sensitivity analyses performed on the inputs, assumptions, structure, and variables considered.
Abbreviations
LYG, life years gained; QALY, quality-adjusted life years; B€, billions of euros; BIFAP, Database for Pharmacoepidemiological Research in Primary Care; BMD, bone densitometry; DSA, deterministic sensitivity analysis; FLS, Fracture Liaison Service; HUGCDN, University Hospital of Gran Canaria Doctor Negrín; PSA, probabilistic sensitivity analysis; ICER, incremental cost-effectiveness ratio; ICUR, incremental cost-utility ratio; RDL, Royal Decree Law; SNS, Spanish National Health System; SOC, standard of care.
Ethics Statement
Ethics approval is considered unnecessary in accordance to section 5 of Order SAS/3470/2009 and the Royal Decree 957/2020 since it is not a clinical study but an economic assessment based on publicly available information and does not contain personal data. Databases consulted to obtain unit costs of healthcare resource only have aggregated economic data.
Acknowledgments
The authors would like to thank Dr. Soledad Ojeda and Amparo Molina from University Hospital of Gran Canaria Doctor Negrín. Without their invaluable support and coordination, clinical expert panel validation of the model inputs and assumptions would not have been feasible. This manuscript includes preliminary and partial information presented at the World Congress on Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (WCO-IOF-ESCEO) annual congress 2021, the 9th Fragility Fracture Network Global Congress annual congress and the XXV SEIOMM annual congress. Published as congress abstracts at the following site: https://www.wco-iof-esceo.org/sites/wco_22/pdf/WCO21-AbstractBook.pdf.
Author Contributions
Each author affirms that they:
- Made a significant contribution to the study, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas.
- Have drafted or written, or substantially revised or critically reviewed the article.
- Have agreed on the journal to which the article will be submitted.
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
- Agree to take responsibility and be accountable for the contents of the article.
Funding
This research was funded by Amgen. The funding body was not involved in the study design, collection, and interpretation of data, or in the decision to publish.
Disclosure
AN and DPA are employed by the Hospital Universitario de Gran Canaria Dr. Negrín (University of Las Palmas de Gran Canaria) and NIHR Musculoskeletal Biomedical Research Unit (University of Oxford), respectively. AN reports grants and/or personal fees for consulting/speaker bureau fee from Amgen, Lilly and UCB. DPA reports grants for speaker services and advisory board membership from AMGEN, fees for consultancy services to his department from UCB Biopharma and Astra Zeneca, grants from Les Laboratoires Servier, EMA, Chesi-Taylor, and Novartis, outside the submitted work; Janssen, on behalf of IMI-funded EHDEN and EMIF consortiums, and Synapse Management Partners have supported training programmes organised by DPA’s department and open for external participants. APM, JSM and MB are employees of Pharmalex Spain, an independent contracting health economic organization which received consultancy fees from Fundación Canaria Instituto de Investigación Sanitaria de Canarias. The authors report no other conflicts of interest in this work.
References
1. NICE. NICEimpact. Falls and fragility fractures; 2018. Available from: https://www.nice.org.uk/media/default/about/what-we-do/into-practice/measuring-uptake/nice-impact-falls-and-fragility-fractures.pdf.
2. Sanfélix-Genovés J, Reig-Molla B, Sanfélix-Gimeno G, et al. The population-based prevalence of osteoporotic vertebral fracture and densitometric osteoporosis in postmenopausal women over 50 in Valencia, Spain (the FRAVO Study). Bone. 2010;47(3):610–616. doi:10.1016/j.bone.2010.06.015
3. Montoya-García MJ, Giner M, Marcos R, et al. Fragility fractures and imminent fracture risk in the spanish population: a retrospective observational cohort study. J Clin Med. 2021;10(5):1082. doi:10.3390/jcm10051082
4. International Osteoporosis Fundation (IOF). Broken bones, broken lives: a roadmap to solve the fragility fracture crisis in Spain. Available from: https://share.osteoporosis.foundation/EU-6-Material/Reports/IOFReport_SPAIN.pdf.
5. British Orthopaedic Association. The Care of Patients with Fragility Fracture: The ‘Blue Book. British Orthopaedic Association; 2007.
6. Cooper C. Epidemiology and definition of osteoporosis. In: Compston JE, editor. Osteoporosis: New Perspectives on Causes, Prevention and Treatment. London: Royal College of Physicians of London; 1996.
7. Department of Health. National service framework for older people. London: Department of Health; 2001. Available from: https://www.gov.uk/government/publications/quality-standards-for-care-services-for-older-people.
8. Scottish Executive. Adding life to years: report of the expert group on healthcare of older people. Edinburgh: Scottish Executive; 2002. Available from: https://www.sehd.scot.nhs.uk/publications/alty/alty.pdf.
9. Nikitovic M, Wodchis WP, Krahn MD, Cadarette SM. Direct health-care costs attributed to hip fractures among seniors: a matched cohort study. Osteoporos Int. 2013;24(2):659–669. doi:10.1007/s00198-012-2034-6
10. Naranjo A, Ojeda-Bruno S, Bilbao-Cantarero A, Quevedo-Abeledo JC, Diaz-González BV, Rodríguez-Lozano C. Two-year adherence to treatment and associated factors in a fracture liaison service in Spain. Osteoporos Int. 2015;26(11):2579–2585. doi:10.1007/s00198-015-3185-z
11. Caeiro JR, Bartra A, Mesa-Ramos M, et al. Burden of first osteoporotic hip fracture in Spain: a prospective, 12-month, observational study. Calcif Tissue Int. 2017;100(1):29–39. doi:10.1007/s00223-016-0193-8
12. Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5):513. doi:10.1001/jama.2009.50
13. Pisani P, Renna MD, Conversano F, et al. Major osteoporotic fragility fractures: risk factor updates and societal impact. World J Orthop. 2016;7(3):171. doi:10.5312/wjo.v7.i3.171
14. Curtis EM, Moon RJ, Harvey NC, Cooper C. Reprint of: the impact of fragility fracture and approaches to osteoporosis risk assessment worldwide. Int J Orthopaed Trauma Nurs. 2017;26:7–17. doi:10.1016/j.ijotn.2017.04.004
15. McLellan AR, Gallacher SJ, Fraser M, McQuillian C. The fracture liaison service: success of a program for the evaluation and management of patients with osteoporotic fracture. Osteoporos Int. 2003;14(12):1028–1034. doi:10.1007/s00198-003-1507-z
16. Wu CH, Kao IJ, Hung WC, et al. Economic impact and cost-effectiveness of fracture liaison services: a systematic review of the literature. Osteoporos Int. 2018;29(6):1227–1242. doi:10.1007/s00198-018-4411-2
17. Marsh D, Åkesson K, Beaton DE, et al. Coordinator-based systems for secondary prevention in fragility fracture patients. Osteoporos Int. 2011;22(7):2051–2065. doi:10.1007/s00198-011-1642-x
18. Naranjo A, Fernández-Conde S, Ojeda S, et al. Preventing future fractures: effectiveness of an orthogeriatric fracture liaison service compared to an outpatient fracture liaison service and the standard management in patients with hip fracture. Arch Osteoporos. 2017;12(1):3–7. doi:10.1007/s11657-017-0373-9
19. Naranjo A, Ojeda-Bruno S, Saavedra A, Molina A, Negrín M. Impact of the implementation of a Fracture Liaison Service on pharmaceutical expenses for osteoporosis compared to an area without an FLS. Expert Rev Pharmacoecon Outcomes Res. 2019;19(1):81–87. doi:10.1080/14737167.2018.1513791
20. Ojeda-Bruno S, Naranjo A, Francisco-Hernández F, et al. Secondary prevention program for osteoporotic fractures and long-term adherence to bisphosphonates. Osteoporos Int. 2011;22(6):1821–1828. doi:10.1007/s00198-010-1414-z
21. García Renedo RJ, Mella Sousa M, Anaya Rojas M, et al. Estudio epidemiológico de factores de riesgo asociados a refractura en mujeres con fractura vertebral osteoporótica durante 10 años de seguimiento. [Epidemiological study of risk factors associated to refracture in women osteoporotic vertebral fracture during a 10-year follow-up]. Revista Española de Enfermedades Metabólicas Óseas. 2009;18(4):85–89. doi:10.1016/S1132-8460(09)73463-4
22. Martín-Merino E, Huerta-álvarez C, Prieto-Alhambra D, Montero-Corominas D. Cessation rate of anti-osteoporosis treatments and risk factors in Spanish primary care settings: a population-based cohort analysis. Arch Osteoporos. 2017;12(1). doi:10.1007/s11657-017-0331-6
23. Skjødt MK, Khalid S, Ernst M, et al. Secular trends in the initiation of therapy in secondary fracture prevention in Europe: a multi-national cohort study including data from Denmark, Catalonia, and the United Kingdom. Osteoporos Int. 2020;31(8):1535–1544. doi:10.1007/s00198-020-05358-4
24. INE (Instituto Nacional de Estadística). Tablas de mortalidad por año, sexo, edad y funciones. [Population mortality tables for Spain by year, sex, age and functions]; 2020. Available from: https://www.ine.es/.
25. Solomon DH, Patrick AR, Schousboe J, Losina E. The potential economic benefits of improved postfracture care: a cost-effectiveness analysis of a fracture liaison service in the US health-care system. J Bone Mineral Res. 2014;29(7):1667–1674. doi:10.1002/jbmr.2180
26. Cooper MS, Palmer AJ, Seibel MJ. Cost-effectiveness of the Concord Minimal Trauma Fracture Liaison service, a prospective, controlled fracture prevention study. Osteoporos Int. 2012;23(1):97–107. doi:10.1007/s00198-011-1802-z
27. Jonsson E, Borgström F, Ström O. Cost effectiveness evaluation of fracture liaison services for the management of osteoporosis in Sweden. Value Health. 2016;19(7):A612. doi:10.1016/j.jval.2016.09.1529
28. McLellan AR, Wolowacz SE, Zimovetz EA, et al. Fracture liaison services for the evaluation and management of patients with osteoporotic fracture: a cost-effectiveness evaluation based on data collected over 8 years of service provision. Osteoporos Int. 2011;22(7):2083–2098. doi:10.1007/s00198-011-1534-0
29. Ortega Eslava A, Marín Gil R, Fraga Fuentes MD, López-Briz E. Guía de Evaluación Económica e Impacto Presu-Puestario En Los Informes de Evaluación de Medicamentos [Economic Evaluation and Budgetary Impact Guidelines for Assessment Reports on Medicinal Products]. 2016.
30. López Bastida J, Oliva J, Antoñanzas F, et al. Propuesta de guía para la evaluación económica aplicada a las tecnologías sanitarias. [A proposed guideline for economic evaluation of health technologies]. Gaceta Sanitaria. 2010;24(2):154–170. doi:10.1016/j.gaceta.2009.07.011
31. Puig-Junoy J, Oliva-Moreno J, Trapero-Bertrán M, et al. Guía y recomendaciones para la realización y presentación de evaluaciones económicas y análisis de impacto presupuestario de medicamentos en el ámbito del CatSalut [Guidelines and recommendations to conduct and present economic assessments and budget impact analysis of medicines to the CatSalut setting]. Generalitat de Catalunya Dept de Salut Servei Català de la Salut. 2014;2014:9–11.
32. Hiligsmann M, Reginster JY, Tosteson ANA, et al. Recommendations for the conduct of economic evaluations in osteoporosis: outcomes of an experts’ consensus meeting organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) and. Osteoporos Int. 2019;30(1):45–57. doi:10.1007/s00198-018-4744-x
33. Naranjo A, Ojeda-Bruno S, Bilbao Cantarero A, Quevedo Abeledo JC, Henríquez-Hernández LA, Rodríguez-Lozano C. Resultados de un modelo de prevención secundaria de fractura osteoporótica coordinado por reumatología centrado en la enfermera y el médico de atención primaria [Results of a model of secondary prevention for osteoporotic fracture coordinated by rheumatology and focused on the nurse and primary care physicians]. Reumatol Clin. 2014;10(5):299–303. doi:10.1016/j.reuma.2013.12.007
34. Rubiño F, Ojeda S, Molina A, Naranjo A. Application of the recommendations of the Spanish Society of Rheumatology on osteoporosis in a Fracture Liaison Service unit. Reumatología Clínica. 2021;17(2):122–123. doi:10.1016/j.reumae.2019.03.011
35. INE (Instituto Nacional de Estadística). Encuesta Nacional de Salud [National Health Survey]; 2014. Available from: https://www.ine.es/.
36. Hiligsmann M, Ethgen O, Richy F, Reginster JY. Utility values associated with osteoporotic fracture: a systematic review of the literature. Calcif Tissue Int. 2008;82(4):288–292. doi:10.1007/s00223-008-9117-6
37. CIMA-AEMPS (Centro de Información online de Medicamentos de la Agencia Española de Medicamentos y Productos Sanitarios). Buscador de medicamentos [Medicines browser for healthcare professionals]. Available from: https://cima.aemps.es/cima/publico/home.html.
38. Naranjo A, Molina A, Sepúlveda C, Rubiño FJ, Martín N, Ojeda S. The evolution of an FLS in search of excellence: the experience of Gran Canaria. Arch Osteoporos. 2020;15(1):108. doi:10.1007/s11657-020-00729-0
39. MSCyBS (Ministerio de Sanidad Consumo y Bienestar Social). Registro de Actividad de Atención Especializada – RAE-CMBD [Registry of Specialized Healthcare Activity - RAE-CMBD]. Available from: https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/S/rae-cmbd.
40. Gisbert R, Brosa M. Spanish Health Costs and cost-effectiveness ratios database: eSalud. Barcelona: Oblikue Consulting, S.L; 2007. Available from: http://www.oblikue.com/bddcostes/.
41. Sacristán JA, Oliva J, Del Llano J, Prieto L, Pinto JL. ¿Qué es una tecnología sanitaria eficiente en España? [What is an efficient health technology in Spain?]. Gaceta Sanitaria. 2002;16(4):334–343. doi:10.1016/S0213-9111(02)71933-X
42. Vallejo-Torres L, Garcia-Lorenzo B, Garcia-Pérez L, Linertová R, Serrano-Aguilar P. Disponibilidad a Pagar de La Sociedad Española Por Un Año de Vida Ajustado Por Calidad [Spannish Society Willingness-To-Pay for One Quality-Adjusted Life Year]. Ministerio de Sanidad, Servicios Sociales e Igualdad. Servicio de Evaluación del Servicio Canario de la Salud; 2017.
43. Borgström F, Karlsson L, Ortsäter G, et al. Fragility fractures in Europe: burden, management and opportunities. Arch Osteoporos. 2020;15(1). doi:10.1007/s11657-020-0706-y
44. Royal College of Physicians. Fracture Liaison Service Database (FLS-DB) Annual Report. Leading FLS Improvement: Secondary Fracture Prevention in the NHS. London: Royal College of Physicians; 2017.
45. Huntjens KMB, van Geel TA, van den Bergh JPW, et al. Fracture liaison service: impact on subsequent nonvertebral fracture incidence and mortality. J Bone Joint Surg. 2014;96(4):e29. doi:10.2106/JBJS.L.00223
46. International Osteoporosis Fundation (IOF). Capture de Fracture Partnership. The need for secondary fracture prevention. Available from: https://www.osteoporosis.foundation/sites/iofbonehealth/files/2021-01/CTFslidekit1_updated_280820.pdf.
47. Catalá-López F, Tobías A, Roqué M. Conceptos básicos del metaanálisis en red. [Basic concepts for network meta-analysis]. Atención Primaria. 2014;46(10):573–581. doi:10.1016/j.aprim.2014.01.006
48. University of Sheffield. FRAX. Fracture risk assessment tool; 2008. Available from: https://www.sheffield.ac.uk/FRAX/index.aspx.
49. Geiger I, Kammerlander C, Höfer C, et al. Implementation of an integrated care programme to avoid fragility fractures of the hip in older adults in 18 Bavarian hospitals – study protocol for the cluster-randomised controlled fracture liaison service FLS-CARE. BMC Geriatr. 2021;21(1):43. doi:10.1186/s12877-020-01966-1
50. Naranjo A, Molina A, Quevedo A, et al. Fracture liaison service model: treatment persistence 5 years later. Arch Osteoporos. 2021;16(1):60. doi:10.1007/s11657-021-00925-6
51. Olmo-Montes FJ, Hernández-Cruz B, Miranda MJ, et al. The fracture liaison service of the virgen macarena university hospital reduces the gap in the management of osteoporosis, particularly in men. It meets the international osteoporosis foundation quality standards. J Clin Med. 2021;10(18):1–17. doi:10.3390/jcm10184220
52. Inderjeeth CA, Raymond W, Geelhoed E, et al. THU0465 fracture liaison service reduces re-fracture rate, cost-effective and cost saving in Western Australia. Ann Rheum Dis. 2016;75(Suppl2):
53. Yates CJ, Chauchard MA, Liew D, Bucknill A, Wark JD. Bridging the osteoporosis treatment gap: performance and cost-effectiveness of a fracture liaison service. J Clin Densitomet. 2015;18(2):150–156. doi:10.1016/j.jocd.2015.01.003
54. Yong JHE, Masucci L, Hoch JS, Sujic R, Beaton D. Cost-effectiveness of a fracture liaison service—a real-world evaluation after 6 years of service provision. Osteoporos Int. 2016;27(1):231–240. doi:10.1007/s00198-015-3280-1
55. Moriwaki K, Noto S. Economic evaluation of osteoporosis liaison service for secondary fracture prevention in postmenopausal osteoporosis patients with previous hip fracture in Japan. Osteoporos Int. 2017;28(2):621–632. doi:10.1007/s00198-016-3777-2
56. Majumdar SR, Johnson JA, Lier DA, et al. Persistence, reproducibility, and cost-effectiveness of an intervention to improve the quality of osteoporosis care after a fracture of the wrist: results of a controlled trial. Osteoporos Int. 2007;18(3):261–270. doi:10.1007/s00198-006-0248-1
57. Majumdar SR, Lier DA, Beaupre LA, et al. Osteoporosis case manager for patients with hip fractures. Arch Intern Med. 2009;169(1):25. doi:10.1001/archinte.169.1.25
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.