Back to Journals » ClinicoEconomics and Outcomes Research » Volume 9
Cost analysis of adverse events associated with non-small cell lung cancer management in France
Authors Chouaid C ![]() , Loirat D, Clay E, Millier A, Godard C, Fannan A, Lévy-Bachelot L, Angevin E
, Loirat D, Clay E, Millier A, Godard C, Fannan A, Lévy-Bachelot L, Angevin E
Received 5 April 2017
Accepted for publication 31 May 2017
Published 27 July 2017 Volume 2017:9 Pages 443—449
DOI https://doi.org/10.2147/CEOR.S138963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Giorgio Colombo
Christos Chouaid,1 Delphine Loirat,2 Emilie Clay,3 Aurélie Millier,3 Chloé Godard,4 Amira Fannan,4 Laurie Lévy-Bachelot,4 Eric Angevin5
1Chest Department, Centre Hospitalier Intercommunal Créteil, Créteil, France; 2Institut Curie, Paris, France; 3Creativ-Ceutical, Paris, France; 4MSD France, Courbevoie, France; 5Institut Gustave Roussy, Villejuif, France
Background: Adverse events (AEs) related to medical treatments in non-small cell lung cancer (NSCLC) are frequent and need an appropriate costing in health economic models. Nevertheless, data on costs associated with AEs in NSCLC are scarce, particularly since the development of immunotherapy with specific immune-related AEs.
Objective: To estimate the costs of grades 3 and 4 AEs related to NSCLC treatments including immunotherapy in France.
Methods: Grades 3 and 4 AEs related to treatment and reported in at least 1% of patients in Phase III clinical trials for erlotinib, ramucirumab plus docetaxel, docetaxel, pemetrexed plus carboplatin plus bevacizumab, platinum-based chemotherapies, nivolumab and pembrolizumab were identified. When no cost evaluation was reported in literature, estimates on standard treatments and medical resource use for each AE were obtained thanks to an expert panel. Total cost per AE was calculated from a French national health insurance perspective and updated in 2017 Euros. Hospital stay costs were estimated based on public and private weighted tariffs and data from the French Medical Information System (Programme de Médicalisation des Systèmes d’Information). Costs of tests, consultations and treatments were calculated based on national reimbursement tariffs.
Results: Overall, costs of grades 3 and 4 AEs related to treatment ranged from €46 per event to €7,742 per year. Fourteen out of 24 AEs identified had a mean estimated cost over €2,000. The highest mean costs were related to type 1 diabetes (€7,742 per year) followed by pneumonitis (€5,786 per event), anemia (€5,752 per event), dehydration (€5,207 per event) and anorexia (€4,349 per event). Costs were mostly driven by hospitalization costs.
Conclusion: Among the AEs identified, a majority appeared to have an important economic impact, with a management cost of at least €2,000 per event mainly driven by hospitalization costs. This study may be of interest for economic evaluations of new interventions in NSCLC.
Keywords: non-small cell lung cancer, adverse events, cost analysis, chemotherapy, immunotherapy
Introduction
According to the World Health Organization, lung cancer is the most common cancer worldwide with 1.8 million new cases and 1.6 million deaths in 2012 which makes it the leading cause of death due to cancer in men and the second one in women after breast cancer.1 The prognosis of lung cancer is generally poor with a 5-year overall survival estimated at 10%–15% due to a diagnosis, generally at an advanced stage of the disease.2 In France, deaths due to lung cancer were estimated at 29,949 in 2012.3
Non-small cell lung cancer (NSCLC) accounts for 85% of all lung cancers.4 For patients who have been diagnosed at an early stage, surgery remains the preferred treatment. At an advanced stage, first-line treatment consists of platinum-based combination therapies. Docetaxel, pemetrexed and erlotinib are considered for subsequent lines and treatment strategy takes into account histology, age and comorbidities.5 These therapies may be associated with toxicities:6 renal, neurologic and hematologic for platinum-based chemotherapy,7 hematologic disorders and diarrhea for docetaxel and pemetrexed,8 skin toxicity, diarrhea and interstitial lung disease for erlotinib.6 Recently, pembrolizumab and nivolumab, two monoclonal antibodies that block the interaction between PD-1 expressed on tumor cells and PD-L1 receptors expressed on T cells, became new therapeutic options for NSCLC. In recent randomized controlled trials, both pembrolizumab and nivolumab were found to significantly increase progression-free survival in patients with NSCLC expressing PD-L1 with a better tolerance profile compared to cytotoxic agents but with some adverse events (AEs) specific to immunotherapy.9–12 However, there are very few data on costs associated with AEs in NSCLC. The objective of this study was to estimate the costs of grades 3 and 4 AEs related to NSCLC treatments including immunotherapy in France by combining literature review, expert opinions and data extraction from a French hospital discharge database.
Materials and methods
Selection of AEs of interest
The following treatments of NSCLC were considered for the analysis as representative of the main therapeutic classes of interest for first- and second-line: docetaxel, pemetrexed, bevacizumab, ramucirumab, erlotinib, nivolumab, pembrolizumab and nonpemetrexed containing platinum-based chemotherapies. After a literature review, the studies of Shepherd et al,14 Patel et al,13 Garon et al,15 Herbst et al11 and Reck et al12 were identified for the selection of AEs in NSCLC treatment. Grades 3 and 4 AEs (as defined by common toxicity criteria)16 related to these drugs and reported in at least 1% of patients from at least one of these pivotal clinical trials for first- or second-line NSCLC treatments were identified.
Literature review
For each AE of interest, costing in France was investigated through a literature review using MEDLINE. We selected articles in English language and gave priority to those published within the past 10 years. The studies by Banz et al17 and Nuijten et al18 about the management of AEs related to treatment in NSCLC were identified. The study by Nuijten et al was considered as a duplicate of the study by Banz et al. The literature research was then extended to the management of AEs related to treatment in melanoma, considering that the management of grades 3 and 4 AEs does not depend on the underlying disease. Two studies were identified19,20 and none was excluded. French experts were asked to complete data when information was lacking. Costs available in literature were updated to 2017 Euros.
Expert panel
For AEs with no published available cost, an expert panel composed of 3 French oncologists (CC, DL and EA) completed a questionnaire on the assessment of resource use in real-life practice for selected AEs. This questionnaire was completed by the experts before the meeting and it included the following items: hospitalization (percentage of patients concerned and duration of hospitalization stay), diagnostic tests (percentage of patients concerned and types of tests), consultations of general practitioner (percentage of patients concerned and number of visits), treatments (percentages of patients concerned, drug name and dosage and treatment duration) and other resources. During the meeting, the methodology considered for identifying AEs was described. Then, experts were asked to give their insight and the answers to the questionnaire were discussed. As AEs were not reported with the same terms in each clinical trial, similar AEs or AEs requiring similar management were merged under a unique term when relevant, based on expert opinion. A consensus was then reached by discussion and the minutes of the meeting were validated by all participants.
Costing
Total cost per AE was calculated from a French national health insurance perspective. Hospital stays costs were estimated based on available tariffs and data from the French Medical Information System (Programme de Médicalisation des Systèmes d’Information [PMSI]). The PMSI database covers all French public and private hospitals, except military and psychiatric hospitals. For each stay, diagnosis, medical procedures, duration and treatment are reported in standardized discharge reports and collected in the PMSI.
PMSI database is primarily used for hospital funding and frequently used for observational research purposes. At the time the study was conducted, the PMSI database was available upon registration, agreement and payment to a habilitated provider or through collaboration with a French university hospital health information management department. Since April 2017, the PMSI database is monitored by the National Institute of Health Data. This institute receives requests for authorization, which must then be submitted for an opinion from the expert committee for research, analysis and evaluation in the area of health. The decision of this committee is based on the relevance and the quality of the protocol submitted, the methodology chosen, the need and the public interest nature of the research.
In a first step, ICD-10 codes (lung cancer, C34; metastatic, C77, C78, C79) allowed selecting in the database patients with lung cancer (as principal, secondary or associated diagnosis); only stays for patients with an age of ≥18 years were kept. Each AE was then identified in 2014 using diagnosis codes (ICD-10) or DRG codes (diagnosis-related groups). Lung cancer patients with AE did not require having a treatment of interest.
For each AE, PMSI database provided mean length and cost of stay depending on the type of hospitalization (in intensive care unit or in general ward). Analyses of data extracted from PMSI database were performed with SAS v.9.3 (SAS Institute, Cary, NC, USA). Costs of tests, consultations and treatments were calculated based on national reimbursement tariffs.
Statistical analysis
Data were analyzed using SAS software (SAS Institute). Quantitative variables were described by median and quartiles or by mean and standard deviation. Qualitative variables were described by numbers and percentages.
Results
Considering relevant clinical trials,11–15 38 AEs met the inclusion criteria; 22 AEs not reported with the same terms, but similar or requiring similar management, were merged under 8 unique terms based on expert opinion (Table 1). Finally, 24 AEs were considered for the cost analysis.
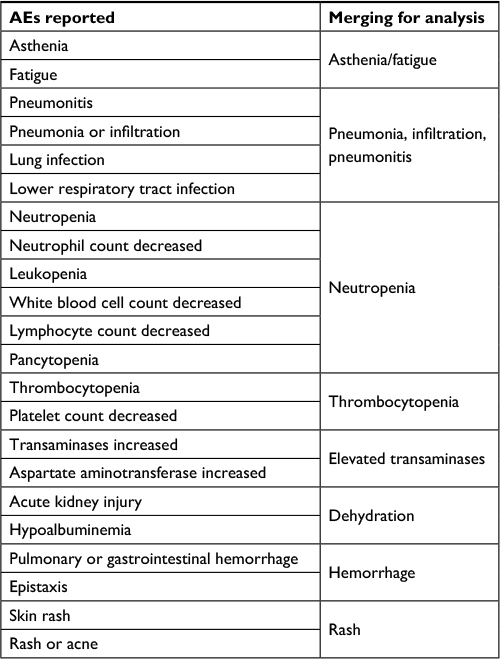 | Table 1 Merging of adverse events (AEs) from different studies |
The costs of 17 AEs were obtained from literature and updated to 2017 Euros. These data and corresponding studies are summarized in Table 2. The study by Banz et al17 provided French costs of grades 3 and 4 AEs in NSCLC patients considering hospitalizations, supplementary diagnostic examinations, drug therapy and follow-up outpatient physician visits through structured data collection sessions with 6 lung cancer specialists. Results were provided only with total cost without further details on items distribution. The study by Wehler et al19 provided French costs of grades 3 and 4 AEs in patients with melanoma considering hospitalizations, supplementary diagnostic examinations, drug therapy and procedures through structured interviews done with physicians experienced in the fields of medical oncology or dermatology in melanoma. The costs of AEs were provided separately for inpatients and outpatients. Therefore, distribution was asked to French experts during the advisory board meeting in order to calculate a mean cost for 3 AEs (elevated transaminases, febrile neutropenia and hypertension). The cost of colitis in France was obtained from the study by Vouk et al, which estimated the costs associated with AEs in patients with metastatic melanoma across Europe through literature review followed by Delphi panel interviews.20 The cost of type 1 diabetes was obtained from the Échantillon national témoin représentatif des personnes diabétiques [National representative sample of people with diabetes] survey performed in France in 6710 adult patients.21 In the particular case of type 1 diabetes, the cost was estimated on a per-year basis; moreover, the cost was weighted by the mean survival duration observed in KEYNOTE-024 according to the type of NSCLC (squamous or nonsquamous carcinoma).
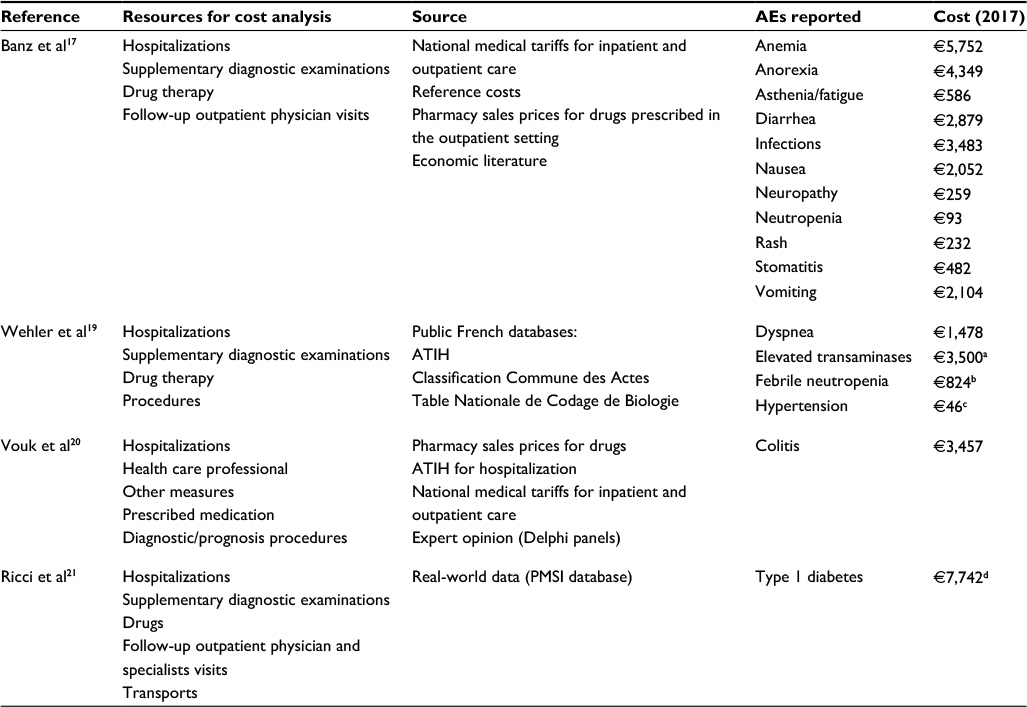 | Table 2 Studies providing French costs of grade 3–4 adverse events Notes: aWith/without hospitalization: €6,972/€28 (50% of hospitalizations; expert opinion); bWith/without hospitalization: €2,017/€29 (40% of hospitalizations; expert opinion); cWith/without hospitalization: €1,633/€30 (1% of hospitalizations: expert opinion); dMean annual cost taking into account mean survival duration observed in KEYNOTE-024 (total cost: squamous carcinoma, €16,581; nonsquamous carcinoma, €21,960). Abbreviations: AE, adverse event; ATIH, Agence Technique de l’information sur l’Hospitalisation [Technical Information on Hospitalization Agency]; PMSI, Programme de Médicalisation des Systèmes d’Information [French Medical Information System]. |
The use of medical resource for 7 grades 3 and 4 AEs not reported in literature were assessed based on experts opinion. The mean costs of these AEs are summarized in Table 3. According to the experts, the occurrence of grades 3 and 4 AEs related to treatment required inpatient hospitalization, systematically for dehydration, pulmonary hemorrhage, pneumonitis and venous thromboembolism. These proportions were more variable for toxic ocular effect, thrombocytopenia and arthralgia with 10%, 25% and 75% of hospitalizations, respectively. Other medical resources were used for the management of arthralgia and toxic ocular effect. Both required tests for 25% of concerned patients, consisting of a complete biological test and a fundus examination, respectively. Moreover, consultations with a specialist were considered relevant for the follow-up of 25% of patients concerned by arthralgia and toxic ocular effect and 100% of patients concerned by pulmonary hemorrhage. However, for many AEs, tests and treatment costs were considered nonsignificant or already included in the hospitalization costs except for venous thromboembolism which required, systematically, the administration of low-molecular-weight heparin by a nurse at home for 90 days.
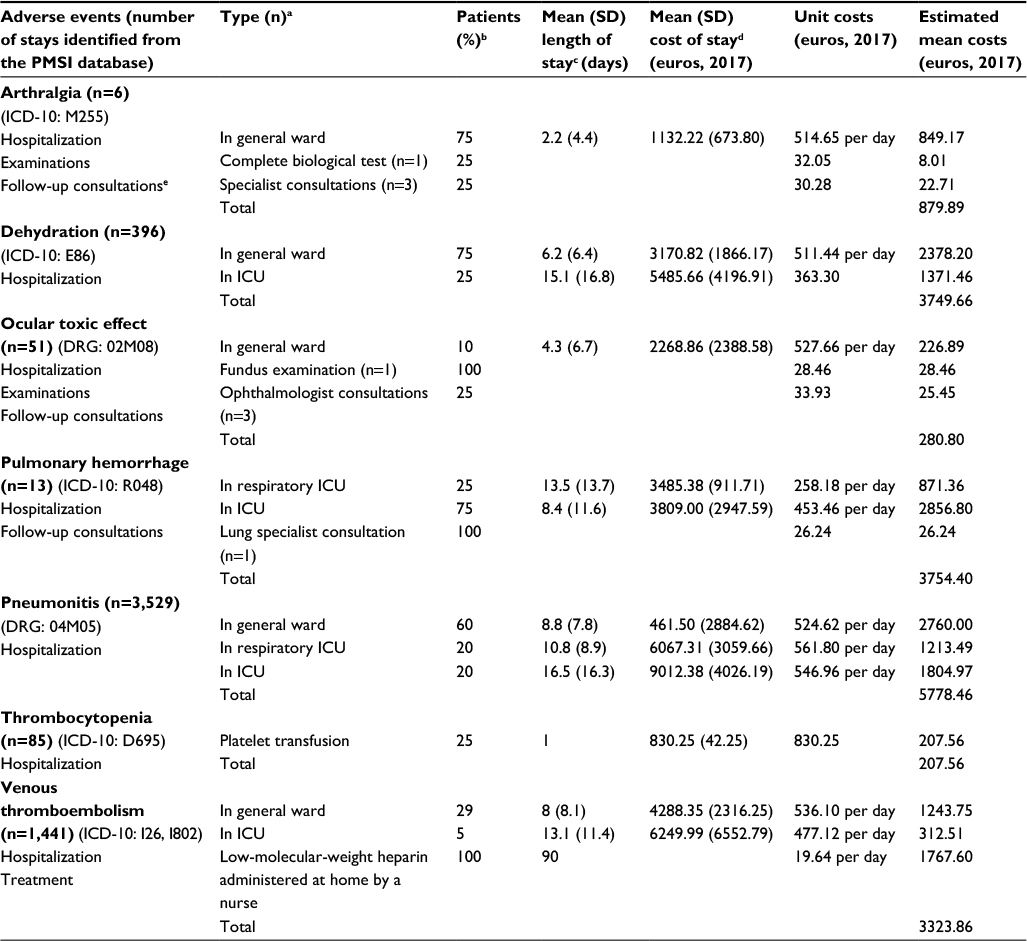 | Table 3 Resource use for grades 3–4 adverse events and mean costs (according to experts and PMSI database) Notes: aType and quantity of resource use per type of AE were assessed according to expert opinion; bPercentage of patients concerned were assessed based on expert opinion; cMean durations of hospitalization were estimated according to the PMSI database; dHospital stay costs were estimated based on public and private weighted tariffs and 2014 PMSI database; costs of diagnostic examinations, follow-up consultations and treatments were calculated based on national reimbursement tariffs; eComplete blood cell count, serum creatinine, serum electrolytes and rheumatoid factor blood test. Abbreviations: DRG, diagnosis-related group; ICD-10, The International Classification of Diseases, Tenth Edition; ICU, intensive care unit; PMSI, Programme de Médicalisation des Systèmes d’Information [French Medical Information System]; SD, standard deviation. |
Overall, costs of grades 3 and 4 AEs related to treatment ranged from €46 per event to €7,742 per year (Tables 2 and 3). Fourteen out of 24 grades 3 and 4 AEs identified had an estimated mean cost over €2,000. The highest mean costs per patient were related to type 1 diabetes (€7,742 per year) followed by pneumonitis (€5,786 per event), anemia (€5,752 per event), dehydration (€5,207 per event) and anorexia (€4,439 per event). The costs of AEs more specifically reported with immunotherapy treatments were €3,457 for colitis, €3,500 for elevated transaminases and €7,742 per year for type 1 diabetes.
Discussion
AEs associated with medical treatment in lung cancer are frequent and their management represent a significant cost. This cost varies according to countries.17,19 For example, Banz et al reported that the management of grades 3 and 4 anemia in NSCLC patients varied from €1,526 in Spain to €5,228 in France.17
The total costs of grades 3 and 4 AEs are, generally, driven by hospitalization. Therefore, the estimation of hospitalization rates and length of stay must be accurate in cost analysis. In their study comparing treatment costs of grades 3 and 4 AEs in NSCLC patients from different countries, Banz et al reported that cost variations were primarily due to differences in clinician’s estimate of hospitalization referral rates.17 An advantage of our study was that the estimations concerning hospitalization (duration of stay, admission to intensive care unit or general ward) were based not only on expert opinion but also when necessary on objective real-life data from the PMSI database. In contrast with Wehler et al, who separately reported outpatient and inpatients costs of grades 3 and 4 AEs, we estimated the proportions of inpatients and outpatients, when necessary, and a mean cost was calculated. This approach was also adopted by Banz et al who reported mean total costs of AEs by taking into account country-specific estimates of admission rates and length of stay at hospital.17
Immunotherapy is a new paradigm in NSCLC therapy and pembrolizumab or nivolumab acts on cancer through the antitumor activity of T cells. As a consequence, different safety profiles can be expected in comparison with cytotoxic agents.
In pivotal trials, AEs were less frequent in immunotherapy arms. Thus, in KEYNOTE-024 study, treatment-related AEs of any grade were less frequent in pembrolizumab 200 mg group compared with the chemotherapy group (73.4% versus 90.0% of patients) as were treatment-related grades 3 and 4 AEs (26.6% versus. 53.3%). In KEYNOTE-010 study, grades 3 and 4 AEs attributed to study treatment were reported in only 12.3% of patients in pembrolizumab 2 mg/kg group versus 35% in docetaxel group.11 The same trends were observed in clinical trials for nivolumab. For this reason, taking into consideration AEs reported in at least 1% of patients of at least 1 pivotal clinical trial appeared to be more relevant than the usual threshold at 5% or 10%.
Then, the present article shows that the costs of management of some AEs are significant. More than half of the identified grades 3 and 4 AEs had a mean estimated cost of >€2,000. Moreover, the costs of AEs specifically reported with immunotherapy treatments were estimated at €3,457 for colitis, €3500 for elevated transaminases and €7,742 per year for type 1 diabetes.
There are some limitations to our study. Costs were calculated in the setting of French healthcare system and extrapolations to other countries should be cautious. Moreover, the assessment of medical resources was not obtained prospectively, but was based, in part, on literature data and expert opinion. Literature data were extracted from clinical trials and reporting of AEs is not standardized; sometimes only AEs of interest are reported. Moreover, the description of some AEs, for example, “infection,” was imprecise and could recover heterogeneous clinical situations.17 A possible criticism is the use of data from the study by Wehler et al who included patients with metastasis melanoma. Indeed, it could be argued that AEs have different medical impacts and costs according to the underlying disease. An additional limitation of literature data is the report of the rates and costs for grade 3 or 4 AEs only as a unique category. Indeed, some grade 4 AEs are potentially life-threatening with most probably an increase of the associated costs. Finally, the estimations of the management schedules of AEs rested on the opinions and experience of the 3 oncology experts who coauthored this article. Their point of view may be not representative of practices in France for the management of AEs in NSCLC. Moreover, the experts represented only a limited number of medical specialties and some costs could have been over- or underestimated. Nevertheless, possible discrepancies that would appear with a larger group of experts should be minimized. Indeed, the 3 experts agreed that the management of the AEs under discussion was rather standard and a consensus was easily achieved.
These limitations must be kept in mind and costs reported, in the present study, must be considered as an indication of the cost that payers have to consider for each AE. For future studies, it could be very helpful to prospectively record medical resource associated with predefined AEs in NSCLC.
Despite these limitations, the specific values reported in the present article for the most frequent grades 3 and 4 AEs in trials with NSCLC patients should be useful for future economic analyses. Indeed, both incidence and costs of hospitalization of these AEs were taken into account. Moreover, immunotherapy, which involves higher costs in comparison with previous treatments, was also considered. Modeling the overall burden of the management of AEs in NSCLC will allow comparisons between treatments with various safety profiles.
In conclusion, this study may be of interest for economic evaluations of new interventions in NSCLC. Among the identified AEs, a majority appeared to have an important economic impact, with a management cost of at least €2,000 mainly driven by hospitalization costs.
Acknowledgments
The abstract of this paper was presented at the ISPOR 19th Annual European Congress, as a poster presentation with interim findings.22 The poster’s abstract has also been published.23
Disclosure
CC has provided consulting services for AstraZeneca, Boehringer Ingelheim, Clovis, Hoffman la Roche, GSK, Lilly, Pfizer, BMS, MSD, Novartis and Amgen. EC and AM are employees of Creativ-Ceutical. CG, AF and LLB are employees of MSD France. DL has provided consulting services for MSD and BMS. EA has provided consulting services for MSD and GSK, has received research funding from AbbVie, Roche and Sanofi and benefited from travels, accommodations or expenses from AbbVie, Roche and Sanofi. The authors report no other conflicts of interest in this work.
References
World Health Organization. World Cancer Report 2014. Available from: http://apps.who.int/bookorders/anglais/detart1.jsp?codlan=1&codcol=76&codcch=31. Accessed June 17, 2017. | ||
Yang P. Epidemiology of lung cancer prognosis: quantity and quality of life. Methods Mol Biol. 2009;471:469–486. | ||
Institut National du Cancer. Le cancer du poumon: points clés [Lung cancer: key points]. Available from: http://www.e-cancer.fr/Patients-et-proches/Les-cancers/Cancer-du-poumon/Quelques-chiffres. Accessed June 17, 2017. French. | ||
Sher T, Dy GK, Adjei AA. Small cell lung cancer. Mayo Clin Proc. 2008;83(3):355–367. | ||
Reck M, Popat S, Reinmuth N, et al. Metastatic non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(Suppl 3):iii27–iii39. | ||
Losanno T, Gridelli C. Safety profiles of first-line therapies for metastatic non-squamous non-small-cell lung cancer. Expert Opin Drug Saf. 2016;15(6):837–851. | ||
Santabarbara G, Maione P, Rossi A, Gridelli C. Pharmacotherapeutic options for treating adverse effects of Cisplatin chemotherapy. Expert Opin Pharmacother. 2016;17(4):561–570. | ||
Di BS, Wei KP, Tian JH, et al. Effectiveness and safety of pemetrexed versus docetaxel as a treatment for advanced non-small cell lung cancer: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15(8):3419–3424. | ||
Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–1639. | ||
Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373(2):123–135. | ||
Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387(10027):1540–1550. | ||
Reck M, Rodriguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. | ||
Patel JD, Socinski MA, Garon EB, et al. PointBreak: a randomized Phase III study of pemetrexed plus carboplatin and bevacizumab followed by maintenance pemetrexed and bevacizumab versus paclitaxel plus carboplatin and bevacizumab followed by maintenance bevacizumab in patients with stage IIIB or IV nonsquamous non-small-cell lung cancer. J Clin Oncol. 2013;31(34):4349–4357. | ||
Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005;353(2):123–132. | ||
Garon EB, Ciuleanu TE, Arrieta O, et al. Ramucirumab plus docetaxel versus placebo plus docetaxel for second-line treatment of stage IV non-small-cell lung cancer after disease progression on platinum-based therapy (REVEL): a multicentre, double-blind, randomized phase 3 trial. Lancet. 2014;384(9944):665–673. | ||
US Department of Health and Human Services; National Institutes of Health; National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE); Version 4.0; 2009. Available from: https://www.eortc.be/services/doc/ctc/. Accessed June 17, 2017. | ||
Banz K, Bischoff H, Brunner M, et al. Comparison of treatment costs of Grade 3/4 adverse events associated with erlotinib or pemetrexed maintenance therapy for patients with advanced non-small-cell lung cancer (NSCLC) in Germany, France, Italy, and Spain. Lung Cancer. 2011;74(3):529–534. | ||
Nuijten MJ, de Castro Carpeno J, Chouaid C, et al. A cross-market cost comparison of erlotinib versus pemetrexed for first-line maintenance treatment of patients with locally advanced or metastatic non-small-cell lung cancer. Lung Cancer. 2012;76(3):465–471. | ||
Wehler E, Zhao Z, Pinar Bilir S, Munakata J, Barber B. Economic burden of toxicities associated with treating metastatic melanoma in eight countries. Eur J Health Econ. 2017;18(1):49–58. | ||
Vouk K, Benter U, Amonkar MM, et al. Cost and economic burden of adverse events associated with metastatic melanoma treatments in five countries. J Med Econ. 2016;19(9):900–912. | ||
Ricci P, Chantry M, Detournay B, Poutignat N, Kusnik-Joinville O, Raimond V, et al. Reimbursed health expenditures of people treated for diabetes by the French National Health Insurance Fund: 2001 and 2007 ENTRED Surveys. Bulletin Epidémiologique Hebdomadaire. 2009(42/43):464–469. | ||
Chouaid C, Angevin E, Godard C, et al. Costs of adverse events associated with cancer therapies in non-small cell lung cancer in France. Poster presented at: ISPOR 19th Annual European Congress; October 29 to November 2, 2016; Vienna, Austria. | ||
Chouaid C, Angevin E, Godard C, et al. Costs of adverse events associated with cancer therapies in non-small cell lung cancer in France. In: Poster abstracts. Value Health. 2016;19:A743. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.