Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Correlations Between Working Memory Impairment and Neurometabolites of the Prefrontal Cortex in Drug-Naive Obsessive-Compulsive Disorder
Authors Yue J, Zhong S, Luo A, Lai S, He T, Luo Y, Wang Y, Zhang Y, Shen S, Huang H, Wen S ![]() , Jia Y
, Jia Y
Received 9 December 2020
Accepted for publication 12 July 2021
Published 14 August 2021 Volume 2021:17 Pages 2647—2657
DOI https://doi.org/10.2147/NDT.S296488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Jihui Yue,1,2,* Shuming Zhong,1,* Aimin Luo,3 Shunkai Lai,1 Tingting He,4 Yuchong Luo,2 Ying Wang,5 Yiliang Zhang,1 Shiyi Shen,4 Hui Huang,4 Shenglin Wen,2 Yanbin Jia1
1Department of Psychiatry, First Affiliated Hospital, Jinan University, Guangzhou, Guangdong Province, People’s Republic of China; 2Department of Psychiatry, The Fifth Affiliated Hospital of Sun Yat-sen University, Zhuhai, Guangdong Province, People’s Republic of China; 3Department of Psychology, Guangdong Sanjiu Brain Hospital, Guangzhou, Guangdong Province, People’s Republic of China; 4School of Management, Jinan University, Guangzhou, Guangdong Province, People’s Republic of China; 5Medical Imaging Center, First Affiliated Hospital, Jinan University, Guangzhou, Guangdong Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanbin Jia
Department of Psychiatry, First Affiliated Hospital, Jinan University, Guangzhou, People’s Republic of China
Tel +86 13392489168
Fax +86 020-38688888
Email [email protected]
Purpose: This study aimed to investigate the mechanism of working memory (WM) impairment in drug-naive obsessive-compulsive disorder (OCD) by using neuropsychological tests and proton magnetic resonance spectroscopy (1H-MRS).
Patients and Methods: A total of 55 patients with drug-naive OCD and 55 healthy controls (HCs) were recruited for this study. The working memory (WM) was evaluated using the digit span test (DST), visual space memory test (VSMT), and the 2-back task and stroop color word test (SCWT). The bilateral metabolite levels of the prefrontal cortex (PFC) were evaluated by 1H-MRS, then determined the ratios of N-acetyl aspartate (NAA), choline-containing compounds (Cho), and myo-inositol (MI) to creatine (Cr). The independent sample t-test was used to analyse the differences in WM performance and neurometabolite ratios. Multivariate linear regression analysis was performed to screen the influential factors of WM, with an introduction level of 0.05 and a rejection level of 0.10.
Results: 1) Patients with OCD performed significantly worse on DST (score), VSMT (score), 2-back task (accuracy rate), SCWT (execution time) when compared with HCs. 2) NAA/Cr and Cho/Cr in the left PFC (lPFC) and MI/Cr ratios in the bilateral PFC of OCD patients were significantly lower when compared to HCs. 3) For OCD patients, the NAA/Cr ratio in the lPFC was negatively correlated with the score of DST (forwards), the Cho/Cr ratio in the lPFC was positively correlated with the accuracy rate of 2-back task, and the MI/Cr ratio in the right PFC (rPFC) was positively correlated with the score of DST (forwards) and the accuracy rate of VSMT. We also found that the compulsive symptoms showed a positive correlation with MI/Cr ratio of the rPFC.
Conclusion: Drug-naive OCD patients have demonstrated WM impairments, including phonological loop, visual-spatial sketchpad and central executive system, and the WM impairments might be associated with hypometabolism in the PFC, especially the lPFC.
Keywords: obsessive compulsive disorder, prefrontal cortex, working memory, neurometabolites, proton magnetic resonance spectroscopy
Introduction
Obsessive compulsive disorder (OCD) is a severe, chronic, and complex neuropsychiatric disorder,1,2 with a lifetime prevalence of 1% to 3%.3,4 The incidence of OCD has recently shown an upward trend, but its diagnosis and treatment are often delayed. In most cases of OCD, it usually takes approximately 8 years from symptom onset to medical treatment,5,6 and the effective rate of treatment remains only between 40% - 60%.7
Most studies in literature have confirmed that OCD involves cognitive impairment, which is considered as one of the neurophenotypic markers of OCD.8–12 Working memory (WM) is considered a key cognitive function13 and is closely related to OCD.14–16 WM is a psychological process that involves storing and processing of information when performing tasks and activities, which include verbal WM, visuospatial WM and central executive system (including updating, shifting and inhibitory functions). WM also supports other high-level cognitive abilities (including but not limited to general fluid intelligence, learning, problem solving and decision-making),17,18 as well as low-level psychological operations that require cognitive control.19,20 Recurrent intrusive thoughts and/or compulsions in OCD are often repetitive behaviors or mental acts, followed by checking, rumination, and disinhibition,1 and these are associated with poorer memory in OCD. For example, memory deficits might explain the compulsive checking behavior.21 Impaired response inhibition accounts for unstoppable repetitive rituals in OCD patients22. There exists a large body of working memory literature on OCD, and yet results from this literature are highly mixed, such as visuospatial WM and verbal memory.15,23,24 The inconsistent pattern of results described is possibly attributed to several factors, which include the highly heterogeneous nature of OCD, the high rate of comorbidity, and incomplete or inconsistent measurement tools. It is also possible that the mechanism of WM impairment in OCD remains unclear. Therefore, we used a more comprehensive assessment tools to study WM, including Digit Span Test (DST), Visual Reproduction Subtest (VSMT), 2-back task and Stroop Color Word Test (SCWT). DST mainly reflects the ability of spatial WM capacity as well as verbal WM, which is included in the phonological loop and episodic buffer subsystem. VSMT is used to measure the visuospatial WM, which is assumed to be responsible for processing and short-term storage of visuospatial information and is the part of visual-spatial sketchpad and episodic buffer.25,26 The 2-back task is one of the verbal n-back tasks, which is a commonly used paradigm to investigate verbal WM and updating function of the central executive system. SCWT is used to evaluate the updating, shifting and inhibitory functions of the central executive system.
A growing body of evidence in imaging studies also revealed neurobiological abnormalities in OCD, which is speculated to be a potential neuroimaging endophenotype.27–30 It has been particularly convincing in suggesting that prefrontal–basal ganglia–thalamic–prefrontal circuits are responsible for the mediation of OCD symptoms.29,30 Complementary approaches examining regional neurochemistry now assure additional insights into the neurobiology of OCD. Some studies have found that the imbalances in neuronal metabolite and neurotransmitter within CSTC circuit have been shown as the leading reasons of the OCD onset.31 In particular, the proton magnetic resonance spectroscopy (1H-MRS) permits in vivo quantification of specific neurochemicals in various regions of the brain. The most commonly reported resonances of 1H-MRS spectrum are N-acetyl aspartate (NAA), choline-containing (Cho) compounds, myo-inositol (MI), and creatine (Cr). The pathophysiology of OCD has been studied by 1H-MRS, but the results are still inconclusive.32,33 Like Pauls et al comments, there is little agreement between these investigations,28 and this is probably because of several factors, such as the sample size, in which most of the studies included low patient samples, with an average of 13 subjects per study. Secondly, the heterogeneity of the disease, wherein the samples are often included into heterogeneous groups (comorbidities, drugs/treatment, untreated, etc.). Thirdly, with regard to the inspection equipment of 1H-MRS technique, only 4 (14%) of 28 studies have used field strength ≥3-Tesla (3T).28,34 In order to reduce the above interference in the current study, we examined biochemical metabolites in the prefrontal cortex (PFC) of treatment-naïve, non-late-life OCD patients without comorbidity by using multi-voxel 3.0T 1H-MRS. The multi-voxel technique used in our study possesses the advantage of simultaneously obtaining multiple 1H-MRS spectra and allowing for examination of a larger volume of tissue than that by single voxel spectroscopy. In addition, the spectra of the normal human brains at 3.0T demonstrated a 20% improvement of the signal to noise ratios compared to 1.5T at a short TE.
The prefrontal cortex (PFC) is a key area of cortico-striato-thalamo-cortical (CSTC) circuit,30 and dysfunction in the PFC might be constituted as a neurophenotype of OCD. However, there is very little research till now that has been conducted in OCD patients on their WM and neurometabolites of the PFC. A combination of metabolic brain alterations with neuropsychological tests might be an effective way to explore the correlation between brain function change and OCD.
Therefore, we examined WM and biochemical metabolites in PFC of patients with drug-naive OCD in this study. We hypothesized that the deficits of WM and abnormal biochemical metabolism could be found in patients with drug-naive OCD. We were also interested in the relationship between WM and abnormal biochemical metabolism in drug-naive OCD. During this approach, characteristic changes of WM and metabolites in OCD patients were explored, and to find out the potentially unknown associations between neural mechanism and WM impairment in OCD.
Materials and Methods
Participants
A total of 55 patients affected by OCD (Diagnostic and Statistical Manual of Mental Disorder, 5th Edition - criteria, DSM-5) (APA, 2013) (29 males, 26 females; mean ± SD: 26.70±7.43 years of age), and 55 healthy controls (HCs) (21 males, 34 females; mean ± SD: 25.33±5.28 years of age) were studied. All subjects were right-handed and belonged to the Han ethnic group. All patients and HCs voluntarily participated in this study and signed an informed consent.
OCD Group
Between March 2014 and July 2015, 55 adults with OCD were recruited from the psychiatric department of the First Affiliated Hospital of Jinan University (Guangzhou, China). All patients were assessed by psychiatrists involved in the study. Written informed consent was obtained from all participants before any study procedure was performed.
The inclusion criteria of OCD group were as follows: diagnosed with OCD according to the DSM-5 criteria, aged between 18 and 50 years, educational level above junior high school, with a total score of the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) of ≥16 points (if only one of the compulsive behaviors or compulsive ideas exist, the evaluation standard then becomes to the total number of Y-BOCS scores of ≥8 points), psychiatric drug naive and treatment naive.
Exclusion criteria of OCD group were as follows: any other psychiatric axis-I or axis-II disorders, pregnant or lactating females, any other neurological disorders, brain organic mental disorders or somatic complaints, a history of alcohol or drug abuse, abnormal brain structure or magnetic resonance contraindications, achromatopsia or hemochromatosis, those who received electric convulsive treatment (ECT) recently or had long-term anti-psychotic drugs.
Healthy Control (HC) Group
A sample of 55 healthy volunteers was recruited by advertising. The inclusion criteria of control group were as follows: healthy adults, aged between 18 and 50, educational level above junior high school.
Exclusion criteria of control group were as follows: a history of psychiatric illness or a family history of mental disorders, pregnant or lactating females, brain organic mental disorders or somatic complaints, a history of alcohol or drug abuse, abnormal brain structure or magnetic resonance contraindications, and achromatopsia or hemochromatosis.
Clinical Assessments
A general information questionnaire was utilized to investigate the subject’s gender, age, nationality, marital status, profession, education, history of somatic diseases, history of drug allergy, status of smoking and alcohol addiction.
Y-BOCS: OCD symptom characteristics and severity were assessed using Y-BOCS. Those with a total score of 25 or more (simple obsessive thinking or compulsive behavior, only 15 points or more) were considered severe; 16–25 points (mere obsessive thinking or compulsive behavior, only 10–14 points) were considered moderately severe; 10–15 points were considered mildly severe; and 10 points were considered extremely low.
WM Assessments
DST (Wechsler, 2000) was used to measure the WM capacity and verbal WM, which consists of digit span forward (DSF) and digit span backward (DSB). Correct responses on the DSF and DSB were calculated. DST mainly reflects the ability of spatial WM capacity as well as verbal WM, which is included in the phonological loop and episodic buffer subsystem.
2-back task is one of verbal n-back task, which is a commonly used paradigm to investigate verbal WM and updating function of the central executive system. The 2-back task was programmed with E-prime 2.0 software. During the test, any number from 1 to 9 is randomly displayed in the center of the computer screen, each number is displayed for 1000 milliseconds, and the number is separated by 1000 milliseconds. If the currently displayed number is consistent with the previously displayed number, press “F” key; if the currently displayed number is inconsistent with the previous number, press “J” key. Reaction time and accuracy rate on the 2-back were calculated.
VSMT was also programmed with E-prime 2.0 software, which was used to measure the visuospatial WM (see Figure 1). During the test, a 4*4 black-and-white grid matrix appears in the center of the computer screen, in which blue patches are randomly distributed. After 1000 milliseconds, the blue color block disappeared, and then the participant marked the position of the blue color block in the blank square matrix. Subjects were requested again to recall the spatial location as quickly and as accurately as possible. Reaction time and accuracy rate on the VSMT were calculated.
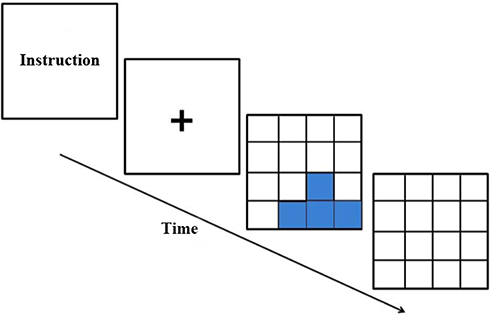 |
Figure 1 During the test, a 4*4 black-and-white grid matrix appears in the center of the computer screen, in which blue patches are randomly distributed. After 1000 milliseconds, the blue color block disappeared, and then the participant marked the position of the blue color block in the blank square matrix. Subjects were requested again to recall the spatial location as quickly and as accurately as possible. |
SCWT-CW was used to evaluate the updating, shifting and inhibitory functions of the central executive system. The stimulus card contains a total of 100 characters. Participants were required to name the color of each Chinese character in the displayed symbol card in turn (for example, the “green” character displayed in yellow font is named “yellow”). The reaction time on the SCWT-CW was calculated.
Image Acquisition
Magnetic resonance imaging (MRI) and 1H-MRS were performed using the Discovery MR 750 3.0 T MRI scanner (General Electric, Milwaukee, WI, USA) with a conventional gradient system. The gradient field strength used was 44mT/m and the gradient switching rate was 200T/m/s. An 8-channel head coil was used for radio-frequency transmission and reception of MR signal. The subjects’ heads were fixed by a sponge pad, in which the center line was in the middle, and symmetrical on both sides in order to avoid motion artifacts.
Routine axial T1-weighted fluid attenuation inversion recovery (T1Flair) [repetition time (TR) = 1750 ms, echo-time (TE) = 24 ms] and fast spin echo T2-weighted MR images (TR = 8400ms, TE = 145ms) were obtained to confirm the absence of any structural and signal abnormalities of the brain.
The magnetic resonance protocol was conducted in the axial plane with a T2-weighted fast spin-echo (FSE) sequence (TR = 3500 ms, TE = 102 ms, number of excitation (NEX) = 2, slice thickness = 5 mm, slice interval = 0 mm, 18 slices, field of view (FOV) = 24×24 cm, matric size = 256×256). For 1H-MRS studies, the location of the PFC volume of interest (VOI) was showed in Figure 2. The prefrontal lobe VOI was localized at the midline and included the dorsolateral prefrontal white matter and anterior cingulate gray regions bilaterally avoiding the striatum, ventricle, scalp, skull base, or sinuses. The posterior boundary of the VOI was placed adjacent to the anterior margin of the frontal horn of the lateral ventricle. The VOI was placed in a uniform manner by the same investigator. Forty-nine nominal voxels (7.5×7.5×10mm3) was included in the VOI. Single section 2D multivoxel 1H-MRS was acquired using a point-resolved spectroscopy sequence (PRESS) with water suppression by a chemical shift selective saturation (CHESS) pulse. The acquisition parameters were as follows: TR = 1000 ms, TE = 144 ms, NEX = 1, matric size = 18x18, FOV = 24×24 cm, slice thickness = 10 mm. Additional saturation bands were placed outside the VOI to minimize lipid contamination from the scalp. Automatic pre-scanning was performed before each spectroscopic scan to achieve an optional full width half maximum of 10 Hz. As a general quality standard spectrum, a line width of above 10 Hz or water suppression of above 98% was excluded. The acquisition time for 1H-MRS sequence was 5 min and 28s.
 |
Figure 2 Magnetic resonance image (MRI) scan of healthy controls showing the location of magnetic resonance spectroscopy (MRS) of volume of interest (VOI) placed in the PFC and proton magnetic resonance spectra in the left and right PFC. The large white box represents the VOIs for MRS acquisition, and small white boxes depict the individual VOIs for spectral analysis. Abbreviations: NAA, N-acetylaspartate; Cho, choline; mI, myo-inositol; Cr, creatine. |
The analyses of spectral dataset were performed using the Function Tool of GE 3.0 T workstation (Sun, Advantage Windows ADW4.5). The distribution maps of different metabolites were obtained, and then the distribution maps and MRI images were fused to obtain 1H-MRS curves. The software was used to automatically conduct the phase, frequency coding and baseline correction for the spectrum. The built-in software of MRI scanner automatically conducted the baseline calibration, signal average and metabolite identification, and measured the peak area of NAA, Cho, MI and Cr, and calculated the NAA/Cr, Cho/Cr and MI/Cr ratios. Each spectrum was evaluated for the peak area of NAA at 2.02 ppm, Cho at 3.22 ppm, MI at 3.0 ppm and Cr at 3.03 ppm. The voxel placements for spectroscopy and all data analyses were carried out by a trained radiologist who was blinded to the diagnosis of each subject.
Statistical Analysis
SPSS Statistical Package Version 20.0 was used for statistical analysis, and two-tailed significance level was set at p < 0.05. All indicators were measured for normal distributions by the Kolmogorov–Smirnov goodness-of-fit test. When comparing group differences in terms of demographics and clinical data, the t-test was used if continuous variables were normal. The Mann–Whitney U-test was used if continuous variables were skewed. Independent sample t-test (normal variables) or Mann–Whitney U (skewed variables) was used to test the differences in WM performance and neurometabolite ratios between OCD and control groups. Bonferroni correction for multiple comparisons was applied and p < 0.004 (0.05/14) was considered significant. Multivariate linear regression analysis was performed using WM of the case group as the dependent variable, and NAA/Cr, Cho/Cr, and MI/Cr ratios of the PFC as independent variables to screen the influential factors of WM, with an introduction level of 0.05 and rejection level of 0.10.
Results
Sample Characteristics
The demographics and clinical data of OCD group and HCs are shown in Table 1. A total of 55 patients with drug-naive OCD and 55 HCs were enrolled in this study. The two groups were matched by age (F = 1.122, p = 0.265), gender (X2 = 2.347, p = 0.126) and educational level (F = −0.335, p = 0.739). In the Y-BOCS score of all patients, the minimum score was 12 and the maximum score was 32 points.
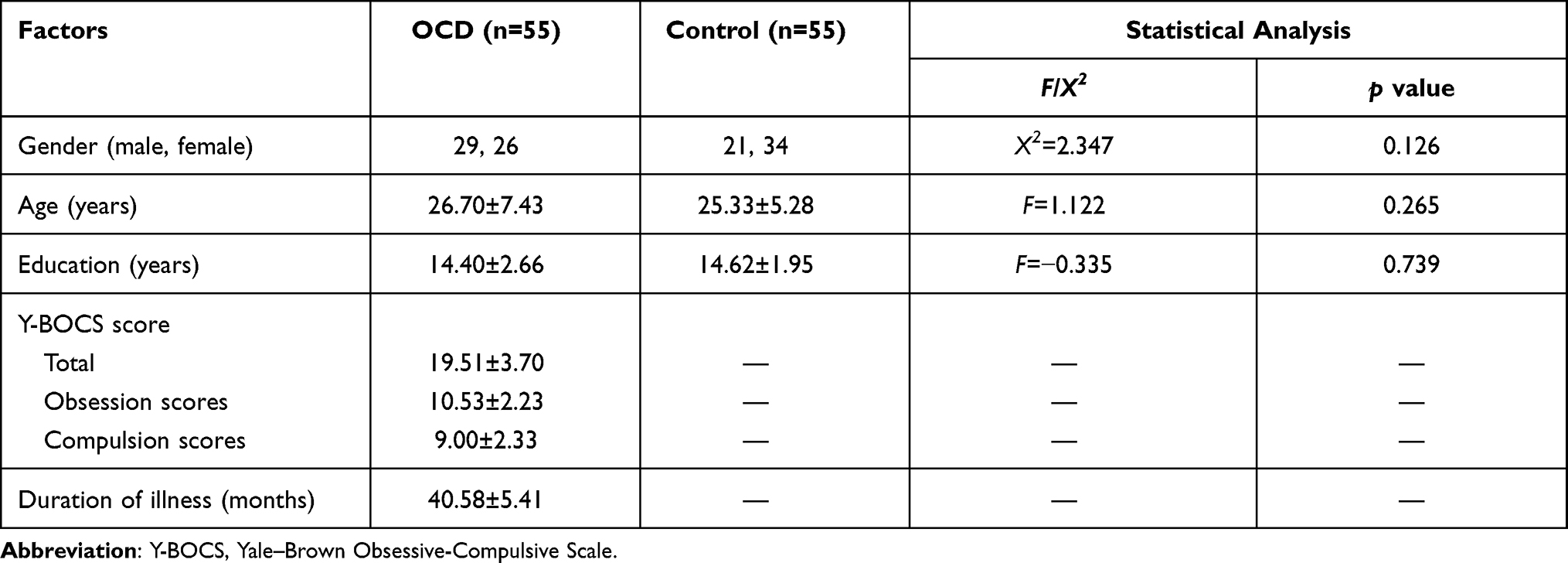 |
Table 1 Characteristics of Patients with OCD and HCs |
The Comparison of WM Indices Between Drug-Naive OCD and HCs
The independent sample t-test was used to compare the WM indices between the two groups, and the results are shown in Table 2. Compared to HCs, patients with OCD had significantly worse DST, VSMT, 2-back task (accuracy rate), and SCWT (execution time) (all p < 0.01). No statistical differences of 2-back task (reaction time) were observed between the two groups (p > 0.05).
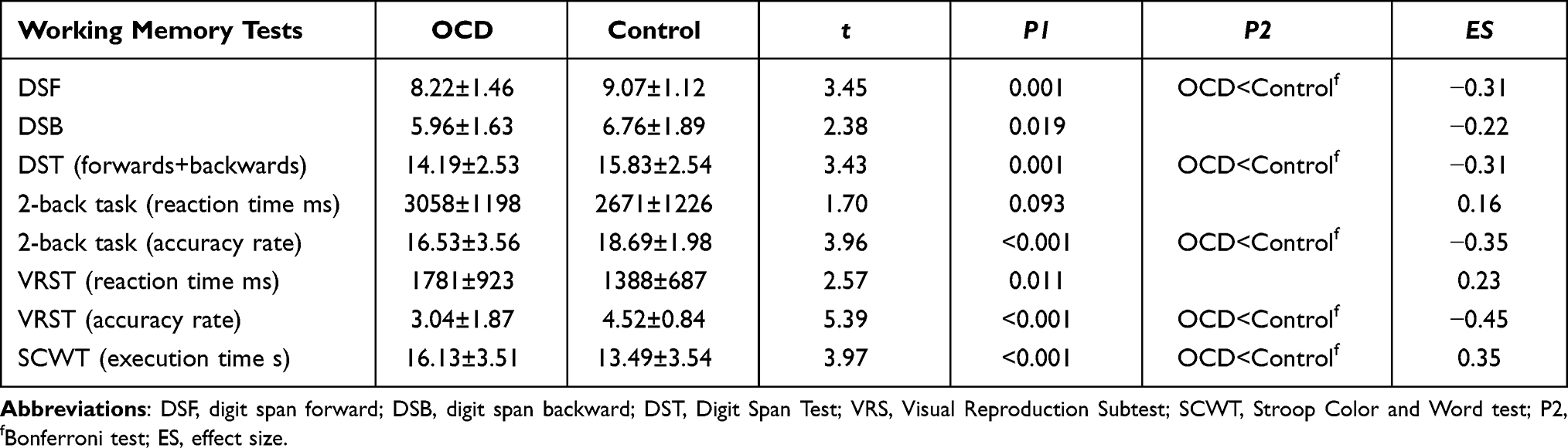 |
Table 2 Comparison of WM Indices Between Drug-Naive OCD and HCs |
Comparison of Neurometabolite Ratios in the PFC Between Drug-Naive OCD and HCs
The independent sample t-test was used to compare the NAA/Cr, Cho/Cr, and MI/Cr ratios of lPFC and rPFC between the two groups, and the results are shown in Table 3. Compared to HCs, patients with OCD had more reduction of NAA/Cr, Cho/Cr, MI/Cr ratios in the lPFC, while MI/Cr ratio in the rPFC, showed statistically significant differences (p < 0.05). There were no significant differences in the ratios of NAA/Cr and Cho/Cr of the rPFC between the two groups (p>0.05).
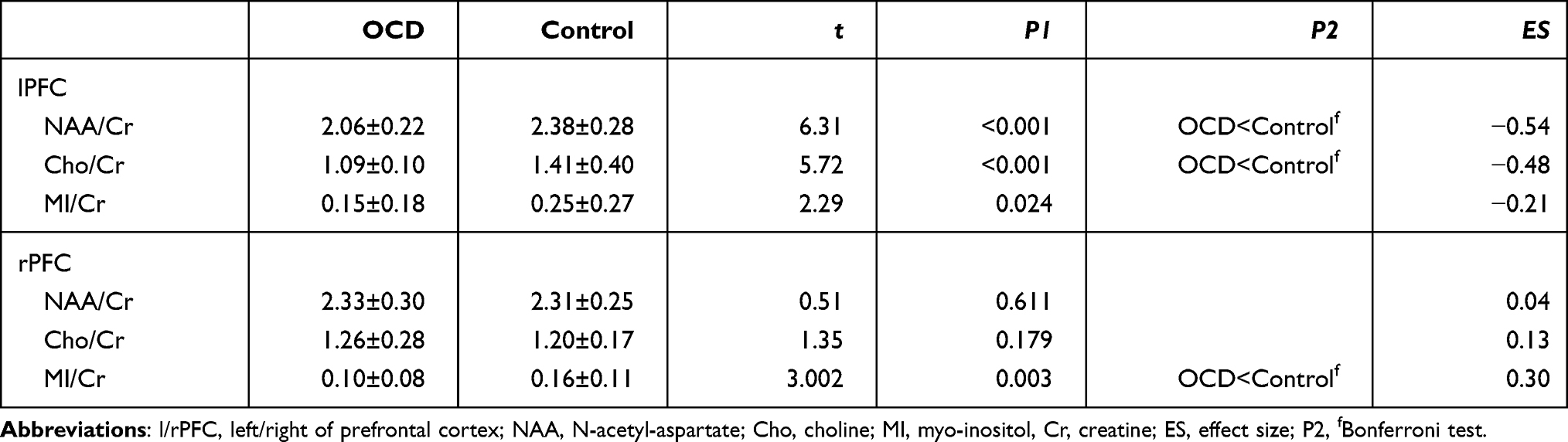 |
Table 3 Comparison of Neurometabolite Ratios in the PFC Between Drug-Naive OCD and HCs |
Correlations Between Abnormal Neurometabolite Ratios and WM Indices, Demographics and Clinical Symptoms in Patients with Drug-Naive OCD
The standardized residual histogram of WM showed an approximated normal distribution. A simple linear regression model was performed with NAA/Cr, Cho/Cr, and MI/Cr ratios of PFC as independent variables and age, gender, education level, duration of illness, Y-BOCS score and WM as a dependent variable. Multivariate linear regression stepwise regression method was used to screen the influential factors of WM. The results are shown in Table 4.
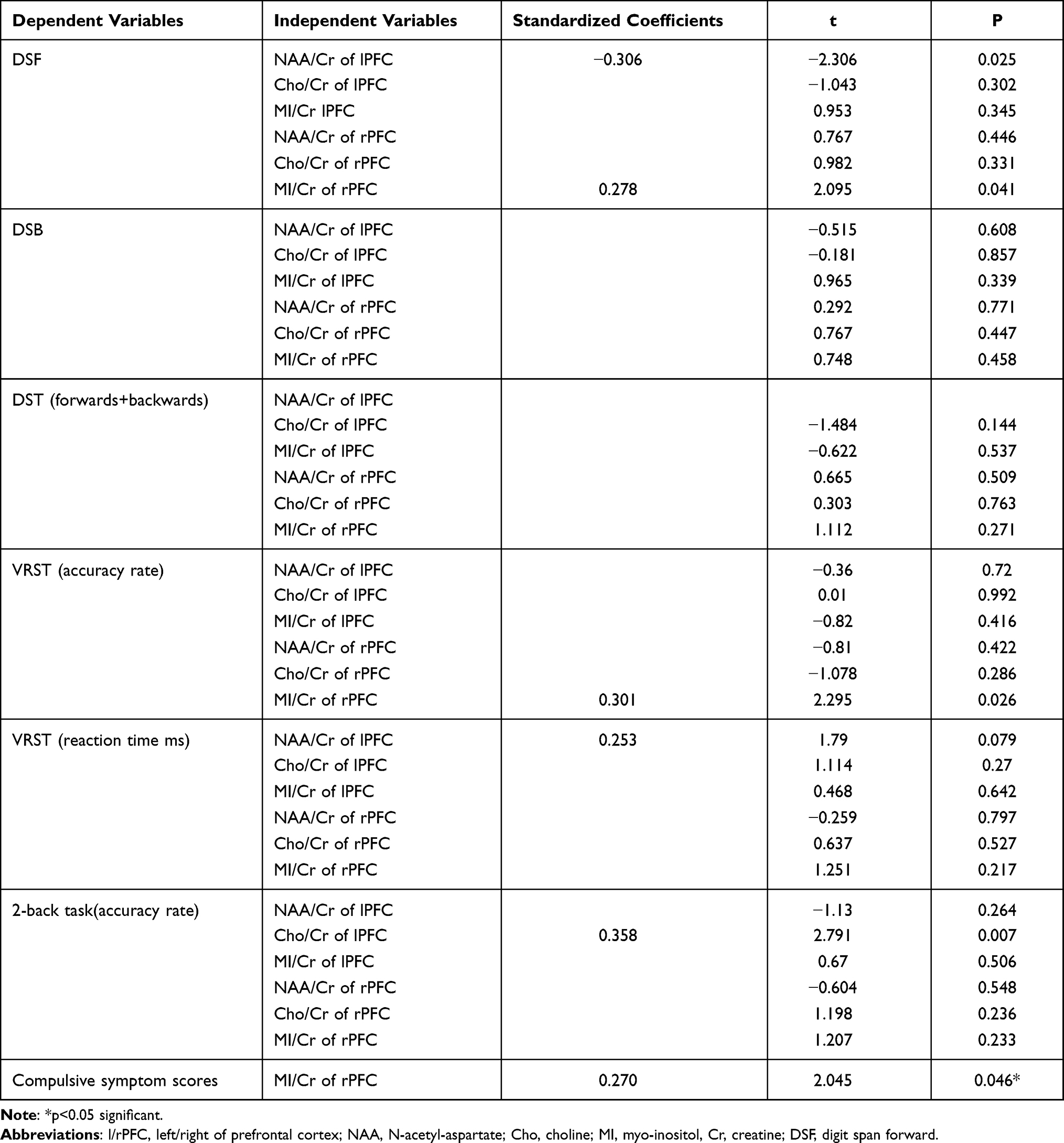 |
Table 4 Multiple Regression Analysis in Patients with OCD |
For OCD patients, the DSF showed a positive correlation with MI/Cr ratios of the rPFC and a negative correlation with NAA/Cr ratios of the lPFC (F = 4.062, R2 = 10.4%, p < 0.05), implying that approximately 10.4% of the DSF scores can be explained by the MI/Cr ratios of the rPFC and NAA/Cr ratios of the lPFC. The VSMT (accuracy rate) showed a positive correlation with MI/Cr ratios of the rPFC (F = 5.266, R2 = 0.09, p < 0.05), implying that approximately 9% of the VSMT (accuracy rate) scores can be explained by MI/Cr ratios of the rPFC. The 2-back task (accuracy rate) showed a positive correlation with Cho/Cr ratios of the lPFC (F = 7.79, R2 = 0.128, p < 0.05), implying that approximately 12.8% of the 2-back task (accuracy rate) scores can be explained by Cho/Cr ratios of the lPFC.
The compulsive symptoms showed a positive correlation with MI/Cr ratios of the rPFC (F = 3.96, R2 = 0.132, p<0.05), which implied that approximately 13.2% of the compulsive symptom scores can be explained by the MI/Cr ratios of the rPFC. We found no significant correlation between neurometabolite ratios and the other demographics and clinical symptoms.
Discussion
The major study findings are as follows. Patients with OCD performed significantly worse on DST (score), VSMT (score), 2-back task (accuracy rate), SCWT (execution time) when compared with HCs, and showed significantly lower NAA/Cr and Cho/Cr ratios in the left PFC (lPFC) and lower MI/Cr ratios in the bilateral PFC. For OCD patients, lower NAA/Cr ratio in the lPFC was negatively correlated with the score of DST (forwards), lower Cho/Cr ratio in the lPFC was positively correlated with the accuracy rate of 2-back task, and the MI/Cr ratio in the right PFC (rPFC) was positively correlated with the score of DST (forwards) and the accuracy rate of VSMT.
The verbal WM is measured by DST and the 2-back task methods. Results showed significant deficits in the performance with DST and 2-back task (accuracy rate), suggestive of a significant impairment of verbal WM in the OCD. This result was consistent with that of previous research findings.9,15 DSF showed a significant correlation with MI/Cr ratios of the rPFC and NAA/Cr ratios of lPFC, while the 2-back task (accuracy rate) showed a significant correlation with Cho/Cr of lPFC. Patients showed a significant decrease in NAA/Cr and Cho/Cr ratios in the lPFC, and MI/Cr ratios in the rPFC when compared to HCs. NAA is one of the most prominent metabolites in magnetic resonance spectrograms of the brain, and is considered as a marker of neuronal integrity and neuron density.35 Furthermore, the patients showed a significant decrease in NAA/Cr ratios in the lPFC and showed a negative correlation with DSF. Lentz et al investigated postmortem frontal lobe tissue by using high-spectral-resolution 1H MR spectroscopy of brain extracts and found NAA/Cr as a sensitive marker of neuronal injury.36 1H-MRS studies demonstrated decreased NAA concentration during psychiatric conditions, including affective disorder, OCD, schizophrenia and dementia, and the decrease of NAA levels is often located in regions of gray matter volume reduction, indicating neuronal reduction.35,37 Additionally, a study with the effect of 12-week treatment using citalopram on NAA/Cr ratios in 13 drug-naive patients with OCD showed a significant increase in the bilateral prefrontal cortex, frontal white matter and anterior cingulate when compared to those before treatment.38 So, the decrease of NAA/Cr ratios in the lPFC might indicate gray matter volume reduction and neuronal damage in OCD, which is closely related to verbal working memory impairment.
In the literature, there are rare reports on the decrease of choline levels of lPFC in OCD. Choline plays a central role in membrane structure and many physiological pathways, including the membrane-mediated cell signaling via phospholipases, acetylcholine synthesis, lipid transport, myelination, growth factor signaling, and methyl-group metabolism.39 Studies have found that choline deficiency can cause nerve cell damage or induce apoptosis, while choline supplementation can inhibit apoptosis and promote neural plasticity.40,41 There are many studies on choline metabolism in patients with OCD, and most of these focused-on thalamus, parietal white matter, hippocampus, striatal, caudate nucleus, and the anterior cingulate cortex among others.32,33 In this study, the patients showed a significant decrease in Cho/Cr ratios in the lPFC and showed a negative correlation with the 2-back task (accuracy rate). The 2-back task was carried out to investigate verbal WM and updating the function of the central executive system. Updating is the constant monitoring and rapid addition/deletion of WM contents, which can be measured through tests such as the n-back, which are typically considered as the probes of WM.42 The ability to acquire new information and manipulate it in real time is critical to adjust one’s behavior to meet the demands of the changing environment.25 So, the impairment of updating ability results in behavioral and cognitive inflexibility and this seems to be consistent with the clinical symptoms of OCD. Moreover, in this study, we also found that SCWT (execution time) showed significant deficits in the performance of the drug-naive OCD group, but we did not find its relationship to the neurometabolites in the brain. SCWT (execution time) can reflect the inhibition function and mainly involves prevention of target task being intervened by irrelevant information, suppressing reactions that are not in conformity with the situation and preventing secondary activation of unwanted internal information in memory. Our results in agreement with those of the previous studies, in which a prominent disturbance in the ability to inhibit the WM of OCD has been reported.16 We speculate that the lack of choline in lPFC may be closely related to the defects of verbal WM and the central executive system in OCD. Choline supplementation might be able to improve this condition, which may provide another option for the treatment of obsessive-compulsive disorder, but further research is needed in the future.
The visuospatial WM is measured by VSMT. In the current study, the results showed significant deficits in performance with VRST (accuracy rate), suggesting a significant impairment of the visuospatial WM in the OCD. When compared to HCs, patients with OCD showed a significant decrease of MI/Cr ratios in the rPFC, which showed a positive correlation with VSMT (accuracy rate). Visual-spatial WM is mainly involved in the maintenance and control of visual and spatial information. Disturbance of the visuospatial WM suggests that OCD has disturbances in maintaining and controlling external information, similar results were found in previous study, but measured it with Cambridge Neuropsychological Automated Battery (CANTAB).43 Myoinositol (MI) is located mainly in the glial cells of the brain, and is considered as a glial marker, and its content is believed to relate with glial cells proliferation.44,45 It might participate in the protection against osmotic shock, signaling pathways, vesicle endocytosis and exocytosis.44 Alterations in the MI levels of brain are associated with diseases of central nervous system, such as schizophrenia, bipolar disorders, and cognitive impairment.45–47 1H-MRS findings in OCD have reported less on the alterations of MI in OCD subjects before 2012.33 Some recent studies on OCD have also found changes in the levels of inositol metabolism in the brain. Parmar et al38 have found significant increase in inositol levels in the caudate nucleus and anterior cingulate cortex of OCD. It is positively correlated with the compulsive symptoms and disease severity, and it is speculated to be related to the potential reversible abnormalities in regulating the neuro-osmotic pressure. Another study48 measured the metabolite levels in the left and right prefrontal white matter and found that children and adolescents with OCD did not differ from those of controls in MI metabolite levels. The metabolic concentration of MI in patients with OCD is increased significantly by 52% when compared with HCs. However, this study included a small sample size (only 14 OCD patients and 14 healthy individuals), and some patients received medications (escitalopram or fluvoxamine). Also, we found out that the levels of MI in bilateral PFC were reduced, which has not been reported in previous studies. MI is also a brain metabolite related to important functions of phosphatidylinositol second messenger system (PI-cycle), and is associated with mental disorders such as OCD, generalized anxiety disorder or schizophrenia.49 MI is transformed by various receptors attached to the PI-cycle, and its concentration or function changes the way the PI-cycle affects specific neurons.50 The abnormal metabolism of MI has extensive effects on neurologic pathways and changes in PI-cycle activation, which might induce OCD. According to our results, verbal and visual-spatial impairments in OCD patients may be closely related to decreased MI metabolism.
Therefore, this study suggests an extensive and significant impairment of WM in OCD including verbal WM, visuospatial WM and central executive system, which may be closely related to the abnormal metabolism of PFC in patients with OCD and may be an important cause of WM damage.
Limitations
This study might offer laboratory markers for etiological studies, and perhaps enhance the identification of WM impairment in OCD. However, some potential limitations in the current study should be taken into account when conducting future research. Firstly, due to statistical effect of the results, the sample size might be reduced, and future studies are needed to expand the sample size, allowing us to verify the results again. Secondly, this study is a cross-sectional study. Longitudinal studies are required to validate these findings. Thirdly, all patients had both obsessive thinking and compulsive behavior, and so the subtype analysis could not be carried out. Fourthly, although a battery of common neuropsychological WM tasks was used in our study, it was still not comprehensive enough to address various aspects of WM. In addition, we investigated WM functions without controlling for executive dysfunction and intelligence quotient (IQ) that could affect WM results (eg short-term memory, attention, vigilance etc.). Lastly, OCD is a disease with abnormal brain regions. In this study, only one ROI region was selected using 1H MRS, and we could not clarify the metabolism of other brain regions.
Conclusion
In conclusion, these preliminary data suggest that the WM of drug-naive OCD is damaged, involving verbal WM, visual WM and central executive system. Also, our study supported the hypothesis of PFC hypometabolism, especially the lPFC, which showed close relation to the WM impairment, and this might be the pathological mechanism of WM.
Ethics Committee Approval
The study was approved by the Regional Ethics Committee of the First Affiliated Hospital of Jinan University District and performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Acknowledgments
We would like to thank all the participants for their contribution to this study. The study was supported by the National Natural Science Foundation of China (No: 81671351; 81801347). The funders have not played any role in the study design, data collection, analysis, manuscript writing and decision to publish.
Disclosure
The authors report no conflicts of interest in this work. None of the authors have any actual or potential conflicts of interest including any financial, personal or other relationships with other people or organizations during the study period.
References
1. Hirschtritt ME, Bloch MH, Mathews CA. Obsessive-compulsive disorder: advances in diagnosis and treatment. JAMA. 2017;317:1358–1367. doi:10.1001/jama.2017.2200
2. Murphy DL, Moya PR, Fox MA, et al. Anxiety and affective disorder comorbidity related to serotonin and other neurotransmitter systems: obsessive-compulsive disorder as an example of overlapping clinical and genetic heterogeneity. Philos Trans R Soc Lond B Biol Sci. 2013;368:20120435. doi:10.1098/rstb.2012.0435
3. Ruscio AM, Stein DJ, Chiu WT, et al. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. 2010;15:53–63. doi:10.1038/mp.2008.94
4. Karno M, Golding JM, Sorenson SB, et al. The epidemiology of obsessive-compulsive disorder in five US communities. Arch Gen Psychiatry. 1988;45:1094–1099. doi:10.1001/archpsyc.1988.01800360042006
5. Altamura AC, Buoli M, Albano A, et al. Age at onset and latency to treatment (duration of untreated illness) in patients with mood and anxiety disorders: a naturalistic study. Int Clin Psychopharmacol. 2010;25:172–179. doi:10.1097/YIC.0b013e3283384c74
6. Dell’Osso B, Camuri G, Benatti B, et al. Differences in latency to first pharmacological treatment (duration of untreated illness) in anxiety disorders: a study on patients with panic disorder, generalized anxiety disorder and obsessive-compulsive disorder. Early Interv Psychiatry. 2013;7:374–380. doi:10.1111/eip.12016
7. Pallanti S, Quercioli L. Treatment-refractory obsessive-compulsive disorder: methodological issues, operational definitions and therapeutic lines. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30:400–412. doi:10.1016/j.pnpbp.2005.11.028
8. Abramovitch A, Abramowitz JS, Mittelman A. The neuropsychology of adult obsessive-compulsive disorder: a meta-analysis. Clin Psychol Rev. 2013;33:1163–1171. doi:10.1016/j.cpr.2013.09.004
9. Bragdon LB, Gibb BE, Coles ME. Does neuropsychological performance in OCD relate to different symptoms? A meta-analysis comparing the symmetry and obsessing dimensions. Depress Anxiety. 2018;35:761–774. doi:10.1002/da.22785
10. Marzuki AA, Pereira DSA, Sahakian BJ, et al. Are candidate neurocognitive endophenotypes of OCD present in paediatric patients? A systematic review. Neurosci Biobehav Rev. 2020;108:617–645. doi:10.1016/j.neubiorev.2019.12.010
11. Negreiros J, Belschner L, Best JR, et al. Neurocognitive risk markers in pediatric obsessive-compulsive disorder. J Child Psychol Psychiatry. 2020;61:605–613. doi:10.1111/jcpp.13153
12. Rajender G, Bhatia MS, Kanwal K, et al. Study of neurocognitive endophenotypes in drug-naive obsessive-compulsive disorder patients, their first-degree relatives and healthy controls. Acta Psychiatr Scand. 2011;124:152–161. doi:10.1111/j.1600-0447.2011.01733.x
13. Silver H, Feldman P, Bilker W, et al. Working memory deficit as a core neuropsychological dysfunction in schizophrenia. Am J Psychiatry. 2003;160:1809–1816. doi:10.1176/appi.ajp.160.10.1809
14. de Vries FE, de Wit SJ, Cath DC, et al. Compensatory frontoparietal activity during working memory: an endophenotype of obsessive-compulsive disorder. Biol Psychiatry. 2014;76:878–887. doi:10.1016/j.biopsych.2013.11.021
15. Harkin B, Kessler K. The role of working memory in compulsive checking and OCD: a systematic classification of 58 experimental findings. Clin Psychol Rev. 2011;31:1004–1021. doi:10.1016/j.cpr.2011.06.004
16. Heinzel S, Kaufmann C, Grutzmann R, et al. Neural correlates of working memory deficits and associations to response inhibition in obsessive compulsive disorder. Neuroimage Clin. 2018;17:426–434. doi:10.1016/j.nicl.2017.10.039
17. Chuderski A, Necka E. The contribution of working memory to fluid reasoning: capacity, control, or both? J Exp Psychol Learn Mem Cogn. 2012;38:1689–1710. doi:10.1037/a0028465
18. Shipstead Z, Harrison TL, Engle RW. Working memory capacity and fluid intelligence: maintenance and disengagement. Perspect Psychol Sci. 2016;11:771–799. doi:10.1177/1745691616650647
19. Grunewaldt KH, Lohaugen GC, Austeng D, et al. Working memory training improves cognitive function in VLBW preschoolers. Pediatrics. 2013;131:e747–e754. doi:10.1542/peds.2012-1965
20. Redick TS, Shipstead Z, Meier ME, et al. Cognitive predictors of a common multitasking ability: contributions from working memory, attention control, and fluid intelligence. J Exp Psychol Gen. 2016;145:1473–1492. doi:10.1037/xge0000219
21. Alcolado GM, Radomsky AS. A novel cognitive intervention for compulsive checking: targeting maladaptive beliefs about memory. J Behav Ther Exp Psychiatry. 2016;53:75–83. doi:10.1016/j.jbtep.2015.02.009
22. Silveira VP, Frydman I, Fontenelle LF, et al. Exploring response inhibition and error monitoring in obsessive-compulsive disorder. J Psychiatr Res. 2020;126:26–33. doi:10.1016/j.jpsychires.2020.04.002
23. Moritz S, Kloss M, von Eckstaedt FV, et al. Comparable performance of patients with obsessive-compulsive disorder (OCD) and healthy controls for verbal and nonverbal memory accuracy and confidence: time to forget the forgetfulness hypothesis of OCD? Psychiatry Res. 2009;166:247–253. doi:10.1016/j.psychres.2008.02.006
24. Gold JM, Barch DM, Feuerstahler LM, et al. Working memory impairment across psychotic disorders. Schizophr Bull. 2019;45:804–812. doi:10.1093/schbul/sby134
25. Baddeley A. Working memory. Curr Biol. 2010;20:R136–R140. doi:10.1016/j.cub.2009.12.014
26. Baddeley A. Working memory: looking back and looking forward. Nat Rev Neurosci. 2003;4:829–839. doi:10.1038/nrn1201
27. Yang X, Luo J, Zhong Z, et al. Abnormal regional homogeneity in patients with obsessive-compulsive disorder and their unaffected siblings: a resting-state fMRI study. Front Psychiatry. 2019;10:452. doi:10.3389/fpsyt.2019.00452
28. Pauls DL, Abramovitch A, Rauch SL, et al. Obsessive-compulsive disorder: an integrative genetic and neurobiological perspective. Nat Rev Neurosci. 2014;15:410–424. doi:10.1038/nrn3746
29. Menzies L, Chamberlain SR, Laird AR, et al. Integrating evidence from neuroimaging and neuropsychological studies of obsessive-compulsive disorder: the orbitofronto-striatal model revisited. Neurosci Biobehav Rev. 2008;32:525–549. doi:10.1016/j.neubiorev.2007.09.005
30. Saxena S, Rauch SL. Functional neuroimaging and the neuroanatomy of obsessive-compulsive disorder. Psychiatr Clin North Am. 2000;23:563–586. doi:10.1016/S0193-953X(05)70181-7
31. Zhu Y, Fan Q, Han X, et al. Decreased thalamic glutamate level in unmedicated adult obsessive-compulsive disorder patients detected by proton magnetic resonance spectroscopy. J Affect Disord. 2015;178:193–200. doi:10.1016/j.jad.2015.03.008
32. Gnanavel S, Sharan P, Khandelwal S, et al. Neurochemicals measured by (1) H-MRspectroscopy: putative vulnerability biomarkers for obsessive compulsive disorder. Magma. 2014;27:407–417. doi:10.1007/s10334-013-0427-y
33. Brennan BP, Rauch SL, Jensen JE, et al. A critical review of magnetic resonance spectroscopy studies of obsessive-compulsive disorder. Biol Psychiatry. 2013;73:24–31. doi:10.1016/j.biopsych.2012.06.023
34. Vester EL, de Joode NT, Vriend C, et al. Little evidence for neurometabolite alterations in obsessive-compulsive disorder - A systematic review of magnetic resonance spectroscopy studies at 3 Tesla. J Obsessive Compuls Relat Disord. 2020;25:100523. doi:10.1016/j.jocrd.2020.100523
35. Moffett JR, Ross B, Arun P, et al. N-acetylaspartate in the CNS: from neurodiagnostics to neurobiology. Prog Neurobiol. 2007;81:89–131. doi:10.1016/j.pneurobio.2006.12.003
36. Lentz MR, Kim JP, Westmoreland SV, et al. Quantitative neuropathologic correlates of changes in ratio of N-acetylaspartate to creatine in macaque brain. Radiology. 2005;235:461–468. doi:10.1148/radiol.2352040003
37. Paslakis G, Traber F, Roberz J, et al. N-acetyl-aspartate (NAA) as a correlate of pharmacological treatment in psychiatric disorders: a systematic review. Eur Neuropsychopharmacol. 2014;24:1659–1675. doi:10.1016/j.euroneuro.2014.06.004
38. Parmar A, Sharan P, Khandelwal SK, et al. Brain neurochemistry in unmedicated obsessive-compulsive disorder patients and effects of 12-week escitalopram treatment: (1) H-magnetic resonance spectroscopy study. Psychiatry Clin Neurosci. 2019;73:386–393. doi:10.1111/pcn.12850
39. Zeisel SH. Choline: an essential nutrient for humans. Nutrition. 2000;16:669–671. doi:10.1016/S0899-9007(00)00349-X
40. Jadavji NM, Emmerson JT, MacFarlane AJ, et al. B-vitamin and choline supplementation increases neuroplasticity and recovery after stroke. Neurobiol Dis. 2017;103:89–100. doi:10.1016/j.nbd.2017.04.001
41. Borges AA, El-Batah PN, Yamashita LF, et al. Neuroprotective effect of oral choline administration after global brain ischemia in rats. Nutr Neurosci. 2015;18:265–274. doi:10.1179/1476830514Y.0000000125
42. Gruner P, Pittenger C. Cognitive inflexibility in obsessive-compulsive disorder. Neuroscience. 2017;345:243–255. doi:10.1016/j.neuroscience.2016.07.030
43. Kim KL, Christensen RE, Ruggieri A, et al. Cognitive performance of youth with primary generalized anxiety disorder versus primary obsessive-compulsive disorder. Depress Anxiety. 2019;36:130–140. doi:10.1002/da.22848
44. Haris M, Cai K, Singh A, et al. In vivo mapping of brain myo-inositol. Neuroimage. 2011;54:2079–2085. doi:10.1016/j.neuroimage.2010.10.017
45. Brand A, Richter-Landsberg C, Leibfritz D. Multinuclear NMR studies on the energy metabolism of glial and neuronal cells. Dev Neurosci. 1993;15:289–298. doi:10.1159/000111347
46. Bustillo JR, Jones T, Qualls C, et al. Proton magnetic resonance spectroscopic imaging of gray and white matter in bipolar-I and schizophrenia. J Affect Disord. 2019;246:745–753. doi:10.1016/j.jad.2018.12.064
47. Voevodskaya O, Poulakis K, Sundgren P, et al. Brain myoinositol as a potential marker of amyloid-related pathology: a longitudinal study. Neurology. 2019;92:e395–e405. doi:10.1212/WNL.0000000000006852
48. Weber AM, Soreni N, Stanley JA, et al. Proton magnetic resonance spectroscopy of prefrontal white matter in psychotropic naive children and adolescents with obsessive-compulsive disorder. Psychiatry Res. 2014;222:67–74. doi:10.1016/j.pscychresns.2014.02.004
49. Kim H, McGrath BM, Silverstone PH. A review of the possible relevance of inositol and the phosphatidylinositol second messenger system (PI-cycle) to psychiatric disorders–focus on magnetic resonance spectroscopy (MRS) studies. Hum Psychopharmacol. 2005;20:309–326. doi:10.1002/hup.693
50. Vaden DL, Ding D, Peterson B, et al. Lithium and valproate decrease inositol mass and increase expression of the yeast INO1 and INO2 genes for inositol biosynthesis. J Biol Chem. 2001;276:15466–15471. doi:10.1074/jbc.M004179200
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.