Back to Journals » International Journal of General Medicine » Volume 14
Correlation Study of Galectin-3 in Patients with an Ascending Aortic Aneurysm and Ventricular Remodeling Before and After Surgical Correction
Authors Gu JJ, Cheng ZH, Bu JQ, Zhang WL, Chen LH, Chen ZY
Received 24 August 2021
Accepted for publication 13 October 2021
Published 30 November 2021 Volume 2021:14 Pages 9001—9006
DOI https://doi.org/10.2147/IJGM.S335300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jian-Jun Gu, Zhi-Hong Cheng, Ji-Qiang Bu, Wen-Li Zhang, Li-Hua Chen, Zi-Ying Chen
Department of Cardiac Surgery, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China
Correspondence: Zi-Ying Chen
Department of Cardiac Surgery, The Second Hospital of Hebei Medical University, No. 215, Heping Road, Shijiazhuang, Hebei, 050000, People’s Republic of China
Tel +86 15803210520
Email [email protected]
Objective: The present study aims to observe the changes in galectin-3 (Gal-3) expression levels in patients with an ascending aortic aneurysm and ventricular remodeling and analyze Gal-3’s correlation with ventricular remodeling.
Methods: A total of 102 patients with an ascending aortic aneurysm were included as the research subjects. Gal-3 expression levels in the peripheral blood of the patients were detected by an enzyme-linked immunosorbent assay before the operation and then three and six months after. The left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVEDD), interventricular septal thickness, and left ventricular posterior wall thickness were recorded, and the left ventricular mass index (LVMI) was calculated. Changes in Gal-3 expression levels, LVMI, LVEF, and LVEDD were observed before and after surgery, and these changes were then analyzed.
Results: There were significant differences in Gal-3 expression levels, LVMI, and LVEDD before surgery and three months after (P < 0.001) but no significant difference in LVEF (P = 0.887). There were significant differences in Gal-3 expression levels, LVMI, LVEDD, and LVEF (P < 0.05) three and six months after surgery. Before surgery and three and six months after surgery, Gal-3 was positively correlated with LVMI and LVEDD (R = 0.697, R = 0.571, and R = 0.454, respectively), and a receiver operating characteristic curve found that Gal-3 was able to predict ventricular remodeling, with an area under the curve value of 0.721.
Conclusion: Gal-3 expression levels are correlated with ascending aortic aneurysms combined with ventricular remodeling, which provides a reference value for predicting ventricular remodeling.
Keywords: ascending aortic aneurysm, ventricular remodeling, galectin-3, left ventricular mass index, ascending aortic replacement
Introduction
Ascending aortic aneurysm-like expansion (ascending aortic aneurysm) is a cardiovascular disease that threatens human health. Despite the rapid developments in modern medicine, the number of patients with ascending aortic aneurysms is growing globally, and its prevalence increases significantly with age. In 2018, about 200 million people worldwide suffered from an ascending aortic aneurysm, resulting in the deaths of more than 2.6 million people.1 The main risk factors for ascending aortic aneurysms are hypertension, smoking, hypercholesterolemia, and type-2 diabetes, of which hypertension is the most pathogenic. Physiologically, it is normal for the elastic media of the aorta to become finer with age and the diameter of the ascending aorta to increase. Hypertension increases the tension of the aortic wall and accelerates the rupture of the elastic media, resulting in aortic expansion and reduced compliance. At the same time, blood pressure continues to rise, aggravating the biological changes of the aortic wall,2 and this vicious cycle increases the left ventricular afterload, leading to ventricular remodeling and further damage to heart function, resulting in irreversible heart failure, loss of surgical opportunity, and increased patient mortality. Current studies have shown that ventricular remodeling is the heart’s response to changes in hemodynamics and metabolic disorders,3 which is mainly manifested as pathological changes in ventricular myocytes caused by hypertrophy, necrosis, and apoptosis of the myocardial cells. The decrease in myocardial parenchymal cells, the proliferation of interstitial cells, and the proliferation of fibroblasts in the myocardium are pathological processes closely related to ventricular remodeling.4 Previous studies have identified that there are a large number of cytokines involved in this pathological process. In recent years, studies on galectin-3 (Gal-3) have shown that it is involved in the process of collagen deposition and fibrin aggregation in body tissue fibrosis. Following an injury to the myocardium, a large number of local macrophages infiltrate it, and Gal-3 is then secreted into the circulation, activating the proliferation of fibroblasts and myofibroblasts and the deposition of type-I collagen, which ultimately leads to ventricular remodeling.5,6 Animal experiments have also shown that injecting Gal-3 into the pericardium of mice can cause ventricular remodeling, and the higher the level of Gal-3 expression, the more severe the degree of ventricular remodeling.7 However, the Gal-3 inhibitor, N-acetyl-seryl-aspartyl-lysyl-proline, injected into the pericardium of mice at the same time as Gal-3, can improve ventricular remodeling to a certain extent.8
Although ventricular remodeling is a highly complex pathophysiological process, it is becoming more common in clinical work. Gal-3 is very important for the occurrence and development of ventricular remodeling, but the relationship between Gal-3 and ventricular remodeling needs further study. Therefore, the present study aims to analyze Gal-3’s correlation with ventricular remodeling and its ability to predict the occurrence of ventricular remodeling, which has important clinical significance.
Methods
This study was conducted in accordance with the Declaration of Helsinki and reviewed and approved by the Ethics Committee of the Second Hospital of Hebei Medical University. Each patient signed an informed consent form. The research objects were 109 patients with ascending aortic aneurysms at the Department of Heart Surgery, Second Hospital of Hebei Medical University, 2018 to 2020; general information on these patients are listed in Table 1.
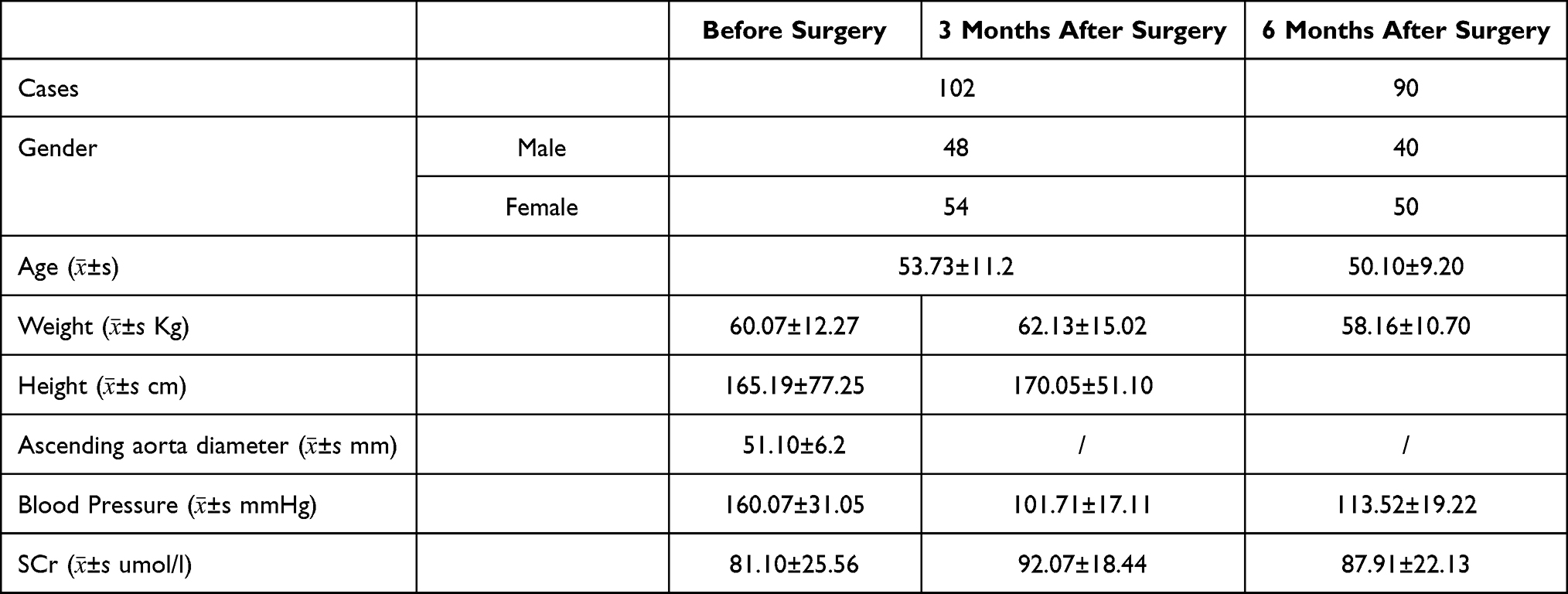 |
Table 1 General Information of the Research Subjects |
Inclusion criteria: patients diagnosed with ascending aortic aneurysms by aortic angiography and echocardiography, in accordance with the indications for surgery.
Exclusion criteria: (1) patients whose ascending aortic aneurysm ruptured and who died before surgery; (2) patients with severe heart failure who were not able to tolerate surgery after drug treatment, accompanied by severe liver and kidney dysfunction, immune diseases, pulmonary hypertension, pulmonary fibrosis, acute myocardial infarction, and malignant tumors; (3) patients who had experienced malignant heart and cerebrovascular events after surgery (including sudden cardiac death, stroke, and ventricular fibrillation); (4) patients who withdrew from the trial for any reason.
The following data on the patients were recorded: age (years), gender, height (cm), weight (kg), and body surface area (BSA; 0.0061 × height + 0.0124 × weight − 0.0099).
The GAL-3 expression level detection method: after the patient was admitted to the hospital, 5 mL of blood was collected in the morning. The sample was centrifuged at 3000 rpm for 5 min. Then, 2 mL of the uppermost plasma was taken for the study sample and was placed in –30°C refrigerated preservation, enzyme-linked immunoadsorption method. In the expression level of GAL-3 in the sample, the detection machine model is MK3, and the kit is Shanghai Key Industrial Co., Ltd.
The cardiac ultrasound detection method: the patient’s chest was exposed on the left lateral position, and the coupling agent was applied to the detection site, using the cardiac phase of the US GE Logiq E8 ultrasound (frequency of 2–4 MHz) to scan all parameters measured during end-expiration. Three consecutive images were recorded, and the mean values of these measurements were used for statistical analysis. It detected and recorded LVEDD (left-ventricular end-diastolic diameter), IVST (interventricular septal thickness), PWT (posterior wall thickness), LVEF (left ventricular ejection fraction), and the data from video recordings of 10 randomly selected patients were analyzed twice by the same observer within a period between the two observations of approximately two weeks. Intraobserver variability was expressed, according to the following formula: left ventricular mass (LVM) = 0.8×1.04 ([IVST + LVEDD + PWT] 3 − LVEDD3) + 0.6. Then, LVM/BSA was used to calculate the LVM index (LVMI). According to the Devereux standard, males LVMI were ≥125 g/m2, while females LVMI were ≥110 g/m2, suggesting left ventricular muscle hypertrophy, we believe that it was ventricular reconstruction. The patients underwent general anesthesia + extracorporeal circulation to replace the ascending aorta and were discharged after the standard treatment. Follow-up was conducted three and six months after surgery. During the follow-up, general patient information was recorded. Samples were then collected, refrigerated, and tested in the same way as mentioned above. The same echocardiologist examined the patient’s ultrasound chart for indicators, and any adverse cardiovascular events were recorded (including ventricular tachycardia, ventricular fibrillation, cardiogenic shock, and death).
The primary observation index was Gal-3, and the secondary observation indicators were the LVMI, LVEDD, and LVEF measurements.
Statistical Methods
The measurement data were tested for normal distribution. The results were expressed as mean ± standard deviation. Comparisons between the groups were performed with the t-test or chi-squared test. The statistical data were processed using SPSS 26.0 statistical software. P < 0.05 was considered to be statistically significant. A minor Pearson correlation analysis was applied to the observation indexes, and a receiver operating curve (ROC) was drawn to obtain the area under the curve (AUC) to assess the ability of Gal-3 expression levels to predict the occurrence of ventricular remodeling. A value of AUC <0.5 meant that there was no predictive value, 0.5–0.7 had a low predictive value, 0.7–0.9 had a medium predictive value, and >0.9 had a high predictive value.
Results
2.1 Gal-3 expression levels in the peripheral blood increased before surgery (127.18 ± 43.88 ng/mL), and LVMI and LVEDD were significantly higher than normal values (128.63 ± 38.01 and 57.76 ± 9.42, respectively).
2.2 Gal-3 expression levels were reduced three months after the operation compared with before, and the LVMI and LVEDD were lower than before the operation. The difference was significant for Gal-3, LVMI, and LVEDD (t1 = 11.984, t1 = 5.236, t1 = 6.565, and t1 = 4.683, respectively; P1 < 0.001), but there was no significant difference in LVEF (t1 = 0.143; P = 0.887; Table 2).
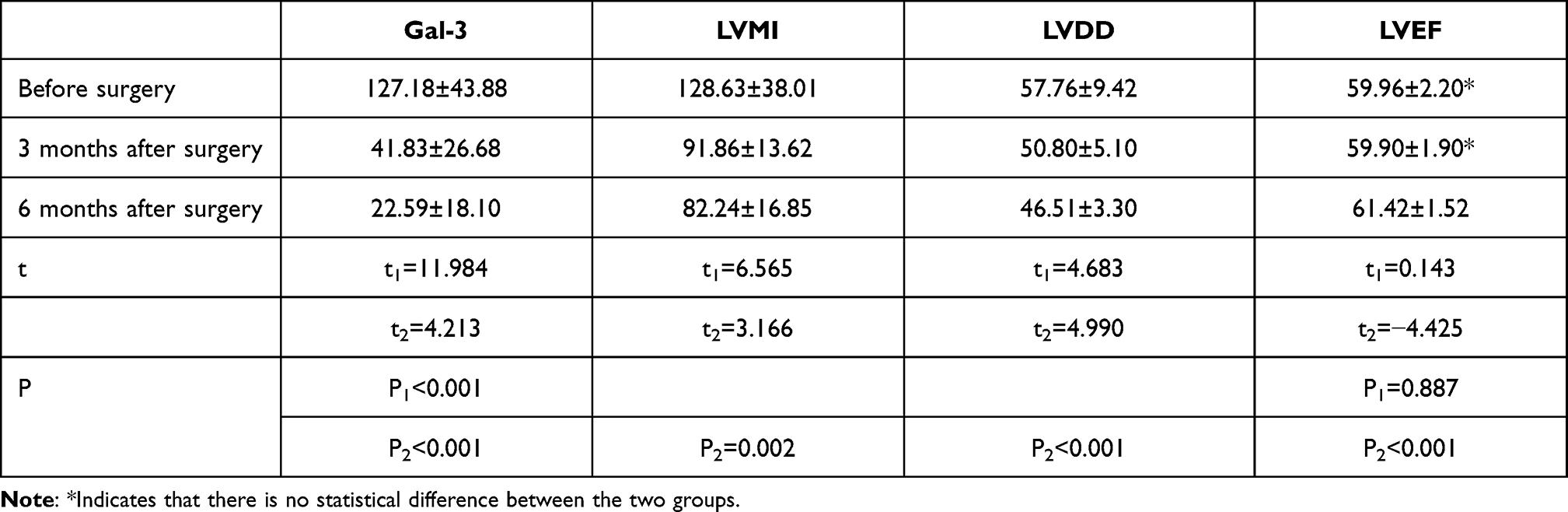 |
Table 2 Comparison Table of Changes in Various Observation Indicators |
2.3 Gal-3 expression levels decreased between three and six months after surgery, and the difference was statistically significant (t2 = 4.213, P2 < 0.001). At the same time, LVMI and LVEDD were also significantly reduced (t2 = 3.166 and P2 = 0.002, t2 = 4.990 and P2 < 0.001, respectively), while LVEF showed an increasing trend, and the difference was statistically significant (t2 = −4.425, P < 0.05; Table 2).
2.4 Gal-3 was positively correlated with the high-sensitivity C-reactive protein (hs-CRP), LVMI, and LVEDD before surgery and three and six months after surgery, but there was no correlation with LVEF. An ROC curve demonstrated that Gal-3 was able to predict the occurrence of ventricular remodeling, with AUC = 0.721; Yi = 126.33 ng/mL (Table 3; Figure 1).
 |
Table 3 Correlation Analysis Between Gal-3 and Other Observed Indicators |
 |
Figure 1 The ROC curve of Gal-3 expression level for predicting the occurrence of ventricular remodeling. |
Discussion
An ascending aortic aneurysm is a pathological change in the elastic media of the aorta caused by a variety of comprehensive and complex factors, leading to abnormal hemodynamics in the aorta. This pathological process leads to a decrease in aortic compliance and further affects the patient’s blood pressure. This vicious cycle gradually increases ventricular myocardial afterload, causing myocardial inflammation, myocardial fibrosis, ventricular muscle hypertrophy, and ventricular diameter increase, as well as other ventricular remodeling phenomena, which further damage cardiac function, eventually leading to end-stage heart failure. However, due to the early stage of ventricular remodeling, the patient has no apparent symptoms of discomfort. After the symptoms of heart failure appear, the condition is often severe, and the opportunity for surgery is lost. Therefore, taking effective measures to diagnose ventricular remodeling as soon as possible plays an essential role in blocking disease progression. Some studies believe that ventricular remodeling is the primary pathological mechanism of patients with heart failure, and the occurrence of ventricular remodeling indicates a poor prognosis.9 Currently, hs-CRP and N-terminal pro-brain natriuretic peptides (NT-proBNP) are reliable indicators for evaluating myocardial inflammation and cardiac function prognosis in clinical work. However, they are affected by factors such as the patient’s age, weight, and renal function.10 Furthermore, hs-CRP and NT-proBNP are not able to indicate ventricular remodeling in a patient, and they have certain limitations in clinical application. Therefore, it is necessary to explore a sensitive biological index closely related to myocardial inflammation and ventricular remodeling to evaluate these two processes.
Previous studies have found that as the continuous myocardial load increases, myocardial inflammation occurs, and a series of reactions caused by the released inflammatory mediators are closely related to the occurrence and development of ventricular remodeling.11 Macrophages infiltrate when myocardial inflammation occurs, and Gal-3 is secreted out of cells, combined with various extracellular matrices. At the same time, macrophage infiltration is induced, promoting cardiomyocyte fibrosis and leading to changes in ventricular morphology and size, ie, ventricular remodeling.12
Through an analysis of the results of this study, it was found that the Gal-3 expression levels of patients with an ascending aortic aneurysm combined with ventricular remodeling were high before surgery and that Gal-3, LVMI, and LVEDD had all decreased three months after surgery compared with before surgery, and these results were statistically significant (t1 = 11.984, t1 = 6.565, t1 = 4.683, respectively; P1 < 0.001). When comparing the measurements six months after surgery with those three months after surgery, the Gal-3 expression levels had decreased, and the difference was statistically significant (t2 = 4.213, P < 0.001), and LVMI and LVEDD had also decreased significantly (t2 = 3.166, P2 = 0.002; t2 = 4.990, P2 < 0.001). At the same time, LVEF showed an increasing trend (t2 = −4.425, P < 0.05).
The above research results indicate that after surgical treatment, the patient’s left ventricular remodeling gradually improved, similar to the research results of Deng et al,13 and previous related studies have shown that Gal-3 may be combined with myocardial extracellular matrix to release inflammation. Factor mediators induce macrophage infiltration, activate fibroblasts, and promote myocardial fibrosis, resulting in ventricular remodeling and further damage to cardiac function,14 indicating that there may be a relationship between Gal-3, LVMI, and LVEDD. Further analysis demonstrated that Gal-3 was positively correlated with LVMI and LVEDD but not with LVEF. This may be because the cardiac function of the patients included in this study is of the ejection-fraction preservation type, and there is a problem of poor correlation. Patients with a reduced or intermediate ejection fraction should be further studied. Studies by Tunc-Ata et al have shown that LVEF is an important indicator of left ventricular ejection function, and LVMI and LVEDD can reflect myocardial fibrosis and ventricular remodeling.15 Since Gal-3 is closely related to myocardial inflammation and ventricular remodeling, it should also have a certain reference value for predicting ventricular remodeling. The ROC curve indicates that Gal-3 predicts the occurrence of ventricular remodeling (AUC = 0.721; Yi = 126.33 ng/mL), and these results are similar to those of Li et al.16 The present study shows that Gal-3 expression levels can reflect myocardial inflammation, ventricular remodeling, and prognosis in patients with an ascending aortic aneurysm and can therefore be used as a reference for predicting ventricular remodeling and evaluating the prognosis of cardiac function in clinical work.
However, there were some limitations to this study. This was a single-center, prospective study, the sample size was small, and 12 patients were lost to follow-up. The results of the study only provide a reference value, and there is still a lack of studies on other cardiovascular disease patients, so further relevant studies are needed.
Conclusion
Gal-3 expression levels are correlated with ascending aortic aneurysms combined with ventricular remodeling, which provides a reference value for predicting ventricular remodeling.
Disclosure
The authors report no conflicts of interest in this work.
References
1. China Cardiovascular Health and Disease Report Writing Group. Summary of China Cardiovascular Health and Disease Report 2019. Chin J Circ. 2020;35(9):833–854. doi:10.3969/j.issn.1000-3614.2020.09.001
2. Okamoto RJ, Xu H, Kouchoukos NT, Moon MR, Sundt TM
3. Yang W, Zhang FF, Tang HP, et al. Summed thickening score by myocardial perfusion imaging: a risk factor of left ventricular remodeling in patients with? Myocardial infarction. J Nucl Cardiol. 2018;25(3):742–753. doi:10.1007/s12350-018-1200-4
4. Li XC, Jin FL, Jing C, et al. Predictive value of left ventricular remodeling by area strain based on three-dimensional wall-motion tracking after PCI in patients with recent NSTEMI. Ultrasound Med Biol. 2012;38(9):1491–1501. doi:10.1016/j.ultrasmedbio.2012.05.006
5. Lin YH, Lin LY, Wu YW. The relationship between serum galectin-3 and serum markers of cardiac extracellular matrix turnover in heart failure patients. Clin Chim Acta. 2009;409(1/2):96–99. doi:10.1016/j.cca.2009.09.001
6. de Boer RA, Lok DJ, Jaarsma T, et al. Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction. Ann Med. 2011;43(1/2):60–68. doi:10.3109/07853890.2010.538080
7. Sharma UC, Pokharel S, van Brakel TJ, et al. Galectin-3 marks activated macrophages in failure-prone hypertrophied hearts and contributes to cardiac dysfunction. Circulation. 2004;110(19):3121–3128. doi:10.1161/01.CIR.0000147181.65298.4D
8. Liu YH, D’ambrosio M, Liao TD, et al. N-acetyl-seryl-aspartyl-lysyl-proline prevents cardiac remodeling and dysfunction induced by galectin-3, a mammalian adhesion/growth-regulatory lectin. Am J Physiol. 2009;296(2 Pt. 1):H404–H412. doi:10.1152/ajpheart.00747.2008
9. Simovic Markovic B, Nikolic A, Gazdic M, et al. Galectin-3 plays an important pro -inflammatory role in the induction phase of acute colitis by promoting activation of NLRP3 inflammasome and production of IL-1β in macrophages. J Crohns Colitis. 2016;10(5):593–606. doi:10.1093/ecco-jcc/jjw013
10. Deng WH, Li SR, Zhang YH, et al. The effect of galactosidin 3 on myocardial fibrosis and ventricular remodeling. Chin J Arterioscler. 2017;25(10):1008–1014. doi:10.3969/j.issn.1007-3949.2017.10.008
11. Xia XH, Ruan DY, Cheng YT. The value of serum Syndecan-4PTX-3 and BNP in the diagnosis of chronic heart failure. Anhui Med. 2017;38(10):1343–1345. doi:10.3969/j.issn.1000-0399.2017.10.036
12. Wang Y, Zhou YZ, Hang Y, et al. The signal transduction mechanism of myocardial fibrosis and the treatment of traditional Chinese medicine. J Integr Trad Chin West Med Cardiovasc Cerebrovasc Dis. 2018;16(4):421–424. doi:10.3969/j.issn.1672-1349.2018.04.010
13. Deng H, Wang X, Wen JF, et al. The relationship between serum galectin-3 and pentamer protein-3 levels and ventricular remodeling and prognosis in patients with chronic heart failure. Chin Gerontol Mag. 2020;40(19):4057–4059. doi:10.3969/j.issn.1005-9202.2020.19.008
14. Suthahar N, Meijers WC, Silljé HHW, de Boer RA. From inflammation to fibrosis-molecular and cellular mechanisms of myocardial tissue remodelling and perspectives on differential treatment opportunities. Curr Heart Fail Rep. 2017;14(4):235–250. PMID: 28707261; PMCID: PMC5527069. doi:10.1007/s11897-017-0343-y
15. Tunc-Ata M, Turgut G, Mergen-Dalyanoglu M, Turgut S. Examination of levels pentraxin-3, interleukin-6, and C-reactive protein in rat model acute and chronic exercise. J Exerc Rehabil. 2017;13(3):279–283. PMID: 28702438; PMCID: PMC5498083. doi:10.12965/jer.1734920.490
16. Li F, Wu HY, Ding XR, et al. The correlation between preoperative serum galectin-3 and amino-terminal B-type brain natriuretic peptide levels and abnormal prosthetic valve function immediately after heart valve replacement. J Cardiovasc Pulm Dis. 2021;40(3):249–253. doi:10.3969/j.issn.1007-5062.2021.03.007
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.