Back to Journals » Vascular Health and Risk Management » Volume 19
Correlation P2Y12 Genetic Polymorphism As Risk Factor of Clopidogrel Resistance in Indonesian Stroke Patients
Authors Hidayat R ![]() , Rasyid A, Harris S, Harahap A, Herqutanto, Louisa M
, Rasyid A, Harris S, Harahap A, Herqutanto, Louisa M ![]() , Listiyaningsih E, Rambe AS, Loho T
, Listiyaningsih E, Rambe AS, Loho T
Received 19 August 2022
Accepted for publication 15 December 2022
Published 29 January 2023 Volume 2023:19 Pages 53—61
DOI https://doi.org/10.2147/VHRM.S386107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Daniel Duprez
Rakhmad Hidayat,1– 3 Al Rasyid,2,3 Salim Harris,2,3 Alida Harahap,2 Herqutanto,2 Melva Louisa,2 Erlin Listiyaningsih,4 Aldy Safruddin Rambe,5 Tonny Loho6
1Doctoral Program in Medical Sciences Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 2Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 3Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia; 4Harapan Kita Hospital, Jakarta, Indonesia; 5Sumatera Utara University, Medan, Indonesia; 6Faculty of Medicine and Health Science, Kristen Krida Wacana University, Jakarta, Indonesia
Correspondence: Rakhmad Hidayat, Tel +62 813 88756299, Email [email protected]
Background: Stroke is one of the highest causes of disability and mortality in several countries worldwide. Secondary prevention is important in the management of stroke. Clopidogrel is widely used in Asia as secondary prevention for ischemic stroke, even though several studies in Western show limited data related to clopidogrel resistance in Asia. This study aims to determine the correlation between P2Y12 genetic polymorphism and clopidogrel resistance in Indonesia.
Methods: This study was conducted on one-year duration, the subjects were chosen through the consecutive sampling method, all subjects were examined for genetics and resistance to clopidogrel. The data were analyzed through statistical analysis, a bivariate analysis was conducted to determine the correlation between several variables and the resistance variable. This study employed resistance diagnostic methods with VerifyNow. Polymorphism of receptor P2Y12 was tested with the Polymerase Chain Reaction method (PCR) and analysis of restriction fragment length polymorphism (RFLP). The genes tested in this study were G52T and C34T.
Results: The number of participants in this study was 112. Examination of gene P2Y12 showed that the majority was homozygote, wild-type C34T allele (67%), and G52T (66.1%). There was no significant correlation between clopidogrel resistance and gene G52T and C34T of P2Y12 (p > 0.05). Hb levels significantly correlated with P2Y12 G52T (p = 0.024). Meanwhile, Fatty Liver significantly correlated with P2Y12 C34T (p = 0.037).
Conclusion: Indonesia showed a low clopidogrel resistance rate and a very low C34T and G52T allele P2Y12 gene mutation, meaning that Indonesia had low mutations in the P2Y12. This is the cause of clopidogrel resistance in this study only 15%. Therefore, in a region with less clopidogrel resistance, examination of the P2Y12 gene would not give significant results.
Keywords: clopidogrel resistance, P2Y12, stroke, antiplatelet
Introduction
The world’s highest cause of disability and mortality and neurological emergency is stroke.1 Asians have a higher rate of stroke than Caucasians. Asians have a high stroke mortality rate. In China, stroke is the main cause of death. Meanwhile, in Malaysia, it is the third highest cause of death.2
Secondary prevention is important in the management of stroke.2 The study of the Reduction of Atherothrombosis for Continued Health (REACH) stated that adequate secondary prevention involves antihypertension, dyslipidemia, and antiplatelet therapy, successfully reducing the rate of secondary stroke in the past 20 years. The rate decreased by 36% from 1995–1998 to 2004–2008.3,4 A Cochrane study in 2003 showed that early administration of antiplatelet within the first 48 hours after a stroke could reduce the risk of recurrent stroke.5
Acetylsalicylic Acid (ASA) is the benchmark of antiplatelet for stroke. On the other hand, there is clopidogrel as an alternative in cases of ASA intolerance or contraindication.6 Clopidogrel has been proven to be more superior in binding platelet receptors (71.5%) compared to ASA (52.6%), P < 0.01.7 Furthermore, NICE (National Institute for Health and Clinical Excellence) in 2010 reported that clopidogrel is the most cost-efficient therapy for patients with ischemic stroke.2
Clopidogrel binds platelet receptor P2Y12, which works in the platelet aggregation pathway through the ADP receptor.8 P2Y12 is the biggest factor in platelet activation and aggregation compared to other ADP receptors (P2X1 and P2Y1).9 Considerable variability in pharmacodynamic response contributes to failure of antiplatelet therapy; this phenomenon is particularly well known for older drugs, such as clopidogrel.30 There is a high on-treatment platelet reactivity (HTPR) phenomenon, which is a high residual post-treatment platelet activity that reflects the pharmacodynamic activity of clopidogrel on platelets. This phenomenon has a persistent response on the ADP-P2Y12 receptor during therapy in 16–50% of patients, which causes the failure to prevent recurrent stroke.2,10 The rate of HTPR or resistance is high in clopidogrel use. This is proved by several specific laboratory examinations that observed platelet reactivity or clopidogrel binding on its receptors.11
Clopidogrel is widely used in Asia as secondary prevention for ischemic stroke, even though several studies in Western show limited data related to clopidogrel resistance in Asia. Hasan et al reported a high resistance of clopidogrel in Chinese-American patients who received coronary stents (68–73%) and in Indian patients with recurrent ACS (72.5%). Kitzmiller et al2 reported that almost 50% of Asians lose one genetic function allele that can reduce the response to clopidogrel. Therefore, this study aims to determine the correlation between P2Y12 genetic polymorphism and clopidogrel resistance in Indonesia.
Methods
This study was conducted in the Neurology Polyclinic of RSCM and RSUI from July 2020 to 2021. The subjects were chosen through the consecutive sampling method by taking each sample that meets the research criteria until it reaches the desired number of samples within 1 year. The method of calculating the sample size for this study is based on the relationship between one of the risk factors for the occurrence of clopidogrel resistance in ischemic stroke cases with the following formula:


Notes:
Type I error is 5%, one-way hypothesis, then Zα = 1. 96
Type II error, by 10%, then Zβ = 1.64
P1 = proportion experiencing resistance = 0.30
Q1 = 1− P1 = 0.70
P2 = proportion that does not experience resistance = 0.70
P1−P2 = the difference in the proportion of minimal exposure that is considered significant = 0.40
Q2 = 1 – P2 = 0.30
P = total proportion = (P1 + P0)/2 = 0.5
Q = 1 – P = 0.5
Calculation of the sample size obtained is 35.75, rounded up to 36 samples for each group. Taking into account the possibility of a drop out of 10%, the number of samples is 40 per group.
The data were analyzed by statistical calculations using IBM SPSS Statistics (Version 26) and the results were presented descriptively. Afterward, a bivariate analysis was conducted to determine the correlation between several variables and the resistance variable. The researchers calculated the direct effect using chi-square, and considered a significant result if the p-value <0.05.
Two frequently employed resistance diagnostic methods with platelet function tests were VerifyNow and LTA. The test observed platelet aggregation through increasing light transmission. VerifyNow employed a whole blood specimen, while LTA employed platelet-rich plasma as a specimen.12 Although LTA was still considered the benchmark for platelet function tests,11 VerifyNow was easier, faster, and equipped with prostaglandin E1 that blocked the ADP P2Y1 receptor to prevent platelet aggregation P2Y1 receptor. Thus, it increased the specificity and sensitivity of the platelet aggregation test induced by the ADP P2Y12 receptor.13–15 This study employed the VerifyNow method with a cut-off value from PRU of 208, in which >208 meant inadequate response, while <208 meant adequate response. Polymorphism of receptor P2Y12 was tested with the Polymerase Chain Reaction method (PCR) and analysis of restriction fragment length polymorphism (RFLP), which was widely employed for genotyping. The first step of PCR-RLFP was amplifying fragments containing mutase, followed by administering an appropriate restriction enzyme to the fragments. The PCR-RFLP method was fast and easy to use. However, this method can only identify polymorphism in the restriction area of the endonuclease, and difficult to identify the correct variant where several single nucleotide polymorphisms were present that affect the restriction area of the enzyme.16,17 The genes tested in this study were G52T and C34T.
Ethical Approval and Consent to Participate
This study complied with the Declaration of Helsinki. The Ethics of the Faculty of Medicine, University of Indonesia – Cipto Mangunkusumo Hospital approved this study, approval number KET-658/UN2/F1/ETIK/PPM.00.02/2020. This study received consent from the subjects by signing informed consent.
Results
The study involved 128 eligible participants. The first step was screening, which included interviews and physical and adjunctive examinations. There were 16 excluded participants (9 with incomplete interview data and 7 with incomplete adjunctive examination results). No participants were excluded from the second step (N = 112).
Epidemiological data from this study showed that the majority of subjects were men (52.9%), older than 57 years old (49.1%), and had BMI < 28 (76.8%). There were 67.0% of subjects with no history of DM, 68.8% with no history of dyspepsia, 45.5% with responsive VerifyNow results, and 40.2% with a risk of hemorrhage (Table 1). Examination of gene P2Y12 showed that the majority was homozygote, wild-type C34T allele (67%), and G52T (66.1%) (Table 2).
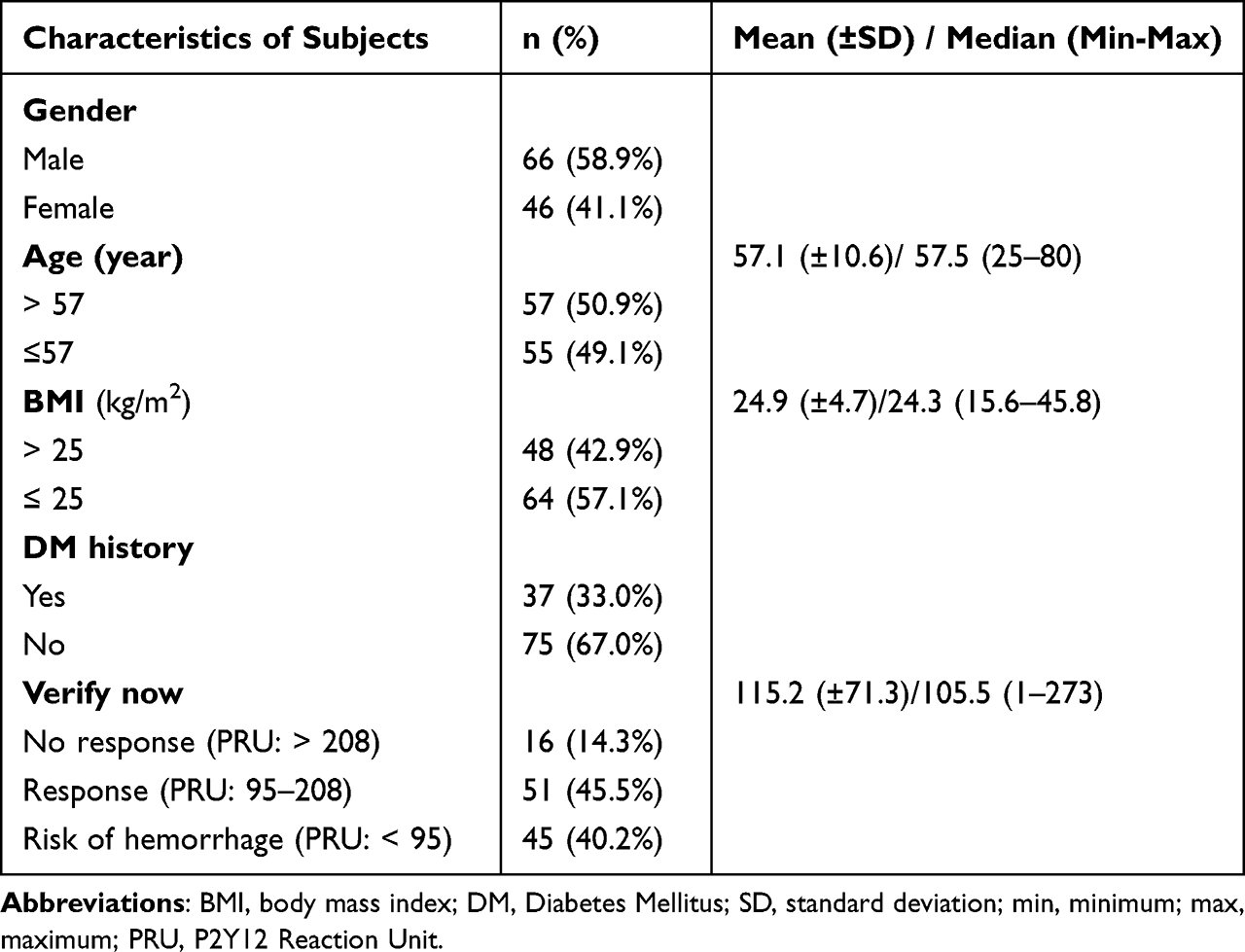 |
Table 1 Demographic Characteristics and Clinical Data of Subjects |
 |
Table 2 Examination of Gene P2Y12 |
The following table shows the characteristics of laboratory results on research subjects (Table 3). This study found that subjects with HbA1c <6.5% were 67%, FBG <126 were 66.1%, HDL <60 were 71.4%, LDL ≥100 were 76.8%, AST <34 were 92, 9%, ALT <55 were 95.5%, and on other laboratory examinations there is not too much difference. As for the results of ultrasound radiological investigations, 53.6% of subjects with fatty liver were found.
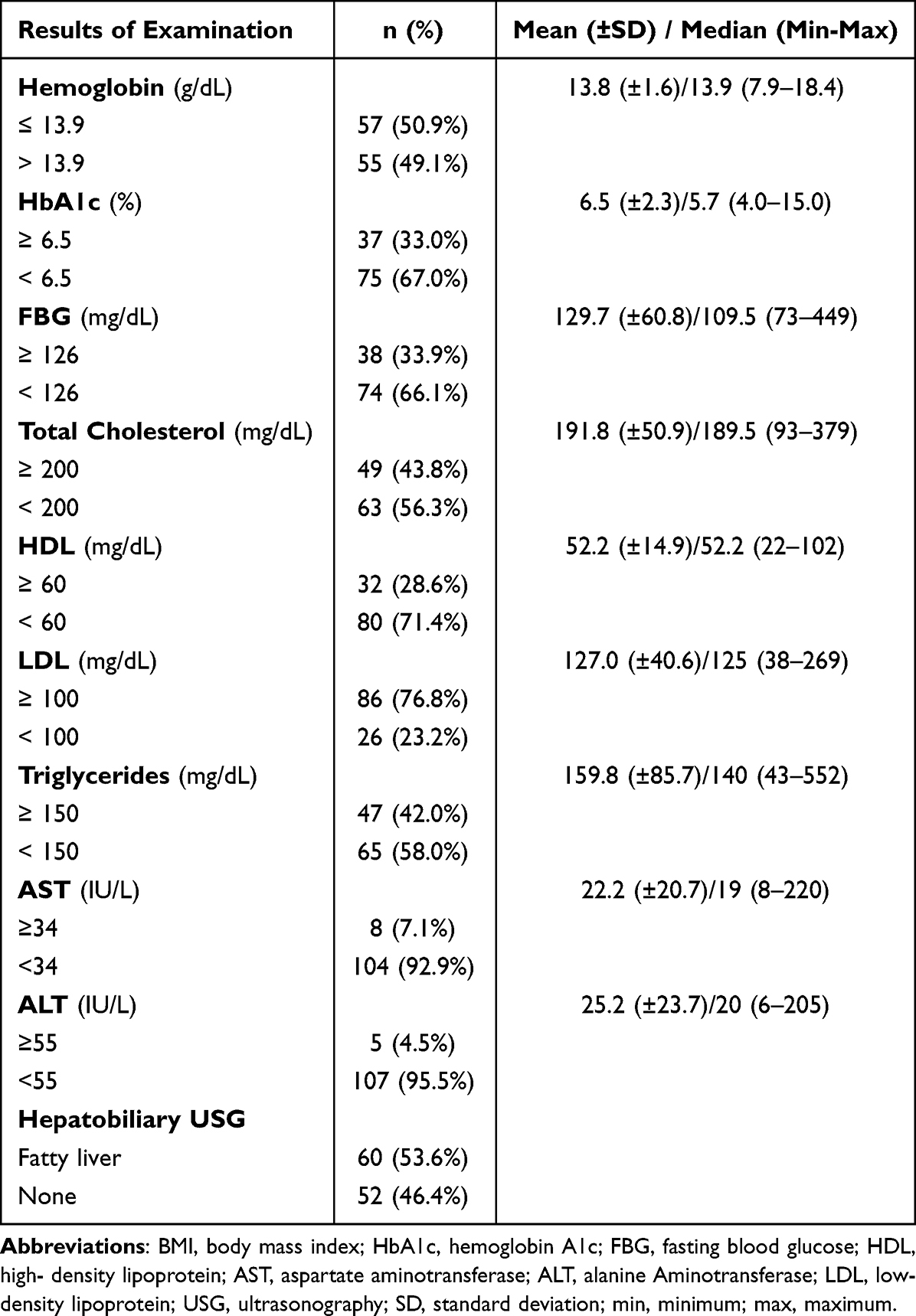 |
Table 3 Characteristics of Adjunctive Examination Results |
The results of the adjunctive examinations were cross-tabulated to the P2Y12 variable (Table 4). The table showed that Hb levels significantly correlated with P2Y12 G52T (p = 0.024). Meanwhile, Fatty Liver significantly correlated with P2Y12 C34T (p = 0.037). The study also conducted a cross-tabulation to determine the correlation between the P2Y12 variable and clopidogrel resistance (Table 5). There was no significant correlation between clopidogrel resistance and gene G52T and C34T of P2Y12 (p > 0.05).
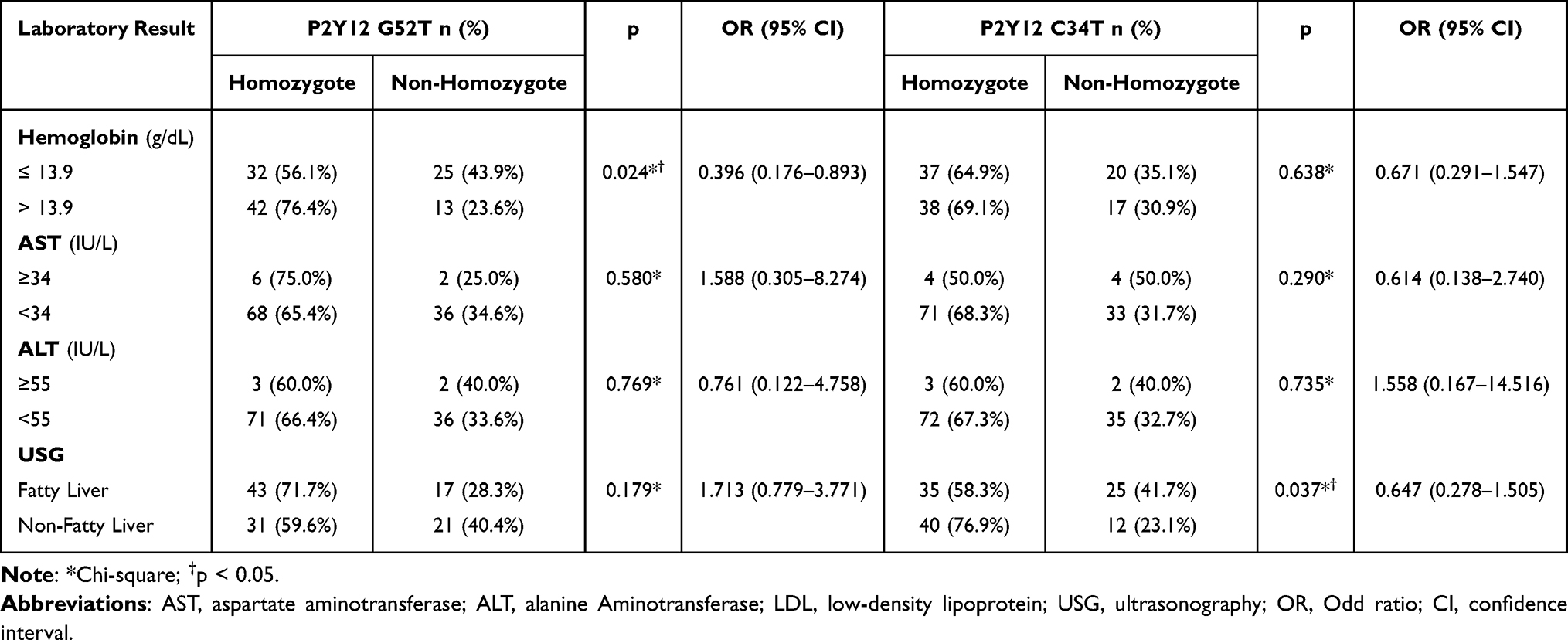 |
Table 4 Correlation Between Adjunctive Examination and P2Y12 |
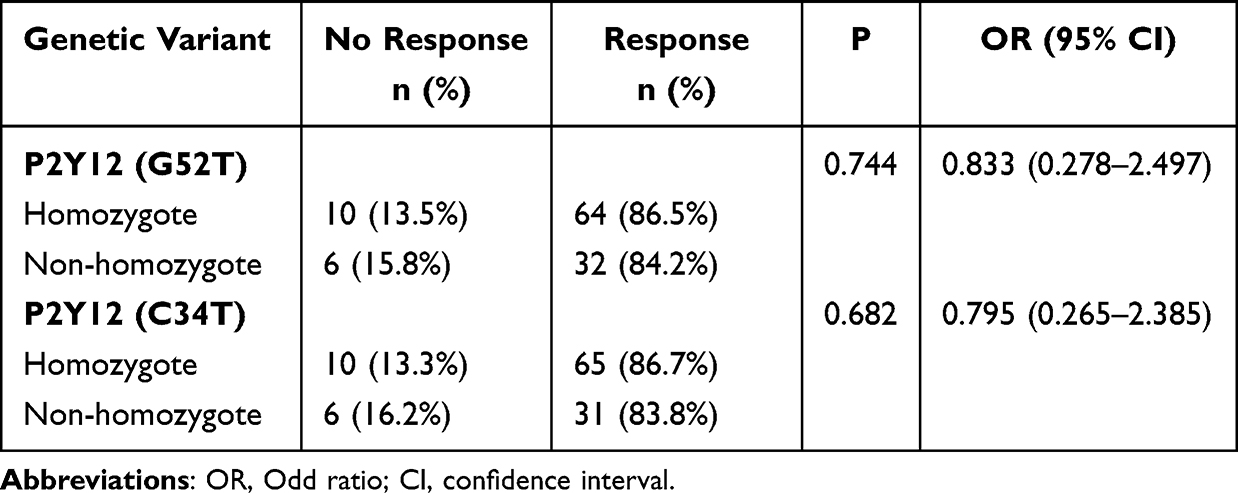 |
Table 5 Correlation Between P2Y12 and Clopidogrel Resistance |
Discussion
The subjects in this study were dominated by men (58.9%). The age median and average scores obtained were 57.5 and 57.14 years, respectively. There were 50.9% of subjects aged older than 57 years old. The results of this study were in line with Virani et al18 They reported that the prevalence of stroke based on age was specifically lower in women compared to men in the young and middle age group but got narrower with age.18 Lower stroke prevalence in women may be caused by genetic factors and the positive effect of estrogen on cerebral circulation, except between the age of 35–44 years and >85 years. Contrary to the oldest population, stroke was higher in women compared to men in the 85–94 age group.19,20 This study found that 57.1% of subjects had BMI ≤ 25 (58.7% women and 56.1% men). The average global BMI is 24, while Indonesian epidemiology data stated that there was 55.9% of people with BMI > 25, similar to the data obtained in the study. BMI in this study did not have a significant correlation with clopidogrel resistance. In contrast to the study of Legrand et al31 and Price et al32 (p < 0.05) which reported differences in the mean BMI, the BMI of the response group was lower (Table 6).
 |
Table 6 Comparison of the Mean BMI in the Response and Non-Response Groups |
Adjunctive examination results showed that one-third of the subjects had DM with an FBG of >126 (33.9%). Thus, it showed that the prevalence in the subjects was in line with a previous study by Lau et al,21 reporting 1 out of 3 stroke patients had DM (24.7–56.2%). The 2018 RISKESDAS data stated that there were 8.5% of people with DM in Indonesia, with the highest proportion in the 45–54 age group (29.3%), which was similar to the population data of the samples in this study.4
This study indicated that only 14.3% of patients in Indonesia did not respond to clopidogrel. Meanwhile, a previous study showed that clopidogrel resistance was high in stroke patients, varying from 28% to 44%.22 In the pilot study by Hidayat et al,23 the researchers found a consistently low resistance to clopidogrel. This showed that only 15% of clopidogrel metabolism still showed very good effectivity in Indonesia. However, there was no study on ABCB1 polymorphism which explains the correlation.
There were 43.8% of patients with dyslipidemia in this study, in which 76.8% had LDL levels of >100 mg/dL, which showed that there was still a high prevalence of patients with cholesterol targets not by the treatment target. There were only 4.5–7.1% of liver function disorders from laboratory examination, while according to the USG examination, there was ten times more fatty liver (53.6%) found from the liver function disorder. This showed a manifestation of dyslipidemia. Cross-tabulation results did not indicate a correlation between Hb, fatty liver, AST, and ALT with gene P2Y12, even though the researchers found a tendency of haplotype H2 in the G52T allele in people with Hb <13.9 (p = 0.054).
Clopidogrel was still often used as a management for stroke prevention in Asia, including Indonesia. 85% of clopidogrel absorbed in the intestines will be hydrolyzed by esterase and converted into an inactive carboxylic acid derivative. The rest (15%) was metabolized by hepatic cytochrome P450 (CYP450) and converted to intermediary metabolite 2-oxo-clopidogrel (Figure 1).33,34
 |
Figure 1 Clopidogrel Metabolism. Notes: Clopidogrel is a prodrug, 85% of clopidogrel is hydrolyzed by esterases and converted to inactive derivatives, another 15% is metabolized by hepatic cytochrome P450 (CYP450) and converted to intermediate metabolites. Adapted from Zhang Y, Li M, Tang J and Chen X. Pharmacokinetic and Pharmacodynamic Responses to Clopidogrel: Evidences and Perspectives. Int. J. Environ. Res. Public Health33 307–316, Copyright 2011, with permission from Elsevier.34 |
Clopidogrel resistance was caused by variability or insufficient formation of clopidogrel active metabolite. The cause of different levels of clopidogrel active metabolites included 1) intestinal absorption that can be affected by polymorphism of the ABCB1 gene and clopidogrel enzymatic activation (pharmacokinetic); 2) variability in isoenzyme P450 activity caused by interaction by other drugs and polymorphism in several isoenzyme genes related to the formation of suboptimal clopidogrel active metabolites and reduced responsivity of clopidogrel in platelet function examination; 3) polymorphism of ADP-P2Y12 receptor that affected the variability of clopidogrel bond on platelet (pharmacodynamic).
The P2Y12 receptor had an important role in the potentiation of platelet activation. P2Y12 receptor will inhibit adenylyl cyclase and cAMP increase mediated by prostaglandin E2 (PGE2) and forskolin.9 Stimulation of receptors P2Y1 and P2Y12 was needed for platelet aggregation induced by ADP.24 On the other hand, epinephrine, which suppressed cAMP levels through the alpha-adrenergic receptor, produced P2Y12 signaling.25
Gene P2Y12 consisted of a minimum of two exons separated by one intron with a length of ≈ 1700 bp located upstream of the ATG codon. Exon 2 coded all 342 amino acid proteins. There were several polymorphisms in an intron, such as two variations on 139 nt and 744 nt on the 5’ intron start site, which consisted of transition of C to T (i-C139T) and T to C (i-T744C), and insertion of a single nucleotide (A) in position 801 in an intron (i–ins801A). Other polymorphism was also found in exon 2, which consisted of transition of C to T (C34T) in 34 nt 5’ start site in exon 2 and transversion of G to T (G52T) in 52 nt 5’ start site in exon 2.26
P2Y12 polymorphism was grouped into 2 haplotypes (H1 and H2). H1 was a major haplotype (C in position 139, T in position 744, and no i–ins801A in intron, and G in position 52 exon 2), and H2 a minor haplotype (T in position 139, C in position 744, i–ins801A in intron, and T in position 52 of exon 2). The H2 type was correlated with the maximum response of ADP aggregation and identified as a gain-of-function haplotype that may cause an increased atherothrombosis and intervention response to clopidogrel.26 Patients with H2 homozygote had high clopidogrel HTPR.27
Polymorphism of the P2Y12 receptor gene acted in the incidence of clopidogrel HTPR. A meta-analysis study by Cui et al28 reported that homozygote and heterozygote genotype of G52T had a significantly higher clopidogrel HTPR (resistance) compared to wild-type homozygote (OR 1.45 CI 95% 1.14–1.85 p = 0.003), polymorphism of gene C34T significantly related to clopidogrel HTPR (p = 0.002), while polymorphism of gene T744C did not correlate with clopidogrel HTPR (OR 0.88 CI 95% 0.58–1.33 p = 0.54).28
Primary haplotype (H1) was a group that did not carry all four polymorphisms. Secondary haplotype (H2) was a group with all four polymorphisms. In H2 haplotype, if there were a gain-of-function (GOF), then atherothrombosis would increase, leading to a high HTPR level. Both polymorphisms (C34T and G52T) were high-risk factors of HTPR.26–28
This study found that the H2 haplotype in gene C34T had a mutation of 5.4% and G52T of 3.6%. The results were in line with the clopidogrel resistance test, which showed a very low resistance. Mutation of H2 haplotype of gene C34T and G52T were rare, especially in Indonesia, and could not affect clopidogrel resistance in the population. The results of this study were in line with Nie et al, who showed no significant correlation between P2Y12 and clopidogrel resistance (p = 0.062).29 Cui et al28 also provided that the P2Y12 G52T and C34T polymorphisms are associated with poor clopidogrel response in patients, reflected by platelet function tests.
The wild-type type was found in more than 67% of the G52T gene and 66.1% in C34T. Another study stated that high wild type in gene C34T and G52T was correlated with low resistance risk of clopidogrel (p = 0.003).2 Cui et al28 reported that patients with the homozygous and heterozygous (TT + GT) G52T genotype had a higher risk of clopidogrel resistance when compared to the wildtype. Whereas in the C34T polymorphism, apart from statistical heterogeneity, all included studies reported a positive association between the risk of clopidogrel resistance and the C34T polymorphism (OR: 2.30, 95% CI: 1.50–3.51, p = 0.0001). Variability in the clopidogrel resistance and different regions of population study may effect the heterogeneity in the comparisons. The use of antiplatelet, such as differences in dose and duration of treatment, can also cause heterogeneity.28 Meanwhile, Danielak et al30 reported most of the P2Y12 genetic polymorphisms (eg, G52T) may contribute to changes in P2Y12 receptor structure, thus reducing the efficacy of antiplatelet therapy. However, the impact of several factors (eg, T744C, C34T, smoking) on antiplatelet therapy has not been fully determined, and their coexistence may lead to resistance to antiplatelet therapy.
The cross-tabulation result between investigations and P2Y12 in this study showed that Hb levels had a significant relationship with P2Y12 G52T (p = 0.024). In contrast, Fatty Liver had a significant relationship with P2Y12 C34T (p = 0.037).26
Study Limitation
The samples in this study showed a tendency not to resist clopidogrel. Therefore, a larger sample was needed because there was a lack of clopidogrel resistance followed by a lack of P2Y12 gene mutation in Indonesia.
Conclusion
Indonesia showed a low clopidogrel resistance rate and a very low C34T and G52T allele P2Y12 gene mutation, meaning that Indonesia had low mutations in the P2Y12. This is the cause of clopidogrel resistance in this study only 15%. Therefore, in a region with less clopidogrel resistance, examination of the P2Y12 gene would not give significant results.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to patients’ privacy concerns.
Funding
The authors thank Universitas Indonesia for funding this research through the PUTI Grant. Contract number NKB-1566/UN2.RST/HKP.05.00/2020
Disclosure
The authors declare no conflicts of interest.
References
1. MONICA Project Principal Invest W. The World Health Organization MONICA Project (monitoring trends and determinants in cardiovascular disease): a major international collaboration. WHO MONICA Project Principal Investigators. J Clin Epidemiol. 1988;41(2):105–114. doi:10.1016/0895-4356(88)90084-4
2. Hasan MS, Basri HB, Hin LP, Stanslas J. Genetic polymorphisms and drug interactions leading to clopidogrel resistance: why the Asian population requires special attention. Int J Neurosci. 2013;123(3):143–154. doi:10.3109/00207454.2012.744308
3. Uchiyama S, Goto S, Matsumoto M, et al. Cardiovascular event rates in patients with cerebrovascular disease and atherothrombosis at other vascular locations: results from 1-year outcomes in the Japanese REACH Registry. J Neurol Sci. 2009;287(1–2):45–51.
4. Pennlert J, Eriksson M, Carlberg B, Wiklund PG. Long-term risk and predictors of recurrent stroke beyond the acute phase. Stroke. 2014;45(6):1839–1841.
5. Sandercock P, Gubitz G, Foley P, Counsell C. Antiplatelet therapy for acute ischaemic stroke. Cochrane Database Syst Rev. 2003;2003(2):CD000029.
6. Pepine CJ. Aspirin and newer orally active antiplatelet agents in the treatment of the post-myocardial infarction patient. J Am Coll Cardiol. 1998;32(4):1126–1128.
7. Collyer TC, Gray DJ, Sandhu R, Berridge J, Lyons G. Assessment of platelet inhibition secondary to clopidogrel and aspirin therapy in preoperative acute surgical patients measured by Thrombelastography® platelet mappingTM. BJA Br J Anaesth. 2009;102(4):492–498.
8. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE steering committee. Lancet Lond Eng. 1996;348(9038):1329–1339.
9. Murugappa S, Kunapuli SP. The role of ADP receptors in platelet function. Front Biosci J Virtual Libr. 2006;11:1977–1986.
10. Bonello L, Tantry US, Marcucci R, et al. Consensus and future directions on the definition of high on-treatment platelet reactivity to adenosine diphosphate. J Am Coll Cardiol. 2010;56(12):919–933. doi:10.1016/j.jacc.2010.04.047
11. Paniccia R, Priora R, Liotta AA, Abbate R. Platelet function tests: a comparative review. Vasc Health Risk Manag. 2015;11:133–148. doi:10.2147/VHRM.S44469
12. Amin AM, Sheau Chin L, Azri Mohamed Noor D, Abdul Kader MA, Kah Hay Y, Ibrahim B. The personalization of clopidogrel antiplatelet therapy: the role of integrative pharmacogenetics and pharmacometabolomics. Cardiol Res Pract. 2017;2017:1. doi:10.1155/2017/8062796
13. Gaglia MA, Torguson R, Pakala R, et al. Correlation between light transmission aggregometry, verifynow P2Y12, and VASP-P platelet reactivity assays following percutaneous coronary intervention. J Intervent Cardiol. 2011;24(6):529–534. doi:10.1111/j.1540-8183.2011.00670.x
14. Gachet C, Aleil B. Testing antiplatelet therapy. Eur Heart J Suppl. 2008;10(suppl_A):A28–34. doi:10.1093/eurheartj/sum081
15. Jakubowski J, Li Y, Small D, et al. A comparison of the verifyNow P2Y12 point-of-care device and light transmission aggregometry to monitor platelet function with prasugrel and clopidogrel: an integrated analysis. J Cardiovasc Pharmacol. 2010;56(1):29–37. doi:10.1097/FJC.0b013e3181dd0ec2
16. Berg H. Restriction fragment length polymorphism analysis of PCR-Amplified Fragments (PCR-RFLP) and Gel electrophoresis - valuable tool for genotyping and genetic fingerprinting. gel electrophoresis - principles and basics. InTech; 2012. Available from: http://www.intechopen.com/books/gel-electrophoresis-principles-and-basics/restriction-fragment-length-polymorphism-analysis-of-pcr-amplified-fragments-pcr-rflp-and-related-te.
17. Kristensen VN, Kelefiotis D, Kristensen T, Børresen-Dale AL. High-throughput methods for detection of genetic variation. BioTechniques. 2001;30(2):318–332. doi:10.2144/01302tt01
18. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254–743. doi:10.1161/CIR.0000000000000950
19. Appelros P, Stegmayr B, Terént A. Sex differences in stroke epidemiology: a systematic review. Stroke. 2009;40(4):1082–1090. doi:10.1161/STROKEAHA.108.540781
20. Goldstein LB, Bushnell CD, Adams RJ, et al. Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(2):517–584. doi:10.1161/STR.0b013e3181fcb238
21. Lau LH, Lew J, Borschmann K, Thijs V, Ekinci EI. Prevalence of diabetes and its effects on stroke outcomes: a meta-analysis and literature review. J Diabetes Investig. 2019;10(3):780–792. doi:10.1111/jdi.12932
22. Fukuoka T, Furuya D, Takeda H, et al. Evaluation of clopidogrel resistance in ischemic stroke patients. Intern Med Tokyo Jpn. 2011;50(1):31–35. doi:10.2169/internalmedicine.50.3713
23. Hidayat R, Nabilah RA, Rasyid A, et al. Clopidogrel resistance among ischemic stroke patients and its risk factors in Indonesia. Acta Medica Acad. 2022;51(1):29–34. doi:10.5644/ama2006-124.367
24. Kunapuli SP, Dorsam RT, Kim S, Quinton TM. Platelet purinergic receptors. Curr Opin Pharmacol. 2003;3(2):175–180. doi:10.1016/S1471-4892(03)00007-9
25. Conley PB, Delaney SM. Scientific and therapeutic insights into the role of the platelet P2Y12 receptor in thrombosis. Curr Opin Hematol. 2003;10(5):333–338. doi:10.1097/00062752-200309000-00002
26. Pierre F, Annabelle D, Sophie G, et al. Adenosine diphosphate–induced platelet aggregation is associated with P2Y12 gene sequence variations in healthy subjects. Circulation. 2003;108(8):989–995.
27. Staritz P, Kurz K, Stoll M, Giannitsis E, Katus HA, Ivandic BT. Platelet reactivity and clopidogrel resistance are associated with the H2 haplotype of the P2Y12-ADP receptor gene. Int J Cardiol. 2009;133(3):341–345.
28. Cui G, Zhang S, Zou J, Chen Y, Chen H. P2Y12 receptor gene polymorphism and the risk of resistance to clopidogrel: a meta-analysis and review of the literature. Adv Clin Exp Med off Organ Wroclaw Med Univ. 2017;26(2):343–349.
29. Nie XY, Li JL, Zhang Y, et al. Haplotype of platelet receptor P2RY12 gene is associated with residual clopidogrel on-treatment platelet reactivity. J Zhejiang Univ Sci B. 2017;18(1):37–47.
30. Danielak D, Pawlak K, Główka F, Karaźniewicz-łada M. Influence of genetic and epigenetic factors of P2Y12 receptor on the safety and efficacy of antiplatelet drugs. Cardiovasc Drugs Ther. 2022;2022:1. doi:10.1007/s10557-022-07370-8
31. Legrand D, Barbato E, Chenu P, et al. The STIB score: a simple clinical test to predict clopidogrel resistance. Acta Cardiol. 2015;70(5):516–521.
32. Price MJ, Berger PB, Teirstein PS, et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011;305(11):1097–1105.
33. Zhang Y, Li M, Tang J and Chen X. 2017. Pharmacokinetic and Pharmacodynamic Responses to Clopidogrel: Evidences and Perspectives. Int. J. Environ. Res. Public Health. 14(3): 301.10.3390/ijerph14030301
34. Yin T, Miyata T. Pharmacogenomics of clopidogrel: evidence and perspectives. Thromb Res. 2011;128:307–316.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.