Back to Journals » Breast Cancer: Targets and Therapy » Volume 7
Correlation of clinicopathological outcomes with changes in IHC4 status after NACT in locally advanced breast cancers: do pre-NACT ER/PR status act as better prognosticators?
Authors Chatterjee S, Saha A, Arun I, Nayak S, Sinha S, Agrawal S, Parihar M, Ahmed R
Received 15 August 2015
Accepted for publication 8 October 2015
Published 10 December 2015 Volume 2015:7 Pages 381—388
DOI https://doi.org/10.2147/BCTT.S94516
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Sanjoy Chatterjee,1 Animesh Saha,1 Indu Arun,2 Sonali Susmita Nayak,2 Subir Sinha,3 Sanjit Agrawal,4 Mayur Parihar,5 Rosina Ahmed4
1Department of Radiation Oncology, 2Department of Pathology, 3Department of Medical Statistics, 4Department of Breast Surgery, 5Department of Molecular Pathology, Tata Medical Center, Kolkata, West Bengal, India
Background: Following neoadjuvant chemotherapy (NACT) for breast cancer, changes in estrogen receptor (ER), progesterone receptor (PR), HER2 status, and Ki-67 index (IHC4 status) and its correlation with pathological complete response (pCR) or relapse-free survival (RFS) rates could lead to better understanding of tumor management.
Patients and methods: Pre- and post-NACT IHC4 status and its changes were analyzed in 156 patients with breast cancer. Associations between pCR, RFS rates to IHC4 status pre- and post-NACT were investigated.
Results: pCR was found in 25.3% patients. Both ER and PR positive tumors had the lowest (14.3%) pCR compared to ER and PR negative (29%) or either ER-/PR-positive (38.6%) tumors. PR positivity was significantly associated with less likelihood of pCR (15% versus 34%). The pCR rate was low for luminal A subtype (13.68%) compared to 24.36%, 26.31%, and 33.33% for luminal B, HER2-enriched, and triple-negative subtypes, respectively. There was significant reduction in ER expression and Ki-67 index post-NACT. RFS of patients in whom the hormonal status changed from positive to negative was better compared to those of patients in whom the hormonal status changed from negative to positive.
Conclusion: Although changes in IHC4 occurred post-NACT, pre-NACT hazard ratio status prognosticated RFS better. pCR and RFS rates were lower in PR-positive tumors.
Keywords: neoadjuvant chemotherapy, IHC4 status changes, survival
Background
Improved understanding of breast cancer biology has been possible after identification of targets such as estrogen receptor (ER), progesterone receptor (PR), HER2 (c-erb-2) receptor, and quantifying Ki-67 index (Ki-67). These are commonly identified using simple immunohistochemical tests in accredited laboratories and are together termed as IHC4.1 Consensus from the 2011 St Gallen’s meeting recommended the use of differential expression of IHC4 in various breast cancers as surrogates to molecular classification of such cancers.2 In summary, tumors are considered to be 1) luminal A (LA) when ER and/or PR is positive, HER2 negative, and Ki-67 is <14%); 2) luminal B (LB) when ER and/or PR is positive and either HER2 is positive or Ki-67 ≥14%); 3) HER2 enriched (HE) if ER and PR is negative and HER2 is positive; and 4) triple negative (TN) if ER, PR, and HER2 are all negative.
Neoadjuvant chemotherapy (NACT) is often used to downstage locally advanced breast cancers to allow breast conservation surgery (BCS) or mastectomy.3 While it is likely that tumor volume regression could be associated with changes in IHC4 expression, the correlation of such changes to tumor pathological response rates and clinical disease relapse rates could lead to better understanding of tumor behavior and facilitate future research.
Patients and methods
Tata Medical Centre Institutional Review Board approval was obtained for the project. Patient consent was not required for the study as this study is a retrospective pathological assessment and hypothesis. Unselected consecutive breast cancer patients who had received NACT during January 2012 to December 2013 were identified from a single tertiary cancer center database. IHC4 status was analyzed on the tumor biopsy prechemotherapy and on the residual tumor postchemotherapy.
Pathological tests were performed in a single accredited institutional laboratory and were reviewed by two experienced pathologists. The paraffin blocks of pretreatment biopsy and postsurgical resection specimen were retrieved from the archives of the Department of Pathology of Tata Medical Center. Tissue sections of 4 μm thickness were stained for ER, PR, HER2, and Ki-67 using validated immunohistochemical (IHC) techniques. CONFIRM anti-ER (SP1) ready-to-use (RTU) rabbit monoclonal antibody, CONFIRM anti-PR (1E2) rabbit monoclonal antibody (RTU), and PATHWAY anti-HER2 neu (4B5) rabbit monoclonal primary antibody (PATHWAY HER2 [4B5]) (RTU) were used for ER, PR, and HER2 immunohistochemistry, respectively, using Ventana BenchMark XT (Ventana Medical Systems, Inc., Tucson, AZ, USA) automated staining system. The interpretation of ER, PR, and HER2 results was carried out according to the current American Society of Clinical Oncology (ASCO)/College of American Pathologists (CAP) guidelines for ER, PR, and HER2 testing.4,5 All cases with equivocal HER2 staining were subjected to a fluorescence in situ hybridization test using US Food and Drug Administration-approved Vysis Pathvysion HER2 neu LSI probe with alpha satellite probe CEP17 used as control (Abbott Molecular–Vysis Inc., Des Plaines, IL, USA). The results were reported as per the ASCO/CAP 2013 guidelines6 as follows: not amplified if HER2 gene copy <4.0 or ratio <1.8, equivocal HER2 gene copy 4.0–6.0 or ratio 1.8–2.2, amplified HER2 gene copy >6.0 or ratio >2.2. MIB-1 stain for Ki-67 was done using RTU mouse antihuman Ki-67 monoclonal antibody, MIB-1 clone 1:300, Dako using Leica Bond automated staining system (Leica Biosystems Nussloch GmbH, Nußloch, Germany). For the determination of Ki-67 proliferation index, 500 invasive cancer cells were counted in three randomly selected high-power (×40 objective) fields. The Ki-67 proliferation index was calculated as the percentage of 500 cells that showed nuclear staining by MIB-1, irrespective of the intensity of staining. Response to chemotherapy was reported as per CAP recommendations 2009 to categorize tumors with pathological complete response (pCR), partial response, and no response.7
The clinical data were retrieved from the patient’s electronic medical record system. Patient-related clinical information, including patient demographics, chemotherapy type and intensity as well as follow-up data for disease relapse were analyzed. For the purposes of this study, any disease that had recurred either locoregionally or as distant metastases was taken as disease relapse.
Associations between changes in protein expression and clinical parameters were performed to identify factors that may predict resistance to chemotherapy response.
Statistical analysis was performed using MedCalc version 12. Associations between IHC markers before and after NACT were evaluated using the McNemar’s test for ER, PR, HER2, and a paired Student’s t-test for the Ki-67. Associations between the pCR rates to other categorical variables were assessed using the chi-square tests (including chi-square test for trends in groups) or Fisher’s exact tests. Associations between pCR and the Ki-67 index were performed using the independent Student’s t-test. Kaplan–Meier plots were analyzed to obtain relapse-free survival (RFS) and overall survival at 2 years follow-up. Cox’s proportional hazards model was used to identify any significant association between changes in IHC4 and RFS. Log-rank test was done to compare the RFS among the groups. Hazard ratios (HR) and confidence intervals (CI) were calculated using SAS version 9.4.
Results
A total of 156 patients with locally advanced breast cancers were identified, six (3.9%) of whom had bilateral breast cancers with a total of 162 evaluable breast cancer cases. Their median age was 48 years (range: 23–71 years). Prechemotherapy, 75.5% were ER or PR positive (referred to as hormone receptor positive), 40.5% HER2 positive, and 15.7% had TN tumor. There was no significant association of any subtype of breast cancer with respect to age. Post-NACT, all patients underwent surgical excision with 30.9% having BCS. In the 53 patients where NACT was given with the intention to downstage for breast conservation, BCS was possible in 94.3%. Overall, 41 (25.3%) patients had pCR reported post-NACT. Data on treatment type and dose intensity were not available in nine patients who received chemotherapy at their local center, where documentation was irretrievable. Of 162 patients, 143 (88.27%) received anthracycline–taxane combination chemotherapy among whom 25.17% achieved pCR. Of 162 patients, 19 (11.73%) patients received no taxanes but only anthracycline containing chemotherapy, 26.32% of whom achieved pCR. There was no statistically significant difference in pCR achieved between the two groups. Of all patients receiving NACT, 73 (49.7%) cases received a >15% dose reduction due to toxicities and 14 (9.5%) had a delay of more than 1 week during chemotherapy. The patients who had <15% dose reduction during chemotherapy had the pCR rate of 28.8% compared to 20.6% pCR rate in those who had >15% dose reduction during chemotherapy. The patients with less than 1 week delay in scheduled chemotherapy cycles had the pCR rate of 25.6% compared to 13.3% pCR rate in those who had more than 1 week delay in chemotherapy. The commonest toxicity reported was hematological (neutropenia) with 13 (8.8%) needing hospital admission and 47 (32%) received growth factor supplements during treatment. Use of taxanes, growth factors, or chemotherapy dose intensity did not have a significant effect on pCR rates on univariate analysis.
The association between clinicopathological variables and pCR rates has been detailed in Table 1. Grade 3 tumors had a higher pCR rate (27.4%) with a significant association (P=0.04) in trend for pCR between the three possible grades of disease. The difference in pCR rates was 30.77% versus 24% in younger versus older women (with a comparison around median age) and 28.8% T1/T2 tumors had pCR versus 13.4% for T3/T4. These differences were not found to be statistically significant. Tumors that were positive for both ER and PR had the lowest (14.3%) pCR rates compared to tumors with both ER and PR negative (29%) or those with either ER or PR positive (38.6%). The trend for difference in pCR among the group was found to be statistically significant (P=0.008 chi-square; P=0.03 chi-square value for trend). pCR rates were significantly lower with increasing Allred scores for ER and PR (Table 1). PR positivity was significantly associated with less likelihood of pCR post-NACT (15% versus 34%; P=0.01), with patients with even a PR Allred score of 3–5 showing just a 11.11% pCR compared to 52.63% pCR in those with a ER score of 3–5. Interestingly, associations between ER or HER2 expression alone and pCR rates alone were not statistically significant. It is worth noting that of 62 patients who were HER2 positive, only 14 (22.58%) had received trastuzumab, due to resource availability. HER2 neu-positive patients receiving trastuzumab had a higher pCR rate (35.7%) compared to those who did not get the medicine. Only seven of these 14 patients could continue trastuzumab after surgery for the recommended total of 17 cycles every 21 days.
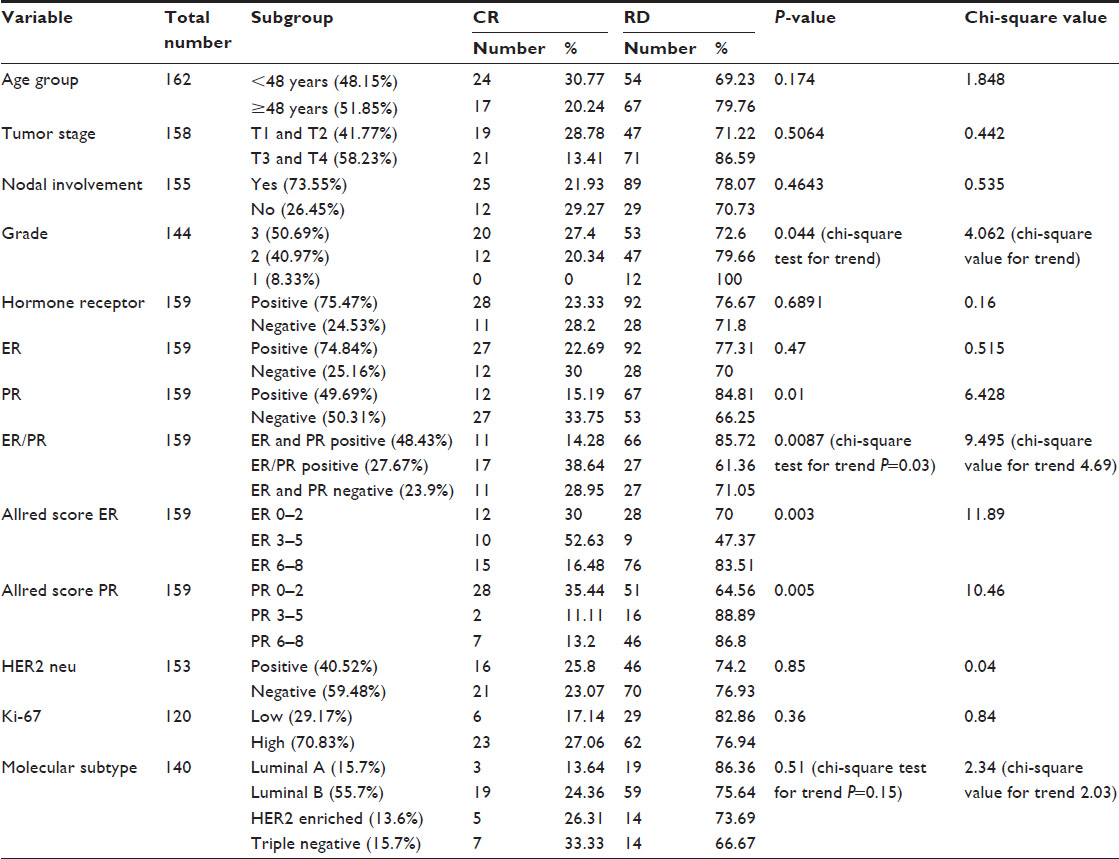 | Table 1 Pathological complete response (pCR) rates and its association to clinicopathological variables |
Ki-67 indices were possible in 140 of the 156 patients (162 samples) due to inadequate tissue retrieval in the remaining 22 cases. A high Ki-67 index (>14%) was found in 70.8% patients. Patients with low Ki-67 had 17.14% pCR rate post-NACT compared 23.07% in those with high Ki-67. The difference in mean Ki-67 rates prior to NACT, among patients achieving pCR versus those not achieving pCR, were not statistically significant (P=0.11).
When we classified the 140 cases into the four molecular subtypes based on the IHC4 data, 78 patients (55.7%) had LB molecular subtype at diagnosis, followed by 22 (15.7%) with LA, 21 (15%) TN, and 17 (13.6%) HE subtypes. The pCR rate was low for LA type tumors (13.68%) compared to 24.36%, 26.31%, and 33.33% for LB, HE, and TN subtypes, respectively (Table 1). The difference between the response rates was statistically insignificant between the four groups.
When pre-NACT IHC4 markers were compared to post-NACT IHC4 (Table 2), there were significant reduction in the expression of ER (P=0.0347) and change in Ki-67 index (P=0.0027), but there were no significant change in PR or HER2 expression. Pre-NACT mean Ki-67 was found to be 30.4% compared to 22.8% post-NACT. Postchemotherapy, 69.14% patients had a decrease in Ki-67 indices, recording a mean decrease of 20.06%. There was no significant difference in changes to Ki-67% postchemotherapy with respect to ER/PR or HER2 status. It is worth noting that adequate tissue for post-NACT ER/PR/HER2 testing was available in 101 out of remaining 121 samples, accounting for pCR in 41 tumors. Post-NACT residual disease sample was adequate for Ki-67 tests in 83 patients.
 | Table 2 Changes in pre- and post-NACT IHC4 |
At a median follow-up of 16 months, two patients (1.28%) developed locoregional recurrence (one in the chest wall and the other in the supraclavicular fossa recurrence), one patient (0.64%) developed contralateral axillary recurrence, and ten patients (6.41%) developed other distant metastases. Seventeen patients (10.89%) were lost to follow-up. Of the 13 patients who recurred or metastasized, seven (53.85%) had LB, four (30.77%) had TN, and two (15.38%) had HE subtype. This accounted for 8.9% of all LB, 19.04% of all TN, and 10.5% of all HE subtypes. No patients with LA subtype had a relapse till the date of the last follow-up. Figure 1 shows the projected difference in relapse-free survival based on ER (Figure 1A) and PR (Figure 1B) expression; P=0.02 and P=0.013, respectively. With respect to the Allred scoring system, the patients were clustered into three different groups (A=0–2, B=3–5, and C=6–8). The HR for the groups based on ER status was calculated with group C as comparator. HR for group A was 8.145 with a 95% CI of 1.59–40.85. HR for group B was 10.243 (95% CI 1.97–57.97). For PR status, log-rank test showed a significant difference between the three Allred groups. The HR between PR Allred 0–2 versus 3–5 was 2.63 (95% CI 0.33–20.34). There was no relapse in PR group Allred 6–8; hence comparison between this group and the others, although appreciable, resulted in a very large HR ratio with CI extending to infinity.
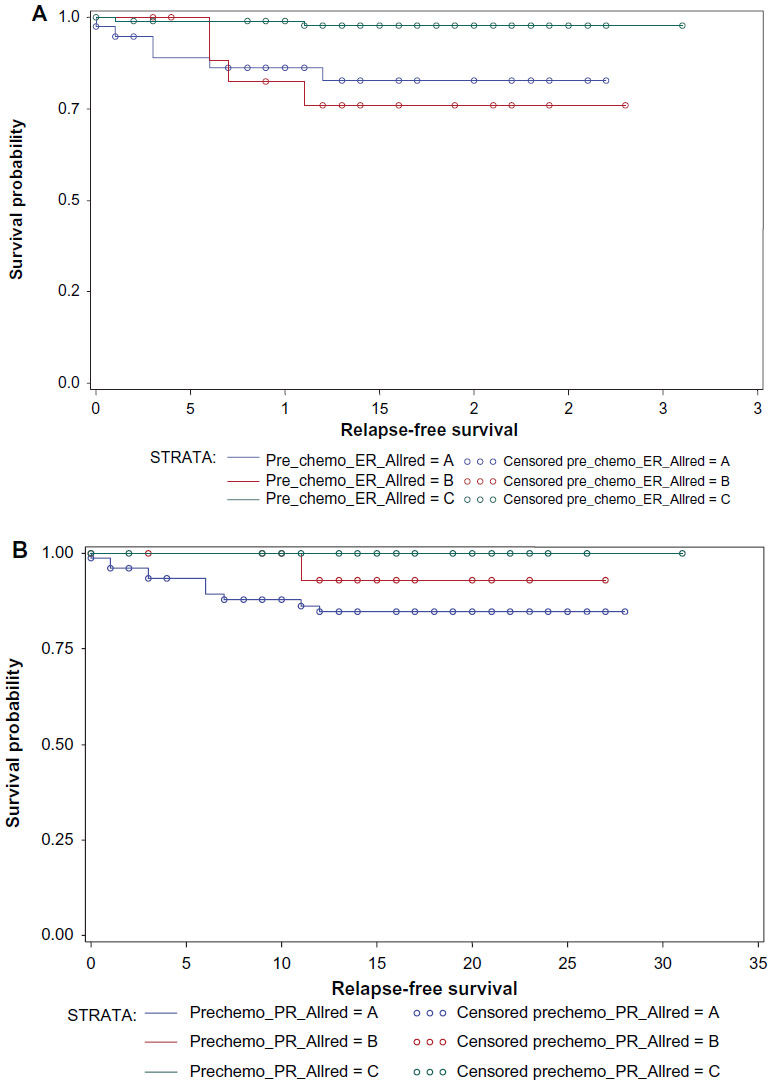 | Figure 1 Kaplan–Meier estimates of relapse-free survival. |
Figure 2 shows the predicted RFS in months at 2 years for the different molecular subtypes. Although the curves show differential RFS for the various molecular subtypes, the log-rank analysis was statistically not significant (P=0.16). Figure 3 shows the predicted RFS for the tumors that had either reduction in Ki-67 or increase/stable Ki-67 or pCR (P=0.86). Figure 4 shows the RFS of patients in whom the hormonal status changed from positive to negative versus those who changed from negative to positive. The curves for RFS although divergent showed a trend toward statistical significance (P=0.06, HR =0.2489, 95% CI 0.18–1.09).
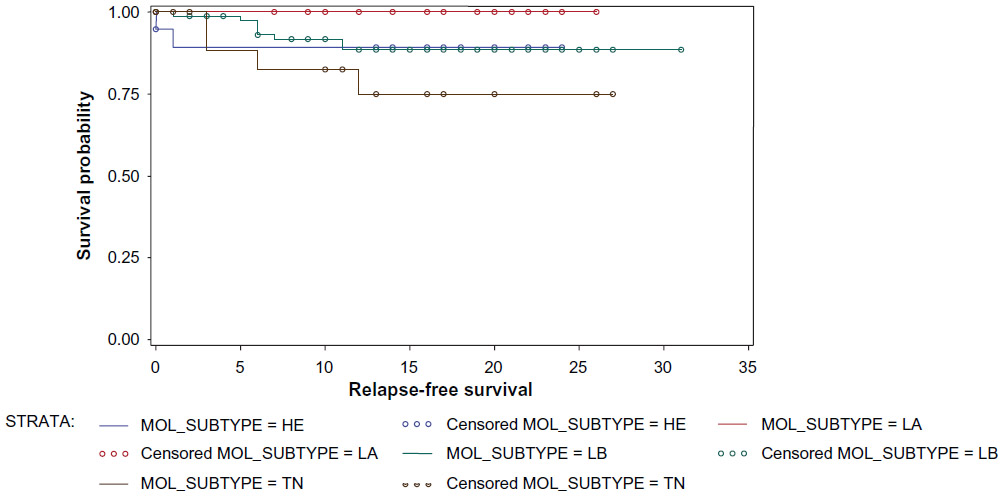 | Figure 2 Kaplan–Meier estimates of relapse-free survival. |
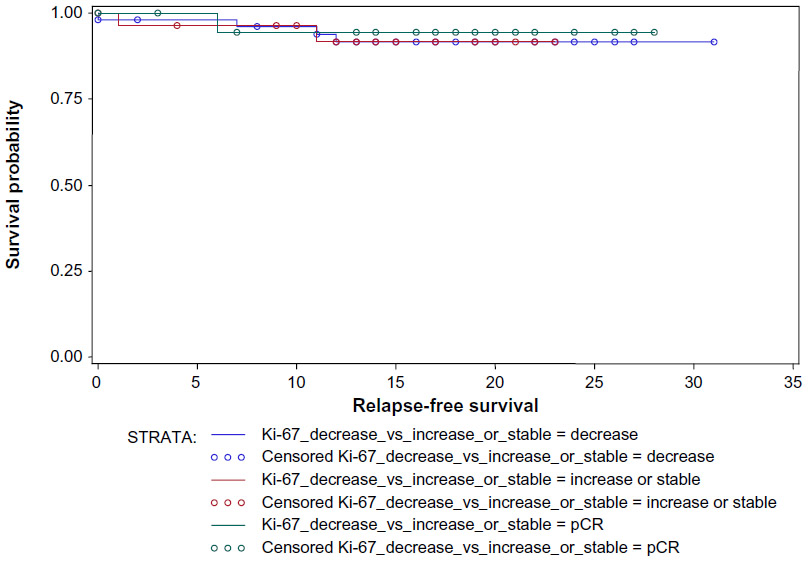 | Figure 3 Kaplan–Meier estimates of relapse-free survival. |
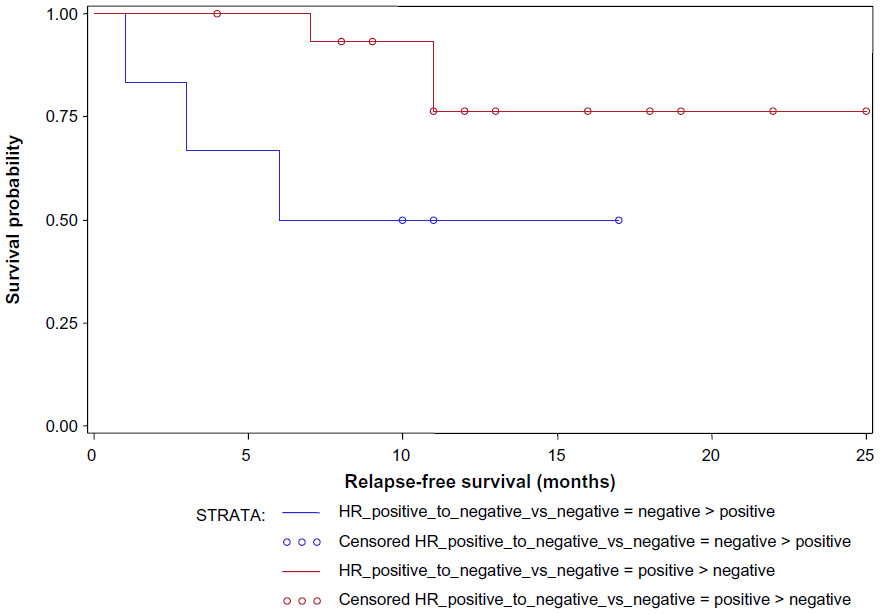 | Figure 4 Kaplan–Meier estimates of relapse-free survival. |
Finally, it is worth noting that although TN cancers had higher pCR rates, paradoxically, relapse in LA tumors was the lowest. This effect, although paradoxical, is a complex area of research. One plausible explanation for the same could be attributed to the fact that endocrine-responsive tumors, such as LA cancers, were intrinsically sensitive to endocrine modulation leading to longer RFS. The use of tamoxifen in low-risk premenopausal patients or aromatase inhibitors in patients, who are postmenopausal or have ovarian ablation, could have accounted for the improvement in relapse rates in these groups.
Discussion
Accurate classification of subtypes of breast cancer can help prognosticate and also predict response to therapy. The use of IHC4 has allowed improved decision-making on the use of adjuvant chemotherapy in patients at intermediate risk of recurrence based on their tumor grade, size, and nodal metastases.1
One of the important issues to consider prior to exploring the differences in the pre- and post-NACT IHC4 status is on how concordant a core biopsy is to the nature of the surgical tumor, without the influence of NACT. Burge et al reported a significant concordance of 95%, 89%, and 96% between 87 core biopsy and surgical specimens for ER, PR, and HER2 status, respectively, in spite of tumor heterogeneity.8 In another study with 175 patients by Lorgis et al, it was concluded that although HER2 status remained the same in almost all cases, core biopsy up-scored ER status in up to 16% and PR status in 22% cases, recommending postsurgery assessments to be more valid.9 Our study was done on 162 samples using set and validated protocols by experienced pathologists. Hence, the statistically significant changes in the ER (>20% cases) and Ki-67% (>40% cases) in our study could not be attributed to just tumor heterogeneity or reporting artifact. There have also been reports of difference in the expression of the ER/PR or HER2 status in the primary versus metastatic sites, but its exact role in the clinical context is yet to be fully understood.10,11
Moreover, when chemotherapy is used to downstage tumors prior to surgery, certain subclones of tumor cells may be preferentially killed, thereby causing a change in IHC4 expression.12 This theory can be validated if there was a better predicted RFS in patients whose more chemosensitive ER-positive clones could have been preferentially eradicated with residual disease exhibiting ER-negative clones only. Our study shows that the predicted RFS is better when hormone receptors changes from ER-positive prechemotherapy to ER-negative postchemotherapy (Figure 4), thereby validating the aforementioned theory. Changes in IHC4 post-NACT have been reported, but these have not shown any consistent trend in the concordance or discordance of the expression of the markers. In the study by Kinsella et al, only 38 pathological specimens were examined pre- and post-NACT.13 The investigators concluded that the PR status is likely to change post-therapy and recommended that the issue warranted further bigger studies. In a recent review of such studies of van de Ven et al, only six out of the 13 studies had more than 100 patients’ specimens analyzed.14 The authors confirmed that bigger studies had shown a 2.5%–17% discordance in the ER status post-NACT, while PR discordance was reported to be between 5.9% and 51.7% cases. In another study by Yang et al, the discordance in ER/PR and HER2 expression post-NACT ranged from 12.4% to 15%.15 Our study analyzed 162 specimens and showed a good concordance in PR and HER2 status post-NACT but confirmed the discordance in ER status in more than 20% cases.
This matter therefore needed an evaluation to ascertain if such pathological changes post-NACT could have any association to tumor response rates or RFS. Although a statistically significant reduction in Ki-67 index postchemotherapy has been reported by Lee et al, as in our study, our results showed a significant change in the ER status post-NACT in contrast to the change in the PR status reported by those authors.16 The pCR rates as reported by us overall and for the various subtypes are in consistence with that reported in the literature confirming that the results of our study can be generalized, and our chemotherapy dose response has been standard.17 The PR expression per se was associated with low pCR rates, and even a moderate PR Allred score of 3–5 was associated with approximately 40% less pCR rates. As expected, Grade 3 tumors showed higher pCR rates. The RFS rates depicted in Figure 1 is in keeping with that expected in the literature with the highest RFS for LA type tumors and lowest for TN types. Nonavailability of trastuzumab for all HER2-positive patients and moderately low-patient numbers in each individual group remain as weaker points of our study and could account for the lack of statistical significance in the difference in RFS between the subtypes.
Importantly, changes in Ki-67 post-NACT did not translate to differential RFS in our study, but PR positivity alone with moderate PR expression or even in the presence of ER positivity was associated with a significantly less pCR rate. Also, it was quite interesting to note that patients with a change in hormone receptors from positive to negative seemed to have better RFS compared to those in whom hormone receptors changed from negative to positive, confirming that prechemotherapy rather than postchemotherapy positivity in the ER/PR status had a better prognostic value.
Conclusion
Changes in IHC4 occur post-NACT. pCR rates were lower with increasing Allred scores for ER and PR. Overall, pCR rates seemed to be lower in PR-positive tumors and pre-NACT, not post-NACT, and HR status seemed to prognosticate RFS better. pCR rates were low for LA type tumors and high with TN subtypes. In contrast, RFS for LA tumors was found to be better possibly due to the endocrine sensitivity of such tumors and available affordable targeted endocrine therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
Barton S, Zabaglo L, A’Hern R, et al. Assessment of the contribution of the IHC4+C score to decision making in clinical practice in early breast cancer. Br J Cancer. 2012;106(11):1760–1765. | |
Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Senn H-J; Panel members. Strategies for subtypes – dealing with the diversity of breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22:1736–1747. | |
Kim R, Osaki A, Toge T. Current and future roles of neoadjuvant chemotherapy in operable breast cancer. Clin Breast Cancer. 2005;6(3):223–234. | |
Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. Arch Pathol Lab Med. 2014; 138(2):241–256. | |
Hammond ME, Hayes DF, Dowsett M, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. Arch Pathol Lab Med. 2010;134(6):907–922. | |
Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31(31):3997–4013. | |
Lester SC, Bose S, Chen YY, et al; Members of the Cancer Committee, College of American Pathologists. Protocol for the examination of specimens from patients with invasive carcinoma of the breast. Arch Pathol Lab Med. 2009;133(10):1515–1538. | |
Burge CN, Chang HR, Apple SK. Do the histologic features and results of breast cancer biomarker studies differ between core biopsy and surgical excision specimens? Breast. 2006;15(2):167–172. | |
Lorgis V, Algros MP, Villanueva C, et al. Discordance in early breast cancer for tumour grade, estrogen receptor, progesteron receptors and human epidermal receptor-2 status between core needle biopsy and surgical excisional primary tumour. Breast. 2011;20:284–287. | |
Lower EE, Glass E, Blau R, Harman S. HER 2/neu expression in primary and metastatic breast cancer. Breast Cancer Res Treat. 2009;113:301–306. | |
Guarneri V, Giovannelli S, Ficarra G, et al. Comparison of HER 2 and hormone receptor expression in primary breast cancers and asynchronous paired metastases: impact on patient management. Oncologist. 2008;13:838–844. | |
Lee SH, Chung MA, Quddus MR, Steinhoff MM, Cady B. The effect of neoadjuvant chemotherapy on estrogen and progesterone receptor expression and hormone receptor status in breast cancer. Am J Surg. 2003;186(4):348–350. | |
Kinsella MD, Nassar A, Siddiqui MT, Cohen C. Estrogen receptor (ER), progesterone receptor (PR), and HER 2 expression pre- and post-neoadjuvant chemotherapy in primary breast carcinoma: a single institutional experience. Int J Clin Exp Pathol. 2012;5(6):530–536. | |
van de Ven S, Smit VT, Dekker TJ, Nortier JW, Kroep JR. Discordances in ER, PR and HER 2 receptors after neoadjuvant chemotherapy in breast cancer. Cancer Treat Rev. 2011;37:422–430. | |
Yang YF, Liao YY, Li LQ, Xie SR, Xie YF, Peng NF. Changes in ER, PR and HER 2 receptors status after neoadjuvant chemotherapy in breast cancer. Pathol Res Pract. 2013;209:797–802. | |
Lee HC, Ko H, Seol H, et al. Expression of immunohistochemical markers before and after neoadjuvant chemotherapy in breast carcinoma, and their use as predictors of response. J Breast Cancer. 2013;16(4):395–403. | |
Bonnefoi H, Litière S, Piccart M, et al; EORTC 10994/BIG 1-00 Study Investigators. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1-00 phase III trial. Ann Oncol. 2014;(6):1128–1136. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.