Back to Journals » Infection and Drug Resistance » Volume 15
Correlation Between the Number of Fiberoptic Bronchoscopies and Nosocomial Infection/Colonization of Carbapenem-Resistant Enterobacteriaceae
Authors Wang WH, Wu YH, Wang YM, Wang CL, Liu Y, Gao P, Wu XJ, Ying JQ
Received 4 March 2022
Accepted for publication 18 May 2022
Published 20 June 2022 Volume 2022:15 Pages 3205—3211
DOI https://doi.org/10.2147/IDR.S365053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wei-Hua Wang,1 Ying-Hong Wu,2 Yi-Min Wang,3 Chun-Lei Wang,4 Yun Liu,1 Peng Gao,1 Xiao-Jing Wu,3 Jiao-Qian Ying1
1Department of Medical Affairs, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China; 2Department of Nosocomial Infection Control, People’s Hospital of Peking University, Beijing, 100044, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China; 4Laboratory of Clinical Microbiology and Infectious Diseases, Department of Pulmonary and Critical Care Medicine, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
Correspondence: Jiao-Qian Ying, Department of Medical Affairs, China-Japan Friendship Hospital, No. 2 of Yinghua East Street, Chaoyang District, Beijing, 100029, People’s Republic of China, Tel +86 10 84205608, Fax +86 10 84222965, Email [email protected]
Objective: The present study aims to explore the effects of different numbers of fiberoptic bronchoscopic examinations on the nosocomial infection/colonization of carbapenem-resistant Enterobacteriaceae (CRE).
Methods: The data of 129 patients admitted to the intensive care unit of a grade 3A hospital were retrospectively analyzed, and CRE nosocomial infection/colonization situations in patients with fiberoptic bronchoscope application times of 1, 2, 3, and ≥ 4 were statistically analyzed.
Results: The incidence of nosocomial infection/colonization of CRE increased significantly when the number of fiberoptic bronchoscopic examinations was ≥ 3.
Conclusion: Nosocomial infection/colonization of CRE is highly correlated with an increased number of fiberoptic bronchoscopic examinations.
Keywords: nosocomial infection/colonization, carbapenem-resistant Enterobacteriaceae, fiberoptic bronchoscopy, number of inspections
Introduction
With the rapid development of medical technology, fiberoptic bronchoscopy (FBC) has become widely used in clinical diagnosis and treatment due to its advantages of large visual range and convenient operation; it is in a pivotal position especially in the rescuing of patients in a severe state. However, due to the fiberoptic bronchoscope’s fine structure, special materials, and non-resistance to high temperature and pressure, cleaning and disinfection after use is difficult; if the cleaning and disinfection of the fiberoptic bronchoscope are not sufficient, nosocomial infection will occur.1
Nosocomial infection, also known as hospital infection or hospital-acquired infection (HAI),2 refers to an infection acquired by inpatients at a hospital, including infection acquired during hospitalization and infection acquired at the hospital after discharge; however, it does not include infections that began before admission or existed at the time of admission.
Since 2000, there have been many outbreaks of pathogen infection caused by endoscopic contamination;3 some endoscopes were even detected with multidrug-resistant bacteria, such as carbapenem-resistant Enterobacteriaceae (CRE).4 The in-hospital mortality rate of CRE infection was high (64.5%).5
This retrospective study aimed to analyze the correlation between the number of FBC examinations and the occurrence of nosocomial infection/colonization of CRE, to clarify the negative impact of the number of FBC examinations on patients.
Subjects and Methods
Subjects
This study is a retrospective study. Patients who underwent FBC in the intensive care unit (ICU) of a grade 3A hospital between January 1, 2017, and December 31, 2020, were enrolled. A pathogenic test was carried out: the specimens were bronchoalveolar lavage fluid, sputum, and pleural effusion; the results showed a presence of Enterobacteriaceae; and the drug resistance phenotype was carbapenem-resistant (Table 1). Inclusion criteria: ① Patients who underwent FBC in the intensive care unit from 2017 to 2020; ② Patients who were sent for pathogenic examination on admission; ③ Patients with CRE in the etiological results. Exclusion criteria: ①Patients who could not access the complete medical records; ②Patients who submitted non-respiratory specimens for pathogenic specimens.
 |
Table 1 Basic Clinical Information of Analyzing Patients |
Study Methods
Data Source
The present paper is a retrospective study of data obtained from the ICU of a grade 3A hospital. The information was collected from the hospital electronic medical record system, microbiological examination system, and hospital information system.
Diagnostic Criteria
The diagnosis of nosocomial infection was based on the Diagnostic Criteria for Nosocomial Infection (Trial) issued by the Ministry of Health in 2001,2 and the hospital infection cases were reviewed by the hospital infection management department and clinicians.
Definition of Relevant Indicators
Hospital Stay
Hospital stay of nosocomial infection/colonization of CRE = date of first detection of CRE in a respiratory tract specimen − date of admission.
Hospital Colonization
No CRE was detected through etiology when the patient was admitted to the hospital; positive CRE was reported after hospitalization for ≥48 h. The doctor determined that the non-infection was colonization, and antibiotics were not administered.
Research Indicators
Indicators of nosocomial infection/colonization: The correlation between nosocomial infection/colonization of CRE and the number of FBC examinations was analyzed.
Bacterial Culture
The bronchoalveolar lavage fluid, sputum, and pleural effusion samples submitted for clinical examination were inoculated, isolated, and cultured in accordance with the requirements of the National Inspection Technical Operation Procedures. Duplicate strains from the same patient, same sample source, and same site were eliminated.
Bacterial Identification
The bacteria were identified using the Bruker MicroFlex mass spectrometer.
Drug Sensitivity Tests
The sensitivity of carbapenem antibiotics, such as imipenem and meropenem, was determined using the instrumental method (automatic bacterial identification drug sensitivity instrument VITEK 2 compact) and the Kirby–Bauer disk diffusion method. The drug sensitivity test results were determined in accordance with the Clinical and Laboratory Standards Institute 2017 standard.
Statistical Analysis
Microsoft Office Excel 2017 was used for data collection and summary, and Minitab 20.2 was used for statistical data analysis. The Chi-square test was used to analyze the correlation between risk factors for nosocomial infection/colonization of CRE. The data were compared using a two sample t-test and a probability logistic regression test. A P value of <0.05 was considered statistically significant.
Results
General Situations
In order to explore the influence of the collected indicators on the possibility of infection/colonization of patients with CRE, we first used the chi-square correlation test method to analyze the correlation between variables, and obtained the following results. Among the 129 patients included in the present study, 73 (56.6%) had nosocomial infection/colonization of CRE and 56 (43.4%) did not. The statistical analyses revealed that there was no significant difference in the number of cases of nosocomial infection/colonization of CRE among the age groups (ages ≤19, 20–49, 50–69, and ≥70) (Pearson = 0.240, degrees of freedom (DF)= 3, P = 0.971).
The patients comprised 90 males (69.8%) and 39 females (30.2%); there was no significant difference in the proportion of gender (Pearson = 0.001, DF = 1, P = 0.978). Among these patients, carbapenems were used in 74 patients (57.4%) and not used in 55 patients (42.6%); the difference in the proportion of patients who were/were not treated with carbapenems was not statistically significant (Pearson = 0.582, DF = 1, P = 0.445). Respiratory diseases were the main diagnoses in 105 of the patients (81.4%), and the remaining 24 patients (18.6%) had a different main diagnosis; the difference in the proportion of diagnosis of patients was not statistically significant (Pearson = 0.521, DF = 1, P = 0.470).
Length of Hospital Stay
2.2.1 A descriptive statistical analysis of the length of hospital stay was carried out: minimum value = 0.0, lower interquartile = 2.0, median value = 8.0, mean value = 35.9, upper interquartile = 19.5, maximum value = 1424.0, interquartile spacing = 17.5, and coefficient of variation = 386.48.
According to the analysis results, the length of hospital stay was divided into four groups, and the number of FBC examinations was compared among the different groups. The number of FBC examinations increased with the extension of the hospital stay length.
The statistical analysis results revealed that the length of hospital stay was correlated with the number of FBC examinations; the difference was statistically significant (Pearson = 103.872, DF = 9, P = 0.000 < 0.05; Table 2).
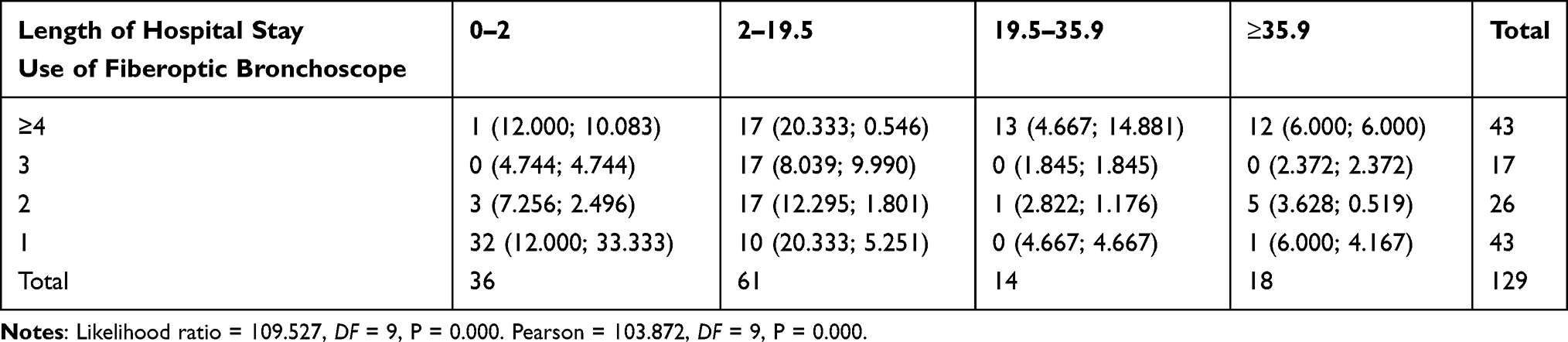 |
Table 2 The Length of Hospital Stay and Number of Fiberoptic Bronchoscopic Examinations |
2.2.2 The data on nosocomial infection/colonization of CRE were compared among the length of hospital stay groups. The results revealed that the rate of nosocomial infection/colonization of CRE increased with the extension of hospital stay length. The data comparison revealed that the length of hospital stay was correlated with nosocomial infection/colonization of CRE; the difference was statistically significant (Pearson = 60.911, DF = 3, P = 0.000 < 0.05; Table 3).
 |
Table 3 The Incidence of Nosocomial Infection/Colonization of CRE and Length of Hospital Stay |
Analysis of Risk Factors for Nosocomial Infection/Colonization of CRE
The results of the present study revealed that nosocomial infection/colonization of CRE was associated with the use of FBC; the analysis results are presented in Table 4. Additionally, the data showed that the chance of nosocomial infection/colonization of CRE was significantly higher in patients with an FBC examination number of ≥3 than in patients with a number of 1–2; the analysis results are presented in Table 5.
 |
Table 4 Correlation Between Nosocomial Infection/Colonization of CRE and the Use of Fiberoptic Bronchoscopy |
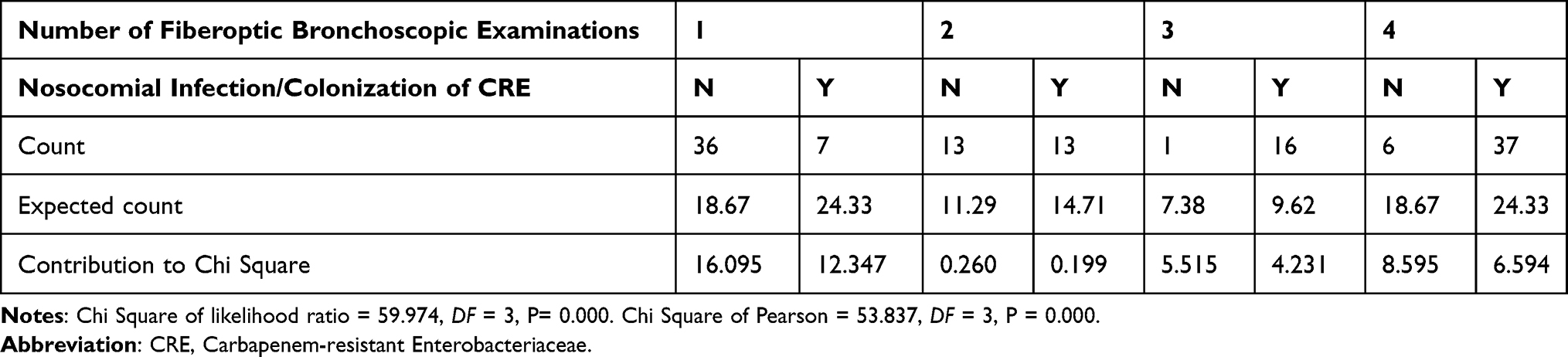 |
Table 5 Correlation Between Nosocomial Infection/Colonization of CRE and the Number of Fiberoptic Bronchoscopic Examinations |
Among the patients included in the present study, the FBC examination number was: 1 time with 43 patients (33.3%); 2 times with 26 patients (20.1%); 3 times with 17 patients (13.1%); and ≥4 times with 43 patients (33.3%). Logistic regression method was used for this group of data. The occurrence of nosocomial infection/colonization of CRE was used as the dependent variable, and the remaining indicators were used as independent variables for regression. The results showed that the P value was 0.052 when hospitalization time was used as a risk factor, and the P value was 0.000 when FBC examination number was used as a risk factor, both of which were less than 0.1, indicating that these two variables have a greater impact on the occurrence of nosocomial infection/colonization of CRE. And the OR values were 1.062 and 2.647, both greater than 1, indicating that both factors would increase the probability of nosocomial infection/colonization of CRE (Table 6). The area under the ROC curve was 0.894, indicating that this judgment method has good diagnostic authenticity.
 |
Table 6 Logistic Analysis of Different Risk Factors and Nosocomial Infection/Colonization of CRE |
Discussion
In this study, the related factors of nosocomial infection/colonization of CRE were explored. The analysis revealed that FBC was highly correlated with nosocomial infection/colonization of CRE. Furthermore, the results revealed that the higher the number of FBC examinations, the higher the chance of nosocomial infection/colonization of CRE.
These findings in the present study suggest that bronchoscopes may pose an under-recognized potential for transmission of CRE and related multidrug-resistant organisms (MDROs), warranting greater public awareness, enhanced preventive measures, and updated reprocessing guidance.6 Many research reports worldwide pointed out that non-standard fiberoptic bronchoscope use or cleaning and disinfection as well as equipment obstacles have caused single or mixed bacterial cross infection, such as multidrug-resistant Acinetobacter baumannii,7 multidrug-resistant Pseudomonas aeruginosa,8,9 carbapenem-resistant Klebsiella pneumoniae,8 maltophilia,10,11 and even hospital acquired Infection (HAP).
Any deviation from proper reprocessing (eg, crevices associated with the elevator channel) could lead to failure to eliminate contamination, with a possibility of subsequent patient-to-patient transmission.12 However, there is no data showing the relationship between the number of FBC examinations and the occurrence of HAI.
The use of FBC was an important risk factor for cross infection of MDROs in the ICU. Non-standard fiberoptic bronchoscope cleaning and disinfection is one of the most important factors.6 Therefore, the management team of the hospital should pay attention to FBC management, establish a multidisciplinary team model, and implement multi-department cooperation.
Implementing unified and standardized management, such as setting up an endoscopy center, uniformly allocating personnel, integrating resources, and promoting fiberoptic bronchoscope sharing, should be carried out to serve the clinical work with the clinical work as the center.
Hospitals should update the professional knowledge of medical personnel and continuously improve the process and layout with the introduction of new national standards. According to the workload requirement, hospitals should appropriately increase their number of endoscopes, update the cleaning and disinfection facilities, ensure endoscope cleaning and disinfection quality, and ensure the safety of patients.
Of course, our research still has certain limitations. For example, our research is a retrospective study without randomization, and the data may be biased to a certain extent. In the future, we plan to conduct a prospective randomized controlled study to expand the sample size. With a view to eliminating data gaps as much as possible.
Conclusion
The statistical data analysis in the present study revealed that the length of hospital stay was correlated with nosocomial infection/colonization of CRE. Several studies have evaluated risk factors for acquiring CRE versus carbapenem-susceptible Enterobacteriaceae, identifying antibiotic use and length of hospital stay as major players.[13] Lastly, CRE acquisition resulted in prolonged hospitalization;5 therefore, nosocomial infection/colonization of CRE is highly correlated with an increased number of fiberoptic bronchoscopic examinations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Han L, Yu RZ, Lin L, Yuan M. Exploring the effect of process re-engineering in the cleaning, disinfection, packaging and supply of fiberoptic bronchoscopes in a sterile supply center. Zhong Guo Wei Sheng Chan Ye. 2019;16(19):150–151. Chinese.
2. Ministry of Health of the People’s Republic of China. Diagnostic criteria for hospital-acquired infections (trial). Beijing; 2001.
3. Cai L, Zhang HJ, Yang YH. Research progress of prevention and control of endoscopy-related infection. Zhong Guo Gan Ran Kong Zhi Za Zhi. 2016;15(7):533–536. Chinese.
4. Muscarella LF. Risk of transmission of carbapenem-resistant Enterobacteriaceae and related “superbugs” during gastrointestinal endoscopy. World J Gastrointest Endosc. 2014;6(10):457–474. PMID: 25324917; PMCID: PMC4198391. doi:10.4253/wjge.v6.i10.457
5. Chuah CH, Gani Y, Sim B, Chidambaram SK. Risk factors of carbapenem-resistant Enterobacteriaceae infection and colonisation: a Malaysian tertiary care hospital based case-control study. J R Coll Physicians Edinb. 2021;51(1):24–30. PMID: 33877130. doi:10.4997/JRCPE.2021.107
6. Mehta AC, Muscarella LF. Bronchoscope-related “Superbug” infections. Chest. 2020;157(2):454–469. PMID: 31421109. doi:10.1016/j.chest.2019.08.003
7. Xia Y, Lu C, Zhao J, et al. A bronchofiberoscopy-associated outbreak of multidrug-resistant Acinetobacter baumannii in an intensive care unit in Beijing, China. BMC Infect Dis. 2012;12:335. PMID: 23198973; PMCID: PMC3562511. doi:10.1186/1471-2334-12-335
8. Galdys AL, Marsh JW, Delgado E, et al. Bronchoscope-associated clusters of multidrug-resistant Pseudomonas aeruginosa and carbapenem-resistant Klebsiella pneumoniae. Infect Control Hosp Epidemiol. 2019;40(1):40–46. PMID: 30451128. doi:10.1017/ice.2018.263
9. Alipour N, Karagoz A, Taner A, et al. Outbreak of hospital infection from biofilm-embedded pan drug-resistant Pseudomonas aeroginosa, due to a contaminated bronchoscope. J Prev Med. 2017;2(2):1. PMID: 29225413. doi:10.21767/2572-5483.100014
10. Guy M, Vanhems P, Dananché C, et al. Outbreak of pulmonary Pseudomonas aeruginosa and Stenotrophomonas maltophilia infections related to contaminated bronchoscope suction valves, Lyon, France, 2014. Euro Surveill. 2016;21(28). PMID: 27458712. doi:10.2807/1560-7917.ES.2016.21.28.30286
11. Waite TD, Georgiou A, Abrishami M, Beck CR. Pseudo-outbreaks of Stenotrophomonas maltophilia on an intensive care unit in England. J Hosp Infect. 2016;92(4):392–396. PMID: 26876747. doi:10.1016/j.jhin.2015.12.014
12. Rutala WA, Weber DJ. Outbreaks of carbapenem-resistant Enterobacteriaceae infections associated with duodenoscopes: what can we do to prevent infections? Am J Infect Control. 2016;44(5Suppl):e47–e51. PMID: 27131135. doi:10.1016/j.ajic.2015.10.037
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.