Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Correlation Between Lipid Accumulation Product and Metabolic Dysfunction-Associated Steatotic Liver Disease in Chinese Adults with Type 2 Diabetes Mellitus
Authors Liu W, Xu L ![]() , Yu Y, Qiao L, Zhang L, Chu X, Jing H, Cao L
, Yu Y, Qiao L, Zhang L, Chu X, Jing H, Cao L
Received 22 February 2025
Accepted for publication 7 June 2025
Published 24 June 2025 Volume 2025:18 Pages 2007—2017
DOI https://doi.org/10.2147/DMSO.S518649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Wei Liu,1,* Lingling Xu,1,* Yuan Yu,2 Liang Qiao,1 Lijuan Zhang,1 Xiaoqiu Chu,1 Haibo Jing,3 Lin Cao1
1Department of Endocrinology, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210028, People’s Republic of China; 2Department of Gastroenterology, Jiangning Hospital of Traditional Chinese Medicine, Nanjing, Jiangsu, 211100, People’s Republic of China; 3Department of General Surgery, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210028, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lin Cao, Department of Endocrinology, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, NO. 100 Shizi Street, Hongshan Road, Nanjing, Jiangsu, 210028, People’s Republic of China, Tel/Fax +86-25-85608733, Email [email protected] Xiaoqiu Chu, Department of Endocrinology, Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, NO. 100 Shizi Street, Hongshan Road, Nanjing, Jiangsu, 210028, People’s Republic of China, Tel/Fax +86-25-85608735, Email [email protected]
Objective: To evaluate the value and feasibility of the lipid accumulation product (LAP) in the prediction of metabolic dysfunction-associated steatotic liver disease (MASLD) in Chinese adults with type 2 diabetes mellitus (T2DM).
Methods: In this cross-sectional study, we assessed the value of LAP and other novel indices in the prediction of MASLD in Chinese adults with T2DM in a total of 642 patients. Receiver Operating Characteristic (ROC) curves were plotted to assess the predictive ability of the indices for the occurrence of MASLD in T2DM.
Results: The results showed that LAP had a strong predictive ability for the occurrence of MASLD in T2DM in both men and women and was superior to other traditional visceral fat-related indices. In men, the area under curve (AUC) (95% CI) was 0.815 (0.771– 0.859) with cut-off value of 36.01, and its sensitivity and specificity were 71.91% and 77.44%, respectively. And in women, the AUC (95% CI) was 0.816 (0.762– 0.870) with cut-off value of 24.22, and its sensitivity and specificity were 84.93% and 63.54%, respectively.
Conclusion: LAP has a high predictive ability for the occurrence of MASLD in T2DM in both men and women and are superior to other traditional visceral fat-related indices.
Keywords: diabetes mellitus, type 2, metabolic dysfunction-associated steatotic liver disease, lipid accumulation product
Introduction
The Global Diabetes Map (11th Edition) shows that there are currently more than 589 million people living with diabetes globally, and by 2050, the number of people with diabetes will reach 853 million.1 Diabetes has become one of the major global public health problems. Among the diabetic population, about 90% or more suffer from type 2 diabetes mellitus (T2DM). In the development of T2DM, it is often comorbid with metabolic disorders such as dyslipidemia, insulin resistance (IR), obesity, and metabolic dysfunction-associated steatotic liver disease (MASLD). A meta-analysis showed that the global prevalence of MASLD in T2DM patients is as high as 55.5%, and the risk of liver fibrosis is about 17%.2 The coexistence of the two not only increases the risk of diabetes-related complications but also increases the occurrence of cirrhosis and hepatocellular carcinoma. Therefore, early screening for MASLD in the T2DM population and timely intervention are necessary. In recent years, scholars at home and abroad have made many explorations in the predictive diagnostic models of MASLD, among which the more representative ones in China include the fatty liver disease index, the MASLD screening score, the MASLD ridge regression score, etc. However, most of them are still in the research stage and lack external validation, so they cannot be widely used in the clinic. Besides that, clinical tests such as computed tomography (CT), magnetic resonance imaging (MRI), liver biopsy and so on cannot be used for population screening due to the high price and low acceptance of the patients. Recent studies have indicated that indicators such as the hepatic steatosis index (HSI),3 fatty liver index (FLI),4 and serum galectin-15 exhibit potential predictive value for the onset and progression of MASLD. In contrast, this study focuses on the clinical significance and predictive efficacy of the lipid accumulation product (LAP). LAP is a new type of visceral fat-related index based on the calculation of waist circumference and blood lipid index, which can better reflect individual fat distribution and visceral fat accumulation. Furthermore, it is closely related to IR, T2DM, metabolic syndrome (MetS), CVD, etc.6 IR serves as the central pathological link between MASLD and MetS.7 Driven by IR, enhanced lipolysis in adipocytes and excessive production of free fatty acids (FFA)8 lead to the accumulation of lipotoxic substances within hepatocytes, resulting in cellular injury and eventual progression to fibrosis.9 In this process, abdominal obesity and elevated triglyceride (TG) levels act synergistically: visceral adipose tissue exacerbates systemic inflammation and metabolic dysregulation through the secretion of adipokines such as leptin, adiponectin, resistin, visfatin, and chemerin,10 while abnormal TG deposition directly contributes to hepatic steatosis. Recent studies further demonstrate that omega-3 fatty acid interventions reducing TG levels significantly ameliorate liver steatosis,11,12 which not only confirms the pivotal role of TG in the pathogenesis of MASLD but also provides mechanistic evidence supporting the strong association between the LAP—a composite index integrating waist circumference (WC) and TG—and MASLD. Previous studies showed that LAP was significantly associated with the prevalence and severity of MASLD and had good accuracy in the diagnosis of MASLD.13 Also, LAP had a good predictive value for MASLD in obese children and was closely related to IR and uric acid levels.14 There are fewer studies on the correlation between LAP and T2DM complicated with MASLD in China. Therefore, we aimed to assess its predictive value for the risk of MASLD and provide new insight for the prevention and diagnosis of MASLD in T2DM.
Materials and Methods
Study Population
This cross-sectional study included 642 patients with T2DM aged 18–80 years old who were admitted to the Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine, from January 2018 to December 2023, and all of them met the 1999 WHO diagnostic criteria for diabetes mellitus.15 Exclusion criteria: (1) type 1 diabetes mellitus (T1DM), gestational diabetes mellitus (GDM), or special types of diabetes mellitus; (2) history of severe infections or advanced diabetes mellitus complications [advanced cardiovascular disease (CVD), congestive heart failure (CHF), chronic kidney disease (CKD) > stage 3]; (3) history of acute and chronic liver diseases such as viral hepatitis, alcoholic liver disease, autoimmune liver disease, drug-induced liver injury, and drug (eg, tamoxifen, valproate, methotrexate, and glucocorticoids) induced hepatic fat deposition; (4) any biliary tract disease (ie, primary biliary cirrhosis, primary sclerosing cholangitis, and history of biliary tract obstruction); (5) history of alcohol consumption, more than 140 grams per week for men and 70 grams per week for women; (6) combination of other serious comorbidities such as severe cardiovascular, cerebrovascular, hepatic and renal insufficiency, infectious diseases, psychiatric disorders, or malignant neoplasms; (7) taking lipid lowering medications, following weight loss diets, or taking weight loss supplements; (8) pregnant or breastfeeding women.
Clinical Parameters
Age, sex, smoking status, and history of hypertension and dyslipidemia were recorded on admission to the hospital. Height and weight were measured using a calibrated integrated electronic measuring device (Bingyu RGZ-160) with patients in a standing position, without shoes, and wearing light undergarments only. Measurements were recorded to the nearest 0.5 cm for height and 0.1 kg for weight. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured with the patients’ arms placed at the same level as the heart after sitting still for 5 minutes, and three measurements were taken using an Omron electronic blood pressure monitor (HEM-752FUZZY). Body mass index (BMI) was calculated as weight (kg)/height (m2). WC was measured by detecting the distance between the lowest point of the lower edge of the ribs and the midpoint of the line of the anterior superior iliac spine using a soft ruler.
Biochemical examinations were performed in the morning after overnight fasting (at least 10 hours without any food, except water). Indicators included total cholesterol (TC), TG, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting blood glucose (FBG), alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), and alkaline phosphatase (ALP), serum creatinine (SCr), blood urea nitrogen (BUN), and uric acid (UA) were measured by Roche Cobas 8000. 2-hour postprandial blood glucose (2hPG) was measured by the glucose oxidase method, and hemoglobin A1c (HbA1c) was detected by high-performance liquid chromatography.
Formula
(1) Waist-to-height ratio (WHtR) calculated by dividing WC by height, is an age-independent, easy-to-use screening tool that is more sensitive and cost-effective than BMI for detecting health risks.16

(2) Metabolic score of insulin resistance (METS-IR) evaluates IR by integrating routine metabolic parameters such as BMI, TG0 (fasting triglycerides), G0 (fasting glucose) and HDL-C, without requiring direct insulin measurements. This index effectively identifies IR-related pathological mechanisms associated with MetS.18

(3) Metabolic score for visceral fat (METS-VF) estimates visceral adipose tissue by integrating clinical parameters including age, sex, WHtR, and METS-IR, demonstrating broad applicability and reliability across diverse ethnic populations.20

(4) LAP is a novel obesity-related indicator that assesses abdominal fat accumulation, particularly quantifying visceral adipose deposition. Extensive studies have validated its strong association with MetS, CVD, and T2DM, demonstrating its utility in accurately predicting risks of IR, CVD, and MetS.22


(5) Visceral adiposity index (VAI) is a novel method for quantifying visceral obesity using WC, BMI, TG, and HDL-C. Studies have demonstrated strong concordance between VAI and CT-measured visceral fat, highlighting its robust predictive capacity for the onset of glucose and lipid metabolic disorders.24


(6) A body shape index (ABSI) is a novel anthropometric index that incorporates waist circumference, height, and body mass to better reflect an individual’s fat distribution and visceral fat proportion, offering a more nuanced assessment than BMI.
(7) Body roundness index (BRI), calculated using height and WC, is an effective tool for assessing body fat percentage and visceral adipose distribution. Compared to the BMI, BRI demonstrates superior accuracy in predicting metabolic disease risks, particularly in individuals with normal BMI but abnormal body fat distribution.

(8) Cardiometabolic index (CMI) is a novel metric that integrates WC, TG, HDL-C, and height. Compared with traditional indicators such as BMI, CMI provides a more comprehensive assessment of metabolic health by reflecting both visceral adiposity and lipid-glucose dysregulation.

Ultrasonic Measurement
The diagnosis of MASLD was made with reference to the guidelines for the prevention and treatment of metabolic dysfunction-associated (non-alcoholic) fatty liver disease of Chinese Society of Hepatology in 2024.29 The diagnosis of MASLD was mainly based on the results of an abdominal ultrasound examination, which was performed by a color ultrasound model of the Siemens Acuson X300 with a probe frequency of 3.5 MHz and was carried out by a highly experienced and uniformly trained senior ultrasonographer.
Statistical Analysis
SPSS 25.0 statistical software was used for data analysis. The data processing workflow included normality testing. Normally distributed data are presented as mean ± standard deviation (SD), while non-normally distributed data are expressed as median with interquartile ranges (IQR). Intergroup comparisons were conducted using independent samples t-tests for normally distributed variables and Mann–Whitney U-test for non-normally distributed variables. Categorical variables are expressed as frequencies and percentages (%), with intergroup comparisons performed using Pearson’s chi-square (χ²) test or Fisher’s exact test as appropriate. Logistic regression models were employed to identify risk factors associated with MASLD: Model 1 (unadjusted); Model 2 (adjusted for BMI and diastolic blood pressure in females). Receiver operating characteristic (ROC) curve analysis was performed to compare the predictive capabilities of indicators and determine optimal cut-off values. Two-tailed p-values < 0.05 were considered statistically significant.
Results
Baseline Characteristics
Based on the inclusion and exclusion criteria, 642 T2DM patients with a mean age of 57 (50, 64) years were finally included in the study, of which 242 (37.69%) were females and 400 (62.31%) were males. MASLD was diagnosed by ultrasound in 413 patients with an overall detection rate of 64.33%, of which 60.33% were females and 66.75% were males. The baseline characteristics of the 642 T2DM patients who were included are shown in Table 1.
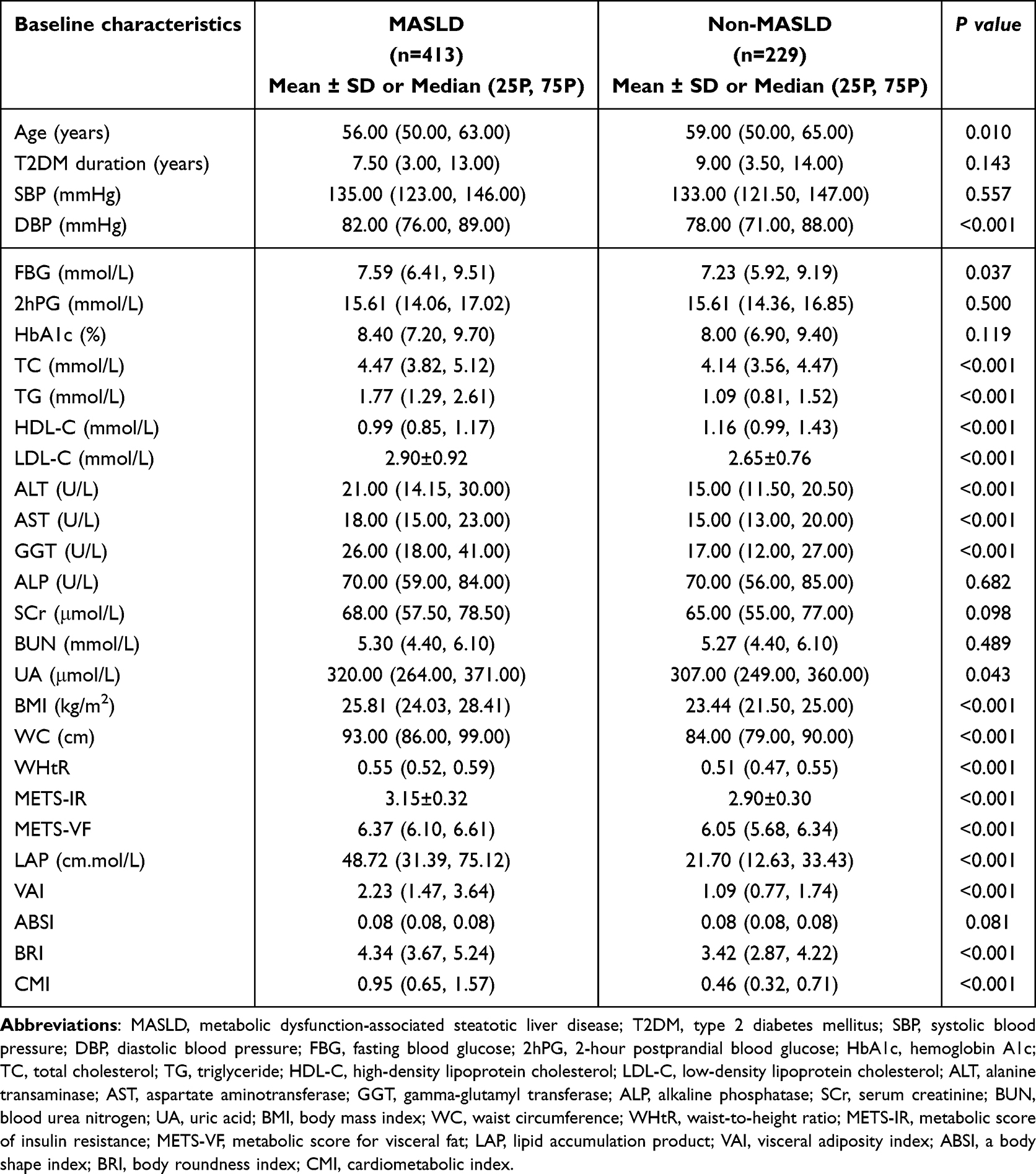 |
Table 1 Comparison of Baseline Characteristics of Study Participants |
MASLD Detection in LAP Quartile Subgroups in T2DM Patients
The detection rate of MASLD in both males and females increased progressively with increasing LAP values, as is shown in Figure 1. In male patients, the detection rates of MASLD in the Q1 (LAP ≤ 23.02), Q2 (23.02 ≤ LAP < 40.91), Q3 (40.91 ≤ LAP < 67.03), and Q4 (LAP ≥ 67.03) groups were 30%, 62%, 83%, and 92% (χ2=102.492, P< 0.001). In female patients, the detection rates of MASLD in the Q1 (LAP ≤ 19.28), Q2 (19.28 ≤ LAP < 33.66), Q3 (33.66 ≤ LAP < 52.20), and Q4 (LAP ≥ 52.20) groups were 19.7%, 60%, 70.5%, and 91.7%, respectively (χ2=69.387, P< 0.001).
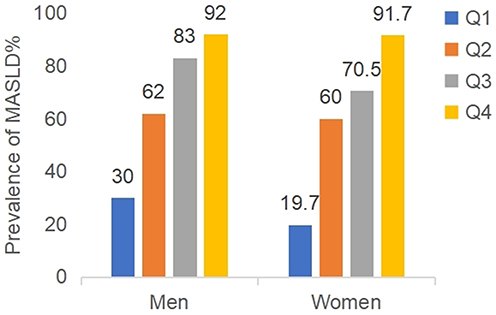 |
Figure 1 Prevalence of MASLD in LAP quartile subgroups in T2DM patients. |
Multifactorial Analysis of the Corelationship Between LAP and MASLD
In multifactorial logistic regression model 1, different quartile levels of LAP were positively associated with the risk of MASLD in both male and female populations. In model 2, the odds ratio for MASLD were 1.000 (reference group), 3.807 (2.114–6.855), 11.392 (5.802–22.367), and 26.833 (11.589–62.129) with increased LAP levels in men (P< 0.001). In model 2 for women, after adjusting for BMI and SBP, the odds ratio for MASLD were 1.000 (reference group), 4.773 (1.953–11.667), 5.887 (2.295–15.102), and 20.412 (5.781–72.069) respectively (P< 0.001) (Table 2).
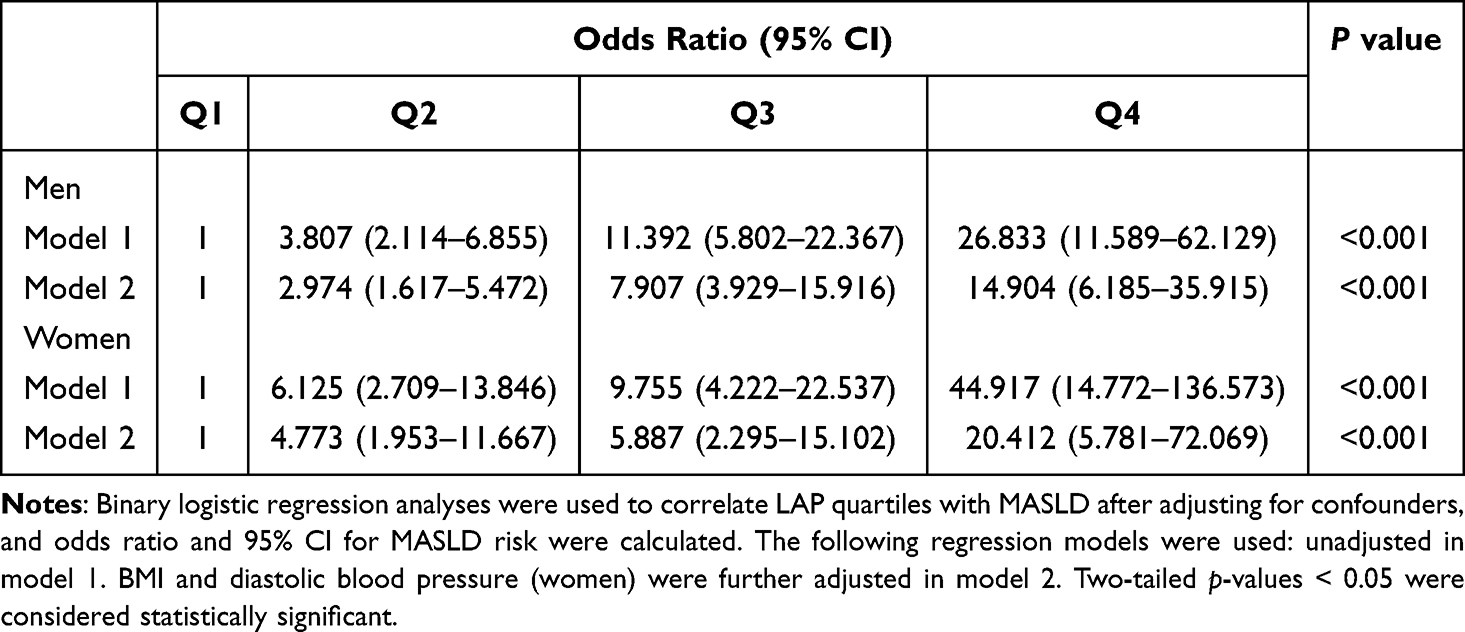 |
Table 2 Multifactorial Analysis of the Relationship Between LAP Quartiles and MASLD |
Diagnostic Value of LAP and Other Visceral Fat-Related Indices in MASLD
ROC curves were plotted to assess the predictive ability of LAP, BMI, WC, WHtR, METS-IR, METS-VF, VAI, ABSI, BRI, and CMI for the occurrence of MASLD in T2DM. The results showed that LAP had a high predictive ability for the occurrence of MASLD in T2DM in both men and women, and was superior to other visceral fat-related indices. In men, the AUC (95% CI) was 0.815 (0.771–0.859) with cut-off value of 36.01, and its sensitivity and specificity were 71.91% and 77.44%, respectively. And in women, the AUC (95% CI) was 0.816 (0.762–0.870) with cut-off value of 24.22, and its sensitivity and specificity were 84.93% and 63.54% (Table 3 and Figures 2, 3).
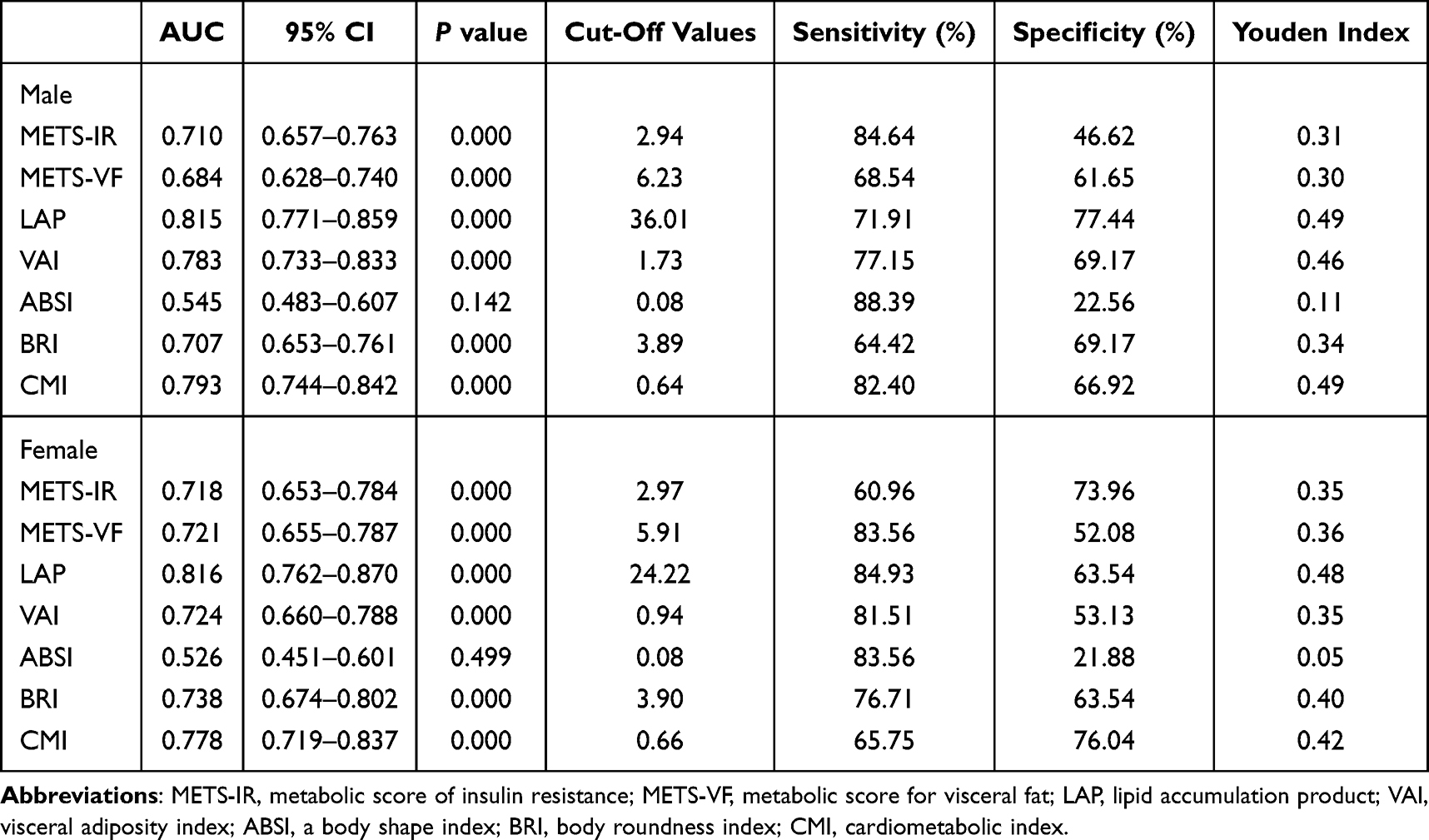 |
Table 3 ROC Curve Analysis of the Predictive Ability of LAP and Other Visceral Fat-Related Indices for the Development of MASLD in T2DM |
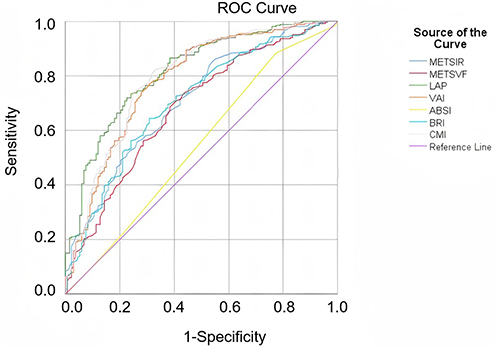 |
Figure 2 Diagnostic value of LAP and other visceral fat-related indices for the diagnosis of MASLD in men analysed using ROC curves. |
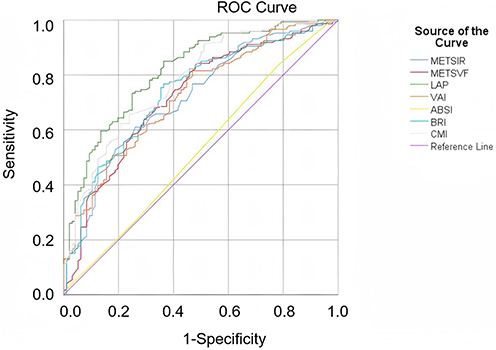 |
Figure 3 Diagnostic value of LAP and other visceral fat-related indices for the diagnosis of MASLD in women analysed using ROC curves. |
Discussion
In this study, we retrospectively analyzed clinical data from 642 patients with T2DM and found that LAP was positively associated with the risk of MASLD in both men and women with T2DM. LAP has a strong predictive ability for T2DM with MASLD and is better than other traditional visceral fat-related indices. The results of this study suggested that LAP can be used as a risk predictor of T2DM complicated with MASLD, which is beneficial to early detection and intervention of MASLD as well as reducing the occurrence and development of T2DM complicated with MASLD.
As is already known, MASLD is associated with T2DM. When T2DM is complicated with MASLD, it will not only increase the risk of diabetes complications but also promote the further progression of MASLD and the vicious cycle. Therefore, earlier screening of MASLD in T2DM patients can delay the progression of the disease and provide more space for clinical treatment. Obesity and the visceral fat-related indices are the most effective indicators for predicting MASLD.30 As mentioned in our introduction, the strong predictive capacity of LAP stems from its integration of two core pathological mechanisms: visceral adipose accumulation (WC) and lipid metabolism dysregulation (TG). The visceral fat-driven hepatic steatosis and lipotoxicity-induced pancreatic β-cell damage represent the shared pathological foundation for the comorbidity of MASLD and T2DM.31,32 Traditional metrics such as BMI solely assess overall obesity and fail to differentiate metabolic status, while composite formulas (eg, VAI) lack stability due to their inclusion of variables like HDL-C, which are prone to confounding factors. This advantage has been validated in recent years: multiple studies confirm that LAP demonstrates superior diagnostic accuracy for MetS compared to BMI, WC, and WHtR.33,34 A cross-sectional study35 further revealed that VAI exhibits the lowest diagnostic efficacy for MASLD, as its formula includes HDL-C, which shows high variability in MASLD patients. Additionally, ABSI was primarily developed using data from Western populations, limiting its applicability.36 Studies have found that LAP is significantly correlated with the onset and severity of MASLD and has high diagnostic accuracy in identifying MASLD in the general population.13 Also, a systematic review and meta-analysis synthesized sixteen observational studies with 96,101 participants, including four cohort studies, one case-control study, and 11 cross-sectional studies with baseline data. The LAP index was compared in subjects with and without MASLD, and the difference was significant with 34.90 units (95% CI: 30.59–39.31, P< 0.001) of the LAP index. The DTA meta-analysis was conducted and showed that the LAP index pooled sensitivity and specificity for screening for MASLD were 94% (95% CI: 72%–99%, P < 0.001) and 85% (95% CI: 62%–96%, P < 0.001), respectively. This study showed that the LAP is an inexpensive, sensitive, and specific method to evaluate MASLD and may be valuable for MASLD screening.6 By far, the pathogenesis of T2DM complicated with MASLD is still unclear and may be related to many factors such as lipotoxic reactions, oxidative stress reactions, intestinal flora imbalances, and IR.37 In addition, T2DM is an important risk factor for MASLD and the most important clinical predictor of adverse clinical outcomes such as advanced liver fibrosis and mortality.2 Although existing studies have found a significant association between LAP and MASLD, the association between LAP and the incidence of MASLD associated with T2DM remains unclear. Dai et al found that LAP showed high diagnostic accuracy in identifying MASLD in adults. The identified cut-off values for LAP in men and women were 30.5 (sensitivity: 77%, specificity: 75%) and 23.0 (sensitivity: 82%, specificity: 79%), respectively. In addition, the diagnostic accuracy of LAP was found to be particularly high in younger age groups.13 Our study showed that in T2DM patients with MASLD, the cut-off value of LAP in male patients was 36.01, and its sensitivity and specificity were 71.91% and 77.44%. The cut-off value of LAP in female patients was 24.22, and its sensitivity and specificity were 84.93% and 63.54%, respectively. While the observed sex-specific differences may be attributed to variations in adipose tissue distribution patterns, the precise mechanisms underlying these disparities remain to be fully elucidated. We speculate that the differences in sensitivity and specificity between sexes may stem from variations in fat distribution: females have a higher proportion of subcutaneous fat, whereas males exhibit more prominent visceral adipose tissue (VAT), a critical fat depot driving IR and metabolic abnormalities.36 Since LAP is based on WC, a marker of visceral fat, it may demonstrate greater sensitivity in males. Additionally, the sharp decline in estrogen levels post-menopause triggers a redistribution of adipose tissue to the abdominal region.38 This age-related estrogen deficiency exacerbates metabolic risks,36 which are closely linked to increased IR, cardiovascular diseases, and MASLD.39 Compared with Dai et al’s study, we further demonstrated the predictive ability of LAP for T2DM complicated with MASLD and revealed that the detection rate of MASLD in males and females would gradually increase with the increase in LAP value.
Strengths and Limitations
A strength of our study is that it was conducted in a large population of representative Chinese adults, which provided high statistical power for data analyses. However, some limitations should also be noted. Firstly, we only collected baseline data on LAP, so the effect of dynamic changes in LAP in T2DM with MASLD is unclear. Secondly, our study was a single-center retrospective cohort design, and it was impossible to draw conclusions about a causal association between LAP and T2DM combined with the risk of MASLD. Finally, the gold standard for diagnosing MASLD is liver biopsy, not abdominal ultrasound, so the detection rate of MASLD may be underestimated to a certain extent, resulting in some error in the results. To compensate for these limitations, future research must focus on standardized and confirmatory studies, which will provide more reliable cut-off values that make LAP a more universally applicable predictive marker.
Conclusions
LAP has a high predictive ability for T2DM with MASLD and can provide new insights for the prevention and diagnosis of T2DM with MASLD in the future.
Abbreviations
MASLD, metabolic dysfunction-associated steatotic liver disease; T2DM, type 2 diabetes mellitus; ROC, receiver operating characteristic; AUC, area under curve; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; 2hPG, 2-hour postprandial blood glucose; HbA1c, hemoglobin A1c; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; ALT, alanine transaminase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; ALP, alkaline phosphatase; SCr, serum creatinine; BUN, blood urea nitrogen; UA, uric acid; BMI, body mass index; WC, waist circumference; WHtR, waist-to-height ratio; METS-IR, metabolic score of insulin resistance; METS-VF, metabolic score for visceral fat; LAP, lipid accumulation product; VAI, visceral adiposity index; ABSI, a body shape index; BRI, body roundness index; CMI, cardiometabolic index; HIS, hepatic steatosis index; FLI, fatty liver index; IR, insulin resistance; MetS, metabolic syndrome; FFA, free fatty acids; VAT, visceral adipose tissue.
Ethics Approval and Consent to Participants
This retrospective study was performed in accordance with the Declaration of Helsinki and approved by the Clinical Ethics Committee of Affiliated Hospital of Integrated Traditional Chinese and Western Medicine, Nanjing University of Chinese Medicine (2021-LWXY-006-02). All patients signed an informed consent form and their rights were protected.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Development Plan Project of Jiangsu Provincial Bureau of Traditional Chinese Medicine (ZT202207 to LC and MS2022029 to XC), as well as the Nature Science Foundation of Nanjing University of Chinese Medicine (XZR2023050 to HJ).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Magliano DJ, Boyko EJ. IDF Diabetes Atlas 11th Edition. Available from: https://diabetesatlas.org/resources/idf-diabetes-atlas-2025/.
2. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
3. Mari L, Lazzer S, Gatti A, et al. Visceral adiposity, anthropometric and liver function indexes for identifying Metabolic Dysfunction Associated Steatotic Liver Disease (MASLD) in adolescents with obesity: which performs better? J Clin Med. 2025;14(6). doi:10.3390/jcm14062085
4. Saberian A, Dehghan A, Homayounfar R, et al. Determining the sensitivity and specificity of the calculated fatty liver index in comparison with ultrasound. BMC Gastroenterol. 2024;24(1):443. doi:10.1186/s12876-024-03535-x
5. Zeng T, Li F, Yang M, et al. Feasibility of serum galectin-1 as a diagnostic biomarker for metabolic dysfunction-associated steatotic liver disease: a study on a segment of the Chinese population using convenience sampling. Biomedicines. 2025;13(2). doi:10.3390/biomedicines13020425
6. Ebrahimi M, Seyedi SA, Nabipoorashrafi SA, et al. Lipid accumulation product (LAP) index for the diagnosis of nonalcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis. Lipids Health Dis. 2023;22(1):41. doi:10.1186/s12944-023-01802-6
7. Palma R, Pronio A, Romeo M, et al. The role of insulin resistance in fueling NAFLD pathogenesis: from molecular mechanisms to clinical implications. J Clin Med. 2022;11(13). doi:10.3390/jcm11133649
8. Fujii H, Kawada N; Japan Study Group of N. The role of insulin resistance and diabetes in nonalcoholic fatty liver disease. Int J Mol Sci. 2020;21(11):3863. doi:10.3390/ijms21113863
9. Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021;397(10290):2212–2224. doi:10.1016/s0140-6736(20)32511-3
10. Zorena K, Jachimowicz-Duda O, Ślęzak D, Robakowska M, Mrugacz M. Adipokines and obesity. Potential link to metabolic disorders and chronic complications. Int J Mol Sci. 2020;21(10). doi:10.3390/ijms21103570
11. Antraco VJ, Hirata BKS, de Jesus Simão J, et al. Omega-3 polyunsaturated fatty acids prevent Nonalcoholic Steatohepatitis (NASH) and stimulate adipogenesis. Nutrients. 2021;13(2):622. doi:10.3390/nu13020622
12. Kobyliak N, Falalyeyeva T, Bodnar P, Beregova T. Probiotics supplemented with omega-3 fatty acids are more effective for hepatic steatosis reduction in an animal model of obesity. Probiotics Antimicrob Proteins. 2017;9(2):123–130. doi:10.1007/s12602-016-9230-1
13. Dai H, Wang W, Chen R, Chen Z, Lu Y, Yuan H. Lipid accumulation product is a powerful tool to predict non-alcoholic fatty liver disease in Chinese adults. Nutr Metab. 2017;14:49. doi:10.1186/s12986-017-0206-2
14. Özcabı B, Demirhan S, Akyol M, Öztürkmen Akay H, Güven A. Lipid accumulation product is a predictor of nonalcoholic fatty liver disease in childhood obesity. Korean J Pediatr. 2019;62(12):450–455. doi:10.3345/kjp.2019.00248
15. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(sici)1096-9136(199807)15:7<539::Aid-dia668>3.0.Co;2-s
16. Yoo EG. Waist-to-height ratio as a screening tool for obesity and cardiometabolic risk. Korean J Pediatr. 2016;59(11):425–431. doi:10.3345/kjp.2016.59.11.425
17. Khoury M, Manlhiot C, McCrindle BW. Role of the waist/height ratio in the cardiometabolic risk assessment of children classified by body mass index. J Am Coll Cardiol. 2013;62(8):742–751. doi:10.1016/j.jacc.2013.01.026
18. Li H, Tan H, OuYang Z, et al. Association between METS-IR and female infertility: a cross-sectional study of NHANES 2013–2018. Front Nutr. 2025;12:1549525. doi:10.3389/fnut.2025.1549525
19. Bello-Chavolla OY, Almeda-Valdes P, Gomez-Velasco D, et al. METS-IR, a novel score to evaluate insulin sensitivity, is predictive of visceral adiposity and incident type 2 diabetes. Eur J Endocrinol. 2018;178(5):533–544. doi:10.1530/eje-17-0883
20. Ji L, Jiang W, Huang J, et al. Association of Metabolic Score for Visceral Fat (METS-VF) with gout risk in patients with hypertension and hyperuricemia: a multicenter study based on the Chinese population. Diabetes Metab Syndr Obes. 2025;18:761–779. doi:10.2147/dmso.S502675
21. Bello-Chavolla OY, Antonio-Villa NE, Vargas-Vázquez A, et al. Metabolic Score for Visceral Fat (METS-VF), a novel estimator of intra-abdominal fat content and cardio-metabolic health. Clin Nutr. 2020;39(5):1613–1621. doi:10.1016/j.clnu.2019.07.012
22. Ma N, Cui XN, Wang N. The predictive value of triglyceride-glucose index, lipid accumulation product and lipid ratio on metabolic syndrome in polycystic ovary syndrome patients. J Obstet Gynaecol Res. 2025;51(4):e16283. doi:10.1111/jog.16283
23. Kahn HS. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: a population-based comparison. BMC Cardiovasc Disord. 2005;5:26. doi:10.1186/1471-2261-5-26
24. Huang L, Liao J, Lu C, Yin Y, Ma Y, Wen Y. The non-linear relationship between the visceral adiposity index and the risk of prediabetes and diabetes. Front Endocrinol. 2025;16:1407873. doi:10.3389/fendo.2025.1407873
25. Amato MC, Giordano C, Galia M, et al. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33(4):920–922. doi:10.2337/dc09-1825
26. Krakauer NY, Krakauer JC. A new body shape index predicts mortality hazard independently of body mass index. PLoS One. 2012;7(7):e39504. doi:10.1371/journal.pone.0039504
27. Thomas DM, Bredlau C, Bosy-Westphal A, et al. Relationships between body roundness with body fat and visceral adipose tissue emerging from a new geometrical model. Obesity. 2013;21(11):2264–2271. doi:10.1002/oby.20408
28. Wakabayashi I, Daimon T. The “cardiometabolic index” as a new marker determined by adiposity and blood lipids for discrimination of diabetes mellitus. Clin Chim Acta. 2015;438:274–278. doi:10.1016/j.cca.2014.08.042
29. Guidelines for the prevention and treatment of metabolic dysfunction-associated (non-alcoholic) fatty liver disease (Version 2024). Zhonghua Gan Zang Bing Za Zhi. 2024; 32(5): 418–34. doi:10.3760/cma.j.cn501113-20240327-00163
30. Sheng G, Lu S, Xie Q, Peng N, Kuang M, Zou Y. The usefulness of obesity and lipid-related indices to predict the presence of Non-alcoholic fatty liver disease. Lipids Health Dis. 2021;20(1):134. doi:10.1186/s12944-021-01561-2
31. Samuel VT, Shulman GI. Nonalcoholic fatty liver disease as a nexus of metabolic and hepatic diseases. Cell Metab. 2018;27(1):22–41. doi:10.1016/j.cmet.2017.08.002
32. Targher G, Corey KE, Byrne CD, Roden M. The complex link between NAFLD and type 2 diabetes mellitus - mechanisms and treatments. Nat Rev Gastroenterol Hepatol. 2021;18(9):599–612. doi:10.1038/s41575-021-00448-y
33. Nascimento-Ferreira MV, Rendo-Urteaga T, Vilanova-Campelo RC, et al. The lipid accumulation product is a powerful tool to predict metabolic syndrome in undiagnosed Brazilian adults. Clin Nutr. 2017;36(6):1693–1700. doi:10.1016/j.clnu.2016.12.020
34. Karatas S, Beysel S. Visceral adiposity index, triglyceride/high-density lipoprotein ratio, and lipid accumulation product index to discriminate metabolic syndrome among adult type 1 diabetes patients. Metab Syndr Relat Disord. 2021;19(9):507–512. doi:10.1089/met.2021.0047
35. Vassilatou E, Lafoyianni S, Vassiliadi DA, et al. Visceral adiposity index for the diagnosis of nonalcoholic fatty liver disease in premenopausal women with and without polycystic ovary syndrome. Maturitas. 2018;116:1–7. doi:10.1016/j.maturitas.2018.06.013
36. Chiu T-H, Huang Y-C, Chiu H, et al. Comparison of various obesity-related indices for identification of metabolic syndrome: a population-based study from Taiwan biobank. Diagnostics. 2020;10(12):1081. doi:10.3390/diagnostics10121081
37. Tanase DM, Gosav EM, Costea CF, et al. The intricate relationship between Type 2 Diabetes Mellitus (T2DM), Insulin Resistance (IR), and Nonalcoholic Fatty Liver Disease (NAFLD). J Diabetes Res. 2020;2020:3920196. doi:10.1155/2020/3920196
38. Lonardo A, Nascimbeni F, Ballestri S, et al. Sex differences in nonalcoholic fatty liver disease: state of the art and identification of research gaps. Hepatology. 2019;70(4):1457–1469. doi:10.1002/hep.30626
39. Liu Y, Wang W. Sex-specific contribution of lipid accumulation product and cardiometabolic index in the identification of nonalcoholic fatty liver disease among Chinese adults. Lipids Health Dis. 2022;21(1):8. doi:10.1186/s12944-021-01617-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.