Back to Journals » Risk Management and Healthcare Policy » Volume 16
Correlation Between Cystatin C and the Severity of Cardiac Dysfunction in Patients with Systolic Heart Failure
Authors Ge J, Ji Y, Wang F, Zhou X, Wei J, Qi C
Received 29 August 2023
Accepted for publication 2 November 2023
Published 13 November 2023 Volume 2023:16 Pages 2419—2426
DOI https://doi.org/10.2147/RMHP.S437678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Jiyong Ge,1 Yuan Ji,1 Fangfang Wang,1 Xuejun Zhou,1 Jiazhan Wei,1 Chunjian Qi2
1Department of Cardiology, The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Changzhou, Jiangsu, 213003, People’s Republic of China; 2Oncology Institute, The Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Changzhou, Jiangsu, 213003, People’s Republic of China
Correspondence: Chunjian Qi, Oncology Institute, The Affiliated Changzhou Second People’s Hospital, Nanjing Medical University, Xinglong Alley 29, Changzhou, Jiangsu, 213003, People’s Republic of China, Tel +86 519 88119730, Fax +86 519 88115560, Email [email protected]
Introduction: To investigate the relationship between cystatin C and cardiac dysfunction severity in patients with systolic heart failure.
Methods: We recruited 100 hospitalized patients with systolic heart failure and 100 age-gender-matched controls. The clinical information of each patient was collected. Blood pressure, heart rate, height, and weight were measured, as were serum concentrations of cholesterol, renal function indices, cystatin C, and B-type natriuretic peptide (BNP). Transthoracic echocardiography was performed on each patient.
Results: Cystatin C and other indices of renal function, such as urea nitrogen, creatinine, and uric acid, were significantly elevated in the serum of patients with heart failure and those with more severe cardiac dysfunction. The stepwise regression analyses showed that cystatin C was positively associated with BNP (β = 0.18, P = 0.04, 95% CI: 21.1 ~ 1420.4) and left atrial diameter (LAD) (β = 0.19, P = 0.04, 95% CI: 0.03 ~ 9.21) and was negatively associated with ejection fraction (β = − 0.22, P = 0.023, 95% CI: − 12.4 ~ − 0.93), while creatinine was only positively correlated with BNP (β = 0.23, P = 0.03, 95% CI: 1.11 ~ 20.7). The Receiver Operating Characteristic (ROC) curves demonstrated significantly more severe cardiac dysfunction (NYHA III/IV) in patients with cystatin C ≥ 0.895mg/L (sensitivity was 83.0%, specificity was 80.9%, AUC = 0.893) and creatinine ≥ 91.5μmol/L (sensitivity was 71.7%, specificity was 70.2%, AUC = 0.764).
Conclusion: Cystatin C was significantly correlated with cardiac structure and function in patients with systolic heart failure, and it was more valuable than creatinine to evaluate the severity of heart failure.
Keywords: cystatin C, renal function, systolic heart failure
Introduction
Heart failure (HF) is a global healthcare burden associated with an unacceptable risk of morbidity, rehospitalization, and mortality.1,2 Low cardiac output, accelerated atherosclerosis, inflammation, and increased venous pressure may all contribute to HF-related renal dysfunction and cardiorenal syndrome.3 Renal function provides valuable prognostic information for the classification of patients with stable or decompensated HF.4
Fontan circulation is associated with kidney injury and dysfunction, often unappreciated until Fontan circulatory failure.5 It hypothesized that cystatin C-estimated glomerular filtration rate (eGFR) would identify chronic kidney disease more frequently and that urine kidney injury biomarkers would be higher with declining Fontan physiological features.5
Cystatin C levels were associated with disease severity and prognosis in patients with pre-capillary PH.6 A combination of high cystatin C and advanced WHO-FC identifies patients at particularly high risk of clinical deterioration.6
Cystatin C is a cysteine protease inhibitor generated by all nucleated cells in mammals at a constant rate, in contrast to creatinine, is less influenced by changes in muscle mass.7 Among HF patients, Cystatin C may more accurately reflect directly measured kidney function8 and has demonstrated superior prognostic value when compared with creatinine.9,10 However, the value of serial Cystatin C measurements for the assessment of kidney function during and following HF hospitalization has not been well described.
Due to its potential role in extracellular matrix (ECM) remodeling, it has not only been advocated as a more accurate estimate of glomerular filtration rate (eGFR) than serum creatinine, but it has also been shown to be associated with left ventricular structural and functional parameters.11–13 The level of circulating cystatin C has been introduced as a more sensitive biomarker of early renal impairment14 particularly in patients with normal creatinine levels.15 Previous studies16 have demonstrated a strong association between cystatin C and cardiovascular events such as stroke, myocardial infarction, and cardiovascular mortality in various populations.17,18 However, the benefits of using cystatin C rather than creatinine in patients with heart failure were not well established. Therefore, in the present study, we investigated the relationship between cystatin C and heart failure as reflected by left ventricular structure, left ventricular function, and B-type natriuretic peptide (BNP). We also compared the predictive value of cystatin C to creatinine for the severity of heart failure.
Methods
Study Population
A total of 100 hospitalized patients with decompensated HF who were treated at the Second People’s Hospital of Changzhou were included in this investigation. Participants should have a left ventricular ejection fraction (LVEF) < 50%, while the exclusion criteria include organic mitral regurgitation, severe renal or liver dysfunction, autoimmune disease, cancer, or any other condition believed to influence the results of the study. The decompensation stage of renal function (Glomerular Filtration Rate < 30mL/min·1.73m2) according to the Kidney Disease Outcomes Quality Initiative (K/DOQI) clinical practice guidelines.19 These patients were always accompanied with electrolyte disturbance, endocrine disorders or unstable vital signs. Such status would be confounding factors for the statistical analyses. As controls, we recruited 100 patients of the same age and gender without HF. According to the New York Heart Association (NYHA) classification criteria, the HF patients were further subdivided into NYHA I group (n = 7), NYHA II group (n = 40), NYHA III group (n = 37), NYHA IV group (n = 16). We analyzed the data according to the combined NYHA I/II group (n = 47) as a mild cardiac dysfunction group and the combined NYHA III/IV group (n = 53) as a severe cardiac dysfunction group. This research adhered to the Declaration of Helsinki. The Ethics Committee of the Second People’s Hospital in Changzhou authorized the protocol. Each participant gave their informed consent and signed it.
We collected data on the patients’ medical history, smoking habits, alcohol consumption, and use of medications with diuretics, angiotensin-converting enzyme inhibitor/angiotensin receptor blockers, calcium channel blockers, and β-blockers. After each patient rested in a seated position for at least 5 minutes, their blood pressure was measured using a mercury sphygmomanometer by trained examiners. The weight and height of the patients were measured while they wore light indoor clothing without shoes. The body mass index (BMI) of the patients was determined by dividing their weight in kilograms by their height in meters squared (kg/m2).
Measurement of Serum Biomarkers
After an overnight fast, venous blood was collected. We determined the levels of serum urea nitrogen, serum creatinine, serum cystatin C, serum triglycerides, serum total cholesterol, and serum high-density lipoprotein (HDL) cholesterol using an automated enzymatic method (Chemistry Analyzer AU2700, Olympus Medical Engineering Company, Tokyo, Japan). Using the Friedewald formula, the serum low-density lipoprotein (LDL) cholesterol concentration was determined.
Transthoracic Echocardiography
A trained and certified echocardiographer performed 2D transthoracic echocardiography, including continuous and pulse-wave Doppler measurements (Sonos 7500 echocardiography system, Philips Medical Systems, Andover, MA, USA), in accordance with standard operating procedures. Indices of left atrial diameter (LAD), left ventricular end systolic diameter (LVSD), left ventricular end diastolic diameter (LVDD), and ejection fraction (EF) were calculated.
Statistical Analysis
We used SPSS 16.0 for database management and statistical analysis. The continuous variables and categorical variables are presented as the mean ± standard deviation, and proportions, respectively. The t-test and the chi-square test were used to compare the means and proportions, respectively. The factors associated with BNP and the indices of heart structure and function, including LAD, LVDD, LVSD, and ejection fraction, were determined using stepwise regression analyses. Finally, we used the receiver operating characteristic (ROC) curve to test the predicted value of cystatin C and creatinine in relation to the severity of heart failure. P < 0.05 was considered statistically significant.
Results
Clinical Characteristics Between Heart Failure Group and Control Group
Table 1 compares the baseline clinical characteristics of the heart failure and control groups. The rate of medications (P = 0.02), concentration of urea nitrogen (P < 0.0001), creatinine (P < 0.0001), uric acid (P < 0.0001), cystatin C (P < 0.0001), BNP (P < 0.0001), LAD (P < 0.0001), LVSD (P < 0.0001), and LVDD (P < 0.0001) were significantly increased in the heart failure group than in the control group, while the EF was lower in the heart failure group (P <0.0001). Age, sex, smoking habit, alcohol consumption, systolic blood pressure, diastolic blood pressure, heart rate, body mass index, total cholesterol, triglycerides, HDL cholesterol, and LDL cholesterol did not differ significantly between the two groups (P > 0.05).
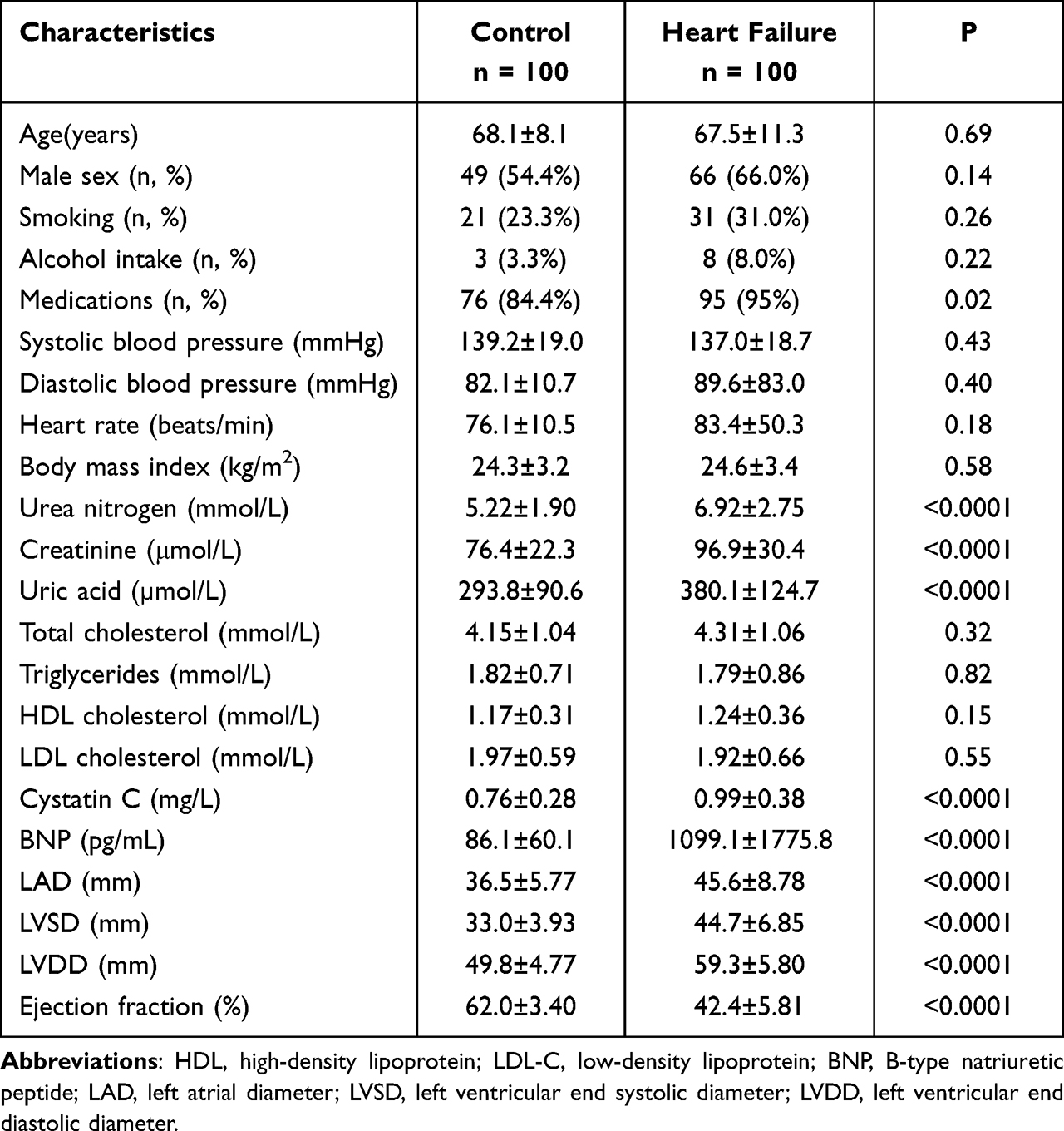 |
Table 1 Clinical Characteristics Between Heart Failure Group and Control Group |
Clinical Characteristics Between Different NYHA Groups (NYHA I/II Group vs NYHA III/IV Group)
Table 2 compares the clinical characteristics between the NYHA I/II group and the NYHA III/IV group. The concentration of urea nitrogen (P = 0.003), creatinine (P < 0.0001), uric acid (P = 0.01), cystatin C (P < 0.0001), BNP (P < 0.0001), left atrial diameter (P = 0.001), left ventricular end systolic diameter (P < 0.0001) and left ventricular end diastolic diameter (P < 0.0001) were significantly higher in NYHA III/IV group than that in NYHA I/II group, while body mass index (P = 0.03) and ejection fraction (P < 0.0001) were significantly decreased in NYHA III/IV group. Age, sex, smoking habit, alcohol consumption, medications, systolic blood pressure, diastolic blood pressure, heart rate, total cholesterol, triglycerides, HDL cholesterol, and LDL cholesterol were not significantly different between the two groups (P > 0.05).
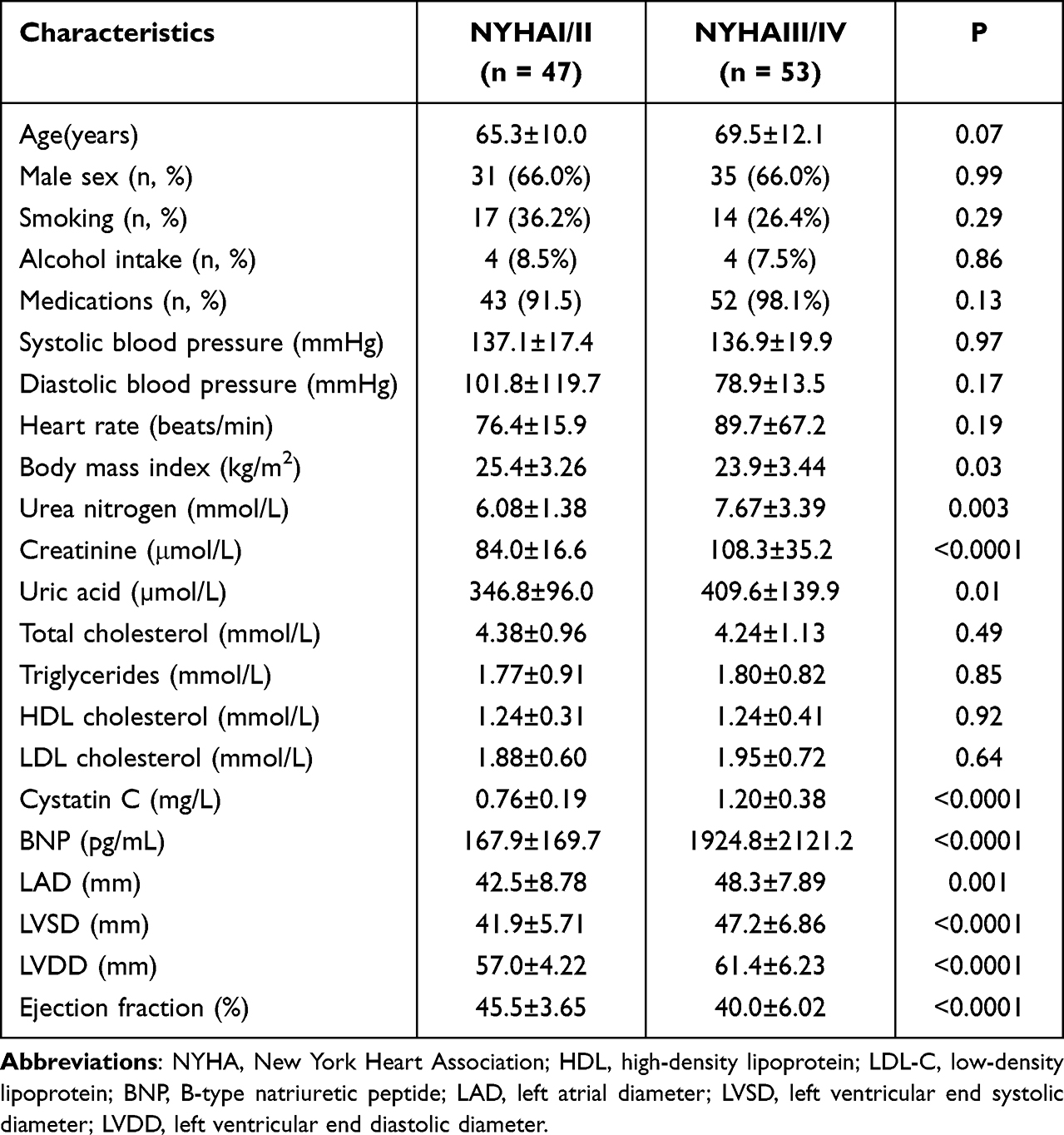 |
Table 2 Clinical Characteristics Between Different NYHA Groups |
Stepwise Regression Analyses in a Group of Heart Failure
Stepwise regression analyses were used to analyze the influence of BNP, LAD, LVDD, LVSD, and ejection fraction on the group with heart failure. As independent variables, Table 3 included age, sex, smoking habit, alcohol consumption, medication, systolic blood pressure, diastolic blood pressure, heart rate, body mass index, urea nitrogen, uric acid, total cholesterol, triglycerides, high-density lipoprotein, low-density lipoprotein, and cystatin C. The results showed that cystatin C was positively associated with BNP (β = 0.18, P = 0.04, 95% CI: 21.1 ~ 1420.4) and LAD (β = 0.19, P = 0.04, 95% CI: 0.03 ~ 9.21) and was negatively associated with ejection fraction (β = −0.22, P = 0.023, 95% CI: −12.4 ~ −0.93), while creatinine was only positively correlated with BNP (β = 0.23, P = 0.03, 95% CI: 1.11 ~ 20.7). Higher levels of BNP (β = 0.20, P = 0.009, 95% CI: 151.1 ~ 1063.5) and lower levels of ejection fraction (β = −0.17, P = 0.034, 95% CI: −7.82 ~ −0.32) were associated with smoking. Female gender was associated with greater LAD (β = −0.18, P = 0.04, 95% CI: −6.20 ~ −0.15). The serum concentration of uric acid was positively correlated with LAD (β = 0.29, P = 0.001, 95% CI: 0.01 ~ 0.04) and was negatively correlated with EF (β = −0.19, P = 0.036, 95% CI: −0.03 ~ −0.001). None of these independent variables was associated with the values of LVDD and LVSD (P > 0.05).
 |
Table 3 Stepwise Regression Analyses in Group of Heart Failure |
The ROC Curves of Cystatin C and Creatinine Were Correlated with the Severity of Cardiac Dysfunction
The ROC curves revealed significantly more severe cardiac dysfunction (NYHA III/IV) in patients with cystatin C ≥ 0.895mg/L (sensitivity was 83.0%, specificity was 80.9%, AUC = 0.893, Figure 1) and creatinine ≥ 91.5μmol/L (sensitivity was 71.7%, specificity was 70.2%, AUC = 0.764, Figure 1).
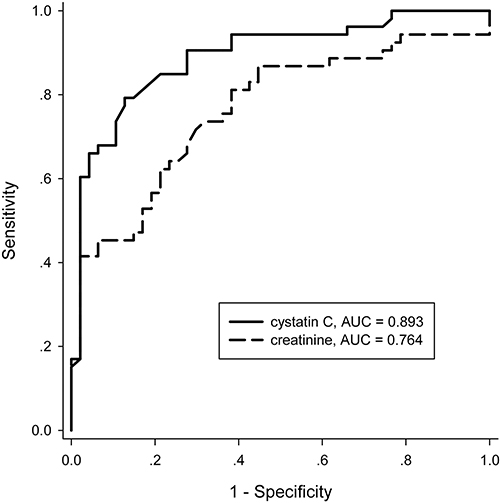 |
Figure 1 ROC curves of cystatin C and creatinine for predicting the severity of heart failure. For cystatin C, the cut-off point was 0.895 mg/L, the sensitivity was 83.0%, and the specificity was 80.9%; the area under the curve (AUC) was 0.893; For creatinine, the cut-off point was 91.5 μmol/L, the sensitivity was 71.7%, and the specificity was 70.2%; and the AUC was 0.764. |
Discussion
Serum concentrations of cystatin C and other indices of renal function such as urea nitrogen, creatinine, and uric acid were significantly higher in patients with heart failure and those with more severe cardiac dysfunction, according to the findings of this study. The stepwise regression analyses demonstrated that levels of cystatin C, creatinine, and uric acid were associated with indices of cardiac structure and function as well as values of BNP. According to the ROC curves, evaluating the severity of heart failure with cystatin C was more advantageous than with creatinine.
Cardiorenal syndrome refers to a spectrum of cardiac and kidney disorders. The initial renal hemodynamic response to chronic heart failure is low renal plasma flow and relative preservation of the glomerular filtration rate (GFR), resulting in an increased filtration fraction. An increase in efferent arteriolar resistance and glomerular capillary hydrostatic pressure preserves GFR until cardiac function is severely compromised.20 In the present study, indices of renal function, including cystatin C, creatinine, and uric acid, were found to be correlated with the severity of heart failure; furthermore, the stepwise regression analyses demonstrated that these indices were independently associated with BNP, LAD, and EF. Elevated central venous pressures (CVPs) associated with chronic heart failure can typically lead to renal venous hypertension, increased renal resistance, and ultimately impaired intrarenal blood flow, as demonstrated in a number of recent studies utilizing invasive hemodynamic monitoring in patients with acute HF.21,22 In addition to these changes in the kidney, sodium reabsorption in the loop of Henle was enhanced, and multiple neurohormonal factors, such as the sympathetic nervous system (SNS) and the renin-angiotensin-aldosterone system (RAAS), were activated, resulting in the formation of a vicious cycle.23
Cystatin C is a 13-kDa cysteine protease that is found in all nucleated cells, produced at a constant rate, easily filtered, completely reabsorbed, and not secreted by renal tubules. In contrast to plasma creatinine, the levels of cystatin C have not been shown to be influenced by diet, gender, body muscle mass,24 inflammation, or malignancy.25 The Dallas heart study26 also demonstrated a correlation between higher levels of cystatin C, left ventricular hypertrophy, and increased left ventricular mass as determined by magnetic resonance imaging (MRI). In a subset of patients with chronic HF from the Cardiovascular Health Study, the highest quartile of serum cystatin C was associated with twice the risk of cardiovascular mortality adjusted for baseline characteristics.27 In patients presenting with acute HF, serum cystatin C was a strong indicator of rehospitalization and mortality28,29 and also had additive prognostic value for HF.30 Consistent with these results, the present study revealed that the levels of cystatin C were significantly correlated with the severity of heart failure and were associated with BNP, LAD, and EF independently of creatinine in the stepwise regression analyses. Furthermore, the ROC curves indicated that cystatin C may be a more sensitive index for evaluating the severity of cardiac function than creatinine in patients with HF and normal or slightly impaired renal function; when the levels of cystatin C ≥ 0.895mg/L, the sensitivity of having more severe cardiac function was 83.0% and the specificity was 80.9%.
Our current research must be interpreted within the context of its limitations. The small sample size from a single center is a significant limitation of our investigation. This was due to the exclusion of patients with additional comorbidities, mainly renal impairment and autoimmune diseases or malignancies, which could have influenced the levels of cystatin C and renal function. Aside from this, our study was cross-sectional, so no causal inferences could be drawn.
Conclusion
Cystatin C is significantly associated with cardiac structure and function in patients with systolic heart failure, and it is more valuable than creatinine in evaluating the severity of heart failure. Furthermore, large sample size from multi-center and prospective studies are required to confirm our findings and clarify the underlying mechanisms of this relationship.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
The study was supported by grants from Changzhou Health Bureau (ZD202216).
Disclosure
The authors declare that they have no competing interests.
References
1. Butrous H, Hummel SL. Heart failure in older adults. Can J Cardiol. 2016;32(2):1140–1147. doi:10.1016/j.cjca.2016.05.005
2. Wang K, Tian J, Zheng C, et al. Improving risk identification of adverse outcomes in chronic heart failure using SMOTE+ENN and machine learning. Risk Manag Healthc Policy. 2021;14:2453–2463. doi:10.2147/RMHP.S310295
3. Cole RT, Masoumi A, Triposkiadis F, et al. Renal dysfunction in heart failure. Med Clin North Am. 2012;96(5):955–974. doi:10.1016/j.mcna.2012.07.005
4. Dini FL, Simioniuc A, Carluccio E, et al. Echo and BNP serial assessment in ambulatory heart failure care: data on loop diuretic use and renal function. Data Brief. 2016;9:1074–1076. doi:10.1016/j.dib.2016.11.009
5. Katz DA, Gao Z, Freytag J, et al. Associations between characteristics of individuals with Fontan circulation with blood and urine biomarkers of kidney injury and dysfunction. J Am Heart Assoc. 2023;12(13):e029130. doi:10.1161/JAHA.122.029130
6. Duan A, Huang Z, Zhao Z, et al. The potential of cystatin C as a predictive biomarker in pulmonary hypertension. BMC Pulm Med. 2023;23(1):311. doi:10.1186/s12890-023-02595-1
7. Chen CT, Chang LY, Chuang CW, et al. Optimal measuring timing of cystatin C for early detection of contrast-induced acute kidney injury: a systematic review and meta-analysis. Toxicol Lett. 2020;318:65–73. doi:10.1016/j.toxlet.2019.10.011
8. Kervella D, Lemoine S, Sens F, et al. Cystatin C versus creatinine for GFR estimation in CKD due to heart failure. Am J Kidney Dis. 2017;69(2):321–323. doi:10.1053/j.ajkd.2016.09.016
9. Dupont M, Wu Y, Hazen SL, Tang WHW. Cystatin C identifies patients with stable chronic heart fail ure at increased risk for adverse cardiovascular events. Circ Heart Fail. 2012;5(5):602–609. doi:10.1161/CIRCHEARTFAILURE.112.966960
10. Tang WHW, Dupont M, Hernandez AF, et al. Comparative assessment of short-term adverse events in acute heart failure with cystatin C and other estimates of renal function: results from the ASCEND-HF trial. JACC Heart Fail. 2015;3(1):40–49. doi:10.1016/j.jchf.2014.06.014
11. Ferguson TW, Komenda P, Tangri N. Cystatin C as a biomarker for estimating glomerular filtration rate. Curr Opin Nephrol Hypertens. 2015;24(3):295–300. doi:10.1097/MNH.0000000000000115
12. Agarwal S, Thohan V, Shlipak MG, et al. Association between cystatin C and MRI measures of left ventricular structure and function: multi-ethnic study of atherosclerosis. Int J Nephrol. 2011;2011:153868. doi:10.4061/2011/153868
13. Xie L, Terrand J, Xu B, Tsaprailis G, Boyer J, Chen QM. Cystatin C increases in cardiac injury: a role in extracellular matrix protein modulation. Cardiovasc Res. 2010;87(4):628–635. doi:10.1093/cvr/cvq138
14. Kar S, Paglialunga S, Islam R. Cystatin C is a more reliable biomarker for determining eGFR to support drug development studies. J Clin Pharmacol. 2018;58(10):1239–1247. doi:10.1002/jcph.1132
15. Serezlija E, Serdarevic N, Begic L. The estimation of glomerular filtration rate based on the serum cystatin C and creatinine values. Clin Lab. 2017;63(7):1099–1106. doi:10.7754/Clin.Lab.2017.161211
16. Shlipak MG, Matsushita K, Ärnlöv J, et al.; CKD Prognosis Consortium. Cystatin C versus creatinine in determining risk based on kidney function. N Engl J Med. 2013;369(10):932–943. doi:10.1056/NEJMoa1214234
17. Shen G, Zhu H, Ding H, et al. Increased cystatin C Level in ST-elevation myocardial infarction predisposes the prognosis of angioplasty. Am J Med Sci. 2018;355(6):530–536. doi:10.1016/j.amjms.2018.03.003
18. Garcia-Carretero R, Vigil-Medina L, Barquero-Perez O, et al. Cystatin C as a predictor of cardiovascular outcomes in a hypertensive population. J Hum Hypertens. 2017;31(12):801–807. doi:10.1038/jhh.2017.68
19. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266.
20. Ronco C, Bellasi A, Di Lullo L. Cardiorenal syndrome: an overview. Adv Chronic Kidney Dis. 2018;25(5):382–390. doi:10.1053/j.ackd.2018.08.004
21. Mullens W, Abrahams Z, Francis GS, et al. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol. 2009;53(7):589–596. doi:10.1016/j.jacc.2008.05.068
22. Damman K, Navis G, Smilde TD, et al. Decreased cardiac output, venous congestion and the association with renal impairment in patients with cardiac dysfunction. Eur J Heart Fail. 2007;9(9):872–878. doi:10.1016/j.ejheart.2007.05.010
23. Costanzo MR. The cardiorenal syndrome in heart failure. Heart Fail Clin. 2020;16(1):81–97. doi:10.1016/j.hfc.2019.08.010
24. Westhuyzen J. Cystatin C: a promising marker and predictor of impaired renal function. Ann Clin Lab Sci. 2006;36(4):387–394.
25. De Souza V, Hadj-Aissa A, Dolomanova O, et al. Creatinine-versus cystatine C-based equations in assessing the renal function of candidates for liver transplantation with cirrhosis. Hepatology. 2014;59(4):1522–1531. doi:10.1002/hep.26886
26. Patel PC, Ayers CR, Murphy SA, et al. Association of cystatin C with left ventricular structure and function: the Dallas Heart Study. Circ Heart Fail. 2009;2(2):98–104. doi:10.1161/CIRCHEARTFAILURE.108.807271
27. Shlipak MG, Katz R, Fried LF, et al. Cystatin-C and mortality in elderly persons with heart failure. J Am Coll Cardiol. 2005;45(2):268–271. doi:10.1016/j.jacc.2004.09.061
28. Breidthardt T, Sabti Z, Ziller R, et al. Diagnostic and prognostic value of cystatin C in acute heart failure. Clin Biochem. 2017;50(18):1007–1013. doi:10.1016/j.clinbiochem.2017.07.016
29. Kim TH, Kim H, Kim IC. The potential of cystatin-C to evaluate the prognosis of acute heart failure: a comparative study. Acute Card Care. 2015;17(4):72–76. doi:10.1080/17482941.2016.1203440
30. Manzano-Fernández S, Boronat-Garcia M, Albaladejo-Otón MD, et al. Complementary prognostic value of cystatin C, N-terminal pro-B-type natriuretic peptide and cardiac troponin T in patients with acute heart failure. Am J Cardiol. 2009;103(12):1753–1759. doi:10.1016/j.amjcard.2009.02.029
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.