Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Correlation Between CD38+ Cell Levels and Pulmonary Tuberculosis Complicated with Diabetes Mellitus: A Retrospective Analysis Based on Lymphocyte Subsets and Clinical Features
Authors Wang Y ![]() , Mao W, Xu L, Xu W
, Mao W, Xu L, Xu W
Received 30 July 2025
Accepted for publication 24 November 2025
Published 6 December 2025 Volume 2025:18 Pages 4483—4491
DOI https://doi.org/10.2147/DMSO.S556747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hillary Keenan
Yanan Wang, Weifang Mao, Lin Xu, Wenfang Xu
Clinical Laboratory, Affiliated Hospital of Shaoxing University, Shaoxing, Zhejiang, People’s Republic of China
Correspondence: Wenfang Xu, Affiliated Hospital of Shaoxing University, No. 999 Zhongxing South Road, Yuecheng District, Shaoxing, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: This study aimed to investigate the association between CD38+ cells and the risk of pulmonary tuberculosis (PTB) complicated with diabetes mellitus (DM), providing insights into the immune mechanisms underlying PTB-DM.
Patients and Methods: Clinical data and lymphocyte subset profiles of 596 TB patients admitted to Affiliated Hospital of Shaoxing University from November 2022 to November 2024 were analyzed, including 115 DM-complicated and 481 non-DM cases. Logistic regression was used to evaluate the correlations between clinical indicators, lymphocyte subsets and PTB-DM. Generalized linear models were employed to assess the association of CD38+ cells with PTB-DM risk, while restricted cubic spline curves were used to explore potential linear relationships.
Results: The PTB-DM group exhibited a significantly higher prevalence of advanced age, male gender, and hypertension compared to the non-DM group (p < 0.05). Lymphocyte subset analysis revealed marginally elevated NKT cells but reduced B lymphocytes, B1 cells, and CD38+ cells in the DM group, with the most pronounced difference in CD38+ cells (p < 0.001). Multivariate logistic regression identified multidrug-resistant TB and hypertension as independent risk factors, whereas higher CD38+ cell counts served as an independent protective factor for TB-DM comorbidity (OR 0.50, 95% CI 0.32– 0.77). Generalized linear models demonstrated a persistent negative correlation between CD38+ cell levels (analyzed as continuous or quartile-categorized variables) and PTB-DM risk after adjusting for confounders. Restricted cubic spline analysis confirmed a significant linear inverse association (p = 0.003) without evidence of nonlinearity (p = 0.450).
Conclusion: CD38+ cells play a critical role in the immune regulation of PTB patients, with elevated expression conferring protective effects against PTB-DM comorbidity.
Keywords: CD38+ cells, tuberculosis, diabetes mellitus, immune regulation
Introduction
Tuberculosis (TB) remains a significant global health emergency, with the World Health Organization (WHO) classifying it returns to top global cause of death from a single infectious disease.1 Pulmonary tuberculosis (PTB) is the most predominant form of TB infection, accounting for 85%.2 The pathogenesis of tuberculosis is closely related to the immune status of the host.3 Meanwhile, diabetes mellitus (DM) has seen a dramatic increase in prevalence globally, contributing to high morbidity and mortality rates.4 The bidirectional relationship between TB and DM is well-established: DM increases the risk of TB infection, while TB infection exacerbates abnormal blood glucose levels, creating a vicious cycle that complicates patient management and outcomes.5,6 The interplay between the two diseases underscores the necessity of elucidating their combined impact on immune status and disease progression.
Immune dysfunction is a central mechanism in the pathogenesis of PTB and DM, and lymphocyte subset analysis provides a practical tool for monitoring immune status.7,8 CD38, a transmembrane glycoprotein, is expressed on various immune cells, including lymphocytes, and is involved in immune activation, cell signaling, and inflammation.9 Studies have shown that CD38+ cells are involved in immune responses and the regulation of inflammatory processes.10 In the studies of TB, CD38+ macrophages were shown to be a key subpopulation controlling Mycobacterium tuberculosis (Mtb) proliferation and its expression on Mtb - specific T cells has diagnostic value.11,12 In type 2 diabetes mellitus (T2DM), the frequency of CD19+CD24+CD38+ regulatory B cells is increased and correlates with impaired β-cell function, insulin resistance and adverse lipid profiles, indicating that elevated CD38 expression reflects metabolic dysregulation.13 However, existing studies have primarily focused on the individual impacts of TB or DM on CD38+ cell levels. How CD38+ cell levels are altered when PTB and DM coexist remains unknown. Crucially, clarifying this gap is essential for developing targeted therapies and improving outcomes in PTB-DM patients.
Given the bidirectional relationship between TB and DM, Our study retrospectively analyzed the clinical features and lymphocyte subsets in patients with TB and DM compared to those with TB alone. According to the statistics result, we focus on the correlation between CD38+ cell levels and disease risk. Identifying CD38+ cell levels as a potential biomarker for TB in patients with DM holds significant clinical importance. In summary, monitoring the immune status of TB and DM can help in timely intervention, improve treatment strategies and enhance patient prognosis. This study aims to inform the development of targeted therapies that modulate the immune response to mitigate the progression of tuberculosis-combined diabetes.
Materials and Methods
Study Population
We conducted a single-center, retrospective study at Affiliated Hospital of Shaoxing University. Between November 2022 and November 2024, 1127 patients admitted to the department of tuberculosis were analyzed for peripheral blood lymphocyte subsets. After applying the exclusion criteria detailed below, 596 patients with a definitive diagnosis of PTB were enrolled. According to the discharge diagnosis, they were divided into: PTB group (n = 481), and PTB-DM group (n = 115).
PTB was diagnosed in accordance with the “Technical guidelines for tuberculosis prevention and control in China”.14 DM was ascertained by documented fasting plasma glucose ≥ 7.0mmol/L, random plasma glucose ≥ 11.1mmol/L, or HbA1c ≥ 6.5%, supported by clinical records of antidiabetic therapy. Patients with any of the following were excluded: (1) primary PTB or extra-pulmonary TB, (2) active systemic autoimmune disease, (3) HIV infection, (4) receipt of immunosuppressive or glucocorticoid therapy within 3 months, (5) lymphocytic leukaemia or (6) incomplete lymphocyte-subset data.
Data Collection
Electronic medical records were reviewed to obtain demographic and clinical variables recorded. Clinical variables collected included age, gender, sputum smear for Mtb, Multidrug-Resistant Tuberculosis (MDR-TB) or not, primary treatment or not and comorbidities (hypertension, malignancy and anaemia). Within 24 h of admission, peripheral blood was collected in EDTA tubes and analyzed by flow cytometry (Beckman Coulter, USA). We quantified 16 parameters: percentage values for CD3+ (total T lymphocyte), CD3+CD4+ (Th/Ti lymphocyte), CD3+CD8+ (Ts/Tc lymphocyte), CD3+CD4−CD8− (double-negative T lymphocyte), CD4+/CD8+ ratio, CD3−CD16+CD56+ (NK cell), CD3+CD16+CD56+ (NKT cells), CD3−CD19+ (total B lymphocyte), CD3−CD19+CD5+ (B1 lymphocyte), CD3−CD19+CD5− (B2 lymphocyte), and CD38+ cells; and absolute counts of total T lymphocytes, Th/Ti lymphocytes, Ts/Tc lymphocytes, NK cells, and total B lymphocytes. The flow cytometry results were also collected and retrieved from electronic medical records.
Statistical Analysis
Baseline characteristics were stratified by the presence or absence of diabetes. Normally distributed continuous variables are reported as mean ± standard deviation (SD) and were compared between groups using the independent-samples t-test. Non-normally distributed continuous variables are expressed as median (Q1, Q3) and were compared with the Mann–Whitney U-test. Categorical variables are presented as n (%) and were analyzed using the χ2-test or Fisher’s exact test, as appropriate. Logistic regression models were constructed to identify independent determinants of PTB-DM. Variables with p < 0.1 in univariable analyses were entered into multivariable analysis, which was performed using bidirectional stepwise selection.
Multivariable generalized linear models (GLMs) with a quasibinomial family and logit link were fitted to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the association between CD38+ cell expression and diabetes among patients with pulmonary tuberculosis. To control for confounding, variables that showed statistical significance (p < 0.05) in univariable analyses were included as covariates in the multivariable models, allowing for potential overdispersion. CD38+ cell level was analyzed both as a continuous variable and after categorisation into quartiles (Q1–Q4). Three models were specified: Model 1 (unadjusted); Model 2 (adjusted for sex, hypertension, and MDR-TB); Model 3 (adjusted for sex, hypertension, MDR-TB, NKT cells, B lymphocytes, and B2 lymphocytes). The same modelling strategy was repeated using CD38+ quartiles, with the lowest quartile (Q1) serving as the reference. A linear trend across quartiles was evaluated by entering the median value of each quartile as a continuous variable in the regression models. We used restricted cubic splines (RCS) to model the shape of the association between CD38+ cell percentage and diabetes. The number of knots was set to three, as this configuration yielded the lowest Akaike information criterion (AIC) within a multivariable logistic model adjusted for sex, hypertension, MDR-TB, NKT, B and B2 cells; deviation from linearity was formally tested. All analyses were performed in R version 4.3.1; a two-sided p < 0.05 was considered statistically significant.
Results
General Characteristics in PTB Patients with or Without DM
Among 596 enrolled participants, 115 (19.3%) were classified as PTB-DM comorbidity (Table 1). Compared with non-DM PTB patients, those with DM were more likely to be male (76.52% vs 64.24%; χ2 = 6.29, p = 0.012) and older (median 66 vs 64 years; Z = –2.05, p = 0.040), and they exhibited a higher prevalence of hypertension (40.00% vs 27.23%; χ2 = 7.24, p = 0.007) and MDR-TB (13.91% vs 7.48%; χ2 = 4.82, p = 0.028). No significant differences were observed between the two groups in sputum smear positivity, primary treatment history, cancer, or anemia (all p > 0.05).
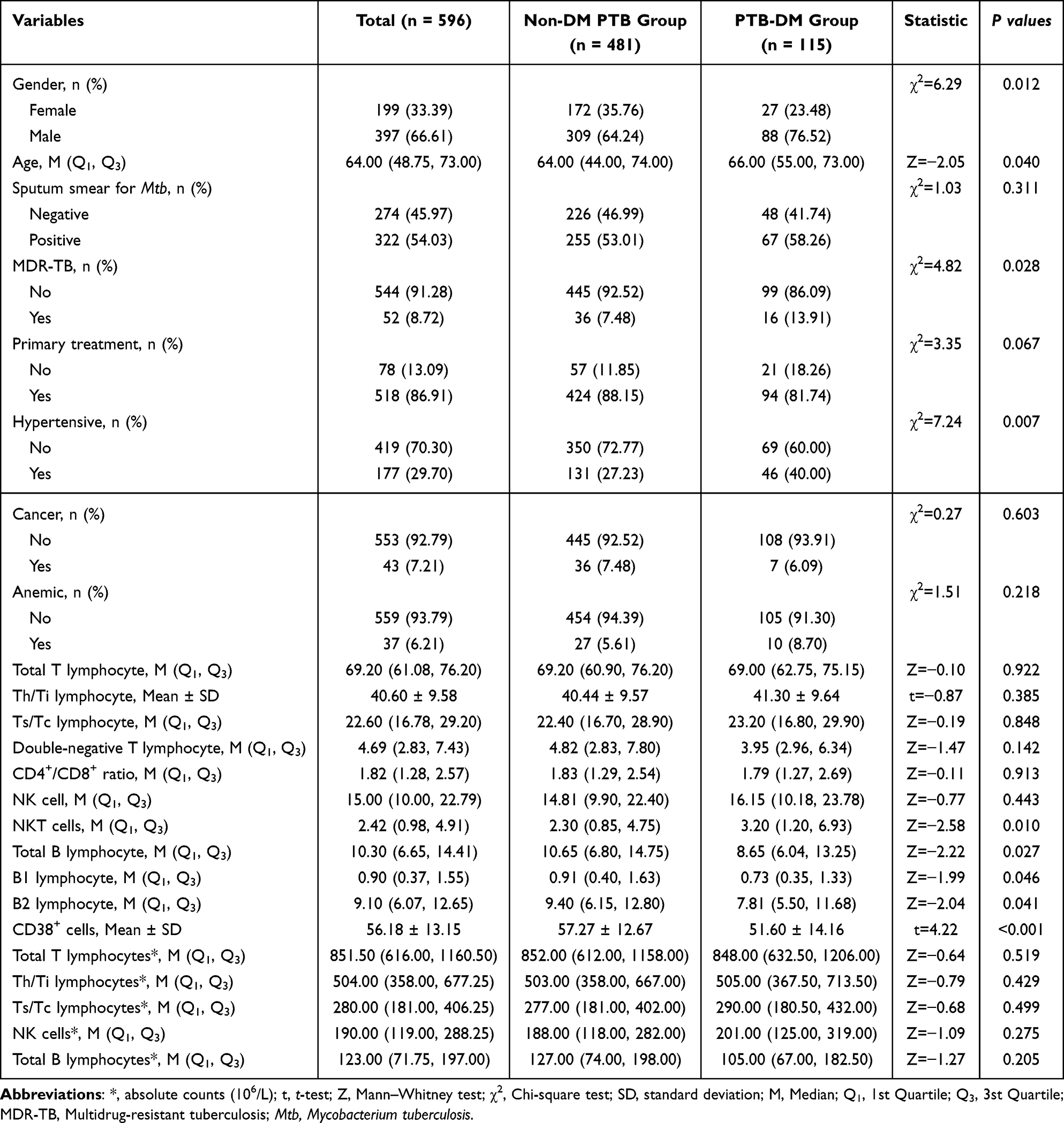 |
Table 1 Baseline Characteristics of PTB Patients with or Without Diabetes Mellitus |
Regarding lymphocyte subsets, absolute counts did not differ between groups. However, relative percentages indicated that PTB-DM patients had lower total B lymphocytes (8.65% vs 10.65%; Z = –2.22, p = 0.027), B1 (0.73% vs 0.91%; Z = –1.99, p = 0.046), and B2 cells (7.81% vs 9.40%; Z = –2.04, p = 0.041), whereas NKT cells were modestly increased (3.20% vs 2.30%; Z = –2.58, p = 0.010). Notably, CD38+ cell percentage was significantly lower in the PTB-DM group (51.60% ± 14.16%) than in the non-DM group (57.27% ± 12.67%; t = 4.22, p < 0.001).
Logistic Regression Analysis of Factors Associated with DM in PTB
Univariate screening identified male sex (OR = 1.81, 95% CI: 1.13–2.90, p = 0.013), hypertension (OR = 1.78, 95% CI: 1.17–2.72, p = 0.008), MDR-TB (OR = 2.00, 95% CI: 1.07–3.74, p = 0.031), NKT cells (OR =1.51, 95% CI: 1.01–2.28, p = 0.049), total B lymphocytes (OR = 0.60, 95% CI: 0.40–0.91, p = 0.016), B2 lymphocytes (OR = 0.63, 95% CI: 0.42–0.95, p = 0.027) and CD38+ cells (OR = 0.48, 95% CI: 0.32–0.74, p < 0.001) as potential determinants (Table 2). These variables, together with Total B lymphocytes absolute counts and primary treatment status (P < 0.10), were consequently entered into a multivariable model constructed by bidirectional stepwise selection. After full adjustment, MDR-TB (OR = 2.03, 95% CI: 1.06–3.88, p = 0.033) and hypertension (OR = 1.56, 95% CI: 1.01–2.41, p = 0.048) emerged as independent risk factors, whereas CD38+ cells retained a strong inverse association (OR = 0.50, 95% CI: 0.32–0.77, p = 0.002).
 |
Table 2 Logistic Regression Analysis of Clinical Characteristics and Lymphocyte Subsets Associated with DM in PTB Patients |
CD38+ Cell Level is Inversely Associated with Diabetes Risk in PTB
CD38+ cell percentage was inversely associated with diabetes in PTB. As showing in Table 3, when CD38+ cells were treated as a continuous variable, each 1-percentage-point increase corresponded to a 3% reduction in the odds of diabetes (OR = 0.97, 95% CI: 0.95–0.99, p < 0.001) after full adjustment for sex, hypertension, MDR-TB, NKT cells, B cells and B2 cells (Model 3). Compared with the lowest quartile (Q1), higher CD38+ cell levels showed lower point estimates for diabetes risk in the fully adjusted model (Model 3): ORs (95% CI) were 0.61 (0.35–1.07) for Q2, 0.42 (0.23–0.77) for Q3, and 0.39 (0.21–0.73) for Q4, with a significant linear trend across quartiles (p for trend = 0.001). The magnitude and direction of the associations were broadly consistent across Models 1–3, indicating that the observed inverse relationship was not materially altered by the additional covariates.
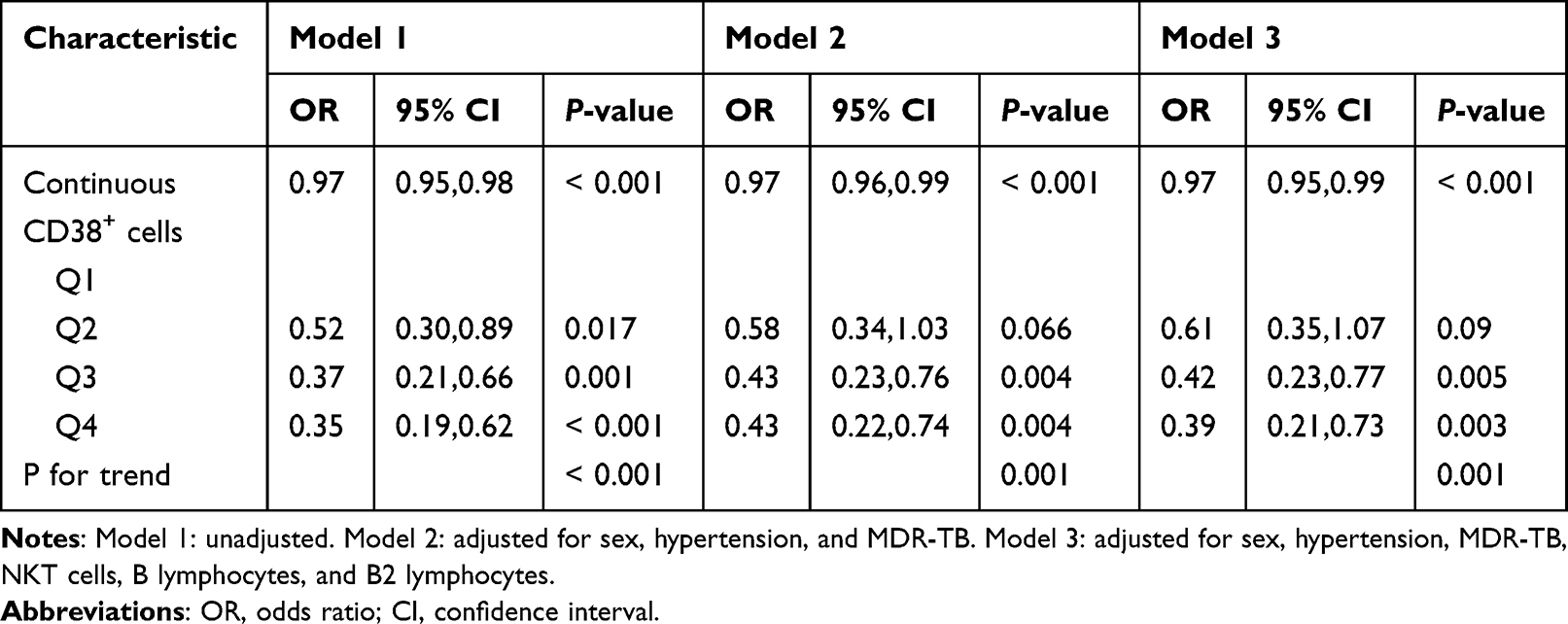 |
Table 3 Association Between CD38+ Cell Level and Diabetes in Patients with Pulmonary Tuberculosis |
Linear Relationship Between CD38+ Cells and Diabetes Risk in PTB
RCS analysis was used to characterize the relationship between CD38+ cell percentage and the risk of diabetes among patients with PTB. After adjustment for sex, hypertension, MDR-TB, NKT cells, total B cells, and B2 cells, the model with three knots yielded the lowest AIC and was therefore selected. As shown in Figure 1, CD38+ cell percentage exhibited a linear inverse association with diabetes risk (p for overall = 0.001), whereas the test for non-linearity was not significant (p for non-linear = 0.451). These findings indicate that the risk of diabetes decreases continuously with increasing CD38+ cell levels, without evidence of a threshold or plateau effect.
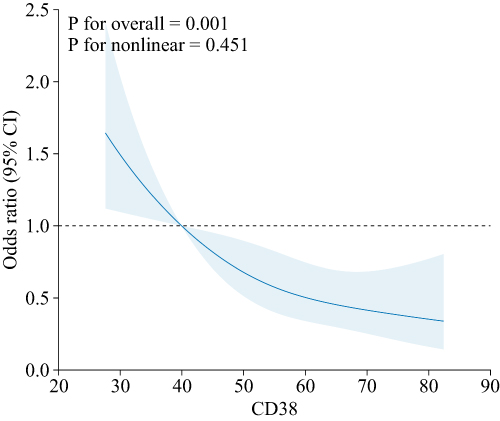 |
Figure 1 Restricted cubic spline depicting the relationship between CD38+ cell percentage and the risk of diabetes in patients with PTB. The solid blue line represents the adjusted odds ratio (OR); the shaded area indicates the 95% confidence interval (CI). The model was adjusted for sex, hypertension, MDR-TB, NKT cells, total B cells, and B2 cells. |
Discussion
Among 596 PTB patients, 115 (19.3%) had co-existing DM. In terms of clinical characteristics and treatment outcomes, PTB patients with DM were more often male, older, hypertensive, and had MDR-TB. They also exhibited lower B-cell subsets and significantly reduced CD38+ cells compared to those without DM. Importantly, CD38+ cell levels in PTB patients with DM were strongly inversely associated with diabetes risk (OR = 0.50, 95% CI: 0.32–0.77, p = 0.002). Our findings suggest that CD38+ cells could serve as a potential biomarker for early screening and personalized treatment strategies for PTB patients with DM, thereby improving their prognosis.
DM increases the risk of tuberculosis disease.15,16 Patients with tuberculosis combined with diabetes are more likely to have poor treatment outcomes than patients with tuberculosis alone.17 In our study, 19.3% of PTB patients already had co-existing diabetes. These individuals were predominantly male, older, and showed higher prevalence of hypertension and MDR-TB, generally consistent with previous reports.16,18 Immune dysfunction is a plausible mechanistic contributor to the pathogenesis of PTB-DM.19,20 Consequently, identifying immune-metabolic predictor for PTB-DM is critical for TB management and control. Previous studies have focused on the inflammatory biomarkers for active tuberculosis risk in diabetic patients.21 Lymphocyte-subset dynamics and clinical phenotypes were characterized in elderly PTB-DM patients. But the detection of lymphocyte types was limited, including only T cells, B cells, and NK cells and their subsets.8 To refine the immunological landscape of PTB-DM, we retrospectively analyzed 16 indicators of lymphocyte subpopulations and leveraged generalized linear models and restricted cubic splines to adjust for confounders. After stepwise adjustment, our multivariable model revealed that male, hypertension, and MDR-TB independently associated with PTB-DM, while CD38+ cell levels emerged as a novel, inverse correlate of diabetes risk.
CD38 is a multifunctional cell surface protein involved in nicotinamide adenine dinucleotide (NAD) metabolism, expressed in a wide range of immune and non-immune cells, and plays an important role in the regulation of immune responses.22 Clinically, CD38 expression on Mtb-specific T cells is markedly higher in active tuberculosis than in asymptomatic contacts or healthy controls, serving as a T-cell activation marker of immunopathology.23 During standard anti-TB therapy, the CD27−CD38− fraction within IFN-γ+CD4+ T cells declines to levels observed in latent infection and healthy donors (AUC = 0.779), indicating its value as a treatment-response biomarker.24 It’s worth noting that CD38− macrophages are the primary infected cells during the initial phase of TB infection. Subsequently, CD38+ alveolar macrophages emerge as potent controllers of Mtb proliferation, and BCG vaccination increases CD38+ cell numbers while enhancing their bacteriostatic capacity.11 Collectively, these findings indicate that elevated CD38+ cells in the early stage of active tuberculosis confer a protective host response against disease progression.
Emerging evidence positions CD38 at the intersection of immunity and metabolism in T2DM. Mendelian-randomisation analyses reveal that elevated IgD+CD38+ B-cell abundance mediates 20.7% of the protective effect conferred by BDH1 against T2DM.25 Mechanistically, in hepatocytes, nuclear CD38 (nCD38) drives glucagon-induced gluconeogenesis by sustaining TRPM2-mediated nuclear Ca2+ signaling after NAD+ loading through PKCδ-phosphorylated connexin 43, thereby enhancing the transcription of G6Pase and PEPCK1.26 In diabetic kidney disease (DKD), CD38 exacerbates renal injury by degrading NAD+, reducing Sirt3 activity, and increasing mitochondrial oxidative stress in renal tubular cells, as demonstrated by the protective effects of the CD38 inhibitor apigenin in both in vivo and in vitro models.27 Similarly, in diabetic cardiomyopathy, CD38 deficiency mitigates cardiac dysfunction and fibrosis by enhancing NAD+/Sirt3/FOXO3a signaling, reducing pyroptosis and apoptosis, as shown in CD38 knockout mice subjected to high-fat diet and streptozotocin.28 Thus, CD38 exerts dual, cell-type- and tissue-specific effects in T2DM: within B-cell subsets it may confer metabolic protection, whereas in cardiomyocytes and renal tubular cells it promotes diabetic complications via NAD+ metabolic dysregulation. We now demonstrate that systemic CD38+ lymphocytes are significantly reduced in PTB–DM (51.6% ± 14.2%) compared with non-DM PTB (57.3% ± 12.7%, t = 4.22, p < 0.001), suggesting that CD38+ cell depletion reflects not only tuberculosis-associated immune exhaustion but also diabetes-driven immune-metabolic dysregulation.
Previous studies have identified elevated ESR and reduced MLR/PLR as inflammatory hallmarks of PTB-DM.29 The present study proposes an immune dimension—insufficient activation of CD38+ cells. Integrating these inflammatory indices with lymphocyte function into a multidimensional panel will allow more accurate identification and management of PTB-DM patients. The CD38+ lymphocyte ratio serves as both a point-of-care screening tool for diabetes in patients with tuberculosis and a dynamic biomarker throughout treatment, with sustained levels below the baseline prompting early intervention.
Our study benefits from a comprehensive 16-colour flow-cytometry panel and rigorous confounder adjustment via GLMs and RCS analyses. Nevertheless, the retrospective design, absence of longitudinal follow-up, and lack of functional assays temper causal inference. Prospective cohorts are now warranted to validate these findings and to track CD38+ cell dynamics across anti-tuberculosis and anti-diabetic treatment trajectories.
Conclusion
In summary, this study compared clinical and lymphocyte-subset profiles between PTB patients with and without concomitant DM. Among 596 PTB patients, 115 (19.3%) had co-existing DM. They were more often male, older, hypertensive and MDR-TB, and displayed lower B-cell subsets and significantly reduced CD38+ cells compared to those without DM. After bidirectional stepwise adjustment, gender, MDR-TB and hypertension independently associated with PTB-DM, while CD38+ cells remained strongly and inversely associated with diabetes risk. Notably, CD38+ cell percentage showed a robust, inverse association with PTB-DM and RCS revealed a linear, inverse relationship between CD38+ cell percentage and PTB-DM risk. Circulating CD38+ lymphocytes serve as a quantifiable nexus of immune-metabolic crosstalk in PTB-DM; their depletion not only flags increased diabetes risk but also offers a mechanistic target for host-directed, immune-metabolic therapy. These findings highlight the potential of CD38+ cells as a biomarker and therapeutic target in the management of PTB-DM comorbidity.
Data Sharing Statement
The raw data of this study are available from the corresponding author or first author upon reasonable request.
Ethics Statement
This retrospective study utilized anonymized data and was approved by the Ethics Committee of the Affiliated Hospital of Shaoxing University, which granted a waiver of informed consent (approval no. 2025-004-01). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We would like to extend our sincere thanks to our colleagues at the clinical laboratory for their collaboration and contributions to this work. Special thanks to Dongfang Zhu and for her technical assistance and insightful discussions, which have significantly enhanced the quality of our research.
Author Contributions
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Yanan Wang: Methodology; Data curation; Formal analysis; Writing – original draft; Funding acquisition.
Weifang Mao: Data curation; Formal analysis; Validation; Writing – review & editing.
Lin Xu: Investigation; Resources; Writing – review & editing.
Wenfang Xu: Conceptualization; Supervision; Project administration; Writing – review & editing.
Funding
This study was supported by the Medical and Health Research Project of Zhejiang Province (Grant No. 2025KY389) and the Medical and Health Program of Shaoxing (Grant No. 2022KY064).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. WHO. Global tuberculosis report 2024. World Health Organization;2024.
2. Afriyie-Mensah JS, Aryee R, Zigah F, Amaning-Kwarteng E, Seraphin MN. The burden of bacteriologically negative TB diagnosis: a four-year review of tuberculosis cases at a tertiary facility. Tuberc Res Treat. 2023;2023:6648137. doi:10.1155/2023/6648137
3. Chandra P, Grigsby SJ, Philips JA. Immune evasion and provocation by mycobacterium tuberculosis. Nat Rev Microbiol. 2022;20(12):750–766. doi:10.1038/s41579-022-00763-4
4. Collaboration NCDRF. Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. 2024;404(10467):2077–2093. doi:10.1016/S0140-6736(24)02317-1
5. Boadu AA, Yeboah-Manu M, Osei-Wusu S, Yeboah-Manu D. Tuberculosis and diabetes mellitus: the complexity of the comorbid interactions. Int J Infect Dis. 2024;146:107140. doi:10.1016/j.ijid.2024.107140
6. Trajman A, Campbell JR, Kunor T, et al. Tuberculosis. Lancet. 2025;405(10481):850–866. doi:10.1016/S0140-6736(24)02479-6
7. Ye Z, Li L, Yang L, et al. Impact of diabetes mellitus on tuberculosis prevention, diagnosis, and treatment from an immunologic perspective. Exploration. 2024;4(5):20230138. doi:10.1002/EXP.20230138
8. Wang X, Song Y, Li N, et al. Elderly patients with tuberculosis combined with diabetes mellitus: a comprehensive analysis of lymphocyte subpopulation dynamics, clinical features, drug resistance and disease regression. Int J Gen Med. 2025;18:1271–1282. doi:10.2147/IJGM.S502996
9. Piedra-Quintero ZL, Wilson Z, Nava P, Guerau-de-Arellano M. CD38: an immunomodulatory molecule in inflammation and autoimmunity. Front Immunol. 2020;11:597959. doi:10.3389/fimmu.2020.597959
10. Zhang X, He T, Wu Z, et al. The role of CD38 in inflammation-induced depression-like behavior and the antidepressant effect of (R)-ketamine. Brain Behav Immun. 2024;115:64–79. doi:10.1016/j.bbi.2023.09.026
11. Pisu D, Johnston L, Mattila JT, Russell DG. The frequency of CD38(+) alveolar macrophages correlates with early control of M. tuberculosis in the murine lung. Nat Commun. 2024;15(1):8522. doi:10.1038/s41467-024-52846-w
12. Hiza H, Hella J, Arbues A, et al. Case-control diagnostic accuracy study of a non-sputum CD38-based TAM-TB test from a single milliliter of blood. Sci Rep. 2021;11(1):13190. doi:10.1038/s41598-021-92596-z
13. Mendez-Frausto G, Romero-Aguilera G, Sanchez-Gutierrez R, et al. B regulatory cells associated with changes in biochemical and inflammatory parameters in normal-glycemic individuals, pre-diabetes and T2DM patients. Diabet Res Clin Pract. 2021;173:108692. doi:10.1016/j.diabres.2021.108692
14. Zhao YL, C MT. Technical Guidelines for Tuberculosis Prevention and Control in China. Beijing: People’s Medical Publishing House; 2021.
15. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. 2008;5(7):e152. doi:10.1371/journal.pmed.0050152
16. Wu L, Chen N, Xia D, Jiang X. Risk factors for multidrug resistance in pulmonary tuberculosis patients with diabetes mellitus. Front Med. 2025;12:1516207. doi:10.3389/fmed.2025.1516207
17. Tan J, Shi X, Pi Y, Xiang M, Li T. Nutritional scores predict the prognosis of patients with pulmonary tuberculosis. Front Nutr. 2024;11:1454207. doi:10.3389/fnut.2024.1454207
18. Kong D, Xia Y, Wang X, et al. Prevalence trends, population characteristics and treatment outcomes of tuberculosis combined with diabetes in Southwest China: a register-based retrospective study. Front Public Health. 2024;12:1445857. doi:10.3389/fpubh.2024.1445857
19. He X, Wang Y, Yang Y, He Q, Sun L, Jin J. Quantitative proteomics reveals plasma protein profile and potential pathways in pulmonary tuberculosis patients with and without diabetes. Tuberculosis. 2023;143:102424. doi:10.1016/j.tube.2023.102424
20. Panda S, Arora A, Luthra K, et al. Hyperglycemia modulates M1/M2 macrophage polarization in chronic diabetic patients with pulmonary tuberculosis infection. Immunobiology. 2024;229(2):152787. doi:10.1016/j.imbio.2024.152787
21. Zhang X, Fu H, Li J, et al. Development and validation of a predictive model using inflammatory biomarkers for active tuberculosis risk in diabetic patients. J Inflamm Res. 2025;18:4725–4739. doi:10.2147/JIR.S512075
22. Ye X, Zhao Y, Ma W, et al. The potential of CD38 protein as a target for autoimmune diseases. Autoimmun Rev. 2023;22(4):103289. doi:10.1016/j.autrev.2023.103289
23. Acheampong I, Minadzi D, Laing EF, et al. Differences in PPD- and mitogen-induced T-cell activation marker expression characterize immunopathology in acute tuberculosis patients. Eur J Clin Microbiol Infect Dis. 2024;43(3):611–616. doi:10.1007/s10096-023-04741-3
24. Fang Y, Tang Y, Luo QX, et al. Changes of mycobacterium tuberculosis specific antigen-stimulated CD27(-)CD38(+)IFN-gamma(+)CD4(+) T cells before and after anti-tuberculosis treatment. Eur J Med Res. 2024;29(1):147. doi:10.1186/s40001-024-01713-x
25. Liu YY, Zhang YY, Wan Q. immunocytes play a crucial role as mediators in the protective effects of D-beta-hydroxybutyrate dehydrogenase 1 against type 2 diabetes mellitus: a mendelian randomization study. Endocr Metab Immune Disord Drug Targets. 2025;25. doi:10.2174/0118715303380282250225071730
26. Rah SY, Joe Y, Park J, et al. CD38/ADP-ribose/TRPM2-mediated nuclear Ca(2+) signaling is essential for hepatic gluconeogenesis in fasting and diabetes. Exp Mol Med. 2023;55(7):1492–1505. doi:10.1038/s12276-023-01034-9
27. Ogura Y, Kitada M, Xu J, Monno I, Koya D. CD38 inhibition by apigenin ameliorates mitochondrial oxidative stress through restoration of the intracellular NAD(+)/NADH ratio and Sirt3 activity in renal tubular cells in diabetic rats. Aging. 2020;12(12):11325–11336. doi:10.18632/aging.103410
28. Wang LF, Li Q, Wen K, et al. CD38 deficiency alleviates diabetic cardiomyopathy by coordinately inhibiting pyroptosis and apoptosis. Int J Mol Sci. 2023;24(21). doi:10.3390/ijms242116008
29. He X, Jiang Y, Hou H, Wu W. Inflammatory markers as predictors of diabetes mellitus in patients with pulmonary tuberculosis: a retrospective analysis of hematological parameters and clinical features. Diab Metabol Syndr Obes. 2025;18:2203–2212. doi:10.2147/DMSO.S523027
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.