Back to Journals » Clinical Interventions in Aging » Volume 11
Correlation between bone mineral density and serum trace elements in response to supervised aerobic training in older adults
Authors Alghadir A, Gabr S ![]() , S. Al-Eisa E, Al-Ghadir M
, S. Al-Eisa E, Al-Ghadir M
Received 15 November 2015
Accepted for publication 13 January 2016
Published 29 February 2016 Volume 2016:11 Pages 265—273
DOI https://doi.org/10.2147/CIA.S100566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Ahmad H Alghadir,1 Sami A Gabr,1,2 Einas S Al-Eisa,1 Muaz H Alghadir3
1Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Kingdom of Saudi Arabia; 2Department of Anatomy, Faculty of Medicine, Mansoura University, Mansoura, Egypt; 3Department of Orthopedics, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia
Background: Life style and physical activity play a pivotal role in prevention and treatment of osteoporosis. The mechanism for better bone metabolism and improvement of physical disorders is not clear yet. Trace minerals such as Ca, Mn, Cu, and Zn are essential precursors for most vital biological process, especially those of bone health.
Objective: The main target of this study was evaluating the effective role of supervised aerobic exercise for 1 hour/day, 3 days/week for 12 weeks in the functions of trace elements in bone health through measuring bone mineral density (BMD), osteoporosis (T-score), bone markers, and trace element concentrations in healthy subjects aged 30–60 years with age average of 41.2±4.9.
Methods: A total of 100 healthy subjects (47 males, 53 females; age range 30–60 years) were recruited for this study. Based on dual-energy x-ray absorptiometry (DEXA) scan analysis, the participants were classified into three groups: normal (n=30), osteopenic (n=40), and osteoporotic (n=30). Following, 12 weeks of moderate aerobic exercise, bone-specific alkaline phosphatase (BAP), BMD, T-score, and trace elements such as Ca, Mn, Cu, and Zn were assessed at baseline and post-intervention.
Results: Significant improvement in serum BAP level, T-score, and BMD were observed in all participants following 12 weeks of moderate exercise. Participants with osteopenia and osteoporosis showed significant increase in serum Ca and Mn, along with decrease in serum Cu and Zn levels following 12 weeks of aerobic training. In control group, the improvements in serum trace elements and body mass index were significantly linked with the enhancement in the levels of BAP, BMD hip, and BMD spine. These results supported the preventive effects of moderate exercise in healthy subjects against osteoporosis. In both sexes, the changes in serum trace elements significantly correlated (P<0.05) with the improvement in BAP, BMD hip, BMD spine, and body mass index in all groups.
Conclusion: The observed changes in the levels of Ca, Mn, Cu, and Zn were shown to be positively correlated with improved bone mass density among control and osteoporosis subjects of both sexes. These results demonstrate that aerobic exercise of moderate intensity might protect bone and cartilage by regulation of body trace elements which are involved in the biosynthesis of bone matrix structures and inhibition of bone resorption process via a proposed anti-free radical mechanism.
Keywords: essential minerals, osteoporosis, bone density, aerobic exercise, BMD, bone metabolism
Introduction
Trace elements perform many important physiologic functions as a catalyst or as an enzyme component within biological systems;1 they are involved in many physiologic roles including antioxidant activity and bone health, and maintain an essential hemostatic balance for proper metabolic functioning.2 It was reported that the main mineral of bone is a crystalline hydroxyapatite (Ca10(PO4)6(OH)2) which comprises most of the matrix of bone cartilage tissue, along with 95% of collagen which gives the bone its tensile strength.3 The significant role of trace elements in bone formation clearly appeared in the mineralization and formation of the organic matrix which subsequently forms bone scaffolds. Recent studies signify the importance of most trace elements in bone metabolism, but copper, zinc, and manganese are among the most important.4,5 Different important functions were reported for trace elements in bone health. Calcium homeostasis is essential for most of the biological processes, including bone metabolism.6 It was reported that serum calcium contributes significantly as biomarker to measure bone metabolism.7,8
Copper was significantly involved in the formation of enzyme lysyl oxidase which is responsible for the crosslinking of elastin and collagen in the organic matrix of bone.4 This ultimately promotes tensile strength and elasticity to bones.
Manganese was reported as an essential cofactor in the biosynthesis of the bone hyaline cartilage structure.9 It was involved in the formation of chondroitin sulfate via polymerization and galacto-transferase processes;10 this is the most important step in bone hyaline cartilage structure. So, any deficiency in Mn causes significant reduction in bone size,11 likely due to reduced chondroitin sulfate content of the bone organic matrix.10 Also, zinc is a cofactor of both collagenase12 and bone alkaline phosphatase.13 Collagenase cleaves procollagen into collagen, and alkaline phosphatase releases phosphorus from phosphates at the site of bone calcification for formation of hydroxyapatite.
Additionally, zinc has many important functions in bone formation; it stimulates osteoblast proliferation and osteoprotegerin activity,14 and gene transcription at the growth plate during long bone growth,15 whereas the deficiency in zinc levels significantly affects bone integrity, and reduces collagenase activity and subsequently collagen synthesis and mineralization of bone.12,16 Osteoporosis is associated with increased bone fragility due to decreased bone mass and altered bone microstructure with bone fracture. This may be due to a reduction in bone mineral content, particularly of the hip.17,18
Many research studies reported that osteoporosis, skeletal abnormalities, and inhibition of boner growth are linked with deficiency in Cu as shown in Menkin’s disease,19 manganese as reported in chondrodystrophy,20 and zinc as reported in osteoporosis.14,16
The changes in the levels of trace elements such as magnesium, copper, zinc, manganese, cadmium, and lead and their influence on the development or treatment of osteoporosis status have yet to be fully elucidated.21
Exercise is the most important parameter in life style that affects bone health; however, its effects on bone metabolism and mass are not fully elucidated.22 In particular, little is known about the changes in bone metabolism induced by various forms of systematic exercises.23 The benefits of mechanical loading or exercise on bone mass and strength have been previously identified.24,25
Beneficial osteogenic effects were significantly reported in bone resorption and formation of subjects performing exercise training with vigorous intensity as jumping or resistive exercise.25 Previously, it was also reported that age, sex, and type of exercise significantly effect on the response of physiological and metabolic parameters of bone formation to physical activity.26
Exercise training programs with varying frequency, duration, and intensity play a pivotal role in reformation of compensatory structures either by increasing the cortical enlargement periosteal or by preventing age-related bone loss at the endosteal surfaces.27 This study was conducted to assess the effects of aerobic exercise of moderate intensity on bone mineral density (BMD), T-score, changes in bone markers, and trace element concentrations in healthy subjects.
Materials and methods
Subjects
A total of 100 healthy subjects (47 males, 53 females) aged 30–60 years were randomly selected for this study after having written informed consent (Table 1). None of them had a history of metabolic bone or chronic or infectious diseases. Also, subjects with physical disability and who had drugs that could interfere with bone turnover were excluded from this study. Demographic and obesity-related parameters such as body mass index (BMI), waist, hip, and waist-to-hip ratio (WHR) were measured using standard girth measurements before and after training sessions. Waist circumference was measured as the minimum circumference between the iliac crest and the rib cage, while hip was measured at the widest part of buttocks,28 and WHR was calculated as waist circumference divided by hip. This study was approved by ethical committee of Rehabilitation Research Chair of King Saud University, under file number ID: RRC-2013-011.
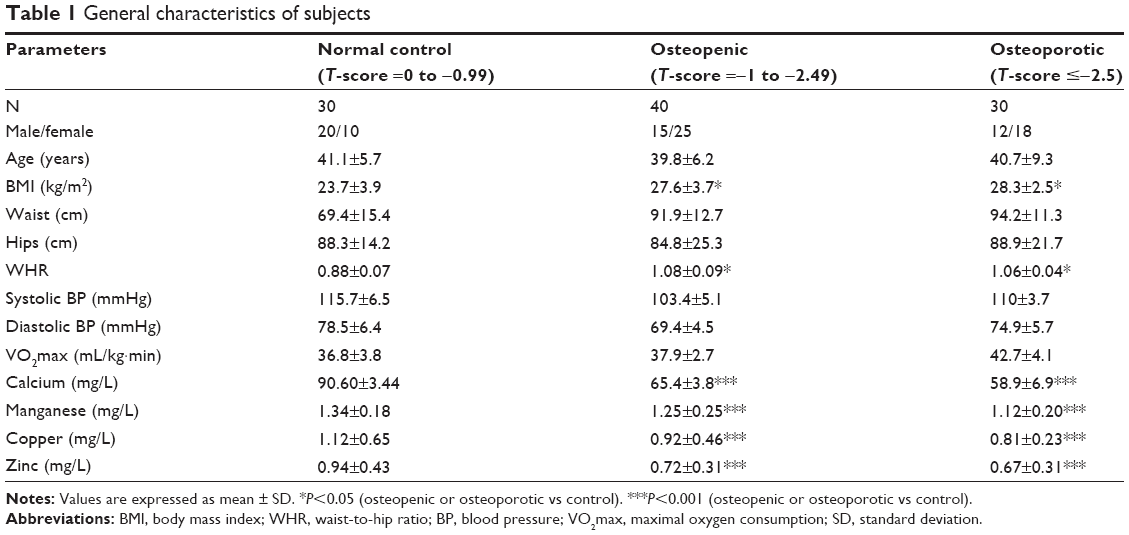 | Table 1 General characteristics of subjects |
Assessment of BMD
BMD was assessed using DEXA scans (Lunar, DPXL/PED; Madison, Winconsin, WI, USA). Total hip and spine BMD were calculated using standard measurements. The data obtained from DEXA test were used to calculate T-score which facilitate the diagnosis of osteoporosis among participants. The participants were scored for osteoporosis as normal (n=30; T-score =0 to −0.99), osteopenic (n=40; T-score =−1 to −2.49), and osteoporotic (n=30; T-score ≤−2.5).
Training procedure
Participants were subjected to supervised exercise program for 45–60 minutes three times per week for 12 weeks using treadmill. The exercise program with moderate intensity was shown to be suitable for most of the sedentary subjects, especially those with osteoporosis. The maximum exercise intensity of each participant was calculated as training heart rate (THR) according to Karvonen’s formula:29 THR = HRrest + (HRmax – HRrest) × TF, where HRrest was resting heart rate (bpm), HRmax was maximum heart rate (bpm), and TF was training fraction which was 65%–75% for moderate intensity and used in this study.29 The subjects performed 5–10 minutes warming up by stretching exercises before each session. During the active phase, the subject was allowed to reach his pre-calculated THR in bouts form with total time of 45–60 minutes performed as circuit training using treadmill, bicycle, and stair master. The exercise test was performed to give the participants physical activities corresponding to 30%–45% of VO2max uptake.30 Participants were monitored by electrocardiogram, and blood pressure was noted throughout the training session.
Assessment of serum bone alkaline phosphatase
Serum bone-specific alkaline phosphatase (sBAP) concentrations (U/L) were measured in all participants in pre- and postexercise training periods using immunoenzymetric assay (MicroVue BAP; Quidel Corporation, San Diego, CA, USA).
Assessment of serum trace elements
Levels of calcium, manganese, copper, and zinc in the sera were determined using an atomic absorption spectrophotometer device (Varian AA240FS model; Varian Inc., Belrose, Australia). The measurements were conducted twice for each sample, using light at 2,139 nm wavelength according to flame atomization method. Levels of serum Ca, Cu, Zn, and Mn were determined in milligram per liter.
Statistical analysis
The data were statistically analyzed and expressed as means plus standard deviation using SPSS version 17. Participant’s demographic characteristics and results were summarized and reported as mean ± standard deviation. Comparisons and significant relationships between studied variables in all groups were evaluated by analysis of variance, independent samples Student’s t-test, and Pearson’s correlation coefficient. P-values <0.05 were considered to be significant.
Results
A total of 100 healthy subjects were recruited for this study. Out of them, 47% were female, and 53% were male. They were classified according to BMD measurements and osteoporosis T-score into normal, osteopenic, and osteoporotic participants. There was a significant difference in BMI and WHR of osteopenic and osteoporotic participants compared with the normal group (Table 1). Trace element concentrations were evaluated in this study. In osteopenic and osteoporotic subjects, there was significant (P=0.001) decrease in the serum levels of Ca, Mn, Cu, and Zn compared to control subjects (Table 1).
The effects of supervised aerobic exercise of moderate intensity for 1 hour/day, 3 days/week for 12 weeks on the levels of trace elements and bone indices sBAP, BMD hip, and BMD spine were assessed in male and female subjects of all studied groups. There were significant increases in the serum levels of Ca and Mn and decrease in Cu and Zn serum concentrations among osteopenic, osteoporotic, and control subjects. These changes are significantly linked with the increase in serum levels of sBAP and improvements in BMD hip and BMD spine measurements as shown in Tables 2 and 3. The data showed that moderate exercise interventions could provide a preventive activity against bone loss and osteoporosis through considerable enhancement in the serum levels of trace elements and bone mass density markers, especially among control subjects.
 | Table 2 Comparison of serum trace element (mg/L) and the bone metabolism markers for female subjects (N=53) before and after 12-week aerobic exercise training (mean ± SD) |
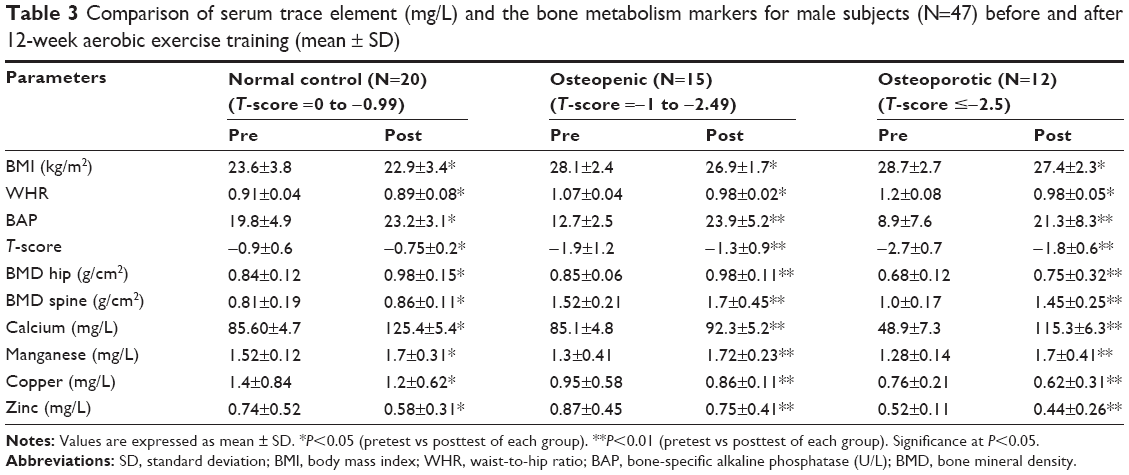 | Table 3 Comparison of serum trace element (mg/L) and the bone metabolism markers for male subjects (N=47) before and after 12-week aerobic exercise training (mean ± SD) |
The increase in serum levels of sBAP and enhancement of bone density indices BMD hip and BMD spine are significantly correlated with the change in the serum levels of trace elements, BMI, and sex in osteopenic and osteoporotic subjects. Bone density markers correlated positively with BMI, sex, Ca, and Mn, and negatively with Cu and Zn levels (Table 4).
 | Table 4 Correlations of serum trace elements concentration with sBAP and total hip and spine BMD in male and female participants with osteopenia and osteoporosis (n=70) following 12-week aerobic training |
Discussion
Exercise interventions with varying intensities play a pivotal role in bone reformation, especially in compensatory structures.27
In most countries, more of social and economic interests were reported for osteoporosis, whereas the size of the aging population having bone loss continues to grow in both sexes of healthy younger and adult subjects.31–35
In adults aged ~30, there was hemostatic equilibrium in bone resorption and formation, after which bone density starts to decline slowly.36 Therefore, it was reported that the magnitude of the problem may be even larger in developing countries.35 The effects of osteoporosis treatment were efficiently explored using reliable methods such as DEXA and BMD measures.37
This study was assessed to evaluate the effects of moderate aerobic exercise on BMD, serum trace element levels, and serum sBAP as marker of bone turnover in healthy subjects.
The current study showed lower levels of Ca, Mn, Cu, and Zn in serum samples from participants with osteoporosis and osteopenia than in normal controls. Previous studies have shown that Ca, Mn, Cu, and Zn are essential for organic bone matrix synthesis.4,6,7,9,10,12,38
Protein and calcium are the major components of organic matrix of healthy bone,7 whereas certain minerals and vitamins were required for preserving bone health.39,40
In addition to its importance in >200 enzymes, zinc is known to be necessary for normal collagen synthesis and mineralization of bone,41,42 and its deficiency has been associated with abnormalities in growth, formation, strength, and mineralization of bone.43,44 It was reported that women and men with low bone mass or osteoporosis showed significant lower levels of plasma zinc and higher urinary zinc excretion.45–49 Also, previous studies have demonstrated that Zn and Cu deficiency can cause an increase in the risk of bone resorption by inhibiting bone growth and subsequently progression of osteoporosis.46,50 Similarly, Mn was reported to be involved in the formation of chondroitin sulfate that is important in biosynthesis of the bone hyaline cartilage structure,9,10 and deficiency in Mn content produces significant reduction in bone size,11 due to a reduction in chondroitin sulfate content of the bone organic matrix.10
Low BMD is the most essential indicator related to bone fractures, and BMD accounts for ~70% of bone strength;51 thus, mechanical forces such as physical exercise exerted on skeleton are of great importance to preserve and improve BMD and in good bone formation in both adolescent and the elderly.52 However, the mechanisms by which systematic exercise leads to changes in bone metabolism are not fully understood.22
In this study, significant improvements in T-score and BMD were reported in all subjects following moderate aerobic training for 12 weeks. T-score and BMD postexercise values showed significant improvements approaching to normal levels in osteopenic, osteoporotic, as well as control subjects. This may support the efficacy of moderate aerobic training in enhancing BMD and preventing osteoporosis.
The data obtained showed significant correlation with the improvement in BMI in osteopenic and osteoporotic participants as previously reported,24,53 supporting the preservation effect of moderate regular exercises as aerobics on bone health, especially increment of femur neck-BMD in osteopenic women.54 Also, it was reported that exercise promotes bone formation and prevents age-related bone loss that depends mainly on the frequency, duration, and exercise intensity.55 Similarly, significant increase in BMD was reported among the athletes compared to the nonathletes of similar age. It was concluded that mechanical stress in the form of exercise activity may be a major factor in bone mineralization. The proposed mechanism is that the bone cells (osteocytes) act as mechanoreceptors which respond and subsequently release chemical activators for promoting osteoblast proliferation at the local bone site.56
Recently, a study performed on both males and females concluded that aerobic training of moderate intensity exerts significant positive effects on bone formation marker and bone density along with reported significant decrease in the rate of bone resorption in both males and females aged (30–60 years) that could assist in preventing or decelerating osteoporosis.57
In this study, post-training results showed significant increase in the level of sBAP as a marker of bone formation. The level of sBAP has been shown to be sensitive to alterations in bone metabolism due to physical exercise, and it was concluded that aerobic exercise may accelerate the rate of bone remodeling. Although, our results were in line with other research study which reported an increase in the level of BAP following 16 weeks of resistance training,22 and conversely reported a significant improvement in either muscle strength or BMD without change in bone markers.24 Similarly, aerobic exercise of long duration significantly produces elevation in biomarkers of bone remodeling, reduction in bone resorption, and increase in the rate of bone formation,26,58 and the increase in bone formation and resorption markers was significantly stimulated with combined resistance and aerobic training.59
The relationship between trace elements and the etiology of osteoporosis in this study was reported following 12 weeks of aerobic training. There was significant increase in Ca and Mn, and decrease in Cu and Zn serum concentrations in participants with osteopenia and osteoporosis as well as in normal controls.
The participants of the present study showed significant increase in the level of serum calcium following moderate training interventions. It was reported that physical activity exerted from various exercise training intensities stimulates parathyroid glands to release more parathyroid hormone that controls the liberation of calcium from its reserves toward blood.60,61 Other previous study reported that ~40% of the variance in bone density was shown to be linked with environmental factors such as physical activity and calcium intake.62,63
The results of this study showed significant increase in manganese serum levels among participants with osteopenia and osteoporosis following aerobic training. It was reported that skeletal abnormalities, such as osteoporosis, and congenital disorders of skeleton including chondrodystrophy were significantly linked with prolonged deficiency in Mn concentrations.20 Also, in Reginster et al study, lower levels of serum Mn were estimated in postmenopausal women with osteoporosis compared to controls.64 The deficiency in Mn concentration provides significant reduction in bone size as a result of suppression in the biosynthesis of chondroitin sulfate that comprises the most important step in bone hyaline cartilage structure.9–11 Recent studies showed that physically active young healthy boys reported an increase in the serum levels of trace elements, especially Mn concentrations.61
It seemed that application of physical exercise may lead to a redistribution of various trace elements between body reserves, blood, and tissues. So, the increase in the level of Mn in serum samples of participants plays significant role as a cofactor in the formation of bone cartilage and bone collagen, as well as in bone mineralization.46
Most recent studies showed that Mn trace element is a part of Mn-dependent superoxide dismutase (SOD) enzymes. These enzymes have a positive significant effect against oxidative free radicals initially increased in osteoporotic subjects and also after exercise interventions. The increase in the levels of oxidative stress parameters significantly equalized with a set of antioxidant enzymes including Mn-dependent SOD.65,66 The extreme mechanical loading was shown to increase oxidative stress free radicals in chondrocytes67,68 and osteoblast-like cells,69 and exercise leads to a substantial increase of SOD activity in skeletal muscle70 and cartilage.71 In heterozygous SOD2-deficient mice, the osteocytes showed significant reduction in oxidative stress parameters following aerobic running exercise for 8 weeks and exercise might protect bone against oxidative stress with preservation morphological, structural, and mechanical properties of both osteocyte and chondrocyte tissues.72 Also, another recent study reported a significant increase in the levels of many trace elements including Mn following nighttime treadmill exercise.73
The changes in trace element levels depend on the type, length, and intensity of the exercise which affects on human physiological and biochemical events, especially bone health.74 Recently, it was reported that Zn and Cu are essential cofactors of enzymes involved in bone metabolism.75 Therefore, it is important to examine that whether the exercise effects on the function of these elements or not, especially in elderly participants with osteoporosis.
In this study, there was significant decrease in Cu and Zn serum levels of participants with osteopenia and osteoporosis as well as control subjects following 12-week moderate aerobic training. This matched with earlier studies which reported significant decrease in Cu and Zn levels following exercise training.46 It can be pointed out that the people who have regular exercises should pay attention to their nutrition because they may have health problems based on the lack of trace element if they do not pay attention to their nutrition.76
It was reported that both Cu and Zn were involved in the inhibition of bone resorption by inhibiting osteoclast-like cell formation.21,42,76 The decrease in the levels of Cu and Zn reported in our subjects following moderate exercise might be due to a redistribution of these trace elements between body reserves, blood, and tissues,46 and might be because a part of these elements was involved in the biosynthesis of Cu-/Zn-SOD antioxidant enzymes which act as a free radical scavenger, neutralizing the superoxide radicals produced by osteoclasts during bone resorption.48,77,78
The change in serum level of Cu and Zn by moderate aerobic exercise was significantly correlated with the improvement in BMD, sBAP, and BMI within the studied subjects of both sexes.
The decrease in Cu and Zn concentration following physical exercise may be related to an increase in the metabolism of these trace elements and suggest its involvement in the biosynthesis of enzymes needed for bone formation process.74,75 Similarly, the evidences from human and animal studies showed that a lack of Cu leads to both abnormal bone formation and fracture.46 In addition, studies have shown that Zn and Cu levels in serum play an important role in the regulation of bone formation,4,14,15 whereas both Zn and Cu were reported to be an essential cofactors of enzymes involved in synthesis of various bone matrix constituents. Thus, these elements play an important role in the regulation of bone deposition and resorption.76
Conclusion
The observed changes in the levels of Ca, Mn, Cu, and Zn were shown to be positively correlated with improved bone mass density among control and osteoporosis subjects of both sexes. These results demonstrate that aerobic exercise of moderate intensity might protect bone and cartilage by regulation of body trace elements which are involved in the biosynthesis of bone matrix structures and inhibition of bone resorption process via a proposed anti-free radical mechanism.
Acknowledgment
The project was financially supported by King Saud University, through Vice Deanship of Research Chairs, Rehabilitation Research Chair.
Disclosure
The authors report no conflicts of interest in this work.
References
Aras NK, Taman DYA. Trace Element Analysis of Food and Diet. Cambridge, UK: RSC Publishing; 2006. | ||
Hazar M, Sever O, Otag A. Physiological responses of macro-elements to maximal aerobic exercise among elite women and men field hockey players. Health Med. 2012;6(9):3084–3090. | ||
Saito M, Marumo K. Collagen crosslinks as a determinant of bone quality: a possible explanation for bone fragility in aging, osteoporosis, and diabetes mellitus. Osteoporosis Int. 2010;21:195–214. | ||
Marturano JE, Xylas JF, Sridharan GV, Georgakoudi I, Kuo CK. Lysyl oxidase mediated collagen crosslinks may be assessed as markers of functional properties of tendon tissue formation. Acta Biomater. 2014;10:1370–1379. | ||
Zofkova I, Nemcikova P, Matucha P. Trace elements and bone health. Clin Chem Lab Med. 2013;51:1555–1561. | ||
Narattaphol C. Physical activity and exercise affect intestinal calcium absorption: a perspective review. J Sports Sci Technol. 2007;7(1):171–181. | ||
Rubinacci A, Covini M, Bisogni C, et al. Bone as an ion exchange system: evidence for a link between mechanotransduction and metabolic needs. Am J Physiol Endocrinol Metab. 2002;282:E851–E864. | ||
Marenzana M, Shipley AM, Squitiero P, Kunkel JG, Rubinacci A. Bone as an ion exchange organ: evidence for instantaneous cell-dependent calcium efflux from bone not due to resorption. Bone. 2005;37:545–554. | ||
Eyre DR. Collagens and cartilage matrix homeostasis. Clin Orthop Relat Res. 2004;427:S118–S122. | ||
Leach JRM, Muenster A, Wien EM. Studies on the role of manganese in bone formation: II. Effect upon chondroitin sulfate synthesis in chick epiphyseal cartilage. Arch Biochem Biophys. 1969;133:22–28. | ||
Caskey CD, Gailup WD, Norris LC. The need for manganese in the bone development of the chick. J Nutr. 1939;17:407–417. | ||
Starcher BC, Hill CH, Madaras JG. Effect of zinc deficiency on bone collagenase and collagen turnover. J Nutr. 1980;110:2095–2102. | ||
Seo H, Cho Y, Kim T, Shin H, Kwun I. Zinc may increase bone formation through stimulating cell proliferation, alkaline phosphatase activity and collagen synthesis in osteoblastic MC3T3E1 cells. Nutr Res Pract. 2010;4:356–361. | ||
Liang D, Yang M, Guo B, Cao J, Yang L, Guo X. Zinc up regulates the expression of osteoprotegerin in mouse osteoblasts MC3T3E1 through PKC/MAPK pathways. Biol Trace Elem Res. 2012;146:340–348. | ||
Oviedo-Rondon EO, Ferket PR, Havestein GB. Understanding long bone development in broilers and turkeys. Avian Poult Biol Rev. 2006;17:77–88. | ||
Hyun TH, Barret-Connor J, Milne DB. Zinc intakes and plasma concentrations in men with osteoporosis the Rancho Bernardo Study. Am J Clin Nutr. 2004;80:715–721. | ||
Raisz LG. Pathogenesis of osteoporosis: concepts, conflicts, and prospects. J Clin Invest. 2005;115(12):3318–3325. | ||
Kanis JA, Melton LJ III, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137–1141. | ||
Opsahl W, Zeronian H, Ellison M, Lewis D, Rucker RB, Riggins RS. Role of copper in collagen cross-linking and its influence on selected mechanical properties of chick bone and tendon. J Nutr. 1982;112:708–716. | ||
Strause LG, Hegenauer J, Saltman P, Cone R, Resnick D. Effects of long term dietary manganese and copper deficiency on rat skeleton. J Nutr. 1986;116:135–141. | ||
Yamaguchi M. Role of nutritional zinc in the prevention of osteoporosis. Mol Cell Biochem. 2010;338(1–2):241–254. | ||
Gonzalez-Aguero A, Vicente-Rodriguez G, Gomez-Cabello A, Ara I, Moreno LA, Casajus JA. A 21week bone deposition promoting exercise programme increases bone mass in youths with Down syndrome. Dev Med Child Neurol. 2012;54:552–556. | ||
Kohrt WM, Bloomfield SA, Little KD, Nelson ME, Yingling VR. American College of Sports Medicine Position Stand: physical activity and bone health. Med Sci Sports Exerc. 2004;36(11):1985–1996. | ||
Umemura Y, Nagasawa S, Honda A, Singh R. High impact exercise frequency per week or day for osteogenic response in rats. J Bone Miner Metab. 2008;26(5):456–460. | ||
Bemben DA, Buchanan TD, Bemben MG, Kenhans AW. Influence of type of mechanical loading, menstrual status, and training season on bone density in young women athletes. J Strength Cond Res. 2004;18:220–226. | ||
Duncan CS, Blimkie CJ, Kemp A, et al. Mid-femur geometry and biomechanical properties in 15- to 18-yr-old female athletes. Med Sci Sports Exerc. 2002;34:673–681. | ||
Walker RC, Dhawan V, Romney JD, Kellermann KI, Vermeulen RC. VLBA absorption imaging of ionized gas associated with the accretion disk in NGC 1275. Astrophys J. 2000;530:233. | ||
Aekplakorn W, Kosulwat V, Suriyawongpaisal P. Obesity indices and cardiovascular risk factors in Thai adults. Int J Obes. 2006;30:1782–1790. | ||
Karvonen M, Kentala K, Mustala O. The effects of training heart rate: a longitudinal study. Ann Med Exp Biol Fenn. 1957;35:307–315. | ||
Guezenne CY, Satabin P, Legrand H, BigardI AX. Physical performance and metabolic changes induced by combined prolonged exercise and different energy intakes in humans. Eur J Appl Physiol. 1994;68:525–530. | ||
Bonura F. Prevention, screening and management of osteoporosis: an overview of the current strategies. Postgrad Med. 2009;121:5–17. | ||
Limpaphayom KK, Taechakraichana N, Jaisamrarn U, et al. Prevalence of osteopenia and osteoporosis in Thai women. Menopause. 2001;8:65–69. | ||
Pongchaiyakul C, Apinyanurag C, Soontrapa S, et al. Prevalence of osteoporosis in Thai men. J Med Assoc Thai. 2006;89:160–169. | ||
Trivitayaratana W, Trivitayaratana P. Peripheral BMD T-scores in the diagnosis of osteoporosis. J Med Assoc Thai. 2005;88:S8–S12. | ||
Handa R, Kalla AA, Maalouf G. Osteoporosis in developing countries. Best Pract Res Clin Rheumatol. 2008;22:693–708. | ||
Clarke B. Normal bone anatomy and physiology. Clin J Am Soc Nephrol. 2008;3:S131–S139. doi:10.2215/CJN.04151206. | ||
Rizer MK. Osteoporosis. Prim Care. 2006;33:943–951. | ||
Mutlu M, Kilic E. Magnesium, zinc and copper status in osteoporotic, osteopenic and normal post-menopausal women. J Int Med Res. 2007;35:692–695. | ||
Ilich JZ, Kerstetter JE. Nutrition in bone health revisited: a story beyond calcium. J Am Coll Nutr. 2000;19:715–737. | ||
Heaney R. Osteoporosis. In: Coulston AM, Rock CL, Monsen ER, editors. Nutrition in the Prevention and Treatment of Disease. San Diego: Academic Press; 2001:653–684. | ||
Calhoun NR, Smith JC, Becker KL. The role of zinc in bone metabolism. Clin Orthop. 1974;103:212–234. | ||
Wallwork JC, Sandstead HH. Zinc. In: Simmons DJ, editor. Nutrition and Bone Development. New York: Oxford University Press; 1990:316–339. | ||
Yamaguchi M. Role of zinc in bone formation and bone resorption. J Trace Elem Exp Med. 1998;11:119–135. | ||
Alhava EM, Olkkonen H, Puittinen J, Nokso-Koivisto VM. Zinc content of human cancellous bone. Acta Orthop Scand. 1977;48:1–4. | ||
Freudenheim JL, Johnson NE, Smith EL. Relationships between usual nutrient intake and bone mineral content of women 35–65 years of age: longitudinal and cross-sectional analysis. Am J Clin Nutr. 1986;44:863–876. | ||
Gur A, Colpan L, Nas K, et al. The role of trace minerals in the pathogenesis of postmenopausal osteoporosis and a new effect of calcitonin. J Bone Miner Metab. 2002;20:39–43. | ||
Lowe NM, Fraser WD, Jackson MJ. Is there a potential therapeutic value of copper and zinc for osteoporosis? Proc Nutr Soc. 2002;61:181–185. | ||
Relea P, Revilla M, Ripoll E, Arribas I, Villa LF, Rico H. Zinc, biochemical markers of nutrition, and type I osteoporosis. Age Ageing. 1995;24:303–307. | ||
Herzberg M, Foldes J, Steinberg R, Menczel J. Zinc excretion in osteoporotic women. J Bone Miner Res. 1990;5:251–257. | ||
Anke M. Die Rolle von Spurenelementen in der Dynamik der Arteriosklerose. [Role of trace elements in the dynamics of arteriosclerosis]. Z Gesamte Inn Med. 1986;41(4):105–111. German. | ||
Follin SL, Hansen LB. Current approaches to the prevention and treatment of postmenopausal osteoporosis. Am J Health Syst Pharm. 2003;60(9):883–901; quiz 903–904. | ||
Scerpella TA, Davenport M, Morganti CM. Dose related association of impact activity and bone mineral density in prepubertal girls. Calcif Tissue Int. 2003;72(1):24–31. | ||
Sahmani M, Omidian S, Javadi A, Sabet MS, Abbasi M. Association between the serum levels of zinc, copper and lipid profile with osteoporosis in Iranian postmenopausal women. Biotechnol Health Sci. 2014;1(1):e19190. | ||
Weisman SM, Matkovic V. Potential use of biochemical markers of bone turnover for assessing the effect of calcium supplementation and predicting fracture risk. Clin Ther. 2005;27:299–308. | ||
Gabrie A, Detilleux J, Jolly S, Reginster J-Y, Collin B, Dessy-Doize C. Morphometric study of the equine navicular bone: age-related changes and influence of exercise. Vet Res Commun. 1999;23:15–40. | ||
Andreoli A, Monteleone M, Loan MV, Promenzio L, Tarantino U, Lorenzo A. Effects of different sports on BMD and muscle mass in highly trained athletes. Off J Am Coll Sports Med. 2001;33:507–511. | ||
Alghadir AH, Aly FA, Gabr SA. Effect of moderate aerobic training on bone metabolism indices among adult humans. Pak J Med Sci. 2014;30(4):840–844. | ||
Lester ME, Urso ML, Evans RK, Pierce JR, Spiering BA, Maresh CM. Influence of exercise mode and osteogenic index on bone biomarker responses during short-term physical training. Bone. 2009;45:768–776. | ||
Maimoun L, Mariano-Goulart D, Couret I, et al. Effects of physical activities that induce moderate external loading on bone metabolism in male athletes. J Sports Sci. 2004;22:875–883. | ||
Pourvaghar MJ. The effect of 2 month-regular aerobic training on students’ rest time serum calcium, phosphorus and magnesium variations. Gazzeta Medica Italiana. 2008;167(3):105–108. | ||
Kara E. Effect of a three-month football training program on trace element metabolism of boys in the eight to twelve age groups. Afr J Biotechnol. 2011;11(1):169–172. | ||
Kelly PJ, Eisman JA, Sambrook PN. Interaction of genetic and environmental influences on peak bone density. Osteoporosis Int.1990;1:56–60. | ||
Joo NS, Dawson-Hughes B, Kim YS, Oh K, Yeum KJ. Impact of calcium and vitamin D insufficiencies on serum parathyroid hormone and bone mineral density: analysis of the fourth and fifth Korea National Health and Nutrition Examination Survey (KNHANES IV-3, 2009 and KNHANES V-1, 2010). J Bone Miner Res. 2013;28(4):764–770. | ||
Reginster JY, Strause L, Saltman P, Frachimont P. Trace elements and osteoporosis: a preliminary study of decreased serum manganese. Med Sci Res. 1998;16:337–338. | ||
Henrotin Y, Kurz B, Aigner T. Oxygen and reactive oxygen species in cartilage degradation: friends or foes? Osteoarthritis Cartilage. 2005;13:643–654. | ||
Banfi G, Iorio EL, Corsi MM. Oxidative stress, free radicals and bone remodeling. Clin Chem Lab Med. 2008;46:1550–1555. | ||
Beecher BR, Martin JA, Pedersen DR, Heiner AD, Buckwalter JA. Antioxidants block cyclic loading induced chondrocyte death. Iowa Orthop J. 2007;27:1–8. | ||
Tomiyama T, Fukuda K, Yamazaki K, et al. Cyclic compression loaded on cartilage explants enhances the production of reactive oxygen species. J Rheumatol. 2007;34:556–562. | ||
Yamamoto N, Fukuda K, Matsushita T, Matsukawa M, Hara F, Hamanishi C. Cyclic tensile stretch stimulates the release of reactive oxygen species from osteoblast-like cells. Calcif Tissue Int. 2005;76:433–438. | ||
Oh-ishi S, Kizaki T, Nagasawa J, et al. Effects of endurance training on superoxide dismutase activity, content and mRNA expression in rat muscle. Clin Exp Pharmacol Physiol. 1997;24:326–332. | ||
Cifuentes DJ, Rocha LG, Silva LA, et al. Decrease in oxidative stress and histological changes induced by physical exercise calibrated in rats with osteoarthritis induced by monosodium iodoacetate. Osteoarthritis Cartilage. 2010;18:1088–1095. | ||
Alexander B, Jan H, Wilhelm B, et al. Effect of exercise on bone and articular cartilage in heterozygous manganese superoxide dismutase (SOD2) deficient mice. Free Radic Res. 2011;45(5):550–558. | ||
Patlar S, Gulnar U, Baltaci AK, Mogulkoc R. Effect of nocturnal exhaustion exercise on the metabolism of selected elements. Arch Biol Sci Belgrade. 2014;66(4):1595–1601. | ||
Bednarek-Tupikowska G, Jodkowska A, Antonowicz-Juchniewicz J. Zinc, copper, manganese, and selenium status in pre- and postmenopausal women during sex hormone therapy. Adv Clin Exp Med. 2010;19(3):337–345. | ||
Kara E, Akil M, Yalcinkaya O. The effect of aerobic exercise programme on trace element levels of young men. Afr J Microbiol Res. 2012;6(1):165–168. | ||
Lowe NM, Lowe NM, Fraser WD, Jackson MJ. Is there a potential therapeutic value of copper and zinc for osteoporosis? Proc Nutr Soc. 2002;61(2):181–185. | ||
Rucker RB, Kosonen T, Clegg MS, et al. Copper, lysyl oxidase and extracellular matrix protein cross-linking. Am J Clin Nutr. 1998;67:996S–1002S. | ||
Rico H. Minerals and osteoporosis. Osteoporosis Int. 1991;2:20–25. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.