")
Back to Journals » Clinical Interventions in Aging » Volume 18
Correlation Between Benign Prostatic Hyperplasia/Lower Urinary Tract Symptoms and Renal Function in Elderly Men Aged 80 Years and Older
Authors Wang Q, Zhang B, Li B, Yang S, Wang Z, Han C, Wu J, Tian R
Received 7 October 2022
Accepted for publication 4 January 2023
Published 13 January 2023 Volume 2023:18 Pages 61—69
DOI https://doi.org/10.2147/CIA.S392519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Qian Wang,1,* Bin Zhang,1,* Bing Li,1 Shengnan Yang,1 Zhifang Wang,2 Chao Han,3 Jie Wu,4 Rui Tian1
1The Second Division of General Geriatrics, Department of Geriatrics, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Division of Endocrinology, Department of Medicine, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 3Department of Pharmacy, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 4Division of Ultrasound, Department of Medical Imaging, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qian Wang; Rui Tian, The Second Division of General Geriatrics, Department of Geriatrics, the First Affiliated Hospital of Zhengzhou University, No. 1 Eastern Jianshe Road, Erqi District, Zhengzhou, Henan, 450052, People’s Republic of China, Tel +8615838328873, Fax +8637166295183, Email [email protected]; [email protected]
Purpose: To investigate the relationship between benign prostatic hyperplasia (BPH)/lower urinary tract symptoms (LUTS) and renal function in elderly men aged 80 years and older.
Patients and Methods: We selected 389 elderly men aged 80– 97 years with BPH/LUTS hospitalized at The Second Division of General Geriatrics, The First Affiliated Hospital of Zhengzhou University, between July 2018 and July 2020. In the cross-sectional study, patients were divided into the treatment (233 patients) and non-treatment (156 patients) groups based on whether they received treatment for BPH/LUTS. In the prospective self-case-control study, we included 129 of the non-treatment group patients who received oral BPH/LUTS medication and completed the 6-month outpatient follow-up. We compared prostate indicators and renal function in the cross-sectional study and baseline and after-treatment data in the prospective self-case-control study. Multiple linear regression analysis was performed for risk factors affecting renal function before and after BPH/LUTS treatment.
Results: In the cross-sectional study, renal function was significantly better in the treatment group than in the non-treatment group. In the subgroup analysis of the prospective self-case-control study, renal function significantly improved after treatment among patients with hypertension and those with chronic kidney disease (CKD) 3a, but not in the entire cohort. Multivariable linear regression analysis showed that hypertension (β=2.06, 95% CI 0.40 to 3.71) and CKD 3a (β=17.16, 95% CI 15.53 to 18.79) were independent risk factors for creatinine differences before and after treatment, whereas hypertension (β=− 2.27, 95% CI − 3.65 to − 0.89), CKD 3a (β=− 11.93, 95% CI − 13.29 to − 10.58), and baseline prostate volume (β=− 0.11, 95% CI − 0.20 to − 0.02) were independent risk factors for estimated glomerular filtration rate differences before and after treatment.
Conclusion: Treatment for moderate and severe BPH/LUTS can improve renal function in elderly patients with hypertension or CKD 3a.
Keywords: benign prostatic hyperplasia, lower urinary tract symptoms, renal function, elderly men, drug therapy
Introduction
Benign prostatic hyperplasia (BPH) and a decline in the glomerular filtration rate have become common comorbidities and important public health problems in elderly men aged 80 years and older. The histological changes associated with BPH begin at age 40, and the incidence of BPH increases with age, with incidences of >50% at age 60 and 83% at age 80.1 The decrease in nephrons among older individuals is associated with a decrease in renal blood flow, which leads to an age-related decline in the glomerular filtration rate.2 Most patients with BPH develop lower urinary tract symptoms (LUTS),1 and prostate size correlated with a higher proportion of urinary catheters,3 which could relieve acute or chronic retention. Therefore, in addition to LUTS, older men with BPH can have acute or chronic retention that accelerates the decline of the glomerular filtration rate, eventually causing or aggravating renal dysfunction.4 Although the 2003 updated guidelines of the American Urological Association (AUA) no longer recommend that men with LUTS be regularly screened for serum creatinine.5 Patients with chronic kidney disease and chronic BPH/LUTS are commonly seen in the clinic.6 However, whether BPH/LUTS increases the risk of renal dysfunction remains unknown.
Here, we sought to investigate the relationship between BPH/LUTS and renal function through a cross-sectional study in 389 elderly men aged 80 years and older with BPH/LUTS and through a prospective self-case-control study evaluating the effect of BPH/LUTS treatment on renal function before and after treatment in 129 elderly men with BPH/LUTS. This study provides data support for improving renal function from the perspective of prostatic hyperplasia in elderly men aged 80 years and older.
Materials and Methods
Study Population
A total of 389 elderly men aged 80–97 years with BPH/LUTS hospitalized at The Second Division of General Geriatrics, The First Affiliated Hospital of Zhengzhou University, between July 2018 and July 2020 were selected. The diagnostic criteria for BPH conformed to the diagnostic criteria in China’s Guidelines for Diagnosis and Treatment of Benign Prostatic Hyperplasia (2007 Edition)7 and 2021 AUA guidelines8 as follows: LUTS, an International Prostate Symptoms Score (IPSS) ≥7 points, and a prostate volume (PV) (longitudinal diameter × transverse diameter × anteroposterior diameter × 0.52) >20 mL, as revealed by color Doppler ultrasonography. The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation was used to calculate the estimated glomerular filtration rate (eGFR). We excluded patients with acute kidney injury, CKD 3b or higher, urinary microalbumin/urinary creatinine >30 mg/g, prostate cancer, urethral stricture of various causes, neurogenic bladder, acute stroke, Parkinson’s disease, acute infections, severe hepatic insufficiency, acute coronary syndrome, severe cardiac insufficiency, diabetic ketosis, or unilateral nephrectomy. This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was provided by the Ethics Committee of The First Affiliated Hospital of Zhengzhou University (approval number: 2020-KY-233). All enrolled patients signed an informed consent form.
Study Design
In the cross-sectional study, the 389 patients were divided into a treatment group (233 patients) and a non-treatment group (156 patients) based on whether they received treatment for BPH/LUTS. The treatment group included patients who received one or more medications for treating prostatic hyperplasia (tamsulosin, doxazosin, or finasteride) or had undergone prostate surgery. In the treatment group, 30 patients received tamsulosin alone, 11 received doxazosin alone, 127 received tamsulosin combined with finasteride, 38 received doxazosin combined with finasteride, and 27 underwent surgery. The non-treatment group did not receive any treatment for BPH/LUTS.
For the prospective self-case-control study, we included 129 patients in the non-treatment group who later received oral BPH/LUTS medication (tamsulosin 0.2 mg/d and finasteride 5 mg/d) and completed the 6-month outpatient follow-up. Figure 1 shows the details of patient selection and treatment. Patients were further divided based on their blood pressure into a normal blood pressure subgroup and a hypertension subgroup and based on CKD into a normal renal function subgroup and a CKD 3a subgroup.
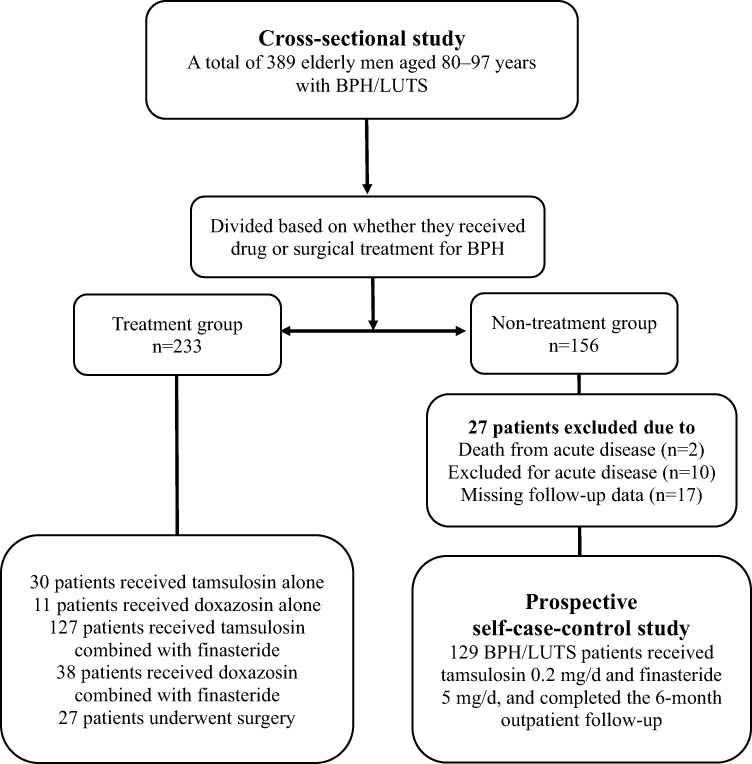 |
Figure 1 Flow diagram showing the major elements of the study design. Abbreviations: BPH, benign prostatic hyperplasia; LUTS, lower urinary tract symptoms. |
Data Collection
We collected the medical history of all patients (coronary heart disease, hypertension, diabetes, cerebral infarction, and CKD) and relevant clinical indicators, including indicators for renal function and BPH, at the time of enrolment and at 1, 3, and 6 months after the initial treatment. The renal function indicators included the serum creatinine level and eGFR. The serum creatinine level was assessed using an automatic biochemical analyzer. The eGFR was calculated using the CKD-EPI equation and included creatinine, age, race, and sex. The BPH/LUTS indicators included IPSS, PV, and post-void residual urine volume (PVR). The IPSS was calculated based on the results of a questionnaire, and the PV and PVR were measured by ultrasonography.
Statistical Analyses
Continuous variables are expressed as mean ± standard deviation and/or medians with interquartile range. The t-test was used to assess differences in homogeneous variables, and the rank-sum test was used to assess differences in heterogeneous variables. Categorical variables are expressed by the number of cases, and the chi-square test was used to assess differences between groups. In the prospective self-case-control study, we assessed the differences in serum creatinine levels and eGFR before and after treatment as dependent variables and performed a single-factor regression analysis with each indicator. Significant variables and potentially clinically significant variables were included in the regression model. Multiple linear regression analysis was performed for related risk factors affecting renal function before and after treatment, and p-values < 0.05 were considered statistically significant. All analyses were performed using SPSS statistical software (ver 26.0).
Results
Baseline Characteristics in the Cross-Sectional and Self-Case-Control Studies
The characteristics of patients in the cross-sectional study are shown in Table 1. There were no significant differences between the treatment and non-treatment groups in terms of age (85 [80, 94] years and 84 [80, 97] years, respectively) or the proportions of patients with hypertension (146/62.67% and 95/60.90%, respectively), diabetes (88/37.77% and 53/33.97%, respectively), coronary heart disease (149/63.95% and 92/58.97%, respectively), or cerebral infarction (109/46.78% and 64/41.03%, respectively) (all p > 0.05). However, the rate of comorbid CKD 3a in the treatment group was significantly lower than that in the non-treatment group (50/21.46% and 65/41.67%, respectively; p < 0.05).
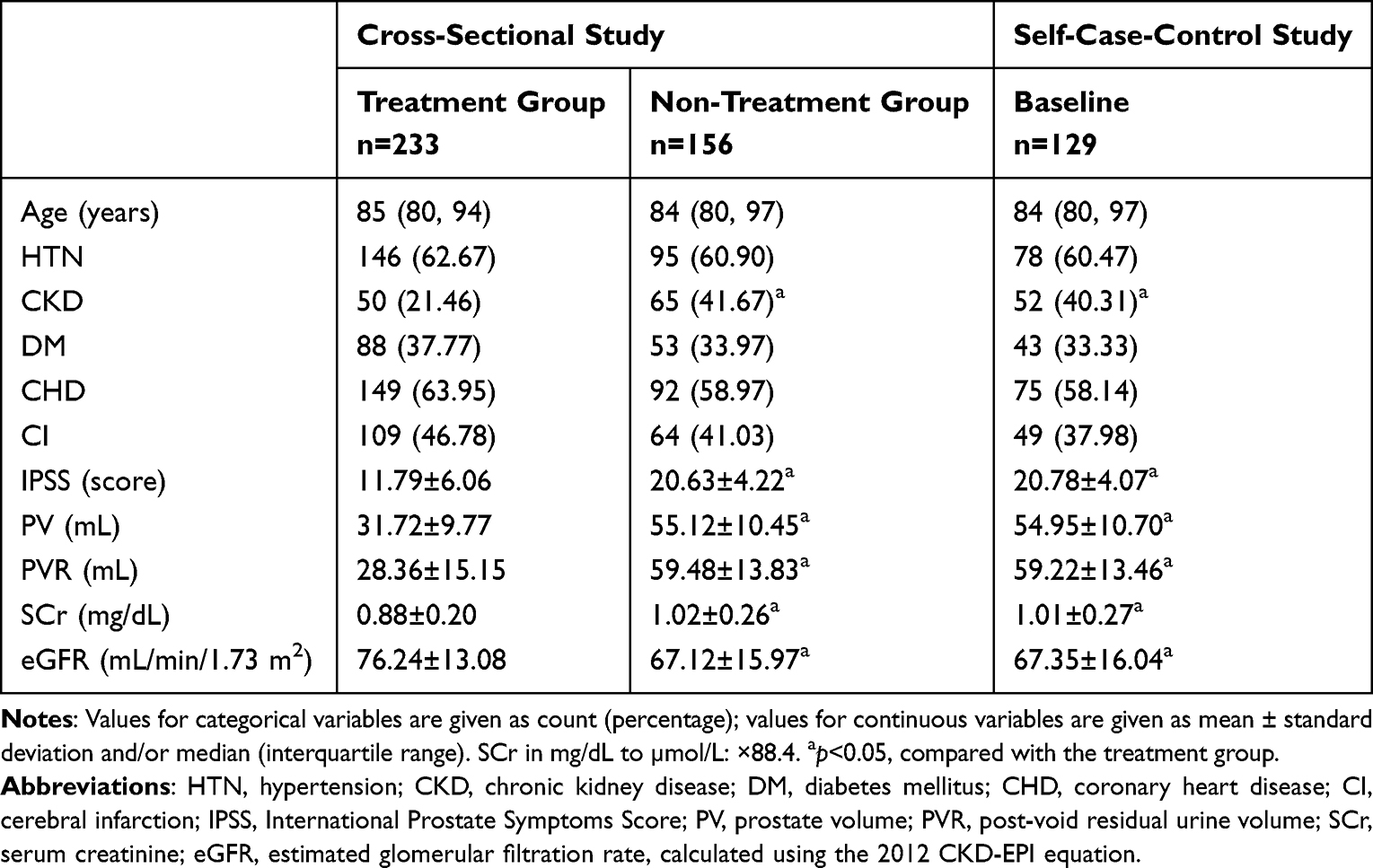 |
Table 1 Baseline Characteristics of Patients in the Cross-Sectional and Self-Case-Control Studies |
The characteristics of patients in the prospective self-case-control study are shown in Table 2. A total of 129 patients with BPH/LUTS were included, with an average age of 84 (80, 97) years. Among them, 78 patients (60.47%) had hypertension, 43 (33.33%) had diabetes, 75 (58.14%) had coronary heart disease, 49 (37.98%) had cerebrovascular diseases, and 52 (40.31%) had CKD 3a. There were no significant differences in age between the normal blood pressure and hypertension groups or between the normal renal function and CKD 3a groups (all p > 0.05). However, the incidences of coronary heart disease and CKD were significantly higher in the hypertension group than in the normal blood pressure group (both p < 0.05). Further, the incidence of hypertension was significantly higher in the CKD 3a group than in the normal renal function group (p < 0.05). There were no significant differences in the incidences of other diseases between the two groups (all p > 0.05).
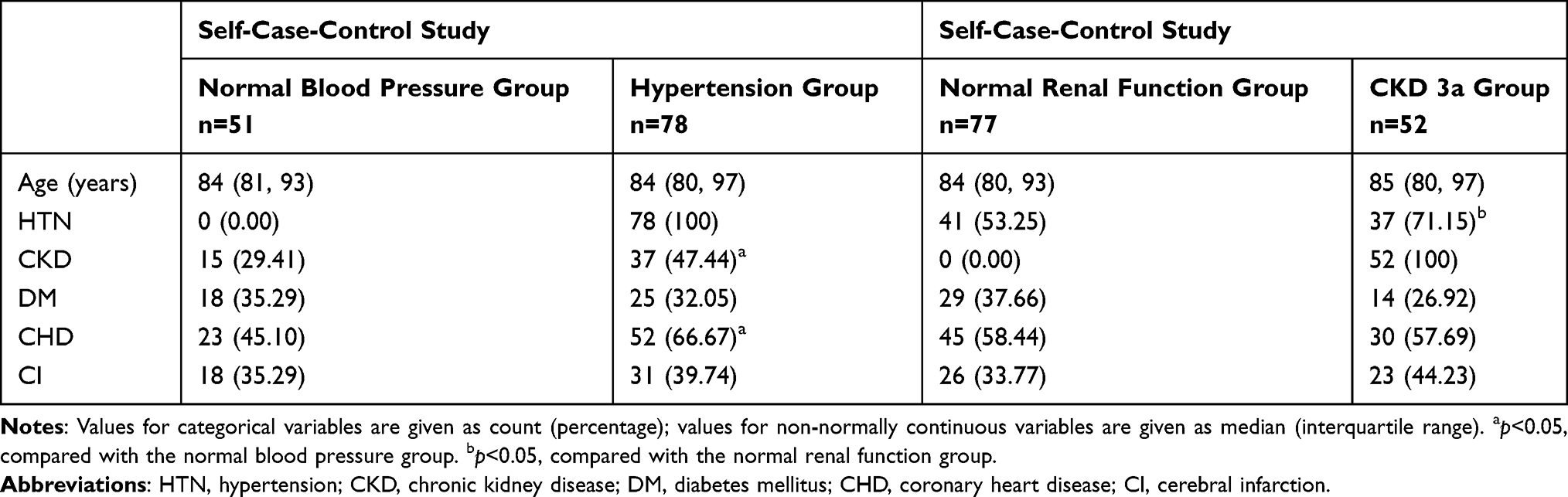 |
Table 2 Baseline Characteristics of Patients in the Self-Case-Control Study |
BPH-Related Indicators
In the cross-sectional study, PV, IPSS, and PVR were significantly lower in the treatment group than in the non-treatment group (all p < 0.05) (Table 1). In the prospective self-case-control study, the IPSS and PVR decreased significantly at 1, 3, and 6 months after treatment compared with those before treatment (p < 0.01); there was no significant change in the PV (p > 0.05) (Table 3).
 |
Table 3 Comparison of Renal Function and BPH-Related Indicators Before and After Treatment |
Renal Function-Related Indicators
In the cross-sectional study, the serum creatinine level of the treatment group was significantly lower than that of the non-treatment group (p < 0.05), and the eGFR of the treatment group was significantly higher than that of the non-treatment group (p < 0.05) (Table 1).
In the prospective self-case-control study, the serum creatinine level and eGFR did not significantly improve at 6 months after treatment compared with those before treatment (both p > 0.05) (Table 3). In the subgroup analysis, compared with the normal blood pressure and normal renal function groups, the hypertension and CKD 3a groups, respectively, showed significantly higher baseline serum creatinine levels (both p < 0.05). Further, the baseline eGFR of the CKD 3a group was significantly lower than that of the normal renal function group (p < 0.05). Renal function (serum creatinine level and eGFR) significantly improved after a 3-month treatment in the hypertension group and after a 1-month treatment in the CKD 3a group (all p < 0.05). There were no significant changes in the serum creatinine level or eGFR in the normal blood pressure and normal renal function groups at 6 months after treatment (all p > 0.05) (Table 4).
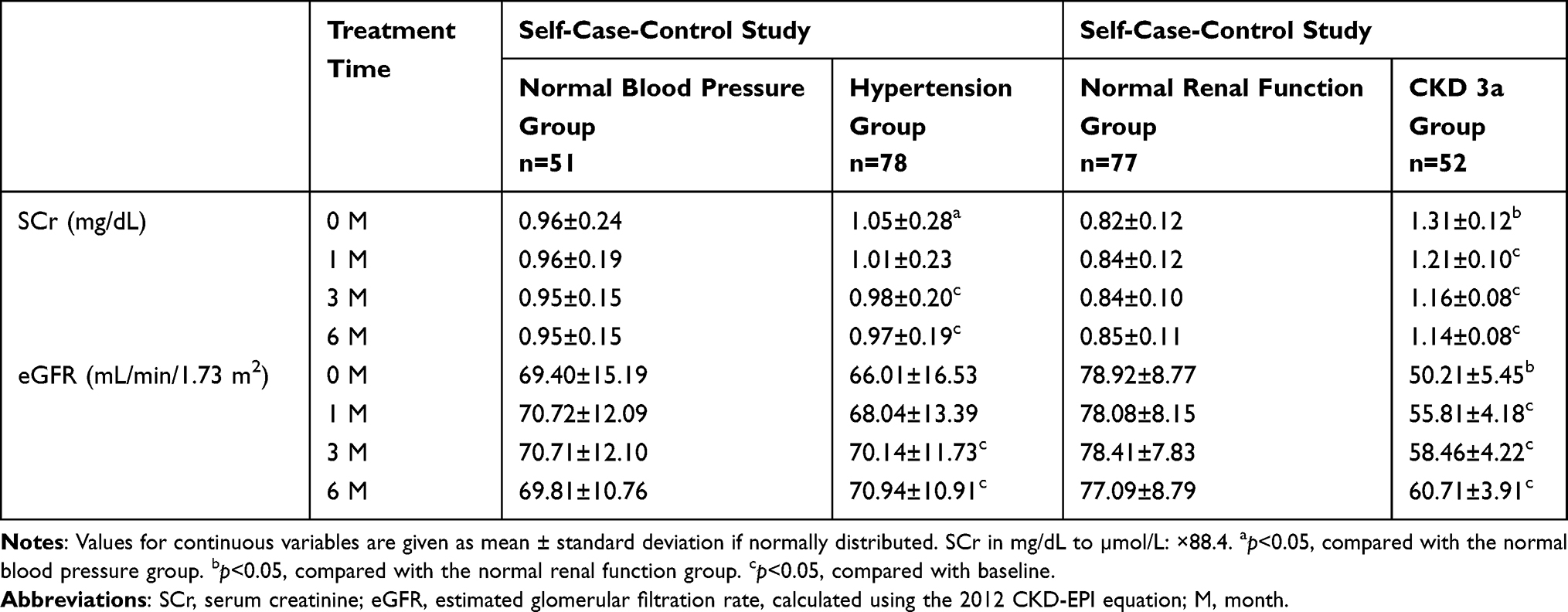 |
Table 4 Comparison of Renal Function Before and After Treatment in the Subgroups of the Self-Case-Control Study |
Risk Factors for Renal Function
In the prospective self-case-control study, the differences in serum creatinine levels and eGFR before and after treatment were used as dependent variables and clinical indicators of BPH, including age, coronary heart disease, hypertension, diabetes, CKD, baseline IPSS, baseline PV, and baseline PVR, were analyzed by multiple linear regression (Table 5). Hypertension (β=2.06 [95% CI, 0.40 to 3.71]) and CKD 3a (β=17.16 [95% CI, 15.53 to 18.79]) were independent risk factors for creatinine level differences before and after treatment (adjusted R2 of 0.808, F[3,50] = 63.186, all p < 0.05), whereas hypertension (β=−2.27 [95% CI, −3.65 to −0.89]), CKD 3a (β=−11.93 [95% CI, −13.29 to −10.58]), and baseline PV (β=−0.11 [95% CI, −0.20 to −0.02]) were independent risk factors for differences in eGFR before and after treatment (adjusted R2 of 0.754, F[3,50]=46.092, all p < 0.05). Therefore, multiple linear regression analysis showed that hypertension, CKD 3a, and baseline PV were the factors influencing renal function improvement after drug treatment for BPH.
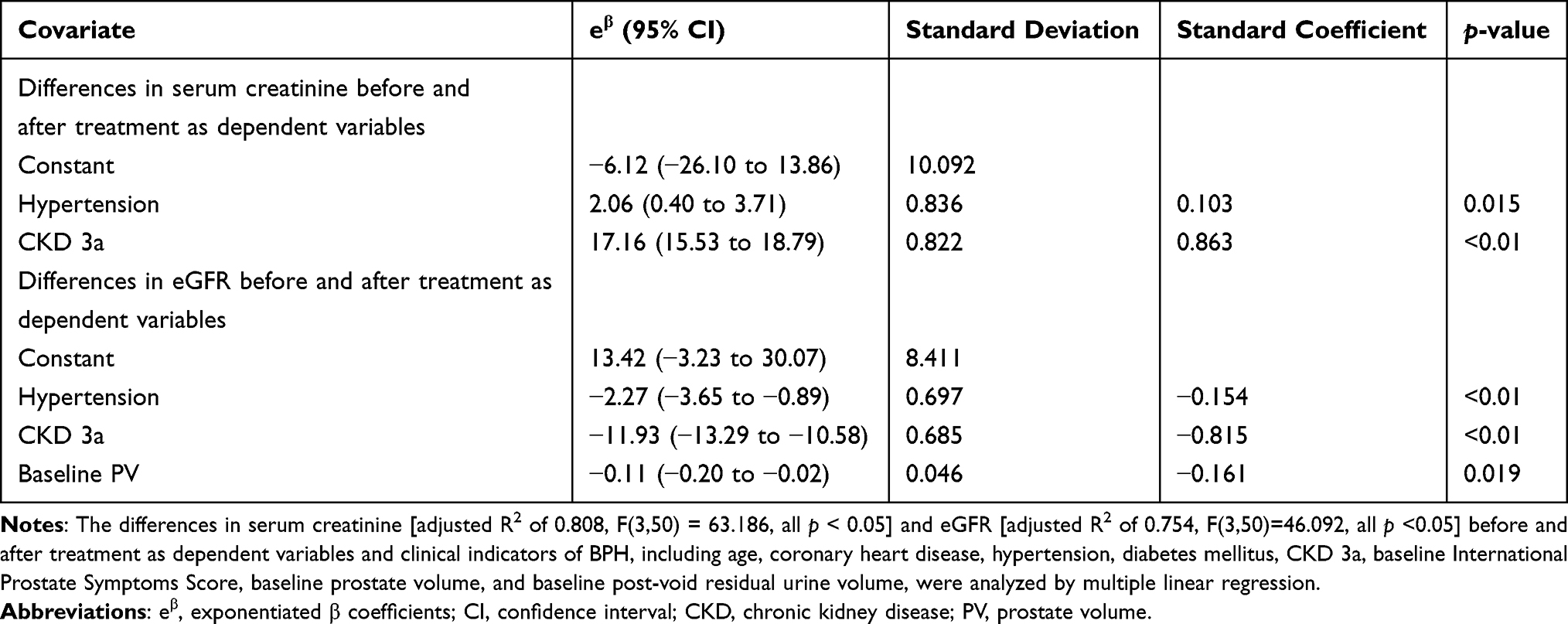 |
Table 5 Linear Regression for the Differences in Renal Function (Serum Creatinine and eGFR) Before and After Treatment as Dependent Variables (as a Continuous Variable) |
Discussion
CKD is a multifactorial disease.2,9 BPH can aggravate the progression of CKD in some patients with hypertension- and diabetes-related CKD.10 In our study, elderly men aged 80 years and older with normal or slightly impaired renal function were selected as the research subjects. Men over 80 years old have a reduced renal reserve function, poor compensatory ability, and sensitive response to external adverse stimuli,2 including BPH and hypertension. Therefore, observing early changes in the glomerular filtration rate in patients with normal serum creatinine levels can accurately reflect the influence of BPH on renal function. We first analyzed the relationship between BPH and renal function in elderly men over 80 years old by a cross-sectional study. The results showed that prostate indicators (PV, IPSS, and PVR) and renal function (serum creatinine level and eGFR) in the treatment group were significantly better than those in the non-treatment group. Therefore, renal function can be ameliorated by improving LUTS and reducing PVR, which relieves the post-renal pressure. A further prospective self-case-control study showed that oral finasteride and tamsulosin treatment in patients over 80 years old with BPH/LUTS improved the symptoms of BPH/LUTS, but renal function did not change. Subgroup analysis showed that patients with BPH/LUTS and hypertension or CKD 3a achieved an improvement in their renal function to some extent after treatment for BPH/LUTS. The multiple linear regression model showed that hypertension and CKD 3a were independent risk factors for renal function improvement after BPH/LUTS treatment.
Multimorbidity and comorbidity are clinical characteristics of the elderly,9 and it is common for elderly men to have BPH and a decreased glomerular filtration rate. Old age, high BMI, hypertension, diabetes, and cardiovascular diseases are independent risk factors for a decreased glomerular filtration rate.2,9,11 In addition to LUTS, BPH can cause acute urinary retention, post-renal renal failure, and uremia.1,4 However, oral BPH/LUTS drug administration and surgical intervention have decreased the incidences of severe obstructive nephropathy and renal failure caused by BPH/LUTS.
The 1994 AUA clinical practice guidelines on BPH recommended that men with LUTS be regularly screened for serum creatinine,12 but regular screening is no longer recommended following the 2003 update.5 This was changed because a clinical trial evaluating BPH treatment indicated a low incidence of CKD among these patients.12 However, the European Association of Urology guidelines on non-neurogenic LUTS recommend renal function evaluation before surgery if an abnormal renal function is suspected based on the patient’s medical history and clinical examination,13 suggesting a possible correlation between renal function and LUTS. Previous studies have shown that acute and chronic renal failure caused by acute and chronic urinary retention is uncommon, but with the aging of the population, there is an increasing incidence of patients with BPH complicated with acute and chronic kidney diseases.4 Rule et al4 retrospectively analyzed the literature concerning BPH and chronic renal failure (serum creatinine 1.5–3.0 mg/dL) from 1966 to 2003 and demonstrated that factors related to chronic urinary retention, such as a higher PVR (>300 mL), detrusor instability, and decreased bladder compliance, all correlated with chronic renal failure, and renal function improved significantly after prostatectomy, suggesting that obstructive BPH correlated with renal function. A prospective cohort study9 of 30,466 men (accounting for 66.8% of Norwegian men from the HUNT II study) analyzed the risk of future kidney failure in men with LUTS by IPSS, with an average follow-up of 10.5 years. The outcome was future kidney failure defined as starting renal replacement therapy or death from CKD with an eGFR <15 mL/min/1.73 m2. The risks of kidney failure were 2.60 and 4.08 times higher for men with moderate and severe LUTS compared with men with no/mild LUTS, respectively. After adjusting for age, the risk was still 1.27 times greater in men with moderate or severe LUTS. Although there was no causal relationship between LUTS and renal failure in the multivariate Cox regression analysis, the authors still recommended renal function screening for men aged over 60 years with moderate and severe LUTS with hypertension, diabetes, or cardiovascular disease. In cross-sectional studies of 2115 male community residents,14 2741 outpatients with BPH/LUTS,15 and male police officers with moderate to severe LUTS with an average age of 50 years,16 after adjusting for factors such as age, hypertension, diabetes, metabolic syndrome, and urinary infection, CKD mainly correlated with a decreased peak flow rate. In men without known urinary tract disease, LUTS and renal function had a negative association, especially in older men.17 In men over 50 years old with a bladder outlet obstruction, the eGFR in patients with a normal maximum flow rate was significantly higher than that in patients with a decreased maximum flow rate (81±17 mL/min/1.73 m2 vs 65±25 mL/min/1.73 m2).18 In retrospective studies of BPH/LUTS in renal transplantation recipients, serum creatinine, IPSS, and PVR significantly decreased after 1 and 6 months of prostate surgery.19,20 Although the causal relationship between moderate to severe LUTS or a decreased peak flow rate and CKD has not been clearly defined, they are closely correlated clinically and deserve attention.
However, some clinical trials have not confirmed a correlation of LUTS and PV with the development and progression of CKD.21–23 This might be related to the relatively young age, small sample size, and high serum creatinine level at the endpoint of these studies.
Currently, the average age in studies on BPH/LUTS is mostly less than 80 years old, and there is a lack of data on BPH/LUTS in individuals over 80 years old. The symptoms of BPH/LUTS in this population are severe, the proportions of multimorbidity with hypertension and CKD are high, and the reserve capacity and compensatory ability of the kidneys are significantly reduced. Recent studies have shown that holmium laser enucleation of the prostate should be a safe and efficient option even in patients over 80 years old if they are unable to take LUTS medications due to side effects.24,25 Further, these patients are relatively sensitive to various adverse stimuli, including increases in post-renal pressure caused by BPH/LUTS. Therefore, interventions on this basis may have a significant effect on improving renal function. In our study, we showed that BPH/LUTS may accelerate the progression of renal dysfunction in patients over 80 years old with hypertension and CKD 3a.
This study had some limitations. Our follow-up was limited to 6 months and lacked randomized double-blind controlled study data. It is difficult to carry out real-world studies in elderly patients aged 80 years and older because of increased multimorbidity and comorbidity, greater differences in geriatric syndromes and polypharmacy, and higher rates of missing follow-up. Moreover, because patients with BPH/LUTS have severe symptoms and a high demand for treatment, it is impossible to conduct randomized double-blind controlled studies. Therefore, our conclusion needs further study, including larger sample sizes and extending the follow-up period to observe the stability of the treatment outcome.
Conclusion
Treatment for moderate and severe BPH/LUTS can improve renal function in elderly patients with hypertension or CKD 3a.
Data Sharing Statement
All data generated or analyzed during this study are included in the article. Further inquiries can be directed to the correspondence author.
Acknowledgments
We are grateful to all the individuals who participated in this study. We also thank the staff of The Second Division of General Geriatrics for their contributions to this work.
Author Contributions
All authors contributed significantly to this work, whether it be in ideation, study design, implementation, data collection, analysis, and interpretation, or in all of these areas. They also participated in writing, revising, or critically evaluating the article; provided their final approval for the version that will be published; agreed on the journal to which the article will be submitted; and agreed to be responsible for all aspects of the work.
Funding
This work was supported by the Key Scientific and Technological Projects in the Department of Science and Technology of Henan Province (grant number 222102310435 to QW) and the Major Projects of Scientific and Technological Innovation 2030 “new generation of artificial intelligence” in China (grant number 2021ZD0111001 to RT).
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Madersbacher S, Sampson N, Culig Z. Pathophysiology of benign prostatic hyperplasia and benign prostatic enlargement: a mini-review. Gerontology. 2019;65(5):458–464. doi:10.1159/000496289
2. O’Sullivan E, Hughes J, Ferenbach D. Renal aging: causes and consequences. J Am Soc Nephrol. 2017;28:407–420. doi:10.1681/ASN.2015121308
3. Tamalunas A, Westhofen T, Schott M, et al. Holmium laser enucleation of the prostate: a truly size-independent method? Low Urin Tract Symptoms. 2022;14:17–26. doi:10.1111/luts.12404
4. Rule AD, Lieber MM, Jacobsen SJ. Is benign prostatic hyperplasia a risk factor for chronic renal failure? J Urol. 2005;173:691–696. doi:10.1097/01.ju.0000153518.11501.d2
5. AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: diagnosis and treatment recommendations. J Urol. 2003;170(170):530–547. doi:10.1097/01.ju.0000078083.38675.79
6. Welliver C, Feinstein L, Ward J, et al. Poor clinical guideline adherence and inappropriate testing for incident lower urinary tract symptoms associated with benign prostatic hyperplasia. Prostate Cancer Prostatic Dis. 2022;25(2):269–273. doi:10.1038/s41391-021-00435-z
7. Zhang X, Wang X, Wang G, et al. Clinical guideline for the diagnosis and treatment of benign prostatic hyperplasia. Chin J Surg. 2007;45:1704–1707.
8. Lerner L, McVary K, Barry M, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA GUIDELINE PART I-initial work-up and medical management. J Urol. 2021;206:806–817. doi:10.1097/JU.0000000000002183
9. Stevens P, Lamb E, Levin A. Integrating guidelines, CKD, multimorbidity, and older adults. Am J Kidney Dis. 2015;65:494–501. doi:10.1053/j.ajkd.2014.09.024
10. Hallan S, Kwong D, Vikse B, Stevens P. Use of a prostate symptom score to identify men at risk of future kidney failure: insights from the HUNT II Study. Am J Kidney Dis. 2010;56:477–485. doi:10.1053/j.ajkd.2010.03.021
11. Malhotra R, Katz R, Jotwani V, et al. Estimated GFR variability and risk of cardiovascular events and mortality in SPRINT (Systolic Blood Pressure Intervention Trial). Am J Kidney Dis. 2021;78:48–56. doi:10.1053/j.ajkd.2020.10.016
12. Gee W, Holtgrewe H, Albertsen P, et al. Practice trends in the diagnosis and management of benign prostatic hyperplasia in the United States. J Urol. 1995;154:205–206. doi:10.1016/S0022-5347(01)67269-0
13. Gratzke C, Bachmann A, Descazeaud A, et al. EAU guidelines on the assessment of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2015;67:1099–1109. doi:10.1016/j.eururo.2014.12.038
14. Rule A, Jacobson D, Roberts R, et al. The association between benign prostatic hyperplasia and chronic kidney disease in community-dwelling men. Kidney Int. 2005;67:2376–2382. doi:10.1111/j.1523-1755.2005.00344.x
15. Hong S, Lee S, Jeong S, et al. Chronic kidney disease among men with lower urinary tract symptoms due to benign prostatic hyperplasia. BJU Int. 2010;105:1424–1428. doi:10.1111/j.1464-410X.2009.08975.x
16. Lee J, Kwon H, Park Y, Cho I, Min S. Relationship of estimated glomerular filtration rate with lower urinary tract symptoms/benign prostatic hyperplasia measures in middle-aged men with moderate to severe lower urinary tract symptoms. Urology. 2013;82:1381–1385. doi:10.1016/j.urology.2013.07.049
17. Kwon Y, Cho B, Son K, Choi H, Park S, Park J. Lower urinary tract symptoms have negative associations with glomerular filtration rate irrespective of prostate volume in Korean men. Urology. 2012;79:182–187. doi:10.1016/j.urology.2011.08.011
18. Lai S, Pastore S, Piloni L, et al. Chronic kidney disease and urological disorders: systematic use of uroflowmetry in nephropathic patients. Clin Kidney J. 2019;12:414–419. doi:10.1093/ckj/sfy085
19. Sarier M, Tekin S, Duman İ, et al. Results of transurethral resection of the prostate in renal transplant recipients: a single center experience. World J Urol. 2018;36:99–103. doi:10.1007/s00345-017-2094-5
20. Sarier M, Duman I, Kilic S, et al. Comparative results of transurethral incision with transurethral resection of the prostate in renal transplant recipients with benign prostate hyperplasia. Urol J. 2018;15:209–213. doi:10.22037/uj.v0i0.4074
21. Hamm R, MacDermott S. Renal function in men with lower urinary tract symptoms at first presentation to urology out-patient department. Ann R Coll Surg Engl. 2004;86:182–185. doi:10.1308/003588404323043319
22. Ponholzer A, Temml C, Obermayr R, Rauchenwald M, Madersbacher S. The association between lower urinary tract symptoms and renal function in men: a cross-sectional and 5-year longitudinal analysis. J Urol. 2006;175:1398–1402. doi:10.1016/S0022-5347(05)00641-5
23. Abello A, DeWolf W, Das A. Expectant long-term follow-up of patients with chronic urinary retention. Neurourol Urodyn. 2019;38:305–309. doi:10.1002/nau.23853
24. Tamalunas A, Westhofen T, Schott M, et al. The impact of preoperative lower urinary tract symptoms medication on the functional performance of holmium laser enucleation of the prostate. Cent Eur J Urol. 2021;74:429–436. doi:10.5173/ceju.2021.130
25. Tamalunas A, Westhofen T, Schott M, et al. The clinical value of holmium laser enucleation of the prostate in octogenarians. Low Urin Tract Symptoms. 2021;13:279–285. doi:10.1111/luts.12366
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.