Back to Journals » Orthopedic Research and Reviews » Volume 14
Coronal Correction for Post-Traumatic Malalignment Using Robot-Assisted Total Knee Arthroplasty: A Case Series
Authors Baek JH, Lee SC, Ryu S, Ahn HS, Nam CH
Received 1 September 2022
Accepted for publication 15 November 2022
Published 22 November 2022 Volume 2022:14 Pages 445—451
DOI https://doi.org/10.2147/ORR.S387957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Ji-Hoon Baek,1 Su Chan Lee,1 Suengryol Ryu,2 Hye Sun Ahn,1 Chang Hyun Nam1
1Joint & Arthritis Research, Department of Orthopaedic Surgery, Himchan Hospital, Seoul, Republic of Korea; 2Department of Orthopaedic Surgery, Himnaera Hospital, Busan, Republic of Korea
Correspondence: Chang Hyun Nam, Joint & Arthritis Research, Department of Orthopaedic Surgery, Himchan Hospital, 120, Sinmok-ro, Yangcheon-gu, Seoul, 07999, Republic of Korea, Tel +82-2-3219-9229, Fax +82-2-2061-8605, Email [email protected]
Background: Achieving proper axis alignment can be difficult in the presence of posttraumatic extra-articular deformities in either the femur or the tibia. We present radiological outcomes following robot-assisted total knee arthroplasty (TKA) in patients with osteoarthritis of the knee accompanied by posttraumatic extra-articular deformities.
Methods: We analyzed the outcomes of five knees in five patients with (1) Kellgren-Lawrence (K-L) Grade III–IV osteoarthritic knees, (2) the presence of posttraumatic extra-articular deformities either in the femur or the tibia, and (3) who underwent robot-assisted TKA. Their radiological findings were evaluated.
Results: All five knees with initial deformity (mean 14.8°, range 12.7– 18.5°) were corrected to neutral alignment (mean 0.7°, range − 1.1– 2.7°). There was no postoperative outlier of hip-knee-ankle (HKA) angle.
Conclusion: Our results indicate that robot-assisted TKA can be used to achieve proper limb alignment in patients with posttraumatic extra-articular deformities.
Keywords: total knee arthroplasty, robot-assisted, outcomes
Introduction
Restoration of proper coronal alignment is important in total knee arthroplasty (TKA) for maximal implant longevity and increased patient function.1,2 Several studies have demonstrated that severe preoperative malalignment can result in greater risk of implant failure and early revision, and that proper correction of malalignment can reduce the risk of failure.3,4 However, proper axis alignment can be difficult in cases of severe varus or valgus deformity and is technically demanding, especially in the presence of posttraumatic extra-articular deformities either in the femur or the tibia.5,6 Therefore, technological advancements in surgery have sought to address alignment challenges in extra-articular deformities.
Robot-assisted TKA surgery has been developed to achieve more appropriate coronal alignment compared with conventional TKA surgery.7–9 Many studies have shown that mechanical axis accuracy is improved using robot-assisted systems, and mechanical axis outlier risk is decreased compared to conventional surgery.10–12 However, few studies have addressed the radiological result of robot-assisted TKA in patients with posttraumatic extra-articular deformities either in the femur or the tibia.
This study reports radiological outcomes following robot-assisted TKA in patients with osteoarthritis of the knee accompanied by posttraumatic extra-articular deformities.
Materials and Methods
The design and protocol of this retrospective study were approved by the institutional review board of our hospital. A comprehensive agreement for academic use of information such as type of treatments, treatment progress or any other data acquired during their treatments was obtained from the patients by the hospital at the time of their hospitalization, and that no identifiable information of the participants is included in the manuscript. The robot-assisted TKA system was introduced to our hospital in June 2020. Between July 2020 and December 2020, a consecutive series of 127 primary TKAs for 96 patients was performed at our hospital by a single surgeon using a robot-assisted system. The inclusion criteria were patients with (1) Kellgren-Lawrence (K-L) Grade III–IV osteoarthritic knees, (2) the presence of posttraumatic extra-articular deformities either in the femur or the tibia, and (3) who underwent robot-assisted TKA. Five knees in five patients with knee osteoarthritis (OA) were treated by robot-assisted TKA at our hospital and were analyzed. The cohort consisted of three males and two females with an average age at the time of surgery of 67.2 years (range: 58–73 years) and a mean body mass index of 25.0 kg/m2 (range: 22.7–28.7).
All operations were performed by a single experienced surgeon using a MAKO robotic system (Stryker Orthopaedics, Mahwah, NJ, USA). All patients were treated using a posterior-stabilized Triathlon total knee prosthesis (Stryker Orthopaedics, Mahwah, NJ, USA). Prior to the surgery, a preoperative CT scan was performed and incorporated with the robotic software to identify optimal implant size and positioning. In the operating room, all knees were exposed with a standard anterior midline incision via medial parapatellar approach, and the patella was everted laterally. The anterior and posterior cruciate ligaments were removed from the notch. Robot-assisted tracking arrays13 and check points were positioned on the tibia and femur. Landmark calibration and bone registration were performed via the probe to identify real bone position and intraoperative coronal alignment. The knee was stressed manually to gauge proper tension in extension and flexion gap balancing and to gauge coronal alignment deformity correction without soft tissue release. Soft tissue release was performed in all five cases of severe coronal deformity including osteophyte removal. Appropriate implant position, orientation, and neutral alignment based on per gap balancing were defined and saved in the robot system following the surgeon’s approval. These measurements were incorporated in the MAKO robotic system to identify proper implant placement. The robotic arm saw was then used for distal femur, anterior cortex, posterior condyle, anterior chamfer, and posterior chamfer resection. And then tibial resection was performed within virtual boundaries set by the robot to protect the soft tissues. After box cutting, femoral and tibial trial assessments were performed. The femoral and tibial implants were implanted using bone cement, and polyethylene liner was deemed appropriate and impacted into place.
Patients were mobilized postoperatively with immediate weight-bearing as tolerated, and active exercise was initiated under supervision of a physiotherapist. Patients underwent clinical and radiographic follow-up at 2 weeks, 6 weeks, 3 months, 6 months, 9 months, and 12 months postoperatively, and then each year thereafter. The radiographic analysis included long-leg standing radiography from the pelvis to the ankle joint to evaluate the axis, a weight-bearing anteroposterior view, a non-weight-bearing anteroposterior view, a lateral view at 30° flexion, and a skyline view of the patella. Radiographic analysis included coronal alignment (hip-knee-ankle (HKA)), flexion angle of the femoral component, and posterior tibial slope. Outliers were defined as measured HKA angle exceeding 3° from the neutral alignment in postoperative radiography.
Results
Patient clinical and radiographic information on all 5 cases of posttraumatic extra-articular deformity is presented in Table 1. The intraoperative planning target in the robot-assisted system was neutral alignment. All five knees with initial deformities (mean 14.8°, range 12.7–18.5°) were corrected to neutral alignment (mean 0.7°, range −1.1–2.7°) (Figures 1–5). Mean postoperative flexion angle of the femoral component was 3.8° (range 3.5–4.2°) and mean postoperative posterior tibial slope was 1.9° (range 1.6–2.3°). There was no postoperative outlier in HKA angle and the postoperative component alignments were within normal limits.
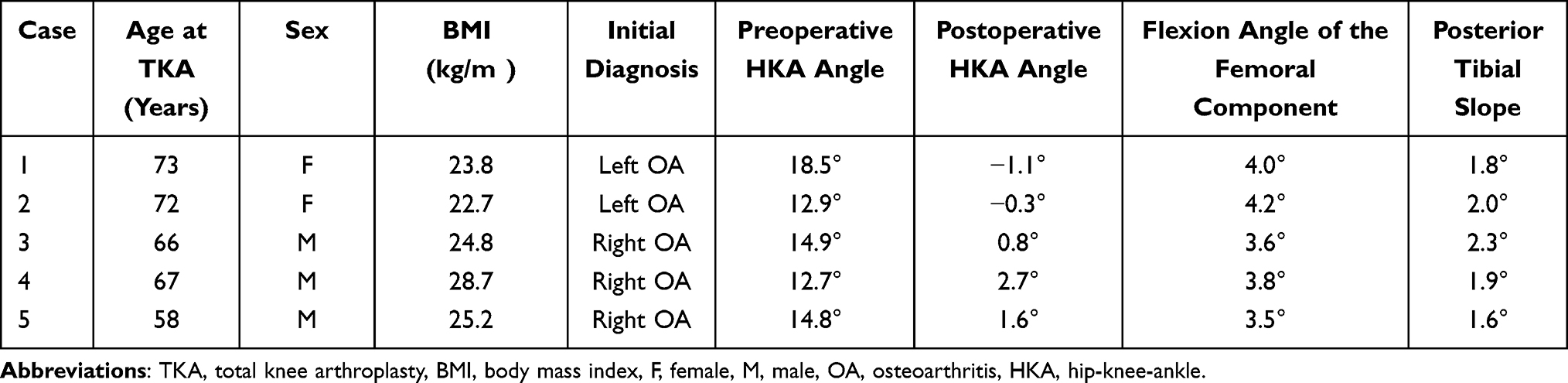 |
Table 1 The Demographics of Patients with Extra-Articular Deformity |
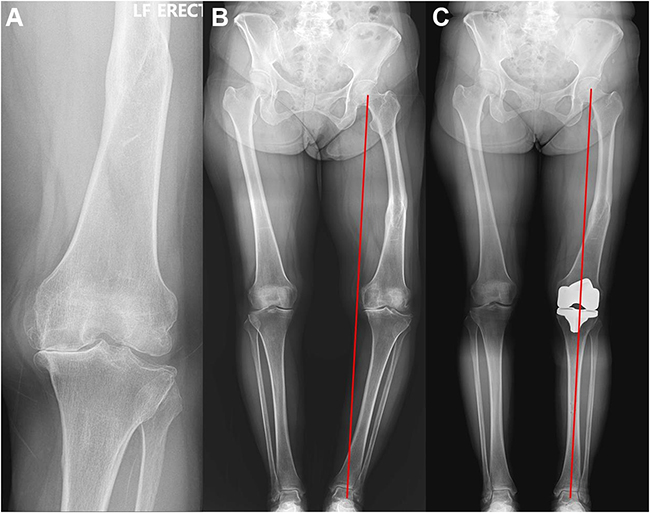 |
Figure 1 (A) An anteroposterior (AP) radiograph of a 73-year-old female patient who developed Kellgren-Lawrence Grade IV osteoarthritic changes in the left knee. Twenty-five years prior, she had undergone open reduction and internal fixation with a plate for a shaft fracture of the left femur. (B) A preoperative standing AP radiograph of the bilateral lower extremities of the same patient, which shows a left Hip-knee-ankle (HKA) angle of 18.5°. (C). A standing AP radiograph of the bilateral lower extremities of the same patient at four weeks postoperative, which revealed a −1.1° left HKA angle. |
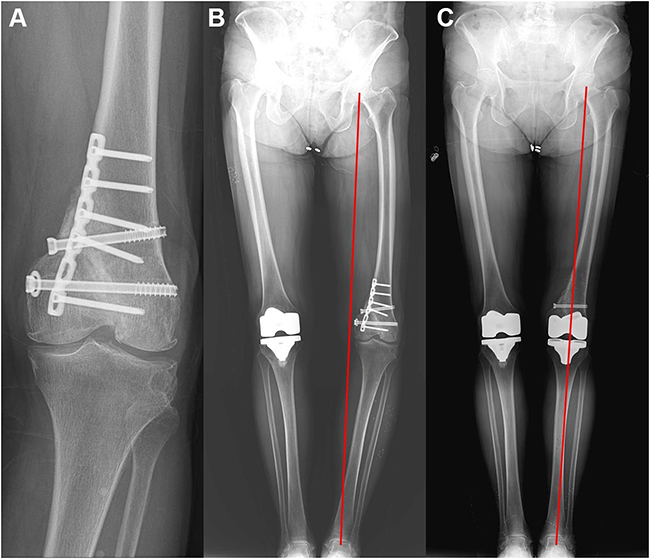 |
Figure 2 (A) An anteroposterior (AP) radiograph of a 72-year-old female patient who developed Kellgren-Lawrence Grade III–IV osteoarthritic changes in the left knee. Two years prior, she underwent open reduction and internal fixation with plate and screw for a left distal femoral fracture. (B) A preoperative standing AP radiograph of the bilateral lower extremities of the same patient, which shows a left Hip-knee-ankle (HKA) angle of 12.9°. (C) A standing AP radiograph of the bilateral lower extremities of the same patient at four weeks postoperative, which revealed a −0.3° left HKA angle. |
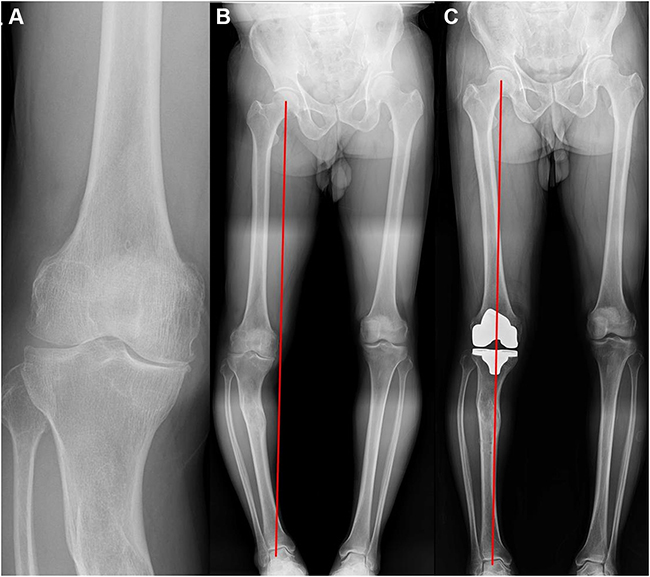 |
Figure 3 (A) An anteroposterior (AP) radiograph of a 66-year-old male patient who developed Kellgren-Lawrence Grade IV osteoarthritic changes in the right knee. Twenty years prior, he had undergone open reduction and internal fixation with a plate for a proximal shaft fracture of the right tibia. (B) A preoperative standing AP radiograph of the bilateral lower extremities of the same patient, which shows a right Hip-knee-ankle (HKA) angle of 14.9°. (C) A standing AP radiograph of the bilateral lower extremities of the same patient at four weeks postoperative, which revealed a 0.8° right HKA angle. |
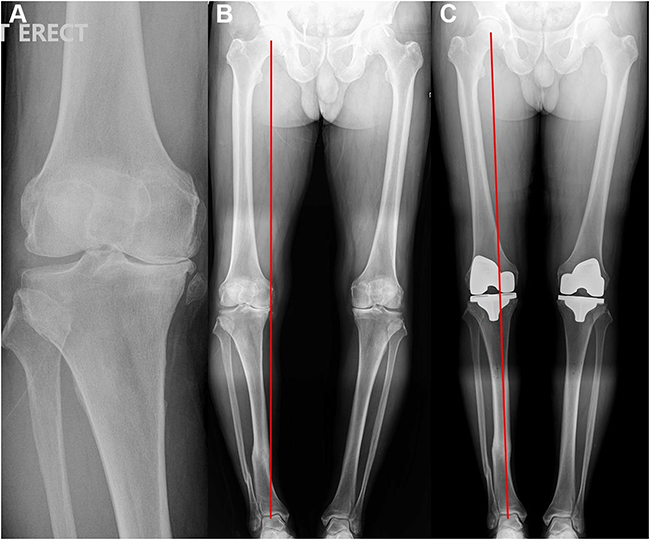 |
Figure 4 (A) An anteroposterior (AP) radiograph of a 67-year-old male patient who developed Kellgren-Lawrence Grade IV osteoarthritic changes in the right knee. Fifteen years prior, he underwent open reduction and internal fixation with a plate for a distal shaft fracture of the right tibia. (B) A preoperative standing AP radiograph of the bilateral lower extremities of the same patient, which shows a right Hip-knee-ankle (HKA) angle of 12.7°. (C) A standing AP radiograph of the bilateral lower extremities of the same patient at four weeks postoperative, which revealed a 2.7° right HKA angle. |
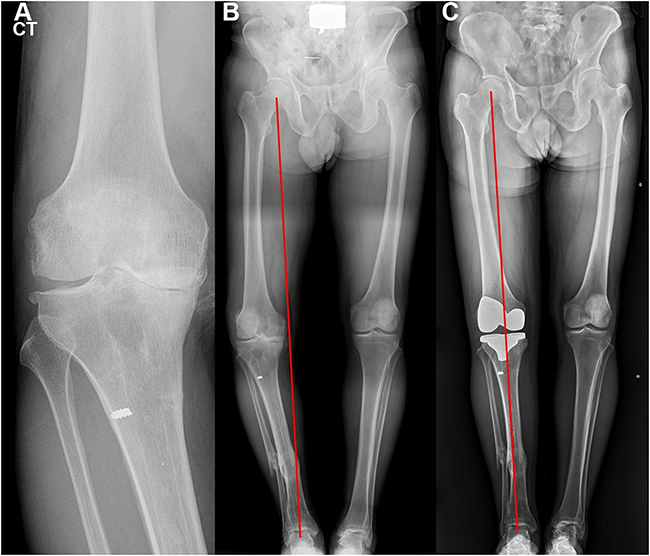 |
Figure 5 (A) An anteroposterior (AP) radiograph of a 58-year-old male patient who developed Kellgren-Lawrence Grade IV osteoarthritic changes in the right knee. Five years prior, he had undergone open reduction and internal fixation with an internal medullary nail (IM-nail) for a shaft fracture of the right tibia. (B) A preoperative standing AP radiograph of the bilateral lower extremities of the same patient, which shows a right Hip-knee-ankle (HKA) angle of 14.8°. (C) A standing AP radiograph of the bilateral lower extremities of the same patient at four weeks postoperative, which revealed a 1.6° right HKA angle. |
Discussion
This study analyzed a single surgeon’s experience using the robot-assisted system to help correct posttraumatic malalignment to proper alignment. The most important finding of this study was the advantages of the robot-assisted system during TKA in helping surgeons achieve planned proper limb alignment in cases of posttraumatic extra-articular deformities.
In the presence of posttraumatic extra-articular deformities either in the femur or the tibia accompanied by OA of knee, this can be difficult to achieve.5,6 Such situations may be encountered in clinical practice. In conventional TKA surgery, such deformity in the femur precludes the use of standard alignment instrumentation such as intramedullary guides, and achieving adequate limb alignment can be limited in these cases. Engh et al reported that the use of an extramedullary femoral guide in TKA is less accurate than the use of an intramedullary guide.14 Thus, robot-assisted surgery could be a viable alternative in cases involving patients with severe extra-articular deformity.
A previous report has shown improved limb alignment in patients with severe deformity when using a robot-assisted system.15 Marchand et al15 assessed primary TKAs using a robot-assisted system in 136 patients with severe varus or valgus (≥7° coronal deformity). They reported that all knees were corrected in the appropriate direction to within a few degrees of neutral alignment. On the other hand, we assessed primary TKAs using a robot-assisted system in patients who had only posttraumatic extra-articular deformity. The results of this study show that robot-assisted TKA can be considered an effective procedure in patients with posttraumatic extra-articular deformity. In addition, robot-assisted TKA has other advantages over conventional TKA. In cases in which hardware from a previous surgery, such as metal plate and screws, is present in the patient, robot-assisted TKA surgery does not necessitate its removal when doing so would be risky (Figure 2).
This study had several limitations. First, because it enrolled a relatively small cohort treated by a single surgeon, its outcomes should be interpreted with caution in terms of generalizability. Second, there were no patient-reported outcomes and no functional outcomes. In addition, postoperative alignment outcomes were not compared with clinical follow-up outcomes or a control group. Therefore, future research should consider whether correction of these deformities correlates with clinical outcomes and patient satisfaction.
Conclusions
In conclusion, robot-assisted TKA can be used to plan and achieve proper limb alignment in patients with posttraumatic extra-articular deformities. Although uncontrollable preoperative deformities exist in some patients, postoperative limb alignment can be controlled by a robot-assisted procedure.
Ethics Approval and Written Consent from the Patient
This study was approved by the Institutional Review Board of Himchan hospital. The privacy and personal identity information of all participants were protected in accordance with the Declaration of Helsinki. Written informed consent has been obtained from all participants.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cherian JJ, Kapadia BH, Banerjee S, Jauregui JJ, Issa K, Mont MA. Mechanical, anatomical, and kinematic axis in TKA: concepts and practical applications. Curr Rev Musculoskelet Med. 2014;7(2):89–95. doi:10.1007/s12178-014-9218-y
2. Rajgopal A, Vasdev A, Dahiya V, Tyagi VC, Gupta H. Total knee arthroplasty in extra articular deformities: a series of 36 knees. Indian J Orthop. 2013;47(1):35–39. doi:10.4103/0019-5413.106893
3. Teeny SM, Krackow KA, Hungerford DS, Jones M. Primary total knee arthroplasty in patients with severe varus deformity. A comparative study. Clin Orthop Relat Res. 1991;273:19–31. doi:10.1097/00003086-199112000-00005
4. Ritter MA, Davis KE, Davis P, et al. Preoperative malalignment increases risk of failure after total knee arthroplasty. J Bone Joint Surg Am. 2013;95(2):126–131. doi:10.2106/JBJS.K.00607
5. Lonner JH, Siliski JM, Lotke PA. Simultaneous femoral osteotomy and total knee arthroplasty for treatment of osteoarthritis associated with severe extra-articular deformity. J Bone Joint Surg Am. 2000;82(3):342–348. doi:10.2106/00004623-200003000-00005
6. Wang JW, Wang CJ. Total knee arthroplasty for arthritis of the knee with extra-articular deformity. J Bone Joint Surg Am. 2002;84(10):1769–1774. doi:10.2106/00004623-200210000-00005
7. Decking J, Theis C, Achenbach T, et al. Robotic total knee arthroplasty: the accuracy of CT-based component placement. Acta Orthop Scand. 2004;75(5):573–579. doi:10.1080/00016470410001448
8. Fadda M, Marcacci M, Toksvig-Larsen S, Wang T, Meneghello R. Improving accuracy of bone resections using robotics tool holder and a high speed milling cutting tool. J Med Eng Technol. 1998;22(6):280–284. doi:10.3109/03091909809010012
9. Siebert W, Mai S, Kober R, Heeckt PF. Technique and first clinical results of robot-assisted total knee replacement. Knee. 2002;9(3):173–180. doi:10.1016/s0968-0160(02)00015-7
10. Liow MHL, Xia Z, Wong MK, Tay KJ, Yeo SJ, Chin PL. Robot-assisted total knee arthroplasty accurately restores the joint line and mechanical axis. A prospective randomised study. J Arthroplasty. 2014;29(12):2373–2377. doi:10.1016/j.arth.2013.12.010
11. Song EK, Seon JK, Park SJ, Jung WB, Park HW, Lee GW. Simultaneous bilateral total knee arthroplasty with robotic and conventional techniques: a prospective, randomized study. Knee Surg Sports Traumatol Arthrosc. 2011;19(7):1069–1076. doi:10.1007/s00167-011-1400-9
12. Song EK, Seon JK, Yim JH, Netravali NA, Bargar WL. Robotic-assisted TKA reduces postoperative alignment outliers and improves gap balance compared to conventional TKA. Clin Orthop Relat Res. 2013;471(1):118–126. doi:10.1007/s11999-012-2407-3
13. Baek JH, Lee SC, Kim JH, Ahn HS, Nam CH. Distal femoral pin tracker placement prevents pin tract-induced fracture in robotic-assisted total knee arthroplasty. J Knee Surg. 2021. doi:10.1055/s-0041-1735462
14. Engh GA, Petersen TL. Comparative experience with intramedullary and extramedullary alignment in total knee arthroplasty. J Arthroplasty. 1990;5(1):1–8. doi:10.1016/s0883-5403(06)80002-1
15. Marchand RC, Sodhi N, Khlopas A, et al. Coronal correction for severe deformity using robotic-assisted total knee arthroplasty. J Knee Surg. 2018;31(1):2–5. doi:10.1055/s-0037-1608840
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.