Back to Journals » Clinical Ophthalmology » Volume 16
Corneal Topographic versus Manifest Refractive Astigmatism in Patients with Keratoconus: A Retrospective Cross-Sectional Study
Authors Elkadim M, Nasef MH ![]() , Alagorie AR
, Alagorie AR ![]() , Allam WA
, Allam WA ![]()
Received 6 February 2022
Accepted for publication 9 June 2022
Published 20 June 2022 Volume 2022:16 Pages 2033—2039
DOI https://doi.org/10.2147/OPTH.S361338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Mohamed Elkadim, Mohamed H Nasef, Ahmed Roshdy Alagorie, Waleed A Allam
Department of Ophthalmology, Faculty of Medicine, Tanta University, Tanta, Egypt
Correspondence: Mohamed Elkadim, Department of Ophthalmology, Faculty of Medicine, Tanta University, Tanta, Egypt, Email [email protected]
ABSTRACT:
Purpose: To compare the subjective manifest astigmatism to the corneal topographic astigmatism in patients with keratoconus.
Methods: This retrospective study included data of 230 keratoconic eyes of 115 patients. Topographic corneal astigmatism (TA), which was measured by pentacam, was compared and correlated to manifest refractive cylinder (MRC) in terms of power, axis, vector components, and mean vector. The difference between TA and MRC was correlated to the maximum keratometric reading (Kmax) and the thinnest pachymetry location (TL), as indicators of keratoconus severity.
Results: There was a significant positive correlation between MRC power and TA power (p < 0.001; r = 0.58). TA power was significantly higher than MRC power (p < 0.001). A significant correlation was present between the axis of TA and MRC (r = 0.73; p < 0.001) with the axis of the MRC tending to be more vertical (more against the rule) than the axis of TA. The vector difference between TA and MRC is correlated to the Kmax (p < 0.001; r = 0.62) and TL (p < 0.001; r = 0.3).
Conclusions: A significant difference is present between TA and MRC in keratoconic eyes, the power of MRC tends to be less and the axis tends to be more vertical than those of TA; this difference increases as keratoconus becomes more advanced.
Keywords: keratoconus, pentacam, tomographic astigmatism
Introduction
Keratoconus is one of the leading causes of visual impairment worldwide.1 Its main therapeutic modalities include corneal cross-linking, intracorneal ring segments, penetrating, and lamellar keratoplasty.2–4
Due to presence of irregular corneal astigmatism and high-order aberrations, accurate refraction is usually difficult in keratoconus patients.5 Eyes with keratoconus have approximately five to six times higher order aberrations than normal eyes, particularly vertical coma.6,7 Accurate refraction with measurement of best-corrected visual acuity is of paramount importance in keratoconus as it is crucial for decision-making, glasses prescription, and monitoring of disease progression. Furthermore, proper identification of cylinder power and axis is essential for planning intracorneal ring segments and toric intraocular lens implantation in suitable candidates.8
Objective refraction was found to be different from subjective manifest refraction in keratoconic eyes. In clinical practice, depending on the subjective trial alone could be difficult and time consuming, particularly in uncooperative patients. Identifying an objective tool to help guide the subjective trial makes it easier, quicker, and repeatable. Considering the fact that manifest refractive astigmatism is the sum of both corneal and lenticular astigmatism with the superadded effect of corneal higher-order aberrations,9 topographic astigmatism measured using the rotating Scheimpflug camera could provide a suitable starting point to initiate the subjective manifest refraction. The aim of this study is to compare topographic corneal astigmatism to subjective manifest astigmatism in keratoconic eyes and the impact of keratoconus severity on any disparities between those two methods.
Materials and Methods
This retrospective cross-sectional single-center observational study was carried out at the Department of Ophthalmology, Tanta University Eye Hospital, Tanta, Egypt. The study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Tanta University Faculty of Medicine. Based on the retrospective and the observational nature of the study, obtaining informed consent from the study participants was not required by the ethics committee. All patients’ data were deidentified to keep confidentiality and privacy.
The retrospective reviews included the records of 115 patients diagnosed with keratoconus at our hospital during the period from January 2017 to December 2021.
Inclusion criteria included patients with keratoconus diagnosed at any age. The diagnosis of keratoconus was based on clinical examination and corneal tomography (Pentacam HR; Oculus Optikgeräte, Wetzelar, Germany). Exclusion criteria included patients with previous corneal or lenticular surgery, cataract, corneal scarring, patients using hard contact lenses, patients with advanced keratoconus, and patients with concomitant ocular surface disorders.
Manifest refraction was performed, one eye at a time, by the same physician (WA) in dim illumination using a manual minus-cylinder phoropter (Reichert, Inc., New York. USA) and an automatic chart projector (ACP-8. Topcon Corp., Tokyo, Japan). The values of cycloplegic refraction obtained using retinoscopy or patient’s previous glasses prescriptions were used as a starting point in all subjective trials. The Donder’s method10 was used to determine the manifest refraction. First, the strongest plus lens or the weakest minus lens that offers the patient the best visual acuity was used. After adjusting the power of the spherical lens, subjects were asked to rotate the axis knob of the cylindrical lens on the phoropter till they get the sharpest vision in order to fine-tune the cylinder axis. Finally, the minus cylinder power was increased or decreased according to the effect on visual acuity.
Corneal tomography was performed to all subjects using a rotating Scheimpflug camera (Pentacam HR; Oculus Optikgeräte, Wetzelar, Germany). The quality status (QS) detected by the machine had to be OK for all maps included in the study. The data extracted from the maps included K1, K2, topographic astigmatism (power and axis), Kmax, and the thinnest location on the pachymetry map.
Topographic astigmatism (TA) and manifest refractive cylinder (MRC) were compared and correlated in terms of power, axis, and vector analysis. The vector components were calculated using previously described equations:11,12 X = C x cos (2A); Y = C x sin (2A), where “X” is the X-axis component of astigmatism, “Y” is the Y-axis component of astigmatism, “C” is the cylinder power, and “A” is the cylinder axis.
Vector difference between TA and MRC was calculated, and the mean vector of TA and MRC was calculated for right eyes and left eyes separately using Alpins vector analysis.11,13
All data collected in the study were entered into an electronic database via Microsoft Excel 2016 (Microsoft Corp., Redmond, WA). Statistical analysis was performed using the Statistical Package for Social Sciences software (SPSS. IBM Corp., Armonk, New York. USA) Version 16. Numerical variables were reported as Mean ± Standard Deviation (SD). Correlations were examined with Pearson’s correlation coefficient and Spearman rank correlation test. The Wilcoxon signed-rank test was used to test the difference between the two groups. A P value less than 0.05 was considered statistically significant.
Results
This study included 230 eyes of 115 patients, criteria of studied cases included age, visual acuity, manifest and topographic astigmatism, maximum k reading (Kmax), and thinnest pachymetry location (TL), and they are reported in Table 1.
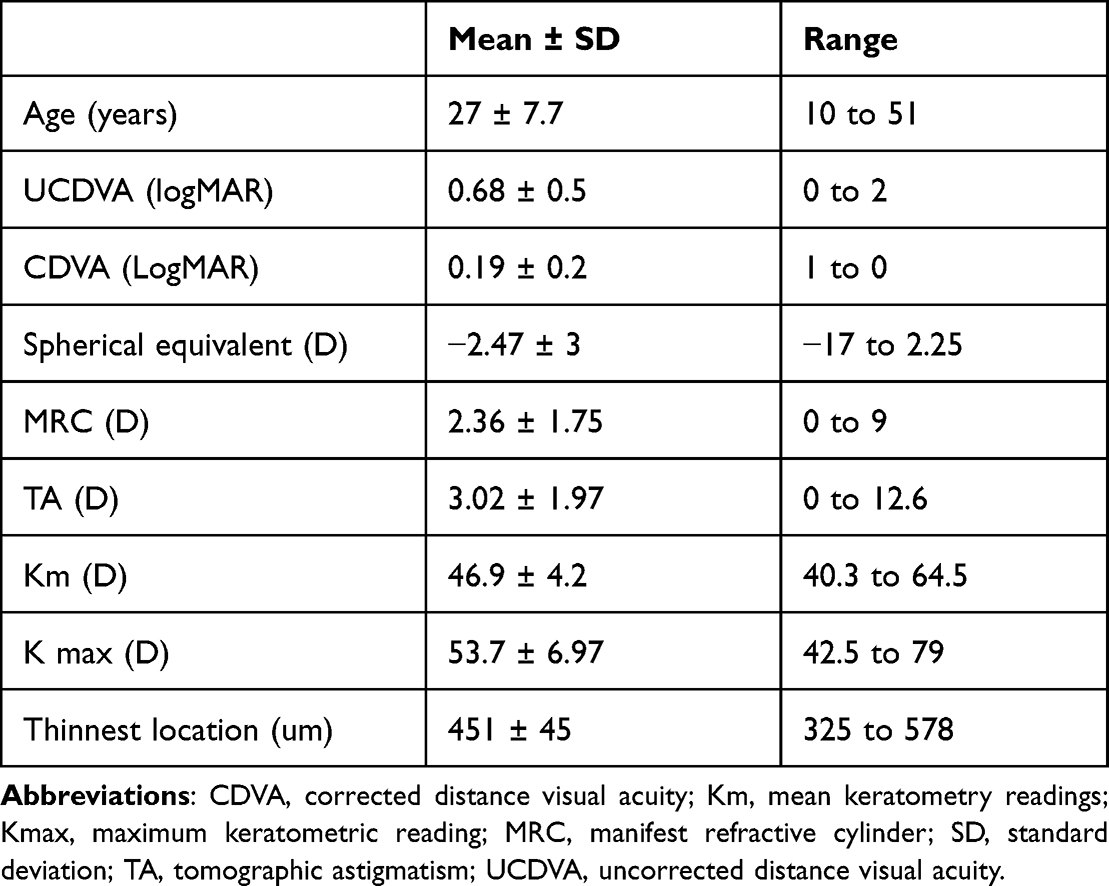 |
Table 1 Criteria of Studied Cases |
There was a statistically significant positive correlation between MRC power and TA power (r = 0.58; p < 0.001, Spearman correlation test) (Absolute agreement Interclass correlation coefficient ICC = 0.72) (Figure 1). Topographic astigmatism (TA) power was significantly higher than MRC power (p < 0.001) with a mean difference of 0.66 ± 1.72 diopter. Additionally, there was a significant correlation between the TA and the mean difference between TA and MRC (r = 0.56; p < 0.001, Spearman correlation test).
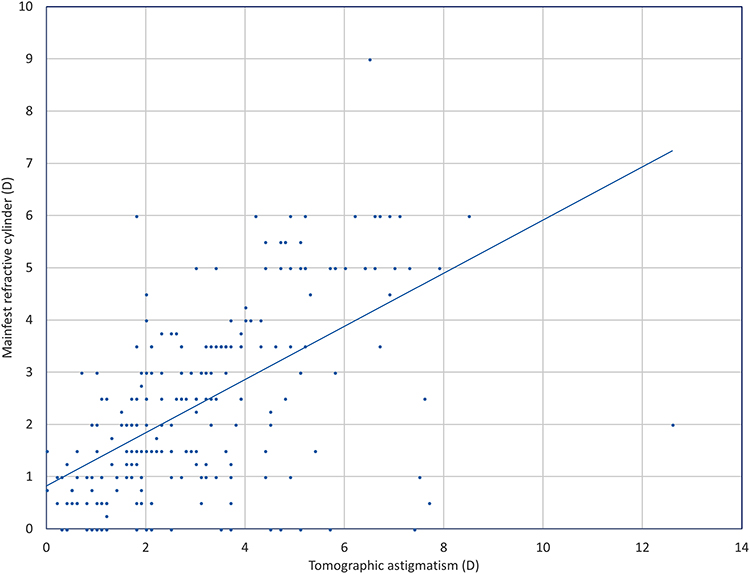 |
Figure 1 Correlation between power of topographic corneal astigmatism and manifest refractive astigmatism. |
As regards the astigmatism axis, a significant correlation was present between the axis of TA and MRC (r = 0.73; p < 0.001, Spearman correlation test) (Absolute agreement Interclass correlation coefficient ICC = 0.47). The axis of the MRC tends to be more vertical (more against the rule) than the axis of TA (Figures 2 and 3).
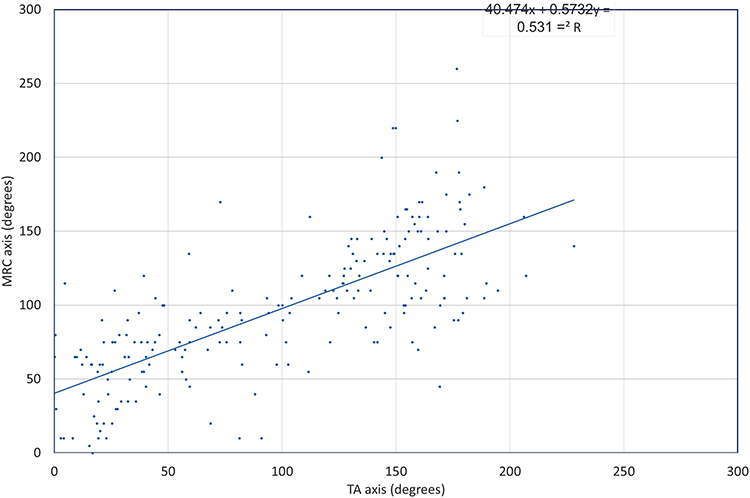 |
Figure 2 Correlation between axis of topographic corneal astigmatism (TA) and manifest refractive astigmatism (MRC). |
 |
Figure 3 Polar plot of astigmatism power and axis of studied cases; right eyes (OD) above and left eyes (OS) below. Abbreviations: TA, topographic astigmatism (blue triangles); MRC, manifest refractive cylinder (red triangles) showing more vertical orientation of MRC in comparison of TA. |
There was a significant difference between TA and MRC as regards X and Y components of vector analysis (Table 2); the vector difference between TA and MRC (VD) is correlated to the Kmax (r = 0.62; p < 0.001, Spearman correlation test) (Figure 4) and TL (r = 0.3; p < 0.001, Spearman correlation test). Multivariate regression analysis shows a significant correlation between VD and Kmax (Coefficient = 0.21; p < 0.0001), but not the thinnest location (Coefficient = 0.002; p = 0.49).
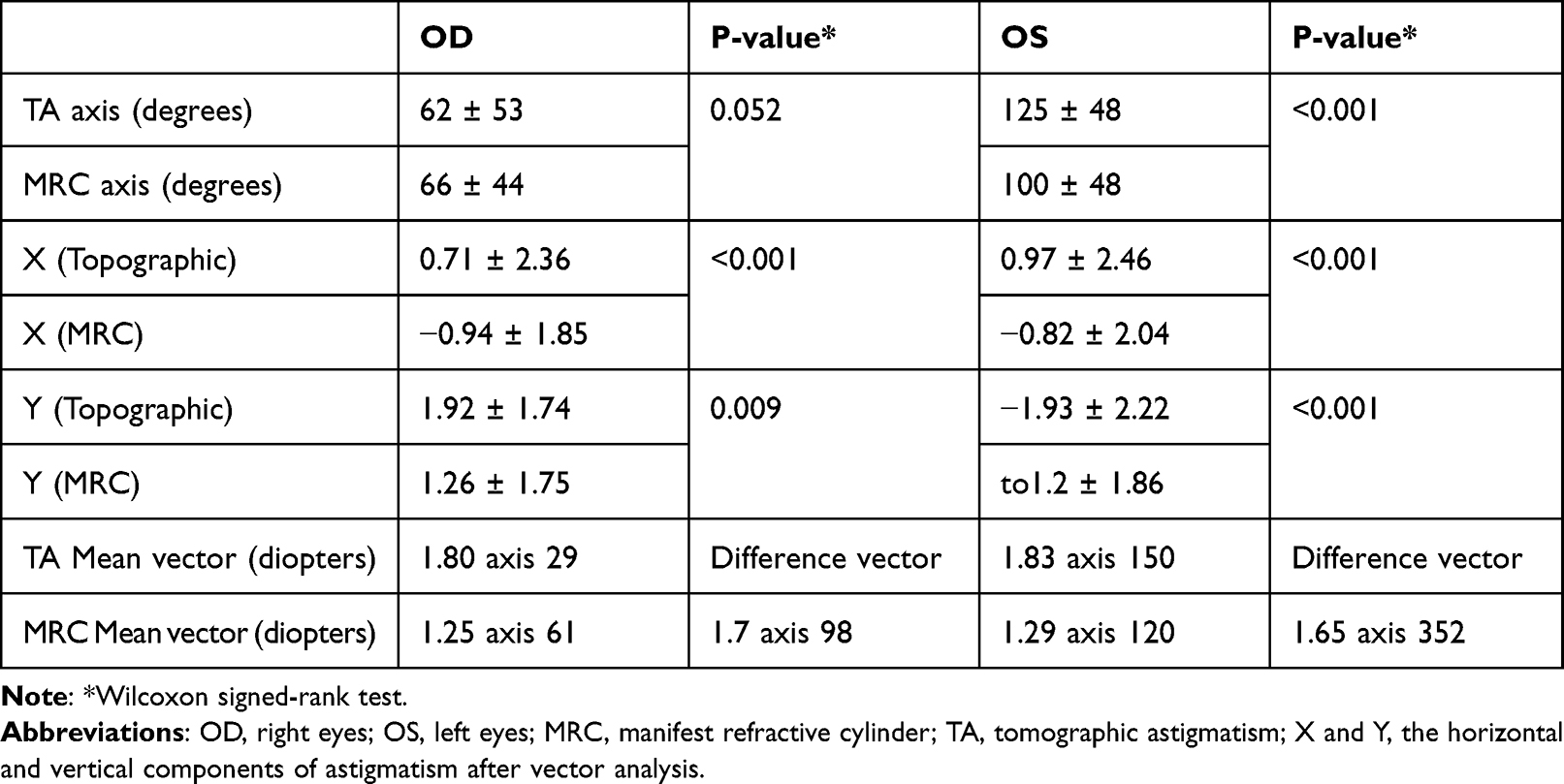 |
Table 2 Difference Between Axis of Tomographic Astigmatism (TA) and Manifest Refractive Cylinder (MRC) and Results of Vector Analysis |
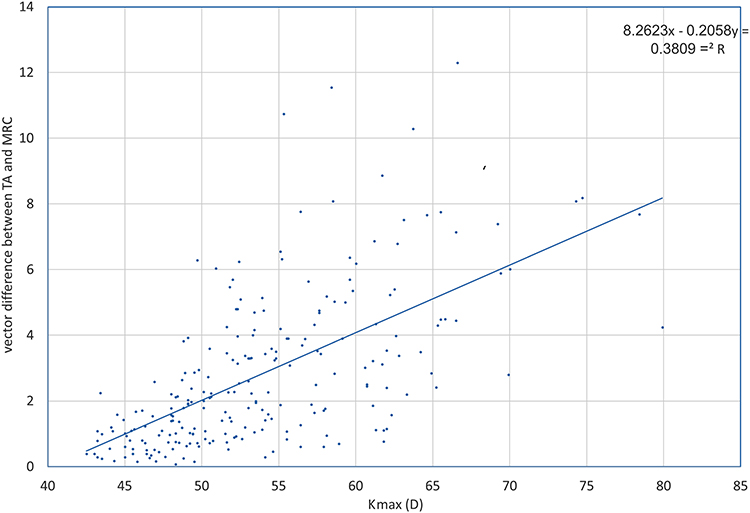 |
Figure 4 Correlation between Kmax (D) and vector difference between topographic and manifest astigmatism. |
Discussion
The cornea is responsible for about two-thirds of ocular refractive power, that is why the manifest astigmatism is expected to correlate to the corneal astigmatism.14 However, unlike normal corneas, keratoconic corneas have irregular astigmatism. Consequently, the relationship between the topographic corneal astigmatism and the manifest astigmatism is complicated by the higher order aberrations resulting from the corneal ectasia. The principal findings of this study were that the MRC power is supposed to be less than the TA power, the axis of the MRC tends to be more vertical (more against the rule) than the axis of TA, and this disparity in power and axis increases when the keratoconus is more advanced.
These findings could be explained by coma aberration that was found to refract as astigmatism.15 During subjective refraction, the resultant MRC power and axis will be a sum of two components: the astigmatism and the coma. In keratoconus, there is a high incidence of vertical coma resulting in astigmatism that tends to be against the rule. This is a finding of this study that the MRC axis tends to be more vertical than the TA axis that is relatively oblique. In Zhou’s small case series of irregular corneas, they found that vertical coma influenced manifest refractive cylinder by reducing the effect of (WTR) corneal astigmatism and increasing the effect of against-the-rule (ATR) astigmatism.15 This shift was also described in this study, with MRC being more vertical (ATR).
Another explanation is that the K readings of the pentacam represent the astigmatism of only the central 3 mm of the corneal that may not be representative of the effective corneal astigmatism.16 This may point to the need to revise our concept about simulated keratometry, which represents the power of the central 3 mm of the cornea only, if it is really the functional or effective corneal power or we have to go more peripheral, particularly in keratoconic corneas. Additionally, this concept was noted in a study that reported a relation between the axis of peripheral corneal astigmatism (8 mm rather than central 3 mm) in keratoconic corneas and postoperative astigmatism after deep anterior lamellar keratoplasty.17 A previous study in non-keratoconic eyes reported reduction in the power of peripheral corneal astigmatism in comparison to central corneal astigmatism.18 Another study reported the same results, with more difference between central and peripheral astigmatism in patients with against the rule, oblique and high astigmatism.19 A comprehensive study of corneal, central and peripheral, anterior, and posterior astigmatism, and the impact of corneal changes on optical performance in keratoconic eyes is therefore recommended to develop a more accurate strategies for visual rehabilitation procedures.
The more advanced the cone, the more the impact of high order aberration on the manifest refraction. That is why readings of autorefractors are usually not accurate.20 Pentacam TA despite showing disparity with MRC, a good correlation still could be found particularly in less advanced cases. Among the benefits that can be obtained from these results is finding a relation between TA and MRC in advanced keratoconus, for such cases using the TA power and axis unmodified for glasses prescription, intracorneal ring segment planning, biometry calculation or toric IOL orientation may be deceiving. Any procedure for visual rehabilitation in keratoconic eyes should certainly consider correction of manifest rather than topographic astigmatism if it is a corneal procedure or neutralizing this manifest astigmatism in a lenticular procedure.
The concept behind correlating the topographic to MR is to understand how the KC eye sees and how to best compensate for the error. Rendering the keratoconus patient with useful vision independent of rigid contact lens or keratoplasty is the pinnacle of success of keratoconus subjective refraction.
Our study has some limitations including its retrospective design, with the possibility of selection bias, and lack of assessment of high order aberrations which have impact on vision and refraction in eyes with keratoconus.
Conclusion
The topographic astigmatism (TA) should not be used unprocessed in decision-making or glasses prescription as it demonstrated difference in power and axis in comparison to MRC, with MRC tending to be less in power and more vertical in the axis in comparison to TA; this disparity becomes more evident as the keratoconus becomes more advanced. These findings may help clinicians to use the TA as a guide to help in finding the MRC based on the relation between both and to obtain more accurate refraction in patients with keratoconus.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Maskari AZ. Keratoconus in high-prevalence populations: is it time for a screen-and-crosslink approach?. Oman J Ophthalmol. 2018;11:193–194. doi:10.4103/ojo.OJO_202_2018
2. Santodomingo-Rubido J, Carracedo G, Suzaki A, Villa-Collar C, Vincent SJ, Wolffsohn JS. Keratoconus: an updated review. Contact Lens Anterior Eye. 2022;101559. doi:10.1016/j.clae.2021.101559
3. Rechichi M, Mazzotta C, Oliverio GW, et al. Selective transepithelial ablation with simultaneous accelerated corneal crosslinking for corneal regularization of keratoconus: STARE-X protocol. J Cataract Refract Surg. 2021;47:1403–1410. doi:10.1097/j.jcrs.0000000000000640
4. Mazzotta C, Ferrise M, Gabriele G, Gennaro P, Meduri A. Chemically-boosted corneal cross-linking for the treatment of keratoconus through a riboflavin 0.25% optimized solution with high superoxide anion release. J Clin Med. 2021;10:1324. doi:10.3390/jcm10061324
5. Roh HC, Chuck RS, Lee JK, Park CY. The effect of corneal irregularity on astigmatism measurement by automated versus ray tracing keratometry. Medicine. 2015;94:e677. doi:10.1097/MD.0000000000000677
6. Pantanelli S, MacRae S, Jeong TM, Yoon G. Characterizing the wave aberration in eyes with keratoconus or penetrating keratoplasty using a high-dynamic range wavefront sensor. Ophthalmology. 2007;114:2013–2021. doi:10.1016/j.ophtha.2007.01.008
7. Sabesan R, Yoon G. Visual performance after correcting higher order aberrations in keratoconic eyes. J Vis. 2009;9:
8. Konda S, Ambati BK. Intracorneal ring segments followed by toric pseudoaccomodating IOL for treatment of patients with corneal ectasia and cataract. Am J Ophthalmol Case Rep. 2020;18:100693. doi:10.1016/j.ajoc.2020.100693
9. Zhou W, Stojanovic F, Reinstein DZ, et al. Coma influence on manifest astigmatism in coma-dominant irregular corneal optics. J Refract Surg. 2021;37:274–282. doi:10.3928/1081597X-20210119-02
10. Taalas A, Yu Z. Comparison of assessment of refractive error by autorefraction and manual refraction with digital visual acuity chart. 2020.
11. Alpins NA, Goggin M. Practical astigmatism analysis for refractive outcomes in cataract and refractive surgery. Surv Ophthalmol. 2004;49:109–122. doi:10.1016/j.survophthal.2003.10.010
12. Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19:524–533. doi:10.1016/S0886-3350(13)80617-7
13. Reinstein DZ, Archer TJ, Randleman JB. JRS standard for reporting astigmatism outcomes of refractive surgery. J Refract Surg. 2014;30:654–659. doi:10.3928/1081597X-20140903-01
14. Sridhar MS. Anatomy of cornea and ocular surface. Indian J Ophthalmol. 2018;66:190–194. doi:10.4103/ijo.IJO_646_17
15. Zhou W, Stojanovic A, Utheim TP. Assessment of refractive astigmatism and simulated therapeutic refractive surgery strategies in coma-like-aberrations-dominant corneal optics. Eye Vision. 2016;3:13. doi:10.1186/s40662-016-0044-8
16. Alpins N, Ong JKY, Stamatelatos G. Corneal topographic astigmatism (CorT) to quantify total corneal astigmatism. J Refract Surg. 2015;31:182–186. doi:10.3928/1081597X-20150224-02
17. Elkadim M, Myerscough J, Bovone C, Busin M. Astigmatism orientation after deep anterior lamellar keratoplasty for keratoconus and its correlation with preoperative peripheral corneal astigmatism. Cornea. 2020;39:192–195. doi:10.1097/ICO.0000000000002175
18. Kawamorita T, Shimizu K, Hoshikawa R, Kamiya K, Shoji N. Relationship between central and peripheral corneal astigmatism in elderly patients. Opt Rev. 2018;25:336–339. doi:10.1007/s10043-018-0427-2
19. Łabuz G, Varadi D, Khoramnia R, Auffarth GU. Central and mid-peripheral corneal astigmatism in an elderly population: a retrospective analysis of Scheimpflug topography results. Sci Rep. 2021;11:1–9. doi:10.1038/s41598-021-81772-w
20. Soeters N, Muijzer MB, Molenaar J, Godefrooij DA, Wisse RPL. Autorefraction versus manifest refraction in patients with keratoconus. J Refract Surg. 2018;34:30–34. doi:10.3928/1081597X-20171130-01
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.