Back to Journals » Clinical Ophthalmology » Volume 15
Corneal Thickness and Anterior Chamber Flare After Cataract Surgery: A Randomized Controlled Trial Comparing Five Regimens for Anti-Inflammatory Prophylaxis
Authors Hansen NC ![]() , Erichsen JH, Holm LM, Kessel L
, Erichsen JH, Holm LM, Kessel L ![]()
Received 23 March 2021
Accepted for publication 10 May 2021
Published 29 June 2021 Volume 2021:15 Pages 2835—2845
DOI https://doi.org/10.2147/OPTH.S312350
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Niklas Cyril Hansen,1 Jesper Høiberg Erichsen,1 Lars Morten Holm,1,2 Line Kessel1,2
1Department of Ophthalmology, Rigshospitalet-Glostrup, Glostrup, Denmark; 2Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Correspondence: Jesper Høiberg Erichsen
Department of Ophthalmology, Rigshospitalet-Glostrup, Valdemar Hansens Vej 1-23, Glostrup, 2600, Denmark
Tel +45 38 63 47 70
Fax +45 38 63 46 69
Email [email protected]
Purpose: To investigate the relationship between early post-operative anterior chamber inflammation (aqueous flare) and central corneal thickness (CCT) after cataract surgery and to evaluate the effect of anti-inflammatory prophylaxis on CCT.
Setting: Department of Ophthalmology, Rigshospitalet-Glostrup, University Hospital Copenhagen, Denmark.
Design: Post-hoc analysis of a prospective randomized controlled trial.
Patients and Methods: A total of 470 participants who underwent standard cataract surgery were randomly allocated to prophylactic treatment with nonsteroidal anti-inflammatory drug (NSAID, groups C and D) or a combination of NSAID and steroid eye drops (groups A and B), commenced either pre-operatively (A and C) or post-operatively on the day of surgery (B and D), or “drop-less surgery” (peri-operative subtenon depot of dexamethasone, group E). Aqueous flare was measured before and three days after surgery. CCT was measured before surgery, three days, three weeks, and three months after surgery. Data were analyzed according to the intention-to-treat method.
Results: Doubling of aqueous flare increased mean CCT by 15.6 microns (95% CI 9.8; 21.3, P< 0.001) three days after surgery. Mean CCT increased from 549 microns (95% CI 545; 552) at baseline to 594 microns (95% CI 585; 602) three days after surgery and returned to 551 microns (95% CI 545; 557) three months after surgery. Mean CCT was thinner in group C compared to group A three days after surgery. No difference was found for any other groups or time points.
Conclusion: Increased anterior chamber inflammation was associated with significant corneal thickening three days after cataract surgery. Choice of anti-inflammatory regimen seemed to be of no or minimal importance on CCT when the effect of inflammation was accounted for. Corneal thickening is possibly mediated by underlying deterioration of the blood-aqueous barrier and corneal endothelium pump function caused by a post-operative inflammatory response.
Keywords: cataract surgery, anterior chamber inflammation, central corneal thickness, NSAID
Introduction
Cataract surgery is one of the most commonly performed surgical procedures in the world with an estimated 5 million procedures performed annually in the European Union.1 Cataract surgery has a low complication rate, but the sheer volume performed entails that a significant number of patients experience complications.
One such complication is opacification of the cornea due to increased central corneal thickness (CCT) referred to as corneal edema. In most cases, the edema resolves within days to weeks after surgery and in this period the visual acuity is adversely affected. In some cases however, increased corneal thickness becomes permanent and severely impairs vision. This is usually observed in patients with preexisting corneal disease.2 The cornea has an important role in the transmission and refraction of light onto the retina and must be transparent. Maintaining transparency requires an intact blood-aqueous barrier (BAB) and a functioning corneal endothelial pump.3 Cataract surgery is followed by an inflammatory response thought to arise from surgical manipulation of the iris, breakdown of the BAB4 and liberation of lens proteins. Increased anterior chamber inflammation may adversely affect the corneal endothelium,5 exacerbating the risk of corneal thickening. In clinical practice, post-operative corneal edema is treated by intensifying the anti-inflammatory treatment as this have been shown to suppress the post-operative breakdown of the BAB.6
Anterior chamber inflammation can be observed as aqueous flare - an optical phenomenon caused by back-scattered light from increased protein concentration in the aqueous humor. Aqueous flare is measurable by laser flare photometry which offers a non-invasive, objective and quantitative evaluation of anterior chamber inflammation.6
Studies have shown that both aqueous flare and CCT increase post-operatively.7–9 To our knowledge, the association between post-operative inflammation and corneal thickness has so far only been described in one study based on femtosecond laser-assisted surgery (FLACS) on 97 participants. They did not find any significant associations between aqueous flare immediately following the laser procedure (pre-phacoemulsification) and post-operative CCT.9
In this study, we investigated the effect of increased early post-operative anterior chamber inflammation, measured by laser flare photometry, on CCT after standard cataract surgery. In addition, we investigated how the effect was mitigated by different choices of anti-inflammatory prophylactic regimen.
Materials and Methods
Study Design and Setting
A randomized controlled clinical trial was conducted on patients undergoing standard cataract surgery at the Department of Ophthalmology, Rigshospitalet-Glostrup, Denmark. Study participants were randomized to one of five different prophylactic anti-inflammatory regimens. Participants were enrolled in the study from February 2018 to August 2019. Follow-up took place from February 2018 to December 2019.
Trial Registration
The study was first registered in the European Clinical Trials Database (EudraCT, 2017-002666-47) 30/06/2017 and at www.clinicaltrials.gov (NCT03383328) 26/12/2017, prior to initiation.
Intervention
Study participants were randomized by computer algorithm to one of five interventional groups prescribed a regimen consisting either of topical ketorolac (Acular 0.5%) + prednisolone (Pred Forte 1%, prednisolone acetate) (groups “A” and “B”) versus topical ketorolac (groups “C” and “D”) versus a subtenon depot of dexamethasone (group “E”). Each intervention regimen served as the sole means of post-operative anti-inflammatory prophylaxis for the respective group. Participants in groups A and C initiated eye drops three days before surgery while participants in groups B and D initiated therapy post-operatively on the day of surgery. Participants allocated to group A and B received a combination of prednisolone and ketorolac both three drops per day for three weeks. Participants allocated to group C and D received ketorolac three drops per day for three weeks. Participants allocated to group E were not prescribed eye drops but instead were treated with a depot of dexamethasone dihydrogen phosphate (Dexamethason Krka 4 mg/mL, Krka or Dexavital 4 mg/mL) in the subtenon space at the end of surgery. The amount injected was 0.5 mL, equivalent to a dose of 2 mg. Group A served as control for the other groups.
Participants
The study included participants who were scheduled to undergo cataract surgery for age-related cataract at Rigshospitalet-Glostrup, Denmark. Only one eye per participant was included. If both eyes were eligible for inclusion, the study eye was chosen by computerized coin toss. Women had to be postmenopausal. Exclusion criteria were known allergies to any content of the pharmaceuticals used in the study, a medical history of retinal disease (epiretinal membrane, retinal vein occlusion, retinal detachment, uveitis, glaucoma, diabetes mellitus, exudative age-related macular degeneration (AMD) or AMD with geographic atrophy), or significant surgical complications (posterior capsule rupture/vitreous loss, choroidal hemorrhage, and residual lens material).
Measurements
Corneal tomographic data were measured by Scheimpflug imaging (Oculus GmbH, Pentacam HR system, Wetzlar, Germany) at the pre-operative visit (baseline), three days, three weeks and three months after surgery. The corneal thickness at the pupil center was chosen as the measure of CCT based on the premise that it illustrates the CCT closest to the visual axis. Aqueous flare was measured by laser flare photometry (KOWA Company, KOWA FM-600, Aichi, Japan) on undilated pupils at baseline and three days after surgery. The mean of five reliable flare measurements was used. Anterior chamber depth was measured by anterior segment OCT biometry (Carl Zeiss Meditec, IOL master 700, Jena, Germany). Cataract was graded according to the “Age-Related Eye Disease Study (AREDS) system for classifying cataracts from photographs”.10 Cumulated dissipated energy (CDE), the amount of energy delivered to the eye during surgery, was recorded. Intra-ocular pressure (IOP) was measured by a rebound tonometer (iCare USA, iCare, Raleigh, North Carolina, United States) at all visits. Corrected distance visual acuity (CDVA) was measured at all visits using the “Early Treatment Diabetic Retinopathy Study” (ETDRS) visual acuity chart and presented as Logarithm to the Minimal Angle of Resolution (LogMAR). Anterior chamber cells were counted in a 1 mm by 1 mm light beam using the slit lamp at baseline and three days after surgery.
Outcomes
Primary outcome measure was the effect of change in aqueous flare between the baseline visit and three days after surgery (change in aqueous flare) on the CCT three days after surgery. Secondary outcome measures were the effect of anti-inflammatory prophylactic treatment group on the CCT three weeks and three months after surgery and surgery- and patient-specific variables, including the effects of anterior chamber depth (ACD) measured pre-operatively, age, baseline CCT, CDE, gender, and IOP, on post-operative CCT.
Surgical Procedure
The surgeon had to be experienced, defined by a minimum of 1000 surgeries performed within the past two years. Surgery was performed under local anesthesia. Topical phenylephrine 10%, tropicamide 1% and ketorolac 0.5% were applied to the eye pre-operatively. Subsequently, the conjunctiva was disinfected with povidone iodide 1% and the periorbital region was disinfected with chlorhexidine ethanol 0.5% and finally covered by a sterile draping. A 2.4 mm main incision and a 1 mm side-port incision were made followed by intracameral lidocaine 1% and viscoelastic (Healon OVD, Abbott medical Optics). Hereafter capsulorhexis and hydrodissection were performed. Ultrasound phacoemulsification was performed with a mini-flared 0.9 mm tip (Alcon Infiniti machine, Texas USA). Any residual cortex was removed by co-axial irrigation and aspiration (I/A). More viscoelastic was instilled to inflate the bag before implanting the intra-ocular lens (IOL). Viscoelastic was removed by I/A, the incisions were hydrated, followed by irrigation of the anterior chamber with 1 mL cefuroxime 2.5 mg/mL.
Statistical Methods
A post-hoc analysis was conducted using linear mixed models with unstructured covariance patterns, under the assumption that baseline values were equal between treatment groups. The linear mixed models were constructed using the R statistical software for Windows (version 4.0.2, R Core Team). Aqueous flare measurements were transformed to log-scale to achieve a normal distribution. Data were analyzed according to the intention-to-treat method. P-values were adjusted for multiple testing using the False Discovery Rate (FDR). Effect estimates with an adjusted P-value <0.05 were considered statistically significant.
Results
A total of 470 participants were enrolled in the study and randomized to one of the five intervention groups. The age of included participants ranged from 52 to 88 years and 290 (62%) of participants were female (Table 1). Values of baseline characteristics were comparable between groups except for a larger percentage of female participants in group C. AREDS nuclear cataract grading of the study eyes are presented in Figure 1. Fourteen (3%) participants were excluded from the study after randomization: four were excluded because of residual lens material, two because the inserted toric IOL required repositioning, two were operated by a surgeon with less than 1000 surgeries within the last two years, one was operated on the fellow eye and no longer needed surgery on the study eye, two had retinal conditions that met exclusion criteria first discovered after randomization, two had a posterior capsule break, and one had post-operative pseudophakic retinal detachment with subsequent vitrectomy. In addition, 14 (3%) participants withdrew their consent before surgery, finally leaving 456 (97%) participants available for statistical analysis.
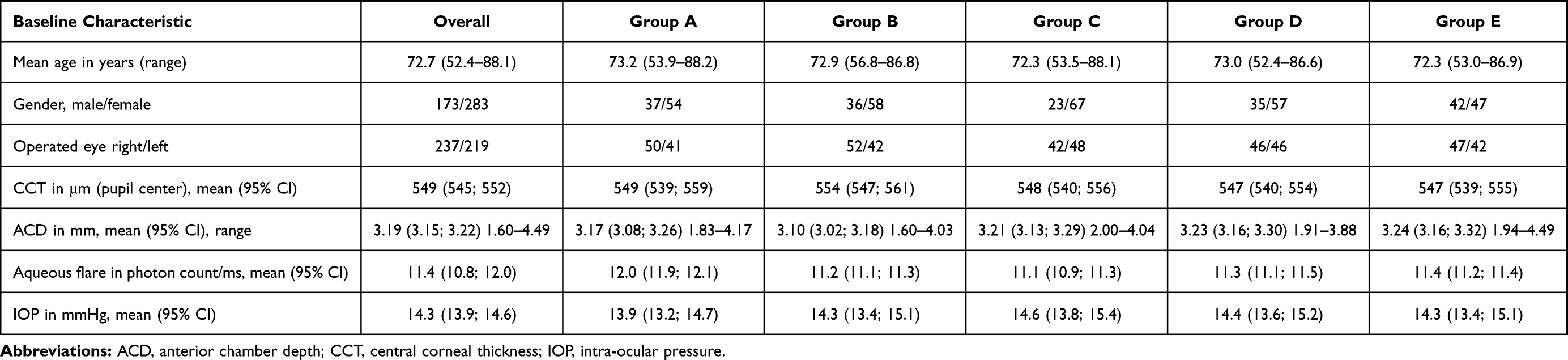 |
Table 1 Baseline Characteristics |
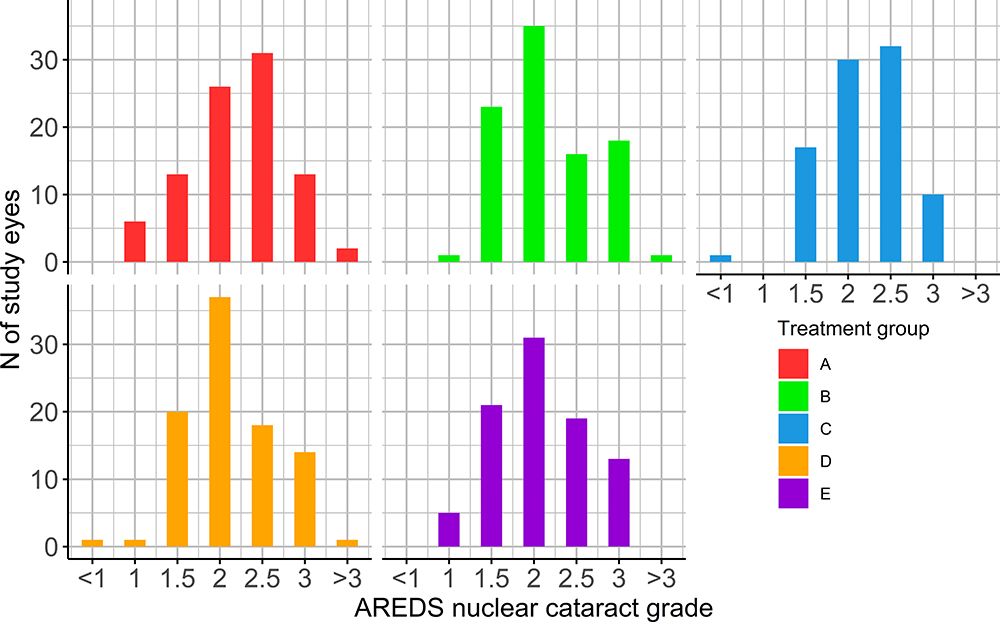 |
Figure 1 AREDS (Age-Related Eye Disease Study) nuclear cataract grading of study eyes divided by group, from smallest to highest grade: <1, 1, 1.5, 2, 2.5, 3, >3. N = Number; Treatment group A: initiated NSAID (non-steroidal anti-inflammatory drug) and steroid eye drops three days pre-operatively; treatment group B: initiated NSAID and steroid eye drops post-operatively; treatment group C: initiated NSAID eye drops three days pre-operatively, treatment group D: initiated NSAID eye drops post-operatively; treatment group E: received a subtenon depot of dexamethasone peri-operatively. |
Changes in Mean Central Corneal Thickness
The overall mean CCT was 549 microns (95% CI 545; 552) before surgery (Table 1) and increased to 594 microns (95% CI 585; 602) three days after surgery, 562 microns (95% CI 556; 570) three weeks after surgery and returned to 551 microns (95% CI 545; 557) three months after surgery. The mean CCT over time for each interventional group is presented in Figure 2.
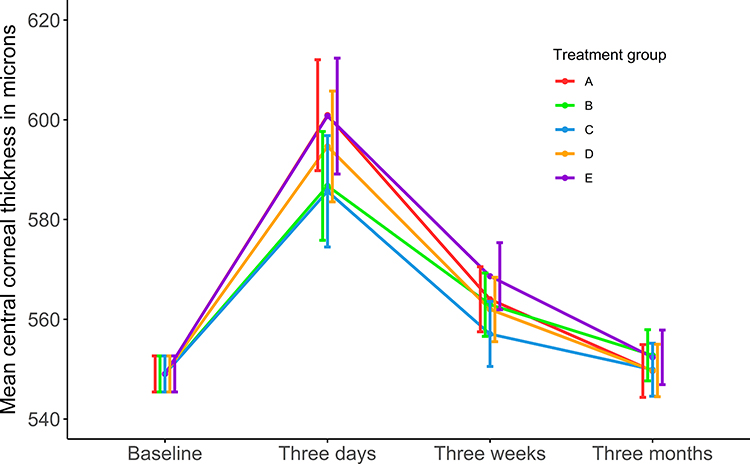 |
Figure 2 Estimated changes in mean central corneal thickness in microns as a function of treatment group across post-operative visits. Treatment group A: initiated NSAID (non-steroidal anti-inflammatory drug) and steroid eye drops three days pre-operatively; treatment group B: initiated NSAID and steroid eye drops post-operatively; treatment group C: initiated NSAID eye drops three days pre-operatively; treatment group D: initiated NSAID eye drops post-operatively; treatment group E: received a subtenon depot of dexamethasone peri-operatively. |
Central Corneal Thickness as a Function of Change in Aqueous Flare and Anti-Inflammatory Regimen
Increased aqueous flare was associated with increased CCT three days after surgery (Figure 3); A doubling of aqueous flare was associated with thickening of the CCT by 15.6 microns (95% CI 9.8; 21.3, P < 0.001, Table 2) three days after surgery. The effect on CCT associated with a doubling in flare at day three after surgery was reduced to 2.8 microns (95% CI −0.8; 6.4, P = 0.23) three weeks after surgery and to 0.9 microns (95% CI −19.0; −9.2, P = 0.73) three months after surgery. The CCT was significantly thinner in group C (−19.8 microns (95% CI −35.1; −4.4, P = 0.03)) compared to group A (control group) three days after surgery. No significant differences were found for any other time points or any other groups. Eighty-seven participants (20%) received additional anti-inflammatory treatment. The above-mentioned results remained significant when adjusted for additional anti-inflammatory treatment and other surgery- and patient-specific variables, including ACD and CCT measured before surgery, CDE and IOP.
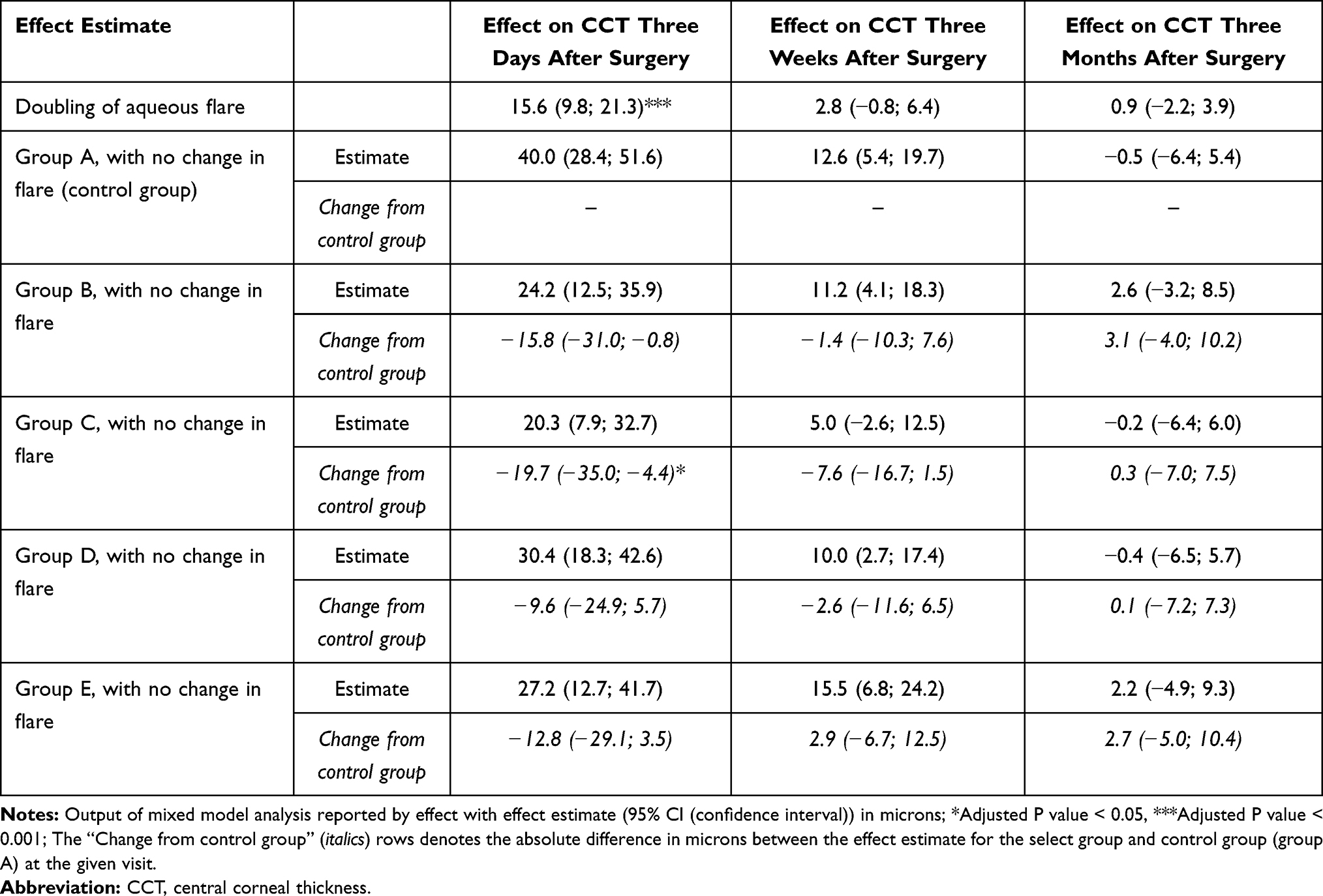 |
Table 2 Change in Central Corneal Thickness After Surgery in Microns as Function of Aqueous Flare and Anti-Inflammatory Regimen |
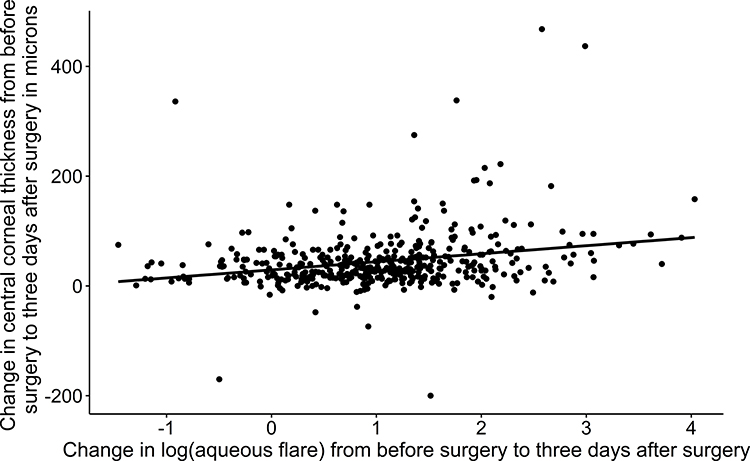 |
Figure 3 Change in central corneal thickness in microns as a function of change in log (aqueous flare) from before surgery to three days after surgery. Estimates for linear regression (95% confidence interval, P value): intercept/α = 29.3 (21.8; 36.8, P < 0.001), slope/β = 14.7 (9.2; 20.2, P < 0.001), adjusted r2 = 0.058. |
Surgery-Specific Variables and Their Effect on Central Corneal Thickness
Shallower ACD was associated with thickening of the CCT; having a 0.1mm shallower ACD before surgery was associated with thickening of the CCT by 1.9 microns (95% CI 0.7; 3.1, P < 0.01, Table 3) three days after surgery and by 1.2 microns (0.5; 2.0, P < 0.01) three weeks after surgery. The effect of pre-operative ACD on CCT was no longer significant three months after surgery. A shallow ACD three days after surgery was associated with CCT thickening (P < 0.001, Figure 4). Mean values of CDE were comparable between groups being 10.7 (95% CI 9.5; 11.9), 9.7 (95% CI 8.4; 11.0), 8.5 (95% CI 7.5; 9.5), 8.9 (95% CI 7.9; 9.9) and 8.0 (95% CI 7.0; 9.0) percent-seconds in the A, B, C, D and E groups, respectively. Increasing CDE by one percent-second was associated with thickening of the CCT by 1.7 microns (95% CI 0.8; 2.6, P < 0.01) three days after surgery. Increasing CDE had no significant effect on post-operative CCT at the other follow-up visits.
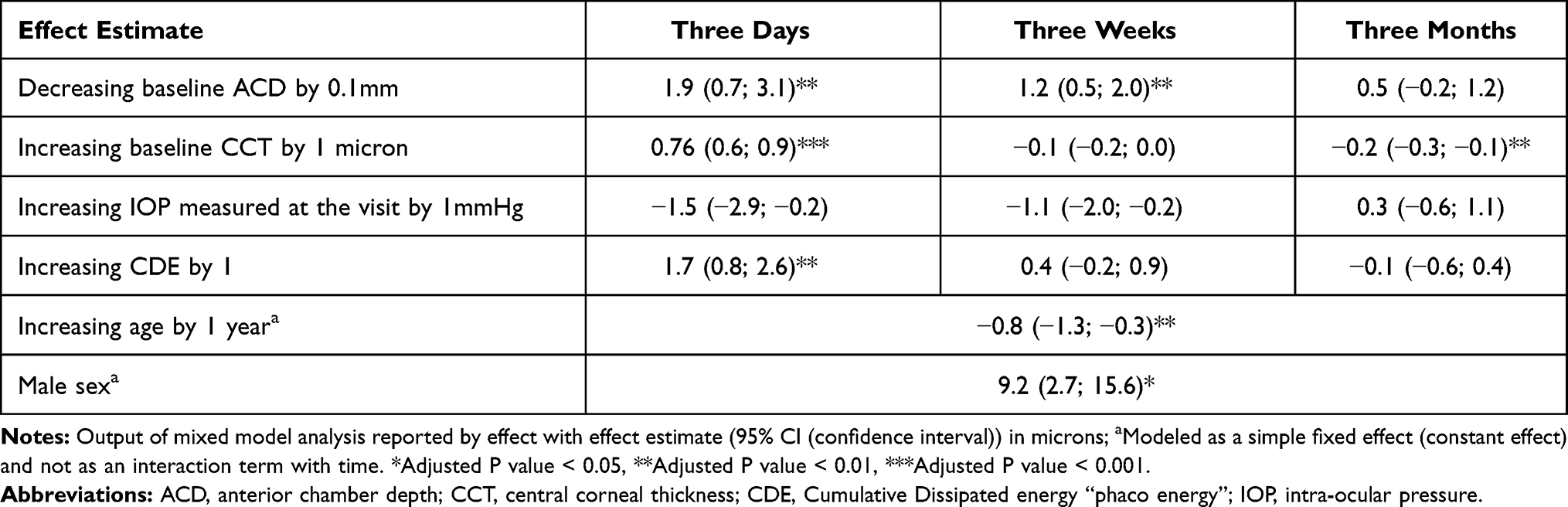 |
Table 3 Effect on Central Corneal Thickness After Surgery in Microns by Surgery- and Patient-Specific Variables |
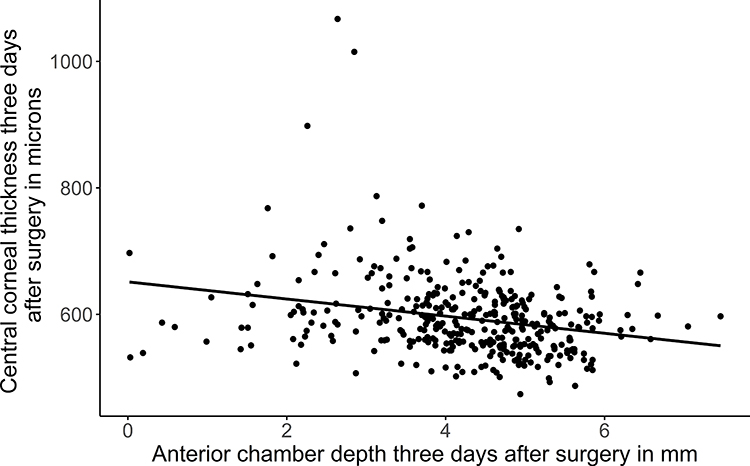 |
Figure 4 Central corneal thickness in microns as a function of anterior chamber depth three days after surgery. Estimates for linear regression (95% confidence interval, P value): intercept/α = 651.4 (627,8; 675, P < 0.001), slope/β = −13.5 (−18.9; −8.1, P < 0.001), adjusted r2 = 0.061. |
Patient-Specific Variables and Their Effect on Central Corneal Thickness
A thicker CCT before surgery was associated with a significantly thicker CCT three days after surgery (0.76 microns (95% CI 0.6; 0.9, P < 0.001)), corresponding to a 7.6 micron thicker CCT three days after surgery per 10 micron increase in pre-operative CCT when all other parameters were kept constant. Males had a 9.2 microns (95% CI 2.7; 15.6, P < 0.05) thicker CCT. Increasing age of study participants by one year thinned the cornea by 0.8 microns (1.3; 0.3, P < 0.05). Mean IOP was comparable between groups before surgery (Table 1). IOP had no significant effect on CCT at any time points (Table 3). No anterior chamber cells were found at the baseline visit. The means of anterior chamber cell counts three days after surgery were 3.4 (95% CI 3.0; 3.9), 3.9 (95% CI 3.3; 4.4), 4.1 (95% CI 3.3; 5.0), 4.0 (95% CI 3.4; 4.5) and 5.5 (95% CI 4.5; 6.6) for the A, B, C, D and E groups, respectively. The mean of anterior chamber cell count was significantly greater in group E compared to group A three days after surgery (P = 0.004).
Effect of Central Corneal Thickness on Corrected Distance Visual Acuity
Visual acuity, CDVA, was reduced in participants with a thicker CCT three days after surgery (P < 0.001, Figure 5). CDVA was not associated with CCT three months after surgery (P = 0.81).
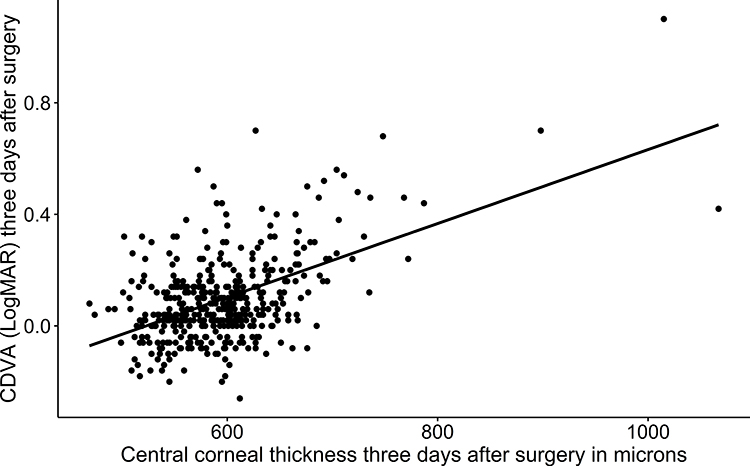 |
Figure 5 Corrected distance visual acuity (CDVA, denoted as LogMAR (Logarithm to the Minimal Angle of Resolution)) as a function of central corneal thickness in microns three days after surgery. Estimates for linear regression (95% confidence interval, P value): intercept/α = −0.69 (−0.57; −0.81, P < 0.001), slope/β = 0.0013 (0.0011; 0.0015, P < 0.001), adjusted r2 = 0.273. |
Discussion
We found a strong association between early post-operative inflammation and central corneal thickening, but we did not find any clinically significant independent effects of anti-inflammatory regimen. A thicker pre-operative corneal thickness was strongly associated with corneal thickening three days after surgery and a shallow pre-operative anterior chamber depth was associated with corneal thickening three days and three weeks after surgery.
Postoperative corneal thickening may occur for a number of reasons. While surgical trauma to the corneal endothelium plays a major role, anterior chamber inflammation is also presumed to independently contribute to corneal thickening. To quantify these effects of the surgical trauma, we adjusted for surgery-specific variables such as CDE and pre-operative ACD and found that the effect of early post-operative aqueous flare on post-operative CCT remained significant. It should be noted that all patients in our study were operated by experienced surgeons (defined as >1000 surgeries within the last two years). Ocular hypertension is known to increase corneal edema by impairing the function of the corneal endothelial pump.11 Intraocular pressure (IOP) was within the acceptable range in all of our participants and we did not find any effect of IOP on corneal thickness.
Studies have shown that anterior chamber inflammation increases after surgery8,9 but the association with corneal thickening has not been thoroughly examined. A study based on femtosecond laser treatment did not find a statistically significant association between aqueous flare measured ten minutes after the laser procedure but before phacoemulsification, and CCT thickening the day after surgery.9 This discrepancy between their study and ours may in part be attributed to their measurement of aqueous flare immediately following the laser procedure before phacoemulsification and the associated liberation of lens proteins promotes a considerable inflammatory response; Moreover, we measured CCT three days after surgery allowing ample time for this inflammatory response to affect the CCT, an effect that might not be apparent the day after surgery. In addition, our larger sample size (N = 456 vs N = 97) provided additional statistical power to detect such an association. The study also found a shallow anterior chamber depth (ACD) measured before FLACS was associated with increased aqueous flare ten minutes after femtosecond laser treatment but before the phacoemulsification procedure.9 In clinical practice, a shallow ACD complicates the surgical procedure by necessitating closer proximity between the tip of the ultrasonic handpiece and the corneal endothelium. This proximity increases the harmful effects of the ultrasound energy and exacerbates the risk of post-operative complications such as corneal thickening. A shallower ACD also implies a smaller anterior chamber volume; Increased aqueous flare in an anterior chamber with shallow ACD compared with a typical ACD might simply reflect the same amount of inflammatory material in a smaller volume and not a causal link between shallow ACD and an increased inflammatory response. We found a thickening effect of shallow pre-operative ACD on post-operative CCT three days and three weeks after surgery but accounting for this effect did not influence the independent effect of inflammation. These findings suggest the increased risk of post-operative corneal thickening in participants with a shallow ACD is in part potentially mediated by an increased inflammatory response resulting from a more complicated surgical procedure.
Post-operative inflammation is controlled by prescription of anti-inflammatory eye drops, either steroids or NSAID or a combination of the two. We found that post-operative CCT was comparable between groups at all time points except for a thinner CCT three days after surgery in group C compared to group A. Our findings are supported by two studies that compared the effect of steroid-NSAID combination treatment and NSAID monotherapy on post-operative CCT.8,12 These findings suggest that NSAID monotherapy is as effective as steroid and NSAID combination therapy in the prophylaxis of post-operative corneal thickening.
An oft-cited concern for preferring steroids to NSAIDs in post-operative anti-inflammatory prophylaxis is the rare occurrence of corneal melts associated with topical application of NSAID eye drops. Two randomized controlled trials evaluating the safety and efficacy of NSAID eye drops found no cases of corneal melts,13,14 although these have been observed in a number of case reports.15 The prevalence of corneal melts associated with NSAID eye drops is reputedly very low, plausibly making the absence of observations in clinical trials a question of sample size. In our study, although we only examined the CCT, we did not find that NSAID eye drops caused a corneal thinning effect compared to drop-less surgery (group E) or that the number of daily eye drops had an effect on CCT when the direct effect of inflammation was accounted for. In other words, we found no indication of an increased prevalence of corneal thinning among participants treated with NSAID eye drops compared to participants receiving drop-less surgery. While our findings do not negate the perceived rare risk of corneal melts, they do substantiate that more often than not NSAID eye drop application is not associated with corneal thinning: fear of post-operative corneal thinning should therefore not be used as an argument against the use of NSAID monotherapy post-operatively.
A limitation in our study was that we only measured aqueous flare before surgery and three days after surgery. Aqueous flare remains elevated up to at least 28 days after cataract surgery.16 We chose the corneal thickness at the pupil center as our measure of CCT. Post-operative corneal thickening at the pupil center served as a surrogate measure for corneal edema. A reasonable criticism leveled against our conclusions might be that CCT measured at this location does not rule out potential corneal thickening elsewhere and as such does not entirely reflect the clinical manifestations of corneal edema. While a valid point, CCT measured at the pupil center is significantly associated with post-operative visual acuity, arguably the most important clinical implication of post-operative corneal edema. We conducted multiple comparisons increasing the likelihood of committing a type I error. We utilized the False Discovery Rate (FDR) with the Benjamini-Hochberg procedure to minimize this risk. Participants in our study had to be informed of their treatment regimen and surgeons had to be aware of whether to administer drop-less treatment which prevented the study from being fully masked.
Conclusions
Increased early post-operative anterior chamber inflammation was associated with corneal thickening three days after surgery but when the effect of inflammation was accounted for, there were no clinically relevant independent effects of prophylactic anti-inflammatory regimen. Three weeks of treatment with NSAID eye drops did not seem to show signs of central corneal thinning. A shallow anterior chamber depth was associated with corneal thickening after surgery. Corneal thickening is possibly mediated by underlying deterioration of the blood-aqueous barrier and corneal endothelium pump function caused by a post-operative inflammatory response.
Abbreviations
ACD, anterior chamber depth; AMD, age-related macular degeneration; AREDS, age-related eye disease study; BAB, blood-aqueous barrier; CCT, central corneal thickness; CDE, cumulated dissipated energy; CDVA, corrected distance visual acuity; CI, confidence interval; drop-less surgery, surgery where a peri-operatively placed subtenon depot of dexamethasone acted as post-operative anti-inflammatory treatment; ETDRS, Early Treatment Diabetic Retinopathy Study; EudraCT, European Union Drug Regulating Authorities Clinical Trials; FDA, United States Food and Drug Administration; FDR, False Discovery Rate; FLACS, Femtosecond laser-assisted cataract surgery; GCP, good clinical practice; Group A, intervention group that received Prednisolone + NSAID eye drop combination therapy initiated three days before surgery; Group B, intervention group that received Prednisolone + NSAID eye drop combination therapy initiated post-operatively on the day of surgery; Group C, intervention group that received NSAID eye drop mono therapy initiated three days before surgery; Group D, intervention group that received NSAID eye drop mono therapy initiated post-operatively on the day of surgery; Group E, intervention group that received therapy with a peri-operative subtenon depot of dexamethasone (drop-less surgery); IOL, intra-ocular lens; IOP, intra-ocular pressure; LogMAR, Logarithm to the Minimal Angle of Resolution; NSAID, nonsteroidal anti-inflammatory drug; OCT, optical coherence tomography.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available to avoid compromising patient confidentiality. Data are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Danish Medicines Agency (Journal nr.: 2017064331), the Committee on Health Research Ethics, Capital Region, Denmark (Journal nr.: H-17025182) and The Danish Data Protection Agency (RH-2017-291, I-Suite nr.: 05860) and was monitored according to the good clinical practice (GCP) quality standard by the GCP unit at Copenhagen University Hospital. The study was conducted in accordance with the Declaration of Helsinki and all study participants provided written informed consent.
Author Contributions
JHE was responsible for data collection. NCH and JHE performed the statistical analysis. JHE, LMH and LK secured funding. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The study received funding from the Independent Research Fund Denmark (DFF – 7016-00161), Fight for Sight - Denmark and Henry og Astrid Møllers Fond. Funding bodies had no role in the study design, collection of data, data analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eurostat. Almost 5 million cataract surgeries in the EU in 2017. Available from: https://ec.europa.eu/eurostat/en/web/products-eurostat-news/-/DDN-20191204-1.
2. Fan W, Yan H, Zhang G. Femtosecond laser-assisted cataract surgery in Fuchs endothelial corneal dystrophy: long-term outcomes. J Cataract Refract Surg. 2018;44(7):864–870. doi:10.1016/j.jcrs.2018.05.007
3. Costagliola C, Romano V, Forbice E, et al. Corneal oedema and its medical treatment. Clin Exp Optom. 2013;96(6):529–535. doi:10.1111/cxo.12060
4. Shah SM, Spalton DJ. Changes in anterior chamber flare and cells following cataract surgery. Br J Ophthalmol. 1994;78(2):91–94. doi:10.1136/bjo.78.2.91
5. Alfawaz AM, Holland GN, Yu F, Margolis MS, Giaconi JA, Aldave AJ. Corneal endothelium in patients with anterior uveitis. Ophthalmology. 2016;123(8):1637–1645. doi:10.1016/j.ophtha.2016.04.036
6. Sawa M. Laser flare-cell photometer: principle and significance in clinical and basic ophthalmology. Jpn J Ophthalmol. 2017;61(1):21–42. doi:10.1007/s10384-016-0488-3
7. Chen P-Q, Han X-M, Zhu Y-N, Xu J. Comparison of the anti-inflammatory effects of fluorometholone 0.1% combined with levofloxacin 0.5% and tobramycin/dexamethasone eye drops after cataract surgery. Int J Ophthalmol. 2016;9(11):1619–1623. doi:10.18240/ijo.2016.11.13
8. Miyanaga M, Miyai T, Nejima R, Maruyama Y, Miyata K, Kato S. Effect of bromfenac ophthalmic solution on ocular inflammation following cataract surgery. Acta Ophthalmol. 2009;87(3):300–305. doi:10.1111/j.1755-3768.2008.01433.x
9. Pahlitzsch M, Torun N, Pahlitzsch ML, et al. Correlation between anterior chamber characteristics and laser flare photometry immediately after femtosecond laser treatment before phacoemulsification. Eye. 2016;30(8):1110–1117. doi:10.1038/eye.2016.110
10. Kassoff A, Kassoff J, Mehu M, et al. The Age-Related Eye Disease Study (AREDS) system for classifying cataracts from photographs: AREDS Report No. 4. Am J Ophthalmol. 2001;131(2):167–175. doi:10.1016/S0002-9394(00)00732-7
11. Li X, Zhang Z, Ye L, et al. Acute ocular hypertension disrupts barrier integrity and pump function in rat corneal endothelial cells. Sci Rep. 2017;7(1):1–9. doi:10.1038/s41598-017-07534-9
12. Moschos MM, Chatziralli IP, Pantazis P, Rouvas AA, Sergentanis TN. Is topical diclofenac essential before and after uneventful phacoemulsification cataract surgery? J Ocul Pharmacol Ther. 2012;28(4):335–339. doi:10.1089/jop.2011.0256
13. Flach AJ, Dolan BJ, Donahue ME, Faktorovich EG, Gonzalez GA. Comparative effects of ketorolac 0.5% or diclofenac 0.1% ophthalmic solutions on inflammation after cataract surgery. Ophthalmology. 1998;105(9):1775–1779. PMID: 9754191. doi:10.1016/S0161-6420(98)99053-4
14. Solomon KD, Cheetham JK, DeGryse R, Brint SF, Rosenthal A. Topical ketorolac tromethamine 0.5% ophthalmic solution in ocular inflammation after cataract surgery. Ophthalmology. 2001;108(2):331–337. PMID: 11158809. doi:10.1016/s0161-6420(00)00543-1
15. Flach AJ. Corneal melts associated with topically applied nonsteroidal anti-inflammatory drugs. Trans Am Ophthalmol Soc. 2001;99:202–205.
16. Ylinen P, Holmström E, Laine I, Lindholm JM, Tuuminen R. Anti-inflammatory medication following cataract surgery: a randomized trial between preservative-free dexamethasone, diclofenac and their combination. Acta Ophthalmol. 2018;96(5):486–493. doi:10.1111/aos.13670
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.