Back to Journals » Clinical Ophthalmology » Volume 18
Corneal Collagen Crosslinking for Ectasia After Refractive Surgery: A Systematic Review and Meta-Analysis
Authors Amaral DC ![]() , Menezes AHG
, Menezes AHG ![]() , Vilaça Lima LC
, Vilaça Lima LC ![]() , Faneli AC
, Faneli AC ![]() , Neto PFS
, Neto PFS ![]() , Canedo ALC
, Canedo ALC ![]() , Mora-Paez DJ
, Mora-Paez DJ ![]() , Guedes JAF
, Guedes JAF ![]() , Louzada RN
, Louzada RN ![]() , Fontes BM
, Fontes BM ![]()
Received 6 December 2023
Accepted for publication 26 February 2024
Published 19 March 2024 Volume 2024:18 Pages 865—879
DOI https://doi.org/10.2147/OPTH.S451232
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dillan Cunha Amaral,1 Adriano Henrique Gomes Menezes,1 Luan Cavalcante Vilaça Lima,1 Adriano Cypriano Faneli,2 Pedro Fernandes Souza Neto,3 Ana Laura Caiado Canedo,4 Denisse Josefina Mora-Paez,5 Jaime Augusto Ferreira Guedes,5 Ricardo Noguera Louzada,1 Bruno Machado Fontes6
1Faculdade de Medicina, Universidade Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brazil; 2Faculdade de Medicina, Escola Bahiana de Medicina e Saúde Pública, Salvador, BA, Brazil; 3Hospital Universitário Professor Edgard Santos, Universidade Federal da Bahia, Salvador, BA, Brazil; 4Ophthalmology, Hospital Israelita Albert Einstein, Goiânia, GO, Brazil; 5Glaucoma Research Center, Wills Eye Hospital, Philadelphia, PA, USA; 6Ophthalmology, Opty Group, Rio de Janeiro, RJ, Brazil
Correspondence: Dillan Cunha Amaral, Centro de Ciências da Saúde, Bloco K - Av. Carlos Chagas Filho, 373 - 2° andar, Sala 49 - Cidade Universitária, Rio de Janeiro, RJ, 21044-020, Brazil, Email [email protected]
Introduction: Corneal ectasia leads to progressive irregular corneal curvature and reduced visual acuity.
Objective: To assess the safety and effectiveness of corneal collagen cross-linking (CXL) for managing corneal ectasia resulting from refractive laser surgery (RSL).
Methods: A systematic review and meta-analysis were realized according to PRISMA guidelines. We searched PubMed, EMBASE, Cochrane, and Web of Science databases for studies on CXL in patients with ectasia after RLS. The outcomes of interest included visual acuity, refractive outcomes, topographic parameters (Kmax, index surface variance (ISV), index of Vertical Asymmetry (IVA), keratoconus index (KI), central keratoconus index (CKI), index of height asymmetry (IHA), index of height decentration (IHD) and Rmin (minimum sagittal curvature)), central corneal thickness, endothelial cell count, and possible adverse events. Statistical analysis was performed using the R software (version 4.2.3, R Foundation for Statistical Computing, Vienna, Austria).
Results: 15 studies encompassing 421 patients (512 eyes) were included. The mean age was 32.03 ± 4.4 years. The pooled results showed a stable uncorrected visual acuity post-CXL, with a significant improvement in corrected distance visual acuity (SMD = 0.09; 95% CI: − 0.07 to 0.26). The spherical equivalent decreased significantly (SMD = − 0.09; 95% CI: − 0.35, − 0.02). The topographic parameter Kmax decreased significantly (SMD = 0.15; 95% CI:0.01 to 0.28); however, the other parameters, ISV, IVA, KI, CKI, IHA, IHD, and Rmin, did not change significantly. Central corneal thickness decreased significantly (SMD = 0.24; 95% CI:0.07 to 0.41), and the endothelial cell count remained stable The complications were rare.
Conclusion: CXL is a safe and effective technique for managing corneal ectasia after RLS.
Keywords: cross-linking, corneal ectasia, laser refractive surgery, meta-analysis, systematic review
Introduction
Corneal ectasia is a rare but potentially vision-threatening complication that may occur after refractive laser surgery (RSL), leading to deterioration of visual acuity and the need for additional treatment.1–3 Ectatic corneal diseases encompass conditions marked by gradual thinning and bulging of the corneal structure.4 This condition leads to irregular astigmatism (corneal distortion) and subsequent decrease in visual acuity.5 This may occur within weeks or even 45 months of the surgical procedure.6 Post-refractive ectasia was extremely rare in eyes without risk factors for PRK (0.020%), LASIK (0.090%), or SMILE (0.011%) per 100,000 eyes. The overall incidence was low even when including eyes with preoperative risk factors: 0.025% for PRK, 0.100% for LASIK, and 0.020% for SMILE per 100,000 eyes.7 A retrospective study of 30,000 LASIK cases revealed that the risk of postoperative corneal ectasia after LASIK is equal to or lower than the risk of developing keratoconus without LASIK.8,9 This suggests that corneal ectasia following RLS may occur by chance, even without such surgery. Furthermore, post-RLS ectasia causes have not been completely elucidated, but many risk factors have been described, such as personal/family history of keratoconus, younger age, abnormal corneal topography and tomography, high myopia, low residual stromal bed, excessive stromal ablation, high percentage of tissue altered, deep primary keratotomy leading to a thick corneal flap, forme fruste keratoconus, pellucid marginal degeneration, lamellar procedures, deeper ablations and low preoperative corneal thickness.10–18
Current treatment options for visual rehabilitation include rigid contact lenses, penetrating or lamellar keratoplasty, intrastromal corneal ring segments, and corneal collagen cross-linking (CXL).19–22 This method increases the biomechanical stability and stiffness of the cornea in a photochemical process by adding additional polymer bands between the collagen fibers using ultraviolet (UV) light and riboflavin.23–25 As a consequence, additional covalent bonds are formed between collagen molecules, stabilizing the collagen structure.25 To date, few studies have evaluated the use of CXL for treating corneal ectasia after refractive surgery, and the available results do not show good congruence. As it is a rare complication, the number of patients included in these studies was low. The last meta-analysis produced on the subject was in 2017,26 and since then, there have been results from new high-impact clinical trials with more significant sample numbers. Hence, a new meta-analysis is essential to consolidate the findings from past and recent studies.
This systematic review and meta-analysis aimed to assess CXL’s safety and efficacy in addressing corneal ectasia after RLS.
Methods
Search Strategy and Data Extraction
The protocol for this systematic review of the literature on CXL therapy in cases of corneal ectasia after RLS was registered in the PROSPERO International Prospective Register of Systematic Reviews (CRD42023452904). We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for data extraction.27 The terms (“Corneal Collagen Cross Linking” OR “Corneal Cross Linking” OR “Corneal” OR “Epi off Corneal Cross Linking” OR “Epi off CXL” OR “Epi on CXL” OR “Epi-off Corneal” OR “Cross-Linking” OR “Epi-off CXL” OR “Epi-on CXL” OR “Epithelium off Corneal Cross Linking” OR “Epithelium off CXL” OR “Epithelium on Corneal Cross Linking” OR “Epithelium on CXL” OR “Epithelium-off Corneal Cross-Linking” OR “Epithelium-off Corneal” OR “Cross-Linkings” OR “Epithelium-off CXL” OR “Epithelium-on Corneal Cross-Linking” OR “Epithelium-on CXL” OR “Transepithelial Corneal Cross Linking” OR “Transepithelial Corneal Cross-Linking” OR “Transepithelial CXL” OR “crosslinking” OR “cross-linking”) AND (“post-LASIK keratectasia” OR “Postoperative Ectasia” OR “keratectasia” OR “corneal ectasia” OR “Post-LASIK ectasia”) AND (“Keratorefractive Surgical Procedure” OR “Keratorefractive Surgical Procedures” OR “Refractive Surgeries” OR “Refractive Surgery” OR “Refractive Surgical Procedure”) were used for the search. Search terms were used to query the PubMed, Embase, Cochrane, and Web of Science databases. The searches started on July 20, 2023, and ended on August 20, 2023. References from all the included studies, previous systematic reviews, and meta-analyses were manually searched for additional studies. Two authors (A.H. and L.C.) independently extracted data using predefined search criteria and quality assessment. The full articles of eligible publications were then scrutinized. Only trials that met the following criteria were included in the meta-analysis.
Eligibility Criteria
Inclusion in this meta-analysis was restricted to studies that met all the following eligibility criteria: (1) human study; (2) participants: patients with corneal ectasia after RLS, defined as progressive corneal curvature steepening, increasing myopia and astigmatism, and loss of visual acuity postoperative;18,28 (3) intervention: CXL; (4) at least one or more clinical outcomes representing intraoperative and/or postoperative outcome parameters must be assessed and published; and (5) design: randomized clinical trials (RCT) or non-randomized cohorts, and studies were included only if they reported any of the clinical outcomes of interest. We excluded studies with (1) animal studies or cadaver subjects and (2) studies that were not published in English.
Outcomes
Our study aimed to evaluate multiple outcomes, encompassing the endpoints of (1) visual acuity outcomes with corrected distance visual acuity (CDVA) and uncorrected distance visual acuity (UCVA); (2) refractive outcome with Spherical Equivalent (SE); (3) topographic and tomographic parameter outcomes with Kmax, Index surface variance (ISV), Index of Vertical Asymmetry (IVA), Keratoconus Index (KI), Center Keratoconus Index (CKI), Index of Height Asymmetry (IHA), Index of Height Decentration (IHD), and minimum sagittal curvature (Rmin); (4) endothelial cell count (EEC), central corneal thickness (CCT); and (5) serious complications.
Data Extraction
Two reviewers (L.C. and A.M.) independently evaluated the quality of the citations and extracted data. Any disagreements were resolved by another reviewer (D.A). The following information was extracted: name of first author, year of publication, trial location, research design, number of eyes, mean patient age, sex proportion, follow-up duration, and type of refractive surgery.
Adverse events and complications encompassed those possibly related to the procedure, such as epithelial ingrowth, infectious keratitis, flap margin elevation, retinal damage, persistent corneal edema, corneal scarring, and cataract formation in the patient population.
Statistical Analysis
This systematic review and meta-analysis were performed using the Cochrane Collaboration and Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines.27 Relative risk (RR) with 95% confidence intervals was used to compare treatment effects for categorical outcomes. Continuous outcomes were compared using standardized mean differences (SMD). Outcomes were measured as the mean ± standard deviation (SD). Statistical significance was set than 0.05. Cochran’s Q-test and I2 statistics were used to assess heterogeneity, and I2 > 50% indicated substantial heterogeneity. We used a random-effects model for outcomes with significant heterogeneity. Statistical analysis was performed using the R software (version 4.2.3, R Foundation for Statistical Computing, Vienna, Austria).
Results
Study Selection and Baseline Characteristics
As detailed in Figure 1, we found 1324 articles, with 225 articles in PubMed, 493 in Embase, 606 in Web of Science, and 23 in Cochrane databases. Of these, 785 duplicates were excluded from the analysis. After removing duplicate records and ineligible studies, 31 studies remained and were thoroughly reviewed based on inclusion criteria. Eighteen articles were excluded based on these criteria. Finally, 15 studies were included in this review, including four RCTs29–32 and eleven non-randomized cohorts.33–43
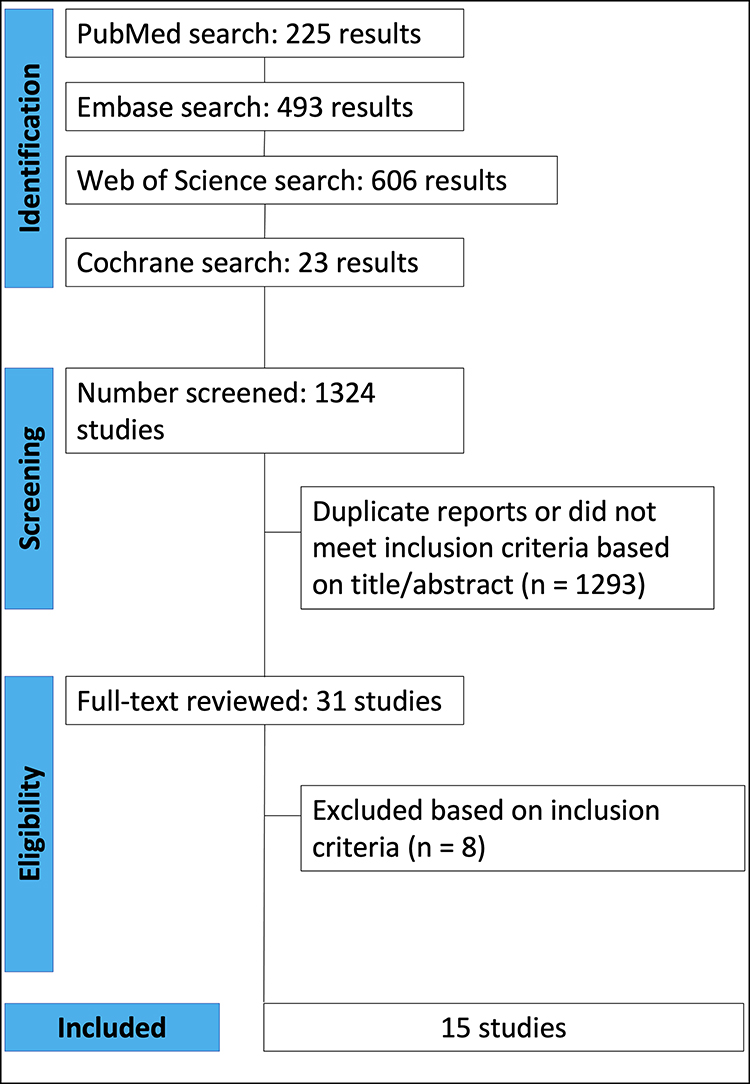 |
Figure 1 Flow diagram of study selection. |
We analyzed 421 patients, including 512 eyes diagnosed with post-laser corneal ectasia. The sample sizes of these trials ranged from 11 to 91. These trials were performed in eight countries (three in the United States; two in China, Egypt, and Switzerland; and one in Australia, Germany, Lebanon, and Turkey). Eleven trials reported that their patients were followed-up for 12 months or more post-CXL. The mean age of the studies that provided this information was 43.05 ± 11.6 years old with range (20–67). The characteristics of other studies are listed in Table 1.
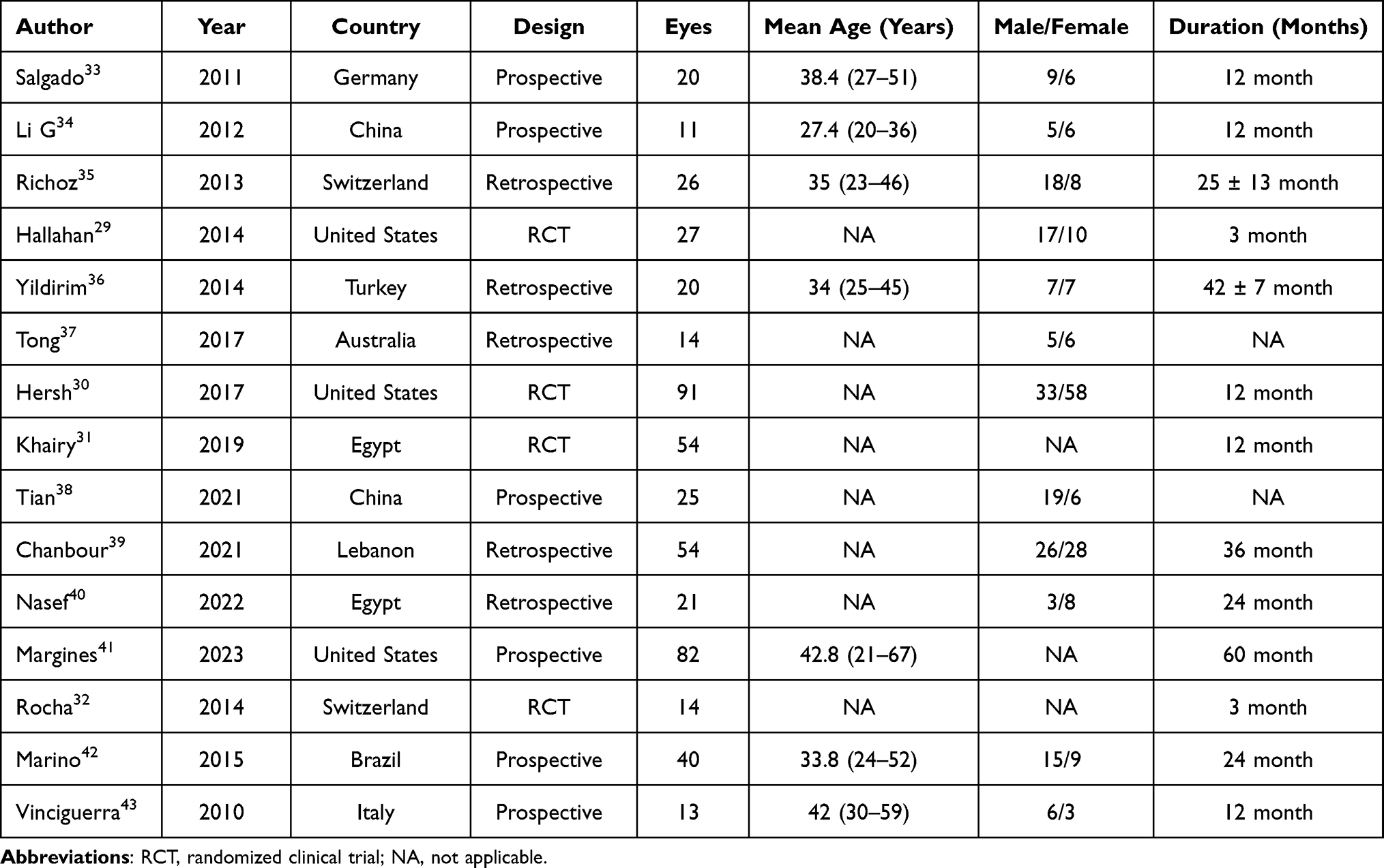 |
Table 1 Baseline Characteristics of the Studies Included |
Visual Acuity and Refractive Outcomes
Visual acuity was recorded and analyzed as the logarithm of the minimum angle of resolution (logMAR) value. Compared to the preoperative baseline, there was no significant difference in UCVA after the CXL procedure (SMD = 0.09; 95% CI: −0.07, 0.26; Figure 2), and no statistically significant heterogeneity between studies was identified (P = 0.64, I2 = 0%). However, compared with the preoperative values, the CDVA significantly improved post-CXL (SMD = 0.33; 95% CI:0.12 to 0.54; Figure 3), and heterogeneity was observed (P < 0.01, I2 = 54%).
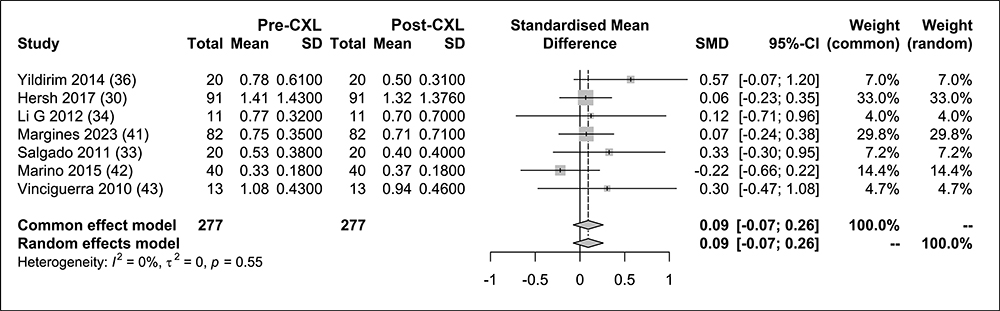 |
Figure 2 UCVA forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslining; SMD, standardized mean difference. |
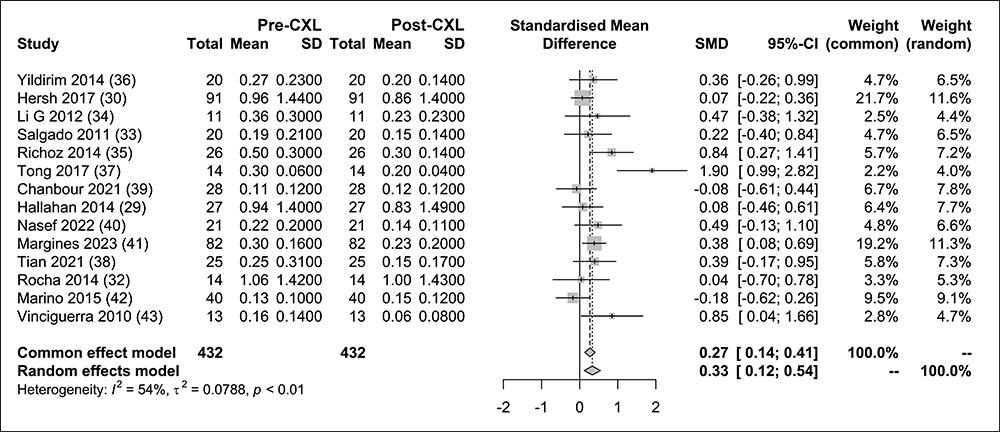 |
Figure 3 CDVA forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
Compared to the preoperative baseline, SE significantly decreased after the CXL procedure (SMD = −0.09; 95% CI: −0.35 − −0.02; Figure 4), and no statistically significant heterogeneity between studies was identified (P = 0.82, I2 = 0%).
 |
Figure 4 SE forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
Topographic Results
Kmax significantly decreased after corneal CXL treatment (SMD = 0.15; 95% CI:0.01 0.28; Figure 5). No heterogeneity was observed (P = 0.94, I2 = 0%). However, ISV did not exhibit a significant difference post-CXL (SMD = 0.15; 95% CI: −0.24, 0.54; Figure 6), with no observed heterogeneity (P = 0.51, I2 = 0%). Similarly, the IVA did not show a significant difference post-CXL (SMD = 0.03; 95% CI: −0.35, 0.42; Figure 7), and there was no heterogeneity (P = 0.38, I2 = 0%). KI also demonstrated no significant difference post-CXL (SMD = −0.02; 95% CI: −0.40 0.37; Figure 8), and no heterogeneity was observed (P = 0.99, I2 = 0%). In contrast, CKI showed no significant difference post-CXL (SMD = −0.73; 95% CI: −2.79 1.32; Figure 9), but heterogeneity was present (P < 0.01, I2 = 93%). Rmin did not show significant changes post-CXL (SMD = −0.12; 95% CI: −0.51, 0.26; Figure 10), and there was no heterogeneity (P = 0.83, I2 = 93%). The IHA did not differ significantly post-CXL (SMD = −0.21; 95% CI: −0.18, 0.59; Figure 11), and there was no heterogeneity (P = 0.65, I2 = 0%). Lastly, IHD did not show significant differences post-CXL (SMD = 1.13; 95% CI: −1.01 to 3.27; Figure 12), but heterogeneity was observed (P < 0.01, I2 = 92%).
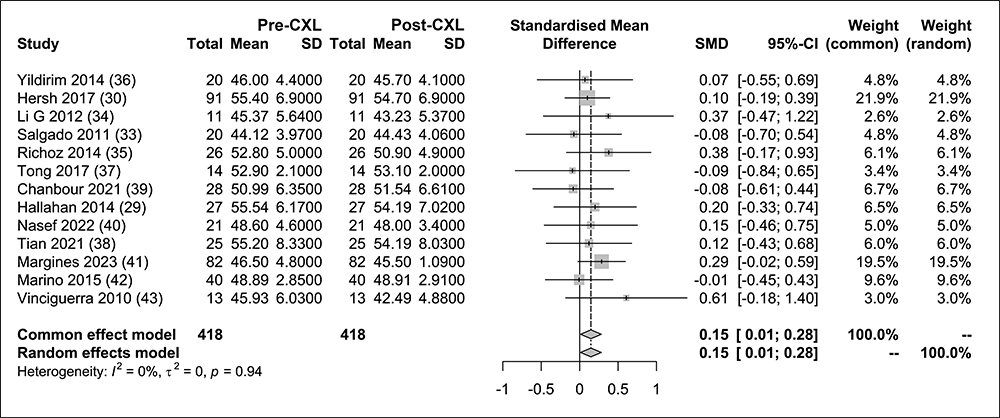 |
Figure 5 Kmax forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
 |
Figure 6 ISV forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
 |
Figure 7 IVA forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
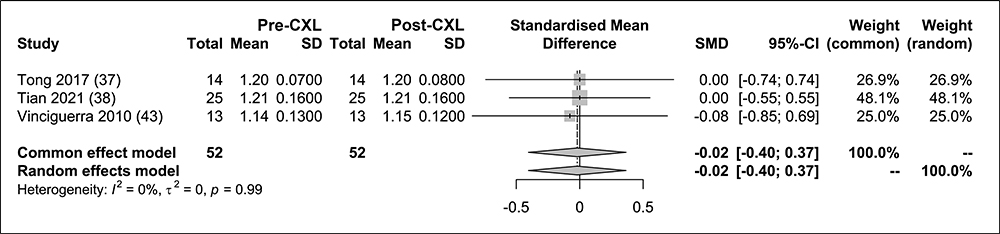 |
Figure 8 KI forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
 |
Figure 9 CKI forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
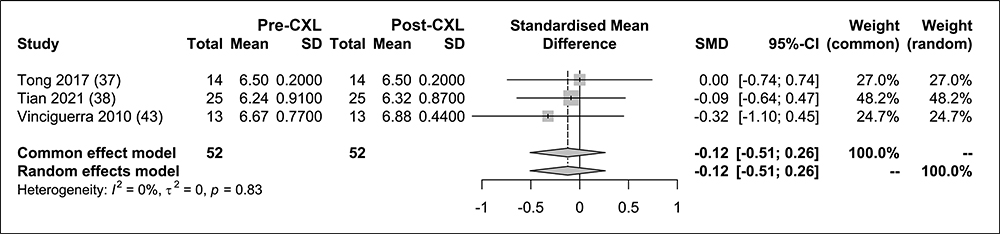 |
Figure 10 Rmin forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
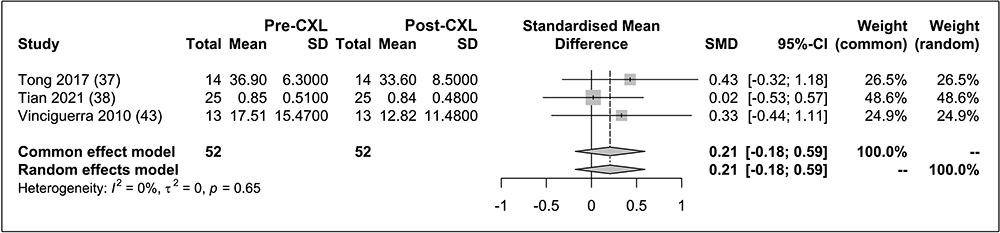 |
Figure 11 IHA forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
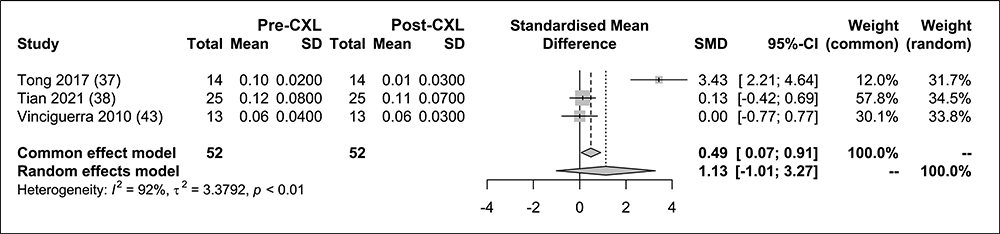 |
Figure 12 IHD forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
Central Corneal Thickness and Endothelial Cell Count
The analysis of these data revealed that the pre- and post-CXL value differences in CCT were statistically significant (SMD = 0.24; 95% CI:0.07 to 0.41; Figure 13), with decreased values after treatment.
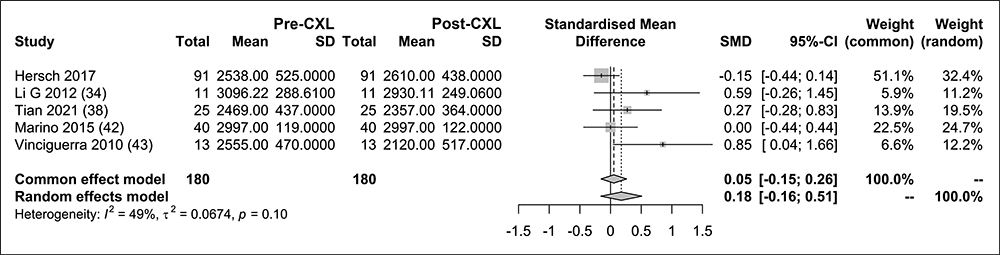 |
Figure 13 EEC forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
The difference in EEC was not statistically significant (SMD = 0.05; 95% CI: −0.15 to 0.26; Figure 14). Additionally, no statistically significant heterogeneity between studies was identified in the comparison of CCT (P = 0.58, I2 = 0%) and EEC (P = 0.10, I2 = 49%).
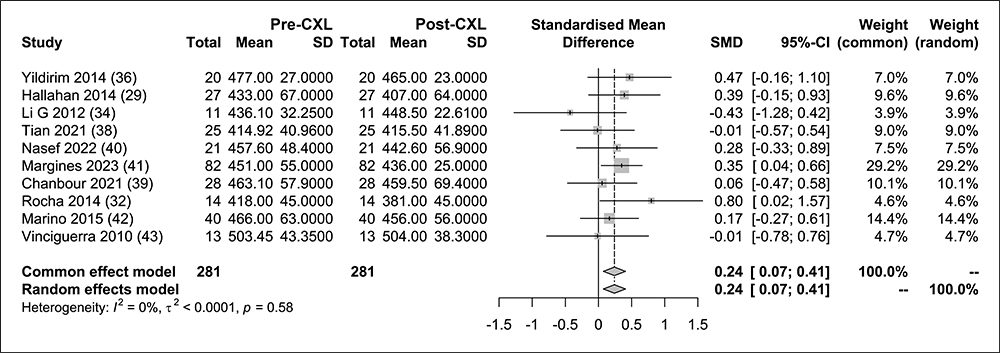 |
Figure 14 CCT forest plot. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking; SMD, standardized mean difference. |
Adverse Events and Complications
The outcomes of severe complications are illustrated in Figure 15. A solitary instance of a serious complication emerged from one study, specifically a case involving epithelial ingrowth beneath the LASIK flap. Consequently, these findings indicate an aggregate occurrence rate of 0% (accompanied by a 95% confidence interval ranging from 0% to 1%). It is worth noting that there was no statistically significant variance among the studies (P = 1.00, I² = 0%).
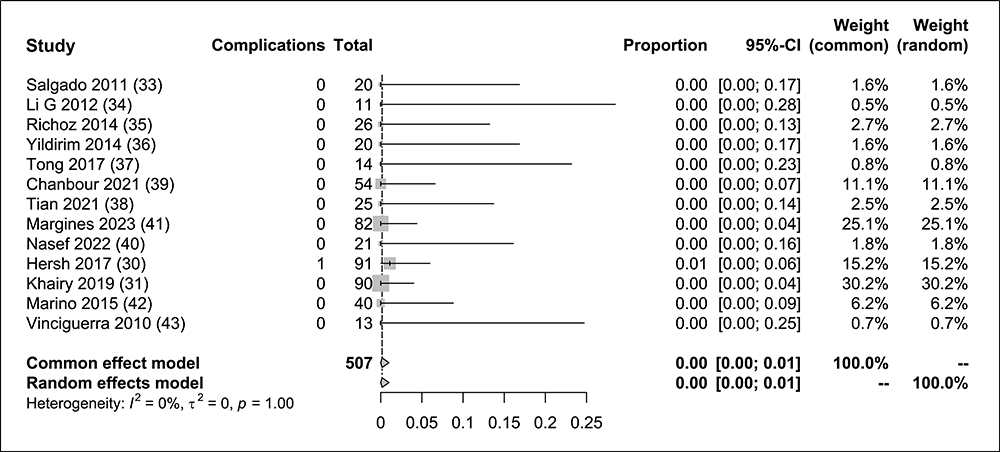 |
Figure 15 Serious Complications rates. Abbreviations: I2, heterogeneity; p, p-value; Pre-CXL, before crosslinking; Post-CXL, after crosslinking. |
Discussion
Following the introduction of corneal collagen cross-linking in the treatment of keratoconus in 2003, many researchers have demonstrated the possibility of using CXL to slow or prevent corneal ectasia progression.23,44–49 Removal of the corneal epithelium remains essential with the current techniques and technology but raises the possibility of adverse events and complications such as infections and reduced corneal transparency.2,50 Therefore, this is an updated meta-analysis of epi-off CXL for corneal ectasia following refractive surgery.
In our systematic review and meta-analysis encompassing 15 studies with 421 patients, we assessed the safety and efficacy of CXL for treating corneal ectasia following RSL. Compared to a meta-analysis involving 118 patients, our analysis included additional outcome measures such as SE, IVA, CKI, IHA, ISV, and IHD. In contrast to the previous meta-analysis, our findings revealed improved results for Kmax and SE values and reduced in CCT post-CXL. Other outcomes analyzed in the previous study remained consistent.
The benefit of visual acuity improvement appears to be the leading indicator of CXL treatment. Although the UCVA remained stable, CDVA improved significantly. In this context, Hersch et al reported that CDVA improved by 1–9 letters in 32 (44%) eyes and by ten or more letters in 23 (32%) eyes after 12 months of follow-up. Potential explanations for the enhancement in CDVA, as opposed to UDVA, following CXL could be attributed to the effect of CXL on improving corneal anterior surface regularity and potentially facilitating partial repositioning of the optical zone. Similar findings have been reported in the context of keratoconus post-crosslinking treatment.51
SE analyses are essential for evaluating refractive outcomes following corneal cross-linking in post-refractive surgery corneal ectasia. The results show a statistically significant decrease in SE after CXL, indicating a beneficial impact on refractive error, similar to other systematic reviews of CXL.52 This reduction in SE suggests that CXL contributes to the correction of defocus and possibly higher-order aberrations due to improvements in the corneal surface, which are critical for achieving better visual acuity. This can be explained by corneal flattening resulting from CXL. This flattening is associated with potential myopia correction. However, its effect on hypermetropia remains a subject of ongoing debate.53 Furthermore, the heterogeneity was low, unlike in other studies that compared SE with CXL treatment.25
Analysis of the topographic results further supports the positive impact of CXL on corneal anatomy. Significant reductions in parameters, such as Kmax, indicate flattening of the corneal curvature and might improve refractive and visual outcomes.54 One possible explanation for these differences in the outcomes is the specific focus and sensitivity of each parameter. Parameters such as Kmax are directly related to corneal curvature and astigmatism; thus, changes in these parameters are likely to be clinically significant and readily detectable.55 In contrast, other indices such as ISV and IVA may be more subtle and less responsive to the effects of CXL, particularly in cases where extreme changes in surface variance or vertical asymmetry do not primarily characterize ectasia. Additionally, individual patient variability and heterogeneity of corneal ectasia patterns could contribute to the lack of significant changes in specific parameters. Corneas with different ectatic patterns may respond differently to CXL, and this diversity could attenuate the observed effects on specific indices.56 Furthermore, because simulated keratometry does not consider the total corneal surface, we considered the Klyce57–60 and Ambrósio61 indices of keratoconus. The CKI decreased with decreasing severity of central keratoconus. This augmentation may be consistent with the fact that ectatic corneas after excimer laser refractive surgery may have the most pronounced curvature changes near the center and that CXL may result in improvements in this central corneal area, where the deepest ablation and tissue removal are found. Therefore, there seemed to be a stabilization of corneal curvature and a trend towards central flattening, leading to an enhanced refractive outcome.
In contrast to the previous meta-analysis, this analysis revealed a statistically significant decrease in CCT after CXL. This occurs because of the regularization of epithelium and compaction of the collagen lamellae in the corneal stroma. Similar results have been reported for keratoconus after postoperative crosslinking.62,63 The lack of statistical heterogeneity in this outcome enhanced the reliability of this finding, indicating consistency across the included studies. Conversely, the evaluation of the EEC did not show a statistically significant change after CXL. The stability in EEC implies that the CXL procedure does not harm endothelial cells, which are essential for maintaining corneal deturgescence and transparency, as well as in previous studies.35,64 The moderate heterogeneity observed in this result suggests that variations in study methodologies and patient populations may play a role in changes in EEC.
The observed results in parameters like Kmax value (showing tissue applanation) are likely due to the improved biomechanical stability of the cornea after CXL, a trend consistent with findings in primary keratoconus patients undergoing similar treatment.23,34 Another study noted corneal changes after CXL in a comparable manner, though less pronounced, in eyes with keratoconus.43,46 However, contrasting results emerged from a different study, where the progression rate post-CXL was notably higher in patients with ectasia compared to those with keratoconus over three years.39 Additionally, in another investigation, CDVA and Kmax were inferior in patients with ectasia compared to keratoconus patients after CXL.65 This discrepancy may be attributed to heightened variability in the timeline of changes in ectasia patients compared to those with keratoconus. The underlying cause of these potential differences between keratoconus and post-RSL ectatic corneas remains unclear. Various factors, such as biomechanical disparities introduced by the LASIK flap, possible differences in riboflavin diffusion rates in post-LASIK corneas (especially at the flap interface), and intrinsic pathophysiologic distinctions between keratoconus and post-RSL ectasia may contribute to the varied responses to CXL observed in these groups.65 To gain a more comprehensive understanding of these differences and determine which is more stable between eyes with keratoconus and eyes with corneal ectasia after RLS, further research involving a more significant number of eyes is essential.
Some investigations of ectasia risk factors have shown it is necessary. LASIK surgery may compromise the cornea’s structural integrity by diminishing the total load-bearing tissue available and reallocating the load-bearing duty to the structurally less robust posterior stromal layer of the cornea.66 The eye asymmetry scoring67 and the presence of abnormal topography are the other risk factors for ectasia.68–70 The Belin-Ambrosio Enhanced Ectasia Display (BAD) uses nine specific parameters, including elevation and pachymetry data, to generate a “D value”. This value identifies patients at risk for keratoconus or conditions like keratoconus who might not be suitable for refractive surgery or may have a poor prognosis.70 The BAD provides an exhaustive perspective on the corneal tomography architecture, thereby enabling the identification of such patients via a holistic examination. Thus, factors including the topographic abnormality, percentage tissue altered, residual stromal thickness, inferior-superior index of the sagittal map, Bellin Ambrosio display data, and information from the thickness curve map are acknowledged risk factors for ectasia development.68,69,71 However, our investigation into this topic was constrained by inconsistent data availability across the analyzed studies. The lack of detailed information about this data in many of the included studies limited our ability to delve deeper into understanding these risk factors’ role in CXL treatment. Due to this, it is necessary future research that consistently incorporates these metrics, allowing for more robust analyses and more definitive conclusions about the causes of ectasia after RLS and different prognoses after CXL.
CXL for corneal ectasia after RLS proved to be a safe procedure, with an extremely low complication rate. The absence of statistically significant variance among the studies suggests that complications after CXL are relatively rare and are not significantly affected by variations in the study methodologies. Most CXL complications are caused by corneal epithelial removal. Innovative protocol modifications are used to improve safety and efficacy without the need for epithelial removal and to expand indications in thinner corneas.64,72–77 We look forward to reviewing the results of these new techniques and technologies shortly.
Our meta-analysis had limitations and biases due to the quality of the selected studies. While the results of this meta-analysis provide valuable insights into the safety and efficacy of corneal collagen cross-linking for treating post-refractive surgery corneal ectasia, it is essential to consider the limitations of this study. As corneal ectasia after refractive surgery has a low occurrence, our analysis included a relatively small number of studies and patients. Although the inclusion of 15 studies is a strength, a larger dataset would provide more robust and generalizable conclusions. The presence of heterogeneity in some outcomes, such as CKI, IHD, and EEC, suggests variability in treatment responses across studies. This variability could be influenced by factors, such as variations in CXL protocols, patient populations, and study methodologies. Many studies included in this analysis reported follow-up periods ≥ 12 months. However, long-term outcomes beyond the follow-up period were not assessed. It is essential to evaluate the stability of CXL effects over an extended period. The possibility of publication bias cannot be ruled out, as studies with positive or significant results may be more likely to be published, whereas studies with negative or non-significant findings may not. This bias may have affected the overall conclusions of the meta-analysis. Different studies may have employed variations in CXL protocols, such as the type of riboflavin used, ultraviolet light intensity, and duration of treatment. These variations can influence treatment outcomes and introduce heterogeneity. The meta-analysis relied on aggregated data from published studies. Individual patient data were not available for analysis, which could have provided a more detailed understanding of the treatment effects and potential predictors of response. The included studies were conducted in various countries, potentially introducing variability in the patient demographics, surgical techniques, and follow-up protocols. This may limit the generalizability of the findings to a broader population. This meta-analysis primarily focused on assessing the outcomes of CXL treatment compared with the preoperative baseline values. It did not include a direct comparison with alternative treatments for post-refractive surgery corneal ectasia, limiting its ability to determine the relative efficacy of CXL.
Conclusions
In conclusion, this systematic review and meta-analysis suggest that CXL for managing cases of corneal ectasia after surgery is a safe and effective technique, successfully arresting or stopping the process of corneal ectasia, improving topographic indices, and providing good refractive and visual outcomes with a very low risk of severe complications. There is a need to standardize protocols for riboflavin concentration, duration of UV exposure, and classification of corneal ectasia severity before treatment for better understanding and indication of this treatment and patient counseling. Moreover, conducting a new meta-analysis to validate these findings is essential, especially as more randomized, more significant, and longer clinical trials become available for publication.
Data Sharing Statement
All relevant data are within the paper.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
References
1. Comaish IF, Lawless MA. Progressive post-LASIK keratectasia: biomechanical instability or chronic disease process? J Cataract Refract Surg. 2002;28(12):2206–2213. doi:10.1016/s0886-3350(02)01698-x
2. Seiler T, Koufala K, Richter G. Iatrogenic keratectasia after laser in situ keratomileusis. J Refract Surg. 1998;14(3):312–317. doi:10.3928/1081-597X-19980501-15
3. Gomes JA, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359–369. doi:10.1097/ICO.0000000000000408
4. Hafezi F, Kanellopoulos J, Wiltfang R, Seiler T. Corneal collagen crosslinking with riboflavin and ultraviolet A to treat induced keratectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2007;33(12):2035–2040. doi:10.1016/j.jcrs.2007.07.028
5. Binder PS. Ectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2003;29(12):2419–2429. doi:10.1016/j.jcrs.2003.10.012
6. Ambrosio R, Randleman JB. Screening for ectasia risk: what are we screening for and how should we screen for it? J Refract Surg. 2013;29(4):230–232. doi:10.3928/1081597X-20130318-01
7. Moshirfar M, Tukan AN, Bundogji N, et al. Ectasia after corneal refractive surgery: a systematic review. Ophthalmol Ther. 2021;10(4):753–776. doi:10.1007/s40123-021-00383-w
8. Bohac M, Koncarevic M, Pasalic A, et al. Incidence and Clinical Characteristics of Post LASIK Ectasia: a Review of over 30,000 LASIK Cases. Semin Ophthalmol. 2018;33(7–8):869–877. doi:10.1080/08820538.2018.1539183
9. Romero-Jiménez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: a review. Cont Lens Anterior Eye. 2010;33(4):157–66; quiz 205. doi:10.1016/j.clae.2010.04.006
10. Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008;115(1):37–50. doi:10.1016/j.ophtha.2007.03.073
11. Ortiz D, Piñero D, Shabayek MH, Arnalich-Montiel F, Alió JL. Corneal biomechanical properties in normal, post-laser in situ keratomileusis, and keratoconic eyes. J Cataract Refract Surg. 2007;33(8):1371–1375. doi:10.1016/j.jcrs.2007.04.021
12. González-Méijome JM, Villa-Collar C, Queirós A, Jorge J, Parafita MA. Pilot study on the influence of corneal biomechanical properties over the short term in response to corneal refractive therapy for myopia. Cornea. 2008;27(4):421–426. doi:10.1097/ICO.0b013e318164e49d
13. Kirwan C, O’Keefe M. Corneal hysteresis using the Reichert ocular response analyser: findings pre- and post-LASIK and LASEK. Acta Ophthalmol. 2008;86(2):215–218. doi:10.1111/j.1600-0420.2007.01023.x
14. Ambrósio R, Salomão MQ, Barros L, et al. Multimodal diagnostics for keratoconus and ectatic corneal diseases: a paradigm shift. Eye Vis. 2023;10(1):45. doi:10.1186/s40662-023-00363-0
15. Salomão MQ, Hoffling-Lima AL, Sena N, Lopes BT, Guedes J, Ambrósio R. Enhanced screening for ectasia risk: multimodal refractive imaging observations from the fellow unoperated eye of patients with post-laser in situ Keratomileusis Ectasia. Cornea Open. 2024;3(1):e0023. doi:10.1097/coa.0000000000000023
16. Salomao MQ, Hofling-Lima AL, Gomes Esporcatte LP, et al. Ectatic diseases. Exp Eye Res. 2021;202:108347. doi:10.1016/j.exer.2020.108347
17. Belin MW, Alizadeh R, Torres-Netto EA, Hafezi F, Ambrosio R, Pajic B. Determining progression in ectatic corneal disease. Asia Pac J Ophthalmol. 2020;9(6):541–548. doi:10.1097/APO.0000000000000333
18. Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prognosis for corneal ectasia after LASIK. Ophthalmology. 2003;110(2):267–275. doi:10.1016/S0161-6420(02)01727-X
19. Tan DT, Por YM. Current treatment options for corneal ectasia. Curr Opin Ophthalmol. 2007;18(4):284–289. doi:10.1097/ICU.0b013e3281a7ecaa
20. Rodriguez LA, Guillen PB, Benavides MA, Garcia L, Porras D, Daqui-Garay RM. Penetrating keratoplasty versus intrastromal corneal ring segments to correct bilateral corneal ectasia: preliminary study. J Cataract Refract Surg. 2007;33(3):488–496. doi:10.1016/j.jcrs.2006.09.048
21. Bilgihan K, Ozdek SC, Sari A, Hasanreisoglu B. Excimer laser-assisted anterior lamellar keratoplasty for keratoconus, corneal problems after laser in situ keratomileusis, and corneal stromal opacities. J Cataract Refract Surg. 2006;32(8):1264–1269. doi:10.1016/j.jcrs.2006.02.056
22. Hashemi H, Ambrosio R, Vinciguerra R, et al. Two-year changes in corneal stiffness parameters after accelerated corneal cross-linking. J Biomech. 2019;93:209–212. doi:10.1016/j.jbiomech.2019.06.011
23. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/s0002-9394(02)02220-1
24. Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;66(1):97–103. doi:10.1006/exer.1997.0410
25. Chunyu T, Xiujun P, Zhengjun F, Xia Z, Feihu Z. Corneal collagen cross-linking in keratoconus: a systematic review and meta-analysis. Sci Rep. 2014;4:5652. doi:10.1038/srep05652
26. Wan Q, Wang D, Ye H, Tang J, Han Y. A review and meta-analysis of corneal cross-linking for post-laser vision correction ectasia. J Curr Ophthalmol. 2017;29(3):145–153. doi:10.1016/j.joco.2017.02.008
27. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol. 2021;74(9):790–799. doi:10.1016/j.rec.2021.07.010
28. Santhiago MR, Smadja D, Gomes BF, et al. Association between the percent tissue altered and post-laser in situ keratomileusis ectasia in eyes with normal preoperative topography. Am J Ophthalmol. 2014;158(1):87–95 e1. doi:10.1016/j.ajo.2014.04.002
29. Hallahan KM, Rocha K, Roy AS, Randleman JB, Stulting RD, Dupps WJ. Effects of corneal cross-linking on ocular response analyzer waveform-derived variables in keratoconus and postrefractive surgery ectasia. Eye Contact Lens. 2014;40(6):339–344. doi:10.1097/ICL.0000000000000090
30. Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK; Group USCS. U.S. multicenter clinical trial of corneal collagen crosslinking for treatment of corneal ectasia after refractive surgery. Ophthalmology. 2017;124(10):1475–1484. doi:10.1016/j.ophtha.2017.05.036
31. Khairy HA, Elsawy MF, Said-Ahmed K, Zaki MA, Mandour SS. Accelerated versus standard corneal cross linking in the treatment of ectasia post refractive surgery and penetrating keratoplasty: a medium term randomized trial. Int J Ophthalmol. 2019;12(11):1714–1719. doi:10.18240/ijo.2019.11.08
32. Rocha KM, Perez-Straziota CE, Stulting RD, Randleman JB. Epithelial and stromal remodeling after corneal collagen cross-linking evaluated by spectral-domain OCT. J Refract Surg. 2014;30(2):122–127. doi:10.3928/1081597X-20140120-08
33. Salgado JP, Khoramnia R, Lohmann CP, Winkler von Mohrenfels C. Corneal collagen crosslinking in post-LASIK keratectasia. Br J Ophthalmol. 2011;95(4):493–497. doi:10.1136/bjo.2010.179424
34. Li G, Fan ZJ, Peng XJ. Corneal collagen crosslinking for corneal ectasia of post-LASIK: one-year results. Int J Ophthalmol. 2012;5(2):190–195. doi:10.3980/j.issn.2222-3959.2012.02.15
35. Richoz O, Mavrakanas N, Pajic B, Hafezi F. Corneal collagen cross-linking for ectasia after LASIK and photorefractive keratectomy: long-term results. Ophthalmology. 2013;120(7):1354–1359. doi:10.1016/j.ophtha.2012.12.027
36. Yildirim A, Cakir H, Kara N, et al. Corneal collagen crosslinking for ectasia after laser in situ keratomileusis: long-term results. J Cataract Refract Surg. 2014;40(10):1591–1596. doi:10.1016/j.jcrs.2014.01.042
37. Tong JY, Viswanathan D, Hodge C, Sutton G, Chan C, Males JJ. Corneal Collagen Crosslinking for Post-LASIK Ectasia: an Australian Study. Asia Pac J Ophthalmol. 2017;6(3):228–232. doi:10.22608/APO.2016197
38. Tian M, Zhang X, Jian W, Sun L, Shen Y, Zhou X. Long-term follow-up of accelerated transepithelial corneal crosslinking for post-LASIK Ectasia: a pilot prospective observational study. Front Bioeng Biotechnol. 2021;9:809262. doi:10.3389/fbioe.2021.809262
39. Chanbour W, El Zein L, Younes MA, et al. corneal cross-linking for keratoconus and post-LASIK Ectasia and failure rate: a 3 years follow-up study. Cureus. 2021;13(11):e19552. doi:10.7759/cureus.19552
40. Nasef MH, El Emam SY, Haleem TI, Shalaby WS, Allam WA. Visual and topographic outcomes of corneal collagen cross linking for post LASIK Ectasia. Clin Ophthalmol. 2022;16:2025–2032. doi:10.2147/OPTH.S370033
41. Margines JB, Rabinowitz YS, Li X, Gaster RN. Results of corneal collagen cross-linking in patients with corneal ectasia after laser refractive surgery-A prospective study. Photodiagnosis Photodyn Ther. 2023;42:103521. doi:10.1016/j.pdpdt.2023.103521
42. Marino GK, Torricelli AA, Giacomin N, Santhiago MR, Espindola R, Netto MV. Accelerated corneal collagen cross-linking for postoperative LASIK Ectasia: two-year outcomes. J Refract Surg. 2015;31(6):380–384. doi:10.3928/1081597X-20150521-04
43. Vinciguerra P, Camesasca FI, Albe E, Trazza S. Corneal collagen cross-linking for ectasia after excimer laser refractive surgery: 1-year results. J Refract Surg. 2010;26(7):486–497. doi:10.3928/1081597X-20090910-02
44. O’Brart DP, Kwong TQ, Patel P, McDonald RJ, O’Brart NA. Long-term follow-up of riboflavin/ultraviolet A (370 nm) corneal collagen cross-linking to halt the progression of keratoconus. Br J Ophthalmol. 2013;97(4):433–437. doi:10.1136/bjophthalmol-2012-302556
45. Hashemi H, Seyedian MA, Miraftab M, Fotouhi A, Asgari S. Corneal collagen cross-linking with riboflavin and ultraviolet a irradiation for keratoconus: long-term results. Ophthalmology. 2013;120(8):1515–1520. doi:10.1016/j.ophtha.2013.01.012
46. Vinciguerra P, Albe E, Trazza S, et al. Refractive, topographic, tomographic, and aberrometric analysis of keratoconic eyes undergoing corneal cross-linking. Ophthalmology. 2009;116(3):369–378. doi:10.1016/j.ophtha.2008.09.048
47. Coskunseven E, Jankov MR, Hafezi F. Contralateral eye study of corneal collagen cross-linking with riboflavin and UVA irradiation in patients with keratoconus. J Refract Surg. 2009;25(4):371–376. doi:10.3928/1081597X-20090401-02
48. Kymionis GD, Mikropoulos DG, Portaliou DM, Voudouragkaki IC, Kozobolis VP, Konstas AG. An overview of corneal collagen cross-linking (CXL). Adv Ther. 2013;30(10):858–869. doi:10.1007/s12325-013-0065-9
49. Shetty R, Kaweri L, Pahuja N, et al. Current review and a simplified ”five-point management algorithm” for keratoconus. Indian J Ophthalmol. 2015;63(1):46–53. doi:10.4103/0301-4738.151468
50. Seiler T, Quurke AW. Iatrogenic keratectasia after LASIK in a case of forme fruste keratoconus. J Cataract Refract Surg. 1998;24(7):1007–1009. doi:10.1016/s0886-3350(98)80057-6
51. Caporossi A, Baiocchi S, Mazzotta C, Traversi C, Caporossi T. Parasurgical therapy for keratoconus by riboflavin-ultraviolet type A rays induced cross-linking of corneal collagen: preliminary refractive results in an Italian study. J Cataract Refract Surg. 2006;32(5):837–845. doi:10.1016/j.jcrs.2006.01.091
52. Shajari M, Kolb CM, Agha B, et al. Comparison of standard and accelerated corneal cross-linking for the treatment of keratoconus: a meta-analysis. Acta Ophthalmol. 2019;97(1):e22–e35. doi:10.1111/aos.13814
53. Juthani VV, Chuck RS. Corneal Crosslinking in Refractive Corrections. Transl Vis Sci Technol. 2021;10(5):4. doi:10.1167/tvst.10.5.4
54. Knutsson KA, Genovese PN, Paganoni G, et al. Safety and efficacy of corneal cross-linking in patients affected by keratoconus: long-term results. Med Sci. 2023;11:2.
55. Hashemi H, Asgari S, Mahmoud AM, Mehravaran S, Roberts CJ. Variability of CLMI-X parameters, zonal Kmax, and single-point Kmax in keratoconus progression. Eye. 2023;37(15):3197–3202. doi:10.1038/s41433-023-02476-1
56. Greenstein SA, Hersh PS. Characteristics influencing outcomes of corneal collagen crosslinking for keratoconus and ectasia: implications for patient selection. J Cataract Refract Surg. 2013;39(8):1133–1140. doi:10.1016/j.jcrs.2013.06.007
57. Smolek MK, Klyce SD. Current keratoconus detection methods compared with a neural network approach. Invest Ophthalmol Vis Sci. 1997;38(11):2290–2299.
58. Maeda N, Klyce SD, Smolek MK. Comparison of methods for detecting keratoconus using videokeratography. Arch Ophthalmol. 1995;113(7):870–874. doi:10.1001/archopht.1995.01100070044023
59. Maeda N, Klyce SD, Smolek MK, Thompson HW. Automated keratoconus screening with corneal topography analysis. Invest Ophthalmol Vis Sci. 1994;35(6):2749–2757.
60. Smolek MK, Klyce SD. Zernike polynomial fitting fails to represent all visually significant corneal aberrations. Invest Ophthalmol Vis Sci. 2003;44(11):4676–4681. doi:10.1167/iovs.03-0190
61. Ambrosio R, Alonso RS, Luz A, Coca Velarde LG. Corneal-thickness spatial profile and corneal-volume distribution: tomographic indices to detect keratoconus. J Cataract Refract Surg. 2006;32(11):1851–1859. doi:10.1016/j.jcrs.2006.06.025
62. Dupps WJ, Wilson SE. Biomechanics and wound healing in the cornea. Exp Eye Res. 2006;83(4):709–720. doi:10.1016/j.exer.2006.03.015
63. Saleh S, Koo EB, Lambert SR, Manche EE. Outcomes after corneal crosslinking for keratoconus in children and young adults. Cornea. 2022;41(4):408–416. doi:10.1097/ICO.0000000000002730
64. Hafezi F, Mrochen M, Iseli HP, Seiler T. Collagen crosslinking with ultraviolet-A and hypoosmolar riboflavin solution in thin corneas. J Cataract Refract Surg. 2009;35(4):621–624. doi:10.1016/j.jcrs.2008.10.060
65. Hersh PS, Greenstein SA, Fry KL. Corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(1):149–160. doi:10.1016/j.jcrs.2010.07.030
66. Shah Z, Singh S, Shilpy N, Purohit D. Prevalence of corneal topographic patterns in ectatic corneal diseases. Optom Vis Sci. 2022;99(7):560–567. doi:10.1097/OPX.0000000000001908
67. Vahdati A, Seven I, Mysore N, Randleman JB, Dupps WJ. Computational biomechanical analysis of asymmetric ectasia risk in unilateral post-LASIK Ectasia. J Refract Surg. 2016;32(12):811–820. doi:10.3928/1081597X-20160929-01
68. Randleman JB, Trattler WB, Stulting RD. Validation of the Ectasia Risk Score System for preoperative laser in situ keratomileusis screening. Am J Ophthalmol. 2008;145(5):813–818. doi:10.1016/j.ajo.2007.12.033
69. Santhiago MR, Giacomin NT, Smadja D, Bechara SJ. Ectasia risk factors in refractive surgery. Clin Ophthalmol. 2016;10:713–720. doi:10.2147/OPTH.S51313
70. Ambrósio R, Faria-Correia F, Ramos I, et al. Enhanced screening for ectasia susceptibility among refractive candidates: the role of corneal tomography and biomechanics. Curr Ophthalmol Rep. 2013;1(1):28–38. doi:10.1007/s40135-012-0003-z
71. Santhiago MR, Smadja D, Wilson SE, Krueger RR, Monteiro ML, Randleman JB. Role of percent tissue altered on ectasia after LASIK in eyes with suspicious topography. J Refract Surg. 2015;31(4):258–265. doi:10.3928/1081597X-20150319-05
72. Kymionis GD, Diakonis VF, Coskunseven E, Jankov M, Yoo SH, Pallikaris IG. Customized pachymetric guided epithelial debridement for corneal collagen cross linking. BMC Ophthalmol. 2009;9:10. doi:10.1186/1471-2415-9-10
73. Sachdev MS, Gupta D, Sachdev G, Sachdev R. Tailored stromal expansion with a refractive lenticule for crosslinking the ultrathin cornea. J Cataract Refract Surg. 2015;41(5):918–923. doi:10.1016/j.jcrs.2015.04.007
74. Jacob S, Kumar DA, Agarwal A, Basu S, Sinha P, Agarwal A. Contact lens-assisted collagen cross-linking (CACXL): a new technique for cross-linking thin corneas. J Refract Surg. 2014;30(6):366–372. doi:10.3928/1081597X-20140523-01
75. Leccisotti A, Islam T. Transepithelial corneal collagen cross-linking in keratoconus. J Refract Surg. 2010;26(12):942–948. doi:10.3928/1081597X-20100212-09
76. Bikbova G, Bikbov M. Transepithelial corneal collagen cross-linking by iontophoresis of riboflavin. Acta Ophthalmol. 2014;92(1):e30–4. doi:10.1111/aos.12235
77. Agarwal R, Jain P, Arora R. Complications of corneal collagen cross-linking. Indian J Ophthalmol. 2022;70(5):1466–1474. doi:10.4103/ijo.IJO_1595_21
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.