Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Core Symptoms and Candidate Targets for Symptom Management in Late Pregnancy: A Network Analysis
Authors Zhang X, Zhao Y, Yang J, Xu J, Jiang P, Zhu Y, Mu T, Li Y
Received 27 March 2026
Accepted for publication 30 June 2026
Published 10 July 2026 Volume 2026:19 611736
DOI https://doi.org/10.2147/JMDH.S611736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jagdish Khubchandani
Xingruo Zhang,1 Yunfeng Zhao,1 Jiani Yang,1 Jing Xu,1 Panpan Jiang,1 Yanxia Zhu,2 Tingyu Mu,1 Yuhong Li1,3
1School of Nursing, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 2Department of Science and Education, Anhui Province Maternity and Child Health Hospital, Hefei, Anhui, People’s Republic of China; 3Department of Nursing, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
Correspondence: Yuhong Li, School of Nursing, Anhui Medical University, No. 81 Meishan Road, Shushan District, Hefei, Anhui, 230032, People’s Republic of China, Email [email protected] Tingyu Mu, School of Nursing, Anhui Medical University, No. 81 Meishan Road, Shushan District, Hefei, Anhui, 230032, People’s Republic of China, Email [email protected]
Purpose: Women in late pregnancy experience multiple co-occurring physical and psychological symptoms that may affect daily functioning and well-being. However, conventional approaches are limited in identifying priority intervention targets within complex symptom patterns. This study aimed to identify core symptoms and potential targets for symptom management using a network-based approach.
Patients and Methods: A cross-sectional study was conducted among 444 women in late pregnancy recruited by convenience sampling from a maternal and child health hospital and a tertiary general hospital. Data were collected using a general information questionnaire and a Symptom Assessment Scale for Women in Late Pregnancy, which demonstrated good content validity and internal consistency. Symptom clusters were identified using exploratory factor analysis with principal component extraction, and a covariate-adjusted symptom network was constructed to explore inter-symptom relationships. Computer-simulated interventions were performed to examine the potential impact of symptom alleviation and aggravation within the network.
Results: Six symptom clusters were identified: sleep and physical discomfort, cardiopulmonary load-related, emotional, gastrointestinal, uterine activity-related, and limb/skin clusters. After controlling for covariates, the cluster-specific core symptoms were fatigue (strength = 0.93), chest tightness (strength = 1.18), anxiety (strength = 1.15), nausea (strength = 0.70), abdominal tightness (strength = 1.26), and numbness or tingling in the hands, feet, or legs (strength = − 0.11). Simulation analyses suggested that, in the alleviation simulations, shortness of breath/dyspnoea, fatigue, and chest tightness were associated with the largest simulated reductions in overall symptom burden. In the aggravation simulations, loss of appetite, nausea, and anxiety showed the largest simulated increases in overall symptom burden.
Conclusion: This study identified key symptoms and candidate symptom targets within interconnected symptom networks in late pregnancy. The findings may provide exploratory insights for multidisciplinary healthcare professionals, including midwives and obstetricians, to better prioritise and individualise symptom assessment and management in antenatal care.
Keywords: late pregnancy, symptom clusters, network analysis, simulated intervention, intervention targets, clinical prioritisation
Introduction
Late pregnancy represents the stage of gestation with the greatest physical and psychological burden.1,2 As the fetus grows rapidly and maternal physiological demands increase, women commonly experience multiple concurrent symptoms, including difficulty falling asleep,3 pain,4 fatigue,5 and anxiety,6 among others, with an average of 5–16 symptoms reported concurrently.7 The co-occurrence of these symptoms may impair maternal quality of life and is associated with adverse maternal and neonatal outcomes, including gestational hypertension,8 fear of childbirth,9 fetal growth restriction,10 caesarean delivery,11 and adverse offspring outcomes.12 However, the key symptoms requiring priority attention and the interconnections among individual symptoms remain insufficiently understood, which may limit targeted symptom assessment and management and contribute to suboptimal symptom control. Therefore, identifying key symptoms and clarifying intervention priorities has become a critical challenge in contemporary midwifery practice and symptom management.
Against this backdrop, the symptom cluster perspective offers an important conceptual approach. Symptom clusters are typically defined as collections of two or more interrelated symptoms that occur simultaneously, emphasising the potential for synergistic or amplifying effects among symptoms.13 Research in the perinatal field has identified multiple patterns of late-pregnancy symptom clusters, such as those related to body image, activity endurance, and emotional status,14–16 indicating that symptoms in late pregnancy do not occur in isolation but are interconnected in specific patterns. Although symptom cluster analysis has improved understanding of co-occurring symptoms and provided useful information for clinical management, it primarily focuses on symptom grouping and provides limited insight into the complex interrelationships among individual symptoms. Consequently, complementary analytical approaches may be needed to further characterise symptom interconnections within the broader symptom system.
In recent years, network analysis has been widely applied in multi-symptom research as a systems-oriented approach. This method conceptualises symptoms as interconnected nodes and employs centrality metrics to identify core symptoms with high influence within the network.17,18 However, traditional network analysis is primarily based on static associations and may provide limited information regarding how changes in individual symptoms could influence the broader symptom network. Existing studies have primarily focused on identifying symptom clusters or network structures, while the potential impact of targeting specific symptoms on overall symptom burden in late pregnancy remains insufficiently explored.
Traditional clinical intervention studies, however, often face challenges such as high cost, lengthy timeframes, and ethical constraints when testing multiple symptom-targeted strategies simultaneously.19 Computational simulation, as an extension of network analysis, enables systematic testing of the effects of intervening on different symptoms within the network, thereby revealing potential cascading effects that may be undetectable through conventional analyses.20 By adjusting symptom activation probabilities or network parameters, this approach more closely approximates real-world clinical scenarios and allows identification of potential intervention priorities that have the greatest impact on overall symptom burden.21,22 However, the application of simulation-based network approaches in pregnancy research remains limited, and their potential utility for understanding symptom interrelationships in late pregnancy has received relatively little attention.
Accordingly, the present study combines network analysis with computational simulation techniques to identify core symptoms within the symptom network of women in late pregnancy, to characterise inter-symptom relationships, and to explore candidate symptoms that may warrant priority attention in future symptom-management research. These findings may provide exploratory evidence for developing more targeted and individualized symptom-management approaches in antenatal care.
Materials and Methods
This study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement to enhance research quality and transparency.
Study Design and Participants
A cross-sectional survey was conducted using convenience sampling. Given the clinical setting, this recruitment approach allowed eligible women in late pregnancy to be identified and invited during routine antenatal visits and hospitalisation. Because of the cross-sectional design, the associations observed in this study should not be interpreted as evidence of causal relationships. From May to September 2025, pregnant women in late pregnancy who attended the outpatient clinics and inpatient wards of a maternal and child health hospital and a tertiary general hospital in a province were recruited. Inclusion criteria were as follows: (1) age ≥20 years (the legal age of marriage in China); (2) gestational age ≥28 weeks; (3) singleton pregnancy; (4) basic literacy skills with no cognitive impairment (eg. dementia); (5) provision of informed consent and voluntary participation. Exclusion criteria were: (1) history of severe mental illness or dysfunction of major organs such as the heart, lungs, or kidneys; (2) uncertain pregnancy outcomes (eg. scheduled termination of pregnancy, threatened miscarriage).
Sample Size Calculation
For exploratory factor analysis, the recommended sample size is 5~10 times the number of items. This study included 37 symptom items. Considering a possible 10% non-response rate, the required sample size was estimated to be 206~412 participants. The minimum sample size for network analysis was calculated using the formula N+[N×(N−1)/2], where N represents the number of symptoms. Taking into account symptoms with an prevalence lower than 40%, the expected number of symptom nodes included in the network was about 20~30. Accordingly, the estimated minimum sample size ranged from 210 to 465 participants.
Data Collection
Data were collected using a structured questionnaire. Prior to data collection, trained researchers approached women in late pregnancy in the obstetric outpatient waiting area or fetal monitoring room for standardised, face-to-face communication. The purpose, significance, and confidentiality principles of the study were explained in detail, including anonymous participation and encrypted data storage, with an emphasis on voluntary participation and the right to withdraw at any time. After obtaining informed consent, questionnaires were distributed on site. To reduce potential self-report bias, trained researchers provided standardized instructions before questionnaire completion, emphasized anonymous participation and confidentiality, and encouraged participants to answer independently based on their actual symptom experiences. Researchers remained available to clarify questions without guiding responses, and questionnaires were retrieved immediately after completion and checked on site only for completeness. In total, 465 questionnaires were distributed; 21 were excluded due to >20% missing data, leaving 444 valid questionnaires, with a valid response rate of 95.48%.
Measures
Sociodemographic and Antenatal Clinical Characteristics
Sociodemographic data included age, monthly household income per capita, educational attainment, occupation, place of residence, smoking history, and alcohol history. Antenatal clinical characteristics included gestational age, pre-pregnancy body mass index (BMI), gestational weight gain, history of live birth, history of miscarriage, mode of conception, duration of exercise during pregnancy, and pregnancy complications.
Symptoms in Late Pregnancy
A self-developed Symptom Assessment Scale for Women in Late Pregnancy was used to systematically evaluate symptom experiences during the past week. The scale was based on Symptom Management Theory and informed by the Memorial Symptom Assessment Scale.23 Initial items were generated through literature review, open-ended interviews, and subsequently revised via two rounds of expert consultation. A total of 11 experts in obstetrics, psychology, nutrition, and related disciplines participated, all with over 10 years of clinical experience and at least an intermediate professional title. The final scale demonstrated good measurement consistency and content representativeness, with a content validity index of 0.93 and an internal consistency reliability coefficient of 0.922. Confirmatory factor analysis demonstrated acceptable model fit (χ2/df = 2.167, CFI = 0.927, RMSEA = 0.051). Convergent validity was satisfactory (AVE > 0.50, CR > 0.70), and discriminant validity met recommended criteria. The scale comprised 37 symptom items. The first 24 items assessed symptom frequency, severity, and distress, while the remaining 13 items, as they were not directly related to frequency, assessed only severity and distress. During assessment, participants were first asked whether a symptom was present. If absent, a score of 0 was recorded. If present, the following dimensions were rated according to the individual’s experience: (1) frequency (four-point scale: 1 = rarely, 2 = occasionally, 3 = frequently, 4 = almost constantly); (2) severity (four-point scale: 1 = slight, 2 = moderate, 3 = severe, 4 = very severe); and (3) distress (five-point scale: 0 = not at all, 1 = a little bit, 2 = somewhat, 3 = quite a bit, 4 = very much). For the first 24 items, the mean score of frequency, severity, and distress was calculated, whereas for the last 13 items, the mean score of severity and distress was calculated. In the present study, the Cronbach’s α coefficient of the scale was 0.912. The English version of the questionnaire is provided as Supplementary Table S1 for references.
Statistical Analysis
Data entry was conducted using EpiData 3.0, with two researchers independently entering the data to establish the database. Statistical analyses were performed using IBM SPSS 27.0 and R 4.3.3. A two-tailed test with P < 0.05 was considered statistically significant. Descriptive methods were chosen according to the distribution of the data: normally distributed continuous variables were presented as mean ± standard deviation (Mean ± SD); non-normally distributed continuous variables were presented as median and interquartile range [Median (IQR)]; categorical variables were presented as frequency and percentage [n (%)].
Symptom Cluster Analysis
Exploratory factor analysis was employed to identify symptom clusters among women in late pregnancy. To ensure robustness and validity, symptoms with a prevalence lower than 40% were excluded,24 leaving 25 symptoms for analysis. Prior to the analysis, data suitability was assessed using the Kaiser–Meyer–Olkin (KMO) test and Bartlett’s test of sphericity. The suitability criteria were defined as KMO > 0.70 and P < 0.05 for Bartlett’s test. Symptom scores were used as variables for analysis. Principal component extraction was used as the extraction method, followed by Promax oblique rotation to facilitate interpretation and allow correlations among the extracted factors. Components with eigenvalues >1 were retained. The rotation converged after six iterations, and symptoms with rotated factor loadings >0.40 were grouped into the same symptom cluster.25 In total, six symptom clusters comprising 21 symptoms were identified.
Symptom Network Construction and Centrality Estimation
Based on the 21 identified symptoms, a Gaussian Graphical Model was used to construct the symptom network. The qgraph package was applied to the Spearman rank correlation matrix,26 combined with the Least Absolute Shrinkage and Selection Operator and the Extended Bayesian Information Criterion (tuning parameter γ = 0.5) to estimate the network and select edges, thereby achieving sparsity and model optimisation.27,28 The network was visualised using the Fruchterman–Reingold force-directed algorithm.29
To control for confounding, multivariable linear regression was first used to screen variables significantly associated with overall symptom burden (mean score of all 21 symptoms, P < 0.05). These variables were then included as covariates in a Mixed Graphical Model to construct the adjusted network. Each node’s predictability (R2) was also calculated to assess its level of influence within the network.
The qgraph package was used to estimate four types of centrality indices: strength, betweenness, closeness, and expected influence (EI), in order to identify symptom nodes with key roles in the network.30 All centrality indices were standardised, and the reported values represented the relative importance of each node compared with the average level of network connectivity; positive or negative values indicated above- or below-average importance, respectively. Given that betweenness and closeness often show low stability in small- to medium-sized samples,31 core symptoms in this study were mainly identified according to strength and expected influence, in order to enhance interpretability and reliability under the constraint of a limited sample size.
The analytical framework was selected to account for the inherent correlation structure of symptom data. Symptom co-occurrence in late pregnancy is expected and clinically meaningful, as symptoms may interact with or reinforce one another. Therefore, a regularized Gaussian graphical model estimated by EBICglasso was applied to estimate conditional dependencies among symptoms rather than simple pairwise correlations. By using partial correlations together with LASSO shrinkage, this approach reduces weak or potentially spurious associations and helps limit redundancy among highly correlated symptoms, thereby producing a more parsimonious and interpretable network structure.
Network Stability and Accuracy
The bootnet package was used to evaluate the stability and accuracy of the network model via bootstrapping, including the precision of edge-weight estimation and the robustness of centrality indices.32 Edge-weight accuracy: Non-parametric bootstrapping (nBoots = 1000) was applied, and 95% confidence intervals (CIs) were calculated for each edge. Narrower CIs indicated more stable and reliable edge-weight estimates. Centrality stability: Case-dropping bootstrapping (randomly removing 10% of cases per iteration, nBoots = 1000) was used to calculate the correlation stability coefficient (CS-coefficient). A CS ≥ 0.25 was considered acceptable, and CS ≥ 0.5 indicated good stability.
Computer Simulation Intervention Analysis
Finally, to further identify candidate symptoms with potential relevance for future symptom-management research, this study employed the nodeIdentifyR package to conduct computer-simulated intervention analyses.20 Given that the Ising model is designed for binary data, symptom scores were dichotomised into binary indicators, with 0 indicating absence of the symptom and 1 indicating presence of the symptom. Based on the edge-weight parameter matrix and node threshold parameters estimated using the IsingFit algorithm, simulated samples conforming to the original network structure were generated using the simulateResponses function. Under the assumption of an unchanged network structure, the NodeIdentifyR algorithm (NIRA) simulates hypothetical intervention scenarios by perturbing the threshold parameter of a single symptom node.These simulations represent model-based hypothetical scenarios rather than real-world interventions. Two types of scenarios were simulated: alleviation and aggravation, with the perturbation magnitude uniformly set at two standard deviations. Differences in overall symptom burden, defined as the sum of activated symptom states across nodes, between baseline and simulated conditions were compared using independent-samples t tests, with False Discovery Rate (FDR) correction applied for multiple comparisons.
Results
Participant Characteristics
A total of 444 women in late pregnancy were included. The mean age was 30.9 ± 3.86 years. Most participants were in 32~36 weeks of gestation and more than half had attained a bachelor’s degree or above. The majority were primiparous and conceived naturally. Detailed demographic and clinical characteristics are presented in Table 1.
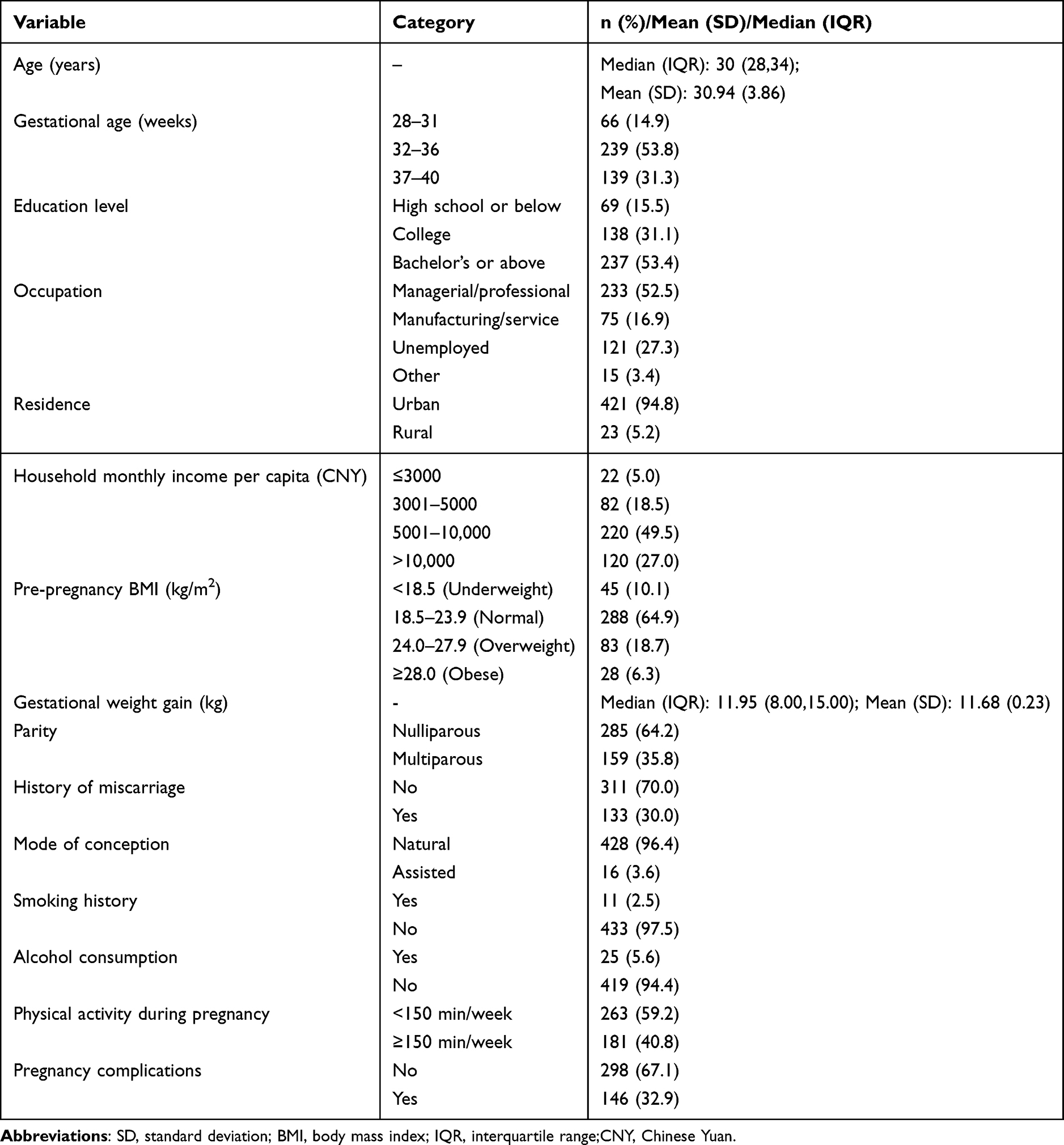 |
Table 1 Characteristics of the Participants (n = 444) |
Symptom Occurrence in Late Pregnancy
The results of this study showed that among 444 women in late pregnancy, the mean number of reported symptoms was 18.47 ± 7.66. The five most prevalent symptoms were Urinary frequency (90.7%), Body aches (pubic / lower back / hip, etc). (84.2%), Abdominal tightness (82.4%), False labour contractions (80.4%), and Fatigue (79.2%). Urinary frequency and body aches were consistently among the most prominent symptoms across prevalence, frequency, severity, and distress dimensions. False labour contractions, fatigue, and frequent waking at night also showed consistently high rankings across multiple symptom dimensions, indicating a stable symptom pattern. To ensure robustness and clinical representativeness, a total of 25 symptoms with an incidence above 40% were included in subsequent analyses. Detailed symptom occurrence is shown in Table 2.
 |
Table 2 Prevalence of Symptom Burden Among Women in Late Pregnancy (n = 444) |
Identification of Symptom Clusters and Influencing Factors
In the first exploratory factor analysis (EFA) of the 25 symptoms with incidence >40%, four items (excessive sweating, leg cramps, impaired memory, and somnolence) showed factor loadings <0.40 and were excluded. A second EFA was then performed on the remaining 21 symptoms. The model showed good sampling adequacy (KMO = 0.882; Bartlett’s test P < 0.001). Six factors with eigenvalues >1.0 were extracted, explaining 62.84% of the total variance. The six symptom clusters were categorized as sleep and physical discomfort symptom cluster, cardiopulmonary load-related symptom cluster, emotional symptom cluster, gastrointestinal symptom cluster, uterine activity-related symptom cluster and limb and skin symptom cluster. Cronbach’s α coefficients indicated acceptable internal consistency for all six clusters. Factor loadings and the final grouping are presented in Table 3.
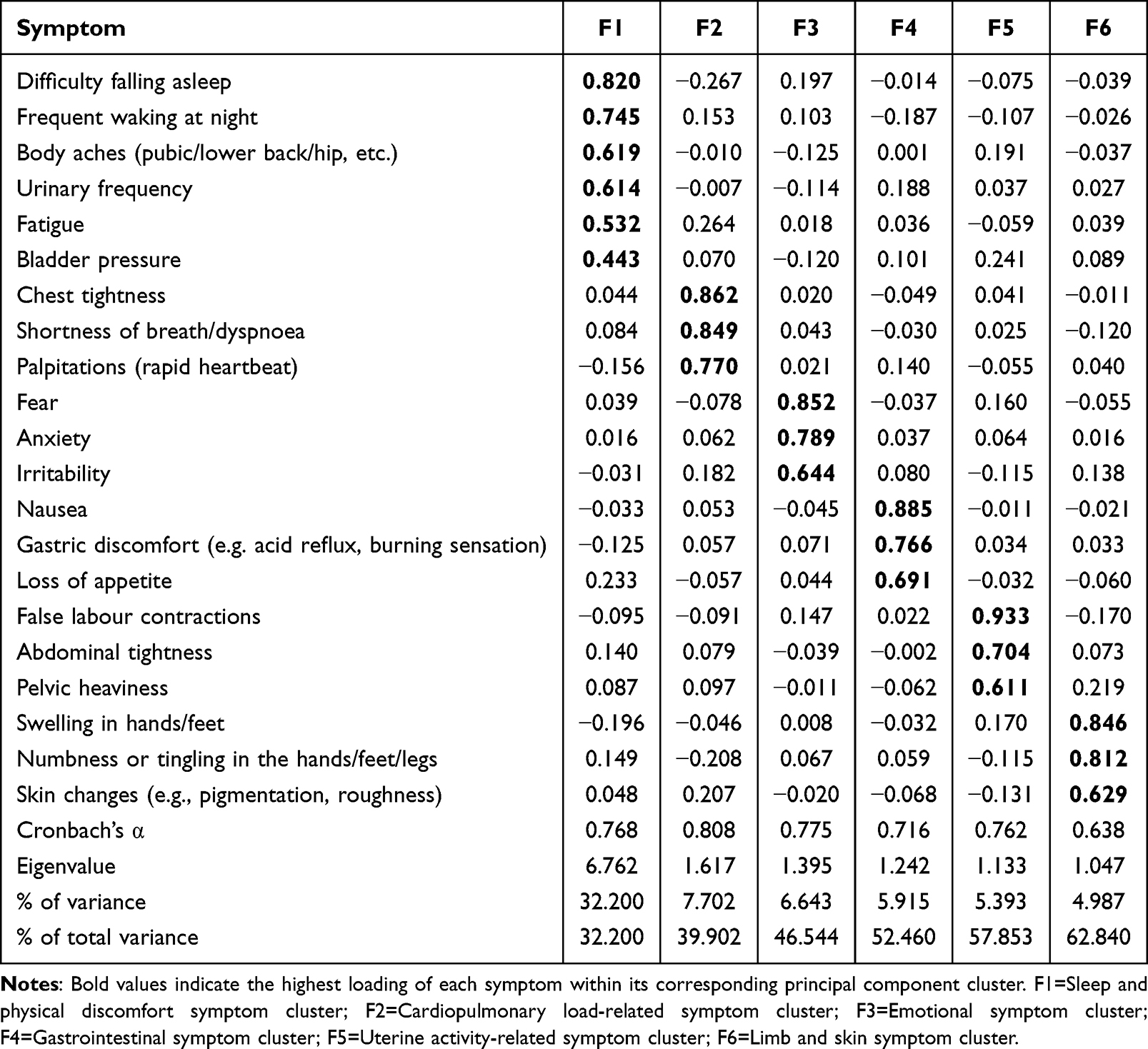 |
Table 3 Factor Loadings and Symptom Clusters Identified Through Principal Component Analysis |
Based on these findings, a multivariable linear regression analysis was performed using the mean total score of the 21 symptoms as the dependent variable. The results showed that age (P = 0.043), gestational age (P = 0.043), physical activity during pregnancy (P = 0.022), and pregnancy complications (P = 0.042) were significantly associated with overall symptom burden (Table 4).
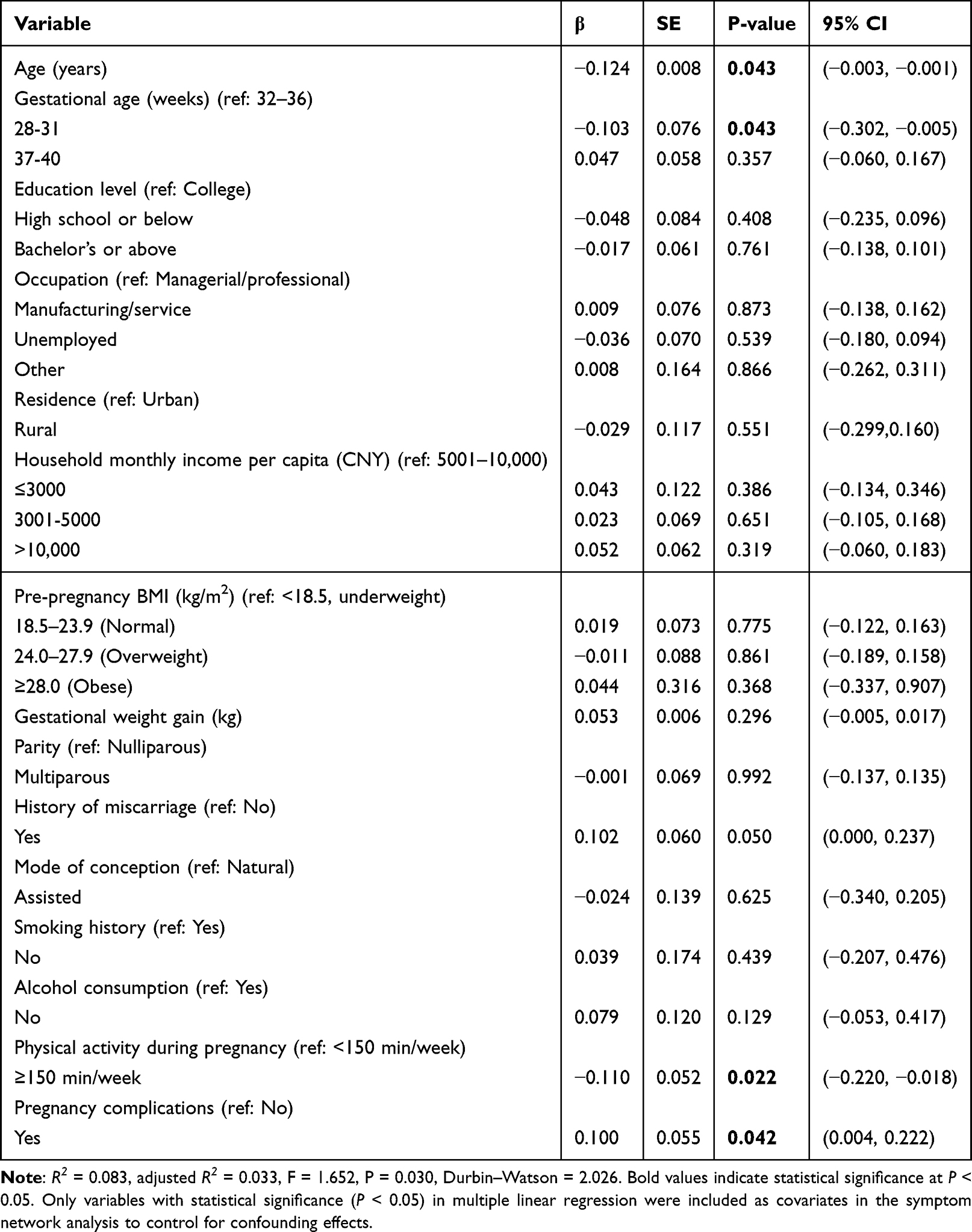 |
Table 4 Linear Regression Analysis of Symptom Burden Among Women in Late Pregnancy (n = 444) |
Network Estimation and Centrality Indices of Symptoms in Late Pregnancy
Based on confounders identified through multivariable linear regression, we constructed symptom networks of 21 symptoms in late pregnancy (with and without covariates). The networks and standardised centrality indices are presented in Figure 1. In the network without covariates (Figure 1A), there were 115 non-zero edges, accounting for 54.76% of the 210 possible edges. In the network with covariates (Figure 1B), there were also 115 non-zero edges, representing 38.33% of the 300 possible edges. In both the unadjusted and covariate-adjusted networks, the strongest connections were consistently observed between shortness of breath/dyspnoea and chest tightness, followed by anxiety and fear, and nausea and loss of appetite. Similar patterns were observed after adjustment, with no substantial changes in the ranking of the strongest edges (see Supplementary Tables S2 and S3). Covariates showed generally low connectivity with individual symptoms (most edge weights ≤ 0.1).
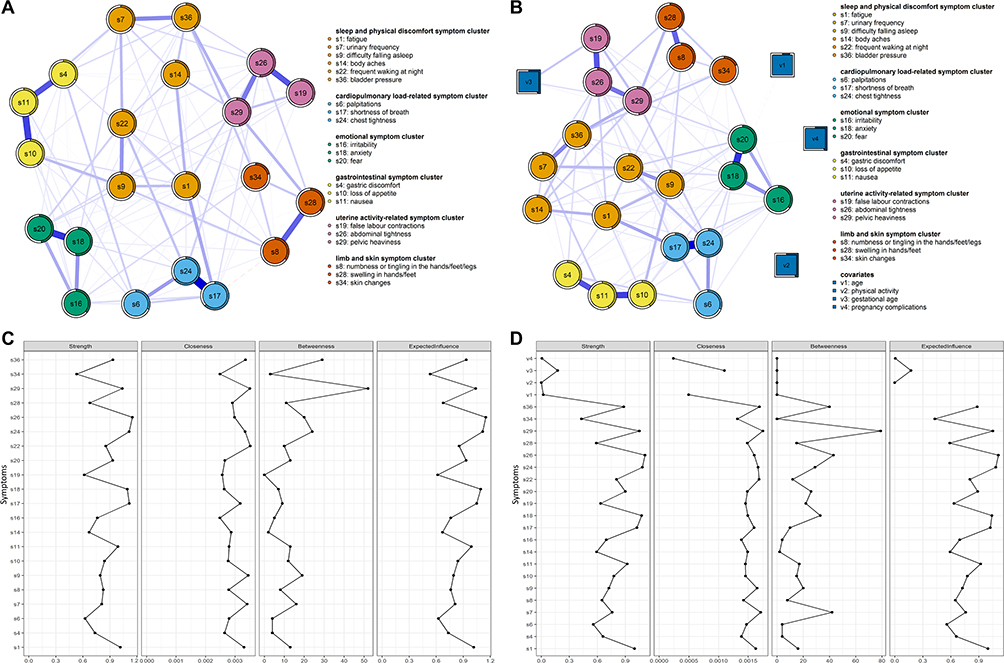 |
Figure 1 Symptoms networks and centrality indices of the total sample with or without covariates.(A) Symptom network and predictability of the total sample without covariates. (B) Symptom network and predictability of the total sample with covariates. (C) Centrality indices of the network without covariates. (D) Centrality indices of the network with covariates. |
Centrality analysis (Figure 1C and D) showed that abdominal tightness, shortness of breath/dyspnoea, chest tightness, anxiety, and pelvic heaviness were located at the core of both networks. In the covariate-adjusted network, strength and expected influence indicated that fatigue (Strength = 0.93, EI = 0.93) was the core symptom in the sleep and physical discomfort symptom cluster; chest tightness (Strength = 1.18, EI = 1.18) was the core symptom in the cardiopulmonary load-related symptom cluster; anxiety (Strength = 1.15, EI = 1.06) was the core symptom in the emotional symptom cluster; nausea (Strength = 0.70, EI = 0.70) was the core symptom in the gastrointestinal symptom cluster; abdominal tightness (Strength = 1.26, EI = 1.26) was the core symptom in the uterine activity-related symptom cluster; and numbness or tingling in the hands/feet/legs (Strength = –0.11, EI = –0.09) was the core symptom in the limb and skin symptom cluster. It is noteworthy that although numbness or tingling in the hands/feet/legs had negative values in this cluster, its centrality remained the highest among symptoms in the same cluster. Detailed centrality values for both networks are shown in Supplementary Table S4 and S5.
Accuracy and Stability of Edges and Nodes
Bootstrap confidence intervals were relatively narrow (Figure 2A and B), suggesting that edge weights and centrality estimates in both the unadjusted and adjusted networks were accurate. Subset bootstrap analysis further showed that, in the network without covariates, the correlation stability coefficients for expected influence and strength were both 0.595 (Figure 2C). After adjusting for covariates, both coefficients were 0.516 (Figure 2D). These findings indicate that the two networks demonstrated good stability, meaning that the identification of core symptoms was minimally affected by sampling variability.
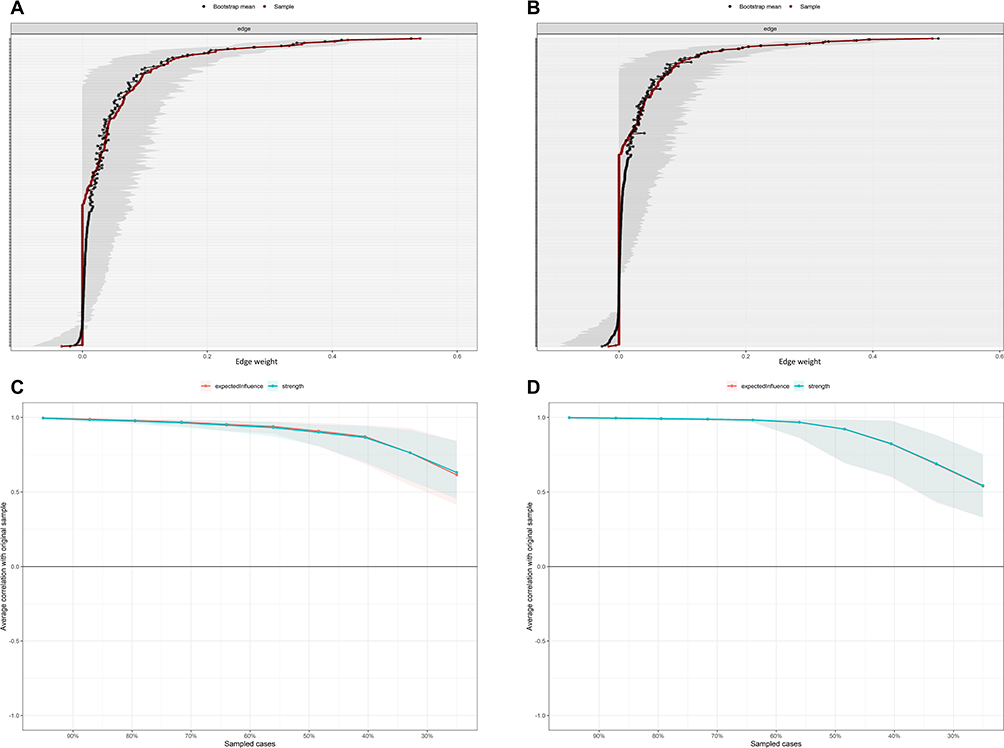 |
Figure 2 Accuracy and stability of network structure model with or without covariates.(A) Bootstrap analysis results of the edge weights without covariates. (B) Bootstrap analysis results of the edge weights with covariates. (C) Correlation stability coefficient for strength, expected influence without covariates. (D) Correlation stability coefficient for strength, expected influence with covariates. |
Computer-Simulated Intervention
The predicted effects of the computer-simulated network intervention are presented in the Figure 3. We compared changes in the total symptom burden score under symptom aggravation and symptom alleviation conditions. Under the alleviation condition, intervention targeting each individual symptom node was associated with a reduction in the total symptom burden score (Figure 3A and C). The most pronounced reduction was observed for Shortness of breath/dyspnoea (s17), followed by Fatigue (s1) and Chest tightness (s24). The simulation further indicated that the total symptom burden score decreased to 9.65, 9.78 and 9.99, corresponding to an approximate reduction of 11.5%~14.5%.
 |
Figure 3 The effect of computer simulated interventions to the symptoms of late pregnancy. (A) Projected Effects of alleviating intervention depicted by sum score of target symptoms. (B) Projected Effects of aggravating intervention depicted by sum score of target symptoms. (C) Relative percentage decrease in total symptom burden score under alleviating conditions. (D) Relative percentage increase in total symptom burden score under aggravating conditions. |
Under the aggravation condition (Figure 3B–D), the intervention effects for Urinary frequency (s7) and Body aches (pubic/lower back/hip, etc). (s14) did not remain statistically significant after adjustment (P > 0.05), suggesting that exacerbation of these two symptoms alone was insufficient to produce a significant increase in the overall symptom burden. By contrast, aggravation of the remaining 19 symptom nodes was associated with a significant increase in the overall symptom burden score. The greatest effect was observed for Loss of appetite (s10), followed by Nausea (s11) and Anxiety (s18). Theoretically, prevention of these three symptoms would reduce the overall symptom burden by 15.4%, 13.1% and 12.7%, respectively. These findings indicate that proactive prevention of these symptoms may help to avert further escalation of overall symptom burden.
Discussion
Symptom Clusters in Late Pregnancy
This study identified six symptom clusters among women in late pregnancy. Compared with previous research, differences were observed in both the number and composition of clusters.14,33 For example, the physical image disturbance cluster previously encompassing numbness or tingling in the hands and feet, sensations of bodily or limb swelling, and “not looking like oneself” was restructured in the present study. The first three symptoms were categorised within the limb and skin symptom cluster, whereas “not looking like oneself” did not cluster with these physical manifestations.
The sleep and physical discomfort cluster identified in this study—including urinary frequency, bodily aches, fatigue, frequent nocturnal awakening, difficulty initiating sleep, and bladder pressure—largely overlaps with sleep-related and activity-related clusters reported in previous studies. A distinct uterine activity–related cluster was also identified, which may reflect physiological changes associated with late pregnancy. Alternatively, this pattern may be explained by shared characteristics of uterine-related symptoms or their tendency to co-occur during late gestation. These discrepancies may be related to variations in measurement tools and cluster extraction methods.17 The questionnaire used in this study was specifically developed for late-pregnancy symptoms, which may improve sensitivity to gestation-specific symptom patterns. Overall, the identified clusters provide a structured understanding of symptom co-occurrence, which may serve as a preliminary foundation for hypothesis generation in future research on symptom assessment and management.
In addition to the identified cluster patterns, several demographic and obstetric factors were associated with overall symptom burden. These variables were adjusted for in the network analyses to minimise potential confounding effects. Younger age, gestational age of 32~36 weeks (vs. 28~31 weeks), insufficient physical activity (<150 minutes per week), and concurrent pregnancy complications were associated with higher symptom burden. These findings are consistent with prior research suggesting that increasing physiological load and complication-related stress may exacerbate symptom experiences during late pregnancy.14,34 Regular physical activity has been suggested to be associated with better cardiopulmonary function and psychological well-being. Older women tended to report lower symptom burden, which may be related to differences in coping or health management behaviors.35–38 Younger women may also be more sensitive to pregnancy-related changes or more likely to report mild symptoms.39
Core Symptoms Within Symptom Clusters
Fatigue as the Core Symptom of the Sleep and Physical Discomfort Symptom Cluster
Fatigue emerged as the central symptom within the sleep and physical discomfort cluster after adjustment for covariates. This cluster included urinary frequency, bodily aches, fatigue, frequent nocturnal awakening, difficulty initiating sleep, and bladder pressure, all of which showed high prevalence in late pregnancy, consistent with previous studies.7 The co-occurrence of fatigue with sleep disruption and physical discomfort may reflect the interrelated nature of these symptoms during late pregnancy. The enlarging uterus in late pregnancy elevates the diaphragm and compresses the bladder and pelvic floor, frequently causing bladder pressure and urinary frequency.40 Sleep cycles are frequently disturbed by frequent nocturnal urination, which further fragments sleep architecture, continually depletes energy stores, and exacerbates fatigue.5 Concurrently, increased relaxin secretion and postural changes may result in joint ligament laxity and muscle strain,41 which causes lumbar, dorsal, and pubic regionsand and worsens the quality of sleep. Moreover, fatigue itself can lead to reduced activity, inadequate muscle blood flow, and metabolic dysfunction, potentially exacerbating aches and pains indirectly, creating a vicious cycle. Clinically, severe fatigue not only diminishes the quality of life for pregnant women but is also associated with an increased risk of labour pain.42 From a clinical perspective, fatigue may represent an important symptom to consider in symptom management strategies for women in late pregnancy. Interventions aimed at improving sleep quality and promoting appropriate physical activity may be beneficial in alleviating overall symptom burden.43,44
Chest Tightness as the Core Symptom of the Cardiopulmonary Load-Related Symptom Cluster
Chest tightness was identified as a central symptom within the cardiopulmonary load-related cluster. This finding may be associated with physiological changes during late pregnancy. The enlarging uterus may elevate the diaphragm and reduce thoracic compliance, which could contribute to increased respiratory workload. In addition, increased blood volume and cardiac output may be associated with sensations of dyspnoea and chest discomfort. Progesterone-related changes in respiratory regulation may also influence subjective breathing perception in some women.45 Consequently, chest tightness could be considered as a symptom that may warrant closer clinical attention in late pregnancy. Following exclusion of complications such as gestational hypertension, anaemia, or cardiopulmonary disease, comprehensive non-pharmacological interventions should be the primary strategy. Guiding women in late pregnancy to adopt a left-lateral recumbent position improves ventilation and venous return.46 Weekly moderate-intensity activity (such as prenatal yoga) may enhance cardiopulmonary reserve and alleviate subjective dyspnoea. Thus, chest tightness may warrant priority attention in future symptom-management research and clinical assessment within the cardiopulmonary load-related symptom cluster, although its clinical applicability requires further validation in future interventional studies.
Anxiety as the Core Symptom of the Emotional Symptom Cluster
Anxiety was identified as the most central symptom within the emotional symptom cluster, with strong connections to fear and irritability. This suggests that anxiety may play a central role in the network structure of emotional symptoms during late pregnancy. Psychological concerns regarding childbirth, foetal health, and role transitions may act as persistent stressors during pregnancy. These factors have been associated with activation of the hypothalamic-pituitary-adrenal axis and alterations in stress-related neuroendocrine regulation. Collectively, these factors contribute to emotional dysregulation symptoms such as anxiety.45 Moreover, fluctuating oestrogen and progesterone levels may be associated with changes in HPA axis sensitivity and monoamine function, which could partly explain the development of anxiety in late pregnancy.47
Previous studies indicate anxiety is the most prevalent emotional symptom during pregnancy, associated with reduced quality of life and adverse maternal-infant outcomes.48 The current network analysis further highlights its central position within the symptom structure, suggesting its potential relevance in understanding emotional symptom co-occurrence. Psychological interventions such as cognitive behavioural therapy and mindfulness-based approaches have been shown to be beneficial in improving emotional regulation in pregnant women.49 Consequently, these findings may inform the development of personalised emotional support strategies for pregnant women, taking into account factors such as anxiety severity, psychological characteristics, and social support, thereby providing more precise and efficient psychological support.
Nausea as the Core Symptom of the Gastrointestinal Symptom Cluster
According to this study, nausea exhibits the highest centrality among gastrointestinal symptom clusters, indicating its status as a core node within this symptom group. This may be related to multiple physiological changes during pregnancy. Elevated progesterone levels have been associated with reduced lower oesophageal sphincter pressure, which may contribute to gastro-oesophageal reflux, while human chorionic gonadotropin and oestradiol have been associated with the occurrence of nausea in pregnancy.50 In addition, genetic and placental factors have been proposed to influence susceptibility to nausea and vomiting during pregnancy.51 Moreover, intense nausea often coexists with reduced appetite in late pregnancy,52 which could create a vicious cycle that worsens overall symptom burden. Consequently, nausea may warrant closer attention in the management of gastrointestinal symptoms during late pregnancy. In clinical practice, comprehensive management—including dietary adjustments, postural interventions, and necessary pharmacological treatments—may be a reasonable strategy for alleviating the burden of this symptom cluster.50
Abdominal Tightness as the Core Symptom of the Uterine Activity-Related Symptom Cluster
The most closely associated core node in the cluster of symptoms connected to uterine activity is abdominal tightness, which is strongly associated with pelvic heaviness and false labor contraction sensations. This arrangement may reflect how pregnant women’s symptom experiences are distinct. In late pregnancy, the enlarging uterus and irregular contractions of the uterine smooth muscle may lead to a tightening sensation perceived by pregnant women, as described in previous physiological studies.53 Concurrently, as the presenting section descends, mechanical pressure exerted by the fetal head on the bladder and anterior pelvic tissues may induce discomfort such as suprapubic/pelvic pressure or a sensation of heaviness.40 This abdominal tightness could be viewed as a potential manifestation of these two physiological processes acting in concert. Based on these findings, abdominal tightness could be considered a candidate for identifying and evaluating uterine activity-related symptom clusters in future research. From a clinical perspective, abdominal tightness may be considered in routine symptom inquiry regarding uterine activity–related discomfort. Simple non-pharmacological approaches such as positional adjustment and rest may help alleviate discomfort.
Numbness or Tingling in the Hands/Feet/Legs as the Core Symptom of the Limb and Skin Symptom Cluster
Network analysis in this study identified numbness or tingling in the hands/feet/legs as the highest centrality core symptom within the limb and skin symptom cluster. Although its intensity centrality and expected influence values were both negative, it ranked highest within this cluster, suggesting a relatively more connected position in the network structure. Previous studies have reported that such symptoms are common in late pregnancy and may be associated with physiological changes such as fluid retention and peripheral oedema. Increased interstitial pressure in the carpal tunnel may be associated with compression of peripheral nerves, contributing to sensory symptoms such as numbness and tingling.54 Additionally, fluctuating hormonal levels during pregnancy can cause changes in distal skin pigmentation, dryness, and roughness.55 Although these symptoms typically do not directly threaten maternal or fetal safety, the associated discomfort may reduce nocturnal sleep quality and restrict daily activities.56 Therefore, our findings suggest that numbness and tingling may deserve attention in clinical assessment, for example by screening for carpal tunnel syndrome or evaluating oedema severity. Approaches addressing numbness and tingling (eg., wrist splinting, postural adjustments) may help alleviate discomfort, although potential effects on sleep and daily functioning require further evaluation.
Simulation Intervention of Symptoms in Women in Late Pregnancy
In addition to identifying symptom clusters and central symptoms through network analysis, we conducted a simulated intervention analysis (aggravation and alleviation simulations) to generate exploratory hypotheses regarding potential symptom targets. In the aggravation simulations, loss of appetite, nausea, and anxiety emerged as the most influential nodes, suggesting that—under simulated conditions—preventing deterioration of these symptoms might reduce overall symptom burden. From a pathophysiological perspective, loss of appetite and nausea may compromise dietary intake, potentially weakening energy reserves and physiological tolerance. Previous research has shown that nausea and vomiting during pregnancy can interfere with adequate nutrition, particularly when symptoms persist or worsen.51 Anxiety, in contrast, may be associated with altered stress-related neuroendocrine regulation, particularly hypothalamic–pituitary–adrenal axis activity, thereby heightening sensitivity to bodily symptoms.57 They may help to further understand patterns of symptom co-occurrence and symptom dynamics during late pregnancy. From a clinical perspective, these findings may help inform understanding of nutritional and emotional experiences during late pregnancy. Supportive approaches such as dietary counselling and psychological support, including mindfulness-based interventions or midwifery-led care, have been reported in previous studies.58,59
Further, the alleviation simulations identified shortness of breath/dyspnoea, fatigue, and chest tightness as the most effective targets for reducing overall symptom burden in the model. These symptoms may be associated with increased cardiopulmonary load and physical demands in the third trimester. Based on these simulation results, non-pharmacological interventions targeting shortness of breath/dyspnoea and chest tightness (eg., postural adjustment and breathing exercises) could be considered as candidates for future interventional studies.60 Moderate antenatal exercise might be explored as a potential strategy for fatigue,61 and adjunctive aromatherapy during the third trimester could be examined for possible additional benefit.62 The simulation model suggests that targeting these key nodes might disrupt cascading symptom interactions, which could in turn contribute to a greater overall reduction in symptom burden, although this remains to be tested.
Overall, the simulation findings were broadly consistent with the core symptoms identified in the static network analysis, providing exploratory and complementary support for identifying candidate symptoms that may warrant further investigation.
Compared with previous studies that mainly described symptom clusters or static symptom associations, the present study adds an exploratory simulation-based perspective within a network framework. By focusing on women in late pregnancy and using a relatively comprehensive symptom set, this study may help extend current understanding of symptom co-occurrence and potential symptom-management priorities in this population. When considering the application of these findings in antenatal care, however, symptom priorities should be interpreted in relation to individual characteristics and care contexts. Symptom burden and symptom interrelationships may vary according to obstetric condition, health literacy, access to antenatal services, and previous pregnancy or childbirth experience. Therefore, these findings may serve as exploratory guidance for symptom assessment rather than as a fixed set of priorities applicable to all pregnant women.
These findings may have implications for clinical assessment and multidisciplinary symptom management in late pregnancy. Nurses may use these findings to inform symptom assessment and identify symptoms that warrant closer attention, while obstetricians may benefit from understanding symptom interrelationships during comprehensive clinical evaluation. In addition, psychological professionals may contribute to the assessment and support of emotionally interconnected symptoms. Collaborative approaches across disciplines may therefore help support more comprehensive and individualized symptom management for women in late pregnancy.
Limitations
Several limitations should be acknowledged. First, because this study used a cross-sectional design, the observed associations and simulation-based findings cannot support causal inference. Second, although key demographic and obstetric variables were adjusted for in the network analyses, residual confounding from unmeasured factors cannot be completely excluded. Third, dichotomisation of symptom variables for the Ising-based simulation analysis may have led to loss of information and reduced statistical power. Fourth, because symptom data were collected using self-reported questionnaires, self-report bias may have occurred despite the use of standardized instructions, anonymous participation, and clarification by trained researchers without guiding responses. Fifth, participants were recruited by convenience sampling from two hospitals in a single province, which may have introduced selection bias and limited the generalisability of the findings. Fifth, the estimated network reflects statistical associations rather than causal mechanisms. Centrality indices should be interpreted cautiously, as they indicate relative connectivity within the sample-specific network and may be influenced by sample characteristics, measurement choices, and model specification. Future multicentre, longitudinal, and interventional studies involving diverse regions, care settings, and population groups are warranted to evaluate the stability, generalisability, and clinical relevance of these findings.
Conclusion
This study employed network analysis combined with computational simulation-based intervention techniques to preliminarily explore the complex network structure of symptoms among women in late pregnancy. Through network analysis, key nodes with relatively high centrality within each symptom cluster were identified. Furthermore, computer simulation intervention analyses suggested potential intervention and preventive targets.These findings may help identify priority symptoms for antenatal symptom assessment and provide a reference for the development and future evaluation of network-informed symptom-management strategies in antenatal care. By highlighting core symptoms and candidate targets within interconnected symptom networks, this study may inform more targeted and individualized approaches aimed at reducing symptom burden and improving maternal well-being among women in late pregnancy.
Data Sharing Statement
The data that support the findings of this study are available from Professor Yuhong Li upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki of the World Medical Association. Ethical approval was obtained from the Research Ethics Committee of Anhui Medical University (Approval Number: 82240215). Informed consent was obtained from all participants prior to their participation in the study. All data were collected anonymously, and strict confidentiality was maintained throughout the study.
Acknowledgments
We would like to thank all the women who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Anhui Provincial Department of Education [2024 Provincial Quality Engineering Project for Graduate Education] (2024lhpysfjd022); School of Nursing, Anhui Medical University [2025 Graduate Young Talent Cultivation Project] (Hlqm12025038).
Disclosure
The authors confirm that they do not have any conflicts of interest in the present article.
References
1. Tan EK, Tan EL. Alterations in physiology and anatomy during pregnancy. Best Pract Res Clin Obstet Gynaecol. 2013;27(6):791–18. doi:10.1016/j.bpobgyn.2013.08.001
2. Răchită A, Strete GE, Suciu LM, Ghiga DV, Sălcudean A, Mărginean C. Psychological stress perceived by pregnant women in the last trimester of pregnancy. Int J Environ Res Public Health. 2022;19(14):8315. doi:10.3390/ijerph19148315
3. Mislu E, Kumsa H, Tadesse S, et al. Sleep quality disparities in different pregnancy trimesters in low- and middle-income countries: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2024;24(1):627. doi:10.1186/s12884-024-06830-3
4. Ertmann RK, Nicolaisdottir DR, Siersma V, et al. Factors in early pregnancy predicting pregnancy-related pain in the second and third trimester. Acta Obstet Gynecol Scand. 2023;102(10):1269–1280. doi:10.1111/aogs.14670
5. Fan Z, Yan S, Sun L, et al. Longitudinal association between sleep quality and fatigue during pregnancy: an observational cohort study. BMC Psychiatry. 2025;25(1):159. doi:10.1186/s12888-025-06513-z
6. Răchită AI, Strete GE, Sălcudean A, et al. Prevalence and risk factors of depression and anxiety among women in the last trimester of pregnancy: a cross-sectional study. Medicina. 2023;59(6):1009. doi:10.3390/medicina59061009
7. Beebe KR, Gay CL, Richoux SE, Lee KA. Symptom experience in late pregnancy. J Obstet Gynecol Neonatal Nurs. 2017;46(4):508–520. doi:10.1016/j.jogn.2017.03.007
8. Tang WZ, Huang KJ, Wang X, et al. Obstructive sleep apnea-associated hypertensive disorders in pregnancy: a literature review and clinical management strategies. Reprod Biol Endocrinol. 2025;23(1):107. doi:10.1186/s12958-025-01431-x
9. Kanellopoulos D, Gourounti K. Tocophobia and women’s desire for a caesarean section: a systematic review. Maedica. 2022;17(1):186–193. doi:10.26574/maedica.2022.17.1.186
10. Li R, Zhang J, Gao Y, et al. Duration and quality of sleep during pregnancy are associated with preterm birth and small for gestational age: a prospective study. Int J Gynaecol Obstet. 2021;155(3):505–511. doi:10.1002/ijgo.13584
11. Chien L-Y, Ko Y-L. Fatigue during pregnancy predicts caesarean deliveries. J Adv Nurs. 2004;45(5):487–494. doi:10.1046/j.1365-2648.2003.02931.x
12. Wang X, Xie J, Wu Y, et al. Gender-specific effect of pregnancy-related anxiety on preschooler’s emotional and behavioral development: a population-based cohort study. J Affect Disord. 2021;279:368–376. doi:10.1016/j.jad.2020.10.014
13. Kim H-J, McGuire DB, Tulman L, Barsevick AM. symptom clusters: concept analysis and clinical implications for cancer nursing. Cancer Nurs. 2005;28(4):270–282. doi:10.1097/00002820-200507000-00005
14. Su A, Jie Z, Jiaming X, Lingling G. Symptom clusters and influencing factors in late pregnancy women (in Chinese). J Nurs. 2021;36(7):26–30.
15. Miller ML, O’Hara MW. The structure of mood and anxiety disorder symptoms in the perinatal period. J Affect Disord. 2023;325:231–239. doi:10.1016/j.jad.2022.12.111
16. Pin M, Guangyi Z, Haixia L, Yan Z, Hui Y, Guangli M. Symptom cluster identification and influencing factors in elderly primiparous women during late pregnancy (in Chinese). Chin J Nurs Educ. 2024;21(2):237–244.
17. Zhu Z, Xing W, Hu Y, Wu B, WKW S. Paradigm shift: moving from symptom clusters to symptom networks. Asia Pac J Oncol Nurs. 2022;9(1):5–6. doi:10.1016/j.apjon.2021.12.001
18. Liang M, Zhu S, Zhang W, Knobf MT, Ye Z. Symptom network approach for management in cancer care. Asia Pac J Oncol Nurs. 2024;11(5):100482. doi:10.1016/j.apjon.2024.100482
19. Johnson SR, Sivertsen E. We have all the time in the world: the law and ethics of time-limited interventions in clinical care. J Law Med Ethics. 2024;52(2):309–320. doi:10.1017/jme.2024.99
20. Lunansky G, Naberman J, van Borkulo CD, Chen C, Wang L, Borsboom D. Intervening on psychopathology networks: evaluating intervention targets through simulations. Methods. 2022;204:29–37. doi:10.1016/j.ymeth.2021.11.006
21. Blanken TF, Deserno MK, Dalege J, et al. The role of stabilizing and communicating symptoms given overlapping communities in psychopathology networks. Sci Rep. 2018;8(1):5854. doi:10.1038/s41598-018-24224-2
22. Barth J, Munder T, Gerger H, et al. Comparative efficacy of seven psychotherapeutic interventions for patients with depression: a network meta-analysis. PLoS Med. 2013;10(5):e1001454. doi:10.1371/journal.pmed.1001454
23. Portenoy RK, Thaler HT, Kornblith AB, et al. The Memorial Symptom Assessment Scale: an instrument for the evaluation of symptom prevalence, characteristics and distress. Eur J Cancer. 1994;30(9):1326–1336. doi:10.1016/0959-8049(94)90182-1
24. Zhou K, Huang X, Chen M, et al. Pre-hospital symptom clusters and symptom network analysis in decompensated cirrhotic patients: a cross-sectional study. J Adv Nurs. 2024;80(7):2785–2800. doi:10.1111/jan.16044
25. Kim HJ. Common factor analysis versus principal component analysis: choice for symptom cluster research. Asian Nurs Res. 2008;2(1):17–24. doi:10.1016/S1976-1317(08)60025-0
26. Epskamp S, Cramer AOJ, Waldorp LJ, Schmittmann VD, Borsboom D. qgraph: network visualizations of relationships in psychometric data. J Stat Softw. 2012;48(4):1–18. doi:10.18637/jss.v048.i04
27. Tibshirani R. Regression Shrinkage and Selection Via the Lasso. J R Stat Soc Ser B Stat Methodol. 1996;58(1):267–288. doi:10.1111/j.2517-6161.1996.tb02080.x
28. Chen J, Chen Z. Extended Bayesian information criteria for model selection with large model spaces. Biometrika. 2008;95(3):759–771. doi:10.1093/biomet/asn034
29. Epskamp S, Fried EI. A tutorial on regularized partial correlation networks. Psychol Methods. 2018;23(4):617–634. doi:10.1037/met0000167
30. Hevey D. Network analysis: a brief overview and tutorial. Health Psychol Behav Med. 2018;6(1):301–328. doi:10.1080/21642850.2018.1521283
31. Castro D, Ferreira F, de Castro I, et al. The differential role of central and bridge symptoms in deactivating psychopathological networks. Front Psychol. 2019;10:2448. doi:10.3389/fpsyg.2019.02448
32. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
33. Zhang Y, Xu X, Xie Z, et al. Identifying symptom clusters among pregnant women during early and late pregnancy. Int J Gynaecol Obstet. 2023;162(2):656–663. doi:10.1002/ijgo.14712
34. Xiaowei L, Yinan L, Zexianfan J, et al. Prevalence and associated factors of symptom clusters in women during late pregnancy(in Chinese). South China J Prev Med. 2021;47(8):989–993.
35. Klemetti R, Kurinczuk JJ, Redshaw M. Older women’s pregnancy related symptoms, health and use of antenatal services. Eur J Obstet Gynecol Reprod Biol. 2011;154(2):157–162. doi:10.1016/j.ejogrb.2010.10.025
36. Pettersson ML, Nedstrand E, Bladh M, Svanberg AS, Lampic C, Sydsjö G. Mothers who have given birth at an advanced age - health status before and after childbirth. Sci Rep. 2020;10(1):9739. doi:10.1038/s41598-020-66774-4
37. Shakarami A, Mirghafourvand M, Abdolalipour S, Jafarabadi MA, Iravani M. Comparison of fear, anxiety and self-efficacy of childbirth among primiparous and multiparous women. BMC Pregnancy Childbirth. 2021;21(1):642. doi:10.1186/s12884-021-04114-8
38. Ahmad M, Sechi C, Vismara L. Advanced maternal age: a scoping review about the psychological impact on mothers, infants, and their relationship. Behav Sci. 2024;14(3):147. doi:10.3390/bs14030147
39. Locock L, Alexander J, Rozmovits L. Women’s responses to nausea and vomiting in pregnancy. Midwifery. 2008;24(2):143–152. doi:10.1016/j.midw.2006.12.001
40. Cunningham FG, Leveno KJ, Bloom SL, et al. Maternal Physiology. In: Williams Obstetrics, 25e. New York, NY: McGraw-Hill Education; 2018.
41. Sward L, Manning N, Murchison AB, Ghahremani T, McCaulley JA, Magann EF. Pelvic girdle pain in pregnancy: a review. Obstet Gynecol Surv. 2023;78(6):349–357. doi:10.1097/OGX.0000000000001140
42. Zhu X, Xia H. Trajectory patterns and factors influencing perinatal fatigue among Chinese women from late pregnancy to 6 months after delivery. PeerJ. 2022;10:e13387. doi:10.7717/peerj.13387
43. Yu H, Mu Q, Lv X, Chen S, He H. Effects of an exercise intervention on maternal depression, anxiety, and fatigue: a systematic review and meta-analysis. Front Psychol. 2024;15:1473710. doi:10.3389/fpsyg.2024.1473710
44. Wang S, Zhang C, Sun M, et al. Effectiveness of mindfulness training on pregnancy stress and the hypothalamic-pituitary-adrenal axis in women in China: a multicenter randomized controlled trial. Front Psychol. 2023;14:1073494. doi:10.3389/fpsyg.2023.1073494
45. LoMauro A, Aliverti A. Respiratory physiology in pregnancy and assessment of pulmonary function. Best Pract Res Clin Obstet Gynaecol. 2022;85:3–16. doi:10.1016/j.bpobgyn.2022.05.007
46. Kember AJ, Anderson JL, House SC, Reuter DG, Goergen CJ, Hobson SR. Impact of maternal posture on fetal physiology in human pregnancy: a narrative review. Front Physiol. 2024;15:1394707. doi:10.3389/fphys.2024.1394707
47. Sheng JA, Bales NJ, Myers SA, et al. The hypothalamic-pituitary-adrenal axis: development, programming actions of hormones, and maternal-fetal interactions. Front Behav Neurosci. 2020;14:601939. doi:10.3389/fnbeh.2020.601939
48. Aziz HA, Yahya HDB, Ang WW, Lau Y. Global prevalence of depression, anxiety, and stress symptoms in different trimesters of pregnancy: a meta-analysis and meta-regression. J Psychiatr Res. 2025;181:528–546. doi:10.1016/j.jpsychires.2024.11.070
49. Leng LL, Yin XC, Ng SM. Mindfulness-based intervention for clinical and subthreshold perinatal depression and anxiety: a systematic review and meta-analysis of randomized controlled trial. Compr Psychiatry. 2023;122:152375. doi:10.1016/j.comppsych.2023.152375
50. Dunbar K, Yadlapati R, Konda VH. Nausea, and vomiting during pregnancy. Am J Gastroenterol. 2022;117(10S):10–15. doi:10.14309/ajg.0000000000001958
51. Fejzo MS, Trovik J, Grooten IJ, et al. Nausea and vomiting of pregnancy and hyperemesis gravidarum. Nat Rev Dis Primers. 2019;5(1):62. doi:10.1038/s41572-019-0110-3
52. Ding W, Weltzien H, Peters C, Klein R. Nausea-induced suppression of feeding is mediated by central amygdala Dlk1-expressing neurons. Cell Rep. 2024;43(4). doi:10.1016/j.celrep.2024.113990
53. Raines DA, Cooper DB. Braxton Hicks Contractions. In: StatPearls. Treasure Island (FL) Ineligible Companies. Disclosure: Danielle Cooper Declares No Relevant Financial Relationships with Ineligible Companies. StatPearls Publishing.
54. Cîmpeanu M-C, Roman N, Grigorescu S, Grigorescu O-D, Miclăuș RS. Management of “de novo” carpal tunnel syndrome in pregnancy: a narrative review. J Pers Med. 2024;14(3):240. doi:10.3390/jpm14030240
55. Gupta SN, Madke B, Ganjre S, Jawade S, Kondalkar A. Cutaneous changes during pregnancy: a comprehensive review. Cureus. 2024;16(9):e69986. doi:10.7759/cureus.69986
56. Meems M, Truijens SEM, Spek V, Visser LH, Pop VJM. Prevalence, course and determinants of carpal tunnel syndrome symptoms during pregnancy: a prospective study. BJOG. 2015;122(8):1112–1118. doi:10.1111/1471-0528.13360
57. Hantsoo L, Jagodnik KM, Novick AM, et al. The role of the hypothalamic-pituitary-adrenal axis in depression across the female reproductive lifecycle: current knowledge and future directions. Front Endocrinol. 2023;14:1295261. doi:10.3389/fendo.2023.1295261
58. CoP B-O. ACOG Practice Bulletin No. 189: nausea And Vomiting Of Pregnancy. Obstet Gynecol. 2018;131(1):e15–e30.
59. Dhillon A, Sparkes E, Duarte RV. Mindfulness-based interventions during pregnancy: a systematic review and meta-analysis. Mindfulness. 2017;8(6):1421–1437. doi:10.1007/s12671-017-0726-x
60. Gao B, Wang S, Jiang S. The occurrence mechanism, assessment, and non-pharmacological treatment of dyspnea. Med Rev. 2024;4(5):395–412. doi:10.1515/mr-2024-0006
61. Celik S, Nazik E. The effect of aromatherapy applied to pregnant women on sleep quality and fatigue level: a randomized clinical trial. Explore. 2025;21(3):103157. doi:10.1016/j.explore.2025.103157
62. Li L, Can Z, Yingjia C, Hanjiao K, Hong Z. Meta-analysis of the effect of exercise intervention on reducing fatigue in pregnant women(in Chinese). Chin Nurs Manage. 2024;24(4):551–558.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.