")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Coping with Epidemic-Related Job Stressors in Healthcare Workers During the Late Stage of the COVID-19 Pandemic: Effects of Reflective Functioning and Cognitive Emotion Regulation
Authors Zhou T, Wang Q, Wang Y, Cheng L
Received 12 July 2023
Accepted for publication 10 October 2023
Published 26 October 2023 Volume 2023:16 Pages 4377—4388
DOI https://doi.org/10.2147/PRBM.S429109
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ting Zhou,1 Qian Wang,2 Youyang Wang,2 Lizhi Cheng2
1Department of Medical Psychology, School of Health Humanities, Peking University, Beijing, 100191, People’s Republic of China; 2National Clinical Research Centre for Mental Disorders, Beijing Anding Hospital of Capital Medical University, Beijing, 100088, People’s Republic of China
Correspondence: Qian Wang, National Clinical Research Centre for Mental Disorders, Beijing Anding Hospital of Capital Medical University, Room 204, He Sheng Cai Fu Building, No. 13, De Sheng Street, Hai Dian District, Beijing, 100088, People’s Republic of China, Email [email protected]
Background: Healthcare workers encountered novel job stressors during the late stage of the COVID-19 pandemic. These stressors possessed potential deleterious effects on mental health outcomes, yet the underlying mediating and moderating mechanisms remained relatively unexplored.
Objective: The current study aimed to examine the role of cognitive emotion regulation as a mediator in the association between pandemic-related job stressors and the psychological symptoms of healthcare professionals in the late stage of the COVID-19 pandemic, and the role of reflective functioning as a resilience factor moderating both the associations of pandemic-related job stressors and cognitive emotion regulation, as well as psychological symptoms.
Methods: This cross-sectional survey conducted in October 2020 included 2393 healthcare professionals working in departments with a high risk of exposure to COVID-19 from 22 hospitals in Beijing, China. Participants were asked to complete questionnaires measuring pandemic-related job stressors, anxiety, depression, reflective functioning, and cognitive emotion regulation strategies. Path analyses were performed to examine the hypothesized model.
Results: Epidemic-related job stressors had significant direct effects on depression (β=0.31, p< 0.001) and anxiety symptoms (β=0.29, p< 0.001) and the indirect effects through mediation of maladaptive cognitive regulation were also significant (for depression, indirect effect=0.06, SE=0.01, CI=[0.04, 0.07]; for anxiety, indirect effect=0.06, SE=0.01, CI=[0.04, 0.08]). The dimension of certainty about mental states in the reflective functioning questionnaire (RFQc) moderated the direct effect of pandemic-related job stressors on depression (β=− 0.05, p< 0.001) and moderated the effect of job stressors on maladaptive cognitive regulation (β=0.06, p< 0.001).
Conclusion: The results shed light on the roles of cognitive emotion regulation and reflective functioning in coping with pandemic-related job stressors in frontline healthcare workers in periods of dealing with major infectious diseases. The findings have implications for developing interventions for healthcare workers in need.
Keywords: pandemic-related job stressors, mental health, healthcare professionals, reflective functioning, cognitive emotion regulation
Introduction
The outbreak of coronavirus 2019 (COVID-19) had a dramatic impact on the lives of people around the world. The long-lasting effects of COVID-19 have damaged the whole of humanity’s welfare. Apart from the infection toll, the psychological adaption of people affected by the pandemic has drawn accumulative attention in the field of psychology.
Because of occupational exposure to the virus, high workload and related psychosocial stressors, healthcare professionals are a high-risk group for developing psychological symptoms during this period of upheaval and social crisis.1–3 Accumulative research has revealed that occupational burnout, psychological distress, insomnia, and depression and anxiety were prevalent among healthcare professionals during the outbreak of COVID-19.4–6
After effectively containing the pandemic outbreak, the Chinese government announced a phase of regular epidemic prevention and control, during which strict preventive measures were consistently implemented in the healthcare system to mitigate against a potential resurgence of the epidemic. In this context, healthcare workers continued to shoulder important responsibilities. Tertiary hospitals in Beijing faced a high risk of outbreaks due to the large and mobile population in Beijing City. Our previous study revealed that healthcare workers in tertiary hospitals of Beijing reported heightened levels of burnout and psychological symptoms associated with their exposure to stressors related to the epidemic during its late stage.7 Thus, it is important to investigate factors facilitating psychological adaptation of healthcare workers under long-lasting disease prevention and control measures.
New Epidemic Job Stressors During the Late Stage of the COVID-19 Pandemic
In the late stage of the COVID-19 pandemic, healthcare workers faced new job stressors related to the pandemic. First, disease prevention and control measures required healthcare workers to maintain a high working commitment in addition to their regular practice, which placed an extra burden on them.8 Second, because of the uncertainty of the epidemic, original psychological stressors during the outbreak period such as threat of exposure continued to impact the psychological status of healthcare workers.9,10 As found in our previous work, stressors related to disease prevention and control, increased working load and infection anxiety were the main sources of stress in the post-COVID-19 period, and they significantly predicted psychological symptoms such as depression and anxiety in healthcare workers.11 The present study attempted to explore the underlying mechanism and moderators of such stress by examining the roles of cognitive emotion regulation and reflective functioning.
Cognitive Coping in Response to Stressors: The Mediating Role of Cognitive Emotion Regulation
Cognitive emotion regulation refers to cognitive processes through which individuals consciously manage emotionally-arousing information to regulate their emotional experience. Garnefski et al identified nine distinct cognitive regulation strategies: self-blame, blaming others, rumination, catastrophizing, acceptance, refocus on planning, positive refocusing, positive reappraisal, and putting into perspective.12 The first four dimensions are maladaptive strategies, which are related with depression and anxiety symptoms, while the following five are adaptive strategies, which are associated with better psychological adaptation in stressful situations.13,14
According to Garnefski et al’s theory, cognitive emotion regulation could be considered a cognitive coping strategy in response to negative emotions induced by stressors such as negative life events.12 This perspective bridges studies on cognitive emotion regulation and studies on coping and prompts researchers to examine the effects of cognitive emotion regulation in the process of coping with stress. As found in some previous research, maladaptive cognitive regulation strategies such as rumination and catastrophizing mediated the association between stressors and psychological problems, including depression and anxiety.15,16
Given the role of cognitive emotion regulation as cognitive coping in response to stressors, it is hypothesized that maladaptive cognitive emotion regulation strategies could positively predict depression/anxiety symptoms, while adaptive cognitive emotion regulation strategies could have protective effects on mental health. In addition, cognitive emotion regulation could mediate the association between pandemic-related job stressors and depression/anxiety symptoms.
Reflective Functioning as a Moderator: Perspective from the Diathesis–Stress Model
The diathesis–stress model provides a perspective to examine moderators which influence coping outcomes in response to stressors. The diathesis–stress model proposes that disorder is the result of the interaction between individual vulnerabilities and environmental stresses.17 Individuals with vulnerabilities are more likely to present psychological symptoms when exposed to external stressors.18 Epidemic-related job stressors during the COVID-19 pandemic might have triggered psychological symptoms in individuals. Thus, as an indicator of personal vulnerabilities, reflective functioning was of interest.
Reflective functioning refers to an individual’s capacity to understand the internal mental states of both the self and others in terms of feelings, attitudes and desires.19 It is a fundamental capacity enabling people to understand themselves and explore the social world. As argued by Luyten et al, reflective functioning is a transdiagnostic concept because of its association with psychopathology.20 Previous studies show that impaired reflective functioning constitutes an essential diathesis component in the developmental course of psychological disorders such as borderline personality disorders and depression.21–25 The effects of reflective functioning have also been examined in some studies on stress and coping. As results indicated, reflective functioning is associated with resilience to stress.26,27 Based on the diathesis–stress model and the empirical evidence on the association between reflective functioning and psychopathology, we hypothesized that impaired reflective functioning could positively predict depression/anxiety symptoms in healthcare workers and strengthen the association between pandemic-related job stressors and depression/anxiety symptoms.
Although there has been some evidence to support the idea that deficit in reflective functioning is related to less usage of cognitive reappraisal28 and poorer emotion regulation abilities,29–31 the role of reflective functioning in the link between stressors and cognitive emotion regulation has been less examined. Cognitive emotion regulation could be considered as cognitive responses when facing stressors. In line with the diathesis–stress theory, deficit in reflective functioning might aggravate the effects of stressors on maladaptive patterns of cognitive regulation. Therefore, we hypothesized that reflective functioning could moderate the association between pandemic-related job stressors and usage of adaptive/maladaptive cognitive regulation in healthcare workers.
Overview of the Present Study and Hypotheses
The present study aimed to examine the mediating effect of cognitive emotion regulation in the association between pandemic-related job stressors and depression/anxiety in healthcare workers working in departments with a high risk of exposure to COVID-19 in the post-pandemic period and the moderating effect of reflective functioning in this mediating model. In line with the theoretical model and previous findings, we proposed the following hypotheses (see Figure 1):
Hypothesis 1: COVID-19-related job stressors are associated with depression/anxiety symptoms in healthcare workers. Hypothesis 2: Cognitive emotion regulation mediates the association between pandemic-related job stressors and depression/anxiety symptoms. Hypothesis 3: Deficit in reflective functioning positively predicts depression/anxiety symptoms. Hypothesis 4: Deficit in reflective functioning aggravates the deleterious effect of pandemic-related job stressors on depression/anxiety symptoms. Hypothesis 5: Deficit in reflective functioning also strengthens the link between pandemic-related job stressors and cognitive emotion regulation.
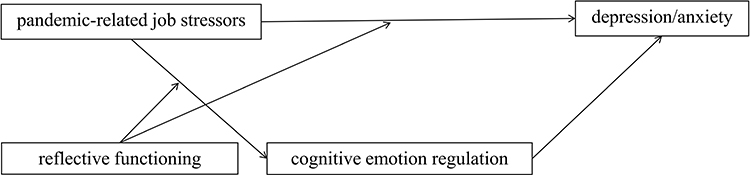 |
Figure 1 The hypothesized model. |
Methods
Participants
Cluster sampling was conducted in 22 municipal hospitals in Beijing. A total of 2393 healthcare workers working in departments with a high risk of exposure to COVID-19, including the infectious disease department, respiratory department, fever clinic, emergency department, intensive care unit, and COVID-19 wards, participated in the present study. There were 514 males (21.5%) and 1879 females (78.5%). The average age was 37.34±8.00. Among them, 523 (21.9%) were doctors, 1376 (57.5%) were nurses, 364 (15.2%) were medical technicians, and 130 (5.4%) were administrators. Detailed demographic information is displayed in Table 1.
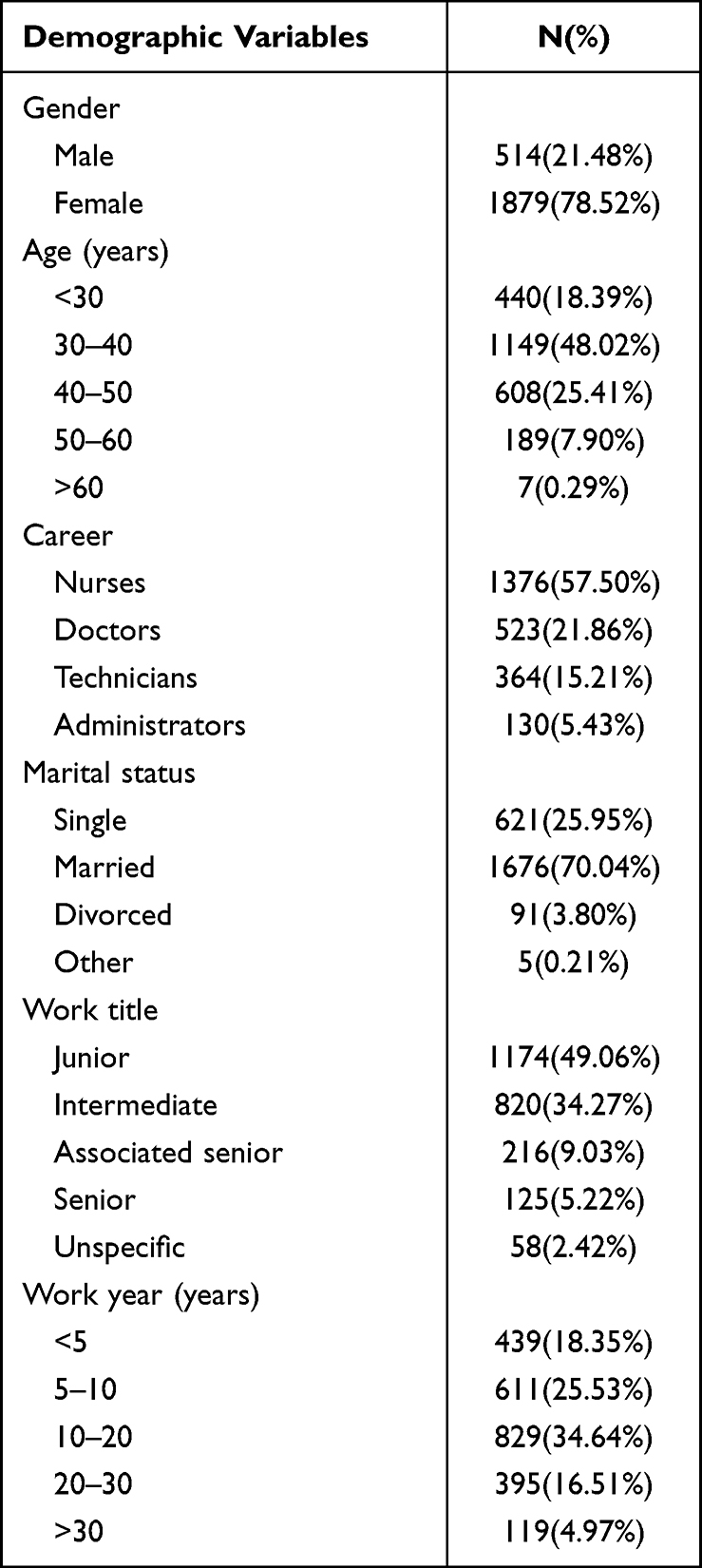 |
Table 1 Demographic Characteristics of Participants |
Measures
Pandemic-Related Job Stressors
As the independent variable in this study, pandemic-related job stressors were measured by the pandemic-related job stressors scale, which was specifically developed to measure stressors experienced by healthcare workers during the late stage of the COVID-19 pandemic.11 The 14-item scale consists of three subscales: stressors related to infection prevention and control measures (9 items, eg, “I am stressed because I am not competent to carry out the infection prevention and control measures”); high workload (3 items, eg, “The epidemic history screen increases the workload”); and infection anxiety (2 items, eg, “When I have a fever or cough, I am worried about being infected by the novel coronavirus”). Items are rated on a 7-point Likert scale (1=very strongly disagree, 7= very strongly agree), with a higher score indicating a higher level of job stressors. The total score of the scale was used in the data analyses. The reliability and validity of this scale were acceptable10 and the Cronbach’s alphas of the whole scale and the three subscales were between 0.72 to 0.89 in the present study.
Depressive Symptoms
As one of the outcome variables of interest, depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9).32 This scale was designed to score each of the nine DSM-IV criteria for major depression on a 4-point Likert scale ranging from “0” (not at all) to “3” (nearly every day) over the previous 2 weeks. The Chinese version of PHQ-9 has good reliability and validity.33 The Cronbach’s alpha for the scale was 0.90 in the current study.
Anxiety Symptoms
Anxiety symptoms was the other outcome variable. GAD-7, a seven-item self-report screening tool,34 was used to assess anxiety symptoms in this study. Each item is rated on a 4-point Likert scale based on how frequently the respondent has experienced the symptom in the past two weeks. Item scores range from 0 (not at all) to 3 (nearly every day). Total score was used in the analysis, with higher scores indicating more severe anxiety symptoms. The Chinese version of GAD-7 has been validated35 and the internal consistency in the present study was 0.91.
Cognitive Emotion Regulation
As the potential mediator of interest, cognitive emotion regulation strategies were measured by the Cognitive Emotion Regulation Scale (CERS).12 This 36-item self-report scale measures nine distinct emotion regulation strategies, four maladaptive strategies (self-blame, blaming others, rumination and catastrophizing) and five adaptive strategies (acceptance, refocus on planning, positive refocusing, positive reappraisal and putting into perspective). A 5-point scoring method is used from 1 (never) to 5 (always). The average scores of the four maladaptive strategies and five adaptive strategies were calculated and used in data analyses. The Chinese version of the CERS has been validated and widely used in Chinese samples.36 The Cronbach’s alphas of the nine subscales ranged from 0.76 to 0.87.
Reflective Functioning
As the potential moderator of interest, reflective functioning was measured by the Reflective Functioning Questionnaire (RFQ),37 which is an 8-item self-report scale consisting of the following dimensions: certainty (RFQc) and uncertainty (RFQu) about mental states. The RFQc subscale comprises 6 items that focus on the extent to which individuals disagree with statements such as, “I don’t always know why I do what I do”. Participants rate each item on a 7-point Likert scale ranging from completely disagree (1) to completely agree (7). The original scores of 1–7 are then recoded into 3, 2, 1, 0, 0, 0, 0 in data analysis. Low scores of this subscale reflect hyper-mentalizing generation of mentalistic representations of actions without appropriate evidence, while high scores reflect more genuine mentalizing. The RFQu subscale captures hypo-mentalizing, an inability to consider complicated models of one’s own mind and/or that of others. It also consists of 6 items, some shared with the RFQc subscale. Participants rate each item on the same Likert scale (eg, “Sometimes I do things without really knowing why”) and the original scores of 1–7 are rescored to 0, 0, 0, 0, 1, 2, 3, to ensure that high scores reflect hypo-mentalizing while low scores reflect genuine mentalizing.
Procedure
This study is a part of the longitudinal research which aimed at investigating the effect of psychological intervention on frontline healthcare staff in China in the context of COVID-19. This study was approved by Beijing Anding Hospital Capital Medical University’s institutional review board. Participants were recruited from 22 tertiary hospitals in Beijing, China. Data collection was conducted in October 2020. Prior to data collection, all participants provided informed consent and were made aware of the importance of completing the questionnaires based on their actual experiences. Upon agreement, the online survey link was distributed to participants. To ensure the validity of responses, probe questions were included in the questionnaire to assess participants’ attentiveness. Responses that scored poorly on the probes or were completed significantly faster than average (3 standard deviations below) were considered invalid and excluded from data analysis.
Statistical Analysis
Descriptive analysis was conducted to obtain demographic characteristics of participants first. Correlations between pandemic-related job stressors, reflective functioning, adaptive emotion regulation strategies, maladaptive emotion regulation strategies, depression and anxiety were calculated next. Path analysis was used to test the hypothesized model. SPSS 18.0 and Mplus 7.4 were used in data analyses.
Results
Correlations Among the Main Variables
Results of correlations among pandemic-related job stressors, reflective functioning (RFQc and RFQu), adaptive/maladaptive cognitive emotion regulation, depression and anxiety are displayed in Table 2. Anxiety was positively correlated with pandemic-related job stressors (r=0.37, p<0.01), maladaptive cognitive regulation (r=0.32, p<0.01) and RFQu (r=0.14, p<0.01) and negatively correlated with RFQc (r=−0.18, p<0.01). Although the correlation between anxiety and adaptive cognitive regulation was significant, the coefficient was very small (r=−0.04, p<0.05). The correlations of depression with other variables were similar with those of anxiety.
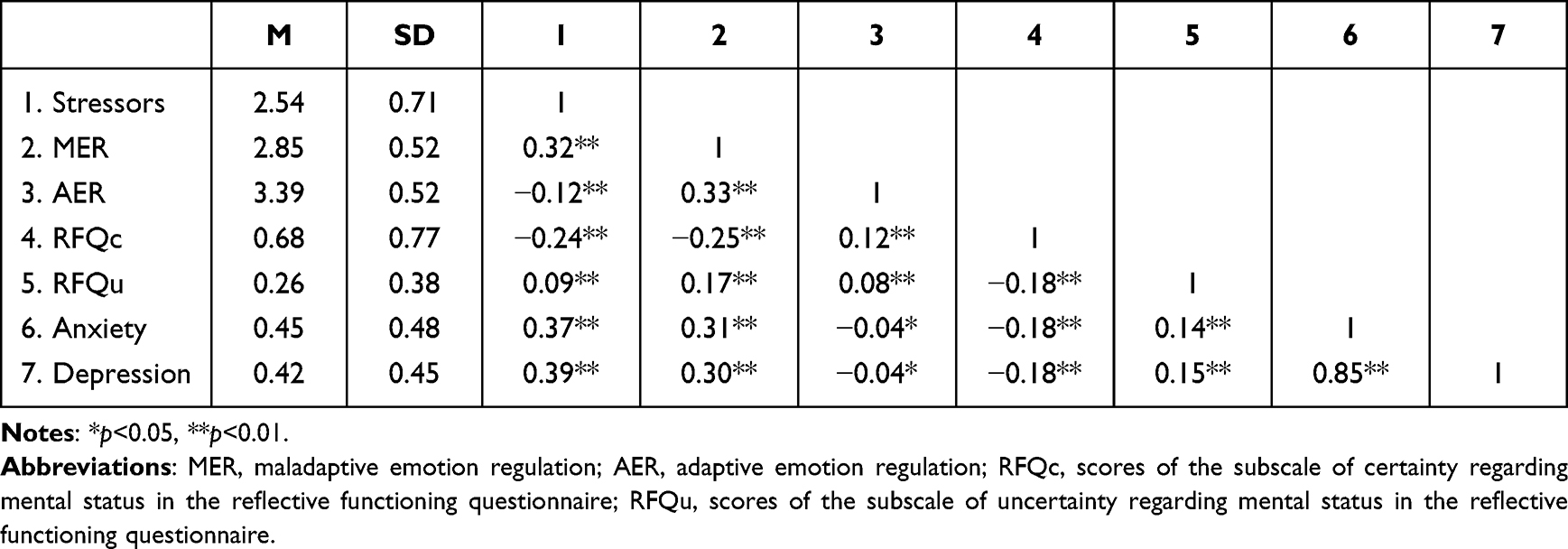 |
Table 2 Correlations Among the Main Variables |
Model Testing
Path analyses were conducted to examine the mediating effect of emotion regulation in the association between pandemic-related stressors and depression/anxiety and the moderating effect of reflective functioning in the direct pathway (pandemic-related stressors → depression/anxiety) and the first half of the mediating pathway (pandemic-related stressors → cognitive emotion regulation). Because the correlation coefficients of adaptive cognitive regulation and reflective functioning, depression and anxiety were too small (ranging from 0.07 to 0.13), only the mediating effect of maladaptive cognitive regulation was examined. The models for depression and anxiety were examined, respectively, and the moderating effects of RFQc and RFQu were examined, respectively. In all models, demographic characteristics, including gender, age, length of working experience and career, were used as covariates because of their significant effects on depression and anxiety.1 All continuous variables were standardized.
For the depression model with RFQc as the moderator, the model fitness was satisfactory, with χ2=7.75, df=6, RMSEA=0.01, CFI=0.99, TLI=0.99. As indicated in Figure 2, pandemic-related job stressors directly predicted depression (β=0.31, p<0.001) and also had an indirect effect through the mediation of maladaptive cognitive regulation. The interaction of stressors and RFQc significantly predicted maladaptive cognitive regulation (β=0.06, p<0.001) and depression (β=−0.05, p<0.001).
 |
Figure 2 The mediating effect of maladaptive emotion regulation in the association between pandemic-related job stressors and depression, with certainty regarding mental status as the moderator. Notes: **p<0.01; RFQc=certainty score regarding mental status in the reflective functioning questionnaire. |
Simple slope tests were conducted to further examine the moderating effects of RFQc. Results indicated that the effect magnitude of stressors on maladaptive cognitive regulation was larger in participants with higher RFQc (β=0.34, p<0.001) than that in participants with lower RFQc (β=0.22, p<0.001) (see Figure 3a). In addition, when RFQc was low (M–SD), pandemic-related stressors had a greater effect on depression (β=0.40, p<0.001) and, when RFQc was high (M+SD), the effect of pandemic-related stressors was smaller (β=0.33, p<0.001) (see Figure 3b).
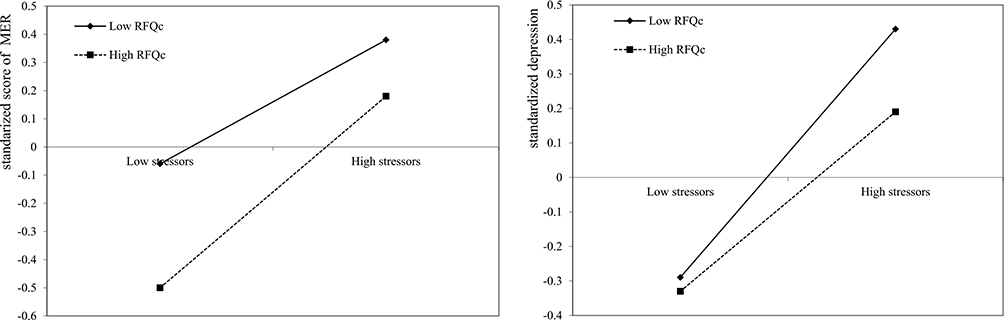 |
Figure 3 (a) Relationship between epidemic-related job stressors and maladaptive emotion regulation at high and low levels of certainty regarding mental status; (b) relationship between epidemic-related job stressors and depression at high and low levels of certainty regarding mental status. Note: RFQc, the certainty score regarding mental status in the reflective functioning questionnaire. |
A bootstrapping procedure was used to examine the mediating effect of maladaptive cognitive regulation on the association between pandemic-related job stressors and depression. The bootstrap samples were set at 1000. As results indicated, the average direct effect of pandemic-related stressors on depression was significant (effect=0.31, SE=0.02, CI=[0.25, 0.34]) and the average indirect effect of pandemic-related stressors through the mediation of maladaptive cognitive regulation was also significant (effect=0.06 SE=0.01, CI=[0.04, 0.07]). The mediating effect of maladaptive cognitive regulation was smaller when RFQc was low (M–SD) (effect=0.04, SE=0.01, CI=[0.03, 0.06]) and larger when RFQc was high (M+SD) (effect=0.07, SE=0.01, CI=[0.05, 0.09]).
For the depression model with RFQu as the moderator, the model fitness was also good, with χ2=8.13, df=6, RMSEA=0.01, CFI=0.99, TLI=0.99. As indicated in Figure 4, depression was directly predicted by pandemic-related job stressors (β=0.31, p<0.001) and impacted by stressors through the mediation of maladaptive cognitive regulation. The mediating effect of maladaptive emotion regulation was the same as that evident in the previous model using RFQc as the moderator. Because the interaction term of RFQu and stressors were not significantly associated with maladaptive cognitive regulation (β=0.002, p=0.920) and depression (β=0.01, p=0.399), the moderating effect of RFQu was not significant.
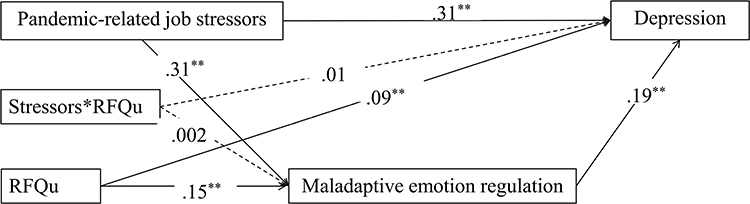 |
Figure 4 The mediating effect of maladaptive emotion regulation in the association between pandemic-related job stressors and depression, with uncertainty regarding mental status as the moderator. Notes: **p<0.01; RFQu=uncertainty score regarding mental status in the reflective functioning questionnaire. |
For the anxiety model with RFQc as the moderator, the model fitness was good, with χ2=7.75, df=6, RMSEA=0.01, CFI=0.99, TLI=0.99. The path coefficients are displayed in Figure 5. Pandemic-related job stressors had a direct effect on anxiety (β=0.29, p<0.001) and also had an indirect effect through the mediation of maladaptive cognitive regulation. The moderating effect of RFQc in the direct path was not significant (β=−0.03, p=0.097) while its moderating effect in the association between pandemic-related job stressors and maladaptive cognitive regulation was significant (β=0.06, p<0.001).
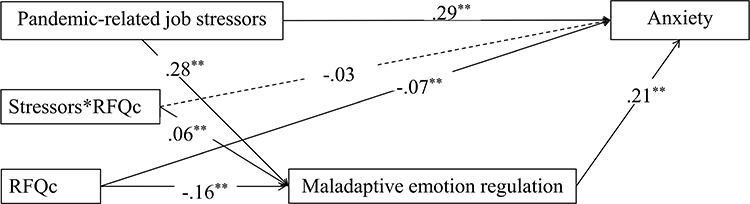 |
Figure 5 The mediating effect of maladaptive emotion regulation in the association between pandemic-related job stressors and anxiety, with certainty regarding mental status as the moderator. Notes: **p<0.01; RFQc=certainty score regarding mental status in the reflective functioning questionnaire. |
In summary, the direct effect of pandemic-related stressors on anxiety was significant (effect=0.29 SE=0.02, CI=[0.23, 0.32]) and the indirect effect through the mediation of maladaptive cognitive regulation was also significant (effect=0.06 SE=0.01, CI=[0.04, 0.08]). The mediating effect of maladaptive cognitive regulation was smaller in participants low in RFQc (M–SD) (effect=0.05, SE=0.01, CI=[0.03, 0.06]) and larger in participants high in RFQc (M+SD) (effect=0.07, SE=0.01, CI=[0.05, 0.10]).
For the anxiety model with RFQu as the moderator, the model fitness was good, with χ2=8.13, df=6, RMSEA=0.01, CFI=0.99, TLI=0.99. As shown in Figure 6, pandemic-related job stressors had a direct effect on anxiety (β=0.29, SE=0.02, CI=[0.24, 0.33]) and also an indirect effect through the mediation of maladaptive cognitive regulation (effect=0.06, SE=0.01, CI=[0.05, 0.08]). The mediating effect accounted for 20% of the total effect. The interaction of RFQu and stressors was not significantly associated with maladaptive cognitive regulation (β=0.02, p=0.097) and anxiety (β=0.03, p=0.109).
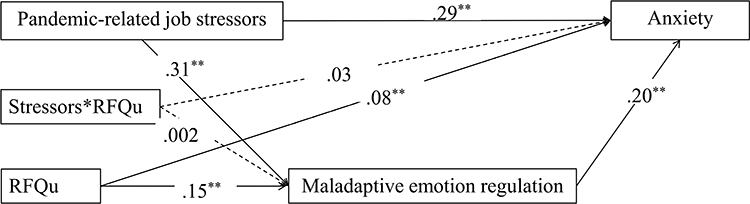 |
Figure 6 The mediating effect of maladaptive emotion regulation in the association between pandemic-related job stressors and anxiety, with uncertainty regarding mental status as the moderator. Notes: **p<0.01; RFQu=uncertainty score regarding mental status in the reflective functioning questionnaire. |
Discussion
The present study focused on stress and coping processes of healthcare workers working in departments with a high risk of exposure to COVID-19 in the late stage of the COVID-19 pandemic. It examined the effects of pandemic-related stressors on depression/anxiety symptoms and the roles of cognitive emotion regulation and reflective functioning in the process of stress and coping.
Pandemic-Related Job Stressors in the Late Stage of the COVID-19 Pandemic and Mental Health of Healthcare Workers
As results indicated, pandemic-related stressors positively predicted depression and anxiety symptoms in healthcare workers. Thus, Hypothesis 1 was supported. This result is in line with some previous research findings38 and suggests that the novel job stressors in the post-pandemic period had potentially deleterious effects on mental health of healthcare workers. Because the pandemic has been lasting for a long time and might still continue to affect the world, the infection prevention and control measures might become a normative work routine of healthcare workers. Therefore, it is important for organizations to provide adequate protective measures and in the meantime help healthcare professionals integrate infection prevention and control measures into their daily work in a clear and convenient way.
Role of Cognitive Emotion Regulation in the Process of Stress and Coping
As indicated in our results, maladaptive cognitive regulation was more pronouncedly related with depression/anxiety compared with adaptive cognitive regulation. This result is consistent with the findings of Aldao et al’s meta-analysis (2010) and suggests that the harmful effects of maladaptive cognitive regulation strategies are greater while the protective effects of adaptive cognitive regulation strategies are smaller.39 However, this differs from Schäfer et al’s study, which found that adaptive cognitive regulation was as important as maladaptive cognitive regulation.40 The difference in results might be related to variance in specific adaptive/maladaptive strategies involved in different studies.
In line with Hypothesis 2, maladaptive cognitive coping was found to mediate the association between pandemic-related job stressors and depression/anxiety. The result is consistent with the transactional model of coping with stress41 and suggests that it is suitable to use cognitive emotion regulation as an indicator of cognitive coping. This result suggests that cognitive coping is an important mechanism which influences individuals’ adaptation in stressful situations and implies that evaluating and reducing maladaptive emotion regulation strategies is critical in interventions to improve psychological adaptation for healthcare workers impacted by pandemic-related job stressors.
Role of Reflective Functioning in the Process of Stress and Coping
Regarding the role of reflective functioning, our results demonstrated that the RFQc subscale score was negatively associated with depression/anxiety and the RFQu subscale score was positively associated with depression/anxiety. Both hyper-mentalizing and hypo-mentalizing contributed to psychological symptoms such as depression and anxiety. Therefore, Hypothesis 3 was supported. Hypothesis 4 was also supported by the significant moderating effect of the RFQc score in the association between pandemic-related job stressors and depression. Specifically, as the level of pandemic-related job stressors increased, individuals who hyper-mentalize problems reported a greater increase in depression symptoms. Reflective functioning is a higher order thinking processes, which enables people to make sense of stressful experience and negative emotions related to it; it is also a prerequisite for effectively communicating emotions and thoughts to others. Therefore, reflective functioning helps cope with stress.42 Individuals who hyper-mentalize problems have difficulty reflecting mental states of themselves and others accurately, which reduces their coping abilities and negatively influences their psychological adaptation. Similar results were found in Aiveal-Naveh et al, which suggested that reflective functioning moderated the association between emotional distress and eating disorders in secular Jewish women.43
In contrast to Hypothesis 5, hyper-mentalizing (measured by the RFQc subscale) alleviated the effects of pandemic-related job stressors on usage of maladaptive cognitive emotion regulation strategies. That is, pandemic-related job stressors had a stronger impact on the reporting of maladaptive cognitive regulation problems by individuals with greater genuine mentalizing abilities than by those with hyper-mentalizing problemss. This reversed effect could be explained as follows: individuals hyper-mentalizing problems might have greater difficulty recognizing and reporting their maladaptive cognitions accurately when stress increases; however, individuals with greater genuine reflective functioning ability can verbalize negative emotions and thoughts generated in stressful situations.42 Given that empirical studies focusing on the role of reflective functioning in the process of stress and cognitive coping are limited, this result and explanation still need to be further examined in future research.
Implications
The present study has theoretical and practical implications. First, theoretically, reflective functioning used to be studied in research on psychopathology, such as borderline personality disorders, eating disorders and depression, and were more often assessed in clinical samples. The present study deepened understanding of the role of reflective functioning in the process of experiencing stress and coping with it in a non-clinical population. Second, the present study also pioneered examining the role of reflective functioning in the association between stressors and cognitive emotion regulation and provids primary empirical evidence for a relationship between these two variables.
Results of the present study have practical implications in managing stress for healthcare workers in the post-pandemic period. First, because of the significant effects of pandemic-related stressors on psychological symptoms of healthcare workers, it is important for organizations to optimize the working conditions and working routine to integrate infection prevention and control measures and reduce stressors experienced by frontline healthcare professionals. Second, reducing usage of maladaptive emotion regulation strategies could be an effective target in interventions to improve the psychological adaptation of healthcare workers when facing pandemic-related job stressors. Finally, third, evaluation of reflective functioning is also necessary to screen for individuals who are vulnerable to psychological problems in stressful situations.
Limitations and Future Directions
There are several limitations to the present study. First, all variables were measured by self-reported questionnaires. Self-report bias might influence the results. The validity of the study could be improved by using a multi-method measurement in future studies to assess variables such as reflective functioning. Second, the effects of adaptive/maladaptive cognitive regulation were examined separately, leaving the patterns of using multiple strategies unexamined. Person-centered approach might be used in further study to explore the role of cognitive regulation patterns in the process of stress and coping.
Conclusions
The present study confirmed the mediating role of maladaptive cognitive emotion regulation as an indicator of cognitive coping in the association between pandemic-related job stressors and psychological symptoms. It found that a deficit in reflective functioning is a factor that contributes to psychological symptoms and amplifies the effect of stressors on those with depression. These findings suggest that psychoeducation or intervention programs targeting the reduction of maladaptive cognitive emotion regulation and enhancement of mentalizing capacity may prove valuable for preventing or managing psychological problems of healthcare workers impacted by pandemic-related stressors.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All participants gave their oral and written informed consent. The study was approved by the Institutional Review Board of Beijing Anding Hospital (#2020-85) and complies with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this study.
References
1. Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2021;49(5):547–554. doi:10.1016/j.ajic.2020.10.001
2. Masiero M, Mazzocco K, Harnois C, Cropley M, Pravettoni G. From individual to social trauma: sources of everyday trauma in Italy, the US and UK during the Covid-19 pandemic. J Trauma Dissoc. 2020;21(5):513–519. doi:10.1080/15299732.2020.1787296
3. Schwartz R, Sinskey JL, Anand U, Margolis RD. Addressing postpandemic clinician mental health: a narrative review and conceptual framework. Ann Intern Med. 2020;173(12):981–988. doi:10.7326/M20-4199
4. Blekas A, Voitsidis P, Athanasiadou M, et al. COVID-19: PTSD symptoms in Greek health care professionals. Psychol Trauma. 2020;12(7):812–819. doi:10.1037/tra0000914
5. Miotto K, Sanford J, Brymer MJ, Bursch B, Pynoos RS. Implementing an emotional support and mental health response plan for healthcare workers during the COVID-19 pandemic. Psychol Trauma. 2020;12(S1):S165–S167. doi:10.1037/tra0000918
6. Vagni M, Maiorano T, Giostra V, Pajardi D. Hardiness, stress and secondary trauma in Italian Healthcare and emergency workers during the COVID-19 pandemic. Sustainability. 2020;12(14):5592. doi:10.3390/su12145592
7. Zhou T, Xu C, Wang C, et al. Burnout and well-being of healthcare workers in the post-pandemic period of COVID-19: a perspective from the job demands-resources model. BMC Health Serv Res. 2022;22(1):284. doi:10.1186/s12913-022-07608-z
8. Krystal JH, Alvarado J, Ball SA, et al. Mobilizing an institutional supportive response for healthcare workers and other staff in the context of COVID-19: the Yale experience. Gen. Hosp Psychiatry. 2021;68:12–18. doi:10.1016/j.genhosppsych.2020.11.005
9. Restauri N, Sheridan AD. Burnout and posttraumatic stress disorder in the Coronavirus disease 2019 (COVID-19) pandemic: intersection, impact, and interventions. J Am Coll Radiol. 2020;17(7):921–926. doi:10.1016/j.jacr.2020.05.021
10. Zhou T, Guan RY, Pu ZN, Zhao W, Sun LQ. Acute stress responses of medical staff treating patients with COVID-19: a moderated mediation model. Chin J Clin Psychol. 2020;28(4):751–755. doi:10.16128/j.cnki.1005-3611.2020.04.021
11. Zhou T, Wang Q, Zhang C, et al. Pilot evaluation of the Epidemic-related Job Stressors Scale for healthcare workers. Chin Ment Health J. 2023;37(4):354–360.
12. Garnefski N, Kraaij V, Spinhoven P. Negative life events, cognitive emotion regulation and emotional problems. Pers Indiv Differ. 2001;30(8):1311–1327. doi:10.1016/s0191-8869(00)00113-6
13. Garnefski N, Kraaij V. Relationships between cognitive emotion regulation strategies and depressive symptoms: a comparative study of five specific samples. Pers Indivl Differ. 2006;40(8):1659–1669. doi:10.1016/j.paid.2005.12.009
14. Van Beveren ML, Harding K, Beyers W, Braet C. Don’t worry, be happy: the role of positive emotionality and adaptive emotion regulation strategies for youth depressive symptoms. Br. J Clin Psychol. 2018;57(1):18–41. doi:10.1111/bjc.12151
15. Chan SM, Poon SFO, Tang EMH. Daily hassles, cognitive emotion regulation and anxiety in children. Vulnerable Child You. 2016;11(3):238–250. doi:10.1080/17450128.2016.1214887
16. Yan J, Kong T, He Y, Mcwhinnie CM, Yao S, Xiao J. Daily hassles and depression in individuals with cognitive vulnerability to depression: the mediating role of maladaptive cognitive emotion regulation strategies. Nord Psychol. 2015;67(1):87–100. doi:10.1080/17450128.2016.1214887
17. Goforth AN, Pham AV, Carlson JS. Diathesis-Stress Model. In: Encyclopedia of Child Behavior and Development. Boston, MA: Springer; 2011.
18. McKeever VM, Huff ME. A diathesis-stress model of posttraumatic stress disorder: ecological, biological, and residual stress pathways. Rev Gen Psychol. 2003;7(3):237–250. doi:10.1037/1089-2680.7.3.237
19. Fonagy P. On tolerating mental states: theory of mind in borderline patients. Bull Anna Freud Cent. 1989;12(2):91–115.
20. Luyten P, Campbell C, Allison E, Fonagy P. The Mentalizing approach to psychopathology: state of the art and future directions. Annu Rev Clin Psycho. 2020;16(1):297–325. doi:10.1146/annurev-clinpsy-071919-015355
21. Chiesa M, Fonagy P. Reflective function as a mediator between childhood adversity, personality disorder and symptom distress. Personal Ment Health. 2014;8(1):52–66. doi:10.1002/pmh.1245
22. De Coninck D, Matthijs K, Luyten P. Depression in Belgian first-year university students: a longitudinal study of self-definition, interpersonal relatedness, mentalizing, and integration. J. Clin Psychol. 2021;77(7):1715–1731. doi:10.1002/jclp.23149
23. Fischer-Kern M, Fonagy P, Kapusta ND, et al. Mentalizing in female inpatients with major depressive disorder. J. Nerv Ment Dis. 2013;201(3):202–207. doi:10.1097/NMD.0b013e3182845c0a
24. Gunderson JG, Lyons-Ruth K. BPD’s interpersonal hypersensitivity phenotype: a gene-environment-developmental model. J Pers Disord. 2008;22(1):22–41. doi:10.1521/pedi.2008.22.1.22
25. Steele M, Bate J, Nikitiades A, Buhl-Nielsen B. Attachment in adolescence and borderline personality disorder. J Infant Child Adolesc Psychother. 2015;14(1):16–32. doi:10.1080/15289168.2015.1004882
26. Schwarzer NH, Gingelmaier S. Mentalizing as protective resource among teaching trainees. Fruhe Bild. 2020;9(3):144–152. doi:10.1026/2191-9186/a000485
27. Schwarzer N, Nolte T, Fonagy P, Gingelmaier S. Self-rated mentalizing mediates the relationship between stress and coping in a non-clinical sample. Psychol Rep. 2022;125(2):742–762. doi:10.1177/0033294121994846
28. Rothschild-Yakar L, Peled M, Enoch-Levy A, Gur E, Stein D. “Eating Me Up from Inside”: a pilot study of mentalization of self and others and emotion regulation strategies among young women with eating disorders. Isr J Psychiatry. 2018;55(1):35–43.
29. Fonagy P, Gergely G, Jurist EL, Target M. Affect Regulation, Mentalization and the Development of the Self. London: Routledge; 2018. doi:10.4324/9780429471643
30. Parada-Fernández P, Herrero-Fernández D, Oliva-Macías M, Rohwer H. Analysis of the mediating effect of mentalization on the relationship between attachment styles and emotion dysregulation. Scand J Psychol. 2021;62(3):312–320. doi:10.1111/sjop.12717
31. Nazzaro MP, Boldrini T, Tanzilli A, Muzi L, Giovanardi G, Lingiardi V. Does reflective functioning mediate the relationship between attachment and personality? Psychiat Res. 2017;256:169–175. doi:10.1016/j.psychres.2017.06.045
32. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
33. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
34. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
35. He XY, Li CB, Qian J, Cui HS, Wu WY. Reliability and validity of a generalized anxiety disorder scale in general hospital outpatients. Shanghai Arch Psychiatr. 2010;22(4):200–203. doi:10.3969/j.issn.1002-0829.2010.04.002
36. Zhu X, Auerbach RP, Yao S, Abela JRZ, Xiao J, Tong X. Psychometric properties of the Cognitive Emotion Regulation Questionnaire: Chinese version. Cognit Emot. 2008;22(2):288–307. doi:10.1080/02699930701369035
37. Fonagy P, Luyten P, Moulton-Perkins A, et al. Development and validation of a self-report measure of mentalizing: the reflective functioning questionnaire. PLoS One. 2016;11(7):e0158678. doi:10.1371/journal.pone.0158678
38. Li J, Xu J, Zhou H, et al. Working conditions and health status of 6317 front line public health workers across five provinces in China during the COVID-19 epidemic: a cross-sectional study. BMC Public Health. 2021;21(1):106. doi:10.1186/s12889-020-10146-0
39. Aldao A, Nolen-Hoeksema S, Schweizer S. Emotion-regulation strategies across psychopathology: a meta-analytic review. Clin Psychol Rev. 2010;30(2):217–237. doi:10.1016/j.cpr.2009.11.004
40. Schäfer JÖ, Naumann E, Holmes EA, Tuschen-Caffier B, Samson AC. Emotion regulation strategies in depressive and anxiety symptoms in youth: a meta-analytic review. J Youth Adolesc. 2017;46(2):261–276. doi:10.1007/s10964-016-0585-0
41. Lazarus RS, Folkman S. Transactional theory and research on emotions and coping. Eur J Pers. 1987;1(3):141–169. doi:10.1002/per.2410010304
42. Robinson P, Skårderud F, Sommerfeldt B. Hunger: Mentalization-Based Treatments for Eating Disorders. Springer International Publishing; 2018. doi:10.1007/978-3-319-95121-8
43. Aival-Naveh E, Rothschild-Yakar L, Kurman J. The moderating effects of self and other mentalizing on the relationship between distress and disordered eating: a cross-cultural examination. J. Clin Psychol. 2021;77(9):1937–1953. doi:10.1002/jclp.23121
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.