Back to Journals » Patient Preference and Adherence » Volume 20
Coping and Resilience in Chinese Couples with Connective Tissue Diseases: A Culturally Informed Qualitative Explanation
Authors Cai X, Xu S, Dong C, Gu Z
Received 19 November 2025
Accepted for publication 5 February 2026
Published 17 February 2026 Volume 2026:20 578038
DOI https://doi.org/10.2147/PPA.S578038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Xingfeng Cai,* Shu Xu,* Chen Dong, Zhifeng Gu
Department of Rheumatology, Affiliated Hospital of Nantong University, Nantong University, Nantong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chen Dong, Department of Rheumatology, Affiliated Hospital of Nantong University, Nantong University, Nantong, People’s Republic of China, Email [email protected] Zhifeng Gu, Department of Rheumatology, Affiliated Hospital of Nantong University, Nantong University, Nantong, People’s Republic of China, Email [email protected]
Purpose: Connective tissue diseases (CTDs) predominantly affect women, creating complex self-care and psychosocial demands that extend to their spouses. Yet, how couple-level interactions shape outcomes—or how nurses can harness dyadic resources in care—remains poorly understood. This study aims to explain and deeply understand how couples co-construct resilience in managing CTDs, thereby elucidating the interactional mechanisms underlying the previously observed null effect of partner coping.
Patients and Methods: A descriptive qualitative study was conducted and reported following the COREQ guidelines. Twelve couples (comprising women with CTDs and their husbands) were purposively sampled. Semi-structured joint interviews, lasting 60– 90 minutes, were audio-recorded, transcribed verbatim, and analyzed using reflexive thematic analysis in NVivo 14. To ensure credibility, member checking and dual-coder consensus were employed.
Results: Three themes emerged: (1) emotional resonance from disease shock, involving shared disbelief, role imbalance, and contagion; (2) an evolution in dyadic coping from joint avoidance to a division of labor and finally to embodied support; and (3) the joint construction of resilience through meaning-making, trust-building rituals, and humorous future re-imagining. However, well-intentioned support was found to subvert patient autonomy, providing a key explanation for the null effect of positive dyadic coping observed in quantitative studies.
Conclusion: Resilience is a dynamic, dyadic construct, co-constructed in moment-to-moment interactions. This necessitates viewing the couple, not the individual, as the essential unit of care in CTDs management. Interventions must therefore be designed to preserve patient autonomy while cultivating authentic emotional disclosure and collaborative problem-solving.
Plain Language Summary: Using joint interviews with 12 Chinese couples in which the wife lived with systemic lupus, rheumatoid arthritis or systemic sclerosis, this qualitative study uncovered how marital interaction shaped resilience. Through reflexive thematic analysis we found that (1) shared shock and emotional contagion initially intensified dyadic distress, (2) couples evolved task-oriented coping that occasionally slipped into protective over-control, silencing the patient, and (3) dyads who sustained co-constructed narratives, micro-rituals and collaborative humor transformed illness into a communal “we-experience”, strengthening joint resilience. The findings foreground the couple—rather than the individual patient—as the minimal unit of care and emphasize preserving patient agency within authentic dyadic dialogue.
Keywords: connective-tissue diseases, dyadic coping, resilience, couple interaction, clinical nursing, qualitative research
Introduction
Connective Tissue Diseases (CTDs), such as systemic lupus erythematosus, rheumatoid arthritis, and Sjögren’s syndrome, represent a group of chronic, highly disabling, and relapsing autoimmune disorders.1,2 The nature of these conditions necessitates that patients and their families confront long-term, complex, and unpredictable challenges. On a physiological level, patients endure multi-systemic symptoms, including pain, profound fatigue, joint deformities, and organ damage.3 Psychologically, disease-related changes in appearance, functional limitations, and uncertainty about the future frequently lead to anxiety, depression, and other forms of psychological distress. Socially, CTDs impair work capacity, disrupt social roles and family dynamics, resulting in a substantial societal burden.4,5
Traditional health psychology research has predominantly focused on individual coping strategies and adaptation outcomes. However, the management of chronic illness is not an individual endeavor, particularly for married patients whose spouses often serve as primary caregivers and the most crucial source of support.6 Viewing the couple as a dynamic, interdependent unit that jointly manages illness-related stress—a process known as Dyadic Coping—has emerged as a cutting-edge area of international research.
A substantial body of evidence indicates that effective dyadic coping can significantly enhance patients’ quality of life, treatment adherence, and psychological well-being, while simultaneously reduce caregiver burden and improve relationship satisfaction for both partners. For instance, Zhang et al found that among cervical cancer patients, positive dyadic coping helped mitigate disease-related stress and strengthened supportive interactions within the couple.7 Similarly, in couples facing breast cancer or perinatal loss, the quality of dyadic coping was positively correlated with levels of post-traumatic growth.8 Consequently, shifting the research focus from the individual to the dyad is an essential step toward deeply understanding and effectively intervening in the family stress associated with chronic illness. Despite the growing recognition of its importance, a significant knowledge gap exists regarding dyadic coping in CTDs populations, particularly research that delves into its underlying processes and lived experiences.
First, there is a lack of in-depth exploration within the Chinese cultural context. Dyadic coping is profoundly influenced by cultural values. While Western studies often emphasize partner equality and direct communication, the “family-centric” ethos in China may foster distinct coping patterns characterized by a greater emphasis on responsibility over emotional expression and a tendency to contain stress within the family unit rather than disclosing it to outsiders. Presently, there is a scarcity of research that explores these culturally embedded psychological processes from the perspectives of both Chinese patients and their spouses. Second, the current understanding of the process and meaning of coping is insufficient. While existing quantitative studies can establish correlations between dyadic coping and outcome variables, they struggle to answer process-oriented and explanatory questions such as “how” couples cope and “why” they cope in specific ways. For example, subtle non-verbal cues, unspoken understandings, and complex interactions like “protective buffering”—where one partner conceals concerns to avoid worrying the other—cannot be fully captured by scale scores. Qualitative methodologies, particularly in-depth interviews, are the key to unlocking this “black box.”
This study examines the coping practices of Chinese CTDs patient–partner dyads to elucidate the core dimensions and dynamic processes of their dyadic coping. The findings will contribute localized empirical evidence to cross-cultural health psychology, inform the design of targeted psychosocial interventions and clinical nursing practices, and ultimately support patient and family agency. The research addresses two central questions:1 How do couples with connective tissue diseases collaboratively build resilience in managing their illness?2 Why do partners’seemingly positive coping behaviors sometimes fail to translate into improved patient resilience?
Methods
Design
In our previous cross-sectional survey involving 260 pairs of CTDs patients and their partners (survey ongoing), researchers found no significant impact of partner coping styles on patients’ psychological resilience. This finding diverges from the common conclusion in most chronic disease studies that “positive coping styles are positively correlated with patients’ psychological resilience”. To explore the reasons behind this discrepancy, this study employs qualitative research methods to systematically investigate the potential causes for the absence of this association in the CTDs population.
Sample and Setting
The study recruited participants from the rheumatology outpatient department of a tertiary general hospital in Jiangsu Province, China, between October 2023 and August 2024. A purposive sampling strategy with maximum variation was employed to capture a broad spectrum of participant characteristics, including age, disease duration, education level, and number of children.
Patient inclusion criteria included: (i) a confirmed diagnosis of SLE, RA, or SSc; (ii) female sex, aged 20–50 years; (iii) married and cohabiting; and (iv) mental competence and willingness to provide informed consent. Exclusion criteria (applied to both patients and spouses): (i) active malignancy; (ii) severe cardio-cerebrovascular or renal disease; (iii) cognitive impairment or major psychiatric illness; (iv) concurrent participation in any psychosocial intervention.
During routine visits, eligible couples were briefed on the study and audio-recording and then chose an interview location (hospital quiet room, home, or online). We enrolled couples until thematic saturation was reached—no new themes emerged after the 10th couple, and two further interviews confirmed this. The final cohort consisted of 12 couples (SLE=5, RA=4, SSc=3). Participant characteristics are summarized in Tables 1 and 2. This study has been approved by the Ethics Committee of Nantong University Affiliated Hospital (Approval No. 2021-K046) and complies with the Declaration of Helsinki. We have obtained written informed consent from all participants and anonymized the patients. The patients and their spouses have consented to the potential publication of their statements.
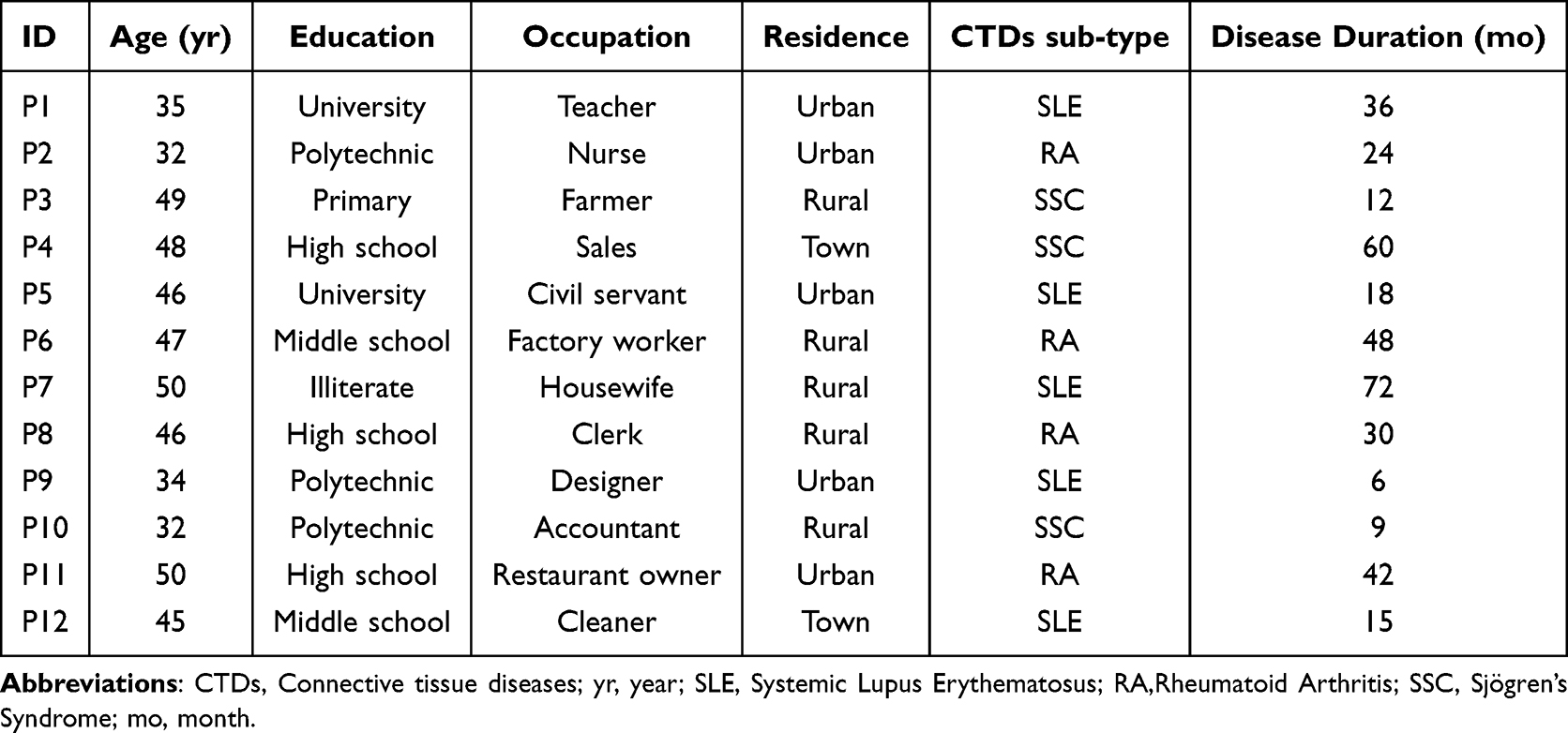 |
Table 1 Characteristics of Female Patients with CTDs (n=12) |
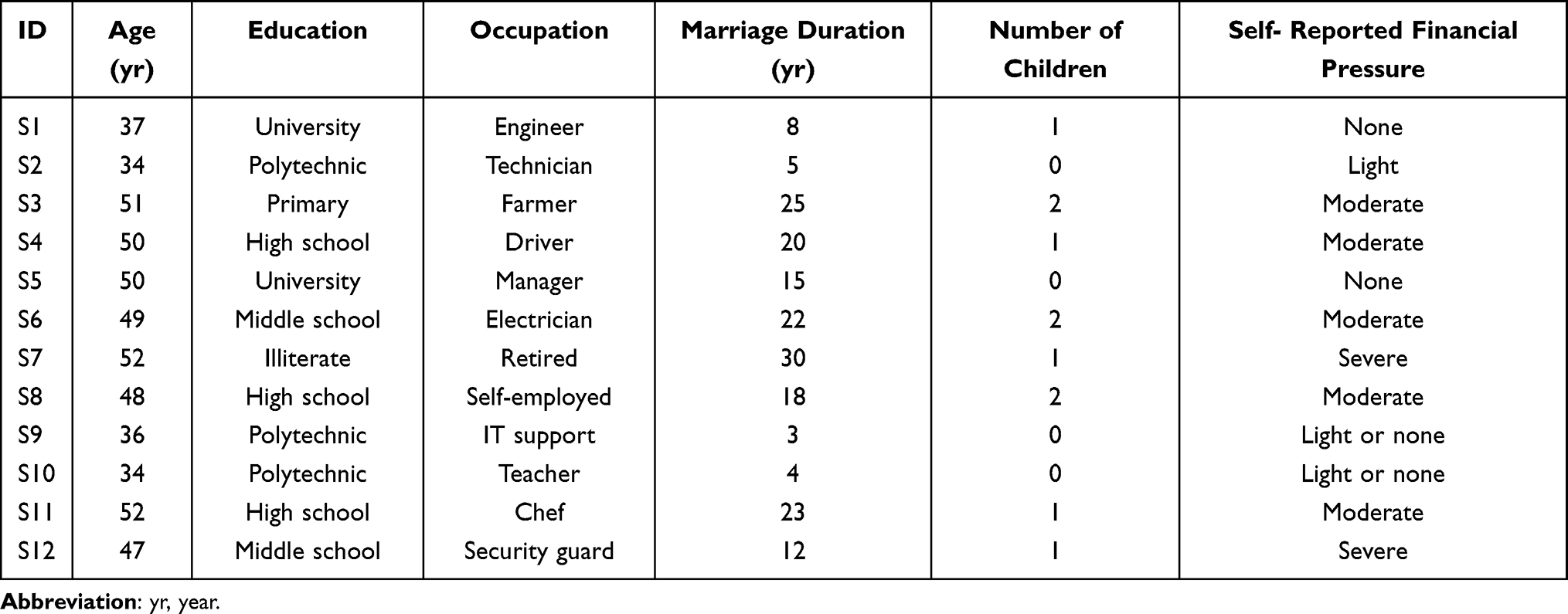 |
Table 2 Characteristics of Spouses (n=12) |
Grounded in dyadic coping theory, which posits that partners appraise illness stress as a shared “we-dimension”, this study applied its core sequential components to guide our methodology.9 This framework informed (i) the interview guide, structured around the stages of stress appraisal (via emotional disclosure), coping (through strategy matching), and adaptation (via resilience co-construction); and (ii) the data interpretation, ensuring the analysis focused on couple-level processes.
The Interview Outline is Detailed Below
The interview outline (Figure 1) was developed from dyadic-coping theory and an extensive literature review. Following two pilot interviews (which were included in the final analysis), the wording was refined, and a fifth question was added to better explore spousal burden. The final guide covered: (1) Initial reactions to the diagnosis (from both partners); (2) Responses to a recent episode of patient low mood; (3) Joint decision-making regarding treatment and daily tasks; (4) Experiences that made the couple feel stronger than the illness; and (5) Interactions that were energizing versus burdensome for the spouse.
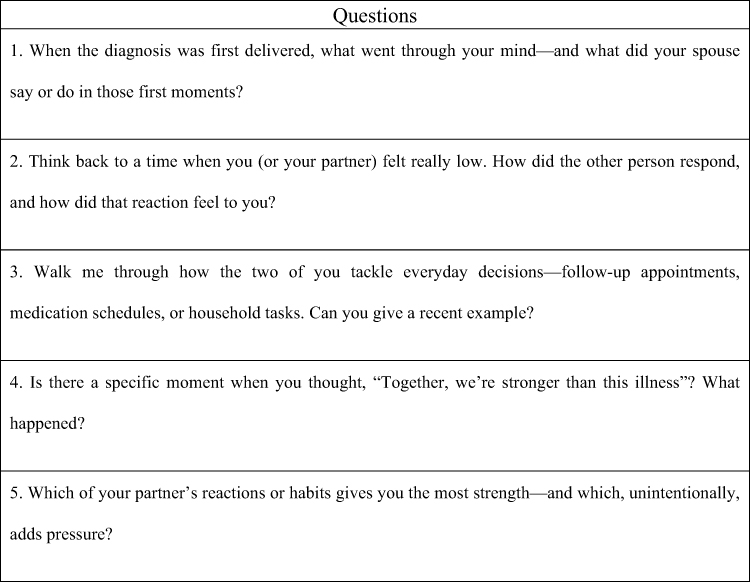 |
Figure 1 Final version of the interview guide. |
Data Collection
One researcher conducted all dyadic interviews in person or online. Sessions were audio-recorded with consent, and non-verbal cues were noted in real time. Comprehensive field notes and reflexive comments were completed within two hours post-interview to prioritize participant accounts. A final five-minute individual probe assessed potential acquiescence bias from the joint interview format, with no notable response discrepancies found.
Data Analysis
Each interview was verbatim transcribed within 24 hours, with non-verbal cues annotated, and then independently checked within 48 hours. Guided by dyadic-coping theory, the analyst adhered to Colaizzi’s seven-step method.10 An a priori three-level codebook (main category, sub-category, operational definition) was constructed in NVivo 14 to ensure consistent coding (Table S1).The process involved: (1) familiarization; (2) extracting 376 significant statements; (3) code generation; (4) theme clustering; (5) thematic mapping; (6) member-checking (which confirmed plausibility); and (7) final refinement into three core themes and nine sub-themes.
Reflexivity
To mitigate potential bias and enhance interpretive rigor, a reflexive journal was maintained to document assumptions, emotional responses, and key analytical decisions. These reflections were regularly reviewed with the research team during the coding and thematic development processes. Through this ongoing, iterative dialogue, the team interrogated preliminary interpretations to ensure the findings were authentically grounded in participant data.
Results
Sample Characteristics
All 12 cohabiting couples (median marriage: 15 years) participated; eight had one child. Mean ages were 44 (patients) and 47 (spouses), with education levels from illiterate to university. While five patients and four spouses were employed, three patients had reduced work due to symptoms. Four families faced financial strain from treatment. Daily life was adapted to symptoms (eg, online shopping), and despite visible skin changes in eight patients, only two couples had discussed future care, highlighting a shared focus on maintaining normalcy.
Theme 1: Emotional Resonance Under Disease Shock
A profound shared “emotional freeze” descended on nearly every couple at diagnosis. Within this state, shock, role disruption, and fear circulated rapidly.11,12 Patients grappled with disorientation and dread of bodily change, while spouses, in attempting to be pillars of strength by suppressing their own turmoil, often found themselves emotionally depleted.13
P1:Although I had suspected lupus, when the doctor told me my anti-SM antibody was positive, my mind went blank — time seemed to stop, and I even forgot to breathe.
P5:I had never imagined that my skin would gradually tighten like an iron coat. When the doctor confirmed it was systemic sclerosis, I was overwhelmed with fear, convinced that my body would eventually turn to stone.
S8:She cried the whole way home. I did not say anything — I just turned off the music because even the sound of the GPS felt unbearable. At that moment, I realized that all the plans we had made for our future would have to be completely rewritten.
The diagnosis of CTDs compelled couples to renegotiate previously taken-for-granted family roles. Routine infusions, fatigue, and hand deformities meant that tasks symbolizing “good motherhood” or “competent fatherhood” had to be surrendered or relearned overnight, evoking a shared sense of inadequacy in both partners.14
P4:The kindergarten requested paper-cut decorations, but my fingers could no longer bend. When I handed the scissors to her father, my daughter insisted, “I want Mummy to do it.” Tears choked me—this illness has even stolen my ability to be the mother I wanted to be.
P3:We had planned to conceive this year, but high-dose steroids made pregnancy impossible. I deleted the pregnancy-tracking app—my quiet way of laying that dream to rest.
S4:I held her through the pain that denied her sleep, but it was futile—a futile gesture, like trying to put out a fire with a cup of water.
Emotional contagion operated at a visceral level: a single sob in the night or one burst of anger was enough to trigger matching physical reactions—hives, tremors, or vomiting—confirming that negative affect traveled through the dyad faster than the disease itself. Fluctuating symptoms, progressive loss of function, and prolonged steroid use kept both partners in a state of constant apprehension, where distress reverberated almost instantaneously between them.
P7:I woke at 3 a.m. in pain, and he woke with me. We lay there feeding each other’s fear until dawn—completely drained.
P8:My stiff fingers could not even pull-on socks. In a surge of frustration, I hurled them away, shouting that I was useless. Ten minutes later, his hand shook while shaving and he cut his lip—as though my despair had leapt straight into his body.
S11:After every clinic visit, she cries. The moment I hear her; my throat tightens and my stomach churns. I run to the bathroom and vomit, as if her lab results have poured directly into me.
These visceral accounts illustrate how emotional contagion permeates the dyad, confirming that negative affect spread between them more rapidly than the disease itself.13
Theme 2: Evolution of Dyadic Coping Strategies
Couples evolved task-oriented coping that enhanced mastery, but protective over-control periodically silenced the patient and eroded trust.
S9:I pre-sort her meds into the weekly pill organizer, and she does the hard part—getting her head in the right space. We have got our own battles to fight.
S11:I took a job with hardship pay to make ends meet; she had to step down from her career to focus on her health. We are like a partnership running a business, and the business is survival.
S2:She said that making it up six flights was like her own personal Everest. So, I carried her. Step by step, all the way up—just like I carried her heart when we first met.
Embodied Emotional Support
Effective support required the spouse to move beyond verbal reassurance to a state of physical, moment-to-moment synchrony. When this tangible form of empathy materialized, patients experienced their pain as shared—and therefore more bearable.
S7:I used to send her daily emojis and motivational texts, but she told me it felt superficial—like it was actually weakening our emotional connection.
P8:My fingers were too swollen to hold a book. He sat next to me reading “Ten Tips to Beat Rheumatism” out loud. It felt like an insult, a constant reminder that I am sick.
S4:She mentioned her joints were hurting, so I squeezed her hand and told her my wrist was aching too. Her tears stopped right then.
S6:I showed her pictures of people who had recovered, hoping to give her some hope. She said it felt like I was “showcasing medical cases.” I felt completely defeated.
P12:When I had night cramps, he laid his leg over mine, using his body weight to ease the spasm. That physical presence really did lessen the pain.
S3:One night at 2 a.m., I reached for her wrist and said, “I’m here—let’s hurt together.” She pulled away and snapped, “Easy for you to say. You’re not the one in pain.” I did not know whether to keep trying to comfort her or just back off.
Over-Controlling Dyadic Coping
When protective behavior shifted to unilateral control—exemplified by the manipulation of medical reports, unauthorized adjustment of dosages, or speaking on behalf of the patient—it resulted in a rapid diminishment of patient autonomy. The consequent erosion of trust increased the risk of medical and emotional relapse for the dyad.
S8:I altered the ANA titer in her lab report to allow her to enjoy the New Year’s holiday. My intention was to shield her from distress.
S10:I unilaterally reduced her steroid dosage to mitigate side effects. The subsequent disease flare resulted in significant distress for her and profound guilt for me.
P1:During family video calls, my partner consistently preempts my responses to inquiries about my health, assuring everyone that I am fine. This assumption of the spokesperson role has effectively silenced my own voice.
Theme 3: Mechanisms of Dyadic Resilience Co-Construction
Through joint meaning-making, micro-rituals and humor, partners converted CTDs from catastrophic threat to shared narrative material and built joint resilience.
Reconstructing the Illness Narrative
When couples began rewriting their medical story together, their chronic illness transformed. It was no longer just a diagnosis to endure but became shared material for creative exchange—ultimately strengthening the resilience of both partners.
P6:We see a drop in her C3 levels like a passing thunderstorm. If it bounces back, we get sunshine. So, we pack an umbrella instead of cursing the weather.
P11:The doctor told us, “No pregnancy this year.” So, we reframed it as our second honeymoon—a year to heal our bodies and rediscover each other.” S9: “I started an online series called” “Life with My Wife and SLE.” Now, with 30,000 followers, what began as an illness has become a platform for our shared growth.
P9:I could not seal the dumpling edges with my stiff fingers. He handed me a fork to crimp them, then laughed at our “limited-edition” shapes. In that moment, the cracked pastry was not a failure—it was just our special texture.
Trust Intensification
As caregiving demands intensified, patients grew more reliant on their spouses, who translated concern into consistent, small-scale actions. These daily rituals, often taken for granted, extended trust from the clinic into everyday life, weaving a strong safety net that steadily built what could be called “shared resilience.”
S3:We only see Dr. Gu; his computer has our complete records, so my wife never has to repeat blood work. She says each visit feels like catching up with an old neighbor.
P3:The steroids kept me sleepless until dawn, so he moved a mint plant to my bedside. Its scent helps me sleep. He waters it every morning—this small ritual soothes me and has become our unspoken promise.
S12:She could not hold the pen to sign her name. So, I wrote it first, then placed my hand beneath hers so she could trace the letters. When the nurse smiled at us, we both laughed—my hand had become her wrist joint.
P2:The steroids make me ravenous at night. I scratch his arm as a signal, and he tiptoes to the fridge, opens it just a crack, slips in a straw, and hands me the milk carton—all without turning on the light. It’s one seamless, muscle-memory motion.
Collaborative Future Reconstruction
Through humor and flexible problem-solving, couples navigated physical constraints as a team. This collaboration helped them reestablish daily rhythms and build a future that accommodates, but is not dominated by, their condition.15
S7:To help cover the cost of biologics, I deliver takeout after work, and she sells handmade crafts online. The illness forced us to diversify our income streams earlier than we had planned, but it actually helped us rebalance our budget.
P12:After I finished crying, my eyes were all puffy. He looked at me and said, “Looks like you got some free plastic surgery.” It made me laugh, and somehow, the joint pain did not feel quite as big.
S4:Her fingers were too swollen for her wedding ring. So, I threaded it onto a necklace for her to wear close to her heart. It’s the same symbol, just a different path; we will move it back to her finger when this flare is over.
P10:My stiff fingers could not manage buttons anymore. He suggested I switch to zip-up tops for now and switch back later. That’s when I realized I’d been fighting a button, not the disease itself—so I made the switch.
S1:We have practiced living with this condition long enough now. We will take it one hurdle at a time, and life will keep getting better.
Discussion
CTDs present particular relational challenges due to their often “invisible” symptoms—such as fatigue and pain—coupled with their fluctuating course and diagnostic complexity. These features frequently lead to significant discrepancies in illness perception between spouses, increasing the likelihood of misunderstanding and communication difficulties. Nevertheless, the distinct dyadic stress arising from these disease characteristics has not yet received adequate scholarly attention or systematic investigation. This study is designed to address this gap through a rigorous qualitative research approach.
This study examines how Chinese couples manage life with chronic time diseases and extends dyadic coping theory through a culturally situated framework that captures core dimensions, dynamic processes, and distinctive adaptation patterns including united resistance, sacrifice compensation, and detachment ambivalence. The findings provide theoretical foundations for developing couple based psychosocial interventions encompassing communication training, shared decision-making support, and coordinated stress management, while also enhancing clinical understanding of family dynamics to promote collaborative care and family centered approaches. Ultimately, this research aims to empower couple through evidence-based resources that foster mutual understanding, reduce relational strain, and strengthen shared efficacy and family resilience in chronic illness management. Our research primarily explores the following content:
Emotional Resonance and Dyadic Psychological Burden
Based on a CTDs-dyad sample, this study reveals that initial diagnosis triggers not only individual distress in female patients but also a synchronized emotional freeze within the couple unit. This extends Ogden’s concept of temporal disruption from an individual to an interactional level, suggesting that illness onset may induce a systemic emotional shock in the marital system.16
As an acute autoimmune condition, CTDs disrupt shared life plans—such as childbearing and career trajectories—creating a shared-loss dynamic between partners. Negative affect rapidly transmits through emotional contagion, manifesting somatically (eg, urticaria, tremors, retching) and revealing dyadic mind–body resonance.13 Visible role limitations in patients often trigger compensatory role-taking by spouses, increasing objective burden and precipitating role conflict.
Thus, CTDs expose both partners to intertwined psychological stress, resulting in circular amplification of negative emotions.17 Clinicians should assess emotional well-being in both partners from diagnosis onward and strengthen their confidence in managing stress together.18 Structured health education and brief interventions should help patients articulate emotions and practice illness communication, while training partners in active listening and perspective-taking.17 These combined strategies can improve dyadic coping and reduce catastrophic appraisals of CTDs.
Hazards of Joint Avoidance and Functionalized Coping
“Joint avoidance” emerged as a distinct strategy wherein couples minimized the visibility of CTDs to avoid external scrutiny. This shared silence provided short-term emotional stabilization but suppressed authentic expression, gradually eroding communication and fostering disengagement.19 By displacing stress into a latent psychological space, such avoidance increased long-term relational risks. Clinicians should therefore respect the couple’s need for privacy while using nonverbal micro-skills—such as mirroring body language and structured listening—to gently shift interactions from covert avoidance toward genuine emotional exchange.20 Similarly, dyadic role segmentation—dividing medical, domestic, and emotional labor—enhanced perceived control and helped integrate illness into daily life.21 However, excessive functionalization rendered support mechanical and risked emotional fatigue. The qualitative analysis suggests this null effect arises from a mialignement between partner’s intentions ans patient’s needs.This finding suggests that future interventions need to move beyond training specific skills and focus on aligning perceptions and expectations within the couple.18,20
Mechanisms Underpinning the “Null Effect” of Positive Dyadic Coping
Quantitative baseline data (n = 260) revealed that spouse-positive dyadic coping did not predict patient resilience (β = –0.013, P = 0.47), a finding consistent with Lucas H. et al.22 The qualitative analysis suggests this null effect arises from a misalignment between partners’ intentions and patients’ needs: partners focused on providing rapid emotional relief and minimizing risks, while patients prioritized having their autonomy validated and their emotions accurately acknowledged. When such “coping” takes the form of surrogate decision-making—such as adjusting medication, concealing test results, or speaking for the patient during medical visits—it marginalizes the patient’s role and undermines, rather than fosters, resilience. These findings indicate that resilience depends not merely on receiving care, but on preserving a sense of agency in managing one’s illness. When well-intentioned support is perceived as controlling, it can trigger a cycle of escalating strategies and emotional dissonance, resulting in the observed statistical null effect.23 Clinically, this underscores the need for healthcare providers to train spouses in empathy and need-recognition—using structured role-playing, simulated consultations, and iterative feedback—to transition from acting as proxies to serving as facilitators of patient empowerment, thereby restoring balanced and effective dyadic coping.
Mechanisms and Clinical Implications of Dyadic Resilience Co-Construction
CTDs extend beyond the individual patient, profoundly permeating the couple’s shared lifeworld by disrupting daily routines, plans, and intimate exchanges. Therefore, adaptation must be understood and addressed at the dyadic level. As shown by Castle et al, family communication and joint narrative construction significantly predict family satisfaction and health outcomes.24 In the context of CTDs, spouses engage in continuous information exchange to co-author an “our-illness story,” utilizing disease fluctuations as both core narrative material and momentum for meaning-making.25
Through metaphor and storytelling, couples reframed CTDs from a “life disruptor” into a “narrative collaborator,” transforming the illness into a catalyst for creativity, wisdom, and humor.26 This symbolic reconfiguration supplied shared scripts and representational resources for the co-construction of resilience. According to couple-resilience theory, trust forms the core of the dyadic system, where shared meaning-making, mutual vulnerability, and reciprocal support together build a robust joint resilience system.27 Supporting this, Turcotte et al demonstrated that frequent, low-intensity daily rituals generate “certainty resources”, which accumulate into stable relational resilience capital.28
In this study, couples facing CTDs did not interpret physical limitations, financial strain, or emotional distress as temporary interruptions to life. Instead, they activated anticipatory adaptation and humorous reframing, transforming anticipated losses into unexpectedly early gains.15,29 By proactively adjusting their cognitions and behaviors, they effectively reshaped their life trajectory and cultivated dyadic resilience.17
Conclusion
This study, examining partners of chronic pain patients, reveals a fundamental disparity in their perceptions of the illness: patients profoundly experience a loss of control and identity, while spouses focus more on practical risks. This leads to two coping patterns: “mutual avoidance” during pain episodes and “task division” in daily management. The core conflict lies in the tension between spousal support that often overlooks the patient’s emotional needs and over-assistance that undermines their autonomy—a dynamic further obscured by cultural norms of “endurance”. However, successfully coordinated couples transform the illness into an opportunity for emotional bonding. By co-narrating their shared experiences, they transcend the “patient-caregiver” dichotomy and become “co-authors” of their life’s meaning. In the future, we will focus on developing and validating clinical intervention communication protocols for partners of individuals with chronic pain. Furthermore, we will validate the findings from this study across other rare CTDs.
Acknowledgments
We would like to express our sincere gratitude to all the couples who participated in this study for sharing their personal experiences with openness and trust. Their contributions were essential to the depth and authenticity of this work. We also thank the nursing and medical staff at the Department of Rheumatology, Affiliated Hospital of Nantong University, for their support in participant recruitment and coordination.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the following funding sources: National Natural Science Foundation of China (grant number:82502178); Jiangsu Provincial Medical Key Discipline Cultivation Unit (grant number: JSDW202205); Jiangsu Provincial Research Hospital (grant number: YJXYY202204); Jiangsu Funding Program for Excellent Postdoctoral Talent; Natural Science Foundation of Jiangsu Province (grant number: BK20241838); Postgraduate Research & Practice Innovation Program of Jiangsu Province (KYCX24_3592); Science and technology Project of Nantong City (grant number: XNBG00031655).
Disclosure
The authors declare that they have no competing interests.
References
1. Osaze O, Olaosebikan HB, Yerima A, et al. Pattern of systemic lupus erythematosus in NIGERIA: a multicentre descriptive hospital-based study. Clin Rheumatol. 2023;42(10):2787–11. doi:10.1007/s10067-023-06672-y
2. Stull C, Sprow G, Werth VP. Cutaneous involvement in systemic lupus erythematosus: a review for the rheumatologist. J Rheumatol. 2023;50(1):27–35. doi:10.3899/jrheum.220089
3. Fine PG. Long-term consequences of chronic pain: mounting evidence for pain as a neurological disease and parallels with other chronic disease states. Pain Med. 2011;12(7):996–1004.
4. Zhang L, Zhu W, Wu B. Network analysis of depression and anxiety symptoms in Chinese rheumatoid arthritis patients. PeerJ. 2023;11e16356.
5. Siegel CH, Kleinman J, Barbhaiya M, et al. The psychosocial impact of undifferentiated connective tissue disease on patient health and well-being: a qualitative study. J Clin Rheumatol. 2022;28(2):e340–e7. doi:10.1097/RHU.0000000000001714
6. Tenório PJ, Katz L, Amorim MMR. Symptoms of anxiety and depression in women with gestational trophoblastic disease compared to women who had a miscarriage: a cross-sectional study. J Psychosomatic Obstetr Gynecol. 2023;44(1):2210747. doi:10.1080/0167482X.2023.2210747
7. Zhang T, Yan P, Wong CL, et al. Psychological resilience, dyadic coping, and dyadic adjustment in couples dealing with cervical cancer in Northwest China: a cross-sectional study. Eur J Oncol Nurs. 2025;74:102785. doi:10.1016/j.ejon.2025.102785
8. Ren L, Ahn S. Dyadic coping, resilience and post-traumatic growth in young and middle-aged coronary heart disease patients and their spousal caregivers: an actor–partner interdependence mediation model. J Adv Nurs. 2025. doi:10.1111/jan.16961
9. Bodenmann G. A systemic-transactional conceptualization of stress and coping in couples. Swiss J Psychol. 1995;54(1):34–49.
10. Morrow R, Rodriguez A, King N, editors.. Colaizzi’s Descriptive Phenomenological Method. 2015.
11. Herrando C, Constantinides E. Emotional contagion: a brief overview and future directions. Front Psychol. 2021;12:712606. doi:10.3389/fpsyg.2021.712606
12. Lim M, Carollo A, Bizzego A, Chen ASH, Esposito G. Synchrony within, synchrony without: establishing the link between interpersonal behavioural and brain-to-brain synchrony during role-play. R Soc Open Sci. 2024;11(9):240331. doi:10.1098/rsos.240331
13. Coutinho J, Oliveira‐Silva P, Fernandes E, et al. Psychophysiological synchrony during verbal interaction in romantic relationships. Fam Process. 2019;58(3):716–733. doi:10.1111/famp.12371
14. Charmaz K. The body, identity, and self: adapting to impairment. Sociologic Quarterly. 1995;36(4):657–680. doi:10.1111/j.1533-8525.1995.tb00459.x
15. Bartzou E, Tsiloni E, Mantzoukas S, Dragioti E, Gouva M. Humor and quality of life in adults with chronic diseases: a systematic review. Cureus. 2024;16(2):e55201.
16. Ogden R, Moore D, Piovesan A, Poole H. Distortions to the passage of time during chronic pain: a mixed method study. Eur J Pain. 2024;28(5):705–718. doi:10.1002/ejp.2211
17. Weitkamp K, Feger F, Landolt SA, Roth M, Bodenmann G. Dyadic coping in couples facing chronic physical illness: a systematic review. Front Psychol. 2021;12:722740.
18. Landolt SA, Weitkamp K, Roth M, Sisson NM, Bodenmann G. Dyadic coping and mental health in couples: a systematic review. Clin Psychol Rev. 2023;106:102344.
19. Helgeson VS, Jakubiak B, Seltman H, Hausmann L, Korytkowski M. Implicit and explicit communal coping in couples with recently diagnosed type 2 diabetes. J Soc Pers Relat. 2017;34(7):1099–1121. doi:10.1177/0265407516669604
20. Monirian F, Khodakarami B, Tapak L, Kimiaei Asadi F, Aghababaei S. The effect of couples coping enhancement counseling on stress and dyadic coping on infertile couples: a parallel randomized controlled trial study. Int J Fertil Steril. 2022;16(4):275–280. doi:10.22074/ijfs.2022.540919.1203
21. Helgeson VS, Jakubiak BK, Van Vleet M, Zajdel M. Communal Coping and adjustment to chronic illness: theory update and evidence. Pers Soc Psychol Rev. 2018;22(2):170–195.
22. Johnson MD, Anderson JR, Walker A, Wilcox A, Lewis VL, Robbins DC. Spousal overprotection is indirectly associated with poorer dietary adherence for patients with type 2 diabetes via diabetes distress when active engagement is low. Br J Health Psychol. 2015;20(2):360–373.
23. Cusimano C, Goodwin G. People regulate each other’s emotion regulation. 2020.
24. Castle KM, editor. Illness narratives of women with systemic lupus erythematosus and family communication: a mixed methods study.
25. Brailovski E, Vinet E, Pineau CA, et al. Marital status and age of systemic lupus erythematous diagnosis: the potential for differences related to sex and gender. Lupus Sci Med. 2019;6(1):e000325. doi:10.1136/lupus-2019-000325
26. Sween E. Using the Metaphor Of Teamwork In Narrative Couples Therapy. J Systemic Therapies. 2000;19(3):76–82. doi:10.1521/jsyt.2000.19.3.76
27. Xu F, Hilpert P, Randall AK, Li Q, Bodenmann G. Validation of the dyadic coping inventory with chinese couples: factorial structure, measurement invariance, and construct validity. Psychol Assess. 2016;28(8):e127–40. doi:10.1037/pas0000329
28. Turcotte K. Matters of the heart: the dyadic effects of psychological resilience and coping on psychological distress and relationship satisfaction among couples undergoing open heart surgery. 2020.
29. Hill J, Stokes L, Higgins K. Career Transitions Caused by chronic illness: a career construction perspective. Rehabil Res Policy Educ. 2022;36(4):292–306. doi:10.1891/RE-21-20
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025