Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Conversations Between Family Members and Physicians in Intensive Care Unit During Shared Decision-Making: A Qualitative Observational Study
Authors Lu Q, Ji J, Lu XY, Yin QH, Yang YQ
Received 28 February 2025
Accepted for publication 24 July 2025
Published 31 July 2025 Volume 2025:18 Pages 4535—4550
DOI https://doi.org/10.2147/JMDH.S525581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Laura Schwab-Reese
Qing Lu,1,* Juan Ji,2,* Xiao-yan Lu,1 Qiong-Hua Yin,1 Yi-Qun Yang3
1Department of Intensive Care Unit, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 2Department of Outpatient, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China; 3Department of Nursing, The First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yi-Qun Yang, Department of Nursing, The First Affiliated Hospital of Soochow University, 899 Pinghai Road, Gu Su Qu, Suzhou, Jiangsu, 215000, People’s Republic of China, Tel +86051213656245355, Email [email protected]
Introduction: It is necessary to understand the decision-making dynamics between physicians and families so as to help families better participate in shared decision-making.
Methods: A qualitative observational research was conducted. Conversations between physicians and families at a tertiary care hospital from July to December 2022 were audio-recorded. The families were those with critically ill patients lacking decision-making capacity in the intensive care unit. Data were analyzed using an inductive content analysis method.
Results: A total of 40 conversations were analyzed. There were 12, 15, and 13 decisions made on the day of hospital admission, when the patient’s condition changed, and during the end-of-life situation, respectively. In all decision-making stages, some sharing of information occurred between physicians and families. The degree of sharing differed depending on the decision-making context. In end-of-life situations, decision-making mostly involved families, which might only represent the values and preferences from family members but not patients.
Conclusion: Evidence of shared decision-making between physicians and family members was low. The levels of shared decision-making varied according to the context in which decisions were made. The shared decision-making between physicians and families might only represent the values and preferences from family members but not patients. Family members often faced decision-making difficulties and regrets.
Keywords: shared decision-making, critical illness, physician–patient relationship, family, intensive care unit
Introduction
Shared decision-making (SDM) refers to the process in which patients, their healthcare proxies, and medical staff work together to make clinical decisions based on the best available scientific evidence and the patients’ goals, values, and preferences.1 In 2016, the American College of Critical Care Medicine and the American Thoracic Association recommended that the SDM model be applied when making major treatment decisions on behalf of intensive care unit (ICU) patients.2 The SDM model has three stages: information exchange, negotiation, and decision-making.2 This model enables physicians to provide professional patient-centered recommendations to patients and family members while considering patient values, goals, and preferences.
However, some studies have reported inadequate implementation of SDM in clinics. In a recent study conducted in seven ICUs in the United States, fewer than 1 in 10 goals-of-care clinician-family meetings for critically ill neurological patients contained all SDM components.3 Moreover, Scheunemann et al4 found that physicians made treatment recommendations based on patients values and preferences in only 8.2% of situations in 13 ICUs from six hospitals in the United States. In China, families of patients in ICU often feel overwhelmed by the medical terms and often rely on physicians to make decisions.5 In addition, due to the collectivistic nature of Chinese culture, family members often play crucial role in medical decision making.6
In the ICU, SDM with family members can be more prevalent compared to other settings due to patients’ critical illness, often including unconsciousness and/or intubation. In a study by Cai et al,7 approximately 95% of patients were critically ill and often comatose or under sedation in the ICU.7 These patients are unable to communicate and express their wishes to physicians. Their families become spokespersons and decision-makers. The medical decisions made by physicians and patients’ families directly affect the prognosis and quality of life of patients. In general, their treatment decisions should follow the ethical principles of autonomy, non-harm, benefit and fairness.8 However, when there is a significant change in the patient’s condition or medical emergency, many physicians or even families are unaware of the patient’s wishes in advance and are likely not to follow the patient’s goals, values, and preferences during emergency resuscitations.9 Some families also feel extreme pressure when they have to share decision-making with physicians.10 In addition, the SDM process should change according to different SDM scenarios and situations.11 Family preferences during SDM can vary significantly.12 Some families choose to strengthen control in decision-making, while others hand over all controls to physicians.13 For example, due to unfamiliarity with the ICU environment, families may have less control in the early stages of their ICU stay.14 Furthermore, the different cultural and religious backgrounds of decision-makers can have a significant impact on the SDM process.15
Overall, SDM can be a critical process during patient management in ICU. However, there is limited understanding of SDM implementation in ICU in China. The purpose of this study was to understand the degree of SDM between physicians and families in the ICU setting.
Methods
Study Design
A qualitative observational study using qualitative content analysis. A qualitative study could enable us to gain an in-depth understanding of family member experience, perspectives, and contextual factors influencing their SDM process.
Settings and Participants
This qualitative study took place in the ICU of the First Affiliated Hospital of Soochow University, China, from July to December 2022. The hospital is a tertiary care hospital with a 16-bed ICU admitting over 300 critically ill patients annually. The physicians leading the conservation had completed specialized training in critical care medicine. Before data collection, all physicians received oral and written information and signed the informed consent.
A purposive sampling method was used. The research associates screened the medical records and looked for critically ill ICU patients who had no decision-making capacity, with an Acute Physiology Assessment and Chronic Health Evaluation II (APACHE II) score >25 and a predicted in-hospital mortality of 50% or greater. Their family members who were aged ≥18 years and in a close relationship to the critically ill patients as determined by the treating physicians and agreed by all family members were invited to the present study. Those family members who had difficulty in effectively expressing themselves, listening to others, or engaging in clear and respectful conversations were excluded. Patients in differing ages, sexes, disease severities, and length of ICU stays were included to increase the generalizability of our research results. Similarly, family members with differing ages, sexes, patient relationship types, and educational levels were included. The study design, process, purpose, and potential outcomes were fully explained to the family members by the research associates.
Our researchers mainly recorded three decision situations in a temporal order, the admission situation referred to the period immediately after ICU admission. The condition change situation referred to the period when the patient’s condition changed, which required invasive procedures, including tracheal intubation and hemodialysis. The end-of-life situation referred to the period when family members had to make a decision to continue resuscitation or withdraw life-support treatments. We did not include temporary meetings, one-on-one bedside conversations, or discussions held during daily family-centered rounds.16
Participant Recruitment and Consent Process
A member of the research team introduced the project to the eligible families and explained the definition of SDM and the purpose of the study. Families who were interested in participating were further informed about the process, duration, and potential outcomes of the study, and then asked for their oral and written consent. Family members were explained that, during the conversation, they could decline to answer any questions and could stop the conversations at any time.
Data Collection
After the informed consent process, a trained research associate followed the physician and patient’s family into a dedicated conference room in the ICU. A voice-recording device was placed in an inconspicuous place. After the meeting, the physicians and the patient’s family members completed the demography and baseline data. We collected patient information through a medical chart review. Research associates identified and transcribed the recordings verbatim within 48 hours.
Data Analysis
The qualitative content analysis was conducted by the inductive content analysis method that was applied previously.17
Four relevant articles on SDM were identified for coding physician and family conversations. First, Charles et al18 and Kon et al2 elaborated on the SDM framework in medical decision-making, which consists of three stages: information exchange, negotiation, and decision-making. Second, White et al19 developed a validated 10-element SDM instrument to assess the extent of SDM. In addition, there was a study that coded conversations between pediatricians and parents in the end-of-life decision.20 Based on these existing literatures, the following coding scheme was developed to accommodate all decision situations in the present study.
The framework of SDM consisted of three stages, which could occur consecutively or iteratively (Table 1). During these stages, the behaviors of physicians and families were defined. A researcher with qualitative research experience (JJ), a researcher with rich experience in the ICU (QL), an expert in the field of oncology care and hospice care (YY), and two researchers in the field of health communication (XL and QY) performed the research.
 |
Table 1 Three Stages of the Shared Decision-Making Process |
All researchers carefully read and re-read the transcripts while simultaneously listening to the audio recordings. The interactions between physicians and families were coded. In the initial draft of our coding scheme, we integrated the three analytical stages with codes for physician behaviors. After carefully reviewing the first ten transcripts, we further detailed the coding elements for physician behaviors and added the following adjustments to the coding scheme: 1) a code of interactions between physicians and families was added, 2) a code on a key decision step on “Description of nature of decision-making” according to White et al19 was added, and 3) integrated codes about emotions to suit all situations were added. Then, two researchers (MAV and BMG) conducted the transcript coding and re-coding for the first ten transcripts. Interrater reliability among all five coders was calculated on ten of the randomly selected transcripts, which were coded separately by these five coders. The inter-rater reliability (Cohen’s κ-statistic) was 0.81, indicating excellent interrater reliability. Any discrepancies in the code application were resolved through discussion. Subsequently, we complied a worksheet containing all dialogue segments for each applied code across all cases.
The extent of SDM was evaluated for the conversations in all stages. Coders iteratively refined the coding taxonomy using constant comparison of codes and achieved consensuses for all coded sections of the text. The extent of sharing was rated as rarely, sometimes, very often, and always. All qualitative analyses were performed in NVIVO 11 software (Lumivero, Denver, CO, USA). The Standards for Reporting Qualitative Research were followed.21
Ethical Considerations
The institutional ethics committee at the First Affiliated Hospital of Soochow University approved this study (approval number: No.059). The study was conducted in compliance with the Declaration of Helsinki. Every study participant had signed the informed consent, including the consent to publish anonymized responses/direct quotes. They were also explained that they could withdraw from the study at any time.
Results
Characteristics of Participants and the Decision-Making Process
One family member withdrew from the conversation due to emotional distress and was excluded from the data analysis. Finally, 40 decision-making conversations from 12 physicians and 30 family members to 25 patients were recorded. The characteristics of family members, physicians, and patients were listed in Tables 2–4, respectively. Most family members were females and spouses to the patients. There were more junior physicians involved in the current study. Most patients were elderly age with an ICU length of stay 1–3 weeks. There were 8, 10, and 7 patients in admission, condition changes, and end-of-life situations (total 25 unique patients, as some patients might have been involved in multiple decision types).
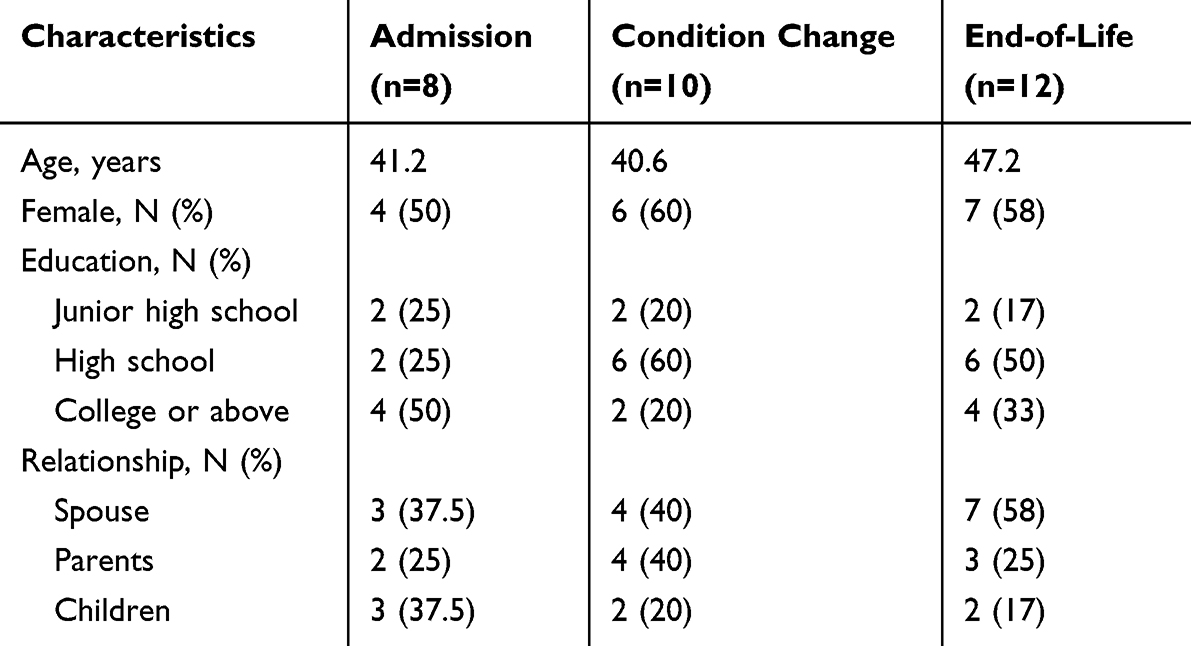 |
Table 2 Family Member Characteristics |
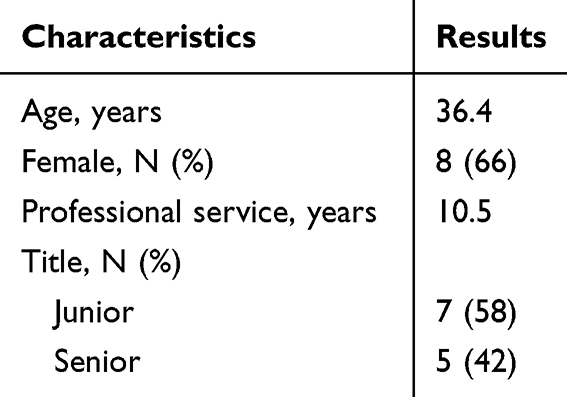 |
Table 3 Physician Characteristics |
 |
Table 4 Patient Demographics and Clinical Characteristics |
There were 12, 15, and 13 decisions made on the day of hospital admission, when the patient’s condition changed, and during the end-of-life situation, respectively (total 40 decisions). All the conversations were categorized as the followings: the admission situation as #1-#12, condition changed situation as #13-#27, end-of-life situation as #28-#40. The conversation #1, #15 and #38, conversation #6, #18 and #23, conversation #8, #19 and #31, conversation #9, #20 and #28, and conversation #11, #22 and #40 were from the same family member (at the admission, condition change, and end of life situations, respectively).
The SDM family meeting lasted an average of 26 minutes (range: 13–44 minutes). Tables 2 and 3 show the characteristics of the 40 family members and 12 physicians, while Table 4 lists patient demographics and clinical characteristics.
Communication Behaviors Throughout the Different Decision-Making Situations
The conversations occurred at three stages: information exchange, negotiation, and decision-making (Table 1). The characteristics of SDM focused on different points in different stages. In admission situations, physicians were busy evaluating patients and providing life-support interventions (Table 5, #2). In the condition-change situation, the physicians needed to negotiate with the family members to change the treatment plan (Table 6, #16 and #19). Decision-making was usually affected by the high cost of drugs and examinations, as well as the informed consent requirement for invasive procedures (Table 6, #16 and #29). In end-of-life situations, the main decision-making content was whether to withdraw life-support treatments. In this situation, family members, as the main decision-makers, often doubted their own decisions without knowing the patient’s prior desire and felt regret and self-blame (Table 7, #38).
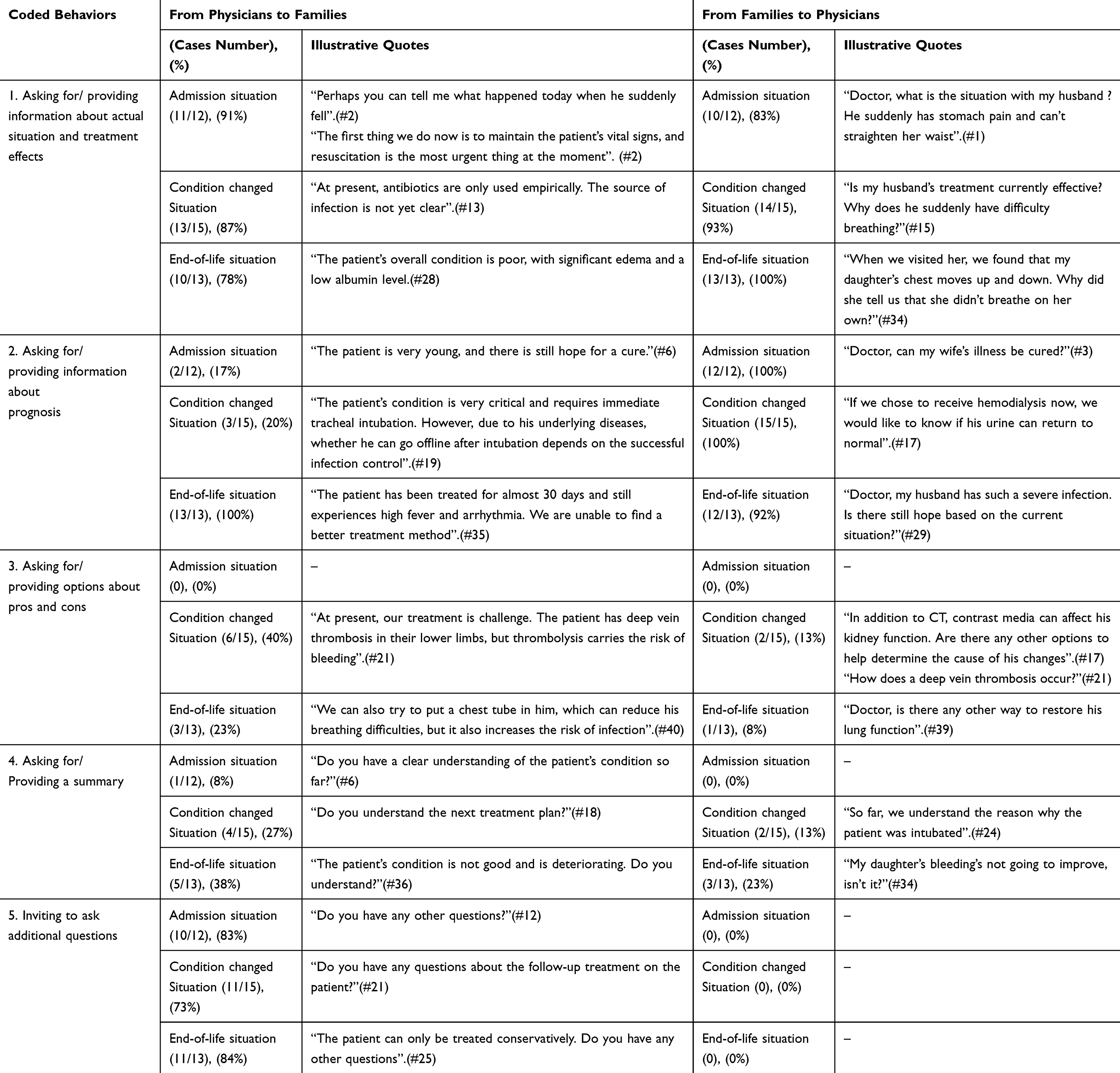 |
Table 5 Stage 1: Exchange of Information |
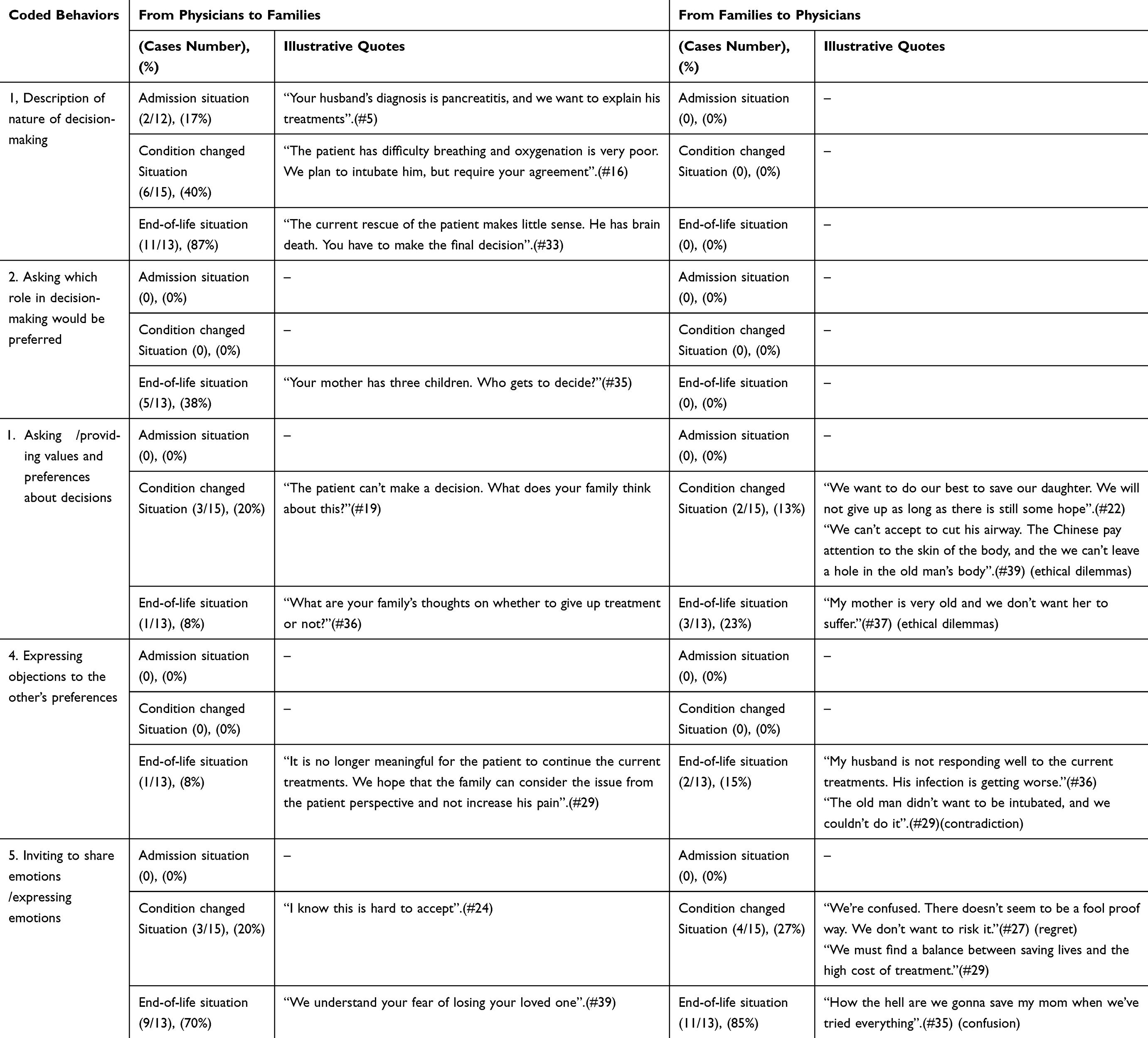 |
Table 6 Stage 2 Negotiation |
 |
Table 7 Stage 3: Reaching a Decision |
Stage 1: Information Exchange
In most recorded conversations, stage 1 was completed (Table 5). The physicians always started the conversations by asking families about the patients’ information (Table 5, #1 and #2). Families always provided information about decisions and asked for treatment effects (Table 5, #3). Families were always concerned about the patient prognosis in all decision situations, which was only clearly explained by the physicians in the end-of-life situations (Table 5, #25 and #29).
About a quarter of physicians explained the pros and cons of each decision in detail in the condition-change and end-of-life situations (Table 5, #21 and #40). However, physicians often used medical terminology in the process of explanation, which could limit the understanding of the family (Table 5, #21). In all decision situations, fewer than one-third of physicians and family members summarized the decision (Table 5, #6, #18, and #36). The pace of the physician–family conversations made it difficult to determine how well the family understood the decisions. At the end of the conversation, most physicians asked the families if they had any additional questions.
Stage 2: Negotiation
In the negotiation stage, many steps were missing (Table 6). At first, some physicians did not explicitly state that now was the time to make a decision, especially in admission situations (Table 6, #5). In line with this, physicians rarely seemed to ask about the family’s role in decision-making. Only in end-of-life decision situations did one physician ask about the family’s role in the decision-making (Table 6, #35). He explained the decision conversation and asked which role the family would play. Patient values and preferences are discussed to different degrees in different decision-making situations. In admission situations and condition-changed situations, physicians and families often ignored the patient values and preferences. In end-of-life decision-making situations, nearly a quarter of decisions were closely related to the patient values and preferences (Table 6, #36 and #37). Physicians often gave different treatment options and advised the family on these options, but the family still needed to make a final decision (Table 6, #29). Of course, end-of-life situations often involved contradictory and conflict-ridden decisions. Physicians and families did not always agree with each other (Table 6, #27 and #35). Some families wanted to continue the patient’s life, which was often determined meaningless by physicians (Table 6, #35). In addition, the emotions of family members were expressed to different degrees in different decisions. In admission situations, the focus of both sides was not on the emotion. In a condition-change situation, some family members were worried about the changes in the patient’s condition and also felt challenged in making a decision (Table 6, #29).
Stage 3: Reaching a Decision
Table 7 gives an overview of decision-making process in this stage. At first, physicians invited the families to make decisions, including decisions that might be affected by personal values, goals, and preferences, as well as limiting or withdrawing life-prolonging interventions (Table 7, #12, #16, and #33). These two types of decisions mainly focused on the latter two decision situations. In addition, most physicians sought the families’ consent in the SDM process. Physicians usually believed that the family was the final decision maker, since some treatments involved financial costs and might bring additional burdens to families (Table 7, #6 and #28). Some families also worried about the patient’s treatment effects and might have questions about the current treatment plan (Table 7, #39). In five cases, mainly end-of-life decisions, physicians and families could not reach an agreement (Table 7, #38 and #39). Families often required more time to make the final decision, which was agreed by the physicians. Obviously, withdrawing life-sustaining treatment brought ethical and moral problems to the families.
Extent of Shared Decision-Making
An overview of the extent of SDM is shown in Table 8. In all stages of the SDM process, there was some sharing of information between physicians and families. However, the extents of sharing were different in different decision situations. Families were most involved in the SDM in end-of-life situations but often expressed difficulties.
 |
Table 8 Extent of Shared Decision-Making (Adapted From Charles et al 1999 and White et al 2007) |
Discussion
The Method and Content are in Different Situations
In this study, we attempted to understand the extent to which family members of critically ill patients participated in SDM throughout the course of illness. We found that the method and content of the patients’ families’ participation in SDM varied according to different situations. In admission situations, due to the sudden notice of ICU admission, the family members were often in a state of pain, shock, and confusion, making it difficult for them to take responsibility for major decisions.22 Most family members actively requested or preferred physicians to make decisions. Physicians made decisions and took the lead in the decision. The decision content of this stage was mostly about value-neutral decisions that followed routine standard practice, such as vital sign monitoring, laboratory tests and medication administrations. The dialog focused primarily on the exchange of information. Obviously, it is also unethical to let families decide on the type and dosage of fluid supply to patients.2
On the basis of information sharing, physicians informed the families of the patient’s treatment plan and prognosis. In the condition-change situations, family members had been adapted to the ICU environment and medical procedures and could maintain a “calm and optimistic” attitude towards the patient’s condition and prognosis, which was consistent with a previous study report.23 When they faced complex decisions, they consulted physicians. The focus of the dialog mainly included all goals of care and preference-sensitive decisions, such as the decision for tracheotomy in patients who could not be weaned from mechanical ventilation.
In end-of-life situations, family members might have felt overwhelmed, anxious, denied, or defensive as well as remembering their past unpleasant decision-making experiences.24 All of these emotions can lead to decision-making difficulties. Some family members found it difficult to accept the patient’s current treatment results, fell into a state of self-blame and often felt conflicted and entangled with their own decisions. The focus of the dialog mainly included withholding or withdrawing life-sustaining treatment.
Families Participating in SDM Face Dilemmas
Consistent with previous research,24,25 we found that it was difficult to take patients’ preferences and values into account in any SDM process. Moreover, in terms of content, we found that these conservations often missed patients’ preferences and values, especially on an acceptable level of functioning and quality of life. Without this information, physicians could not make patient-centered recommendations, and families could not understand how treatments might reflect important patient values. In the end-of-life decision, influenced by the traditional Chinese culture of filial piety, some family members tried everything to save the lives of patients to avoid possible blame later on. It was difficult to give up treatment voluntarily. They often experience complex psychological activities and heavy mental burdens, leading to difficulties in SDM.26
From the physician’s perspective, families were the main decision-makers. “Family requirements” and “ineffective treatment” were the only reasons to give up the treatment. However, a previous study reported a low consistency of decision-making between patients and family members,27 suggesting that most family members were not aware of the patient’s preferences. Therefore, regardless of the different decision-making situations, patients’ values and preferences were often missed during SDM. It was difficult for physicians and family members to make decisions that best aligned with the patient’s “best interests”.
In our study, although most families expressed agreement with physicians, they often experienced decision-making dilemmas due to various internal psychological stresses and many external uncertainties. For instance, a previous study involving 748 ICU patients found that 54% of family members had mild regret and 19% had moderate regret for their previous decisions.28 Many uncertain factors, such as the patient’s condition, unclear information provided by physicians, and patient prognosis, could lead family members to face a dilemma during the SDM process. Among these factors, uncertainty about the patient’s prognosis was present throughout the entire SDM process. The emotions of family members fluctuated as the patient’s condition changed. High uncertainty regarding patient prognosis places a great challenge on patients’ families when participating in SDM. Our study also found that there was little active discussion to assess patient preferences and values, although the conversations between physicians and family members seemed to meet minimum standards of deliberation. Most families had a strong desire to be involved in the decision, especially when there was disagreement, but physicians were more focused on providing detailed information and did not actively invite the family to share the decision. Therefore, hospitals and ICU departments should provide more training and education to physicians and other medical staff to better understand the family members and patient requirements.
The Interprofessional SDM Model Should Be Suggested
Since it was difficult for individual physicians to make accurate judgments on the patient’s condition and prognosis, as well as provide treatment plans, we advise that decisions that can have a profound impact on patient outcomes, such as strengthening or reducing life support therapy, should be made under the interprofessional SDM model (IP-SDM).29 The hospital administrators and relevant authorities should coordinate and facilitate the interprofessional collaborations. This mode focuses on family meetings involving other ICU medical staff and medical providers from other departments, such as pharmacists, dieticians, ethics experts, and psychiatrists. It is necessary to understand the decision-making process of both physicians and families so as to help them better participate in SDM. Based on a comprehensive assessment and agreement on the patient’s disease status and prognosis, an SDM was formed to best suit the patient’s interests.30 The hospital should provide necessary training for medical staff to have better communication skills, listen to families, use plain language during conversation, and provide emotional support by arranging interdisciplinary family meetings with their families. The medical staff can also establish good relationships with family members to increase their trust and empowerment.31 In this mode, both physicians and family members can play a positive role, thereby reducing families’ decision-making difficulties and regrets.
Strengths and Limitations
We described the SDM process and explored the extent to which SDM was implemented. Future research could use our method to analyze audio recordings that cannot be easily obtained in a quantitative study. Compared with the quantitative study method, qualitative audio analysis can preserve tone, inflection, and emotion of the family members, and provide contextual understanding of their thoughts and motivations to reveal emergent themes that may not be anticipated by a quantitative study. The study limitation included its single-center research on ICU patients. Further research is required to validate our findings in other clinical settings, especially in countries other than China due to cultural differences. In China and certain Asian countries, Confucian principle, which emphasizes respect, duty, and care for one’s parents and elders, could push family members taking an active, or even leading, role in the SDM on behalf of the ill patients. Physicians might also discuss the medical situations with family members, rather than the patients, first, especially with grave prognosis. A practice rooted in Confucian values might also let the family members to ask physicians not to fully disclose the poor prognosis to the patients, with the belief to protect the patients from psychological distress.6 All of these could place special challenge in SDM between physicians and families in China, which requires further studies. In addition, we collected data on family meetings only during the daytime, thus missing data at night when a patient’s condition may change and require unplanned decision-making. We applied the audio recordings, but not video recordings, during the conversations, which might limit the analysis of non-verbal communication.
Conclusions
The conversations between physicians and families suggested that the SDM was low in the ICU in China. The levels of SDM varied according to the context in which the decisions were made. The shared decision-making between physicians and families might only represent the values and preferences from family members but not patients. Family members often faced decision-making difficulties and regrets. The hospital administrators and departments should provide necessary training and education for physicians and other ICU medical staff to improve their communications skills and encourage family participation in the SDM depending on the decision-making context, while not missing the values and preference from patients.
Ethical Approval
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Soochow University in 2020 (approval number: No.059).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Zisman-Ilani Y, Chmielowska M, Dixon L, et al. NICE shared decision making guidelines and mental health: challenges for research, practice and implementation. BJPsych Open. 2021:7. doi:10.1192/bjo.2021.1024
2. Kon AA, Davidson JE, Morrison W, Danis M, White DB. Shared decision-making in intensive care units. Executive summary of the American College of Critical Care Medicine and American Thoracic Society Policy Statement. Am J Respir Crit Care Med. 2016;193(12):1334–1336. doi:10.1164/rccm.201602-0269ED
3. Fleming V, Prasad A, Ge C, et al. Prevalence and predictors of shared decision-making in goals-of-care clinician-family meetings for critically ill neurologic patients: a multi-center mixed-methods study. Crit Care. 2023;27(1):403. doi:10.1186/s13054-023-04693-2
4. Scheunemann LP, Ernecoff NC, Buddadhumaruk P, et al. Clinician-family communication about patients’ values and preferences in intensive care units. JAMA Intern Med. 2019;179(5):676–684. doi:10.1001/jamainternmed.2019.0027
5. Wu FX, Zhuang YY, Chen XP. A current study on the participation of family members in decision-making of ICU patients. Clinical Meta. 2020;35(1):5.
6. Meng M, Li X, Zhao J, Hao Y. When western concept meets eastern culture: exploring the impact of Confucianism on shared decision-making in China. Asia Pac J Oncol Nurs. 2024;11(11):100586. doi:10.1016/j.apjon.2024.100586
7. Cai X, Robinson J, Muehlschlegel S, et al. Patient preferences and surrogate decision making in neuroscience intensive care units. Neurocrit Care. 2015;23(1):131–141. doi:10.1007/s12028-015-0149-2
8. Beauchamp C. Principles of Biomedical Ethics [M]. Li Lun.
9. Yu X, Tian K, Zhang X, Huang YQ. The research progress of end-of-life decisions among ICU patients. Chin Nurs Manage. 2017;17(02):271–275.
10. Yang X, Lin Y, Tang A, et al. Tough choices: the experience of family members of critically ill patients participating in ECMO treatment decision-making: a descriptive qualitative study. BMC Med Inform Decis Mak. 2025;25(1):65. doi:10.1186/s12911-025-02876-1
11. Montori VM, Ruissen MM, Hargraves IG, Brito JP, Kunneman M. Shared decision-making as a method of care. BMJ Evid Based Med. 2023;28(4):213–217. doi:10.1136/bmjebm-2022-112068
12. Scherr S, Reifegerste D, Arendt F, van Weert JCM, Alden DL. Family involvement in medical decision making in Europe and the United States: a replication and extension in five countries. Soc Sci Med. 2022;301:114932. doi:10.1016/j.socscimed.2022.114932
13. Dijkman BL, Luttik ML, Van der Wal-Huisman H, Paans W, van Leeuwen BL. Factors influencing family involvement in treatment decision-making for older patients with cancer: a scoping review. J Geriatr Oncol. 2022;13(4):391–397. doi:10.1016/j.jgo.2021.11.003
14. Shorofi SA, Jannati Y, Moghaddam HR, Yazdani-Charati J. Psychosocial needs of families of intensive care patients: perceptions of nurses and families. Niger Med J. 2016;57(1):10–18. doi:10.4103/0300-1652.180557
15. Hawley ST, Morris AM. Cultural challenges to engaging patients in shared decision making. Patient Educ Couns. 2017;100(1):18–24. doi:10.1016/j.pec.2016.07.008
16. Smith MA, Clayman ML, Frader J, et al. A descriptive study of decision-making conversations during pediatric intensive care unit family conferences. J Palliat Med. 2018;21(9):1290–1299. doi:10.1089/jpm.2017.0528
17. Kuckartz U. Qualitative Inhaltsanalyse: Methoden, Praxis, Computerunterstützung.
18. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–692. doi:10.1016/S0277-9536(96)00221-3
19. White DB, Braddock CH 3rd, Bereknyei S, Curtis JR. Toward shared decision making at the end of life in intensive care units: opportunities for improvement. Arch Intern Med. 2007;167(5):461–467. doi:10.1001/archinte.167.5.461
20. de Vos MA, Bos AP, Plötz FB, et al. Talking with parents about end-of-life decisions for their children. Pediatrics. 2015;135(2):e465–476. doi:10.1542/peds.2014-1903
21. Dossett LA, Kaji AH, Cochran A. SRQR and COREQ reporting guidelines for qualitative studies. JAMA Surg. 2021;156(9):875–876. doi:10.1001/jamasurg.2021.0525
22. Zhang M, XL Z. Research progress on post-intensive care syndrome-family and the corresponding interventions. Chin Nurs Manage. 2019;2019:1.
23. Cussen J, Van Scoy LJ, Scott AM, Tobiano G, Heyland DK. Shared decision-making in the intensive care unit requires more frequent and high-quality communication: a research critique. Aust Crit Care. 2020;33(5):480–483. doi:10.1016/j.aucc.2019.12.001
24. Bandini JI. Negotiating the ‘buffet’ of choice: advances in technology and end-of-life decision-making in the intensive care unit setting. Sociol Health Illn. 2020;42(4):877–891. doi:10.1111/1467-9566.13068
25. Kruser JM, Benjamin BT, Gordon EJ, et al. Patient and family engagement during treatment decisions in an icu: a discourse analysis of the electronic health record. Crit Care Med. 2019;47(6):784–791. doi:10.1097/CCM.0000000000003711
26. Wu F, Zhuang Y, Chen X. Systematic evaluation of qualitative researches on decision-making experience of family members of end-of-life patients in ICU. Chin Evid Based Nurs. 2020;6(06):490–497.
27. Sharma RK, Hughes MT, Nolan MT, et al. Family understanding of seriously-ill patient preferences for family involvement in healthcare decision making. J Gen Intern Med. 2011;26(8):881–886. doi:10.1007/s11606-011-1717-6
28. Andersen SK, Butler RA, Chang CH, Arnold R, Angus DC, White DB. Prevalence of long-term decision regret and associated risk factors in a large cohort of ICU surrogate decision makers. Crit Care. 2023;27(1):61. doi:10.1186/s13054-023-04332-w
29. Michalsen A, Long AC, DeKeyser Ganz F, et al. Interprofessional shared decision-making in the icu: a systematic review and recommendations from an expert panel. Crit Care Med. 2019;47(9):1258–1266. doi:10.1097/CCM.0000000000003870
30. Jones TW, Newsome AS, Smith SE, Forehand C. Interprofessional shared decision-making: who is at the table? Crit Care Med. 2020;48(2):e158–e159. doi:10.1097/CCM.0000000000004029
31. Au SS, Roze Des Ordons AL, Parsons Leigh J, et al. A multicenter observational study of family participation in ICU rounds. Crit Care Med. 2018;46(8):1255–1262. doi:10.1097/CCM.0000000000003193
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.