Back to Journals » Risk Management and Healthcare Policy » Volume 19
Convergence-Related Visual Symptoms Across Occupations with Varying Near Visual Demands: A Cross-Sectional Study with Implications for Healthcare Policy
Authors Aljohani S ![]()
Received 20 April 2026
Accepted for publication 6 July 2026
Published 17 July 2026 Volume 2026:19 618271
DOI https://doi.org/10.2147/RMHP.S618271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Saeed Aljohani
Department of Optometry, College of Applied Medical Sciences, Qassim University, Buraydah, Saudi Arabia
Correspondence: Saeed Aljohani, Department of Optometry, College of Applied Medical Sciences, Qassim University, Buraydah, Saudi Arabia, Email [email protected]
Purpose: Convergence insufficiency (CI) is a common binocular vision disorder associated with visual discomfort during near tasks, yet occupational differences in convergence-related symptoms remain poorly understood. Therefore, this study aimed to compare convergence-related symptom burden across eight occupational categories using the validated Arabic Convergence Insufficiency Symptom Survey (CISS) and to identify which occupational groups show the greatest symptom burden.
Methods: In this cross-sectional survey, adults aged 18 years or older from the Qassim region of Saudi Arabia completed the validated Arabic CISS. Participants represented eight occupational categories. Individuals with high refractive error or dry eye disease were excluded. Symptomatic status was defined as CISS ≥ 21. Differences in prevalence across occupations were assessed using chi-square tests. Multivariable logistic regression identified predictors after adjustment for age and gender.
Results: A total of 751 participants were included (mean age 28.9 ± 9.1 years; 56.3% male). The overall mean CISS score was 16.9 ± 10.7, and 268 participants (35.7%) met the symptomatic threshold. Although unadjusted prevalence did not differ significantly across occupations (χ2(7)= 7.63, p= 0.367), adjusted analysis showed higher odds of symptomatic CISS among technology professionals (OR 2.16, 95% CI 1.16– 4.02, p= 0.015), engineers (OR 2.11, 95% CI 1.13– 3.91, p= 0.018), and students (OR 2.03, 95% CI 1.08– 3.81, p= 0.029) compared with health professionals. Increasing age was associated with symptomatic status (OR 1.04 per year, p< 0.001), whereas gender was not significant (p= 0.158).
Conclusion: Convergence-related symptoms are common in working-age adults and show occupational variation after adjustment for demographic factors. Occupations with sustained near visual demands may warrant targeted vision screening and clinical evaluation for convergence insufficiency, supporting the integration of visual health into occupational health policies and preventive healthcare strategies.
Keywords: convergence insufficiency, prevention, healthcare policy, occupational visual demand, visual symptoms
Introduction
Convergence insufficiency (CI) is a binocular vision disorder characterized by difficulty in achieving or maintaining adequate ocular convergence during near tasks. It typically presents with objective clinical findings such as a receded near point of convergence (NPC), commonly defined as 6 cm or greater, reduced positive fusional vergence at near, and greater exophoria at near compared with distance.1,2 Convergence insufficiency is among the most prevalent binocular vision disorders, with population-based prevalence estimates ranging from 7–10% depending on the study population and diagnostic criteria employed.3–6
Clinically, individuals with CI often report symptoms including eye strain, blurred or fluctuating near vision, intermittent diplopia, difficulty sustaining visual attention during reading, and reduced reading speed.2,7–9 These symptoms can have meaningful functional implications, particularly in settings that require sustained near work.10 Despite its potential impact on visual comfort and task performance, CI remains underrecognized and is rarely assessed during routine occupational or primary eye care evaluations. From a healthcare systems perspective, unrecognized visual symptoms related to sustained near work may contribute to reduced productivity, impaired quality of life, and increased demand for clinical services.11–13
Work-related visual strain has become an increasingly recognized occupational health concern in modern workplaces. Studies indicate that approximately 50–90% of individuals engaged in intensive computer use report symptoms consistent with Computer Vision Syndrome or Digital Eye Strain.12,14 These conditions arise from multiple mechanisms, including tear film instability, accommodative stress, and prolonged postural demands.13 Within this spectrum of visual strain, convergence insufficiency represents a distinct and objectively measurable binocular vision dysfunction that has received comparatively little epidemiological attention in occupational populations.
Modern occupations vary considerably in their visual task demands. Technology professionals and office workers often perform prolonged near-distance tasks requiring sustained convergence, whereas healthcare professionals, educators, and engineering personnel typically experience more varied visual demands during the workday.15–17 This variation in occupational visual demands provides a natural framework to examine whether convergence-related symptoms differ across occupational groups. However, systematic investigation of occupational patterns in convergence insufficiency symptoms remains limited. While workplace-based interventions targeting computer-related eye strain have been developed and evaluated in specific occupational settings,18 comparable occupational-stratified evidence specifically for convergence-related symptoms, which are amenable to distinct interventions such as vergence and accommodative therapy beyond generic ergonomic advice, is lacking. This represents a specific gap in the occupational vision and healthcare policy literature that the present study seeks to address. Understanding these patterns could help guide workplace ergonomic strategies, inform occupational vision screening initiatives, and support the development of evidence-based occupational health policies.
The present study aimed to systematically characterize occupational and demographic variation in convergence-related symptom burden across eight professional categories using the Convergence Insufficiency Symptom Survey (CISS), a validated 15-item instrument with established reliability and discriminative validity across different populations.19,20 Based on the known relationship between sustained near visual work and visual fatigue, occupations with greater near visual demands were expected to show higher symptom burden. Secondary objectives included examining differences in symptom patterns by age and gender and identifying occupational subgroups with elevated symptom scores that may warrant further clinical evaluation.
By providing population-level data on convergence-related symptoms across occupational groups, this study contributes to occupational eye health surveillance and establishes a foundation for a subsequent prospective clinical validation study. In that planned phase, representative subsamples from selected occupations will undergo comprehensive binocular vision assessment to determine whether observed differences in symptom burden correspond to variations in the clinical prevalence of convergence insufficiency.
Materials and Methods
Study Design and Participants
This cross-sectional observational study examined the distribution of convergence-related symptoms across different occupational categories in a general adult population sample. Data were collected using a structured electronic survey administered to participants residing in the Qassim region of Saudi Arabia. A stratified quota sampling approach was employed to recruit approximately equal numbers of participants from each of the eight predefined occupational categories. Survey links were disseminated through targeted channels associated with each professional group, including profession-specific WhatsApp groups, institutional Email lists, and professional social media pages, in order to achieve the desired quota per group. This approach was chosen to achieve balanced group sizes suitable for between-group comparisons rather than to represent the true population distribution of occupational groups; as noted below, a formal a priori power calculation was not performed. Recruitment targeted adults representing diverse professional backgrounds in order to capture variation in occupational visual demands. The study was designed to characterize occupational patterns in convergence-related symptoms that may inform targeted screening and preventive healthcare strategies.
Eligible participants were adults aged 18 years or older who were currently engaged in one of the predefined occupational categories and who voluntarily agreed to participate in the study. Participants were required to have adequate cognitive ability and language comprehension to understand and complete the questionnaire independently. Because uncorrected refractive errors may alter accommodative demand and vergence responses and produce symptoms similar to convergence insufficiency,21 individuals reporting moderate or high refractive error (defined as spherical equivalent greater than +2.00 D hyperopia or less than −2.00 D myopia) were excluded. Participants with a self-reported history of dry eye disease, including those with a prior clinical diagnosis or current use of medications for dry eye management, were also excluded, as ocular surface disorders may independently contribute to visual discomfort symptoms.
Ethical Considerations
The study was approved by the Qassim University Institutional Review Board (IRB approval number 24–82-15) and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. All participants provided electronic informed consent before participation. Survey responses were collected anonymously and stored securely; no personally identifiable information was recorded.
Data Collection
After establishing the validity and reliability of the Arabic version of the Convergence Insufficiency Symptom Survey (CISS) in a previously published study,20 data collection was continued between October 2024 and April 2025 using the same validated instrument to recruit additional participants from the Qassim region. Participants were recruited through electronic dissemination of the survey link via X (formerly Twitter), WhatsApp, and email. To reduce the risk of non-genuine responses, the survey was disseminated through closed, professionally identifiable channels (eg, professional WhatsApp groups and institutional Email lists). Participants reported age, gender, and occupation, and stated occupational category were used as an internal consistency check. Nevertheless, formal identity verification was not performed, which is acknowledged as a limitation of the online survey design. Occupational categories were predefined to represent professions with differing patterns of visual task demands, particularly with respect to near visual work.
Assessment of Convergence-Related Symptoms
Convergence-related symptoms were assessed using the Convergence Insufficiency Symptom Survey (CISS), a validated 15-item questionnaire designed to quantify symptoms associated with convergence insufficiency and related binocular vision disorders. Each item is scored on a five-point Likert scale ranging from 0 (never) to 4 (always), yielding a total score from 0 to 60, with higher scores indicating greater symptom burden.22 The Arabic version of the CISS used in this study was previously translated, culturally adapted, and psychometrically validated in a published study.20
Consistent with established clinical thresholds, participants with a CISS score ≥21 were classified as having symptomatic convergence-related visual discomfort, a cutoff commonly used in adult populations to indicate clinically meaningful symptom levels.2
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 30.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for demographic variables and CISS scores. Continuous variables were summarized using means ± standard deviations as well as medians and interquartile ranges, while categorical variables were presented as frequencies and percentages.
Differences in mean CISS scores across occupational categories were evaluated using one-way analysis of variance (ANOVA). Because CISS scores were not normally distributed, Kruskal–Wallis tests were also performed as a non-parametric alternative.
Participants were further categorized according to symptomatic status using the CISS ≥21 cutoff, and differences in the prevalence of symptomatic individuals across occupational groups were assessed using chi-square tests.
To examine independent predictors of symptomatic status, multivariable logistic regression analysis was performed with CISS ≥21 as the binary outcome variable. Age and gender were included as covariates to adjust for potential confounding effects. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for each occupational category using health professionals as the reference group. Health professionals were selected a priori as the reference group because they represent a well-defined occupational group with mixed near and distance visual demands, alternating between close-range documentation, screen use, and distance patient examination, which positions them as a clinically relevant and theoretically intermediate baseline rather than an extreme on either end of the near visual demand spectrum. This a priori designation was consistent with the observed data, in which health professionals also had the lowest prevalence of symptomatic CISS among all eight occupational groups (27.1%), supporting their suitability as a baseline against which upward differences in other groups could be meaningfully compared. Statistical significance was defined as p < 0.05.
A formal a priori power calculation was not performed prior to data collection. The sample size was determined pragmatically based on feasibility and the stratified quota sampling approach. The relatively small group sizes (range 91–98 per group) may limit the statistical power to detect modest effect sizes, and the significant findings reported should be confirmed in larger prospective studies.
There were no missing data among the 751 participants included in the final analysis; all included participants provided complete responses for all CISS items and for age, gender, and occupational category. Multicollinearity was assessed using variance inflation factors (VIF). All occupational dummy predictors showed VIF values ranging from 1.39 to 2.21, indicating no meaningful multicollinearity among the primary predictors of interest. The covariate age showed a VIF of 6.67, reflecting an expected structural correlation between age and occupational group (educators: mean age 39.5 years; students: mean age 21.3 years), which remained below the threshold of 10.0 for severe multicollinearity. Gender showed a VIF of 2.57. Model fit was confirmed using the Hosmer-Lemeshow goodness-of-fit test (χ2 = 1.906, df = 8, p = 0.984). Examination of Cook’s distance identified five observations (0.7%) exceeding the conventional 4/n threshold; however, the maximum Cook’s distance was 0.0112, well below 1.0, indicating no observations with undue influence on the model estimates. Uncertainty in estimates was quantified using 95% confidence intervals, standard deviations, and p-values derived from the statistical models.
Results
Participant Characteristics
A total of 766 individuals completed the questionnaire. After excluding participants with self-reported high refractive error or a history of dry eye disease, 751 participants were included in the final analysis. Participants represented eight occupational categories, including students (n = 98), health professionals (n = 96), engineers (n = 96), educators (n = 94), arts and design professionals (n = 92), office workers (n = 92), lawyers (n = 92), and technology professionals (n = 91). The mean age of participants was 28.9 ± 9.1 years, with age distribution varying across occupational groups. Educators had the highest mean age (39.5 years), followed by office workers (31.6 years), whereas students had the lowest mean age (21.3 years). Overall, 423 participants (56.3%) were male and 328 (43.7%) were female. The overall mean CISS score was 16.9 ± 10.7. Baseline demographic characteristics and CISS score distributions across occupations are summarized in Table 1.
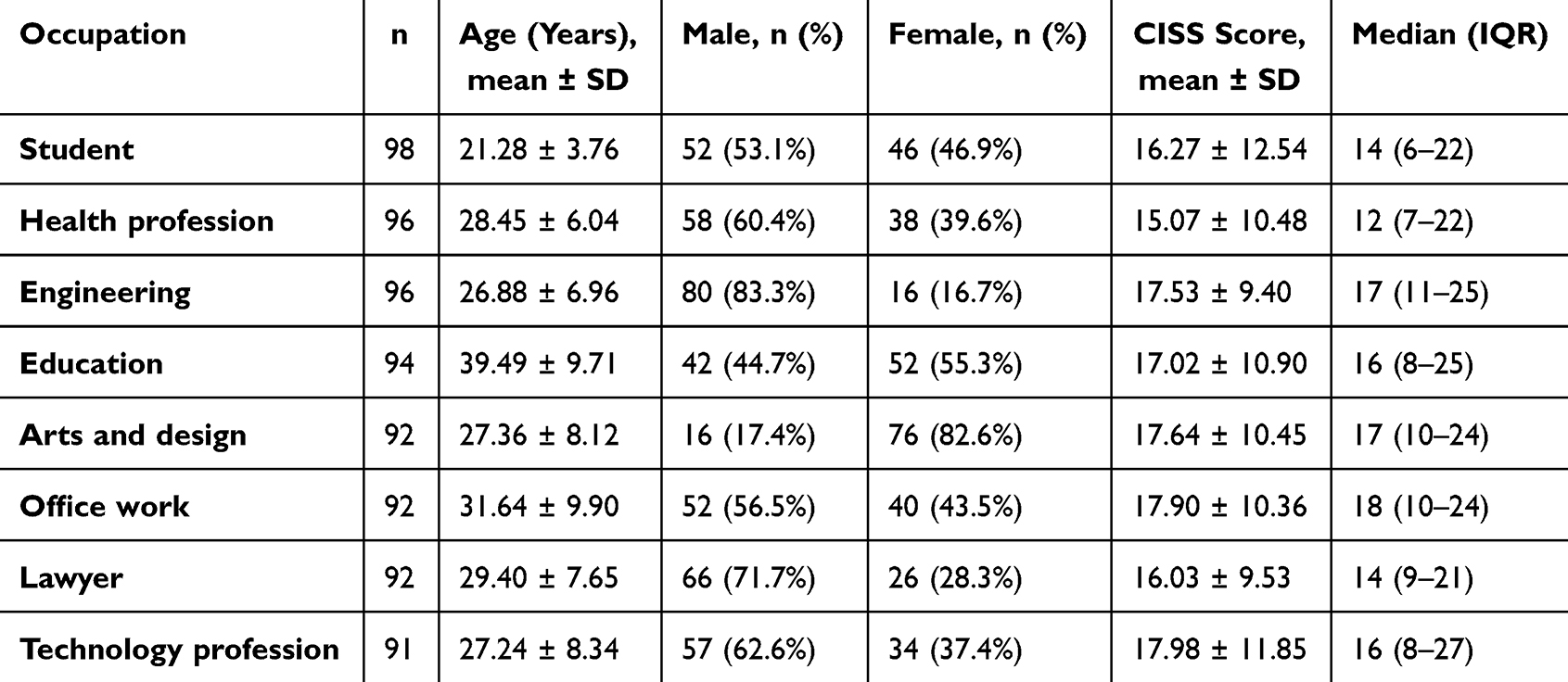 |
Table 1 Baseline Characteristics of Participants According to Occupation |
Prevalence of Symptomatic Convergence-Related Symptoms
The prevalence of symptomatic convergence insufficiency symptoms, defined as CISS ≥21, varied across occupational groups (Table 2). The highest proportions of symptomatic participants were observed among technology professionals, followed by engineers and arts and design professionals, whereas students and office workers also demonstrated relatively high symptom prevalence, and health professionals showed the lowest prevalence of symptomatic CISS. However, the overall comparison of symptomatic prevalence across occupational groups was not statistically significant in the unadjusted analysis (χ2 = 7.63, df = 7, p = 0.367).
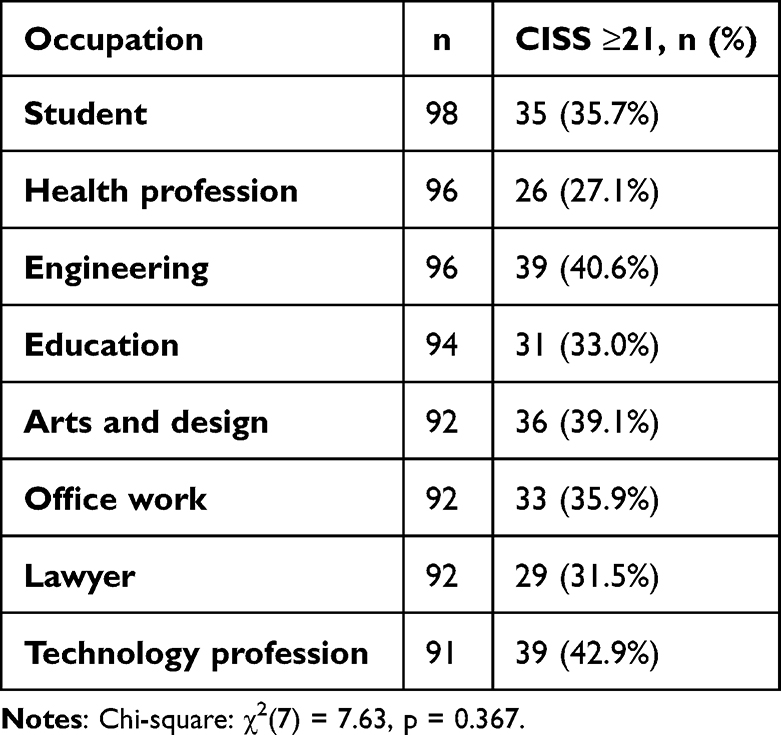 |
Table 2 Prevalence of Symptomatic Participants (CISS ≥21) by Occupation |
Predictors of Symptomatic CISS
Multivariable logistic regression analysis adjusted for age and gender is presented in Table 3, with the corresponding effect estimates illustrated in Figure 1. Compared with health professionals, technology professionals had significantly higher odds of symptomatic CISS (OR 2.16, 95% CI 1.16–4.02, p = 0.015). Engineers also demonstrated increased odds of symptomatic status (OR 2.11, 95% CI 1.13–3.91, p = 0.018), and students showed significantly higher odds as well (OR 2.03, 95% CI 1.08–3.81, p = 0.029). No statistically significant differences were observed for educators, arts and design professionals, office workers, or lawyers relative to the reference group. Overall, the occupational category block was significantly associated with symptomatic status after adjustment (p = 0.021).
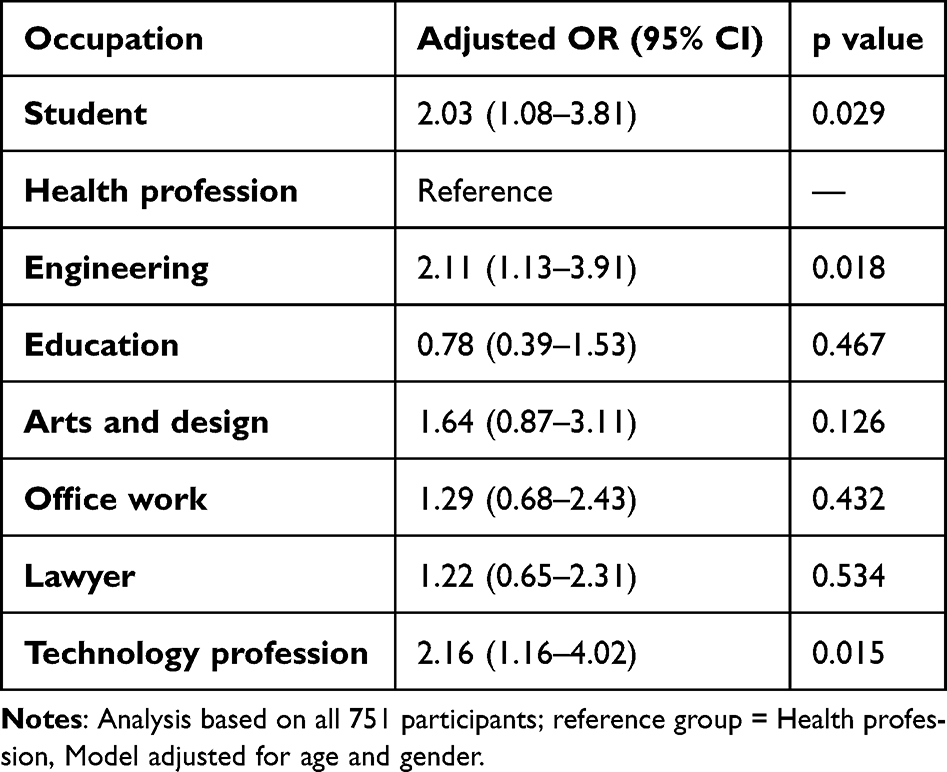 |
Table 3 Multivariable Logistic Regression Predicting Symptomatic CISS (≥21) |
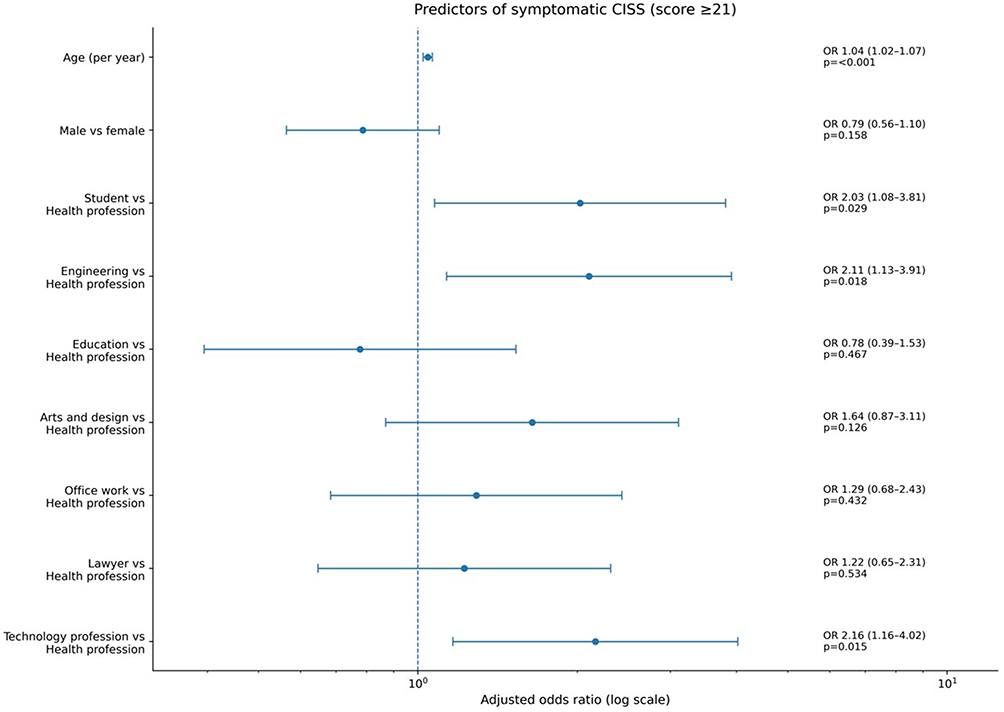 |
Figure 1 Forest plot showing adjusted odds ratios (ORs) and 95% confidence intervals for predictors of symptomatic convergence insufficiency symptoms (CISS ≥21). Estimates were derived from a multivariable logistic regression model adjusted for age and gender, with health professionals used as the reference occupational group. Values to the right of 1 indicate higher odds of symptomatic CISS. |
Age and Gender Effects
Age was independently associated with symptomatic convergence insufficiency symptoms. In the multivariable model, each additional year of age was associated with a modest but statistically significant increase in the odds of symptomatic CISS (OR 1.04, 95% CI 1.02–1.07, p < 0.001). In contrast, gender was not significantly associated with symptom status, although males showed lower odds of symptomatic CISS than females; this difference did not reach statistical significance (OR 0.79, 95% CI 0.56–1.10, p = 0.158). The predicted probability of symptomatic CISS increased progressively with age, as illustrated in Figure 2.
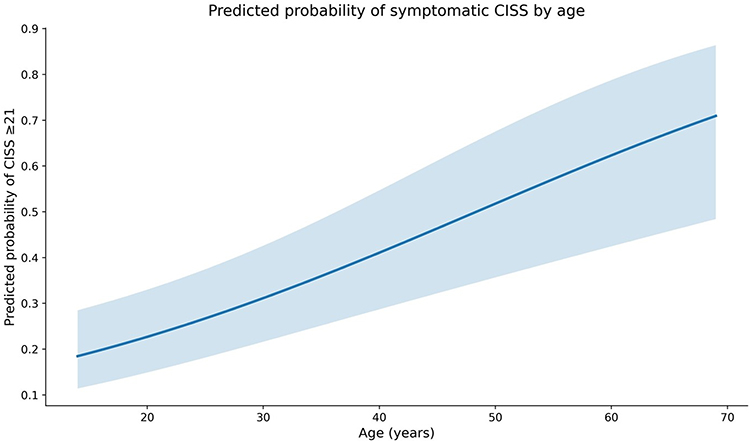 |
Figure 2 Predicted probability of symptomatic convergence insufficiency symptoms (CISS ≥21) across age based on the multivariable logistic regression model. The curve represents the estimated probability of symptomatic status with increasing age, while the shaded area indicates the 95% confidence interval. Predictions are shown for the reference profile used in the regression model. |
Discussion
The present study investigated occupational variation in convergence-related symptom burden in a large adult sample using the Convergence Insufficiency Symptom Survey (CISS). Several important findings emerged. First, convergence-related visual discomfort was common across occupational groups, with 268 of 751 participants (35.7%) exhibiting symptomatic scores (CISS ≥21). Second, although the unadjusted prevalence of symptomatic participants did not differ significantly across occupational categories (χ2 (7) = 7.63, p = 0.367), multivariable analysis revealed that certain occupational groups had significantly greater odds of symptomatic CISS after adjusting for age and gender. Specifically, technology professionals (OR 2.16, 95% CI 1.16–4.02, p = 0.015), engineers (OR 2.11, 95% CI 1.13–3.91, p = 0.018), and students (OR 2.03, 95% CI 1.08–3.81, p = 0.029) demonstrated significantly higher odds of symptomatic convergence-related complaints compared with health professionals. In addition, age was independently associated with symptomatic status (OR 1.04 per year, 95% CI 1.02–1.07, p < 0.001), whereas gender was not significantly associated with symptom burden (OR 0.79, 95% CI 0.56–1.10, p = 0.158). These findings underscore the importance of considering occupational visual demands when evaluating visual discomfort in modern digital work environments. These occupational differences in symptom burden may have relevance for occupational health surveillance, although as a symptom-level, cross-sectional finding, this association should be interpreted as preliminary rather than as evidence of a causal occupational exposure.
The overall symptom distribution observed in this cohort is consistent with previous epidemiological research demonstrating that binocular vision dysfunctions and convergence insufficiency symptoms are relatively common in adult populations.3,4,23–25 Population-based studies have reported prevalence estimates of binocular vision dysfunctions ranging from approximately 7–10% when defined by clinical diagnostic criteria, although higher proportions of individuals may report convergence-related symptoms when symptom-based screening instruments are used.3,5,23 The mean CISS score of 16.9 ± 10.7 observed in the present study is comparable to values reported in previous investigations examining visual discomfort in adult populations.4,6,19 Importantly, the CISS has been shown to possess strong reliability and discriminative validity for identifying individuals with clinically meaningful convergence-related symptoms.22 While symptom surveys cannot establish a definitive diagnosis of convergence insufficiency, they provide valuable population-level insight into the burden of binocular visual discomfort.
One of the most notable findings of the present study was the occupational pattern observed after adjustment for demographic factors. Technology professionals demonstrated the highest prevalence of symptomatic participants (42.9%) and had more than twofold higher odds of symptomatic CISS compared with health professionals (OR 2.16). Engineers showed a similarly elevated odds (40.6% prevalence; OR 2.11), while students also exhibited significantly increased odds of symptomatic status (35.7% prevalence; OR 2.03). These findings are consistent with evidence that occupations involving prolonged near visual tasks and intensive digital device use are associated with increased visual strain, with studies reporting that approximately 50–90% of individuals engaged in sustained computer work experience symptoms consistent with computer vision syndrome or digital eye strain.12,14 These symptoms arise from multiple mechanisms including tear film instability, accommodative stress, and prolonged convergence demand during near tasks. Although digital eye strain is multifactorial, sustained near fixation and prolonged convergence demand are recognized contributors to visual fatigue in screen-intensive environments.13,16 The elevated symptom burden observed among technology professionals and engineers in this study may therefore reflect the cumulative effects of sustained digital work and prolonged near visual activity, although this interpretation remains speculative given the absence of direct exposure measurements in this study.
The finding that students exhibited significantly higher odds of symptomatic CISS is also consistent with earlier investigations demonstrating increased prevalence of binocular vision dysfunctions among university populations engaged in intensive near visual tasks. García-Muñoz et al reported a substantial prevalence of accommodative and binocular dysfunctions in university students performing prolonged reading and screen-based activities.4 Academic environments often involve extended periods of near work under suboptimal ergonomic conditions, which may contribute to sustained vergence demand and visual fatigue. The present findings suggest that convergence-related symptoms may represent an underrecognized source of visual discomfort in educational settings.
In contrast, several occupational groups did not demonstrate significantly increased odds of symptomatic status after adjustment. Educators, office workers, lawyers, and arts and design professionals showed odds ratios that did not differ significantly from the reference group of health professionals. This may reflect the heterogeneous visual demands present in these professions, though this interpretation is speculative in the absence of direct occupational exposure data. For example, educators often alternate between near and distance visual tasks throughout the workday, which may reduce sustained convergence load compared with occupations dominated by continuous screen-based work. However, without objective measures of task distance, screen time, or vergence demand across occupations, this explanation cannot be confirmed. Previous occupational vision research has suggested that variability in task distance, visual posture, and workplace ergonomics can influence the degree of visual fatigue experienced in occupational environments.13
Age was independently associated with symptomatic convergence-related complaints in the present study, with each additional year associated with approximately 4% higher odds of symptomatic CISS (OR 1.04). Although convergence insufficiency is often discussed in pediatric populations, several studies have documented age-related changes in vergence and accommodative function that may contribute to increased near visual discomfort in adults.1,2 The modest but statistically significant age effect observed in the present analysis may therefore reflect gradual changes in binocular visual efficiency or cumulative visual demand over time. In contrast, gender was not significantly associated with symptomatic status after adjustment for occupational category and age. Although males showed somewhat lower odds of symptomatic CISS compared with females (OR 0.79), this difference was not statistically significant (p = 0.158), suggesting that occupational visual demands and individual visual function likely play a larger role in symptom burden than sex-related differences.
Several limitations should be considered when interpreting these findings. First, the study relied on a symptom-based screening instrument rather than objective clinical measures of binocular vision function. While the CISS has demonstrated strong reliability and diagnostic utility in identifying individuals with convergence insufficiency symptoms,22 symptom scores alone cannot establish a definitive clinical diagnosis. Second, the cross-sectional design prevents causal inference regarding the relationship between occupational visual demands and symptom development. Third, occupational categories were defined broadly and did not capture detailed information regarding daily screen time, task duration, viewing distance, or workplace ergonomics, all of which may influence visual fatigue. Fourth, the regression model adjusted only for age and gender; other potential confounders including daily screen time, cumulative near-work duration, optical correction status, working distance, rest break frequency, sleep quality, and prior ocular history were not collected and could not be accounted for; the multivariable results should therefore be interpreted as preliminary and exploratory. Fifth, the exclusion of participants with refractive error or dry eye disease was based on self-report rather than clinical verification, which may have led to incomplete exclusion of these potential confounders of visual symptoms. Finally, the stratified quota sampling approach, while designed to achieve balanced group sizes for between-group comparisons, limits the generalizability of prevalence estimates to the broader population, and the online survey design introduces the possibility of selection bias despite the steps taken to ensure response authenticity.
The present findings should be interpreted as preliminary symptom-level evidence. The absence of objective binocular vision measurements, such as near point of convergence and positive fusional vergence, and the lack of detailed occupational exposure data preclude definitive conclusions about the clinical prevalence of convergence insufficiency across occupations. Future validation through prospective clinical studies incorporating objective binocular assessments in representative subsamples from occupational groups with elevated symptom burden is needed to determine whether the observed symptom differences correspond to objective binocular dysfunction.
Technology professionals, engineers, and students demonstrated significantly higher odds of symptomatic visual discomfort compared with health professionals, an occupation-stratified finding that may be informative for occupational health surveillance. These findings have important implications for healthcare policy and occupational health practice. Integrating vision screening into workplace health programs, particularly in occupations with high digital exposure, may support early identification of individuals who could benefit from binocular vision evaluation. Preventive strategies, including structured visual breaks, awareness initiatives, and clear referral pathways for clinical evaluation, may help reduce symptom burden and improve workplace productivity.
Implications for Healthcare Policy and Occupational Health Practice
This study also offers a specific contribution to healthcare policy and occupational health practice. Workplace-based interventions targeting eye strain have previously demonstrated value in occupational settings; for example, a participatory eye care program developed for staff computer users in Thailand, informed by structured input from workplace stakeholders, was shown to improve eye care knowledge, attitudes, and practices while reducing eye strain symptoms among employees.18 This precedent supports the feasibility of structured, occupation-specific vision interventions as a component of workplace health policy. Symptom-survey methodology comparable to that used in the present study has similarly been applied to characterize digital eye strain burden in screen-exposed populations and to inform practical recommendations for safer digital device use.26 Convergence-related symptoms, captured specifically by the CISS, represent a distinct subset of visual discomfort that may be amenable to targeted interventions such as vergence and accommodative therapy, in addition to generic ergonomic advice. The present findings, identifying technology professionals, engineers, and students as occupational groups with elevated symptom burden, could inform occupation-stratified vision surveillance approaches that prioritize periodic CISS-based screening and referral pathways for these specific groups, rather than uniform screening applied without regard to occupational profile. Such targeted approaches may represent a more efficient allocation of occupational vision-screening resources than undifferentiated programs; however, prospective evaluation of any such program, including its cost-effectiveness and impact on referral and treatment uptake, would be needed before implementation could be recommended.
Conclusion
This study highlights differences in convergence-related visual symptoms across occupational groups and identifies specific populations with elevated symptom burden in modern digital work environments. These findings are based on a validated symptom survey and should be interpreted as preliminary symptom-level evidence rather than clinical diagnoses of convergence insufficiency. The results suggest that sustained near visual demands may be an underrecognized contributor to occupational visual discomfort. Incorporating vision screening into workplace health programs could support earlier detection and timely intervention. Future studies should incorporate objective clinical binocular vision assessments, including near point of convergence and positive fusional vergence measurements, alongside detailed quantification of occupational near-work and screen exposure, to better characterize occupational variation in convergence-related symptoms and establish evidence-based screening thresholds.
EQUATOR Network Checklist
This manuscript was prepared in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies (Supplementary File 1).
AI Statement
The author used Grammarly (Grammarly Inc., USA) for grammar correction and language refinement. No generative AI tools were used in study design, data analysis, interpretation, or generation of scientific content. The author takes full responsibility for the integrity and accuracy of the paper.
Data Sharing Statement
Data and materials used in this study are available and can be shared by the principal investigator upon reasonable request.
Acknowledgments
The Researcher would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2026). The researcher also would like to thank all Doctor of Optometry (OD) students at Qassim University who assisted with data collection.
Funding
This research did not receive external financial support for study design, data collection, analysis, or interpretation. The article processing charge for publication was covered by the Deanship of Graduate Studies and Scientific Research at Qassim University (QU-APC-2026).
Disclosure
The author of this study reports support from Qassim University for this paper and declares no other conflicts of interest.
References
1. Trieu LH, Lavrich JB. Current concepts in convergence insufficiency. Curr Opin Ophthalmol. 2018;29(5):401–11. doi:10.1097/icu.0000000000000502
2. Gantz L, Stiebel-Kalish H. Convergence insufficiency: review of clinical diagnostic signs. J Optom. 2022;15(4):256–270. doi:10.1016/j.optom.2021.11.002
3. Jorge J, Diaz-Rey A, Lira M. Prevalence of binocular vision dysfunctions in professional football players. Clin Exp Optom. 2022;105(8):853–859. doi:10.1080/08164622.2021.2002667
4. García-Muñoz Á, Carbonell-Bonete S, Cantó-Cerdán M, Cacho-Martínez P. Accommodative and binocular dysfunctions: prevalence in a randomised sample of university students. Clin Exp Optom. 2016;99(4):313–321. doi:10.1111/cxo.12376
5. Chen Y. The prevalence of binocular vision dysfunctions in Taiwanese non-presbyopia adults. Invest Ophthalmol Visual Sci. 2022;63(7):2572–F0526.
6. Franco S, Moreira A, Fernandes A, Baptista A. Accommodative and binocular vision dysfunctions in a Portuguese clinical population. J Optometry. 2022;15(4):271–277. doi:10.1016/j.optom.2021.10.002
7. Borsting E, Rouse MW, De Land PN. Prospective comparison of convergence insufficiency and normal binocular children on CIRS symptom surveys. Convergence Insufficiency and Reading Study (CIRS) group. Optom Vis Sci. 1999;76(4):221–228. doi:10.1097/00006324-199904000-00025
8. Alvarez TL, Scheiman M, Santos EM, Yaramothu C, d’Antonio-Bertagnolli JV. Convergence insufficiency neuro-mechanism in adult population study randomized clinical trial: clinical outcome results. Optom Vis Sci. 2020;97(12):1061–1069. doi:10.1097/opx.0000000000001606
9. Scheiman M, Mitchell GL, Cotter SA, et al. Convergence Insufficiency Treatment Trial - Attention and Reading Trial (CITT-ART): design and methods. Vis Dev Rehabil. 2015;1(3):214–228.
10. Scheiman M, Rouse M, Kulp MT, Cotter S, Hertle R, Mitchell GL. Treatment of convergence insufficiency in childhood: a current perspective. Optom Vis Sci. 2009;86(5):420–428. doi:10.1097/OPX.0b013e31819fa712
11. Aljohani S, Alrasheed SH, Alrashidi K, Alharbi A, Alghamdi S, Aljhni M. Impact of adherence to American Optometric Association guidelines on computer vision syndrome and dry eye. computer vision syndrome; dry eye diseases; American Optometric Association; students; symptom; quality of life. Afr Vision Eye Health. 2024;83(1). doi:10.4102/aveh.v83i1.966
12. Kahal F, Al Darra A, Torbey A. Computer vision syndrome: a comprehensive literature review. Future Sci OA. 2025;11(1):2476923. doi:10.1080/20565623.2025.2476923
13. Pavel IA, Bogdanici CM, Donica VC, et al. Computer vision syndrome: an ophthalmic pathology of the modern era. Medicina. 2023;59(2). doi:10.3390/medicina59020412
14. American Optometric Association. Computer vision syndrome. Available from: https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/computer-vision-syndrome?sso=y.
15. Albarrán Morillo C, Suárez-Pérez JF, Demichela M, Camargo Salinas MA, Miranda Arandia NY. Monitoring visual fatigue with eye tracking in a pharmaceutical packing area. Sensors. 2025;25(18):5702. doi:10.3390/s25185702
16. Anshel JR. Visual Ergonomics in the Workplace. AAOHN J. 2007;55(10):414–420. doi:10.1177/216507990705501004
17. Ferguson DA, Major G, Keldoulis T. Vision at work visual defect and the visual demand of tasks. Appl Ergon. 1974;5(2):84–93. doi:10.1016/0003-6870(74)90084-2
18. Lertwisuttipaiboon S, Pumpaibool T, Neeser KJ, Kasetsuwan N. Effectiveness of a participatory eye care program in reducing eye strain among staff computer users in Thailand. Risk Manag Healthc Policy. 2017;10:71–80. doi:10.2147/RMHP.S134940
19. Rouse MW, Borsting EJ, Mitchell GL, et al. Validity and reliability of the revised convergence insufficiency symptom survey in adults. Ophthalmic Physiol Opt. 2004;24(5):384–390. doi:10.1111/j.1475-1313.2004.00202.x
20. Aljohani S, Alnawmasi MM. Cross-cultural adaptation and validation of the Arabic convergence insufficiency symptom survey (Arab-CISS) in Saudi Arabia. British J Visual Impairment. 2024;02646196241261620. doi:10.1177/02646196241261620
21. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders.
22. Rouse M, Borsting E, Mitchell GL, et al. Validity of the convergence insufficiency symptom survey: a confirmatory study. Optom Vis Sci. 2009;86(4):357–363. doi:10.1097/OPX.0b013e3181989252
23. Shrestha P, Kaiti R. Non-strabismic binocular vision dysfunction among the medical students of a teaching hospital: a Descriptive Cross-sectional Study. JNMA J Nepal Med Assoc. 2022;60(252):693–696. doi:10.31729/jnma.7615
24. Alrasheed SH, Osman TM, Aljohani S, Alshammeri S. Clinical features of Sudanese patients presenting with binocular vision anomalies: a hospital-based study. J Med Life. 2023;16(8):1251–1257. doi:10.25122/jml-2023-0132
25. Uwimana A, Ma C, Ma X. Concurrent rising of dry eye and eye strain symptoms among university students during the COVID-19 pandemic era: a cross-sectional study. Risk Manag Healthc Policy. 2022;15:2311–2322. doi:10.2147/RMHP.S388331
26. Bhowmick A, Kumar PP, Ratra D. Frequency of non-strabismic binocular vision anomalies among optometrists in a tertiary eye care center in Southern India. Indian J Occup Environ Med. 2024;28(2):138–142. doi:10.4103/ijoem.ijoem_243_23
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.