Back to Journals » Nature and Science of Sleep » Volume 14
Convergence Between the Child Behavior Checklist Sleep Items, Actigraphy and Other Sleep Measures Among Children of Parents with Alcoholic Disorders and Controls
Authors Wong MM, Brower KJ, Conroy DA, Craun EA
Received 24 June 2021
Accepted for publication 12 September 2022
Published 29 November 2022 Volume 2022:14 Pages 2107—2121
DOI https://doi.org/10.2147/NSS.S324002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Maria M Wong,1 Kirk J Brower,2 Deirdre A Conroy,2 Elizabeth A Craun1
1Department of Psychology, Idaho State University, Pocatello, ID, 83209, USA; 2Department of Psychiatry, University of Michigan, Ann Arbor, MI, 48109, USA
Correspondence: Maria M Wong, Department of Psychology, Idaho State University, Pocatello, ID, 83209, USA, Tel +1 208 282 2752, Fax +1 208-282-4832, Email [email protected]
Purpose: The Child Behavior Checklist (CBCL) is a widely used instrument of children psychosocial functioning. CBCL sleep items have been used in both clinical settings and research. To date, few empirical studies have examined the relationships between CBCL sleep items and other sleep measures such as actigraphy and validated sleep questionnaires. This study extends the literature by examining these relationships in a group of children of parents with an alcohol use disorder (COAs) and matched controls.
Participants and Methods: Two hundred and forty-eight children aged 8– 12 (48% COAs; 50% girls; Mean age =10.37 (Standard deviation = 1.47)), participated in this study. Data presented here were taken from Time 1 of a larger prospective study designed to understand the relationship between sleep and alcohol use. All participants were naïve to alcohol and other illicit drugs. Parents completed the Achenbach CBCL and the Pediatric Sleep Questionnaire (PSQ). Participants wore an actigraph watch on their non-dominant wrists for one week and filled out the Youth Self-Report (YSR).
Results: Multiple regression analyses showed that CBCL sleep items (eg, “trouble sleeping”) correlated with related actigraphy (eg, shorter total sleep time and longer sleep onset latency) and Pediatrics Sleep Questionnaire (PSQ) items (eg, sleep difficulties and daytime sleepiness). Logistic regression analyses indicated that CBCL items (eg, “trouble sleeping) predicted similar items in the Youth Self Report (YSR) (eg, trouble sleeping). Structural equation modeling analyses showed that the latent variable “CBCL sleep” correlated significantly with the latent variables of actigraphy (r = − 0.54, p < 0.001), PSQ (r = 0.93, p < 0.001) and YSR (r = 0.38, p < 0.01). These associations were largely the same for COAs and controls.
Conclusion: CBCL items were significantly associated with actigraphy variables, a validated sleep measure (PSQ) and youth report of sleep for both COAs and non-COAs.
Keywords: sleep measures, actigraph, parental ratings, Youth Self-Report, children
Plain Language Summary
We examined the associations between sleep items of the Child Behavior Checklist for Ages 6–18 (CBCL) with other sleep measures in a group of children of parents with alcoholic disorders (COAs) and controls. The CBCL collects parental ratings on children’s competence, psychosocial functioning and behavioral problems. It is commonly used in both clinical and research settings. In spite of its popularity, few studies have investigated the validity of the CBCL sleep items and its relationships with other validated sleep measures. Two hundred and forty-eight children aged 8–12 (48% COAs; 50% girls; mean age = 10.37) participated in this study. Parents completed the Achenbach CBCL and the Pediatric Sleep Questionnaire (PSQ). Participants wore an actigraph watch on their non-dominant wrists for one week and filled out the Youth Self-Report (YSR). CBCL items were significantly associated with actigraphy variables, a validated sleep measure (PSQ) and youth report of sleep for both COAs and non-COAs. These associations were largely the same for COAs and controls.
Introduction
The Child Behavior Checklist for Ages 6–18 (CBCL)1 collects parental ratings on children’s competence, psychosocial functioning and behavioral problems. It is commonly used in both clinical and research settings. One study found that it is the most widely used instrument among pediatric psychologists in the US, as well as the most cited instrument in studies published by the Journal of Pediatric Psychology between 1976 and 2006.2 In spite of its popularity, few studies have investigated the validity of the CBCL sleep items and its relationships with other validated sleep measures.3–5
The CBCL has been used to measure different aspects of sleep among COAs and non-COAs.6,7 In particular, the CBCL sleep items “trouble sleeping” and “overtiredness without good reason” longitudinally predicted early onset of alcohol and drug use and substance-related problems.6–8 In those studies, there were no differences in sleep difficulties and overtiredness among the two groups. However, studies using actigraphy and polysomnography (PSG) reported differences in sleep physiology between the two groups. One actigraphy study found that COAs had slightly shorter total sleep time (TST) and more nighttime activity compared with non-COAs.9 However, PSG studies showed that the two groups were not different on TST, nighttime activity or any sleep stage variables.10,11 Instead COAs had lower NREM delta power and less power in sleep spindles than non-COAs. It was unclear what explained the inconsistencies in findings. The inconsistencies may stem from differences in methodology (i.e., CBCL items used parental ratings whereas actigraphy and polysomnography are objective sleep measures) or the validity of using CBCL to measure sleep in COAs and non-COAs. The CBCL was not originally designed to measure sleep. It is therefore important to examine its validity by assessing its relationship with other established sleep measures among these two groups of children. To date, no study has systematically examined the differences/similarities in these two groups. This study attempts to fill this gap.
To our knowledge, three studies have examined the relationships between the CBCL sleep items and validated sleep measures.3–5 Gregory et al investigated the relationships between the CBCL sleep items and children’s sleep diaries, actigraphy and polysomnography (PSG) in 122 children and adolescents between 7 and 17 years old (61% female).4 About half (46%) did not have a history of a psychiatric disorder and the other half had a history of anxiety or depressive disorders or both. Results indicated that controlling for age, sex and clinical status, most CBCL sleep items correlated with related actigraphy and PSG items. For instance, “trouble sleeping” was correlated with longer sleep onset latency (SOL) as assessed by both actigraphy and sleep diary. “Overtired without good reason” was correlated with SOL measured by sleep diary and fewer arousals measured by PSG. Even though these results seem to indicate the validity of the CBCL items, some hypothesized correlations were not significant and at least one finding were unexpected. The authors concluded that assessing sleep exclusively using the CBCL is not ideal and studies using these sleep items should also be tested with more rigorous sleep measures.
Belanger et al examined the convergence between CBCL sleep items, actigraphy (3 days) and maternal sleep diaries in 80 2-year-olds (Mage=25.44 months, SDage=1.04; 49% female).5 CBCL items were more strongly correlated with maternal sleep diaries than actigraphy. For instance, maternal ratings of “trouble sleeping” and “resist going to bed at night” were negatively associated with sleep duration in actigraphy. Maternal CBCL items “does not want to sleep alone”, “trouble sleeping” and “resist going to bed at night” were negatively correlated with sleep duration in the diaries. The authors argued that CBCL sleep measures tap into different aspects of sleep. Therefore, researchers should decide on the measures to use based on the aspects of sleep they want to assess.
In a sample of 383 youth (Mage=11.32 years, SDage=3.68; range: 6–18 years; 48% female) evaluated in a behavioral sleep medicine clinic, Becker et al assessed the convergent validity of CBCL sleep items with other validated sleep measures, including Children’s Sleep Habits Questionnaire (parental rating; CSHQ), Sleep Disorders Inventory for Students (parental rating; SDIS), and Adolescent Sleep-Wake Scale (self-report; ASWS).3 Individual CBCL sleep items were significantly correlated with individual items of CSHQ, SDIS and ASWS.3 The authors concluded that even though the CBCL did not provide a thorough assessment of sleep, it was a useful tool for both researchers who lacked a more comprehensive sleep measure and clinicians who did not use other sleep measures.
Though sample size, age and background of the above studies were different, the majority of findings in all three studies indicated expected relations between CBCL sleep items and other sleep measures. The primary goal of this study is to extend previous research by analyzing such relations in a group of COAs and non-COAs between 8 and 12 years old. Specifically, we tested whether CBCL sleep items were related to other sleep measures (actigraphy, Youth Self-Report and other parental ratings) and whether these relationships were the same between the two groups. This comparison has not been done in the past. The inclusion of Youth Self-Report in this study is a novel contribution, as similar measures were not included in the three studies reviewed here. As behavioral problems often correlate with sleep,3,12 we also compared the correlations between CBCL sleep items and behavioral problems (i.e., internalizing, externalizing, attention and social problems) with the correlations between other sleep measures and behavioral problems. Given the popularity of CBCL among both the research and clinical communities, we believe that this will be an important addition to the existing literature.
Materials and Methods
This study was carried out in accordance with the recommendations of the Idaho State University Human Subjects Committee. Parents in the study gave written informed consent and children gave written assent in accordance with the Declaration of Helsinki prior to study participation. The protocol was approved by the Idaho State University Human Subjects Committee (Study 3943).
Participants
Two hundred and forty-eight children aged 8–12 (48% COAs (119 COAs; 129 non-COAs); 50% girls; Mage=10.37, SDage=1.47) participated in a study designed to understand the longitudinal relationship between sleep characteristics and substance use. All data presented here were from Time 1, when all children were naïve to alcohol and other drugs. 64% of participants were Caucasian, 28% were Hispanics and 8% were from other ethnic groups (i.e., African-American, Asian, Native American or biracial).
COAs and their biological parents were recruited through local addiction treatment facilities, Alcoholics Anonymous meetings, community flyers and advertisements in local newspapers, radio stations and Facebook. Non-COAs (controls) and their biological parents were recruited via the same community flyers and advertisements. Non-COAs were matched with COAs on age, sex, and family income on a group basis. All participants and their parents received payment to compensate for their time and effort spent.
Children with the following characteristics were excluded from the study: (i) significant medical problems that could affect sleep (eg, endocrine disorders, chronic pain, asthma) (parental report); (ii) currently taking medications (non-psychiatric or psychiatric medications) that affect sleep (parental report); (iii) a history of psychotic disorders, mania or hypomania, obsessive-compulsive disorder, eating disorders, tic disorders and autism spectrum disorders (parental report); these disorders are less common in children and may affect sleep; (iv) evidence of a primary sleep disorder other than insomnia (eg, obstructive sleep apnea) (parental report and/or diagnosis by a healthcare provider) and (v) evidence of Fetal Alcohol Syndrome (FAS) and Fetal Alcohol Effects (FAEs) (parental report and/or evidence of diagnosis by a healthcare provider). Children with the following characteristics were included: (i) between the ages of 8 to 12; (ii) able and willing to provide informed assent (child) and consent (parent); (iii) among COAs, at least one biological parent had a current or past history of alcohol use disorder as determined by a score of ≥ 6 on the Michigan Alcohol Screening Test (MAST)13 and/or who had a lifetime alcohol use disorder (AUD) according to the MINI International Neuropsychiatric Interview (which yielded diagnoses or abuse or dependence, for which either qualified).14 44% of the participating parent of COAs had a lifetime AUD and 56% did not. Their spouse had a lifetime AUD. Among non-COAs, neither biological parent had a lifetime history of alcohol use disorder.
Procedures
Data for this study were collected in multiple sessions. Families who expressed an interest to participate in the study were asked to schedule an appointment for screening. During the screening interview (Session 1), both the participating parent and the child were administered the MINI.14–16 Parents were also asked to fill out the Michigan Alcoholism Screening Test (MAST) on themselves and the other biological parent of the child. Children with parents who scored a “6” or above on the MAST and/or who had a lifetime alcohol use disorder (AUD) according to the MINI were classified as COAs. If the participating parent was not the one with an AUD, then s/he was asked to answer AUD questions on the MINI about the other biological parent. Parents were also asked to answer questions of the biological mother’s drinking during pregnancy, complete the Child Health and Development History questionnaire, and fill out a demographic questionnaire.
During Session 2 (approximately 1–3 weeks after Session 1), a nurse practitioner did a physical exam and checked facial features of child participants. Screening for FAS, FAE, and other physical problems pertaining to the exclusion criteria were completed by the nurse, using information from this evaluation and the parents’ self-report of drinking habits/patterns of the biological mother during pregnancy. Parents and children were asked to answer several questionnaires on sleep and behavioral problems during this session. Children were also given an actigraph watch and a sleep diary and provided instructions on their use with the parent present.
Sleep Measures
Child Behavior Checklist (CBCL)
The CBCL is a widely used instrument that measures common behavioral problems in the past six months.17 Seven items were used to indicate different problems related to sleep: “nightmares” (item 47), “overtired without good reason” (item 54), “sleeps less than most kids” (item 76), “sleeps more than most kids during day and/or night” (item 77) “talks or walks in sleep” (item 92), “trouble sleeping” (item 100) and “wet the bed” (item 108). Responses to each item were scored on a three-point rating scale (0 = not true; 1 = somewhat or sometimes true; 2 = very true or often true).
Pediatrics Sleep Questionnaire (PSQ)
The PSQ is a well-established instrument measuring children’s sleep difficulties, sleepiness, sleep-disordered breathing and snoring.18 Parents responded “yes”, “no”, or “don’t know” to items concerning their child’s sleep habits and behaviors. Our analyses focused on sleep difficulties (3 items), daytime sleepiness (6 items) and sleep rhythmicity (2 items). The proportion of sleep difficulties, daytime sleepiness and sleep rhythmicity was computed based on a response of “yes” to items related to that scale. Examples of sleep difficulties items include, “Does your child…have difficulty falling asleep at night? …have trouble falling back asleep if he or she wakes up at night?” “…wake up early in the morning and have difficulty going back to sleep?” Examples of daytime sleepiness items include, “Does your child …have a problem with sleepiness during the day? …complain that he or she feels sleepy during the day?” Examples of sleep rhythmicity items include, “Does the time at which your child …goes to bed change a lot from day to day?…or gets up from bed change a lot from day to day?”
Actigraphy
Participants were asked to wear an actigraph watch on their non-dominant wrists for one week, except when they took a shower, bathed or swam. They were instructed to maintain their normal sleep schedule and filled out a simple sleep diary. The diary asked simple questions about bedtime, rise time, amount of time it took to fall asleep, and quality of sleep. The actigraphs (Actiwatch-LTM, Mini-Mitter, Phillips Respironics, Bend, OR) electronically measure the number of movements that exceed 0.01g, gravitation force per minute of recording. In addition, a photoconductive cell records light level exposure, measured in lux. Data were collected in 1-minute-epochs. Trained personnel coded the data for sleep and wake times according to activity level, light exposure and signals as indicated by participants when they were ready to go to bed and when they woke up. Inter-rater agreement ranged from 85% to 90%. Four sleep variables were derived from these data and averaged across the week: total sleep time (TST), sleep efficiency (SE: % time asleep/ total time in bed), sleep onset latency (SOL: time required to fall asleep) and wake time after sleep onset (WASO). The reliability and validity of actigraphy measures have been demonstrated in previous studies.19–21
Youth Self-Report (YSR)
Subjective report of sleep was gathered by sleep items in the YSR, a widely used self-report instrument measuring childhood behavioral problems in the past six months.22 Sleep items on the child-reported YSR match those from the parent-reported CBCL (“I have nightmares”, “I feel overtired”, “I sleep less than most kids”, “I sleep more than most kids during day and/or night” and “I have trouble sleeping”) and were used in the analyses. Items were measured on a three-point scale (0 = not true; 1 = somewhat or sometimes true; 2 = very true or often true).
Behavioral Problems
Behavioral problems were measured by the CBCL. We focused on four behavioral problems that are common in children, internalizing, externalizing, attention and social problems. These problems have been shown to occur more frequently among COAs compared with non-COAs.23,24 Responses were given on a 3-point rating scale (0 = not true; 1 = somewhat or sometimes true; 2 = very true or often true). Mean scores on each problem were calculated. To ensure the independence between sleep measures and behavioral problems, no sleep items were used in the calculation of these problems. The Cronbach’s alphas are 0.86, 0.91, 0.83 and 0.71 for internalizing, externalizing, attention and social problems respectively.
Parental Alcohol Problems
Children with at least one parent who had a score of > 6 on the Michigan Alcoholism Screening Test (MAST)13 and/or who had a lifetime alcohol use disorder (AUD) according to the MINI15,16 were considered to have a positive parental history of alcohol problems (0 = non-COA; 1 = COA). One parent from each family participated in the study. Participating parents answered the MAST for both themselves and the other biological parent of the child. Additionally, they completed the MINI International Neuropsychiatric Interview and answered the MINI alcohol use disorder questions for their partner.15,16 Partners/spouses have been demonstrated to be reliable informants of their partners’ drinking.25,26 MAST scores have been shown to be correlated with alcoholism diagnoses (moderate-to-severe alcohol use disorders).27,28
Analytic Plan
The goals of the study were to (1) examine the relationships between CBCL sleep items and other measures of sleep, including actigraphy, PSQ, and YSR and (2) test whether the relationships were different for COAs and controls. Data were analyzed by multiple linear regression (when the outcomes were continuous), logistic regression (when the outcomes were dichotomous), and structural equation modeling (SEM). Sex (0 = male, 1 = female), age, and ethnicity (0 = non-Caucasian, 1 = Caucasian) were used as covariates. In multiple and logistic regression analyses, CBCL sleep items and COA status (0 = non-COAs, 1 = COAs) were predictors and other sleep measures were outcomes. Group differences among COAs and controls were tested by creating interaction terms between COA status and CBCL sleep items. A significant interaction term indicated that relationships between CBCL sleep items and other sleep measures were different for the two groups. If the interaction term was significant, we computed the analyses separately for the two groups.
In SEM, we used observed sleep variables to estimate latent constructs for each instrument and then examined relationships among the latent variables. The main advantage of using this method lies in the possibility of simultaneously estimating relationships among multiple observed and latent (unobserved) sleep variables. Model fit was evaluated by the Chi-square goodness-of-fit test and three fit indices - Comparative Fit Index (CFI),29 Tucker Lewis Index (TLI),30 and root mean square of approximation (RMSEA).31 The Chi-square statistic evaluates the difference between the data and the fitted covariance matrices, i.e., the hypothetical model.32 An insignificant value indicates a good fit. The test becomes overly conservative when sample size increases.29 Therefore, other indices are also used to evaluate model fit. A value of 0.9 or above on fit indices such as the CFI and TLI indicates a good fit, whereas a value of 0.95 above indicates an excellent fit.33 Values of 0.06 or below on the root mean square of approximation (RMSEA) indicate a satisfactory fit.33
As a supplement to the main analyses, we also computed and compared Kendall’s correlations between CBCL sleep items and four behavioral problems, i.e., internalizing, externalizing, attention and social. These correlations examine the rank correlations among two variables without requiring the variables to be normally distributed. We did this to examine the external validity of the CBCL sleep items compared with other measures, as previous studies have shown that sleep problems are often associated with behavioral problems.3,12
Results
Descriptive Statistics
Table 1 presents data on important demographic variables for the whole sample. BMI and morningness-eveningness scores were also presented because they have been shown to affect sleep. These two variables are not associated with COA status. Table 2 presents descriptive statistics of sleep measures, separately for COAs and non-COAs and for the whole sample. Controlling for sex, age and ethnicity, the two groups were not significantly different on any sleep variables except on two items. Parents of COAs were more likely to report that they walked or talked in their sleep than parents of non-COAs (OR = 1.94, p < 0.05). COAs were less likely to think that they were overtired without good reason (19%) than non-COAs (29%) (OR=0.41, p < 0.05).
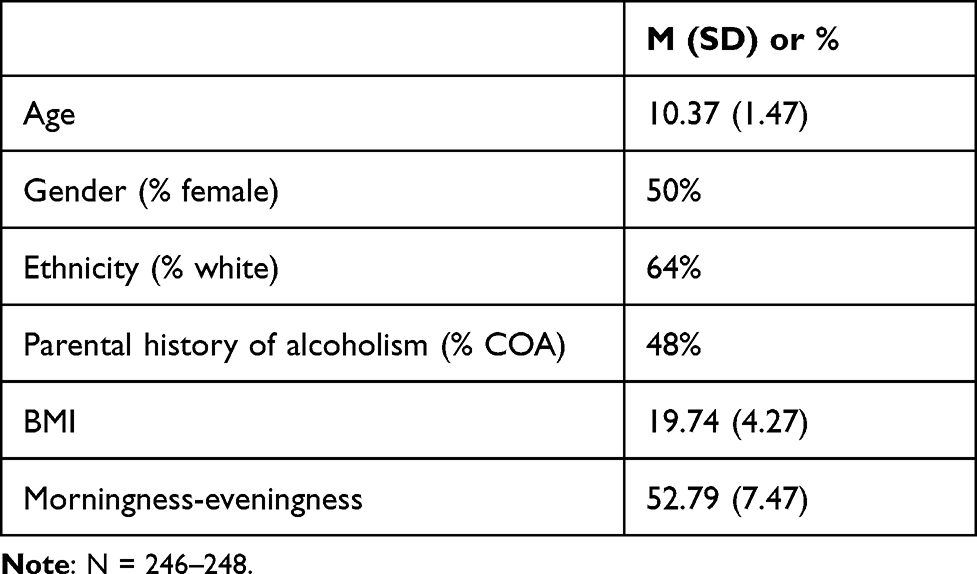 |
Table 1 Characteristics of the Study Sample |
 |
Table 2 Means, Standard Deviations and Percentages of Sleep Measures Among Non-COAs and COAs |
Among COAs, 44% of the participating parent had an alcoholism diagnosis while 56% had a spouse who had a lifetime AUD. None of their ratings on CBCL & PSQ items were significantly different from one another (CBCL: nightmares χ2(1)=.56, p = 0.46; overtired without good reason χ2(1)=.06, p = 0.81; sleeps less than most kids χ2(1)=.02, p=0.88; sleeps more than most kids during day and/or night χ2(1)=1.34, p = 0.25; talks or walks in sleep χ2(1)=.00, p = 0.97; trouble sleeping χ2(1)=1.30, p = 0.25; wet the bed χ2(1)=1.05, p = 0.31. PSQ: sleep difficulty t (107)=.03, p = 0.66; daytime sleepiness t (107)=−.01, p = 0.82; rhythmicity t (107)=−.01, p = 0.92.)
Across the whole sample, CBCL ratings showed that 27% of children had nightmares (i.e., those who scored “1” or “2” on the item), 9% were overtired without good reason, 20% slept less than other children, 7% slept more than other children, 33% talked or walked in their sleep, 26% had trouble sleeping and 8% wet the bed. Percentages on similar items in the YSR were higher – 67% reported having nightmares, 23% felt they were overtired without good reason, 31% believed that they slept less than other children, 22% thought that they slept more than other children and 46% reported that they had trouble sleeping (“talked or walked in sleep” and “wet the bed” are not in YSR). According to PSQ ratings, on the average children scored “yes” on 25% of sleep difficulties items, 14% of sleepiness items and 12% of rhythmicity items. Actigraphy data revealed that participants in this study slept approximately seven and a half hour per night (SD = 40.58 minutes). SOL was approximately 34 minutes (SD = 26.95 minutes). SE was around 80% (SD = 6.33%). WASO was about 55 minutes (SD = 17.2 minutes). The average reported bedtime was 7:45 pm and average reported wake time was 8:01 am.
Relationships Between CBCL Sleep Items and Actigraphy
A relatively small percentage of the sample had a score of 2 on CBCL sleep items (i.e., nightmares: 3.2%; overtiredness: 1.6%; sleeps less: 5.3%; sleeps more: 0.8%; talk/walks in sleep: 5%; trouble sleeping: 7.7%; wets bed: 3%). Therefore, each item was recoded as a dichotomous variable (0 = not true, 1 = sometimes or often true) to avoid violating any statistical assumptions in multiple regression. Both “sleeps less than most kids” and “trouble sleeping” in the CBCL significantly predicted shorter TST and longer SOL. “Overtired without good reason” was significantly associated with longer SOL. Additionally, COAs who were overtired were more likely to have lower sleep efficiency. However, no such relation was found in non-COAs. The relationships between other CBCL items and actigraphy variables are listed in Table 3.
 |
Table 3 Relations Among CBCL Sleep Items, COA Status and Actigraphy |
Relationships Between CBCL and PSQ Sleep Items
“Nightmares”, “overtiredness”, “sleeps less” and “trouble sleeping” were associated with PSQ sleep difficulties. Additionally, “nightmares”, “overtiredness”, “sleeps less”, “sleeps more” and “trouble sleeping” predicted PSQ daytime sleepiness. “Sleeps less” was associated with PSQ low rhythmicity. No significant interaction between CBCL and COA was found, indicating that the relationships between CBCL and PSQ items were the same in COAs and non-COAs. The relationships between other CBCL items and actigraphy variables are listed in Table 4.
 |
Table 4 Relations Among CBCL Sleep Items, COA Status and Pediatrics Sleep Questionnaire |
Relationships Between CBCL and YSR Sleep Items
Few participants endorsed a score of 2 on YSR items (i.e., nightmares: 8.1%; overtiredness: 2.7%; sleeps less: 9.4%; sleeps more: 5.4%; trouble sleeping: 11.3%). These items were recoded to dichotomous variables (0 = no; 1 = yes) to facilitate the interpretation of findings of logistic regression analyses. “Trouble sleeping” in the CBCL significantly predicted the same item in YSR. The estimated odds for having trouble sleeping in the YSR were three and a half (3.58) times as high among participants whose parents rated them as having trouble sleeping compared with participants who did not receive such a rating. CBCL “sleeps less” and “talks or walks in sleep” predicted the YSR nightmare item. The estimated odds for having nightmares in the YSR were about three (2.88) times as high among participants whose parents reported that they slept less than other children compared with participants whose did not have such a rating. Additionally, the estimated odds for having nightmares in the YSR were two (2.28) times as high among participants whose parents believed that they walked or talked in their sleep compared with participants whose parent did not have such a belief. There was no significant interaction between CBCL and COA, suggesting that the relations between CBCL and YSR items were similar among COAs and non-COAs. The relationships between other CBCL items and actigraphy variables are listed in Table 5.
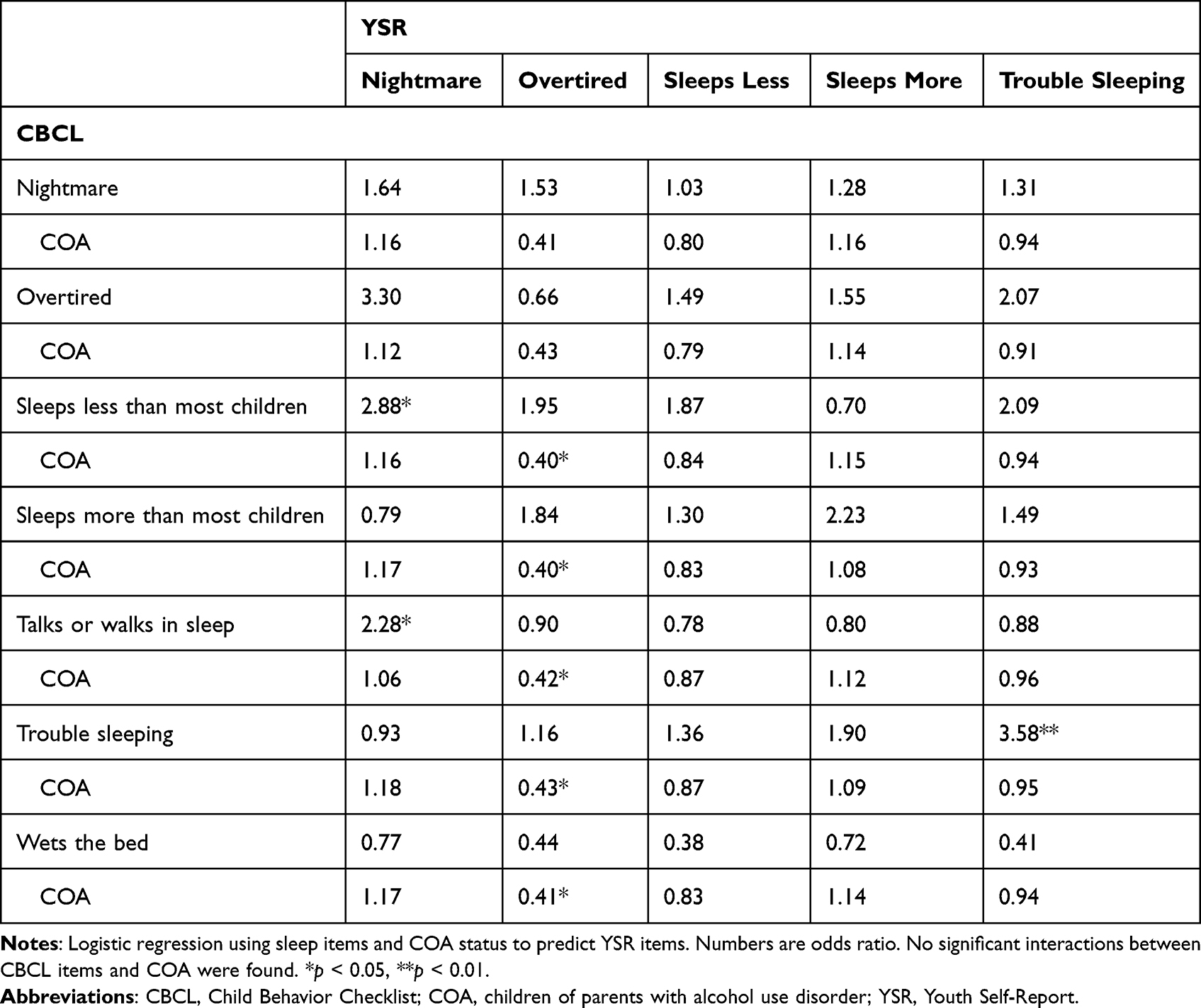 |
Table 5 Relations Among CBCL Sleep Items, COA Status and Youth Self-Report |
Relationships Between Latent Sleep Measures
Measurement Model
Four latent variables, CBCL, PSQ, actigraphy and YSR, were estimated. In considering what CBCL items to include in the analyses, we first examined the factor loadings. “Sleeps more” (r = 0.02, p = 0.77) and “wets the bed” (r = −.09, p = 0.18) had insignificant loadings on the latent variable and were excluded from the analyses. “Talks or walks in sleep” had a small but significant loading (r = 0.20, p < 0.01) but there was not a corresponding YSR item that measures such behavior. As the primary goal of doing SEM analyses was to estimate the relationships between the latent variable of CBCL and latent variables of other sleep measures, we decided to drop “talks or walks in sleep”. SE and WASO measured by actigraphy were highly correlated with other indicators on the same latent variables. Including them in the analyses led to model non-convergence. They were also dropped. All other observed indicators loaded significantly onto their corresponding latent variables. The standardized factor loadings are presented in Figure 1. All loadings were significant at p < 0.01 or below.
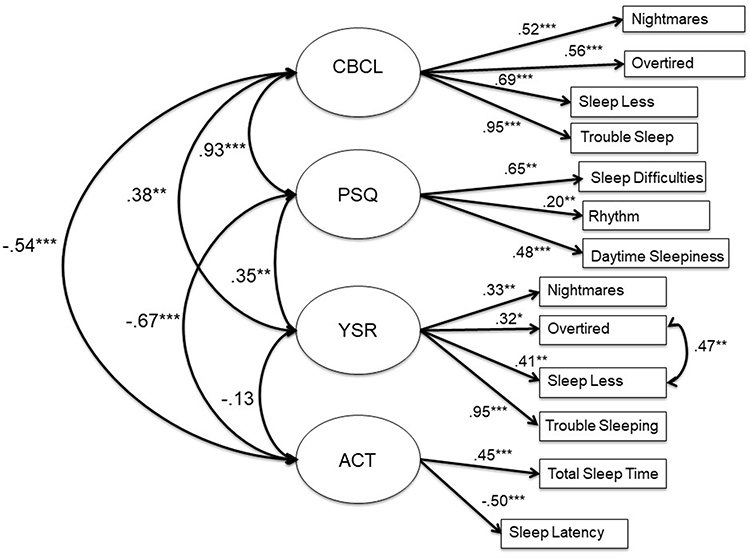 |
Figure 1 Associations between CBCL sleep items and other sleep measures. Notes: *p < 0.05, **p < 0.01, ***p < 0.001. Model fit: χ2(58)=69.83, p = 0.14, CFI = 0.97, TLI = 0.96, RMSEA = 0.03. |
Structural Model
We conducted multiple group analyses to test whether COAs and non-COAs were different in the correlations between CBCL and other sleep measures. Due to the high correlation between CBCL and PSQ latent variables (r = 0.93), there were problems with convergence. PSQ was dropped from the analyses. We tested whether the factor loadings for CBCL, YSR and actigraphy were the same across groups. No comparisons were significant between groups, indicating that there was group invariance in all factor loadings. We then tested whether the correlations among the latent variables were the same across groups. The comparisons were not significant, indicating that there were no group differences in these correlations (CBCL and YSR: χ2(1) = .23, p = 0.63; CBCL and actigraphy: χ2(1) = 2.56, p = 0.11; YSR and actigraphy: χ2(1) = .04, p = 0.84).
Due to the lack of differences, we combined the groups and conducted the analyses on the whole sample. PSQ was retained in these analyses as there were no convergence issues here. CBCL ratings of sleep difficulties were negatively correlated with actigraphy variables (longer TST, shorter SOL) and positively correlated with both PSQ and YSR. The overall fit indices indicate that the model fits the data well, χ2(58)=69.84, p=0.14, CFI = 0.97, TLI = 0.96, RMSEA = 0.03. The final model is presented in Figure 1.
Correlations Between CBCL Sleep Items and Behavioral Problems
There were significant correlations between CBCL sleep items and different types of behavioral problems. “Overtired without good reasons” and “trouble sleeping” were significantly correlated with all four problems. Nightmares were correlated with social, attention and externalizing problems. “Sleeps less” was correlated with social, internalizing and externalizing problems. “Sleeps more”, “talks/walks in sleep” and “wets the bed” were each correlated with one behavioral problem. As seen in Table 6, like other established sleep measures such as PSQ and actigraphy, CBCL sleep items were correlated with behavioral problems in an expected manner.
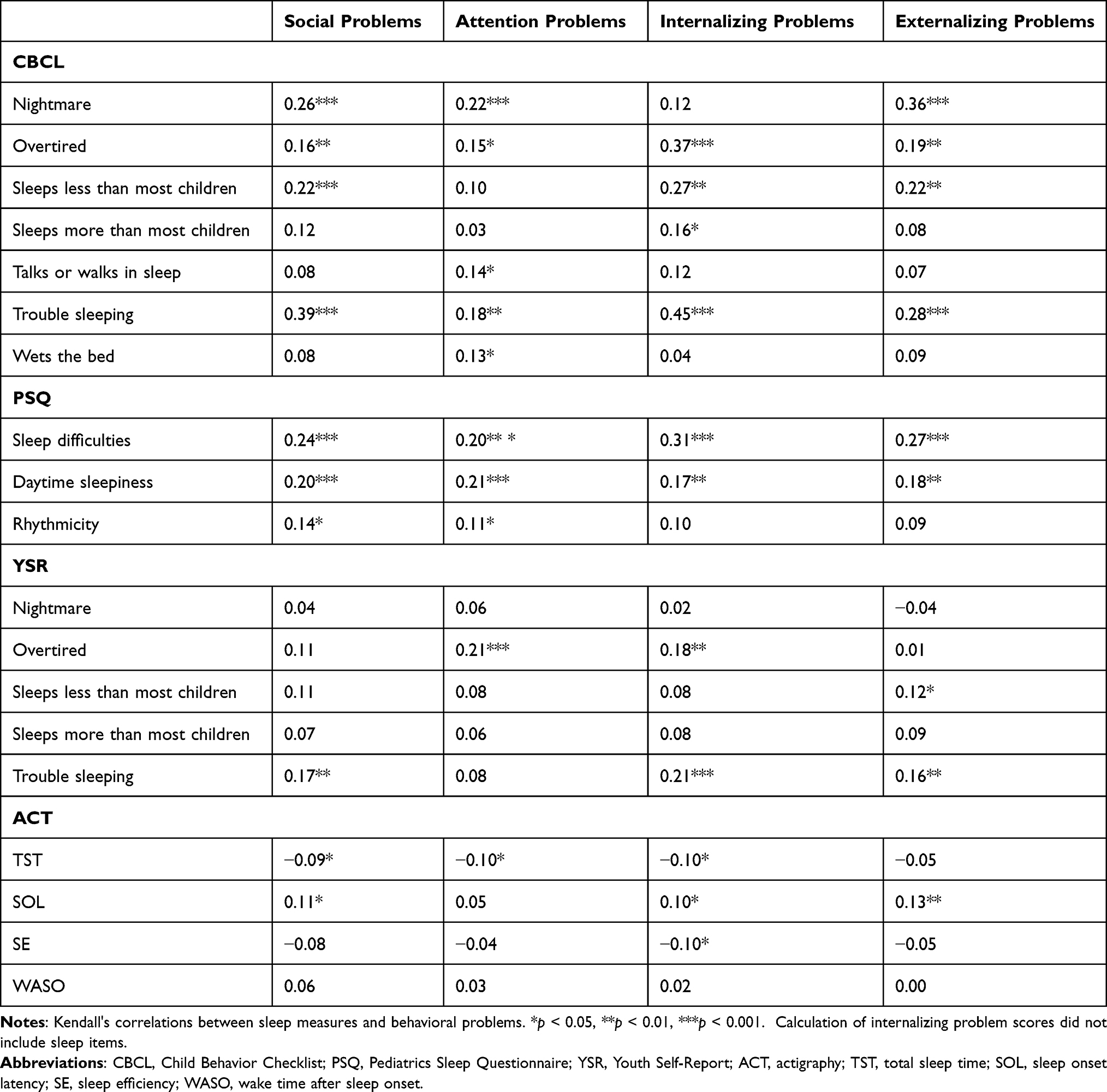 |
Table 6 Relations Between Sleep Measures and Behavioral Problems |
Discussion
We examined the associations between CBCL items and other sleep measures, including actigraphy, a well-established parental sleep questionnaire, PSQ and YSR sleep items in COAs and non-COAs between 8 and 12 years old. The validity of using CBCL sleep items to measure sleep has not previously been established in these two groups. This study is the first one to examine whether these items are associated with several established sleep measures among COAs and non-COAs. These findings are important because several studies reported a longitudinal relationship between sleep problems in early childhood (as measured by the CBCL) and subsequent developmental outcomes such as onset of alcohol and other drug use in adolescence and presence of substance-related problems in young adulthood.6–8 These outcomes are important for all children, especially COAs, who are at risk for substance use. However, the validity of using CBCL items to measure sleep has been questioned by some researchers.4 The results of this study show that CBCL items are valid measures of sleep in both COAs and non-COAs and therefore lend credence to the relationship between sleep problems and substance use reported in previous studies.
Our results show that there were minimal differences on these relationships in these two groups. Multiple linear regression analyses indicated no significant group differences except on one item. COAs who were overtired in the CBCL were more likely to have lower SE on actigraphy. This relationship was absent in non-COAs. To our knowledge, this is the first time that such a finding is reported. It remains to be seen whether this can be replicated in other studies. Future research could examine whether lower SE predicts behavioral differences between the two groups and/or a higher probability of risk behavior (including substance use) among COAs.
Descriptive statistics showed that COAs were less likely to rate themselves as “overtired” than non-COAs. However, we did not find this difference in parental rating of overtiredness. Among COAs, whether the participating parent had an alcoholism diagnosis or not did not affect the rating of this item. Tiredness is a subjective experience. One possible explanation is that parents were not aware of their children’s energy level. Another possible explanation is that parents and children focus on different aspects of sleep. SEM analyses showed that parental ratings were significantly correlated with actigraphy variables whereas youth report was not. The differences between youth report and parental ratings need to be further investigated in future studies. Additionally, future work could assess whether perception of overtiredness is related to any behavioral differences between COAs and non-COAs.
With the exception of the above differences, our analyses did not identify any group differences on the relationships between CBCL sleep items and other sleep measures. Studies comparing sleep characteristics between COAs and non-COAs are still inconclusive, with some studies reporting no major differences in parental ratings and youth report6–8, and others reporting significant differences in actigraphy (eg, shorter TST and more nighttime motor activity)9 and polysomnography (eg, lower delta power in NREM sleep).10,11 This study adds to the existing literature by showing that CBCL sleep items are valid measures of sleep among both COAs and non-COAs. Specifically, the relationships between CBCL items and other established sleep measures are similar in these two groups. Future research could compare whether the relationships between sleep measures and behavior, especially risky behaviors such as alcohol use, are different in COAs and non-COAs. While some studies found no differences between the two groups on the relationships between CBCL sleep items (eg, trouble sleeping) and onset of substance use and substance-related problems,6,7 it remains unclear whether the relationships among other sleep measures (eg, actigraphy, PSG) and risky behaviors are the same between the two groups.
Analyses on the whole sample showed that CBCL sleep items were related to other sleep measures in a theoretically meaningful way. In both COAs and non-COAs, multiple regression analyses showed that the CBCL item, “trouble sleeping”, was associated with shorter TST and longer SOL in actigraphy, as well as sleep difficulties in PSQ and “trouble sleeping” in YSR. The CBCL item, “overtiredness”, was associated with longer SOL in actigraphy and daytime sleepiness in the PSQ. Across both groups, SEM analyses indicated that CBCL sleep items were highly correlated with PSQ at a magnitude of 0.9. This suggested that parental ratings were largely consistent across questionnaires, even though the CBCL measured sleep issues in the last six months whereas PSQ measures sleep and wakefulness behavior without a specific timeframe.
SEM also showed that CBCL sleep ratings were significantly correlated with actigraphy. Regardless of their COA status, children who had nightmares, who were overtired, who slept less than other children and who had trouble sleeping had lower TST and longer SOL. The latent CBCL sleep variable were significantly correlated with the latent actigraphy variable (r=−.54, p<0.001). The significant association offers strong support for the convergence between the two measures and the validity of CBCL sleep items.
Additional SEM analyses showed that the CBCL latent sleep variable was negatively correlated with sleep efficiency but was not correlated with WASO. It is useful to note that past studies using other validated self-report sleep measures also reported significant correlations with TST, SOL and SE but not WASO.34 Our results are therefore consistent with these studies and suggest that CBCL are correlated with actigraphy variables in a comparable manner as other validated sleep measures.
The timeframe of different sleep measures is worthy of attention. The CBCL asked parents to rate children’s sleep in the last six months. Actigraphy data were collected for one week only. The differences in timeframe may have lowered the associations between variables collected by these two methods. The association between the two might have been stronger if we asked parents to provide CBCL ratings in the past week. The advantages of using parental report are that sleep data over a long time may be collected easily and inexpensively. It is costly and impractical to collect actigraphy data over an extended period. The two measures complement each other, offering different information about sleep characteristics of children.
CBCL sleep items were correlated with YSR items in both logistic regression analyses and SEM, though the correlations were modest. Logistic regression analyses showed that CBCL items, “trouble sleeping”, “sleeps less than other kids” and “walks or talks in sleep” were associated with YSR items, “trouble sleeping” and “nightmares”. SEM analyses showed that the two latent variables made up of items from CBCL and YSR were correlated modestly but significantly (r = 0.38, p = 0.001). Critics may argue that this correlation is low. There may be a number of reasons why the two set of items were correlated only modestly. Overall children rated their sleep as worse than their parents did (Table 2). Information about some of these items are not easily accessible to parents, eg, “nightmares” and “overtiredness”. Parents and children may also have different opinion about whether the amount of children’s sleep was more or less compared with other children. In this study, YSR items were not associated with actigraphy significantly. Younger participants in this sample (eg, 8- or 9-years-old) might not yet be able to evaluate their own sleep objectively or compared their sleep with other children accurately. It remains to be seen whether the correlation between YSR and actigraphy will increase as participants get older.
CBCL sleep items were significantly correlated with internalizing, externalizing, social and attention problems. The patterns of correlations were similar to the correlations between other sleep measures and behavioral problems. Sleep difficulties and tiredness in children have been previously shown to predict different types of behavioral problems.35–37 Our findings are consistent with these studies. This suggests that CBCL sleep items have good external validity.
Several limitations of this study should be noted. The sleep measures presented in this study do not include PSG data, which is considered the gold standard of sleep measurement. To our knowledge, only one study examined the relationships between CBCL sleep items and PSG variables.4 In that study, “sleeps less than other kids” in the CBCL was negatively correlated with TST (r = −.23) as measured by PSG and “overtired” was unexpectedly negatively correlated with the number of arousals (r = −.22). Future research could further investigate the relations between CBCL sleep items and PSG. Another limitation is that our study is cross-sectional. Therefore, we do not know the temporal relations among the sleep measures. Longitudinal data are still being collected and processed in our study. A third limitation has to do with the generalizability of study findings. As the study excluded children with certain characteristics (i.e., children with a sleep disorder, children who took medications that affect sleep, children with a history of psychiatric disorders that are relatively uncommon in their age group, children with FAS or FAE), the findings reported here may not be generalized to these individuals. A fourth limitation is that the study did not collect any sleep data from the parents. Parents who slept poorly or slept less than others spent more time awake at night and might be more aware of their children sleep issues (eg, sleep taking or walking). Another limitation is that YSR may not be a valid instrument for individuals younger than 11 years old. YSR is validated for youth 11 to 18 years of age. The participants of this study were between 8 and 12 years old. However, a study found that youth between ages 7 and 10 were able to provide reliable reports on the YSR broad band scales, i.e., internalizing and externalizing scales. As CBCL sleep items are items on the internalizing scale, we believe that those items are reasonably reliable measures for younger participants in this study. Lastly, the family environment of COAs may be different from non-COAs. Parental lifetime alcohol use disorder is associated with a higher likelihood of violence exposure38 and poor parental monitoring,36 which may affect children’s sleep habits and patterns. The absence of data on family violence and parental monitoring in this study is another limitation.
Our findings show significant and meaningful associations between CBCL sleep items and other sleep measures, including actigraphy as an objective measure of sleep, YSR and another validated parental sleep measure, PSQ. These findings are consistent with previous studies. Even though CBCL sleep items do not thoroughly assess sleep, they nevertheless provide useful, though preliminary information about certain aspects of sleep. These items are especially valuable when a thorough assessment of sleep cannot be done. CBCL sleep items are part of a commonly used instrument and can be easily incorporated in many studies. Moreover, the items are straightforward, easy to understand, and require little time for parents to complete, making them a useful sleep measure when more detailed sleep measures cannot be included. Pediatric clinicians also may not have the time or resources to do a thorough sleep assessment.4 These items may draw attention to sleep issues among patients that need further investigation. Though CBCL sleep items were not originally designed for the purpose of measuring sleep, findings in this study demonstrate that they are correlated with more objective and validated sleep measures.
Data Sharing Statement
The datasets for this manuscript are not publicly available until the investigators publish papers related to the specific aims. Requests to access the datasets should be directed to the first author.
Acknowledgments
The work presented here was supported in part by a research grant from the National Institute on Alcohol Abuse and Alcoholism and National Institute of General Medical Sciences (R01 AA020364). However, the funding agencies had no further role in the study design, planning, data collection, analysis and interpretation of data, and writing of the report or the decision to submit the paper for publication. The authors are responsible for the opinions expressed in this paper. We thank all participants and the research staff of this study.
Disclosure
The authors declare no conflict of interest.
References
1. Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms and Profiles. Burlington, VT: University of Vermont; 2001.
2. Holmbeck GN, Thill AW, Bachanas P, et al. Evidence-based assessment in pediatric psychology: measures of psychosocial adjustment and psychopathology. J Pediatr Psychol. 2008;33(9):958–980. doi:10.1093/jpepsy/jsm059
3. Becker SP, Ramsey RR, Byars KC. Convergent validity of the child behavior checklist sleep items with validated sleep measures and sleep disorder diagnoses in children and adolescents referred to a sleep disorders center. Sleep Med. 2015;16(1):79–86. doi:10.1016/j.sleep.2014.09.008
4. Gregory AM, Cousins JC, Forbes EE, et al. Sleep items in the child behavior checklist: a comparison with sleep diaries, actigraphy, and polysomnography. J Am Acad Child Adolesc Psychiatry. 2011;50(5):499–507. doi:10.1016/j.jaac.2011.02.003
5. Belanger ME, Simard V, Bernier A, Carrier J. Investigating the convergence between actigraphy, maternal sleep diaries, and the child behavior checklist as measures of sleep in toddlers. Front Psychiatry. 2014;5:158. doi:10.3389/fpsyt.2014.00158
6. Wong MM, Brower KJ, Nigg JT, Zucker RA. Childhood sleep problems, response inhibition, and alcohol and drug outcomes in adolescence and young adulthood. Alcohol Clin Exp Res. 2010;34(6):1033–1044. doi:10.1111/j.1530-0277.2010.01178.x
7. Wong MM, Brower KJ, Zucker RA. Childhood sleep problems, early onset of substance use and behavioral problems in adolescence. Sleep Med. 2009;10(7):787–796. doi:10.1016/j.sleep.2008.06.015
8. Wong MM, Brower KJ, Fitzgerald HE, Zucker RA. Sleep problems in early childhood and early onset of alcohol and other drug use in adolescence. Alcoholism. 2004;28(4):578–587. doi:10.1097/01.ALC.0000121651.75952.39
9. Conroy DA, Hairston IS, Zucker RA, Heitzeg MM. Sleep patterns in children of alcoholics and the relationship with parental reports. Austin J Sleep Disord. 2015;2(1):1009.
10. Tarokh L, Carskadon MA. Sleep electroencephalogram in children with a parental history of alcohol abuse dependence. J Sleep Res. 2010;19(1, Pt 2):165–174. doi:10.1111/j.1365-2869.2009.00763.x
11. Tarokh L, Van Reen E, Acebo C, et al. Adolescence and parental history of alcoholism: insights from the sleep EEG. Alcohol Clin Exp Res. 2012;36(9):1530–1541. doi:10.1111/j.1530-0277.2012.01756.x
12. Sivertsen B, Harvey AG, Reichborn-Kjennerud T, Torgersen L, Ystrom E, Hysing M. Later emotional and behavioral problems associated with sleep problems in toddlers: a longitudinal study. JAMA Pediatr. 2015;169(6):575–582. doi:10.1001/jamapediatrics.2015.0187
13. Selzer ML. The Michigan alcoholism screening test: the quest for a new diagnostic instrument. Am J Psychiatry. 1971;127(12):1653–1658. doi:10.1176/ajp.127.12.1653
14. Sheehan DV, Sheehan KH, Shytle RD, et al. Reliability and validity of the mini international neuropsychiatric interview for children and adolescents (MINI-KID). J Clin Psychiatry. 2010;71(3):313–326. doi:10.4088/JCP.09m05305whi
15. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Supplemental20):22–33.
16. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The validity of the Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its reliability. Eur Psychiatry. 1997;12(5):232–241. doi:10.1016/S0924-9338(97)83297-X
17. Achenbach T. Manual for the Child Behavior Checklist / 4–18 and 1991 Profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991.
18. Chervin RD, Hedger KM, Dillon JE, Pituch KJ. Pediatric Sleep Questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000;1:21–32. doi:10.1016/S1389-9457(99)00009-X
19. Acebo C, Sadeh A, Seifer R, et al. Estimating sleep patterns with activity monitoring in children and adolescents: how many nights are necessary for reliable measures? Sleep. 1999;22(1):95–103. doi:10.1093/sleep/22.1.95
20. Sadeh A. Sleep and development: advancing theory and research: III. Sleep assessment methods. Monogr Soc Res Child Dev. 2015;80(1):33–48. doi:10.1111/mono.12143
21. Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP. The role of actigraphy in the study of sleep and circadian rhythms. Sleep. 2003;26(3):342–392. doi:10.1093/sleep/26.3.342
22. Achenbach T. Manual for the Youth Self-Report Form and 1991 Profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991.
23. Zucker RA. Alcohol use and the alcohol use disorders: a developmental-biopsychosocial systems formulation covering the life course. In: Cicchetti D, Cohen DJ, editors. Developmental Psychopathology: Risk, Disorder, and Adaptation, Vol. 3.
24. Zucker RA, Heitzeg MM, Nigg JT. Parsing the undercontrol–disinhibition pathway to substance use disorders: a multilevel developmental problem. Child Dev Perspect. 2011;5(4):248–255. doi:10.1111/j.1750-8606.2011.00172.x
25. Rychtarik RG, McGillicuddy NB. Coping skills training and 12-step facilitation for women whose partner has alcoholism: effects on depression, the partner’s drinking, and partner physical violence. J Consult Clin Psychol. 2005;73(2):249–261. doi:10.1037/0022-006X.73.2.249
26. Thomas EJ, Santa C, Bronson D, Oyserman D. Unilateral family therapy with the spouses of alcoholics. J Soc Serv Res. 1986;10(2–4):145–162. doi:10.1300/J079v10n02_09
27. Selzer ML, Barton E. The drunken driver: a psychosocial study. Drug Alcohol Depend. 1977;2(4):239–253. doi:10.1016/0376-8716(77)90002-3
28. Selzer ML, Vanosdall FE, Chapman M. Alcoholism in a problem driver group: a field trial of the Michigan Alcoholism Screening Test (MAST). J Safety Res. 1971;3(4):176–181.
29. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037/0033-2909.107.2.238
30. Tucker LR, Lewis C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika. 1973;38(1):1–10. doi:10.1007/BF02291170
31. Steiger JH, Lind JC. Statistically based tests for the number of common factors.
32. Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychol Bull. 1980;88(3):588–606. doi:10.1037/0033-2909.88.3.588
33. Hu L-T, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
34. Sadeh A. The role and validity of actigraphy in sleep medicine: an update. Sleep Med Rev. 2011;15(4):259–267. doi:10.1016/j.smrv.2010.10.001
35. Carvalho Bos S, Gomes A, Clemente V, et al. Sleep and behavioral/emotional problems in children: a population-based study. Sleep Med. 2009;10(1):66–74. doi:10.1016/j.sleep.2007.10.020
36. Fals-Stewart W, Kelley ML, Fincham FD, Golden J, Logsdon T. Emotional and behavioral problems of children living with drug-abusing fathers: comparisons with children living with alcohol-abusing and non-substance-abusing fathers. J Fam Psychol. 2004;18(2):319. doi:10.1037/0893-3200.18.2.319
37. Gregory AM, Eley TC, O’Connor TG, Plomin R. Etiologies of associations between childhood sleep and behavioral problems in a large twin sample. J Am Acad Child Adolesc Psychiatry. 2004;43(6):744–751. doi:10.1097/01.chi/0000122798.47863.a5
38. Hanson RF, Self-Brown S, Fricker-Elhai A, Kilpatrick DG, Saunders BE, Resnick H. Relations among parental substance use, violence exposure and mental health: the national survey of adolescents. Addict Behav. 2006;31(11):1988–2001. doi:10.1016/j.addbeh.2006.01.012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.