")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Contributions of Japanese Hospitalists During the COVID-19 Pandemic and the Need for Infectious Disease Crisis Management Education for Hospitalists: An Online Cross-Sectional Study
Authors Tago M , Hirata R , Katsuki NE, Otsuka Y, Shimizu T , Sasaki Y , Shikino K , Watari T , Takahashi H, Une K, Naito T , Otsuka F, Thompson R, Tazuma S
Received 22 May 2023
Accepted for publication 4 August 2023
Published 21 August 2023 Volume 2023:16 Pages 1645—1651
DOI https://doi.org/10.2147/RMHP.S422412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Masaki Tago,1 Risa Hirata,1 Naoko E Katsuki,1 Yuki Otsuka,2 Taro Shimizu,3 Yosuke Sasaki,4 Kiyoshi Shikino,5 Takashi Watari,6 Hiromizu Takahashi,7 Kazunobu Une,8 Toshio Naito,7 Fumio Otsuka,2 Rachel Thompson,9 Susumu Tazuma8,10
1Department of General Medicine, Saga University Hospital, Saga, Japan; 2Department of General Medicine, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama, Japan; 3Department of Diagnostic and Generalist Medicine, Dokkyo Medical University, Tochigi, Japan; 4Department of General Medicine and Emergency Care, Toho University School of Medicine, Tokyo, Japan; 5Department of General Medicine, Chiba University Hospital, Chiba, Japan; 6General Medicine Center, Shimane University Hospital, Izumo, Japan; 7Department of General Medicine, Juntendo University Faculty of Medicine, Tokyo, Japan; 8Department of Critical Care and General Medicine, Onomichi General Hospital, Hiroshima, Japan; 9Executive Team, Snoqualmie Valley Hospital, Snoqualmie, WA, USA; 10JR Hiroshima Hospital, Hiroshima, Japan
Correspondence: Masaki Tago, Department of General Medicine, Saga University Hospital, 5-1-1 Nabeshima, Saga, 849-8501, Japan, Tel +81 952 34 3238, Fax +81 952 34 2029, Email [email protected]
Introduction: Hospitalists in Japan have been at the forefront of the COVID-19 pandemic. However, contributions of Japanese hospitalists during the COVID-19 pandemic and hospitalists’ awareness of crisis management education remain unclear.
Material and Methods: We conducted a questionnaire survey to investigate the role of Japanese hospitalists during the COVID-19 pandemic. The questionnaire was conducted using email and Google Forms targeting the chairpersons of facilities certified by the Japanese Society of Hospital General Medicine (JSHGM). Members of the academic committee of the JSHGM and several hospitals conducted a narrative review and determined the questions for the survey in a discussion.
Results: We conducted descriptive statistics based on the responses of 97 hospitals that agreed to participate in this survey. In total, 91.8% of general medicine departments in the included hospitals were involved in the medical care of COVID-19 patients. Furthermore, in 73.2% of hospitals, hospitalists were involved in infection control for COVID-19 inside or outside the hospital. Our survey revealed that Japanese hospitalists were responsible for COVID-19 treatment in over 60% of hospitals and contributed to hospital management, infection control, and vaccination. In total, 79.4% of hospitals answered that “training of personnel who can provide practical care for emerging infectious diseases is necessary”, 78.4% indicated that “the establishment of an infection control system in advance to prepare emerging infectious diseases in the hospital is necessary”, and 74.2% stated that “the establishment of an educational system for responding to emerging infectious diseases is necessary.”.
Conclusion: In conclusion, during the pandemic, in addition to inpatient care, Japanese hospitalists provided outpatient care for COVID-19, which is the role of primary care physicians in other countries. Furthermore, Japanese hospitalists who experienced the COVID-19 pandemic expressed the need for personnel development and education to prepare for future emerging infectious disease pandemics.
Keywords: COVID-19 pandemic, hospitalist, hospital management
Introduction
The coronavirus disease 19 (COVID-19) pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS CoV-2) has resulted in numerous infections and deaths worldwide.1 In the United States, hospitalists have been at the forefront of the pandemic,2 providing inpatient care to patients with COVID-19 and fulfilling their roles as usual, even in emergencies.3 According to the database assessment conducted by experts, hospitalists in the United States treated 75% of COVID-19 patients. A good relationship between hospitalists and specialist physicians in each medical department is essential during a public health emergency, and there are reports of collaboration between volunteer specialists and hospitalists.4 It is believed that in Japan, hospitalists have played a similar role during the COVID-19 pandemic. However, this has not been clarified because of the relatively short history of general medicine and hospitalists in Japan and the diverse roles and lack of clear differentiation between hospitalists and specialized medical departments.5 Furthermore, there were no legal or governmental mandates in Japan concerning the medical departments responsible for managing infectious disease outbreaks. Moreover, there is a shortage of infectious disease specialists in Japan,6 and hospitalists are expected to be involved in patient care and infection control not only for COVID-19 but also for other infectious diseases.7
The COVID-19 pandemic prompted the implementation of thorough infection control measures, caused shortages of medical resources and personnel worldwide, and led to the collapse of medical healthcare systems. Although humankind has experienced emerging infectious diseases such as those caused by novel influenza viruses, severe acute respiratory syndrome (SARS), and Middle East respiratory syndrome coronaviruses, the COVID-19 pandemic has nevertheless posed familiar problems such as shortages of medical resources and personnel—suggesting inadequate preparation and response measures in hospitals to address emerging infectious diseases.8 By enhancing infectious disease crisis management education, the chaos in healthcare that may be caused by future pandemics of emerging infectious diseases can be alleviated.
However, contributions of Japanese hospitalists during the COVID-19 pandemic and hospitalists’ awareness of crisis management education remain unclear. Therefore, we conducted a survey to investigate the role of Japanese hospitalists during the COVID-19 pandemic and the awareness of infectious diseases crisis management education among Japanese hospitalists who experienced the COVID-19 pandemic.
Materials and Methods
We conducted a questionnaire survey using email and Google Forms targeting the chairpersons of general medicine departments in facilities certified by the Japanese Society of Hospital General Medicine (JSHGM). The JSHGM was established in 2010 and currently has approximately 2200 members. In 2022, hospitalist was recognized as a formal specialty for certification. Certified facilities have general medicine departments and hospitalists certified by the JSHGM and are responsible for specialty training programs for hospitalists in Japan. The survey was conducted targeting all 361 facilities certified by the JSHGM. Facilities that did not respond or did not provide consent were excluded from the analysis. The survey period was from December 15, 2022 to January 22, 2023, during which four email requests were sent.
In the questionnaire survey, we asked the information on the background and role of general medicine departments during the COVID-19 pandemic (from January 1, 2020 to October 31, 2022) from Q1 to Q15 (Table 1). Additionally, the following questions were also answered by the respondents.
Q16.What preparations do you think are necessary to protect against future emerging infectious diseases? (Multiple answers were allowed from a list of choices.)
Q17-1.Would you like to receive education on infectious disease crisis management if given the opportunity?
Q17-2.If you answered Yes to Q17-1, please specify the educational themes in which you would be interested. (Multiple answers were possible.)
 |
Table 1 Results of the Questionnaire Survey |
Members of the academic committee of the JSHGM and several hospitals conducted a narrative review and determined the questions for the survey in a discussion. Regarding the analysis, the responses of participants were aggregated. Categorical variables were described using frequencies, and continuous variables were described using medians. One researcher classified and aggregated open-ended responses based on keywords.
All respondents provided informed consent on the questionnaire website and personal information was anonymized in the analysis. This study was approved by the Ethics Committee of Okayama University Hospital (No. 2212–043).
Results
We sent the questionnaire by email to the chairpersons of 347 hospitals, for which we had valid email addresses, among 361 certified facilities. Among the 101 hospitals that responded (response rate, 29.1%), we conducted descriptive statistics based on the responses of 97 hospital chairpersons who agreed to participate in this survey (Figure 1). The median (interquartile range) for the number of beds and medical departments in the participating hospitals was 393 beds (269–614) and 25 departments (18–32), respectively. Details of the results of Q1 to Q15 are shown in Table 1. In total, 91.8% of general medicine departments in the included hospitals were involved in the medical care of patients with COVID-19 (Q1), with 79.4% responsible for outpatient care for suspected COVID-19 cases (Q4) and 78.9% responsible for the medical care of inpatients with confirmed COVID-19 infection (Q5). Additionally, 75.3% of general medicine departments provided COVID-19 vaccination services (Q12-1). Furthermore, in 62.9% of hospitals, hospitalists were responsible for COVID-19 medical care for outpatients or inpatients (Q10), and in 73.2% of hospitals, hospitalists were involved in infection control for COVID-19 inside or outside the hospital (Q11). Additionally, 58.8% of hospitals conducted education and awareness activities on COVID-19 for health care workers (Q13). However, only 26.8% conducted such activities for the public (Q14). Regarding academic activities, a total of 102 English articles related to COVID-19 were published in all hospitals (Q15).
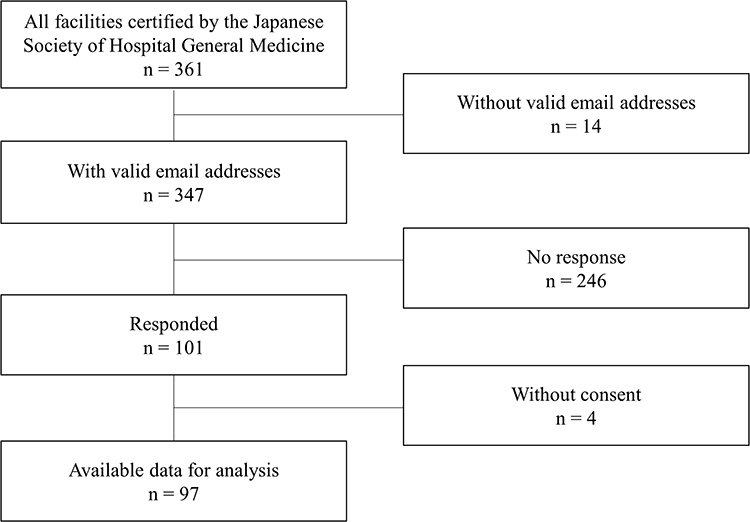 |
Figure 1 Data flow diagram. |
In response to Q16, 79.4% of hospitals answered that “training of personnel who can provide practical care for emerging infectious diseases is necessary”, 78.4% indicated that “the establishment of an infection control system in advance to prepare emerging infectious diseases in the hospital is necessary”, and 74.2% stated that “the establishment of an educational system for responding to emerging infectious diseases (infectious disease crisis management) is necessary” (Table 1). In response to Q17-1, 75.3% of hospitals answered “Yes” to “Would you like to receive education on infectious disease crisis management if given the opportunity?”. Specific themes of interest in infectious disease crisis management education included hospital infection control (ie, infection prevention, zoning, response to an outbreak, triage, hospital management), business continuity planning (BCP), community collaboration, collaboration with public health centers, information on drug-resistant bacteria, crisis management, and knowledge of how to respond to emerging infectious diseases.
Discussion
Japanese hospitalists were involved in COVID-19 medical care in 91.8% of hospitals and played an important role in COVID-19 treatment. Furthermore, many Japanese hospitalists who experienced the COVID-19 pandemic expressed the need for infection control education and personnel development to prepare for future emerging infectious diseases.
During the COVID-19 pandemic, Japanese hospitalists have contributed to COVID-19 patient care and hospital management, similar to hospitalists in the United States. In the United States, hospitalists have a wide range of roles, from frontline activities to organizational leadership in hospitals and health care systems.2 In Japan, hospitalists are expected to perform roles similar to those of hospitalists in the United States,9 not only in patient care but also in hospital management and operation. Furthermore, Japanese hospitalists contributed to the diagnosis of COVID-19, treating patients with COVID-19, and triaging patients with fever or upper respiratory symptoms who regularly visited the hospital. Additionally, hospitalists played an active role in sequelae clinics and clinics monitoring vaccine adverse reactions for patients with COVID-19 in hospitals where these clinics were established, as previously reported.10 In contrast to hospitalists in the United States, Japanese hospitalists have historically contributed not only to inpatient care but also to outpatient care as primary care physicians, and they fulfilled the same roles during the pandemic. This fact illustrates the characteristics and broad contributions of Japanese hospitalists to health care in the country. This study has clarified the roles of hospitalists in Japan during the COVID-19 pandemic. However, it is also essential to continue accumulating evidence regarding their roles in other contexts.
In addition to clinical practice, Japanese hospitalists have contributed to COVID-19 vaccination services and infection prevention education. In other countries, primary care physicians, general practitioners, and family physicians also have essential roles in preventive medicine and primary care.11–13 Japan is known to have strong vaccine hesitancy that is not limited to COVID-19.14 Moreover, the burden on health care workers owing to COVID-19 treatment was substantial, and there was a severe shortage of health care workers to administer vaccines. As a result, the COVID-19 vaccination rate in Japan was low until April 2021.15 However, by October 2021, Japan’s vaccination rate had become one of the highest in the world.15 Apart from the construction of systems by national and local governments, there was a possible contribution by hospitalists to this outcome. The public relies on information from health care professionals, primary care physicians, and public health centers,16 and disease and infection prevention education provided by hospitalists is considered highly useful.
The absence of infection control education for healthcare workers and the lack of preparedness for emergencies caused by emerging infectious diseases are considered major causes of considerable confusion within the medical healthcare system during the COVID-19 pandemic.8 Although the establishment of medical healthcare systems and infrastructure to respond to emerging infectious diseases is essential, cultivating hospital personnel who can treat emerging infectious diseases and manage organizations is also crucial.17 However, despite the emergence of new infectious pathogens such as SARS and novel influenza viruses, education on infectious disease crisis management and preparation against infectious diseases have been insufficient in Japan.18,19 Furthermore, not all hospitals had created manuals for managing emerging infectious diseases by 2015.18 Before the COVID-19 pandemic, crisis management education for emerging infectious diseases was not available for hospitalists in Japan. Infection control education includes basic knowledge and preventive measures related to emerging infectious disease pandemics. Additionally, training in standard precautions is crucial for ensuring learners recognize the importance of infection prevention and practice appropriate measures.17,19 This study further concluded that Japanese hospitalists are interested in specific themes in infectious disease crisis management education, including safety management, emergency response, BCP, the communication of risk, and collaboration with local government and other medical institutions. As with training in infection prevention measures, advance training on these topics can enhance the crisis management of emerging infectious diseases by medical professionals and sufficiently prepare these professionals for future pandemics.
During the pandemic, Japanese hospitalists were involved in the diagnosis and treatment of COVID-19 patients, organizational management and administration, in infection control, and preventive medicine during the pandemic—suggesting that many Japanese hospitalists perceive these tasks as part of their role. The JSHGM specialty program lists infection control, management, and leadership as necessary skills for hospitalists, and hospitalists are expected to take on hospital and organizational management roles.7 Given that the number of infectious disease specialists in Japan is insufficient,9 hospitalists in emerging infectious disease pandemics are expected to play a role not only as front-line healthcare workers but also as leaders in infection prevention and control. However, medical students have reportedly lacked interest in specializing in infectious diseases during the COVID-19 pandemic.20 Therefore, during regular times, government and academic organizations, including general medicine societies such as JSHGM and the Japanese Society of Internal Medicine, must improve education on infectious disease crisis management for Japanese hospitalists in preparation for future emerging infectious disease pandemics. Furthermore, Japanese hospitalists are expected to actively participate in pre- and post-graduate education to cultivate a substantial number of clinical doctors across all medical fields with skills in infectious disease crisis management.
There are several limitations to this study. First, this study focused exclusively on hospitals certified by JSHGM. Second, the survey was conducted only among the chairpersons. Third, the response rate to the questionnaire was low. For these reasons, there is a possibility that it may not accurately reflect the realities of hospitalists in Japan. Therefore, further research targeting individual hospitalists is required to clarify the true contributions of hospitalists to the COVID-19 pandemic and to evaluate the necessity of infectious disease crisis management education.
Conclusions
In conclusion, during the pandemic, in addition to inpatient care, Japanese hospitalists provided outpatient care for COVID-19, which is the role of primary care physicians in other countries. They also contributed to hospital management, infection control, and vaccination. Furthermore, Japanese hospitalists who experienced the COVID-19 pandemic expressed the need for personnel development and education to prepare for future emerging infectious disease pandemics. Therefore, government and academic societies must enhance education on infectious disease crisis management for Japanese hospitalists in preparation for future pandemics.
Abbreviations
BCP, business continuity planning; COVID-19, coronavirus disease 19; JSHGM, Japanese Society of Hospital General Medicine; SARS, severe acute respiratory syndrome; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by Ethics Committee of Okayama University Hospital (No. 2212-043).
Patient Consent Statement
We obtained consents from all the participants.
Acknowledgment
We thank Dr. Eric Howell, Chief Executive Officer, Society of Hospital Medicine for giving us an expert opinion. We also thank Analisa Avila and Anahid Pinchis of Edanz for editing a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported with respect to the conception, study design, execution, acquisition of data, analysis, and interpretation. All authors took part in drafting, revising, or critically reviewing the article and gave their final approval of the version submitted for publication. All the authors have agreed on the journal for submission and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Dr Masaki Tago and Dr Naoko E Katsuki report grants from Japan Society for the Promotion of Science and Japanese Society of Hospital General Medicine, outside the submitted work. The authors declare no other conflicts of interest associated with this manuscript.
References
1. Wang Z, Duan Y, Jin Y, Zheng ZJ. Coronavirus disease 2019 (COVID-19) pandemic: how countries should build more resilient health systems for preparedness and response. Glob Health J. 2020;4(4):139–145. doi:10.1016/j.glohj.2020.12.001
2. Bowden K, Burnham EL, Keniston A, et al. Harnessing the power of hospitalists in operational disaster planning: COVID-19. J Gen Intern Med. 2020;35(9):2732–2737. doi:10.1007/s11606-020-05952-6
3. Dugani SB, Geyer HL, Maniaci MJ, Fischer KM, Croghan IT, Burton C. Psychological wellness of internal medicine hospitalists during the COVID-19 pandemic. Hosp Pract. 2021;49(1):47–55. doi:10.1080/21548331.2020.1832792
4. Hauck KD, Hochman KA, Pochapin MB, et al. The COVID-19 army: experiences from the deployment of non-hospitalist physician volunteers during the COVID-19 pandemic. Disaster Med Public Health Prep. 2021:1–5. doi:10.1017/dmp.2021.109
5. Tago M, Watari T, Shikino K, Sasaki Y, Takahashi H, Shimizu T. Five tips for becoming an ideal general hospitalist. Int J Gen Med. 2021;14:10417–10421. doi:10.2147/IJGM.S341050
6. Iwata K. Quantitative and qualitative problems of infectious diseases fellowship in Japan. Int J Infect Dis. 2013;17(12):e1098–9. doi:10.1016/j.ijid.2013.07.009
7. Japanese Society of Hospital General Medicine. Training guidelines of hospitalist specialty program. Japanese: http://hgm-japan.com/wp-content/uploads/2021/08/kenkyu_shishin_2.pdf.
8. Desborough J, Dykgraaf SH, Phillips C, et al. Lessons for the global primary care response to COVID-19: a rapid review of evidence from past epidemics. Fam Pract. 2021;38(6):811–825. doi:10.1093/fampra/cmaa142
9. Tago M, Watari T, Shikino K, Sasaki Y, Takahashi H, Shimizu T. A statement on the ten skills characteristic of exemplary Japanese hospitalist practice. J Hosp Gen Med. 2021;3(2):68–70.
10. Otsuka Y, Tokumasu K, Nakano Y, et al. Clinical characteristics of Japanese patients who visited a COVID-19 aftercare clinic for post-acute sequelae of COVID-19/long COVID. Cureus. 2021;13(10):e18568. doi:10.7759/cureus.18568
11. Cohidon C, Imhof F, Bovy L, Birrer P, Cornuz J, Senn N. Patients’ and general practitioners’ views about preventive care in family medicine in Switzerland: a cross-sectional study. J Prev Med Public Health. 2019;52(5):323–332. doi:10.3961/jpmph.19.184
12. Prieto-Campo Á, García-Álvarez RM, López-Durán A, et al. Understanding primary care physician vaccination behaviour: a systematic review. Int J Environ Res Public Health. 2022;19(21):13872. doi:10.3390/ijerph192113872
13. Kidd M, de Toca L, Kelly P. Editorial: the invaluable contributions of general practice to Australia’s COVID-19 pandemic response. Aust J Gen Pract. 2022;51(12):917–918. doi:10.31128/AJGP-11-22-6604
14. de Figueiredo A, Simas C, Karafillakis E, Paterson P, Larson HJ. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. Lancet. 2020;396(10255):898–908. doi:10.1016/S0140-6736(20)31558-0
15. Mori H, Naito T. A rapid increase in the COVID-19 vaccination rate during the Olympic and Paralympic games 2021 in Japan. Hum Vaccin Immunother. 2022;18(1):2010440. doi:10.1080/21645515.2021.2010440
16. Malik AA, McFadden SM, Elharake J, Omer SB. Determinants of COVID-19 vaccine acceptance in the US. eClinicalMedicine. 2020;26:100495. doi:10.1016/j.eclinm.2020.100495
17. Kato S, Miyakuni Y, Inoue Y, Yamaguchi Y. Maximizing health-care capacity in response to COVID-19 outbreak: rapid expansion through education by health emergency and disaster experts. Disaster Med Public Health Prep. 2021;15(2):e46–e48. doi:10.1017/dmp.2020.264
18. Kudo D, Sasaki J, Ikeda H, et al. Committee for infection control for the emergency department, the Japanese Association for acute medicine, and the joint working group. A survey on infection control in emergency departments in Japan. Acute Med Surg. 2018;5(4):374–379. doi:10.1002/ams2.360
19. Imai T, Takahashi K, Todoroki M, et al. Perception in relation to a potential influenza pandemic among healthcare workers in Japan: implications for preparedness. J Occup Health. 2008;50(1):13–23. doi:10.1539/joh.50.13
20. Hagiya H, Otsuka Y, Tokumasu K, et al. Interest in infectious diseases specialty among Japanese medical students amidst the COVID-19 pandemic: a web-based, cross-sectional study. PLoS One. 2022;17(4):e0267587. doi:10.1371/journal.pone.0267587
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.