Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Continuous Reduction of Hypoglycemia Incidence Post-Endoscopic Polypectomy Through Quality Control Circle Implementation
Authors Yuan S, Yu B, Song L, Chen L, Hong F ![]()
Received 17 March 2025
Accepted for publication 2 September 2025
Published 6 September 2025 Volume 2025:18 Pages 5621—5634
DOI https://doi.org/10.2147/JMDH.S524337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Shan Yuan, Bingjing Yu, Lingyun Song, Linping Chen, Fenfen Hong
Division of Gastroenterology, Ningbo Yinzhou No.2 Hospital, Ningbo, Zhejiang, People’s Republic of China
Correspondence: Fenfen Hong, Division of Gastroenterology, Ningbo Yinzhou No.2 Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China, Email [email protected]
Objective: This study aimed to reduce the incidence of hypoglycemia following endoscopic polypectomy by implementing Quality Control Circle (QCC) interventions.
Methods: Quality Control Circle (QCC) empowered clinicians to implement PDCA-driven protocol refinements, standardizing care processes to mitigate hypoglycemia risk. Establish a QCC team to investigate the current incidence of hypoglycemia in post-polypectomy patients, conduct a root cause analysis to identify the true causes, formulate corresponding countermeasures, and implement them in phases. The study was conducted in two phases: before-QCC (517 patients from March 13 to May 31, 2023) and after-QCC (1090 patients from June 1 to November 30, 2023). The primary outcome was the incidence of hypoglycemia.
Results: Before QCC implementation, the incidence of hypoglycemia was 6.63%. Following the introduction of QCC interventions, the incidence significantly decreased to 2.94% (p< 0.01). Monthly data revealed a continuous decline in hypoglycemia incidence, with rates dropping from 4.12% in June to 1.47% in November, and the results are statistically significant (p< 0.001). Other confounding factors, including age, gender, education level, diabetes history, polyp size, site, and fasting duration, were not significantly associated with the outcome (p> 0.05).
Conclusion: This study effectively reduced the incidence of hypoglycemia in patients following endoscopic polypectomy through the implementation of QCC activities, significantly enhancing patient safety and treatment outcomes. The successful implementation of the project validated the important role of QCC in continuous quality improvement, providing valuable experience and methods for future clinical nursing management.
Keywords: Quality Control Circle, hypoglycemia, polypectomy, incidence, nursing management
Introduce
Endoscopic polypectomy is a minimally invasive procedure used to excise polyps from the gastrointestinal tract, most commonly during a colonoscopy. Polyps, which can be benign or precancerous, are removed using biopsy forceps or a snare that cauterizes the base, thereby preventing potential malignancies.1 This procedure is essential for colorectal cancer screening and prevention.2 By enabling the histopathological examination of excised polyps, endoscopic polypectomy aids in early diagnosis and management of various gastrointestinal conditions, significantly contributing to patient outcomes and overall public health.3
Hypoglycemia is defined as a fasting blood glucose concentration below 2.8 mmol/L in adults.4 In diabetic patients, a blood glucose value of ≤3.9 mmol/L can be diagnosed as hypoglycemia.4 Hypoglycemia is a clinical syndrome characterized by abnormally low plasma glucose levels, with symptoms predominantly due to adrenergic activation and neuroglycopenia, resulting from various etiologies.5 Common symptoms include diaphoresis, hunger, palpitations, tremors, and pallor, while severe hypoglycemia can present with cognitive impairment, agitation, irritability, seizures, and even coma.6 In this continuous quality improvement project, any occurrence of similar symptoms is considered as potential hypoglycemia. Patients are required to undergo bowel preparation prior to endoscopic procedures, leading to reduced caloric intake, fasting for 12 hours preoperatively, and continued fasting for 4–6 hours or longer postoperatively. Often, blood glucose monitoring is insufficient, and fluid supplementation is inadequate, frequently precipitating hypoglycemic events that can result in serious complications such as neurological impairment or mortality.7
Quality Control Circles (QCCs) in healthcare are groups of healthcare professionals who voluntarily meet to identify, analyze, and solve work-related problems.8 They have been found to improve standards of practice, enhance professional development, and increase psychological well-being among general practitioners.9 For instance, a problem-solving oriented QCC might focus on reducing the rate of surgical site infection.10 QCCs have also been associated with enhancing perceptions of patient safety culture among hospital staff.9 Despite the significant clinical implications of post-polypectomy hypoglycemia, evidence-based preventive strategies remain limited. Previous studies have predominantly focused on perioperative glucose management in diabetic patients,11 with scant evidence addressing procedure-specific risks in heterogeneous populations. Furthermore, although Quality Control Circle (QCC) have proven effective in reducing hospital-acquired infections12 and medication errors,13,14 their application to complications following therapeutic endoscopy has not been documented. This study addresses these gaps by implementing a structured QCC initiative to mitigate hypoglycemia following polypectomy.
Patient
This study is a prospective study divided into two major groups. The investigation group (before QCC) included all patients in our department who underwent endoscopic polypectomy from March 13 to May 31, 2023, totaling 517 patients. The improvement group (after QCC) included all patients in our department who underwent endoscopic polypectomy from June 1 to November 30, 2023, totaling 1090 patients.
Ethics and Confidentiality Statement
This study was approved by the Ethics Committee of Ningbo Yinzhou No.2 Hospital and the methods were carried out in accordance with the approved guidelines. Given the retrospective nature of the study and the use of de-identified patient data, the requirement for informed consent was waived by the IRB. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments. All patient data were anonymized and handled in accordance with applicable data protection regulations. Personal identifiers were removed prior to analysis to ensure confidentiality.
Study Design
Quality Control Circle (QCC) activities are conducted based on QCC theory and are divided into three phases. First, a QCC team is established, selecting the objective of reducing the incidence of hypoglycemia following endoscopic polypectomy. Second, the team analyzes the reasons for the high incidence of post-polypectomy hypoglycemia, formulates strategies, and implements them. Third, the results are validated, and standardized protocols are developed. Hypoglycemic events were identified if any of the following criteria were met: (a) Fingerstick glucose <2.8 mmol/L in non-diabetic individuals; (b) Fingerstick glucose ≤3.9 mmol/L in diabetic patients; (c) Acute neurogenic or neuroglycopenic symptoms (eg, palpitations, diaphoresis, seizures, or cognitive impairment) resolving promptly after oral/intravenous glucose administration, regardless of glucose documentation. Capillary blood glucose was measured using standardized glucometers (Accu-Chek® Performa, Roche Diagnostics).
QCC Activity
QCC Team
The QCC team consists of ten healthcare professionals from the Department of Gastroenterology at Ningbo Yinzhou NO.2 Hospital. The team includes one advisor, one circle leader, and eight circle members. The members range in age from 28 to 52 years, with an average age of 33 years. The QCC team comprises four gastroenterologists and six gastroenterology nurses, including one head nurse.
Theme Selection
The QCC members collect issues encountered in their work or clinical practice and systematically extract several themes from the feedback. These themes are evaluated using a scoring method based on four criteria: leadership attention, feasibility, urgency, and circle capability. Each member rates all themes on these four criteria using a scale where 5 is the highest score, 3 is moderate, and 1 is the lowest. The theme with the highest overall score is selected as the focus of the activity. Ultimately, we identified “Reducing the Incidence of Hypoglycemia in Patients Following Endoscopic Polypectomy” as the theme. The evaluation criterion for this theme is the “Incidence of Hypoglycemia in Patients Following Endoscopic Polypectomy” [Incidence = (Number of patients with hypoglycemia after endoscopic polypectomy ÷ Total number of patients who underwent endoscopic polypectomy during the study period) × 100%].
QCC Plan
Status Survey
This activity begins with a survey of the incidence of hypoglycemia following endoscopic polypectomy in our department from 2023/03/13 to 2023/04/30. The detailed assessment process is outlined in Figure 1. The survey results indicated that from 2023/03/13 to 2023/04/30, a total of 300 patients were monitored post-polypectomy, with 20 cases of hypoglycemia reported. Based on the survey results, the overall incidence of hypoglycemia before the QCC activity was 6.67%. The ten QCC members rated the causes of hypoglycemia in the 20 patients, as shown in Figure 2. Using the 80/20 rule and Pareto analysis, the primary reasons for hypoglycemia following endoscopic polypectomy were identified as patients’ lack of awareness about hypoglycemia, inadequate preventive measures by healthcare providers, and insufficient screening for high-risk patients by healthcare providers. These three factors accounted for a cumulative percentage of 81.25%.
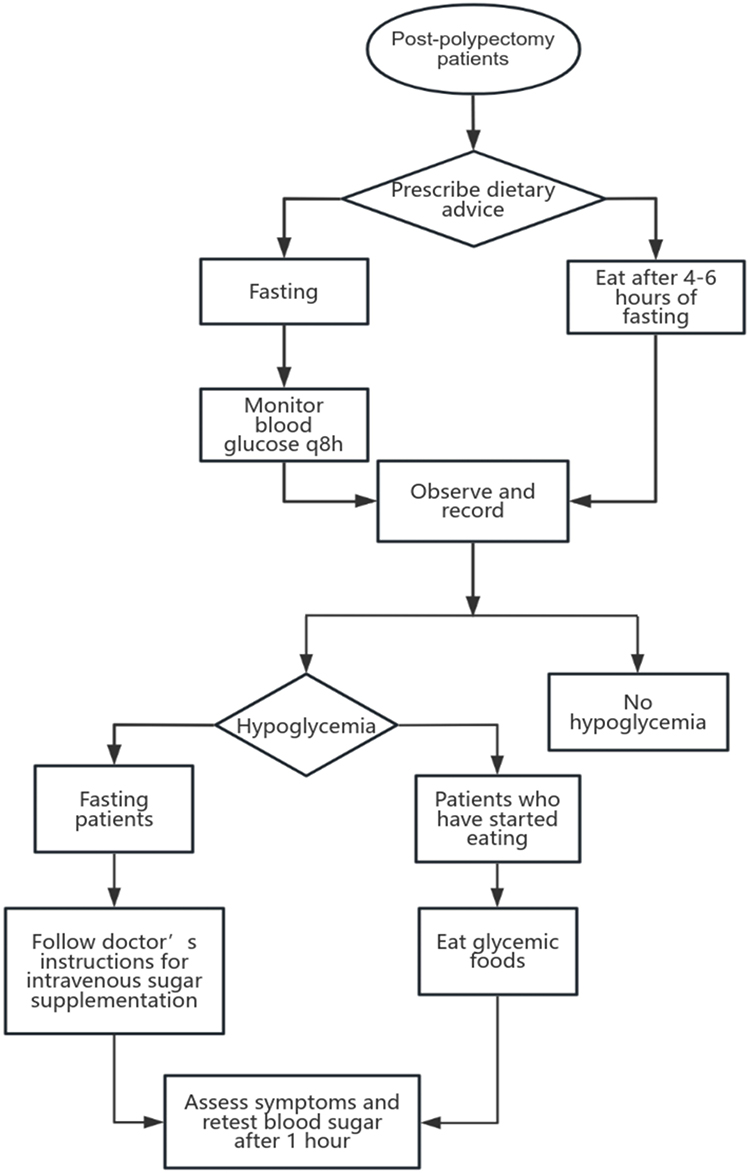 |
Figure 1 The blood glucose assessment process for patients after endoscopic polypectomy (before QCC). |
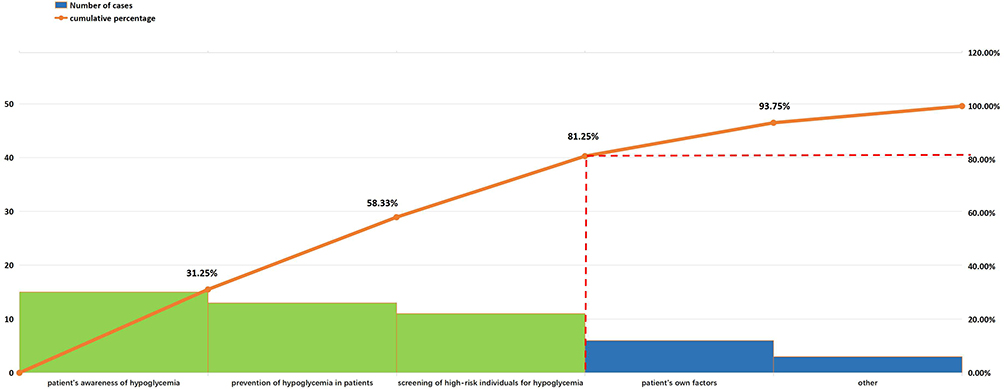 |
Figure 2 Pareto analysis of the reason for hypoglycemia after endoscopic polypectomy. |
The target value for this QCC activity is calculated using the formula: Improvement Value = Current Value × Improvement Focus × Circle Capability = 6.67% × 81.25% × 65.9% = 3.57%. Therefore, the target value is: Current Value – Improvement Value = 6.67–3.57% = 3.1%. The objective of this activity is to reduce the incidence of hypoglycemia following endoscopic polypectomy to below 3.1%.
Based on these three major factors, organize the QCC team members to conduct a brainstorming session, gather ideas, and list all possible causes related to these three factors. Use the four main categories—Human, materials, Management, and Environment—to create three fishbone diagrams, as shown in Figures3–5.
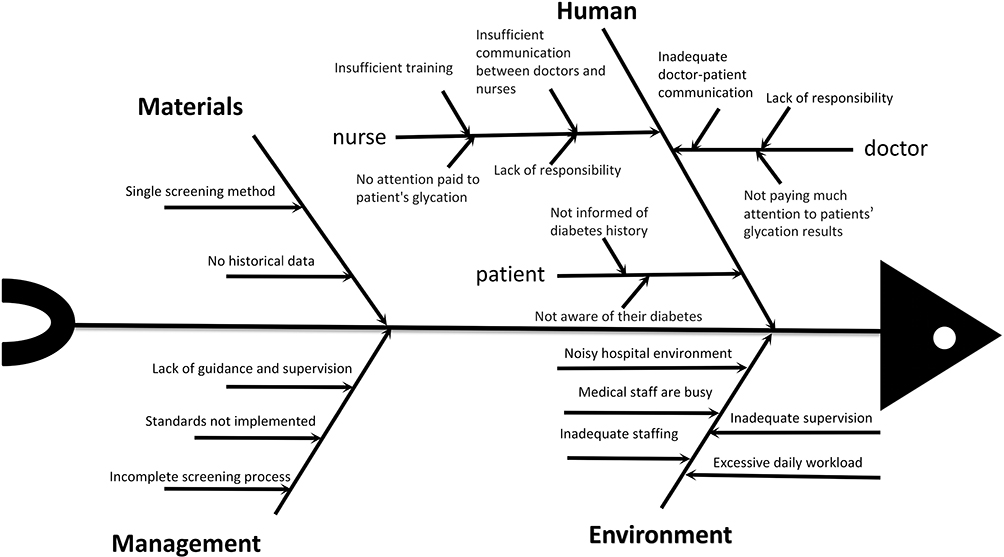 |
Figure 3 The reasons for inadequate screening of high-risk populations for post-polypectomy hypoglycemia by healthcare professionals in a fishbone diagram. |
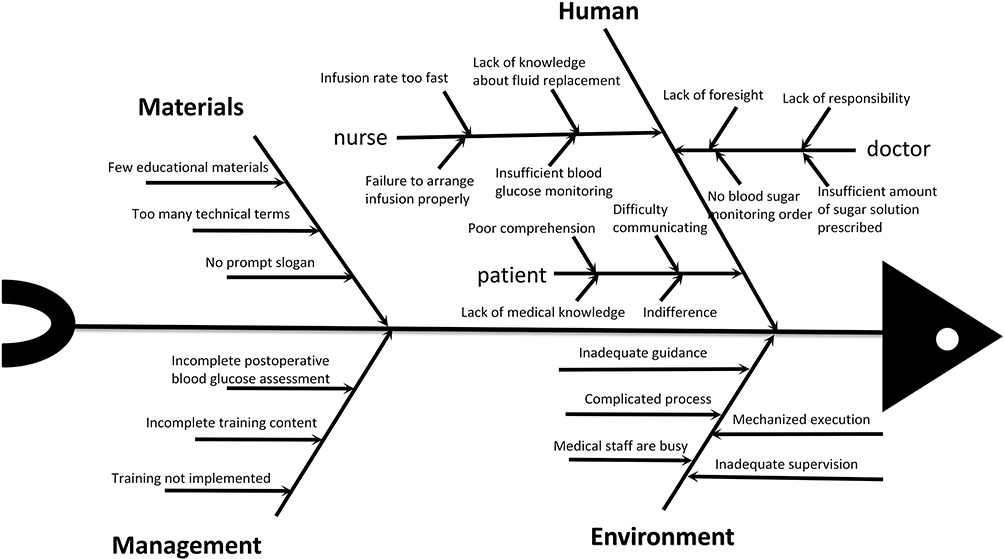 |
Figure 4 Reasons for healthcare professionals’ low awareness of hypoglycemia prevention after endoscopic polypectomy in a fishbone diagram. |
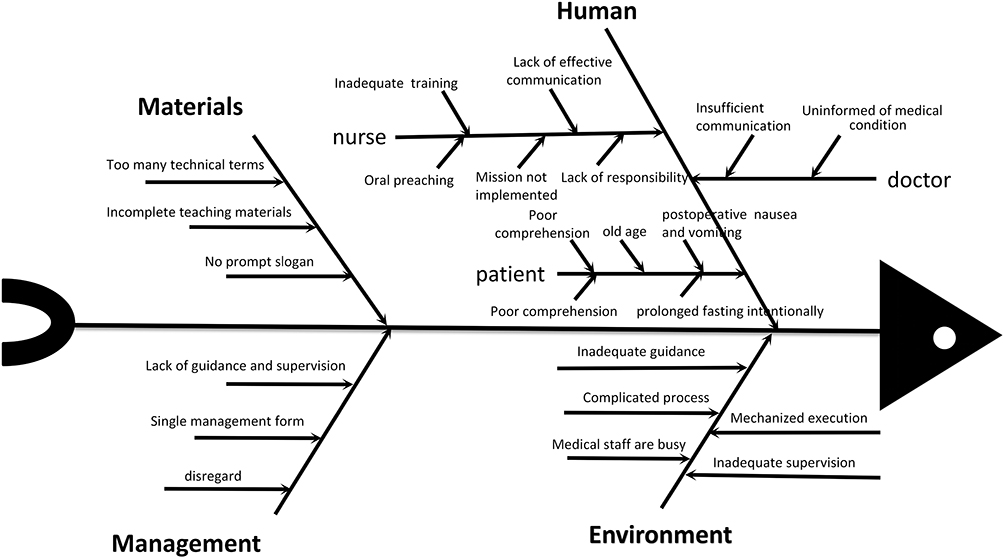 |
Figure 5 Reasons for patients’ lack of awareness about hypoglycemia in a fishbone diagram. |
In-Depth Analysis
During May 1–31, 2023, QCC members investigated 217 cases of endoscopic surgery patients to verify the true causes identified. This was done through the use of checklists, retrospective review of electronic medical records, on-site interviews, and direct questioning/observation. A Pareto chart was drawn based on the findings, as shown in Figure 6. According to the 80/20 rule, the top six true causes of post-endoscopic polypectomy hypoglycemia were identified as follows: incomplete postoperative blood glucose assessment, incomplete educational materials, unreasonable blood glucose monitoring orders, lack of knowledge related to fluid replacement, single preaching method, and not paying attentions to the patient’s glycation results.
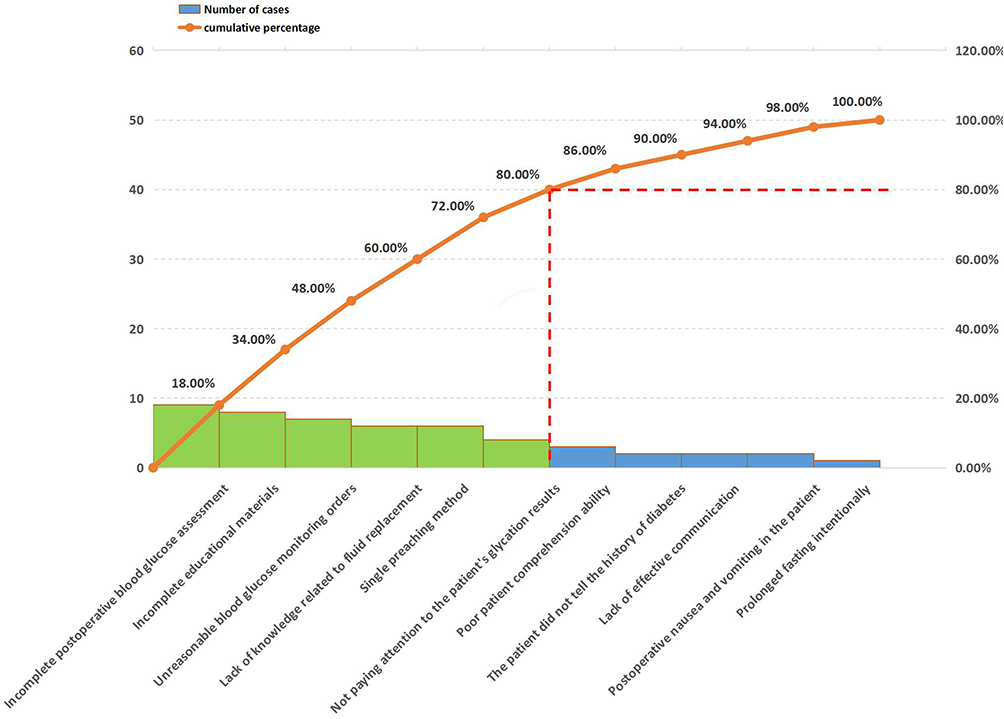 |
Figure 6 Pareto analysis of the primary factors of hypoglycemia in patients following endoscopic polypectomy. |
Countermeasure Formulation
The QCC team conducted another brainstorming session to propose multiple countermeasures for the identified root causes. The ten QCC members evaluated these countermeasures based on feasibility, effectiveness, and circle capability. Countermeasures scoring above 90 were selected as refined strategies for this activity.
Strategy 1: Review and streamline the current evaluation and management process for hypoglycemia in patient post-endoscopic polypectomy. Develop and implement the “Evaluation and Management Process for Hypoglycemia in Patients Post-Endoscopic Polypectomy”. The improved process flowchart is shown in the Figure 7.
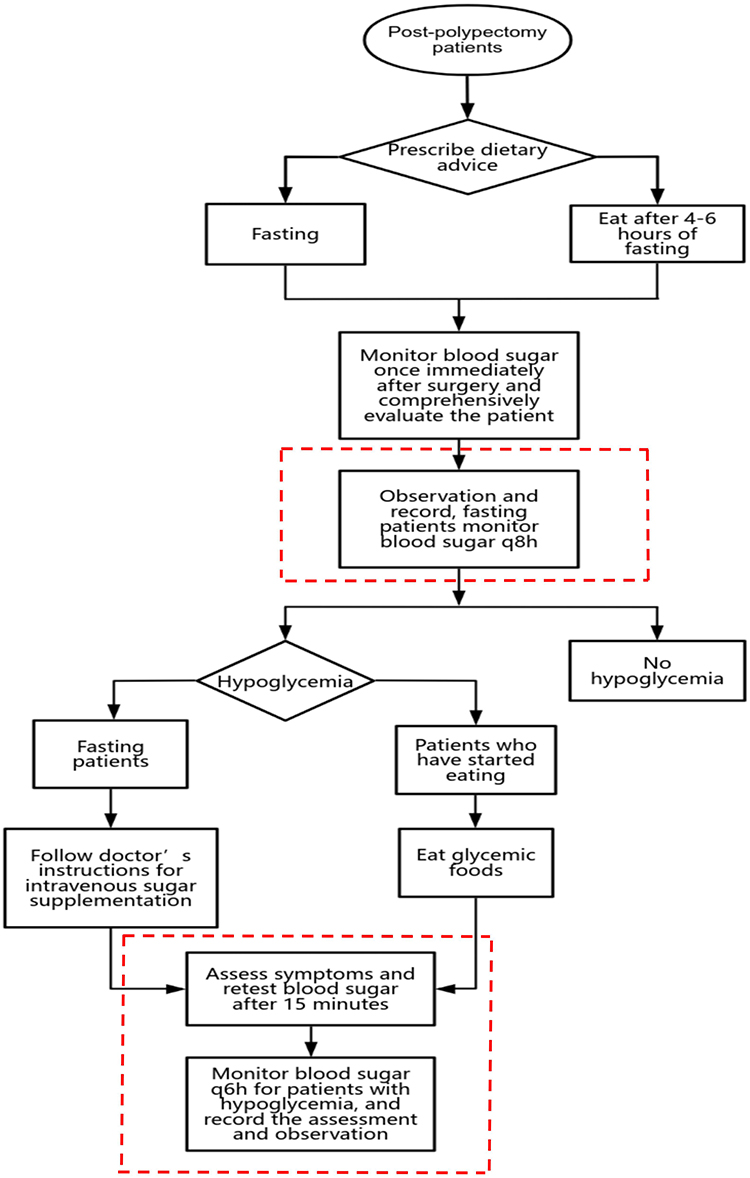 |
Figure 7 The blood glucose assessment process for patients after endoscopic polypectomy (after QCC). |
Strategy 2: Enhancing healthcare providers’ awareness of hypoglycemia risk prevention in patients after endoscopic polypectomy. Organize and identify high-risk groups prone to hypoglycemia based on departmental characteristics, and provide a risk notification and emergency response signature for hypoglycemia. Organize training sessions for departmental nurses on fluid therapy-related knowledge. Supervise doctors to ensure the appropriate prescription of blood glucose orders and timely blood glucose monitoring.
Strategy 3: Enhancing Patient Awareness of Hypoglycemia. Develop and implement “Hypoglycemia Prevention” warning signs for clinical use. Create and display “Beware of Hypoglycemia” educational posters on walls. Conduct two health seminars focused on hypoglycemia.
Statistical Analysis
The data were analyzed using SPSS version 24.0. Comparisons between two groups of quantitative data were performed using the t-test. For comparisons among multiple groups of quantitative data, analysis of variance (ANOVA) was employed. Chi-square tests were used to analyze categorical data between two groups. To detect trends across multiple groups of categorical data, linear regression analysis was applied. Multivariable logistic regression to examine the impact of multiple factors on categorical variables. p<0.01 was considered statistically significant.
Result
Tangible Results
From March 13th to May 31st, the preliminary investigation phase, a total of 517 post-polypectomy patients were recorded, of which 33 patients experienced hypoglycemia, resulting in a hypoglycemia incidence rate of 6.63%. After the gradual implementation of countermeasures, from June to November, a total of 1090 post-polypectomy patients were recorded. There were no statistically significant differences between the two groups in terms of age, gender, education level, history of diabetes, duration of postoperative fasting, polyp size, or polyp location (p>0.05), as shown in the Table 1. The incidence of hypoglycemia after polypectomy before the QCC (March 13th to May 31st) was 6.63%, while the total incidence of hypoglycemia after the QCC (June 1st to November 30th) was 2.94%. The difference in the incidence of post-polypectomy hypoglycemia between these two groups was statistically significant (p<0.01), as shown in the Table 2.
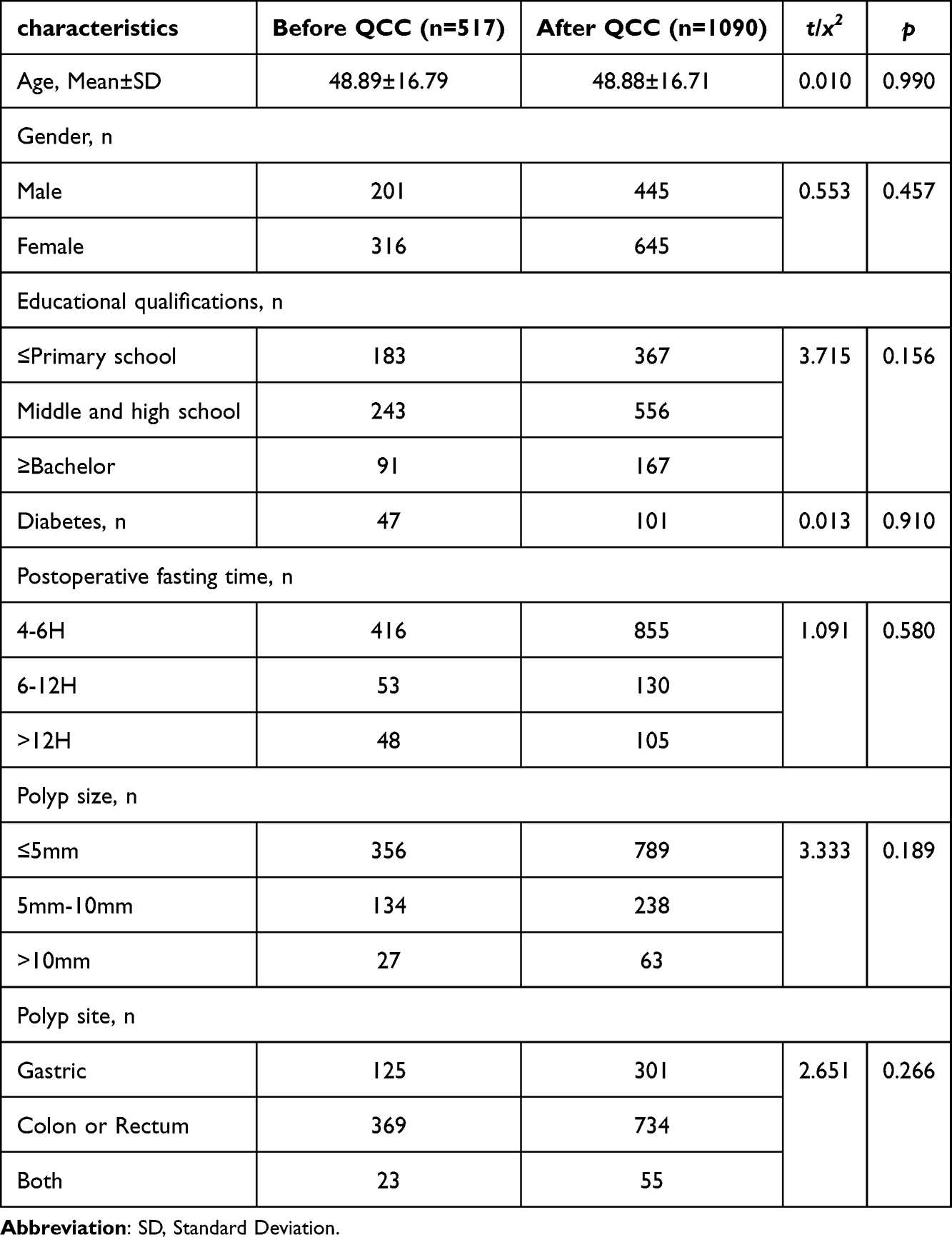 |
Table 1 Patient Characteristics Before QCC and After QCC |
 |
Table 2 Comparison of Hypoglycemia Incidence in Patients After Endoscopic Polypectomy Before and After QCC |
To assess the impact of various factors on the outcome, we performed a multivariable logistic regression analysis, controlling for potential confounders. The results are summarized in Table 3. The QCC intervention was significantly associated with a reduced likelihood of the outcome (aOR = 0.44, 95% CI: 0.27–0.72, p<0.01). Age, gender, educational qualifications, and diabetes status were not significantly associated with the outcome. Postoperative fasting time, polyp size, and polyp site had also no significant effect on the outcome (p>0.05).
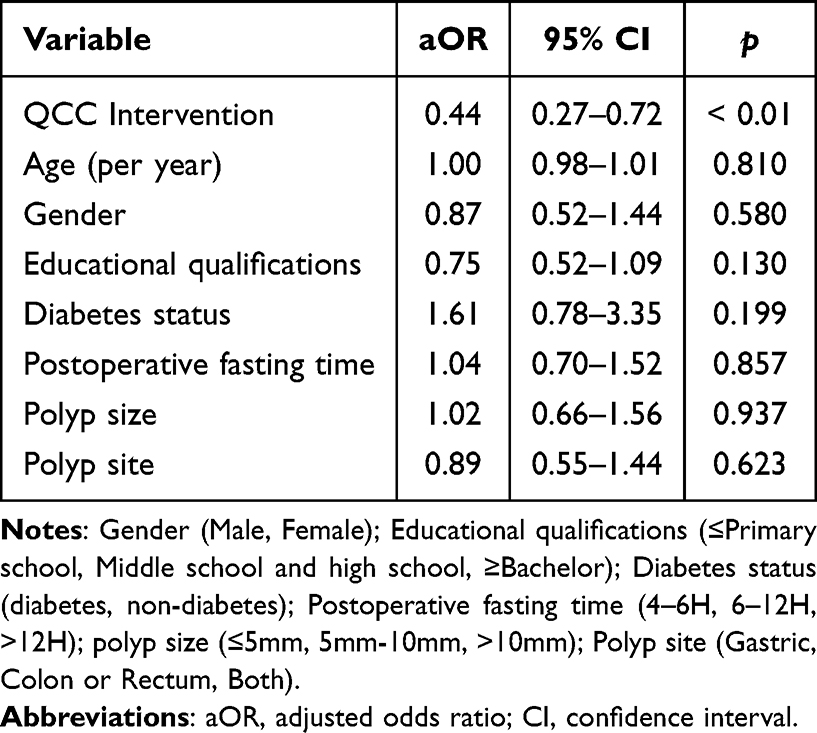 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with Post-Polypectomy Hypoglycemia |
Monthly data reveals the following: In June, 194 post-polypectomy patients were recorded, with 8 cases of hypoglycemia, resulting in an incidence rate of 4.12%. In July, among 192 patients, 7 experienced hypoglycemia, yielding a rate of 3.65%. August saw 198 patients with 6 cases of hypoglycemia, leading to a 3.03% incidence rate. In September, 142 patients were recorded, with 4 cases of hypoglycemia and a rate of 2.82%. October included 160 patients, 4 of whom experienced hypoglycemia, resulting in a 2.50% rate. By November, 204 patients were recorded, with 3 cases of hypoglycemia, bringing the incidence down to 1.47%. Following the implementation of QCC-related measures, the monthly incidence of hypoglycemia in post-polypectomy patients gradually decreased. The differences in the probability of hypoglycemia occurrence across different months were statistically significant (p<0.001), as shown in the Table 4 and Figure 8.
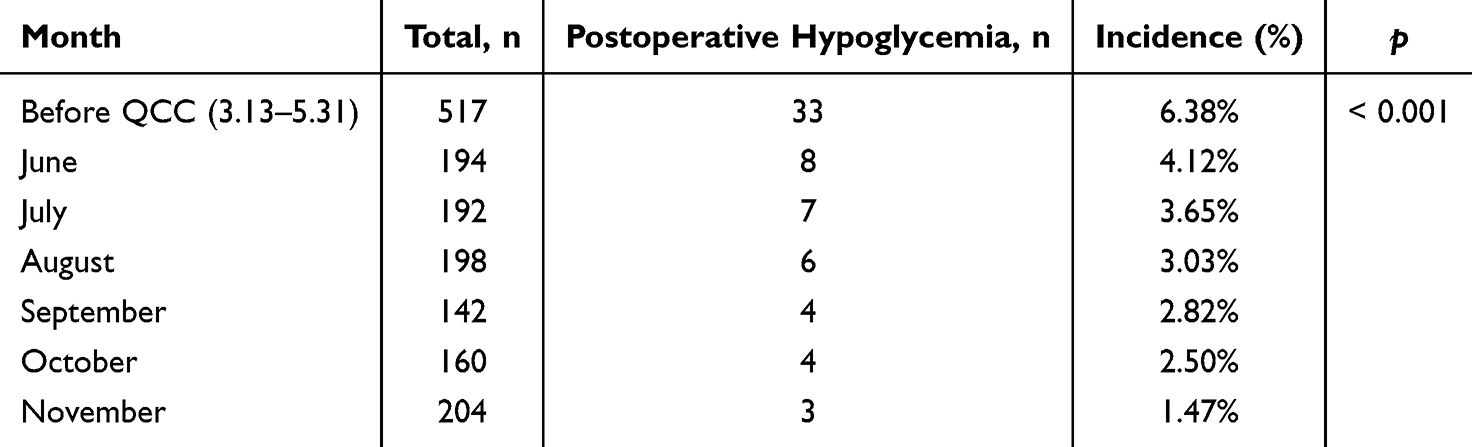 |
Table 4 Monthly Comparison of Hypoglycemia Incidence in Post-Polypectomy Patients Following QCC Implementation |
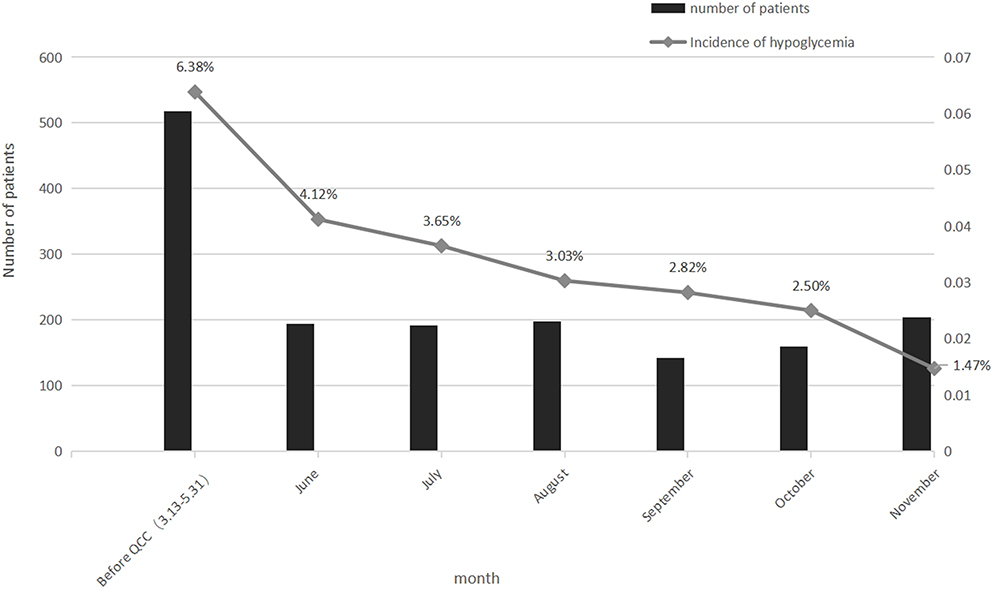 |
Figure 8 Line chart showing monthly hypoglycemia rates in post-polypectomy patients following QCC implementation. |
Linear regression analysis (Table 5) demonstrated a significant inverse relationship between months post-QCC implementation and hypoglycemia incidence (β=−0.943, p<0.001). For each additional month of intervention, the incidence decreased by 0.9% (B=−0.009), with the model explaining 88.7% of variance (aR²=0.887). This reflects the cumulative effect of QCC measures—hypoglycemia risk declined linearly as quality improvement processes matured, free from multicollinearity concerns (VIF=1.0). Coupled with prior logistic regression findings (aOR=0.44), these results confirm that QCC not only provides immediate benefits but also exhibits progressively strengthening protection over time.
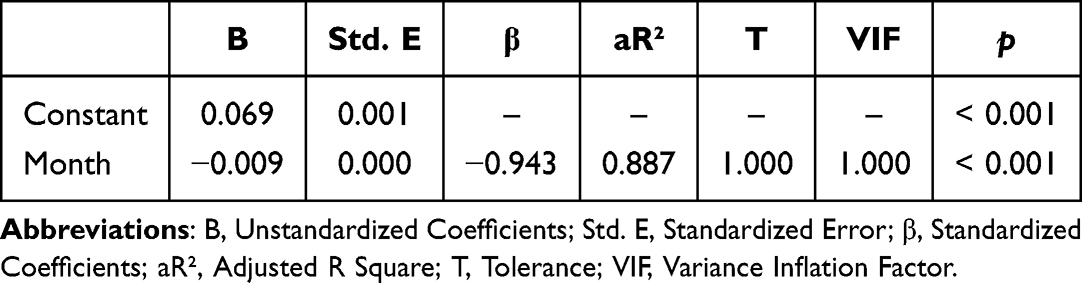 |
Table 5 The Linear Regression Analysis of the Incidence of Hypoglycemia in Post-Polypectomy Patients with the Implementation of QCC Over Subsequent months |
Intangible Results
The self-evaluation questionnaire regarding awareness of hypoglycemia risk, team cohesion, communication skills, personal self-confidence, sense of responsibility, activity enthusiasm, problem detection ability, and quality control skills has been completed. The circle members rated each item with a maximum score of 5 and a minimum score of 1, with a total score of 50, and the results were presented in the form of a radar chart. As shown in the Figure 9, after completing the QCC activities, the circle members’ abilities in the above aspects have significantly improved.
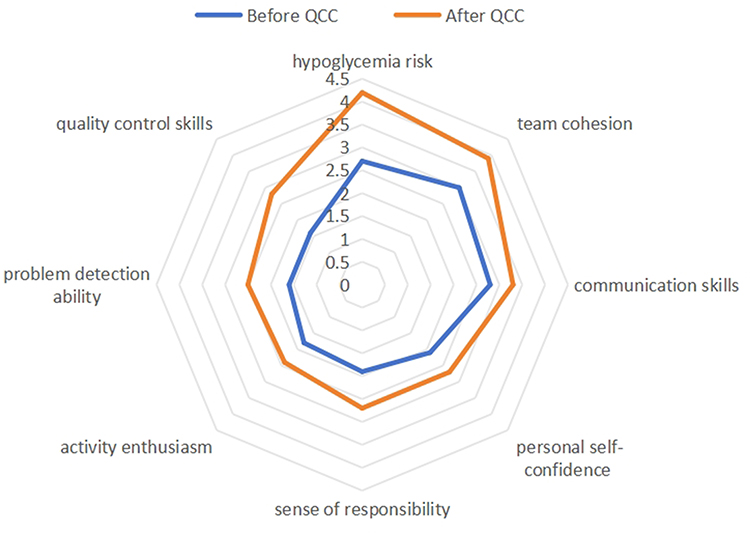 |
Figure 9 Analysis of the circle capability by radar diagram. |
Standardization
The QCC team developed a flowchart for hypoglycemia assessment and management in patients after endoscopic polypectomy, as well as the “Prevention Plan for Hypoglycemia in Post-Polypectomy Patients of the Gastroenterology Department”. Additionally, the team completed the production of a wall-mounted educational chart titled “Beware of Hypoglycemia” and warning signs labeled “Prevent Hypoglycemia”, all of which have been applied in clinical practice.
Discussion
Postoperative hypoglycemia is a common and potentially serious complication,15 especially after procedures like endoscopic polypectomy. The risk of hypoglycemia increases postoperatively due to continued fasting and insufficient fluid supplementation. Hypoglycemia can trigger a range of symptoms, such as sweating, palpitations, tremors, and mental confusion.16,17 In severe cases, it may lead to altered consciousness, seizures, or coma,18 thereby impacting overall recovery and treatment outcomes. Studies have shown that postoperative hypoglycemia following elective craniotomy is associated with increased mortality rates, with patients experiencing hypoglycemia post-surgery having a relatively higher risk of death.19 Articles report that effective blood glucose management can significantly reduce the risk of postoperative infections, thereby improving outcomes for diabetic patients undergoing complex neurosurgical procedures.20 There are also reports linking postoperative hypoglycemia with outcomes in cardiac surgery patients, showing an association between hypoglycemia and higher complication rates, prolonged hospital stays, and increased mortality.21 Timely blood glucose monitoring, nutritional support, and fluid supplementation are essential in postoperative care. Increasing hypoglycemia awareness among the medical team, especially for high-risk patients, along with educating patients and families on symptoms and responses, can reduce hypoglycemia incidents and improve safety and satisfaction. Standardized glucose monitoring and management protocols are crucial for postoperative safety.
This study investigated the efficacy of implementing a Quality Control Circle (QCC) to reduce the incidence of hypoglycemia following endoscopic polypectomy. The findings demonstrate that QCC-led interventions significantly lowered the rate of post-polypectomy hypoglycemia, achieving a reduction from 6.63% to 2.94% over the study period. These results indicate that the systematic use of QCC methods can be highly effective in addressing specific patient safety issues, particularly in the prevention of hypoglycemia, which has not been a common focus in endoscopic procedures previously.
The marked improvement can be attributed to the multifaceted approach undertaken by the QCC team. By identifying critical factors, such as the lack of patient education, incomplete postoperative blood glucose assessments, and inadequate screening of high-risk patients, targeted interventions were formulated. These strategies, including enhanced blood glucose monitoring, improved staff education, and the development of standardized care protocols, directly addressed the root causes of hypoglycemia in this patient cohort. The use of a structured fishbone diagram and Pareto analysis to isolate key issues demonstrates the utility of QCC tools in systematically improving healthcare quality.
The core triggers of perioperative hypoglycemia (such as prolonged preoperative fasting, effects of sedation/anesthesia, delayed postoperative feeding, and variations in diabetes management) are commonly observed in many patient populations undergoing similar short-term procedures or interventions. Departments involved in day surgeries or endoscopic procedures face similar challenges in postoperative glucose management.22,23 The core of this project lies in the systematic framework provided by Quality Control Circle (QCC), rather than being limited to specific technical details, giving it broad applicability for wider implementation. For instance, a multidisciplinary team collaboration model, where a QCC team comprising doctors, nurses, and anesthesiologists works together to analyze issues, develop, and implement improvement measures, is highly applicable. The use of a fishbone diagram to analyze the various factors leading to hypoglycemia is also a universal analytical method. Additionally, the standardized process tools produced by this project, including the postoperative assessment flowchart, the “Post-Polypectomy Hypoglycemia Prevention Plan” for gastroenterology patients, and the “Beware of Hypoglycemia” educational wall chart, are valuable outputs that can be directly adopted or localized by other institutions. Furthermore, support from leadership at the institutional level, such as the establishment of a quality improvement center to provide training and coordinate resource sharing, will greatly facilitate successful implementation.
However, several limitations should be acknowledged. First, the implementation of QCC may have introduced a Hawthorne effect,24,25 where healthcare providers modify their behavior due to awareness of being observed, potentially inflating the observed effectiveness. This bias could be mitigated by extending the monitoring period and implementing further blinded or multi-center studies to confirm the findings.26 Second, the intervention in this study is multifaceted (including optimization and evaluation of management processes, raising awareness among healthcare professionals, organizing staff training, and multiple patient education efforts), which is a typical feature of QCC in addressing complex system problems. As the components work synergistically to drive the final improvement, it is challenging to isolate the independent contribution of each individual component. However, through process evaluation, we can explore the key driving factors. During debriefing meetings and interviews with the project team, QCC members generally agreed that optimizing the postoperative blood glucose assessment process and improving educational materials were crucial, though this conclusion was based solely on internal voting among members without objective data to support it. Nevertheless, we cannot deny that the coordination effect within the QCC project may also have been a key factor in its success, even though it limits the ability to precisely quantify the contribution of each independent component. Based on this, it is suggested that future studies adopt a stepwise wedge design to introduce different components in phases across departments or time periods. Alternatively, more in-depth process evaluations can be conducted, including more systematic observations, more frequent measurement of indicators, and in-depth interviews with participants, to illustrate how each component functions and in which contexts they are most effective.
In conclusion, the application of QCC in the context of reducing hypoglycemia after endoscopic polypectomy has proven to be a successful intervention. The study underscores the importance of comprehensive quality improvement frameworks in enhancing patient safety and optimizing clinical outcomes. Further research should focus on extending these interventions across different hospitals and evaluating their long-term sustainability in clinical practice.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Levin TR, Corley DA, Jensen CD, et al. Effects of organized colorectal cancer screening on cancer incidence and mortality in a large community-based population. Gastroenterology. 2018;155(5):1383–1391.e5. doi:10.1053/j.gastro.2018.07.017
2. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: recommendations for physicians and patients from the U.S. Multi-society task force on colorectal cancer. Am J Gastroenterol. 2017;112(7):1016–1030. doi:10.1038/ajg.2017.174
3. Doubeni CA, Corley DA, Quinn VP, et al. Effectiveness of screening colonoscopy in reducing the risk of death from right and left colon cancer: a large community-based study. Gut. 2018;67(2):291–298. doi:10.1136/gutjnl-2016-312712
4. Cryer PE, Axelrod L, Grossman AB, et al, Endocrine Society. Evaluation and management of adult hypoglycemic disorders: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2009;94(3):709–728. doi:10.1210/jc.2008-1410
5. Sharifi Y, Ebrahimpur M, Tamehrizadeh SS. Hypoglycemic unawareness: challenges, triggers, and recommendations in patients with hypoglycemic unawareness: a case report. J Med Case Rep. 2022;16(1):283. doi:10.1186/s13256-022-03498-1
6. Cardona S, Gomez PC, Vellanki P, et al. Clinical characteristics and outcomes of symptomatic and asymptomatic hypoglycemia in hospitalized patients with diabetes. BMJ Open Diabetes Res Care. 2018;6(1):e000607. doi:10.1136/bmjdrc-2018-000607
7. Torres Roldan VD, Urtecho M, Nayfeh T, et al. A systematic review supporting the endocrine society guidelines: management of diabetes and high risk of hypoglycemia. J Clin Endocrinol Metab. 2023;108(3):592–603. doi:10.1210/clinem/dgac601
8. Rohrbasser A, Wong G, Mickan S, Harris J. Understanding how and why quality circles improve standards of practice, enhance professional development and increase psychological well-being of general practitioners: a realist synthesis. BMJ Open. 2022;12(5):e058453. doi:10.1136/bmjopen-2021-058453
9. Zhang D, Liao M, Zhou Y, Liu T. Quality control circle: a tool for enhancing perceptions of patient safety culture among hospital staff in Chinese hospitals. Int J Qual Health Care. 2020;32(1):64–70. doi:10.1093/intqhc/mzz094
10. Zhang D, Liao M, Liu T. Implementation and promotion of quality control circle: a starter for quality improvement in Chinese hospitals. Risk Manag Healthc Policy. 2020;13:1215–1224. doi:10.2147/RMHP.S261998
11. Yang H, Liu D, Zeng L, Peng S, Liu H. Associations of colonoscopy and risk of hypoglycemia in patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2023;16:893–900. doi:10.2147/DMSO.S401903
12. Zou X, Zhou X, Lei T. Enhancing the efficacy of hospital infection management using the tool of quality control circle. Asian J Surg. 2023;46(12):5555–5556. doi:10.1016/j.asjsur.2023.08.007
13. Ross S, Drynan-Arsenault J, Peirce M, Williams M, Alexander S. Patient-specific blister packaging of medications in the oncology camp setting: optimizing medication safety and dispensing processes. J Pediatr Hematol Oncol Nurs. 2024;41(6):419–424. doi:10.1177/27527530241282427
14. Vidonscky Lüthold R, Henz NC, Fuhrer C, et al. Inappropriate proton-pump inhibitor prescribing in primary care – an observational study with quality circles. Swiss Med Wkly. 2023;153(9):40119. doi:10.57187/smw.2023.40119
15. Akirov A, Grossman A, Shochat T, Shimon I. Mortality among hospitalized patients with hypoglycemia: insulin related and noninsulin related. J Clin Endocrinol Metab. 2017;102(2):416–424. doi:10.1210/jc.2016-2653
16. Finfer S, Liu B, Chittock DR, et al, NICE-SUGAR Study Investigators. Hypoglycemia and risk of death in critically ill patients. N Engl J Med. 2012;367(12):1108–1118. doi:10.1056/NEJMoa1204942
17. Workgroup on Hypoglycemia, American Diabetes Association. Defining and reporting hypoglycemia in diabetes: a report from the American diabetes association workgroup on hypoglycemia. Diabetes Care. 2005;28(5):1245–1249. doi:10.2337/diacare.28.5.1245
18. Rooijackers HM, Wiegers EC, Tack CJ, van der Graaf M, de Galan BE. Brain glucose metabolism during hypoglycemia in type 1 diabetes: insights from functional and metabolic neuroimaging studies. Cell Mol Life Sci. 2016;73(4):705–722. doi:10.1007/s00018-015-2079-8
19. He J, Zhang Y, Cheng X, et al. Association of postoperative hypoglycemia with mortality after elective craniotomy. Neurosurgery. 2024;95(3):682–691. doi:10.1227/neu.0000000000002938
20. Kulikov A, Krovko Y, Zagidullin T, Bilotta F. Implementation of perioperative blood glucose monitoring and insulin infusion protocol can decrease postoperative infection rate in diabetic patients undergoing elective craniotomy: an observational study. J Clin Neurosci. 2024;124:137–141. doi:10.1016/j.jocn.2024.04.031
21. Johnston LE, Kirby JL, Downs EA, et al. Virginia Interdisciplinary Cardiothoracic Outcomes Research (VICTOR) center. Postoperative hypoglycemia is associated with worse outcomes after cardiac operations. Ann Thorac Surg. 2017;103(2):526–532. doi:10.1016/j.athoracsur.2016.05.121
22. Rajan N, Duggan EW, Abdelmalak BB, et al. Society for ambulatory anesthesia updated consensus statement on perioperative blood glucose management in adult patients with diabetes mellitus undergoing ambulatory surgery. Anesth Analg. 2024;139(3):459–477. doi:10.1213/ANE.0000000000006791
23. Himes CP, Ganesh R, Wight EC, Simha V, Liebow M. Perioperative evaluation and management of endocrine disorders. Mayo Clin Proc. 2020;95(12):2760–2774. doi:10.1016/j.mayocp.2020.05.004
24. Demetriou C, Hu L, Smith TO, Hing CB. Hawthorne effect on surgical studies. ANZ J Surg. 2019;89(12):1567–1576. doi:10.1111/ans.15475
25. Sedgwick P, Greenwood N. Understanding the Hawthorne effect. BMJ. 2015;351:h4672. doi:10.1136/bmj.h4672
26. Gachabayov M, Dyatlov A, Bergamaschi R. Hawthorne effect should be controlled for in quality control studies. JAMA Surg. 2019;154(10):977. doi:10.1001/jamasurg.2019.2159
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.