Back to Journals » Journal of Pain Research » Volume 13
Continuous Epidural Hydromorphone Infusion for Post-Cesarean Delivery Analgesia in a Patient on Methadone Maintenance Therapy: A Case Report
Authors Stanislaus MA ![]() , Reno JL, Small RH
, Reno JL, Small RH ![]() , Coffman JH, Prasad M, Meyer AM
, Coffman JH, Prasad M, Meyer AM ![]() , Carpenter KM, Coffman JC
, Carpenter KM, Coffman JC ![]()
Received 18 December 2019
Accepted for publication 17 April 2020
Published 28 April 2020 Volume 2020:13 Pages 837—842
DOI https://doi.org/10.2147/JPR.S242271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Mellany A Stanislaus,1 Joseph L Reno,1 Robert H Small,1 Julie H Coffman,2 Mona Prasad,3 Avery M Meyer,4 Kristen M Carpenter,4 John C Coffman1
1Department of Anesthesiology, The Ohio State University Wexner Medical Center, Columbus, OH, USA; 2Department of Internal Medicine, Riverside Methodist Hospital, Columbus, OH, USA; 3Department of OBGYN, Riverside Methodist Hospital, Columbus, OH, USA; 4Department of Psychiatry, The Ohio State University Wexner Medical Center, Columbus, OH, USA
Correspondence: John C Coffman
Department of Anesthesiology, The Ohio State University Wexner Medical Center, Room N-411 North Doan Hall, 410 West 10th Avenue, Columbus, OH 43210, USA
Tel +116142938487
Fax +116142938153
Email [email protected]
Abstract: The prevalence of opioid use disorder (OUD) in the United States has more than quadrupled over the past two decades. This patient population presents a number of challenges to clinicians, including difficult pain management after surgical procedures due to the development of opioid tolerance. Significantly greater opioid consumption and pain scores after cesarean delivery have been reported in patients with OUD compared to other obstetric patients. A multi-modal analgesic regimen is generally recommended, but there are few well-established pain management strategies after cesarean delivery specific to patients with OUD. We present the case of a patient with OUD maintained on daily methadone that received a continuous epidural hydromorphone infusion for post-cesarean analgesia, a technique not previously reported in obstetric patients and only rarely described for patients undergoing other surgical procedures. The patient received epidural anesthesia for cesarean delivery, and after surgery, the epidural catheter was left in place for the epidural hydromorphone infusion, initiated at 140 mcg/hr and continued for approximately 40 hrs. This strategy reduced her average daily oral opioid consumption by 97%, reduced self-reported pain scores, shortened the length of hospitalization and improved ability to ambulate compared to her previous cesarean delivery. The use of continuous epidural hydromorphone infusion was effective in this case, and this analgesic technique may also be applicable to other types of surgical procedures with the potential for significant post-operative pain, particularly in patients with OUD.
Keywords: continuous epidural hydromorphone, opioid use disorder, cesarean delivery, medication-assisted treatment, methadone
Introduction
Keeping pace with the opioid epidemic in the United States, the prevalence of opioid use disorder (OUD) has more than quadrupled among obstetric patients over the past 20 years.1 Opioid abuse or dependence in pregnancy increases the risk for a number of adverse maternal and fetal outcomes, including maternal death, cardiac arrest, placental abruption, preterm labor, intrauterine growth restriction, stillbirth and neonatal abstinence syndrome.2,3 In addition to these risks, a particularly challenging aspect in patients with OUD is effectively managing their pain after cesarean delivery. Previous retrospective studies have demonstrated approximately a 50–70% increase in daily opioid requirements and increased pain scores after cesarean delivery in patients on either methadone or buprenorphine maintenance therapy compared to control patients.4,5 Despite the increasing prevalence of OUD in obstetric patients and evidence for greater pain and opioid requirements after cesarean delivery, there are only a few published reports and small case series to guide pain management strategies for these patients. Previous authors have described intravenous (IV) patient-controlled analgesia (PCA), IV ketamine and dexmedetomidine infusions, and continuous epidural local anesthetic infusions with and without clonidine for post-cesarean delivery analgesia.6–11 Regional truncal blocks (transversus abdominis plane, quadratus lumborum and ilioinguinal-iliohypogastric blocks) or surgeon wound infiltration have also been suggested as a potentially beneficial part of multi-modal post-cesarean delivery analgesia, though no studies have been specifically performed in OUD patients undergoing cesarean delivery.11,12 We present the novel technique of using continuous epidural hydromorphone infusion for post-cesarean analgesia in a patient with OUD maintained on daily methadone, and compare her daily opioid use, self-reported pain scores, and length of hospitalization to her first cesarean delivery in order to highlight the potential analgesic benefits of post-operative epidural hydromorphone infusion compared to standard management.
Consent
Written informed patient consent was obtained to publish the details of this case. Other than written patient consent, there is no additional institutional approval required to publish the case details.
Case Report
First Delivery
A 27-year-old G1P0 patient at 35 weeks 6 days gestation presented for cesarean delivery of a dichorionic diamniotic twin pregnancy complicated by chronic hypertension with superimposed preeclampsia. Her other significant past medical history included opioid use disorder and morbid obesity (body mass index (BMI) 47.5 kg/m2). Upon initiation of prenatal care, she was maintained on methadone 85 mg daily and reported use for 1 year through an opioid treatment program. The methadone dose was incrementally increased throughout the pregnancy to 105 mg daily and ultimately 165 mg daily through delivery. There were no reported adverse drug interactions and electrocardiogram (ECG) monitoring did not reveal QT prolongation. A combined spinal-epidural (CSE) block procedure was performed at L4/5. Spinal medications included 0.5% bupivacaine 1.8 mL, morphine 200 mcg, fentanyl 10mcg, and epinephrine 200mcg. The epidural was dosed incrementally with 2% lidocaine with 1:200,000 epinephrine 13 mL to maintain patient comfort during the surgical procedure. The operative course was uncomplicated.
The epidural catheter was left in place after surgery and a continuous epidural infusion of 0.0625% bupivacaine with fentanyl 4 mcg/mL was initiated at 10 mL/hr (patient-controlled dose 4 mL, 15-mins lockout) and continued until approximately 18 hrs post-operatively. The patient reported generally effective pain relief during this time, though she was not able to ambulate due to partial motor block from the epidural local anesthetic infusion. Her other postoperative management included scheduled oral methadone 165 mg daily, IV ketorolac (given from 0 to 24 hrs), oral ibuprofen (given from 24 hrs until discharge). Oral oxycodone and oral acetaminophen were available as needed for breakthrough pain. Pain control was difficult after epidural catheter removal, reflected by average daily oral oxycodone 85 mg per 24 hrs (range 45–100 mg per 24 hrs) and average maximum daily pain scores of 8/10 (range 7–10/10) during her hospitalization after delivery. No significant events were observed on continuous pulse oximetry and telemetry monitoring during her hospitalization. Hospital discharge occurred 3 days 22 hrs after delivery (Table 1).
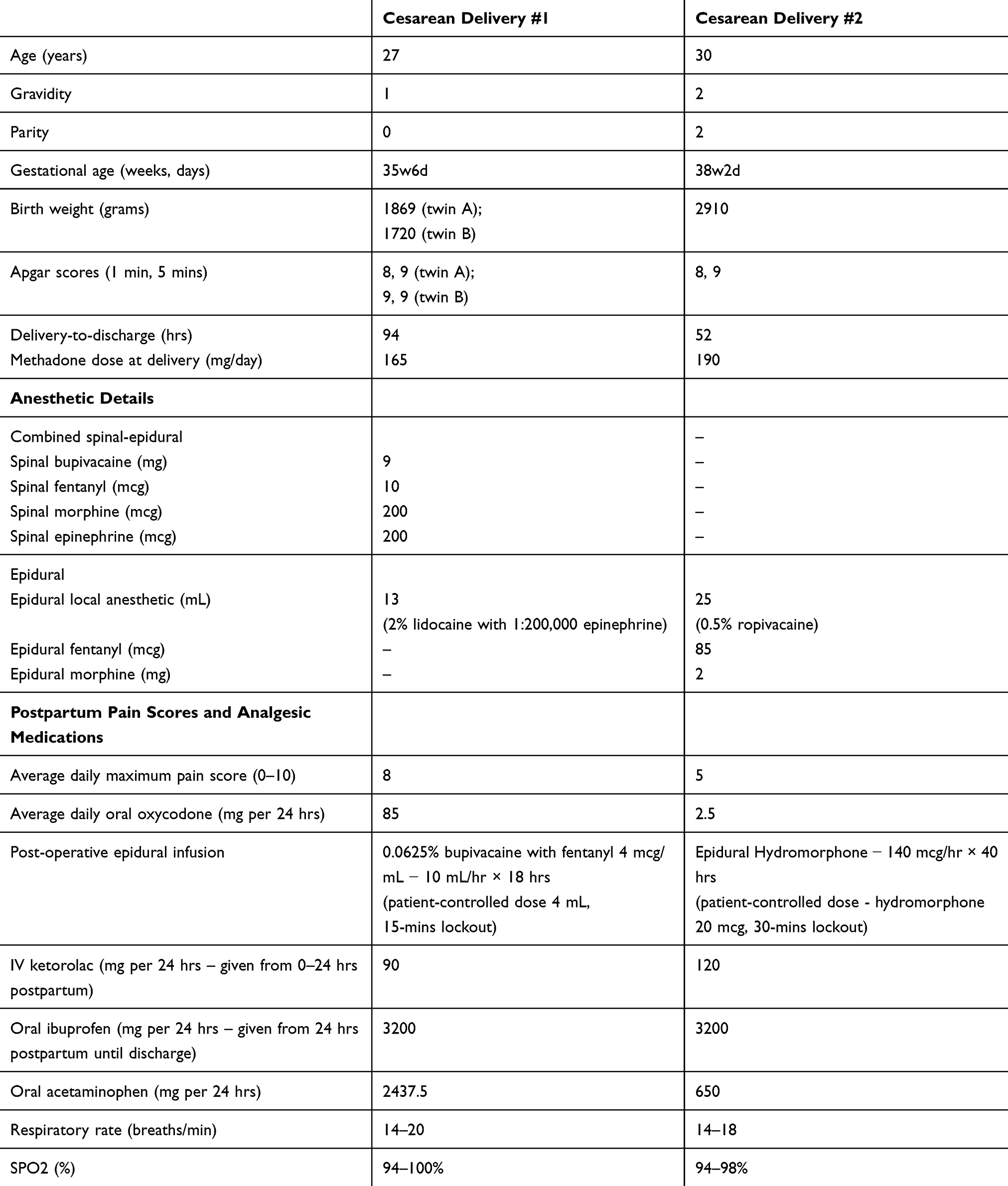 |
Table 1 Patient Characteristics, Anesthetic Details and Analgesic Outcomes After Cesarean Deliveries |
Second Delivery
Approximately 2.5 years after her first delivery, the patient was then a 30-year-old G2P0102 that presented for repeat cesarean delivery at 38 weeks, 2 days gestation. Her past medical history was similar, though she was now maintained on methadone 190 mg daily and her BMI was 39.4 kg/m2 at the time of delivery. At the time prenatal care was initiated, she was maintained on methadone 160 mg daily before being increased by an opioid treatment program to methadone 190 mg daily before the time of delivery. No adverse drug interactions or QT prolongation on ECG were documented. For this cesarean delivery, an epidural was placed at the L3/4 level and incrementally dosed with 0.5% ropivacaine 25 mL, morphine 2 mg and fentanyl 85 mcg. The intraoperative course was uncomplicated.
About 30 mins after delivery, continuous epidural hydromorphone infusion was initiated at 140 mcg/hr (patient-controlled dose 20 mcg, 30-mins lockout). Over 24 hrs, she would receive epidural hydromorphone 3.36 mg from the infusion. No patient-delivered boluses were administered. Her other postoperative analgesic regimen was similar to that of her first delivery, including scheduled oral methadone 190 mg daily, IV ketorolac (0–24 hrs) and oral ibuprofen (from 24 hrs until discharge). Oral oxycodone and oral acetaminophen were available as needed for breakthrough pain. Her overall analgesia was superior compared to the first cesarean delivery, reflected by average daily oral oxycodone 2.5 mg per 24 hrs (range 0–5 mg per 24 hrs) and average maximum daily pain scores of 5/10. Importantly, she was able to ambulate without difficulty during the epidural hydromorphone infusion, which was continued for approximately 40 hrs and stopped 12 hrs prior to hospital discharge. The patient did not experience side effects of nausea or pruritus, and no respiratory depression or somnolence was apparent on clinician assessments or continuous pulse oximetry monitoring (respiratory rate 14–18 breaths/min, SPO2 94–98%). She was discharged 2 days 4 hrs after delivery, and her overall satisfaction was much greater after her second cesarean delivery (Table 1).
Discussion
Obstetric patients with OUD are commonly managed with opioid agonist pharmacotherapy, as supervised withdrawal has been associated with high relapse rates.13 Among recommended medication-assisted treatment options, buprenorphine is commonly utilized for many patients given that they can be treated on an outpatient basis without the need for directly observed therapy and fewer dosage adjustments may be required during pregnancy.13 Additionally, buprenorphine has been associated with a lower incidence of preterm birth and less severe neonatal abstinence syndrome compared to methadone.13–15 Despite these potential advantages of buprenorphine, pregnant women with OUD, such as the one described in this case, may still be maintained on methadone. Due to physiologic changes during pregnancy, methadone dose adjustments are often needed to prevent withdrawal due to rapid drug metabolism, especially in the third trimester.13 Methadone also has the potential for significant drug interactions that increase the risk of complications like respiratory depression.13 Despite having anxiety and bipolar depression, the patient, in this case, was not maintained on benzodiazepines or other medications during either pregnancy, and there were no reported adverse drug interactions. Additionally, ECG monitoring through her opioid treatment program did not demonstrate any QT prolongation and no adverse events were observed on continuous telemetry and pulse oximetry monitoring after each delivery.
Regardless of the type of opioid maintenance therapy, the management of post-cesarean delivery pain in women with OUD remains a formidable challenge for obstetric anesthesiologists. For example, Meyer et al reported that 33 women on maintenance methadone therapy had higher post-cesarean delivery pain scores and as much as a 70% increase in opiate use compared to controls.4 Despite a multimodal approach including both non-steroidal anti-inflammatory drugs (NSAIDs) and acetaminophen, the average daily oxycodone reported in this retrospective cohort was 91.6 mg oxycodone per 24 hrs,4 which is similar to the experience at our institution as well as the first cesarean delivery of the patient in this case report (Table 1). A multimodal analgesic approach emphasizing non-opioid medications is generally recommended for postpartum analgesia.11 Other reported strategies for post-cesarean delivery analgesia in patients with OUD include IV PCAs, IV dexmedetomidine or ketamine infusions, regional anesthesia, and continuous epidural local anesthetic infusions with or without clonidine.6–12 For her first cesarean delivery, the patient, in this case, did have a continuous lumbar epidural infusion (0.0625% bupivacaine, fentanyl 4mcg/mL) continued for 18-hrs post-delivery. This strategy provided effective pain relief while the epidural was in place, but it limited her ability to ambulate and early mobilization after cesarean delivery is generally recommended.16 Prior authors have described epidural placement at T10-11, which enabled that patient to ambulate during the continuous epidural local anesthetic infusion.8
A recent retrospective study compared single-dose neuraxial hydromorphone (intrathecal hydromorphone 60 mcg or epidural hydromorphone 0.6 mg) to morphine (intrathecal morphine 200 mcg or epidural morphine 3 mg) after cesarean delivery, and reported comparable analgesia and side effect profiles, though morphine may provide more prolonged analgesia.17 Although continuous epidural hydromorphone has been used after thoracic, abdominal, pelvic surgeries and post-laminectomy syndrome,18–21 no studies or reports specifically examine its efficacy after a cesarean delivery or in patients with OUD. We selected a continuous epidural hydromorphone infusion for the patient’s second delivery in order to take advantage of the specific ability of epidural opioids to provide analgesia without significant motor blockade.22 Additionally, pharmacologic advantages of epidural hydromorphone include its intermediate lipophilicity, resulting in earlier onset of analgesia compared to morphine (15 vs 30–60 mins) and longer duration of action compared to fentanyl (10–20 vs 2–3 hrs).12,22 Clinical benefits include its equal or lower potential for delayed respiratory depression and significantly less pruritus compared to morphine.12,18-20,22
Prior studies utilizing continuous epidural hydromorphone for postoperative analgesia report infusion rates ranging from 30 mcg/hr to 300 mcg/hr.18–21 Our current institutional standard for continuous hydromorphone epidural infusions utilizes a formulation of hydromorphone 0.1 mg/mL, with common initial infusion rates of 1–1.2 mL/hr (hydromorphone 100–120 mcg/hr), with patient-controlled doses of 0.2 mL (hydromorphone 20 mcg, lockout 30 mins). For the patient in this case, we opted to start epidural hydromorphone at a slightly higher rate, 140mcg/hr, because of her history of OUD and expected tolerance. We were able to optimize her pain relief and she was able to ambulate sooner with the basal rate of epidural hydromorphone 140mcg/hr alone. Additional studies are warranted to determine optimal dosing regimens that maximize pain relief and minimize the potential for side effects.
Limitations of this technique are the potential for maternal side effects, including pruritus, nausea and respiratory depression. Although not observed in our patient, Ruan et al report anasarca extending to a patient’s thorax after continuous lumbar epidural hydromorphone following laminectomy. The rate used in this case was epidural hydromorphone 30mcg/hr, significantly lower than our patient. Following the cessation of the infusion and diuresis, the edema resolved.21 Despite the potential for maternal side effects, none were observed in the patient described in this report. Neonatal side effects of maternal medications should be considered as well. Studies on the effects of hydromorphone on lactation are limited to a case report on maternal use of oral hydromorphone resulting in infant apnea, and transfer of hydromorphone into breast milk after intranasal administration.23,24 Low dose morphine is generally the preferred opiate for postoperative pain control as it has the least amount of secretion in breast milk. Due to the increased potency of hydromorphone, the recommendation is to limit its use while breastfeeding.25 The neonates, in this case, had normal Apgar scores and none were observed to have excessive somnolence, apnea or other concerning symptoms attributable to hydromorphone exposure. All neonates were monitored in the neonatal intensive care unit after birth given maternal methadone use, and all were treated for neonatal abstinence syndrome for 4–5 days prior to hospital discharge.
Conclusion
In this case, the use of a continuous epidural hydromorphone infusion optimized pain relief, as evidenced by significantly reduced pain scores, oral opioid consumption and length of hospitalization compared to her previous delivery. Her ability to ambulate was also improved relative to her previous cesarean delivery in which she received lumbar epidural local anesthetic infusion. We propose that utilization of continuous epidural hydromorphone may, therefore, be a viable approach for improving overall postoperative performance after cesarean delivery in women with OUD. This post-operative analgesic technique may also be applicable to other types of surgical procedures with the potential for significant post-operative pain.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Haight SC, Ko JY, Tong VT, Bohm MK, Callaghan WM. Opioid use disorder documented at delivery hospitalization - United States, 1999–2014. Morb Mortal Wkly Rep. 2018;67:845–849.
2. Maeda A, Bateman BT, Clancy CR, Creanga AA, Leffert LR. Opioid abuse and dependence during pregnancy: temporal trends and obstetrical outcomes. Anesthesiology. 2014;121:1158–1165. doi:10.1097/ALN.0000000000000472
3. Patrick SW, Davis MM, Lehmann CU, Cooper WO. Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012. J Perinatol. 2015;35:650–655. doi:10.1038/jp.2015.36
4. Meyer M, Wagner K, Benvenuto A, Plante D, Howard D. Intrapartum and postpartum analgesia for women maintained on methadone during pregnancy. Obstet Gynecol. 2007;110(2 Pt 1):261–266. doi:10.1097/01.AOG.0000275288.47258.e0
5. Meyer M, Paranya G, Keefer NA, Howard D. Intrapartum and postpartum analgesia for women maintained on buprenorphine during pregnancy. Eur J Pain. 2010;14:939–943. doi:10.1016/j.ejpain.2010.03.002
6. Jones HE, Johnson RE, Milio L. Post-cesarean pain management of patients maintained on methadone or buprenorphine. Am J Addict. 2006;15:258–259. doi:10.1080/10550490600626721
7. Tith S, Bining G, Bollag L. Management of eight labor and delivery patients dependent on buprenorphine (Subutex™): a retrospective chart review. F1000Res. 2018;7:7. doi:10.12688/f1000research.13350.1
8. Leighton BL, Crock LW. Case series of successful postoperative pain management in buprenorphine maintenance therapy patients. Anesth Analg. 2017;125:1779–1783. doi:10.1213/ANE.0000000000002498
9. Wasiluk IM, Castillo D, Panni JK, Stewart S, Panni MK. Postpartum analgesia with dexmedetomidine in opioid tolerance during pregnancy. J Clin Anesth. 2011;23:593–594. doi:10.1016/j.jclinane.2010.09.013
10. Hoyt MR, Shah U, Cooley J, Temple M. Use of epidural clonidine for the management of analgesia in the opioid addicted parturient on buprenorphine maintenance therapy: an observational study. Int J Obstet Anesth. 2018;34:67–72. doi:10.1016/j.ijoa.2018.01.001
11. Landau R. Post-cesarean delivery pain. Management of the opioid-dependent patient before, during and after cesarean delivery. Int J Obstet Anesth. 2019;39:105–116. doi:10.1016/j.ijoa.2019.01.011
12. George RB, Carvalho B, Butwick A, et al. Postoperative analgesia. In: Chestnut DH, Wong CA, Tsen LC, editors. Obstetric Anesthesia Principles and Practice,
13. Committee on Obstetric Practice. Committee opinion no. 711: opioid use and opioid use disorder in pregnancy. Obstet Gynecol. 2017;130:e81–e94. doi:10.1097/AOG.0000000000002235
14. Zedler BK, Mann AL, Kim MM, et al. Buprenorphine compared with methadone to treat pregnant women with opioid use disorder: a systematic review and meta-analysis of safety in the mother, fetus and child. Addiction. 2016;111:2115–2128. doi:10.1111/add.13462
15. Tran TH, Griffin BL, Stone RH, Vest KM, Todd TJ. Methadone, buprenorphine, and naltrexone for the treatment of opioid use disorder in pregnant women. Pharmacotherapy. 2017;37:824–839. doi:10.1002/phar.1958
16. Macones GA, Caughey AB, Wood SL, et al. Guidelines for postoperative care in cesarean delivery: enhanced recovery after surgery (ERAS) society recommendations (part 3). Am J Obstet Gynecol. 2019;221:
17. Marroquin B, Feng C, Balofsky A, et al. Neuraxial opioids for post-cesarean delivery analgesia: can hydromorphone replace morphine? A retrospective study. Int J Obstet Anesth. 2017;30:16–22. doi:10.1016/j.ijoa.2016.12.008
18. Brodsky JB, Chaplan SR, Brose WG, Mark JB. Continuous epidural hydromorphone for postthoracotomy pain relief. Ann Thorac Surg. 1990;50:888–893. doi:10.1016/0003-4975(90)91113-P
19. Chaplan SR, Duncan SR, Brodsky JB, Brose WG. Morphine and hydromorphone epidural analgesia. A prospective, randomized comparison. Anesthesiology. 1992;77:1090–1094. doi:10.1097/00000542-199212000-00008
20. Liu S, Carpenter RL, Mulroy MF, et al. Intravenous versus epidural administration of hydromorphone. Effects on analgesia and recovery after radical retropubic prostatectomy. Anesthesiology. 1995;82:682–688. doi:10.1097/00000542-199503000-00010
21. Ruan X, Tadia R, Liu H, Couch JP, Lee JK. Edema caused by continuous epidural hydromorphone infusion: a case report and review of the literature. J Opioid Manag. 2008;4:255–259. doi:10.5055/jom.2008.0029
22. Macres SM, Moore PG, Fishman SM, et al. Acute pain management. In: Barash PG, Cullen BF, Stoelting RK, editors. Clinical Anesthesia,
23. Schultz ML, Kostic M, Kharasch S. A case of toxic breast-feeding? Ped Emer Care. 2019;35:e9–e10. doi:10.1097/PEC.0000000000001009
24. Edwards JE, Rudy AC, Wermeling DP, Desai N, McNamara PJ. Hydromorphone transfer in breast milk after intranasal administration. Pharmacotherapy. 2003;23:153–158. doi:10.1592/phco.23.2.153.32081
25. Lamvu G, Feranec J, Blanton E. Perioperative pain management: an update for obstetrician-gynecologists. Am J Obstet Gynecol. 2018;218:193–199. doi:10.1016/j.ajog.2017.06.021
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.