Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Construction of Nursing Management Protocol for Promoting Tolerance of Enteral Nutrition in Tube-Fed Perioperative Cancer Patients
Authors Wang J, Wang Y, Jia N, Zhang Y, Zhou J, Bao J, Ni R, Zuo W, Li Y, Yang Z
Received 27 October 2025
Accepted for publication 25 February 2026
Published 12 March 2026 Volume 2026:19 569432
DOI https://doi.org/10.2147/JMDH.S569432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Juan Wang,1 Yu Wang,1 Nan Jia,1 Yunxia Zhang,1 Jin Zhou,2 Jing Bao,1 Runhong Ni,3 Wenqing Zuo,4 Yan Li,5 Zhiying Yang1
1Department of Hepatobiliary Surgery, General Surgery, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 2Department of Cardiothoracic Surgery, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3Department of Gastrointestinal Surgery, General Surgery, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 4Department of Colorectal Surgery, General Surgery, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 5Department of Head and Neck Surgery, China-Japan Friendship Hospital, Beijing, People’s Republic of China
Correspondence: Zhiying Yang, Department of Hepatobiliary Surgery, General Surgery, China-Japan Friendship Hospital, 2 East Yinghuayuan Street, Chaoyang District, Beijing, 100029, People’s Republic of China, Tel/Fax +86-10-8420 5054, Email [email protected]
Purpose: Enteral nutrition tolerance studies are mainly focused on critical care, while perioperative nursing research for cancer patients is relatively scattered. This study aims to develop an evidence-based management protocol for promoting tolerance to perioperative enteral nutrition (tube feeding) for cancer patients in general surgical wards, to provide a practical reference for nursing staff.
Methods: The study used evidence-based methods. Domestic and international databases were searched for articles on perioperative enteral nutrition (tube feeding) in surgical oncology patients. An initial draft of a generalizable management protocol for enteral nutrition tolerance was formulated through evidence synthesis and research team discussion. Two rounds of Delphi consultation were subsequently conducted with experts in enteral nutrition.
Results: A management protocol for perioperative enteral nutrition tolerance in surgical oncology patients was established. The protocol comprised 5 first-level, 12 second-level, and 28 third-level indicators. The expert authority coefficients (Cr) for the two Delphi rounds were 0.857 and 0.880, respectively. The Kendall’s concordance coefficients (W) were 0.215 and 0.257 (both P< 0.05), indicating significant consensus.
Conclusion: The management protocol for tube-fed enteral nutrition tolerance in perioperative surgical oncology patients showed strong expert consensus and high authority indices. The protocol provides a robust evidence-based foundation for the management of enteral nutrition tolerance in this patient population.
Keywords: enteral nutrition, tube feeding, tolerance management, feeding intolerance, perioperative cancer patients
Introduction
The prevalence of malnutrition among surgical patients is estimated to be between 20 and 60%.1 A significant proportion of patients with gastrointestinal cancer present with preoperative nutritional risk, and 50‒80% are malnourished.2 Malnutrition is associated with suboptimal treatment outcomes and adverse clinical consequences (including infections and mortality),3 and represents an independent risk factor for various postoperative complications in patients with cancer.4,5 Advancements in Enhanced Recovery After Surgery (ERAS) protocols and nutritional therapy have led to increased attention on early perioperative enteral nutrition (EN) for oncology patients. However, feeding intolerance (FI) remains a frequent complication associated with EN administration, often occurring during the initial feeding phase and being particularly pronounced in tube-fed patients.
Current literature on EN tolerance has focused predominantly on the critical care setting. In 2016, the American Society for Parenteral and Enteral Nutrition (ASPEN) recommended daily assessment of EN tolerance in critically ill patients.6 However, many assessment strategies are unsuited for perioperative patients in general wards, Critically ill patients often have conditions such as endotracheal intubation, high aspiration risk, and inability to express themselves. Healthcare professionals must utilize monitoring devices for precise assessments, such as using ultrasound equipment for gastric residual volume(GRV) monitoring and intra-abdominal pressure measurement,7,8 to avoid high incidences of aspiration, elevated GRV, increased intra-abdominal pressure, and diarrhea. However, in surgical wards, perioperative tumor patients generally have stabilized conditions, the goal of enteral nutrition here is to meet their perioperative metabolic needs, reduce stress on the digestive system, promote rapid recovery and discharge.3,9 Patients are conscious, able to express discomfort such as abdominal pain, bloating, choking, or diarrhea, and nurse-patient communication is better than in the ICU. Additionally, surgical wards typically lack ultrasound equipment, and nursing staff have not received systematic training for its use. Therefore, based on these considerations, we need to develop a specialized and standardized enteral nutrition protocol for perioperative cancer patients.
Nurses are the primary executors and observers of EN delivery. Currently, there is no standardized protocol for proactive assessment, judgment, and intervention regarding EN tolerance in surgical wards, and nurses often rely on experience. Compounding this issue is the implementation of “hospital-wide unified bed management systems” in many Chinese hospitals. This aims to enhance operational efficiency, enabling rapid turnover in surgical wards. However, Some departments (such as orthopedics), due to their specialty characteristics, have historically had limited experience in tube feeding for enteral nutrition and insufficient training in nutritional support, making it difficult to manage feeding tolerance. This poses significant challenges when admitting patients across specialties. Therefore, the surgical nursing system requires a universal and homogeneous enteral nutrition tolerance management protocol to guide clinical practice.
To address this gap, the study used an evidence-based approach combined with the Delphi method. Published studies on perioperative EN in surgical oncology patients were systematically analyzed and the evidence synthesized, leading to the identification and refinement of key nursing interventions for managing EN tolerance. Subsequent application of the Delphi consensus technique resulted in the development of a management protocol for EN tolerance specifically designed for use by nursing staff in surgical wards. This protocol aims to provide systematic, evidence-based guidance for nurses across various wards, ultimately seeking to improve EN tolerance in perioperative surgical patients and hasten patient recovery.
Methods
Establishment of the Evidence-Based Research Team
The team responsible for searching the literature comprised four members: one head nurse (master’s degree, trained in evidence-based practice), one master’s degree candidate (trained in evidence-based practice), and two staff nurses (with bachelor’s degrees, who had received evidence-based training). This team was responsible for the retrieval and appraisal of suitable publications, development of the expert consultation questionnaire, and the collation and analysis of the expert feedback. Additionally, a seven-member appraisal panel was formed, comprising two clinicians (PhD, Associate Chief Physicians), one dietitian (master’s degree, Attending Physician), two head nurses (one Deputy Chief Nurse and one Nurse-in-Charge), and two staff nurses (both Nurses-in-Charge, and certified Clinical Nutrition Specialty Nurses). This panel was responsible for refining the expert consultation questionnaire.
Evidence-Based Research Process
Evidence Retrieval
The “6S” evidence pyramid model was used to guide searches of relevant guideline repositories,10 published in either Chinese or English, as well as professional society websites, and the UpToDate clinical decision support resource. The databases searched included the Joanna Briggs Institute (JBI) Evidence-Based Practice Database, the Cochrane Library, DynaMed (evidence-based clinical decision support), the Registered Nurses’ Association of Ontario (RNAO) Guidelines, WHO Guidelines, the National Guideline Clearinghouse (NGC), Web of Science, PubMed, CNKI, Wanfang, VIP, and the Chinese Biomedical Literature Database (CBM). A combination of Medical Subject Headings (MeSH) and free-text terms was used. The references of the identified articles were also searched manually. Search strategy: (“neoplasm*” OR “tumor” OR “cancer”) AND (“enteral nutrition” OR “nutrition therapy” OR “nutritional support” OR “artificial feeding” OR “enteral feeding” OR “force feeding*” OR “tube feeding” OR “gastric feeding tube*”) AND (“feeding intolerance” OR “feeding tolerance”). The search period covered the interval between database inception to December 10, 2023.
Inclusion and Exclusion Criteria
The evidence-based question was formulated using the PIPOST framework:11
P (Population): Surgical oncology patients receiving tube-fed EN support during the perioperative period.
I (Intervention): Evidence related to improving tube-fed EN tolerance in oncology patients.
P (Professionals): Nursing staff, physicians, and dietitians, among others.
O (Outcomes): Nutritional status, EN tolerance.
S (Setting): Surgical wards.
T (Type of evidence): Guidelines, systematic reviews, evidence summaries, expert consensus statements, randomized controlled trials (RCTs).
Inclusion Criteria: Studies involving adult oncology patients in the perioperative period, interventions related to assessment of EN tolerance and nursing management; evidence types including clinical practice guidelines, evidence summaries, expert consensus statements, systematic reviews, and RCTs; publications in Chinese or English.
Exclusion Criteria: Studies involving ICU patients; Studies not involving tube-fed EN; Duplicate publications or translations; Low-quality studies; No available full text.
Evidence Quality Appraisal
Two members of the research team, systematically trained in evidence-based nursing, independently appraised the quality of the included publications. The appraisal methods were selected based on the Johns Hopkins evidence level and quality guide and the JBI methodology (2016), utilizing specific critical appraisal tools appropriate to the evidence type:
Guidelines: AGREE II instrument.12
RCTs, systematic reviews, expert consensus: Corresponding JBI critical appraisal tools.13
Evidence summaries: Evidence from the original sources cited in the summaries was retrieved and appraised using the relevant tool based on the appropriate study design.
Following this process, 19 articles were ultimately included: 6 guidelines/expert consensus statements,9,14–18 2 systematic reviews,19,20 1 evidence summary,21 and 10 original research studies.22–31
Evidence Synthesis, Grading, and Determination of Recommendation Strength
Two graduate student members of the research team independently extracted the evidence. The extracted evidence was graded using the JBI Evidence-Based Practice Center (2014) evidence level system.7 Discrepancies in grading were resolved by consultation with a senior researcher from the appraisal panel to reach a consensus. Evidence levels were assigned from Level 1 (highest) to Level 5 (lowest). Based on the JBI (2014) system, the recommendation strength for each piece of evidence was categorized as Grade A (strong recommendation) or Grade B (weak recommendation).
Development of the Draft Tolerance Management Protocol
To enhance clinical relevance, the research team conducted group discussions. Drawing upon established clinical nursing workflows and the steps involved in nutritional diagnosis and therapy,3,4 a tolerance management framework was constructed. This process resulted in an initial draft protocol comprising 5 first-level (nursing workflows), 11 second-level (main work contents), and 31 third-level indicators (specific implementation contents), the detailed breakdown is provided in Table 1.
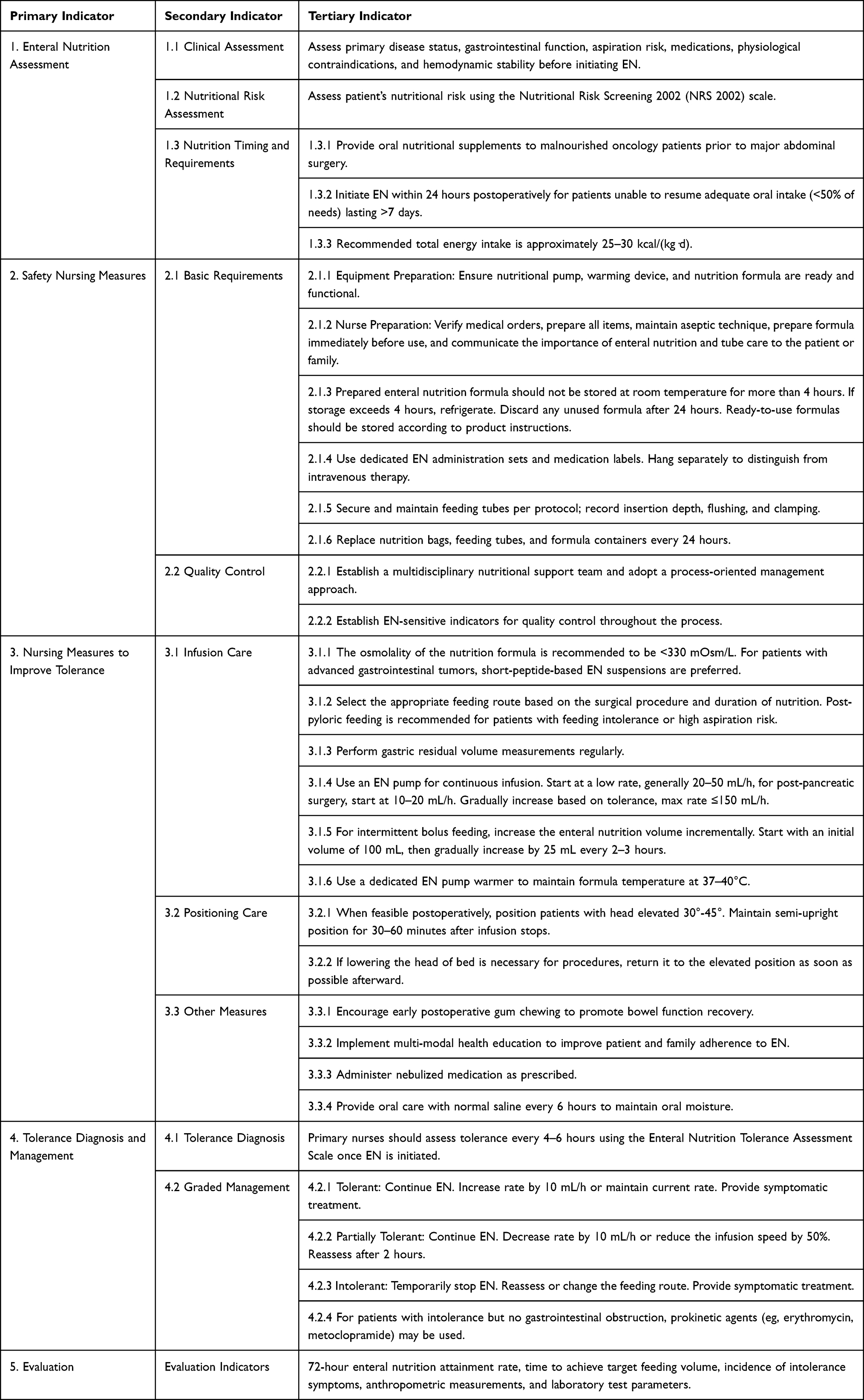 |
Table 1 Nursing Management Program for Promoting Tolerance of Enteral Nutrition in Tube-Fed Perioperative Cancer Patients (Draft) |
Delphi Expert Consultation
Selection of Delphi Consultation Experts
The inclusion criteria for consultation experts were as follows: (1) Engagement in EN-related work in surgical wards or nutrition departments for ≥10 years; (2) Holding an associate senior or higher clinical medical or nursing technical title; (3) Possession of research experience; (4) Motivated and willing to participate in the consultation process. Fifteen experts meeting these criteria were enrolled in the study.
Development of Consultation Questionnaire
The Delphi consultation questionnaire was based on the preliminary protocol, included the following sections: (1) Instructions for completion; (2) Main section: Assessment of the importance of each indicator at all levels using a 5-point Likert scale (1 = “not important” to 5 = “very important”). Experts could offer comments and suggestions in the remarks column for each indicator; (3) Expert demographic information, including education, position, professional title, and years of experience; (4) Expert familiarity was assessed using a 5-level scale ranging from “Unfamiliar” to “Very Familiar,” with corresponding scores of 0.1, 0.3, 0.5, 0.7, and 0.9. The basis for expert judgment was categorized into four aspects: theoretical analysis, practical experience, intuitive perception, and reference to domestic and international literature. The degree of influence from each aspect was further classified into three levels: low, medium, and high. The specific scoring assignments are detailed in Table 2.
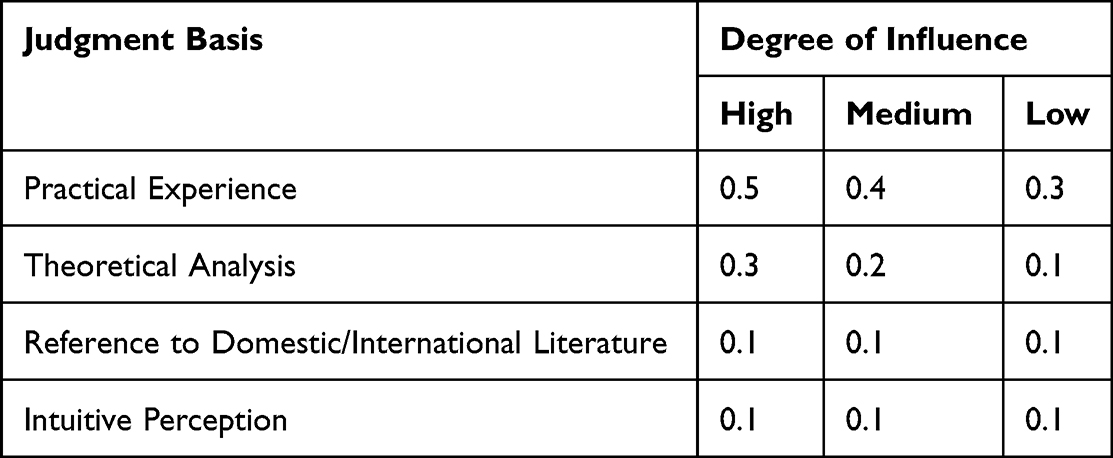 |
Table 2 Expert Judgment Basis Assignment Table |
Implementation of the Delphi Consultation
Two rounds of electronic Delphi consultations were conducted, the response period was 2 weeks. After the return of the first-round questionnaires, the indicators were screened and modified based on the expert feedback. The screening criteria used were an importance score ≥ 4 and a coefficient of variation (CV) < 0.25. The second-round questionnaire was developed after integration of the feedback. The expert opinions in the second round tended to converge, concluding the consultation process.
Statistical Analysis
Statistical analyses were performed using SPSS software version 26.0 (IBM Corp., Armonk, NY, USA). Categorical data are presented as frequencies and percentages, while continuous data are shown as mean ± standard deviation (SD). Expert enthusiasm was measured by the questionnaire response rate and the expert opinion proposal rate. A response rate ≥70% was considered indicative of high enthusiasm. Expert authority was assessed based on the experts’ self-reported judgment basis and familiarity with the consultation content. The expert authority coefficient (Cr) was calculated as: Cr = (Ca + Cs)/2, where Ca represents the judgment coefficient and Cs represents the familiarity coefficient. Generally, Cr≥0.70 is considered acceptable The degree of consensus among experts was assessed using Kendall’s coefficient of concordance (W) and coefficient of variation(CV). P-values < 0.05 obtained in statistical tests were considered statistically significant.
Results
Expert Demographics
The 15 experts consulted in this study included surgeons (4), surgical nursing administrators (6), nurses specialized in clinical nutrition (3), and dietitians (2). The mean age of the experts was 41.40 ± 4.58 years, with a mean working experience of 22.33 ± 6.07 years. The professional and educational backgrounds of the experts are shown in Table 3.
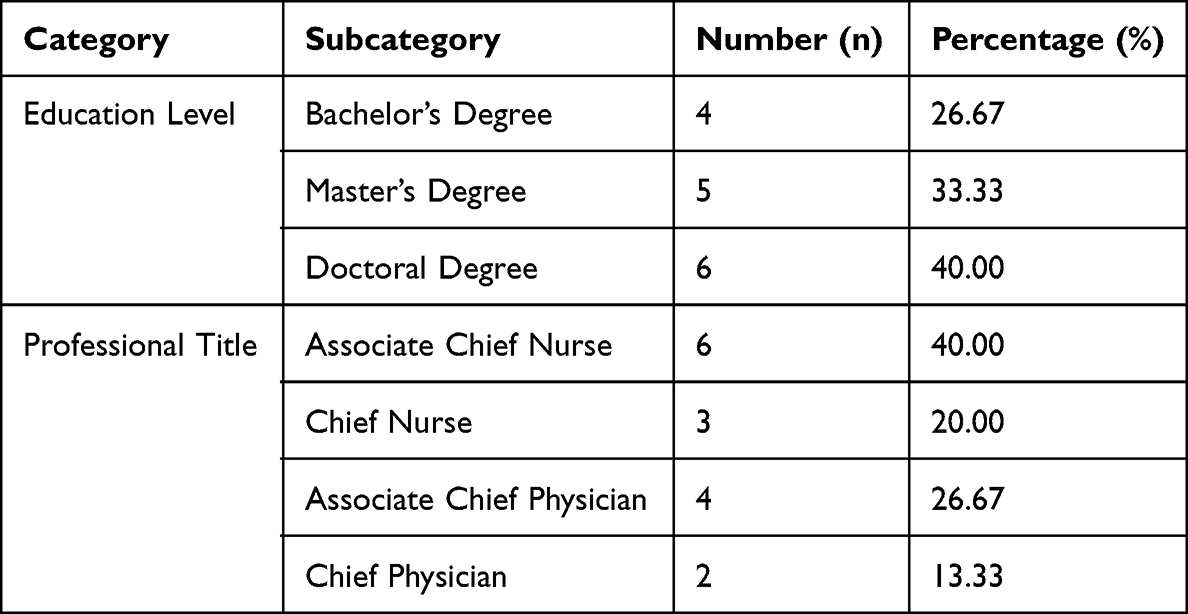 |
Table 3 Distribution of Participants by Education Level and Professional Title |
Expert Enthusiasm and Authority Level
The experts demonstrated high enthusiasm, with a 100% response rate for both rounds of the consultation questionnaire. In the first round, the expert opinion submission rate was 46.67%. The experts’ basis of judgment was 0.973, their familiarity level was 0.740, resulting in an expert authority coefficient of 0.857. In the second round, the expert opinion submission rate was 26.67%, the basis of judgment remained at 0.973, the familiarity level increased to 0.786, leading to an expert authority coefficient of 0.880. The experts had a high level of certainty regarding the items, with the authority coefficient for both rounds of consultation being ≥0.7, indicating that the results are reliable.
Degree of Coordination in Expert Opinions
The results from the first round of expert consultation showed that the third-level indicator “Administer nebulization as prescribed” had a CV of 0.25, while the CV values for all other indicators were from 0 to 0.24, and the Kendall’s coefficient of concordance W for the importance of expert opinions was 0.215 (P = 0.001). After the second round of expert consultation, the CV ranged from 0 to 0.19, and the Kendall’s W for the importance of expert opinions was 0.257 (P = 0.000). As the number of consultation rounds increased, the degree of coordination among expert opinions improved.
Expert Consultation Outcomes
First Round
Following the first round of expert consultation, the mean importance scores and CV for each indicator are presented in Table 4. According to the predetermined indicator selection criteria, two third-level indicators were deleted: “3.3.3 Administer nebulization as prescribed” (Mean score=4.00, CV=0.25) and “3.3.4 Provide saline mouth rinses every 6 hours to maintain oral moisture” (Mean score=3.86). Experts also commented that these two indicators had weak relevance to enteral nutrition tolerance management and recommended their removal. This recommendation was adopted after discussion by the research team. Two experts disagreed on “Gastric residual volume measurement” routines in general wards, after further review of the literature and consultation with physicians, this recommendation was modified.
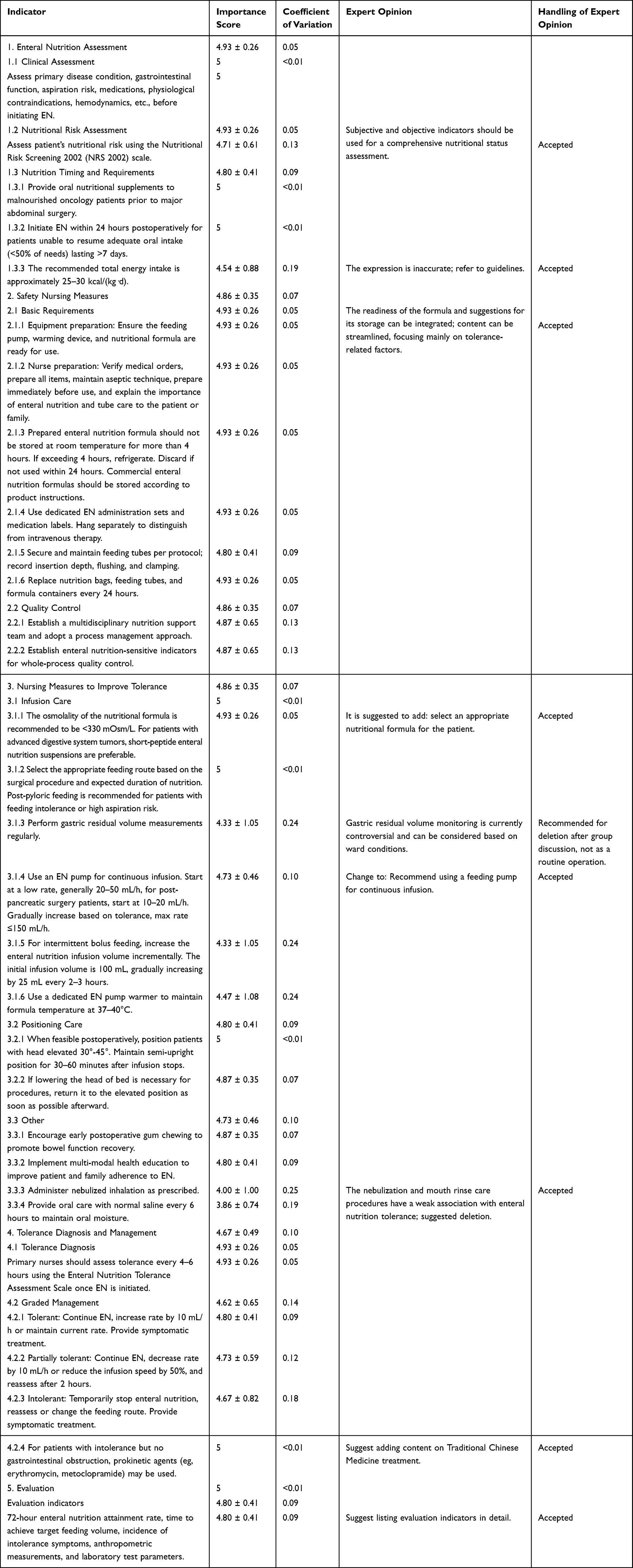 |
Table 4 Nursing Management Program for Promoting Tolerance of Enteral Nutrition in Tube-Fed Perioperative Cancer Patients (First Round of Delphi Survey) |
A total of six items were revised. For instance, experts noted that “1.2 nutritional risk assessment” alone could not comprehensively reflect a patient’s nutritional status. They recommended adopting a holistic assessment utilizing both subjective and objective indicators. After reviewing the literature and group discussion, this item was revised to “Assess nutritional status using tools such as the Nutritional Risk Screening 2002 (NRS-2002), the Patient-Generated Subjective Global Assessment (PG-SGA), anthropometric measurements, and laboratory tests”. Three experts suggested that the description “Energy assessment 25–30 kcal/kg/day” was inaccurate, further literature review led to its revision to reflect the recommendations of guidelines “Postoperative total energy requirement 25–30 kcal/kg/day; Protein target 1.5–2.0 g/kg/day; Achieved gradually over 5–7 days based on tolerance.”3,6,9
Three items (2.1.1–2.1.3) were suggested for consolidation, retaining only content directly relevant to tolerance management. This suggestion was adopted following group discussion. The consolidated item was revised to “Store EN formula correctly, use aseptic technique, and prepare immediately before use.”18 For the final item of the protocol, experts recommended detailing the specific evaluation indicators. This recommendation was adopted after the research team conducted a literature review and discussion. The supplemented details are provided in the evaluation section of Table 5.
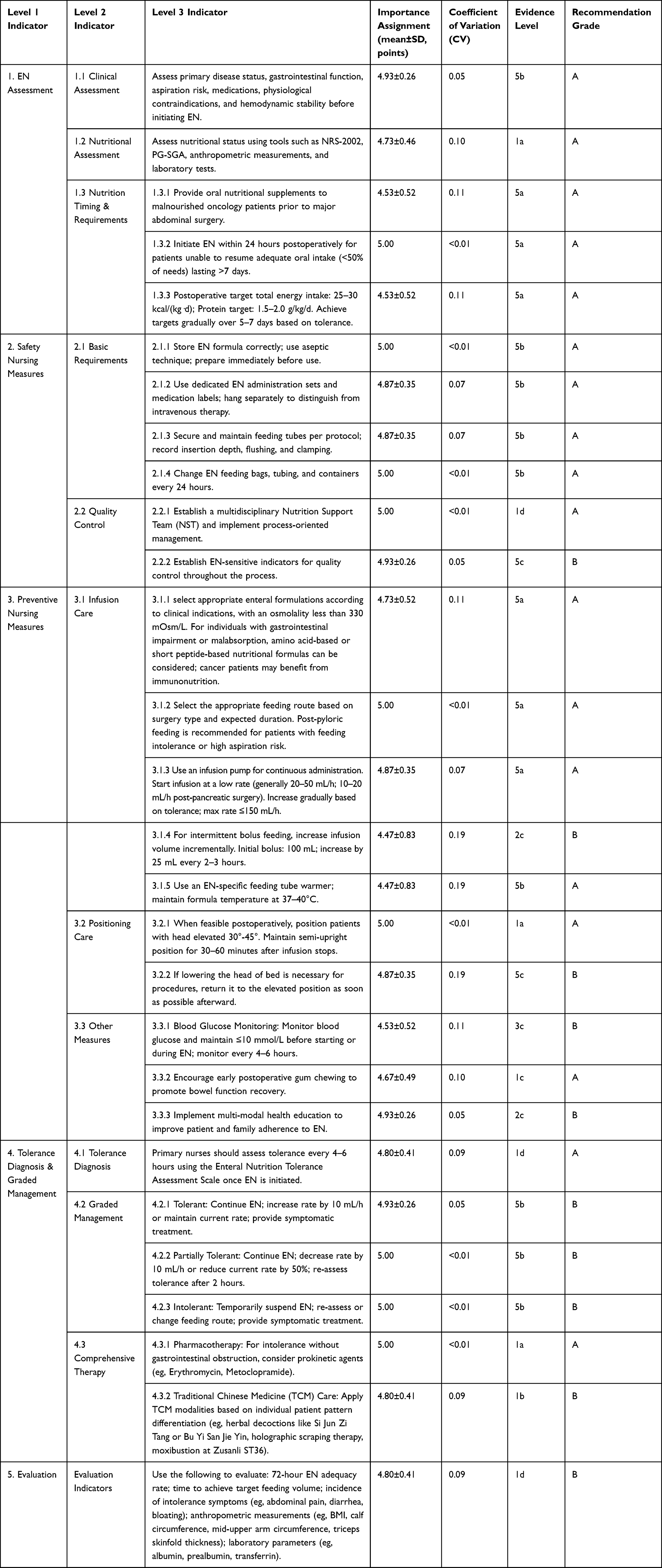 |
Table 5 Nursing Management Program for Promoting Tolerance of Enteral Nutrition in Tube-Fed Perioperative Cancer Patients (Second Round of Delphi Survey) |
Three items were added during this revision. Four experts suggested incorporating “select an appropriate nutritional formula” into the infusion care content. Following a literature review, this was refined to “Select an appropriate nutritional formula with an osmolality less than 330 mOsm/L.”6,22 Separately, two experts recommended adding “blood glucose monitoring” to the “other measures” section, citing its relevance to tolerance management. Another expert noted the beneficial effects of Traditional Chinese Medicine (TCM) in improving tolerance. These suggestions were incorporated after team discussion.
Second Round
Following these adjustments, we developed a management protocol comprising 5 first-level indicators, 12 second-level indicators, and 28 third-level indicators. This revised program was then subjected to a second round of Delphi consultation, the results of which are presented in Table 5. All indicators met the retention criteria, with importance scores greater than 4 and CV less than 0.25, therefore, all were retained.
One expert suggested changing “Nursing measures to improve tolerance” to the more concise “Preventive measures” which was adopted. Another expert pointed out the critical importance of selecting appropriate nutritional formulas, suggesting specific recommendations regarding concentration and type. Therefore, item 3.1.1 was revised to “select appropriate enteral formulations according to clinical indications, with an osmolality less than 330 mOsm/L. For individuals with gastrointestinal impairment or malabsorption, amino acid-based or short peptide-based nutritional formulas can be considered, cancer patients may benefit from immunonutrition”.6,14
After two rounds of expert consultation and subsequent data analysis, a management protocol for perioperative tube-fed EN tolerance in surgical oncology patients was finalized.
Discussion
FI is a common complication encountered during enteral nutrition. The concept of the feeding intolerance syndrome was explicitly defined in 2012 by the Abdominal Problems Working Group of the European Society of Intensive Care Medicine.32 While research on tolerance-related issues has focused predominantly on critically ill patients in the ICU, these procedures are not fully applicable to general wards. In surgical nursing practice, oncology patients face a high risk of perioperative malnutrition. Early initiation of EN is recommended particularly for patients undergoing major surgery,3,9 with tube feeding being the primary route. The effective management of tolerance is therefore crucial for this population. However, there have been no standardized, homogeneous tolerance management protocol for use in surgical settings. This gap is especially significant in the context of the “hospital-wide unified bed management systems” model, in which nurses care for patients across various surgical specialties. The development of a universal management protocol for EN tolerance would provide an evidence-based foundation for cross-specialty nursing care within the surgical system.
Evidence-Based Nature of the Management Protocol for Perioperative Enteral Nutrition Tolerance in Surgical Oncology Patients
This study aimed to address the issue of tube-fed EN tolerance in perioperative surgical oncology patients. Following evidence-based research steps, the PIPOST framework was used for formulation of the clinical question.11 This was followed by the systematic analysis and synthesis of clinical practice guidelines and the primary literature. The quality of evidence was rigorously appraised using established standards, namely, the AGREE II instrument for guidelines,12 JBI critical appraisal tools for systematic reviews and randomized controlled trials, and the JBI tool for expert consensus.13 This process ensured the inclusion of high-quality evidence, thereby guaranteeing the scientific rigor of the research content.
Clinical Applicability of the Management Protocol for Perioperative Enteral Nutrition Tolerance in Surgical Oncology Patients
Expert Selection and Validation
The clinical relevance of the protocol was ensured through the selection of a multidisciplinary expert panel intimately involved in clinical EN delivery, including surgeons, surgical nursing managers, nutrition physicians, and clinical nurses, representing a well-balanced composition. Two rounds of Delphi consultation and multidisciplinary validation were used for further refinement of the protocol to align closely with clinical practice. The results indicated questionnaire response rates of 100% for both rounds, with authority coefficients (Cr) of 0.857 and 0.880, respectively. The Kendall’s harmony coefficients for the importance of each item were statistically significant (P < 0.05), demonstrating high expert engagement, authority, and consensus consistency, thereby affirming the reliability of the program.
Structure and Process
The development of first-level indicators integrated established clinical nursing workflows and clinical nutrition care pathways.3,4 This approach aligns with clinical reasoning and enables planned, continuous, and systematic management of enteral nutrition tolerance in perioperative patients.
The Tolerance Management Protocol Demonstrates Both Generalizability and Professional Value for Surgical Nurses
This tolerance management protocol is specifically designed for perioperative oncology patients within the surgical system. The primary objectives of enteral nutrition in this context are to meet perioperative metabolic demands, reduce gastrointestinal stress, provide nutritional supplementation, and facilitate enhanced recovery, as outlined in key surgical and nutritional guidelines.3,9,16 These goals differ from those guiding enteral nutrition management in critically ill patients. Furthermore, within the surgical system itself, heterogeneity exists across different specialties. Variations in the knowledge training nurses receive, daily operational protocols, and levels of interprofessional collaboration regarding enteral nutrition care can pose significant limitations to the implementation of hospital-wide unified bed management and the provision of cross-specialty nursing. This study addresses this gap by developing a universally applicable and operationally practical tolerance management protocol.
First, assessment is fundamental to clinical decision-making and patient care safety.33 During the first Delphi round, the initial focus on nutritional risk screening was broadened to include a comprehensive nutritional assessment. This expansion encompassed indicators such as NRS2002, PG-SGA, BMI and laboratory parameters.3,9 The aim was to facilitate nurses’ effective participation in Nutrition Support Team (NST) activities by ensuring they thoroughly understand the patient’s baseline condition prior to initiating enteral nutrition. By the second Delphi round, the importance score for this revised indicator increased to 4.73, with a decreased CV of 0.10.
Regarding GRV measurement, although elevated GRV can be an indicator of enteral feeding intolerance, its application in routine intolerance assessment remains controversial. A systematic review incorporating five randomized controlled trials found no statistically significant difference in the incidence of pneumonia or aspiration between critically ill patients managed with or without GRV monitoring.34 Consequently, following team discussion, routine GRV monitoring was not included as a standard indicator for tolerance assessment in general wards and was removed from the protocol. It is acknowledged that GRV measurement remains necessary in clinical practice for critically ill patients or those requiring long-term enteral nutrition.17
Concerning preventive measures for intolerance, the indicator “blood glucose monitoring” was added after the first Delphi round. This addition reflects expert recognition of glycemic control as a significant factor influencing tolerance. A literature review revealed that blood glucose levels >10 mmol/L or persistent hyperglycemia are associated with a higher risk of
Intolerance.35 The Canadian Critical Care Nutrition Guidelines further recommend avoiding hyperglycemia (>10 mmol/L) during nutritional support.36 Given its clinical significance and ease of implementation, this measure was incorporated into the protocol following team discussion, thereby enriching the management strategies compared to traditional approaches for post-upper gastrointestinal or esophageal cancer surgery patients.19,21
Regarding tolerance diagnosis, the use of a standardized tolerance scale has been shown to improve EN adequacy rates.37,38 The management protocol adopted the Enteral Nutrition Tolerance Assessment Scale from the group standard of the Chinese Nursing Association.18 This scale recommends proactive nurse assessment every 4–6 hours, facilitating the early detection of intolerance. Critically, the protocol can guide nurses to implement tolerance-level-specific interventions, which is key to promoting tolerance and ensuring the successful delivery of nutrition. For example, a tolerance score of 4 represents partial intolerance, indicating that nurses should decrease the infusion rate by 10 mL/h or reduce the current rate by 50%, with reassessment after 2 hours, accompanied by dynamic adjustments, rather than discontinuing EN.
Regarding the treatment of feeding intolerance, experts suggested incorporating TCM for alleviating intolerance symptoms. Our findings indicate that TCM modalities such as the herbal decoctions Si Jun Zi Tang and Bu Yi San Jie Yin, holographic scraping therapy, and moxibustion at Zusanli (ST36) have demonstrated efficacy.20,26,39,40 Following the second round of consultation, this indicator achieved an importance score of 4.8 with a coefficient of variation (CV) of 0.02, indicating its reliability. These findings are more comprehensive than those of previous studies and highlight the unique strengths of TCM.
Conclusions
The management protocol for tube-fed enteral nutrition tolerance in perioperative surgical oncology patients showed strong expert consensus and high authority indices. The conceptual framework and indicators of this management protocol offer practical utility for surgical nursing staff. It can actively guide clinical nurses in the provision of structured tolerance management for tube-fed patients, promoting the appropriate implementation of nutritional therapy within the surgical system and contributing significantly to patient recovery.
Acknowledgments
The authors would like to express their gratitude to all those who helped them during the writing of this thesis, the literature review and expert consultation process. Their deepest gratitude goes first and foremost to Professor Yang. Without his constant encouragement and illuminating instruction, this thesis could not have reached its present form.
Funding
This study was funded by the National High Level Hospital Clinical Research Funding (2023-NHLHCRF-GLMS-25); Research Ethics Committee (REC): China-Japan Friendship Hospital Clinical Research Ethics Committee, Ethics No.: 2023-KY-265.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Holst M, Rasmussen HH, Irtun O. Advances in clinical nutrition in GI surgery. Expert Rev Gastroenterol Hepatol. 2015;9(4):467–15. doi:10.1586/17474124.2015.972371
2. Chen XR, Yang K, Zhang XX, et al. Meta-analysis of preoperative oral nutritional supplements for patients with gastric cancer: east Asian experience. Eur J Clin Nutr. 2020;74(7):991–1000. doi:10.1038/s41430-019-0483-0
3. HAN Ting. The standardized nutrition management and implementation in surgery. Shanghai Med Pharmaceut J. 2023;44(3):6–10,17.
4. Gianotti L, Besselink MG, Sandini M, et al. Nutritional support and therapy in pancreatic surgery:a position paper of the International Study Group on Pancreatic Surgery (IsGPs). Surgery. 2018;164(5):1035–1048. doi:10.1016/j.surg.2018.05.040
5. Zhu Y, Fan LH, Geng XF, et al. The predictive value of the prognostic nutritional index to postoperative prognosis and nursing intervention measures for colorectal cancer. Am J Transl Res. 2021;13(12):14096–14101.
6. Nanhai P, Yingchun H. Clinical Nutrition Nursing Guidelines: Enteral Nutrition Section (2nd Ed.). Southeast University Press; 2019.
7. Yuanyuan MI, Peipei H, Dong J, et al. Best evidence summary for prevention and management of enteral feeding intolerance in critically ill patients. Chin J Nurs. 2019;54(12):1868–1875.
8. Zaher S. Barriers to delivery of enteral nutrition in intensive care settings in Saudi Arabia: a comparative study of the perceptions of health care providers working in adult and paediatric ICUs. Risk Manage Healthc Policy. 2022;Volume 15:2357–2370. doi:10.2147/RMHP.S394035
9. Weimann A, Braga M, Carli F, et al. ESPEN guideline: clinical nutrition in surgery. Clin Nutr. 2021;40(7):4745–4761. doi:10.1016/j.clnu.2021.03.031
10. Dicenso A, Bayley L, Haynes RB. Accessing pre—appraised evidence:fine-tuning the 5S model into a 6S model. Evid Based Nuts. 2009;12(4):99–101.
11. Zhu Z, Hu Y, Xing WJ, et al. Composition of different types of evidence-based questions. J Nurs Train. 2017;32(21):1991–1994.
12. Brouwers MC, Lavis JN, Spithoff K, et al. Assessment of health systems guidance using the Appraisal of Guidelines for Research and Evaluation-Health Systems (AGREE-HS) instrument. Health Policy. 2019;123(7):646–651. doi:10.1016/j.healthpol.2019.05.004
13. Zheng Z, Yan H, Yingfeng Z, et al. Promotion evidence to clinical transformation: evidence resource retrieval for the purpose of clinical transformation. J Contin Educ Nurs. 2020;35(11):996–1000.
14. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48.1. doi:10.1016/j.clnu.2016.07.015
15. Chinese Pancreatic Surgery Association. Chinese society for parenteral and enteral nutrition. Chinese expert consensus on perioperative whole-course nutrition management for pancreatic surgery (2020 edition). Chin J Dig Surg. 2020;19(10):1013–1029.
16. Chinese Society for Parenteral and Enteral Nutrition. Enhanced recovery after surgery committee of China Medicine Education Association. Chinese expert consensus on perioperative nutritional support in enhanced recovery after surgery (2019 edition). Chin J Dig Surg. 2019;18(10):897–902.
17. Chinese Society of Nutritional Oncology. Chinese society for parenteral and enteral nutrition. Consensus on treatment for enteral nutrition intolerance among patients with cancer. Electron J Metab Nutr Cancer. 2023;10(4):505–508.
18. Chinese Nursing Association. T/CNAS 19─2020. Nursing care of adult patients with enteral nutrition support. 2021.
19. Li K, Wang D, Zhang X, Yang J, Chen X. Efficacy of early enteral nutrition versus total parenteral nutrition for patients with gastric cancer complicated with diabetes mellitus: a systematic review and meta-analysis. Nutr Diet. 2022;79(1):129–139. doi:10.1111/1747-0080.12721
20. Chen X, Yang K, Yang J, Li K. Meta-analysis of efficacy of sijunzi decoction combined with enteral nutrition for the treatment of gastric cancer. Nutr Cancer. 2020;72(5):723–733. doi:10.1080/01635581.2019.1653470
21. Juzi WANG, Hui LIU, Jianhui LI, et al. Evidence summary of symptom management of feeding intolerance in patients with early enteral nutrition after esophageal cancer surgery. Chin Evid Based Nurs. 2021;7(09):1160–1167.
22. Chao W, Zhihong L, Wenting W, et al. The effects of different osmotic nutrient solutions on the tolerability of enteral nutrition patients with advanced gastric cancer. Chin J Cancer Prevent Treat. 2018;25(S2):60–61.
23. Bing LI, Xiaofei CHU, Jingdan MA, et al. Impact of different incremental infusion rates of enteral nutrition on feeding tolerance in patients after esophageal cancer surgery. Clin Med Engineer. 2023;30(09):1251–1252.
24. He FJ, Wang MJ, Yang K, et al. Effects of preoperative oral nutritional supplements on improving postoperative early enteral feeding intolerance and short-term prognosis for gastric cancer: a prospective, single-center, single-blind, randomized controlled trial. Nutrients. 2022;14(7):1472. doi:10.3390/nu14071472
25. Zhang L, Liu Y, Gao X, et al. Immediate vs. gradual advancement to goal of enteral nutrition after elective abdominal surgery: a multicenter non-inferiority randomized trial. Clin Nutr. 2021;40(12):5802–5811. doi:10.1016/j.clnu.2021.10.014
26. Ping Z, Chuansi W, Hui Y. Effect of holographic scraping therapy on early enteral nutrition tolerance in patients after gastric cancer surgery. J Nurs Sci. 2022;37(02):35–37.
27. Yu-long YAN, Sheng LIJ. Study of start time of early enteral nutritional support in patients with radical gastrectomy. Chin J Gen Pract. 2014;12(08):1272–1274.
28. Min ZHANG, Ling ZHANG. Analysis of the effect of systemic nursing intervention of early nutritional support in postoperative patients with gastric cancer. Chin J Clin Oncol Rehabil. 2014;21(6):758–761.
29. Yan SUN, Liqin LIANG, Min LIU, et al. Evidence-based practice of the effect of chewing gum on bowel function after radical resection in patients with colorectal cancer. Chin J Modern Nurs. 2017;23(23):2972–2976.
30. Shanshan W, Jiawei S, Xiaoguang W. Effect of Iso-Incremental enteral nutrition infusion on nutritional status and tolerance to early enteral nutrition feeding in older patients with pancreatic cancer. Int J Geriatr. 2022;43(2):175–178,252.
31. Shan WANG, Si-tang GE, Juan LI, et al. Preventive effect of probiotics on early enteral nutrition intolerance after gastric cancer operation. J Bengbu Med Coll. 2019;44(07):959–962.
32. Blaser AR, G MMLN, Starkopt J, et al. Gastrointestional function in intensive care patients: terminology, definitions and management. recommendations of the ESICM working group on abdominal problems. Intensive Care Med. 2012;38:384–394. doi:10.1007/s00134-011-2459-y
33. Munroe B, Curtis K, Murphy M, et al. A structured framework improves clinical patient assessment and nontechnical skills of early career emergency nurses: a pre-post study using full immersion simulation. J Clin Nurs. 2016;25(15–16):2262–2274. doi:10.1111/jocn.13284
34. Zhou S, Wang JN, Zha LL, et al. Systematic review on the impact of not monitoring gastric residual volume in ICU patients receiving enteral nutrition. J Nurs Sci. 2017;32(1):91–95.].
35. Nguyen N, Ching K, Fraser R, et al. The relationship between blood glucose, control and intolerance to enteral feeding during critical illness. Intensive Care Med. 2007;33(12):2085–2092. doi:10.1007/s00134-007-0869-7
36. Dhaliwal R, Cahill N, Lemieux M, et al. The Canadian critical care nutrition guidelines in 2013: an update on current recommendations and implementation strategies. Nutr Clin Pract. 2014;29(1):29–43. doi:10.1177/0884533613510948
37. Zhang XJ, Li J, Song DD. The effect of an enteral nutrition tolerance assessment and management protocol on patients after pancreaticoduodenectomy. Nurs Pract Res. 2021;18(17):2605–2608.
38. Zhu L, Gao C, Feng YD, et al. Effect of entetal nutrition tolerance assessment form in early postoperative enteral nutrition support of patients with gastric cancer. Modern Clin Nurs. 2015;14(7):18–22.
39. Jianyao GU, Dandan PAN, Zhenqun WU. Effect of self-made Buyi Sanjie decoction adjuvant therapy on postoperative enteral nutrition tolerance and nutrition level in patients with esophageal cancer. Nurs Pract Res. 2019;16(1):82–84.
40. Yanhong WU, Sicheng YUAN, Qinglin RUI. Effect of different moxibustion temperatures on enteral nutrition tolerance in the early stage after gastric cancer surgery. Shanghai J Acu-Mox. 2017;0841–0847.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.