Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Construction and Validation of an Early Warning Model for Predicting the 28-Day Mortality in Sepsis Patients with Chronic Obstructive Pulmonary Disease
Authors Yu X, Jiao Z, Yang F, Xin Q
Received 10 February 2025
Accepted for publication 25 April 2025
Published 6 May 2025 Volume 2025:20 Pages 1373—1385
DOI https://doi.org/10.2147/COPD.S521816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Xiaoyuan Yu,1 Zihan Jiao,2 Fan Yang,3 Qi Xin4
1Department of Hematology, The Affiliated Hospital of Northwest University, Xi’an No. 3 hospital, Xi’an, Shaanxi, People’s Republic of China; 2Shanxi Medical University, Taiyuan, People’s Republic of China; 3Department of Nephrology, Yuequn Yuan District, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China; 4Department of Hepatobiliary Surgery, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China
Correspondence: Qi Xin, The First Affiliated Hospital of Xi’an Jiaotong University, 277 Yanta West Road, Xi’an, 710061, People’s Republic of China, Tel +86-29-85323900, Fax +86-29-85324642, Email [email protected]
Background: In the intensive care unit (ICU), approximately 45.6% of patients diagnosed with chronic obstructive pulmonary disease (COPD) also presented with sepsis, and this cohort exhibited a significantly higher 28-day mortality rate compared to sepsis patients without COPD (23.6% versus 16.4%). A novel nomogram is necessary to predict the risk of mortality within 28 days for sepsis patients with COPD.
Methods: Clinical data from 501 sepsis patients with COPD were sourced from the MIMIC-IV database. These data were randomly allocated into a training cohort and a validation cohort in a 3:1 ratio. Independent predictors of 28-day mortality were identified through both univariate and multivariate logistic regression analyses. Subsequently, a nomogram model was developed, and its performance was assessed using receiver operating characteristic (ROC) curve analysis, calibration plots, and decision curve analysis.
Results: The 28-day mortality rates in the training and validation cohorts were 32.7% and 27.2%, respectively. Multivariate regression analysis identified age, heart rate (HR), respiratory rate (RR), blood urea nitrogen (BUN), creatinine (Cr), lactate levels, pH, and urine output as independent risk factors for 28-day mortality in sepsis patients with COPD. Furthermore, the nomogram demonstrated superior predictive performance, with an area under the curve (AUC) of 0.784 for the training group and 0.689 for the validation group.
Conclusion: This nomogram integrates laboratory indicators pertinent to the patient’s metabolic status, hypoxia status, and organ function, thereby enhancing the accuracy of early prediction of 28-day mortality in sepsis patients with COPD. Additionally, the model’s comparative advantage over existing scoring systems (eg, SOFA) would enhance its impact. Our findings hold substantial implications for early prognostic assessment and clinical decision-making in this patient population. Therefore, earlier diagnosis within 24 hours of admission and proper identification of high-risk patients may reduce disease-related mortality by promoting timely treatment.
Keywords: sepsis, chronic obstructive pulmonary disease, the 28-day mortality, nomogram
Introduction
The advanced age of patients with Chronic Obstructive Pulmonary Disease (COPD), coupled with prolonged chronic non-specific inflammation of the airway, bronchial mucosa, and surrounding tissues, along with heightened airway responsiveness to various stimuli, impaired immune function, obstructed airflow, and numerous complications, increases the likelihood of sepsis development.1,2 Analysis of Medical Information Mart for Intensive Care IV (MIMIC-IV) data indicates that approximately 45.6% of ICU patients diagnosed with COPD also presented with sepsis. Furthermore, the 28-day mortality rate was significantly elevated in this cohort compared to patients with sepsis who did not have COPD (23.6% vs 16.4%).3 Considering the severity of sepsis with COPD, accurate prognostic prediction is of great significance for guiding treatment and patient management.
When COPD and sepsis coexist, the pathophysiological mechanisms underlying disease progression are intricate and distinct, resulting in further deterioration of respiratory function. This is characterized by persistent systemic inflammation, hypoxemia, and thrombotic conditions.3,4 These factors play a crucial role in disease development and may exacerbate the progression of sepsis by enhancing neutrophil-mediated cytotoxicity and modulating dysregulation of the innate immune response.5,6 Moreover, individuals with COPD exhibit an elevated inflammatory state, which is correlated with a poor prognosis in the context of sepsis. At present, while the Sequential Organ Failure Assessment (SOFA) scoring system and other related prediction model are employed to diagnose sepsis in ICU patients and assess their prognosis, they fall short in accurately predicting the prognosis of sepsis patients with COPD. This limitation arises from the inability of these scoring systems and biomarkers to comprehensively capture the intricate complexities involved, resulting in imprecise prognostic predictions.3 Furthermore, the diagnostic value of potential genetic, microbial, and immune biomarkers in evaluating sepsis prognosis among COPD patients has garnered increasing attention. Those biomarkers might further refine the predictive model. However, clinical application requires validation in large-scale cohorts and standardized detection protocols.
Moreover, COPD was identified as an independent risk factor for 28-day all-cause mortality among patients with sepsis.3 This observation underscores the critical importance of employing 28-day all-cause mortality as a primary endpoint, as it not only reflects short-term outcomes for patients with both sepsis and COPD but also facilitates the identification of high-risk patient populations. This approach informs clinical decision-making and resource allocation. Furthermore, employing 28-day all-cause mortality as a definitive and easily quantifiable endpoint can produce reliable data for clinical trials assessing various treatment strategies.7–9 As a result, this metric was chosen as an outcome measure to deepen our understanding and improve clinical outcomes in sepsis patients with COPD, while offering valuable insights for clinical practice.
The MIMIC-IV database, a substantial public repository, contains extensive clinical data pertaining to critically ill patients in ICU. In light of the complex interactions among immune, inflammatory, hypoxic, and thrombotic conditions and their impact on disease progression in sepsis patients with COPD, we aimed to construct a nomogram model utilizing the MIMIC-IV database. This model is designed to predict the risk of 28-day mortality in this patient cohort. This model based on variables available within 24h of admission, serving as a robust instrument for early prognostic evaluation and clinical decision-making, thereby offering substantial clinical benefits.
Materials and Methods
Database introduction
The data employed in this study is derived from the MIMIC-IV database, a comprehensive clinical repository collaboratively developed by the Massachusetts Institute of Technology (MIT), Beth Israel Deaconess Medical Center, and Philips. This database has received funding from the National Institutes of Health since 2003. The clinical data extraction from the MIMIC database was conducted by Qi Xin, one of the contributing authors, who obtained the necessary certification for the Protection of Human Research Participants (certification number: 53163698).
Study Population and Definitions
The study population comprised adults diagnosed with both sepsis and COPD in the intensive care unit (ICU). Sepsis was identified in accordance with the Sepsis-3 criteria, necessitating a probable infectious etiology and a SOFA score of 2 or higher.10,11 The diagnosis of COPD was established based on the ICD-9 codes.12 The exclusion criteria were as follows: (1) individuals under the age of 18; (2) an ICU stay of less than 24 hours; (3) patients with multiple ICU admissions; and (4) incomplete data, including missing laboratory test indicators. The primary outcome measure in this study is the 28-day mortality rate.
Data Collection
Patient data were extracted from the MIMIC IV database, encompassing the following categories of information: (1) Basic demographic and clinical information, including age, gender, respiratory rate (RR), heart rate (HR), mean arterial pressure (MAP), body temperature (T), and diagnoses such as myocardial infarction, diabetes, and congestive heart failure; (2) Laboratory examination results, comprising hematocrit (HCT), hemoglobin (Hb), platelet count (PLT), white blood cell count (WBC), international normalized ratio (INR), activated partial thromboplastin time (APTT), prothrombin time (PT), pH, peripheral capillary oxygen saturation (SpO2), and partial pressure of carbon dioxide (PCO2), partial pressure of oxygen (PO2), base excess (BE), total carbon dioxide (Total CO2), bicarbonate (HCO3−), anion gap (AG), creatinine (Cr), blood urea nitrogen (BUN), sodium (Na+), potassium (K+), calcium (Ca2+), chloride (Cl−), glucose, lactate, the application of continuous renal replacement therapy (CRRT), length of hospital stay (LOS hospital), length of Intensive Care Unit stay (LOS ICU), SOFA score, and urine output.
Sample Size
Based on previous studies, which identified 5–10 potential predictors for modeling, and considering a 25% 28-day mortality rate observed in preliminary investigations, we estimated that a sample size of 200–400 patients, yielding 50–100 instances of 28-day mortality, would be necessary to achieve sufficient precision in model construction. This estimation adheres to the principle of having at least ten outcome events per variable in regression analysis.
Statistical Analysis
The final cohort of patients was randomly allocated into a training group and a validation group in a 3:1 ratio. Continuous variables following a normal distribution are presented as mean ± standard deviation, whereas those not adhering to a normal distribution are expressed as median with interquartile range. Categorical variables are reported as percentages. Logistic regression analysis was employed to identify potential risk factors for 28-day mortality events, and multivariate logistic regression analysis was utilized to develop a nomogram. Receiver operating characteristic (ROC) curves were employed to evaluate the accuracy of the nomogram in predicting 28-day mortality. Calibration curves were utilized to assess the concordance between observed outcomes and predicted probabilities. Additionally, decision curve analysis (DCA) was conducted to determine the clinical net benefit of the predictive model.
Statistical analyses were conducted utilizing R software, version 4.1.3, with the significance level established at P < 0.05.
Results
Basic Characteristics
The study included a total of 1487 eligible participants sourced from the MIMIC IV database (Figure 1). The participants had a median age of 72 years and consisted of 228 women (45.5%) and 273 men (54.4%). The clinical characteristics of these participants are comprehensively outlined in Table 1. Importantly, the training group demonstrated good comparability with the test group concerning baseline clinical data (p>0.05). Among all participants, 157 individuals (31.3%) succumbed within 28 days of hospitalization.
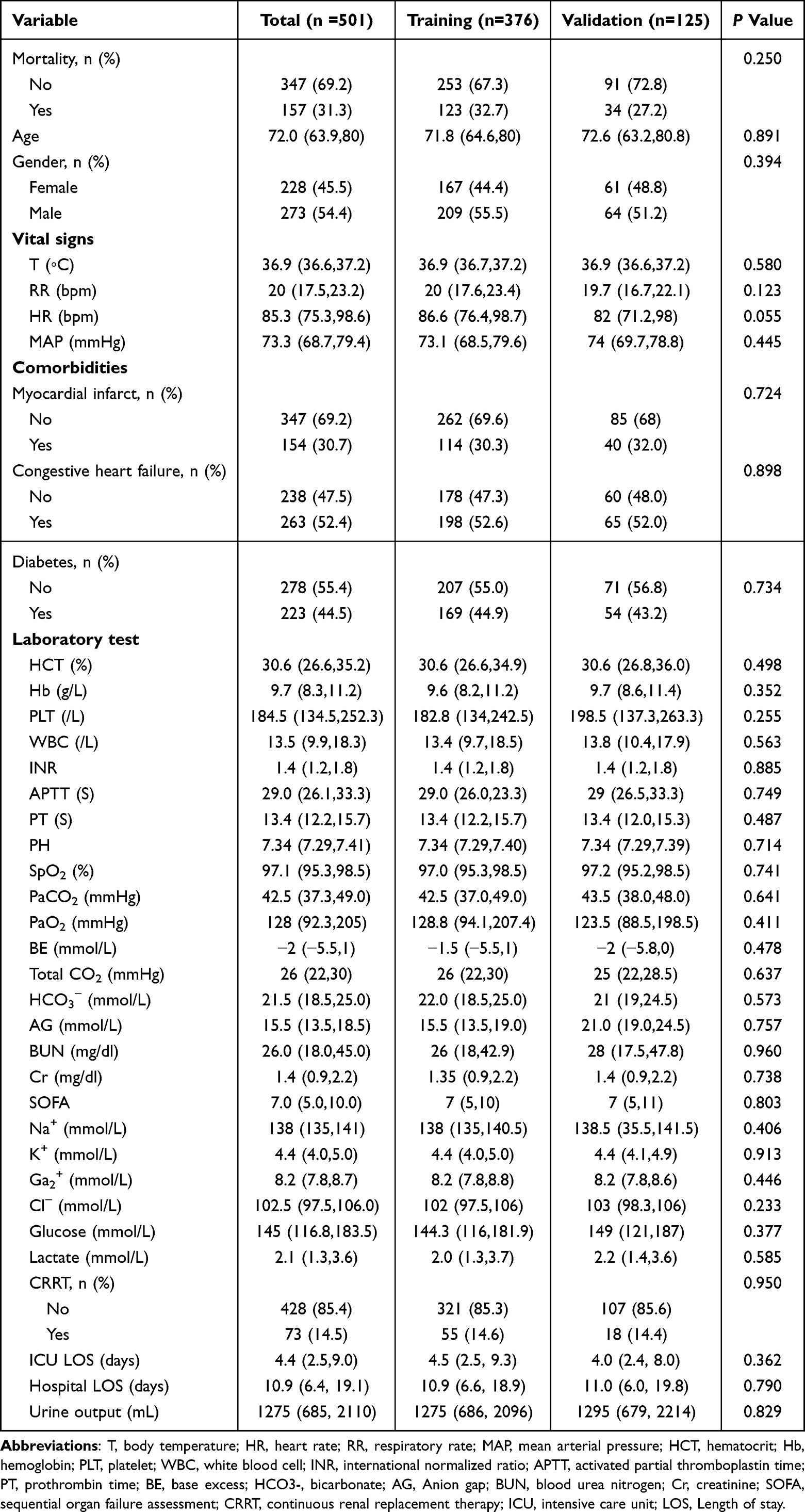 |
Table 1 Baseline Characteristics of the Sepsis Patients with Chronic Obstructive Pulmonary Disease |
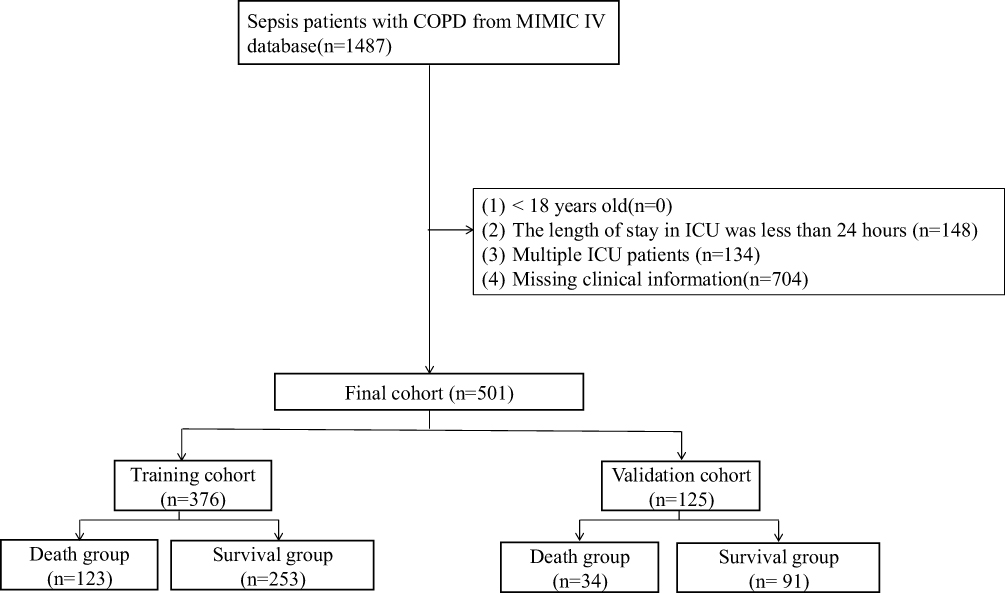 |
Figure 1 The flowchart of patient selection from the MIMIC-IV. |
Development of Nomogram
Univariate logistic regression analysis identified 18 variables significantly associated with 28-day mortality, including age, HR, RR, T, SOFA score, hemoglobin, AG, HCO3−, BUN, Cr, INR, PT, SpO2, lactate, pH, BE, Total CO2, and urine output (Table 2). Subsequent multivariate regression analysis of the training set, utilizing these significantly different variables, identified age, HR, RR, BUN, Cr, LAC, pH, and urine output as independent risk factors for 28-day mortality in sepsis patients with COPD (Table 3). Utilizing these variables, a nomogram was developed to predict the incidence of 28-day mortality in sepsis patients with COPD (Figure 2).
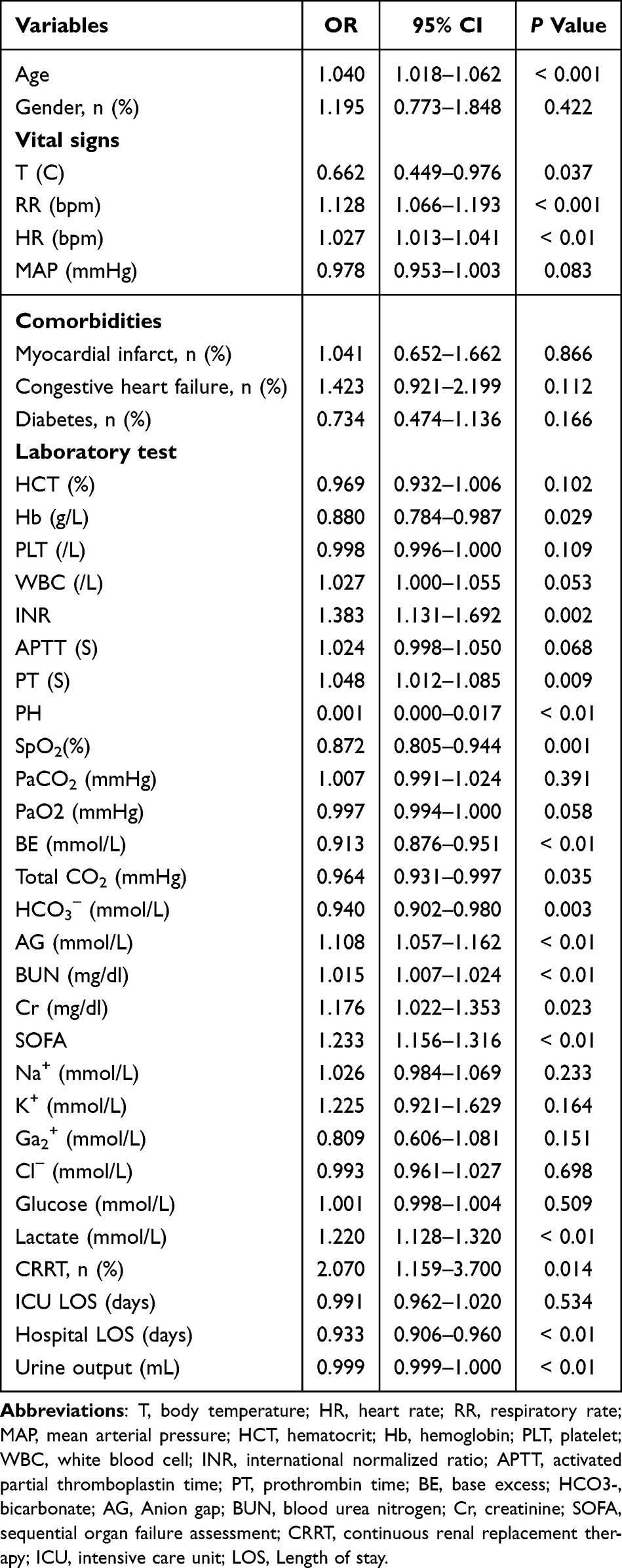 |
Table 2 Univariate Analysis of Predictive Variables of the 28-Day Mortality in the Training Cohort |
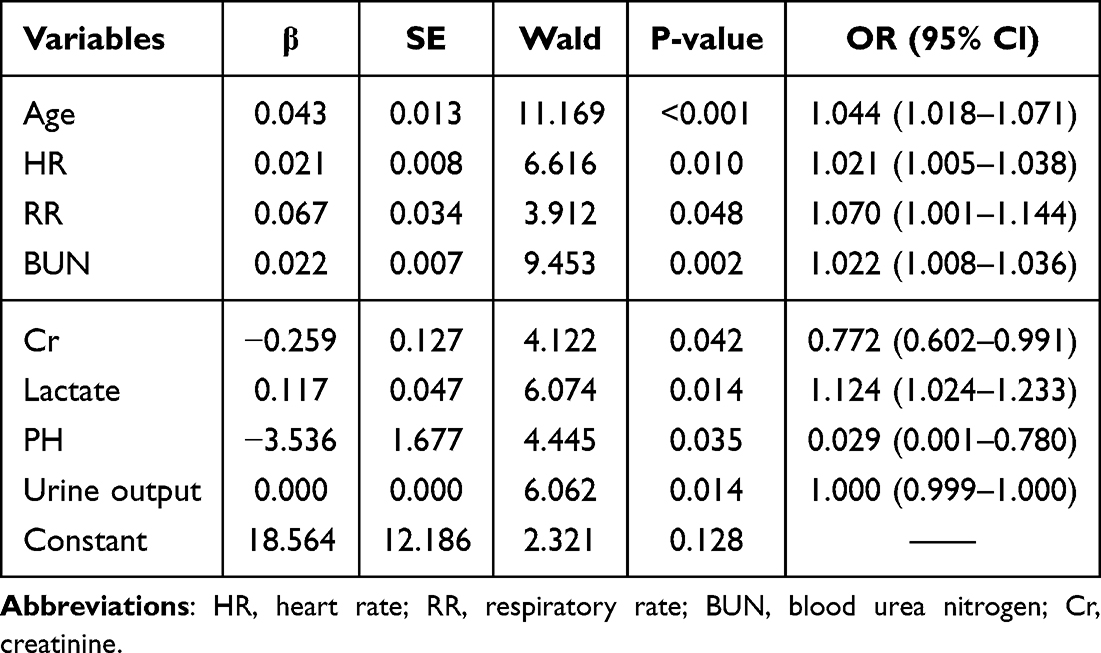 |
Table 3 Multivariate Logistic Regression Analysis of Independent Predictors of the 28-Day Mortality in the Training Cohort |
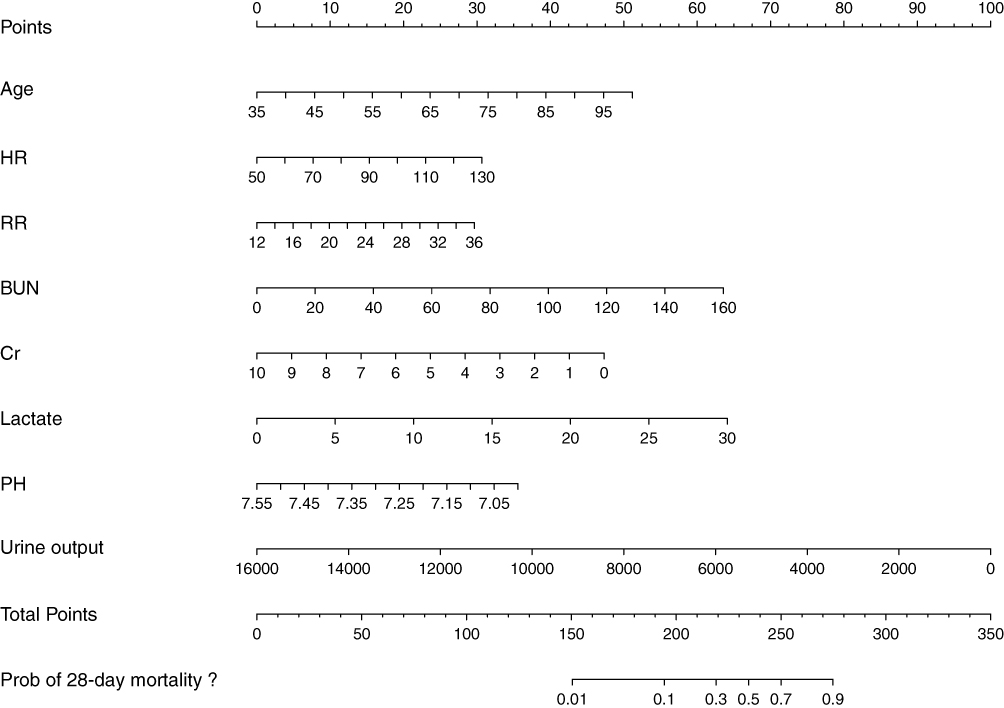 |
Figure 2 Nomogram to estimate the risk of the 28-day mortality in sepsis patients with chronic obstructive pulmonary disease. Abbreviations: HR, heart rate; RR, respiratory rate; BUN, blood urea nitrogen; Cr, creatinine; LAC, lactate. |
Verification of Nomogram
The ROC curve analysis results indicated that the model exhibited a robust capability to differentiate 28-day mortality among sepsis patients with COPD, achieving an AUC of 0.784 in the training cohort (Figure 3A) and 0.689 in the validation cohort (Figure 3B). Conversely, the AUC for predicting 28-day mortality using SOFA scores was 0.703 (Figure 3C) in the training group and 0.654 (Figure 3D) in the validation group. As shown in Table 4, the nomogram had a higher specificity value compared to SOFA scores (85.8% vs 71.1%) in the training cohort. In addition, the nomogram had a higher sensitivity value compared to SOFA scores (61.8% vs 47.1%) in the validation cohort. These findings imply that the nomogram model possesses a superior predictive value compared to SOFA scores. The calibration curve demonstrated that the predicted probabilities were consistently aligned with the observed outcomes in both the training and validation cohorts, indicating successful calibration (Figure 4A and B). An analysis of the DCA (Figure 4C and D) reveals that the nomogram demonstrates a substantial overall net benefit across a wide spectrum of threshold probabilities, suggesting considerable potential for clinical application.
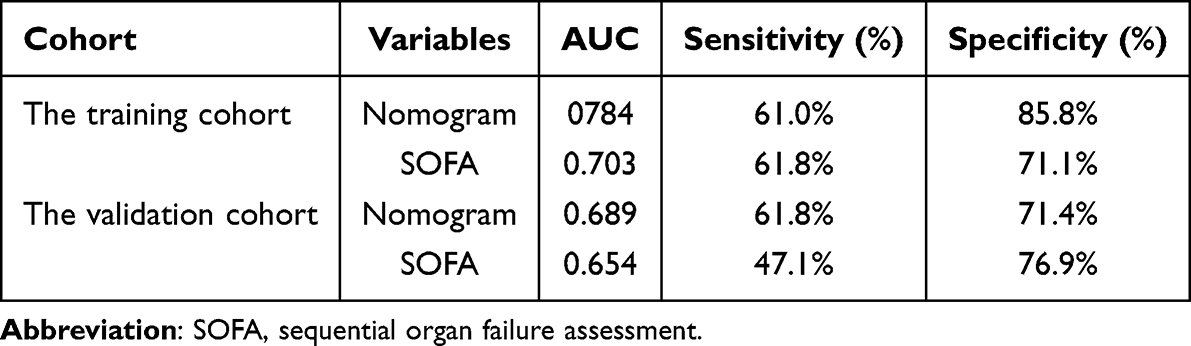 |
Table 4 ROC Curve Analyses of Prediction Model for the 28-Day Mortality |
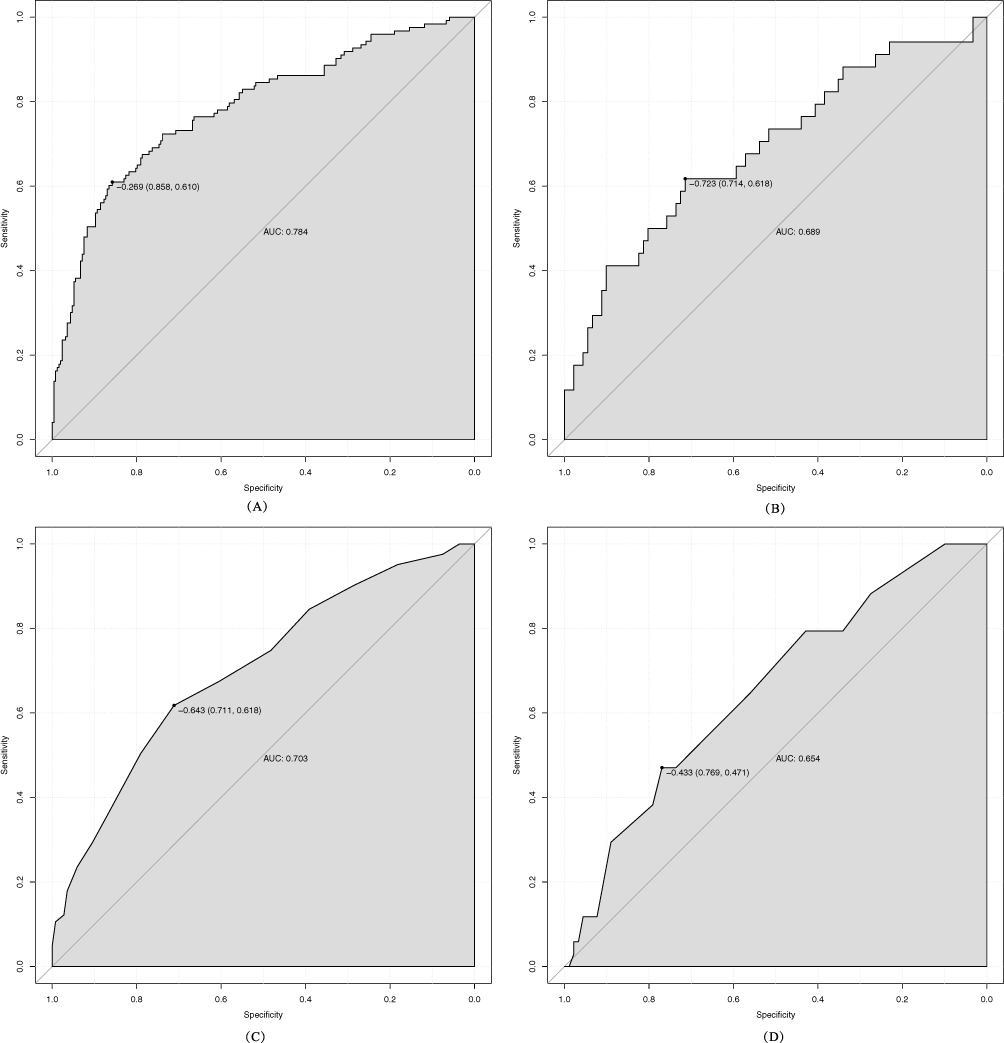 |
Figure 3 The ROC curve of the nomogram for predicting the 28-day mortality in sepsis patients with chronic obstructive pulmonary disease. The AUC of the nomogram for the prediction of the 28-day mortality in the training set (A) and the validation set (B). The AUC of SOFA for the prediction of the 28-day mortality in the training set (C) and the validation set (D). Abbreviations: ROC, receiver operating characteristics curve; SOFA, sequential organ failure assessment. |
 |
Figure 4 Calibration curves and DCA of the nomogram for predicting the 28-day mortality. Calibration curves of the predicted nomogram in training set (A) and validation set (B); DCA of the nomogram in the training set (C) and the validation set (D). Abbreviation: DCA, Decision curve analysis. |
Discussion
COPD is one of the prevalent comorbidities of sepsis. A study conducted based on the MIMIC-IV database indicated that the prevalence of COPD among patients with sepsis was 15.3%, involving 6257 patients with sepsis.3 Recent studies have proposed that systemic inflammation,13 prothrombotic conditions,14,15 and oxidative stress16 associated with COPD may play a role in the progression of sepsis.17 Concurrently, the onset of sepsis can act as a catalyst for acute exacerbations of COPD.18 The interplay between the pathophysiological mechanisms of COPD and sepsis often results in a poorer prognosis for patients experiencing both conditions.3 Nevertheless, the precise factors influencing disease progression and patient outcomes in the context of coexisting COPD and sepsis remain inadequately elucidated. Considering the diverse factors influencing disease progression in patients with COPD complicated by sepsis, we extracted a set of common biomarkers associated with immune function, inflammation, metabolism, and circulation from the MIMIC-IV database for comprehensive analysis. Our findings revealed significant associations between age, respiratory rate, heart rate, blood urea nitrogen, creatinine, urine output, lactic acid, pH, base excess, anion gap, and the SOFA score with mortality events occurring within 28 days. Based on the findings, we identified critical variables including age, respiratory rate, heart rate, urea nitrogen, creatinine, urine volume, lactic acid, and pH, and subsequently developed predictive models utilizing multivariate regression analysis. Our nomogram model demonstrated superior predictive accuracy for 28-day mortality events in comparison to the SOFA scores. The results indicated that the mortality rate among sepsis patients with COPD within 28 days was 32.7% in the training set and 27.2% in the validation set.
Our findings indicate that the risk of 28-day mortality is elevated in older patients suffering from COPD in conjunction with sepsis. Prior research has demonstrated that elderly individuals with COPD tend to exhibit higher Simplified Acute Physiology Score II (SAPSII) values and a greater likelihood of requiring mechanical ventilation support.19,20 This increased risk may be attributed to the generally poorer health status of older patients, diminished immune function, a higher prevalence of comorbidities, a reduced capacity to mobilize physiological reserves in response to sepsis, and more pronounced immune dysfunction during the onset of sepsis.21 Furthermore, the presence of long-term chronic inflammation, hypoxemia, and hypercapnia in elderly patients with COPD may exacerbate the effects of sepsis on the body.22,23 Additional research indicates that older patients with COPD exhibit an elevated incidence of cardiovascular disease, and that systemic inflammation, hypoxia, and prothrombotic conditions may heighten the risk of cardiovascular events in those experiencing sepsis.24,25
In this study, HR and RR were identified as independent risk factors for adverse outcomes in sepsis patients with COPD. This finding is corroborated by previous research. Previous study examined the clinical characteristics of patients with severe pneumonia and sepsis, revealing that the respiratory rate was significantly elevated in the mortality group compared to the survival group.26 A multifactorial retrospective analysis further established respiratory rate as an independent prognostic indicator. In COPD patients, who inherently suffer from airway inflammation and restricted airflow, the additional lung infection and inflammation induced by sepsis exacerbate respiratory dysfunction, leading to an increased respiratory rate. This elevation may represent a compensatory mechanism in response to hypoxia and metabolic acidosis; however, sustained high respiratory rates can further compromise pulmonary function, thereby negatively impacting patient outcomes. Furthermore, an elevated heart rate is also recognized as a crucial prognostic marker in patients with sepsis. The observed elevation in heart rate may be attributed to the systemic inflammatory and stress responses elicited by sepsis.27,28 In individuals with COPD, an increased heart rate may indicate heightened cardiac workload and compromised cardiac function. Cardiac inhibition constitutes a critical aspect of organ dysfunction in sepsis patients, potentially linked to dysregulated nitric oxide (NO) metabolism and cardiomyocyte apoptosis. Consequently, elevated heart and respiratory rates may serve as clinical indicators of inadequate circulating blood volume in these patients.29,30 Monitoring heart and respiratory rates is crucial for assessing the prognosis of patients with COPD and sepsis, as these parameters not only reflect the physiological stress state but also may signal underlying organ dysfunction and an unfavorable prognosis. Further research is warranted to elucidate the relationship between these physiological parameters and patient outcomes in COPD and sepsis, thereby providing more precise guidance for clinical management.
The findings of this study indicate that patients with renal insufficiency who have COPD combined with sepsis exhibit a poor prognosis. Previous retrospective studies have identified BUN, Cr, and urine output as effective indicators for assessing the prognosis of critically ill patients in clinical settings.31–33 Our results further underscore the importance of evaluating and managing renal insufficiency in sepsis patients with COPD to improve their prognosis. Elevated BUN levels may reflect an intensified inflammatory response in COPD patients, which is crucial in the disease’s development and progression.34 Serum levels of inflammatory markers, such as TNF-α and IL-6, are significantly elevated in COPD patients, particularly during acute exacerbations.35 These inflammatory factors may contribute to protein catabolism, resulting in increased BUN levels. Elevated BUN levels indicate heightened metabolic activity as a byproduct of protein metabolism, and sustained high metabolism can lead to compromised nutritional status and immune function.36 This deterioration in baseline health status can exacerbate the risk of infection. Reduced serum creatinine levels serve as a direct indicator of diminished muscle mass. During acute exacerbations of COPD, circulating levels of TNF-α increase significantly. Elevated TNF-α levels are closely associated with acute weight loss and reduced muscle mass, which can lead to diaphragm fatigue and diminished respiratory muscle strength, thereby heightening the risk of respiratory failure and mortality in patients. Urine volume is indicative of renal clearance capacity. In sepsis patients with COPD, impaired renal clearance can result in the accumulation of toxins and metabolic waste, exacerbating organ dysfunction and adversely affecting patient prognosis. Furthermore, sepsis-associated acute kidney injury (S-AKI) is influenced by multiple factors, including a history of chronic kidney disease, elevated cystatin C levels, and organ failure. These factors are implicated in the onset of S-AKI. Identifying and monitoring the risk factors for S-AKI to prevent the early occurrence of acute kidney injury can enhance the prognosis for sepsis patients.
Furthermore, our study identifies pH and lactate levels as independent risk factors for adverse outcomes in sepsis patients with COPD. Previous retrospective analyses have demonstrated a strong correlation between lactate levels and mortality in sepsis patients.37–39 In sepsis individuals with COPD, elevated lactate levels may indicate the degree of tissue hypoxia, a condition often arising from insufficient oxygenation due to the underlying pulmonary disorder. The pH value serves as a critical indicator of the body’s acid-base equilibrium. In sepsis patients, the accumulation of lactic acid can lead to metabolic acidosis, thereby influencing the pH value. A decrease in pH further signifies a diminished capacity of the body to buffer acid loads, which is associated with increased severity and mortality in patients with COPD and sepsis.40
Limitations
The study is subject to several limitations. Firstly, as it is a retrospective analysis utilizing secondary data, there is a potential for inherent selection bias. Secondly, all models are developed and validated using the MIMIC-IV database, which may impact their reliability. To enhance confidence in the findings, future validation efforts should employ independent datasets. Thirdly, the diagnosis of COPD is based on the ICD-9 code rather than spirometry measurements (specifically, a forced expiratory volume in one second/forced vital capacity ratio of less than 0.70 following bronchodilator administration), which may result in the overdiagnosis of COPD.41 Furthermore, the 1-second forced expiratory volume (FEV1), D-dimer and fibrinogen degradation products (FDPs) may be critical risk factors for disease progression in sepsis patients with COPD. Nevertheless, the absence of this data for the majority of patients in the MIMIC-IV database introduces potential confounding variables that may influence the study’s outcomes.42 Therefore, further multi-center prospective studies with more useful variables added would be needed to verify the results.
Conclusion
In this study, parameters including age, heart rate, respiratory rate, urea nitrogen, creatinine, lactic acid, pH, and urine volume were identified as potential biomarkers for assessing the 28-day mortality in sepsis patients with COPD. Such an accurate prognostic nomogram based on the above predictors is crucial for clinicians in formulating personalized management strategies and making timely treatment adjustments, ultimately aiming to reduce mortality rates and improve patient survival outcomes.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and received approval from the Ethical Committee of the First Affiliated Hospital of Xi’an Jiaotong University (approval number: XJTU1AF2020LSL-003). All patient data were analyzed anonymously. The ethics committee waived the requirement for patient consent, as no individual data were published, and no interventions were performed on the patients.
Acknowledgments
We acknowledged the contributions of the MIMIC Program registries for creating and updating the MIMIC-IV databases.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Stephanie AC, Benjamin MS, Mona B, Nirupama P. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242.
2. Daiana S, Takudzwa M, Desirée S, et al. Towards the elimination of chronic obstructive pulmonary disease: a Lancet Commission. Lancet. 2022:400:921––972.
3. Yubiao C, Lifei L, Xicong L, et al. Association between chronic obstructive pulmonary disease and 28-day mortality in patients with sepsis: a retrospective study based on the MIMIC-III database. BMC Pulm Med. 2023:23:435.
4. Umer Ahmed S. Electrolytes Imbalance In Acute Exacerbation Of COPD. Chest. 2019;156(4):A1673.
5. John RH, Antonio A, Jørgen V. Susceptibility to exacerbation in COPD. Lancet Respir Med. 2017;363(27):2670–2671.
6. Suzanne CL, Erika MM, Christopher GS. Exacerbation of COPD. Am J Respiratory Critl Care Med. 2018;2018:1.
7. Erdinç K, Sevgi K, Ahmet A, Umut Sabri K. The influence of SARS-CoV-2 vaccination on 28-day mortality and hospitalization rate of COVID-19 patients under 40 years. Türk Fen ve Saglik Dergisi. 2023;4:147–152.
8. Yazan Majed K, Mohammed Ali Mahmoud O, Abdel Karim Ahmad Dawood A, Mohammad Solaiman Ali A, Ala’a Ibrahim Hamed Dmour Mohammad Ahmad S. The Prognostic Value of Charlson Comorbidity Index for Prognosticating 28-Day Mortality Rate in Critically I’ll Covid-19 Infected Patients. IAR Journal of Anaesthesiology and Critical Care. 2021;2:1.
9. Martin JL, Peter H, Jonathan E, et al. Convalescent plasma in patients admitted to hospital with COVID-19 (RECOVERY): a randomised controlled, open-label, platform trial. Lancet. 2021;399(10342):2049–2059.
10. Mervyn S, Clifford SD, Christopher WS, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315:801–810.
11. Alistair EWJ, Jérôme A, Jesse DR, et al. A Comparative Analysis of Sepsis Identification Methods in an Electronic Database*. Crit Care Med. 2018;46:494–499.
12. Mengling F, Jakob IM, Trung Kien D, et al. Leo Anthony C: transthoracic echocardiography and mortality in sepsis: analysis of the MIMIC-III database. Intensive Care Med. 2018;44:884–892.
13. Wen Qi G, Man SFP, Ambikaipakan S, Don DS. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59:574–580.
14. Christos K, Christos C, Evaggelia P, et al. Prothrombotic state in patients with stable COPD: an observational study. ERJ Open Res. 2021;7:1.
15. Gunnar Reksten H, Esteban CG, Corina D’Alessandro G, et al. Coagulation markers as predictors for clinical events in COPD. Respirology. 2020;26:342.
16. María M, María Mercedes N-G, Francisco D. Oxidative Stress in COPD. J Clin Med. 2019;144:266–273.
17. Annette E, Greg SM. The impact of cormorbid conditions on critical illness. Crit Care Med. 2011;39:2728–2735.
18. Salil C, Arushi K, Suraj S, et al. Impact Of Sepsis On Outcomes Of Hospitalizations Due To COPD. Chest. 2021;160;A1906.
19. Divay C, Jason S, Brian T, et al. Outcomes of Noninvasive Ventilation for Acute Exacerbations of Chronic Obstructive Pulmonary Disease in the United States, 1998–2008. Am J Respiratory Critl Care Med. 2012;185:152–159.
20. Bryan Z, Michael ER. Noninvasive Positive Pressure Ventilation for Exacerbation of Chronic Obstructive Pulmonary Disease. American Family Physician. 2020;101:1.
21. Yuandi W, Zhenyue L, Yuqiong Y, et al. Relationship Between Nutritional Status And Lung Function In Hospitalized Elderly Patients With Acute Exacerbation Of Chronic Obstructive Pulmonary Disease Based On Geriatric Nutritional Risk Index. Respirology. 2019;24:41–42.
22. Rahma S, Fehri SM, Imen K, Kwass H. Chronic obstructive pulmonary disease in elderly. Clinics in Geriatric Medicine. 2023;33:539–552.
23. Xiaowei G, Yanan W, Dan G, Jun M, Caijuan Z, Qiuyan W. Risk factors for the prognosis of patients with sepsis in intensive care units. PLoS One. 2022 17(9):e0273377.
24. Sandra A, Condé B, Elsa F, José Pedro B-T, Vanda A, João C. COPD and Cardiovascular Disease. Pulmonology. 2019;25:168–176.
25. John DM, William M. Cardiovascular Disease in COPD. Chest. 2013;143:798–807.
26. Che Uk L, You Hwan J, Jae Hyuk L, et al. The index of oxygenation to respiratory rate as a prognostic factor for mortality in Sepsis. Am J Emergency Med. 2021;45:426–432.
27. Yukang D, Rui H, Jiangquan F. Association between ROX index with 28-day mortality in sepsis: a retrospective cohort study. Research Square. 2023;45:426–432.
28. R-r H. The analysis of clinical risk factors in elderly patients with severe pneumonia complicated with multiple organ failure. J Clin Exp Medi. 2013;2013:1.
29. Eunice D, Robert SS, Steven PS, Thomas SM. Abstract 15010: myocardial Injury in Sepsis with Acute Respiratory Distress Syndrome. Circulation. 2020;142:A15010.
30. Sivapathan S, Gehardy B, Faraz P, Sam O, Kazuaki N. A review of current landscape and definition of septic cardiomyopathy. Eur Heart J. 2023;44(Supplement_2):655–1107. doi:10.1093/eurheartj/ehad655.1107
31. Guillaume M, Kalyane B-N, Éric B, Damien M, David T. Diagnostic performance of serum blood urea nitrogen to creatinine ratio for distinguishing prerenal from intrinsic acute kidney injury in the emergency department. BMC Nephrol. 2017;18:1–7.
32. Vahid M. Practical approach to detection and management of acute kidney injury in critically ill patient. J Intens Care. 2017;5:1–8.
33. Mohammed E, Peter WC, Argenis C. The Conundrum of Volume Status Assessment: revisiting Current and Future Tools Available for Physicians at the Bedside. Cureus. 2021;13(5):1.
34. Lan C, Lijun C, Han Z, Sunying W, Saibin W. The association of blood urea nitrogen levels upon emergency admission with mortality in acute exacerbation of chronic obstructive pulmonary disease. Chron Respir Dis. 2021;8:14799731211060051.
35. Jie D, Jing N, Lifang M, Yongjie S, Shuili W. Association Between Blood Urea Nitrogen Levels and Length of Stay in Patients with Pneumonic Chronic Obstructive Pulmonary Disease Exacerbation: a Secondary Analysis Based on a Multicentre, Retrospective Cohort Study. Int J Chronic Obstr. 2022;2022:2847–2856.
36. Kevin TB, Sabitha E, Heidi SB, et al. Elevation of blood urea nitrogen is predictive of long-term mortality in critically ill patients independent of “normal” creatinine*. Crit Care Med. 2011;39:305–313.
37. Mark EM, Andrea M, David FG, et al. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock*. Crit Care Med. 2009 37(5):1670–1677.
38. Roberto Rabello F, Leonardo Lima R, Thiago Domingos C, Camila Menezes Souza P, Giancarlo C, Murillo Santucci César de A. Blood Lactate Levels Cutoff and Mortality Prediction in Sepsis—Time for a Reappraisal? A retrospective cohort study. Shock. 2016;46:480–485.
39. Julian V, Jack HS, Geoffrey KL. Lactate predicts both short- and long-term mortality in patients with and without sepsis. Infect Dis. 2019;12:1178633719862776.
40. Kartik G, Sharma RN, Jaicob V, Pillai MG. A profile of metabolic acidosis in patients with sepsis in an Intensive Care Unit setting. Int J Criti Illness Injury Sci. 2016;6:178–181.
41. Dave S, Àlvar A, Antonio A, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Europ resp J. 2019;53:1.
42. Manganas H, Yves L, Stéphanie B, Jean P, François D, François M. Postoperative Outcome after Coronary Artery Bypass Grafting in Chronic Obstructive Pulmonary Disease. Canad Respirat J. 2007, 14:19–24. doi:10.1155/2007/378963
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.