Back to Journals » Risk Management and Healthcare Policy » Volume 16
Construction and Scale Development of Willingness to Utilize Primary Care Services: A Study from China
Received 12 July 2023
Accepted for publication 12 October 2023
Published 20 October 2023 Volume 2023:16 Pages 2171—2185
DOI https://doi.org/10.2147/RMHP.S428369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Ziyang Li, Zhiqiang Ma
School of Management, Jiangsu University, Zhenjiang, People’s Republic of China
Correspondence: Zhiqiang Ma, School of Management, Jiangsu University, Zhenjiang, People’s Republic of China, Tel +86 1 535 858 2636, Email [email protected]
Purpose: The willingness to utilize primary care services is crucial in explaining residents’ healthcare-seeking behavior and decision-making in the context of the free choice of healthcare providers. This study examines China’s family doctor contracting services system to elucidate the conceptual structure of the willingness to utilize primary care services and develop a reliable measurement tool.
Methods: The study was conducted in two phases. Firstly, in-depth interviews were conducted with community residents, resulting in 42 qualitative data sets. Subsequently, a measurement scale for the willingness to utilize family doctor contracting services was developed, and the scale was validated through two surveys using exploratory factor analysis (N = 250) and confirmatory factor analysis (N = 278), respectively.
Results: By employing a grounded theory approach, this study analyzes the connotation of willingness to utilize family doctor contracting services. It constructs a conceptual framework for the willingness to utilize primary care services. This conceptual framework consists of three dimensions: perceived feasibility, perceived desirability, and perceived initiative. Based on this framework, a measurement scale comprising 14 items was developed and subjected to rigorous validation procedures to ensure its reliability and validity.
Conclusion: This study extends prior research on healthcare service utilization willingness by elucidating the internal willingness structure for primary healthcare services. It enhances our understanding of the connotation of healthcare service utilization willingness and develops a scientifically rigorous measurement tool. The findings of this study provide valuable insights into improving both the willingness and behavior of utilizing primary care services in healthcare systems where the hierarchical referral system still needs to be fully developed.
Keywords: family doctor contracting services, primary care utilization willingness, grounded theory, scale development
Introduction
China’s three-tier healthcare system consists of primary healthcare service institutions, secondary hospitals, and tertiary hospitals. Residents have the freedom to choose healthcare service institutions for medical treatment. Therefore, it does not represent a rigorous hierarchical referral system. The unique nature of healthcare services and the insufficient service capacity of primary healthcare institutions have led to a significant inclination among residents to seek higher-level healthcare facilities. Regardless of the severity of their symptoms, residents tend to bypass primary healthcare institutions and directly seek treatment at higher-level hospitals.1 As a result, higher-level hospitals become overcrowded while primary healthcare institutions struggle to fulfill their functions. Consequently, higher-level hospitals continue to attract talent and introduce advanced medical equipment, further widening their advantages within the healthcare system. This situation exacerbates the imbalance in healthcare resource allocation, leading to the overutilization of medical services and the wastage of a substantial amount of healthcare insurance funds. Moreover, residents find it difficult to access high-quality healthcare experiences. To address the chaotic competition among hospitals at different levels, the Chinese government, including the State Council’s Health Reform Office and the Ministry of Civil Affairs, jointly issued the “Guiding Opinions on Promoting Family Doctor Contracting Services” in 2016 to promote the development of family doctor contracted services. The goal is to enable primary care as the first point of contact and implement a hierarchical medical system, providing comprehensive, continuous and coordinated essential healthcare services to the population.2
Family doctor contracting services represent a manifestation of primary care services. They aim to enhance residents’ utilization of primary healthcare institutions by signing service contracts with family doctor teams. The aim is to change residents’ healthcare-seeking habits and facilitate the development of a hierarchical referral system. During the promotion of family doctor contracted services, the Chinese health administration authorities have regarded the signing rate of residents as a primary assessment criterion. Consequently, the number of individuals signing up for family doctor contracted services in China has rapidly increased.3 However, the utilization of primary healthcare institutions has yet to show a corresponding improvement. According to medical service data released by the National Bureau of Statistics of China from January to November 2022, the number of visits to community health service centers decreased by 4.4% compared to the previous year.4 The reasons for this can be attributed to several factors. Firstly, in some provinces and cities, government departments and grassroots healthcare institutions have included residents in the signing service system without their knowledge to increase the number of sign-ups, resulting in inaccurate figures. Secondly, it is related to the establishment of a hierarchical medical system. In countries like the United Kingdom and Australia, residents must consult primary healthcare service providers before seeking referral from their general practitioners for specialist hospital visits. However, in China, residents have complimentary choices for healthcare decisions, and primary healthcare institutions are one option among many. According to rational behavior theory and planned behavior theory, willingness is essential in determining behavior.5,6 Individuals require a certain level of willingness before deciding to utilize a specific service. The willingness of residents to use family doctor services reflects their degree of endorsement for this service model and serves as the foundation for their utilization of primary healthcare services. Furthermore, residents may include primary healthcare services as one of their healthcare options and, in their healthcare decision-making, translate their willingness into actual utilization. This transformational process progressively clarifies the role of primary healthcare services within the tiered healthcare system. Therefore, residents’ willingness to use primary healthcare services can also be considered a prerequisite for the orderly operation of the tiered healthcare system. To accurately grasp the actual attitudes of residents, this study employs a grounded theory approach to explore the essence and scope of willingness to utilize family doctor contracting services. It develops a corresponding measurement scale following scientific procedures to enhance the theoretical framework of willingness to utilize primary care services.
Literature Review
Connotation of Utilization Willingness for Healthcare Services
Fishbein and Ajzen argue that individual behavior cannot be predicted solely based on attitudes and that assessing whether a willingness to carry out the behavior is necessary.7 According to Eagly and Chaiken, willingness is a subjective inclination distinct from individual attitudes and represents the conscious motivation of individuals before carrying out a specific behavior.8 Bell and Bucklin further suggest that willingness is the probability of an individual engaging in a specific behavior, with more vital willingness indicating a greater likelihood of performing that behavior.9 In marketing, Fishbein and Manfredo propose that consumer purchase willingness explains consumers’ final purchase behavior and represents their attitudes before purchasing.10 According to Schiffman and Kanuk, purchase intention is the subjective perception of individual consumers, representing their intention to purchase a particular product. It can measure the likelihood of consumer purchases, showing a positive correlation with purchase behavior. In healthcare-related willingness research, willingness to pay (WTP) to improve health is essential for measuring the willingness to utilize medical and health services. Examples include willingness to pay for digital health technologies,11 willingness to pay for oral health,12 willingness to pay for treating asthma symptoms.13
Regarding primary care services, the researchers examined the willingness of residents to be vaccinated against Covid-19 and the patients with hypertension’s willingness to pay for their preferred medical treatments.14,15 China’s family doctor contracting services encompass a wide range of services, with slight variations in service offerings across different provinces and cities. These services primarily include prevention and treatment of common diseases, health consultations, and home care.16 Qiu et al define the content of contracted services as initial consultation services, referral services, and services for chronic diseases.17 Hu and Huang consider the main content of contracted services to include medication guidance, blood pressure monitoring, blood glucose monitoring, and other services.18 Sun et al in their study on the utilization of family doctor contracting services in a community in Beijing, examined both the free essential services and some additional services, such as distributing health education materials, conducting health knowledge lectures, health promotion activities, health consultations, and referral services.19
In the studies mentioned above, scholars defined the utilization willingness of primary care services as whether residents accept specific service offerings. Some scholars also focus on residents’ willingness for initial consultations.20,21 For instance, the willingness to utilize primary care services is defined as “whether residents are willing to seek medical care at community health service institutions under normal circumstances”.22 In addition, residents’ willingness to enter into service contracts with family doctors23 and their willingness to renew service contracts24–26 have also been used to explain residents’ utilization willingness for primary care services.
Measurement of Medical and Health Service Utilization Willingness
Zeithaml conceptualized willingness as a subjective behavior categorized into positive and negative inclinations, exhibiting a unidimensional structure.27 Prior studies have employed different indicators to measure the intensity of consumers’ purchase willingness. For instance, repurchase willingness was used by Gümüş28 and Pan et al.29 Wang et al assessed future consumption willingness.30 Regarding the measurement of utilization willingness for healthcare services, Zhao et al used indicators such as willing and unwilling,31 while Alsulaiman et al measured parental willingness to vaccinate their children using five indicators: strongly agree, agree, neutral, disagree, and strongly disagree.32
In primary care services, the measurement of willingness primarily focuses on residents’ willingness to sign up or renew service contracts. For instance, Wang et al investigated residents’ willingness to sign up for primary care services using three indicators: willing, unwilling, and undecided.33 Xu et al measured residents’ signing-up willingness using four options: willing, unwilling, undecided, and indifferent.34 Wang et al evaluated residents’ willingness to renew their contracts for family doctor services using the indicators willing and unwilling.25
The existing research on the conceptual definition of utilization willingness for primary care services focuses on residents’ inclination to seek initial consultations and medical care or utilize specific service offerings within primary healthcare institutions. China’s family doctor contracting services encompass a wide range of services, including essential public health services and personalized services that require additional fees, such as health management services for patients with chronic diseases, pregnant women, and postpartum women. Therefore, studies examining the willingness to utilize individual medical service offerings cannot fully capture the characteristics of primary care services nor provide insights into the internal motivations of healthcare service recipients.
Regarding measuring utilization willingness for primary care services, existing research primarily focuses on residents’ willingness to sign up, renew, or pay for the services without fully capturing their overall attitude toward them. In terms of measurement methods, most studies have used a few indicators to measure willingness based on different degrees, needing more scientific rigor and standardization. There needs to be more development of measurement scales for the utilization willingness of primary care services following established psychological measurement methods and research paradigms. Consequently, empirical studies in this area have been unable to obtain practical measurement tools.
Therefore, it is crucial to delve into the conceptual meaning and structure of utilization willingness for primary care services. This exploration can shed light on the decision-making mechanisms underlying residents’ healthcare-seeking behaviors and provide practical measurement tools for empirical research on utilization willingness and behavior regarding primary care services.
Exploring the Structural Dimensions of Willingness to Utilize Family Doctor Contracting Services
Method
This study explores the structure of utilization willingness for family doctor contracting services using a grounded theory approach and statistical analysis methods and subsequently develops a measurement scale. Grounded theory involves collecting, summarizing, categorizing, analyzing, and comparing raw data and utilizing data coding techniques to extract concepts and categories that explain phenomena or issues, thereby constructing and developing theory. Research on the utilization willingness of primary care services must be context-specific. Existing literature reviews indicate that studies on residents’ utilization and willingness for primary care services are relatively limited. Grounded theory is particularly suitable for exploring specific domains where knowledge is limited or not yet fully understood, especially in observing individuals’ cognitive, behavioral, and interactive processes within specific contexts and establishing new theoretical explanations based on prior knowledge.35 Therefore, employing the grounded theory approach for conceptualizing utilization willingness for family doctor contracting services is deemed appropriate.
Sample Selection and Data Collection
This study employed a theoretical sampling method to construct the conceptual structure of utilization willingness for primary care services based on attributes and dimensions. Our criteria for selecting participants were as follows: (1) Adult community residents who themselves or their family members have a certain level of healthcare service needs, thus possessing a certain degree of understanding of medical services’ categorization and functions. (2) Wide distribution across age, gender, and other personal characteristics, with representative coverage at the regional level.
Based on the relevant literature, a preliminary interview outline was developed. Before the formal interview, two public health experts and three doctoral students were invited to participate in a focus group discussion to revise the outline. The interview questions include but are not limited to 1. Are you familiar with the community health service center and family doctor contracting services? Can you briefly describe your views? 2. How did you learn about family doctor contracting services? 3. What is your impression of the medical services provided by community health service centers? 4. Have you ever received medical treatment at a community medical institution? If so, please share your experience. 5. Are you willing to use the family doctor services to meet your medical needs?
In June 2022, we conducted in-depth interviews with 42 participants from various Chinese cities, including Beijing, Shanghai, Chongqing, Changchun, Nanjing, Changzhou, and Zhenjiang. By including participants from multiple cities, we ensured the generalizability of our study. The participants comprised 20 males and 22 females, ranging in age from 20 to 63. The interview sessions lasted for 40 to 60 minutes each. With their consent, we recorded the interviews and transcribed over 60,000 words based on the interview records.
Data Analysis Process
This study referred to the method proposed by Wan et al,36 which involved using open coding, axial coding, and selective coding procedures to analyze textual data.
Open Coding
Open coding is the first step in the grounded theory coding process, which involves exploring qualitative data obtained for conducting open-ended research. It entails defining concepts, attributes, and categories discovered through data analysis. This study used manual coding to process raw data by systematically encoding and labeling interview materials from 36 participants word by word and sentence by sentence. This process aimed to extract valuable concepts and generate initial categories by integrating elements with similar connotations. By organizing interview data, 46 initial concepts were derived, then categorized and organized into 15 initial categories following the principle of semantic similarity. The following excerpt represents a portion of the language corpus obtained through open coding, as shown in Table 1.
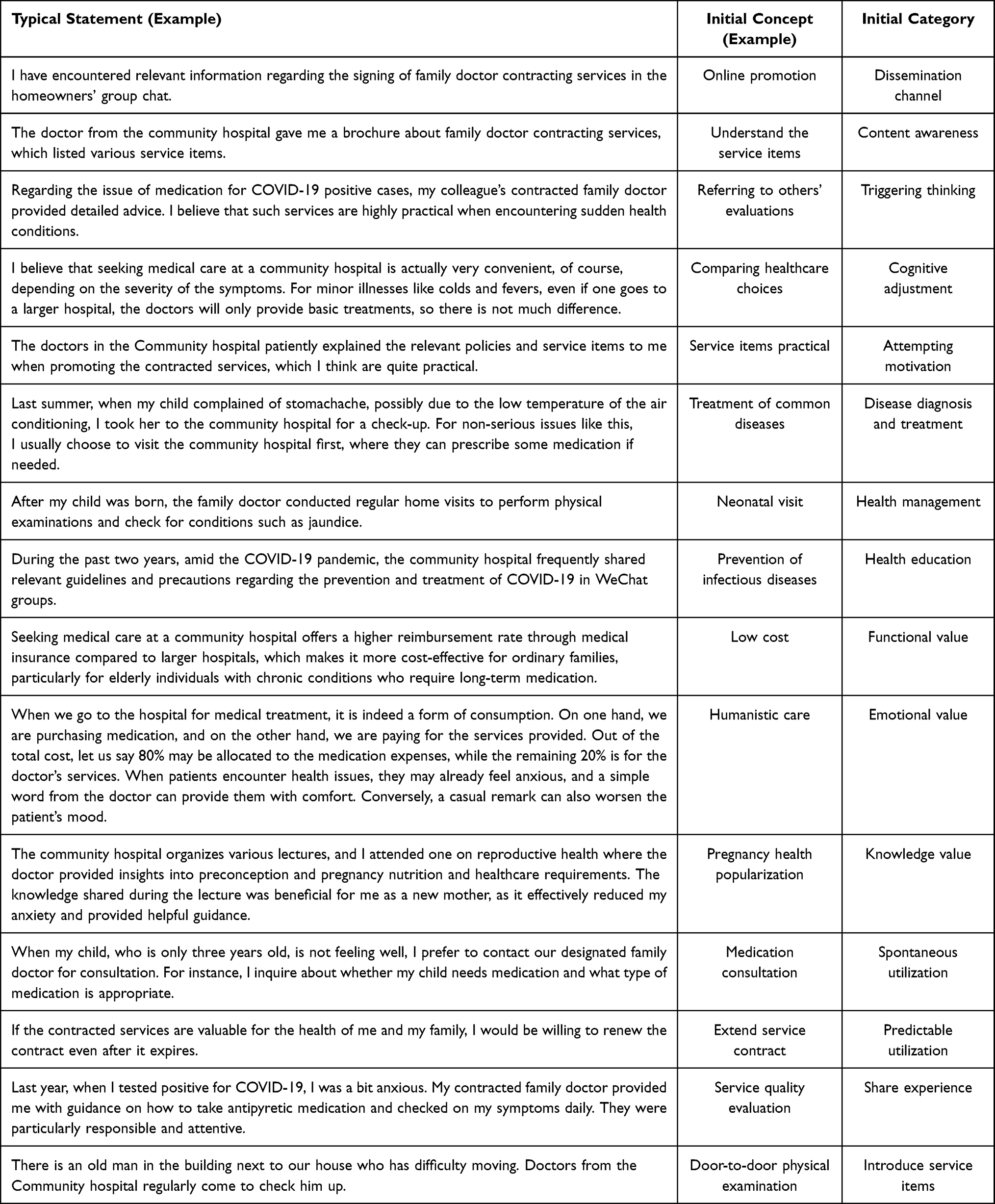 |
Table 1 The Results of Open Coding |
Axial Coding
The axial coding is the second stage of the programmatic grounded theory coding process, aimed at developing main categories and their corresponding subcategories by exploring the logical relationships between categories.37 By analyzing the inherent connections and logical sequence of different categories on a conceptual level, this study further classified and summarized 15 categories into six subcategories, namely information perception, acceptance tendency, functional perception, benefit inclination, sustained tendency, and diffusion inclination. The study further extracted three main categories by analyzing the relationships between subcategories: perceived feasibility, perceived desirability, and perceived initiative. The specific content and category connotation are shown in Table 2.
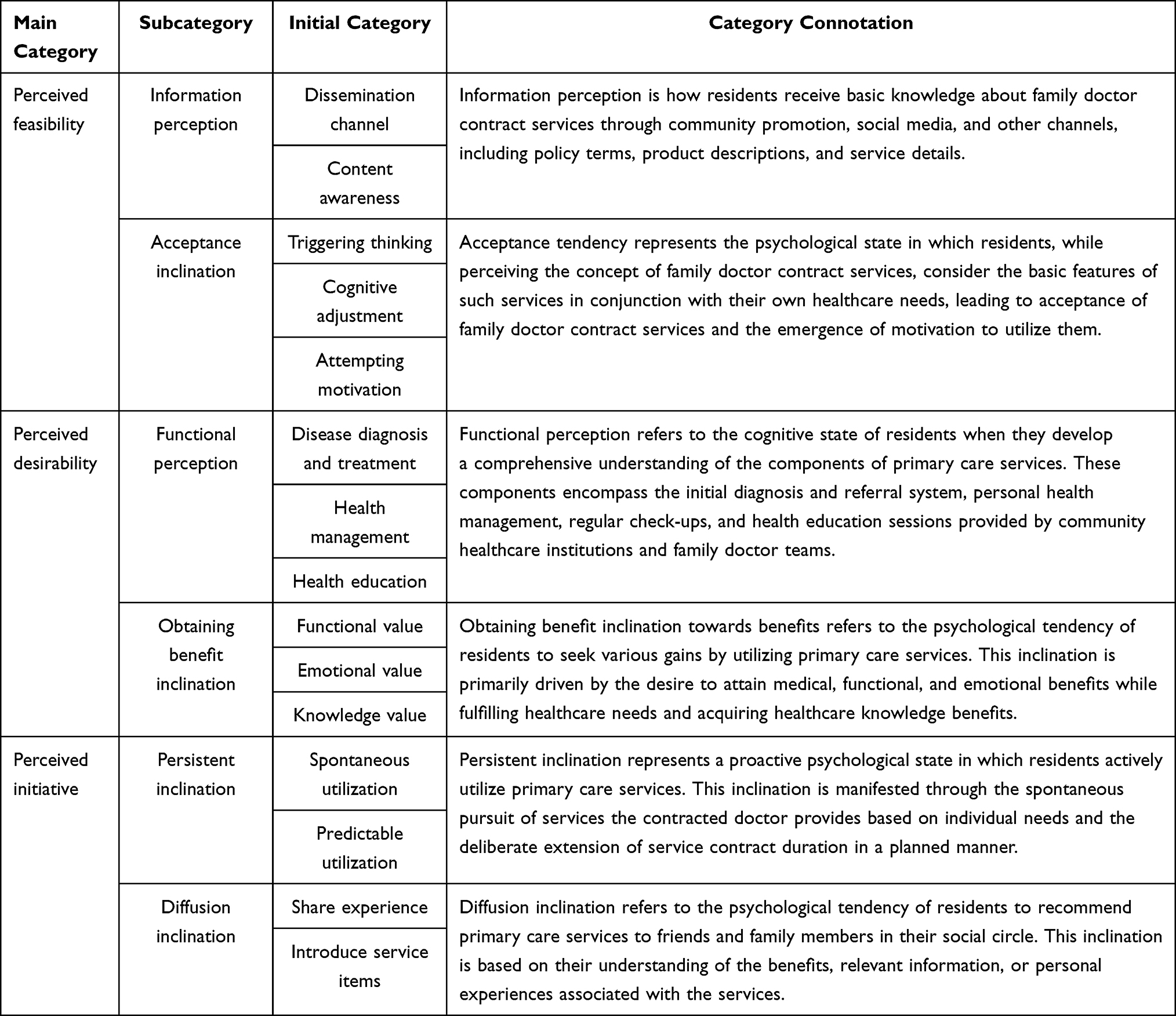 |
Table 2 The Results of Axial Coding |
Selective Coding
Selective encoding involves reintegrating the axial coding content to uncover potential associative structures among core categories, identify and distill critical categories, and develop new theoretical frameworks. In this study, the core category of “willingness to utilize family doctor contracting services” was established, with perceived feasibility, perceived desirability, and perceived initiative as the primary categories surrounding this core category. Family doctor contracting services represent primary care services in China, with community residents potentially using this service model. This study focuses on community residents’ psychological inclination from awareness to utilization of this healthcare model. The willingness to utilize primary care services among residents can be divided into three dimensions:
1. Perceived feasibility involves residents acquiring relevant information about primary care services (such as family doctor contracting services), evaluating them preliminarily, and developing motivation to try utilizing them.
2. Perceived desirability entails residents gaining a deeper understanding of the functionalities of primary care services and recognizing the benefits they can obtain from such services.
3. Perceived initiative encompasses residents’ acceptance of primary care services, willingness to utilize them long-term, and readiness to recommend them to family and friends.
Theoretical Saturation Test
After conducting a three-level coding process, we were able to establish the dimensional indicators of residents’ willingness to utilize family doctor contracting services. To ensure the reliability of our research, we subjected the remaining six resident interview data to theoretical saturation testing during the theoretical sampling process. The testing, which employed open coding, axial coding, and selective coding steps, confirmed that the conceptual indicators within each category dimension of the residents’ willingness to utilize the primary care services model were comprehensive and rich. We did not find any new primary category relationship structures beyond the three primary categories (perceived feasibility, perceived desirability, and perceived initiative), nor did we overlook any new concepts within the existing categories. The original logical relationships between the primary categories remained unchanged. Based on the results of theoretical saturation testing, we can confirm that the structural model of residents’ willingness to utilize family doctor contracting services, as constructed in this study, has achieved theoretical saturation.
Coding Results
Based on an extensive analysis of original interview data, this study employs grounded theory to construct a conceptual model for the willingness to utilize primary care services. The willingness to utilize primary care services reflects residents’ attitudes toward primary care services. Drawing from the results of the coding analysis, this study establishes three dimensions for willingness to utilize primary care services: perceived feasibility, perceived desirability, and perceived initiative. Each dimension comprises two sub-categories. A conceptual structural model for residents’ willingness to utilize primary care services is developed by clarifying the relationships between concepts, dimensions, and sub-categories, as depicted in Figure 1.
 |
Figure 1 Conceptual structure of residents’ willingness to utilize family doctor contracting services. |
Development and Testing of Family Doctor Contract Service Utilization Willingness Scale
Initial Scale Development
The previous research involved in-depth interviews with the participants to obtain raw quotes and form initial concepts. A conceptual model and dimensions were formed using programmatic grounded theory research methods. Building upon the qualitative research findings, a measurement scale for utilizing family doctor contracting services was developed by processing and organizing the initial questionnaire items.
The initial items of the measurement scale for the utilization willingness of family doctor contracting services were mainly based on references to and inspirations from the Policy Acquisition Scale, the Continuous Utilization Willingness Scale, the Product Attitude Scale, the Loyalty Willingness Scale, the Online Medical Service Usage Motivation Scale, the Patient Satisfaction Scale, and Usage Willingness Scale.38–44 While absorbing and integrating relevant theories and contents from existing literature, we extracted qualitative textual data on the conceptual connotations and categories of family doctor contracting service utilization willingness refined in this study to develop a measurement scale of 23 initial items. To ensure the scale’s content validity, we contacted four public health and general medicine research scholars. We invited them to provide feedback on the initial items of the scale. First, we sent the scale to them via email and summarized their feedback after receiving it. We then sent it to them again, and after everyone’s opinions tended to converge, we tentatively determined the content items of the scale. At the same time, according to Armitage and Conner’s views,45 self-prediction and behavioral tendency factors involved in behavioral willingness concepts can be described using expressions such as “how likely is it that”. “I want to”. “I plan to”. Based on these principles, we revised the wording of the items. We repeatedly modified and optimized their content until we reached a final measurement scale for family doctor contracting services utilization willingness.
After revising the measurement items, we conducted small-scale pilot tests and recorded feedback from community residents who met the testing conditions to ensure their acceptability. Through continuous revision and improvement, we finally determined an initial measurement scale for the utilization willingness of family doctor contracting services consisting of 16 items, as shown in Table 3.
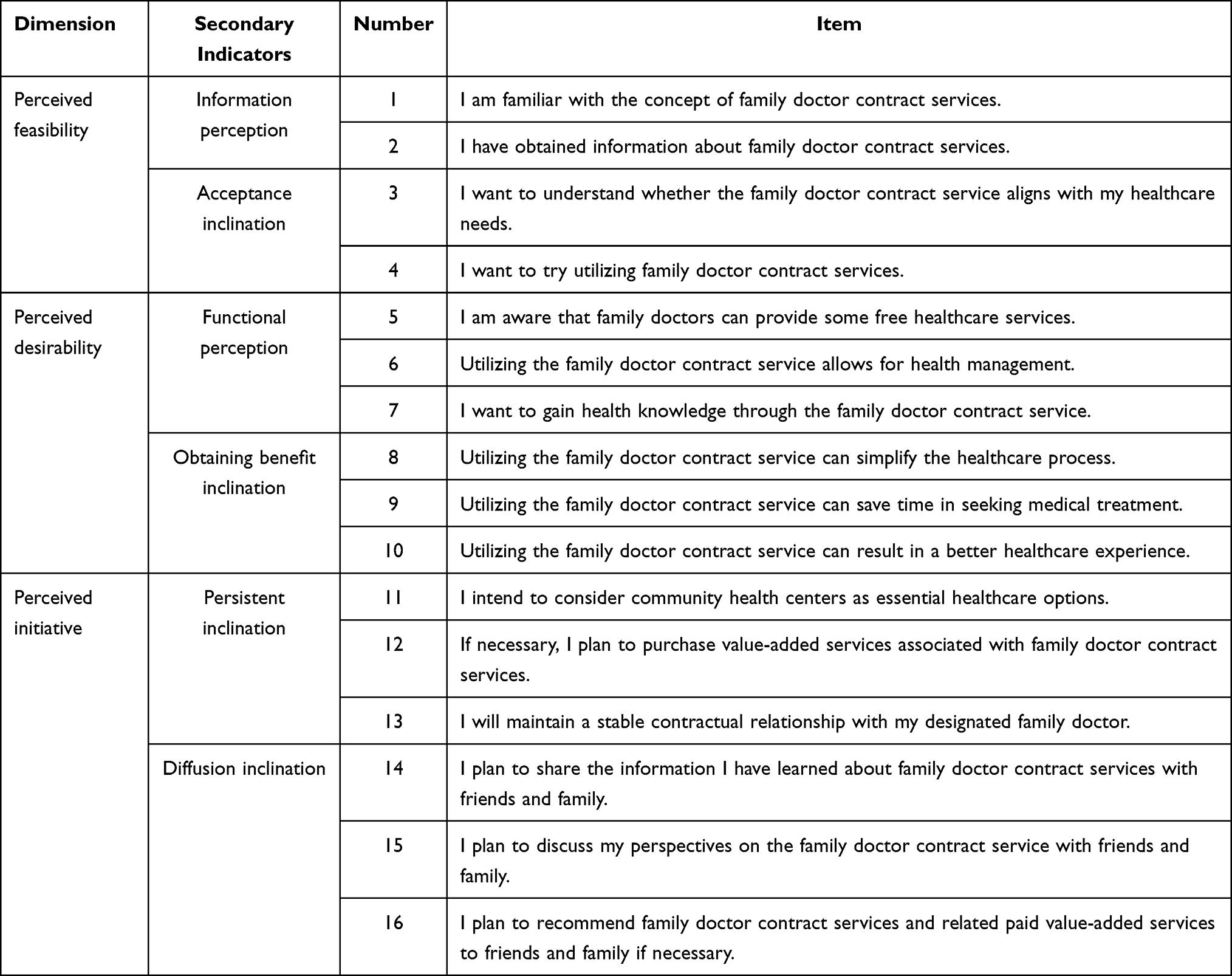 |
Table 3 Original Measurement Items of the Family Doctor Contracting Service Utilization Willingness Scale |
Scale Validity Assessment
Pilot Study and Scale Revision
Questionnaire Collection and Sample Recruitment
The pre-survey questionnaire consisted of three parts. The first part was the questionnaire instructions, briefly explaining the purpose of the survey. The second part included demographic information, such as gender, age, educational level, occupation, monthly income level, chronic health conditions, and family doctor service contract status. The third part comprised the scale of willingness to utilize primary care services, consisting of 16 items. It encompassed four items of perceived feasibility, six items of desired perception, and six items of proactive perception. The questionnaire adopted a 5-point Likert scoring method, where respondents rated their agreement level based on the descriptions provided for each item and their circumstances. The response options ranged from “strongly disagree” to “strongly agree” and were assigned scores from 1 to 5, respectively.
Given the research topic’s specificity, we targeted community residents with medical and health service needs as the survey subjects to ensure the survey results’ accuracy and validity. Therefore, the inclusion criteria for the survey subjects were community residents aged 18 years or older (registered residents or residents who have lived in the community for more than six months). In August 2022, we distributed the questionnaire online using a random sampling method. Considering the ease of use of the survey platform, we used the widely used “Wenjuanxing” platform to distribute electronic questionnaires to improve the convenience and quality of respondents’ use and completion of the questionnaire. We optimized the design of the online questionnaire according to the characteristics of mobile devices, making it easy for respondents to read and complete. We also used a reward survey method to improve respondents’ seriousness in completing the questionnaire and limited duplicate responses through IP address restrictions. Finally, 285 questionnaires were collected. After screening out invalid questionnaires with excessively short or long completion times, all items selected with the same option, or options presented in an obvious pattern, we obtained 250 valid sample data for exploratory analysis of residents’ utilization willingness of family doctor contracting services. These valid samples were from Jiangsu, Zhejiang, Shanghai, Guangdong, Beijing, Shandong, Heilongjiang, and Chongqing. The gender ratio of the sample was relatively balanced, with slightly more females than males. The age distribution was relatively balanced, with slightly more respondents aged 31–40. The educational level was evenly distributed. The monthly income level was mostly below 5000 yuan, while the distribution of chronic disease status and family doctor service contract status was balanced. Overall, the sample distribution was consistent with our research expectations.
Reliability Testing and Item Purification
Regarding the reliability and stability of measurement results, the coefficient alpha of Chronbach’s α is commonly used to assess the scale’s reliability. If Chronbach’s α coefficient is more significant than 0.7, it indicates good internal consistency among the measurement issues of the scale. The reliability of each dimension ranges from 0.783 to 0.873. Among the 16 items in the three dimensions, we retained the items with a Chronbach’s α coefficient greater than 0.6 and a CITC value not less than 0.5, based on Churchill’s criterion that the CITC value should be greater than 0.5.46 After careful consideration, we deleted items PD1 and PD4 in the hope perception dimension because their CITC values did not reach the empirical standard. Cronbach’s α coefficient improved significantly after deleting these items. We followed the principle of streamlining the scale by deleting items PD1 and PD4 to purify the test items.
Exploratory Factor Analysis
After purifying the initial scale by deleting items PD1 and PD4, we conducted exploratory factor analysis. Firstly, we conducted a suitability test for factor analysis on the sample data. When the KMO value is higher than 0.7 and Bartlett’s sphericity test reaches a significant level, the sample data is likely suitable for exploratory factor analysis. We found that the KMO value of the data was 0.938, and the χ2 value of Bartlett’s sphericity test was 2050.293 (p <0.001), which met the requirements of factor analysis. Next, we used principal component analysis to extract factors with eigenvalues greater than 1 through maximum variance orthogonal rotation. Four factors were extracted after continuous factor analysis, consistent with the three-dimensional conceptual structure of willingness to use proposed earlier. The cumulative contribution rate of the total variance was 68.734%. Each item had a factor loading greater than 0.6 on its corresponding dimension and small cross-loadings on other dimensions. The factor aggregation was consistent with grounded theory research, as shown in Table 4.
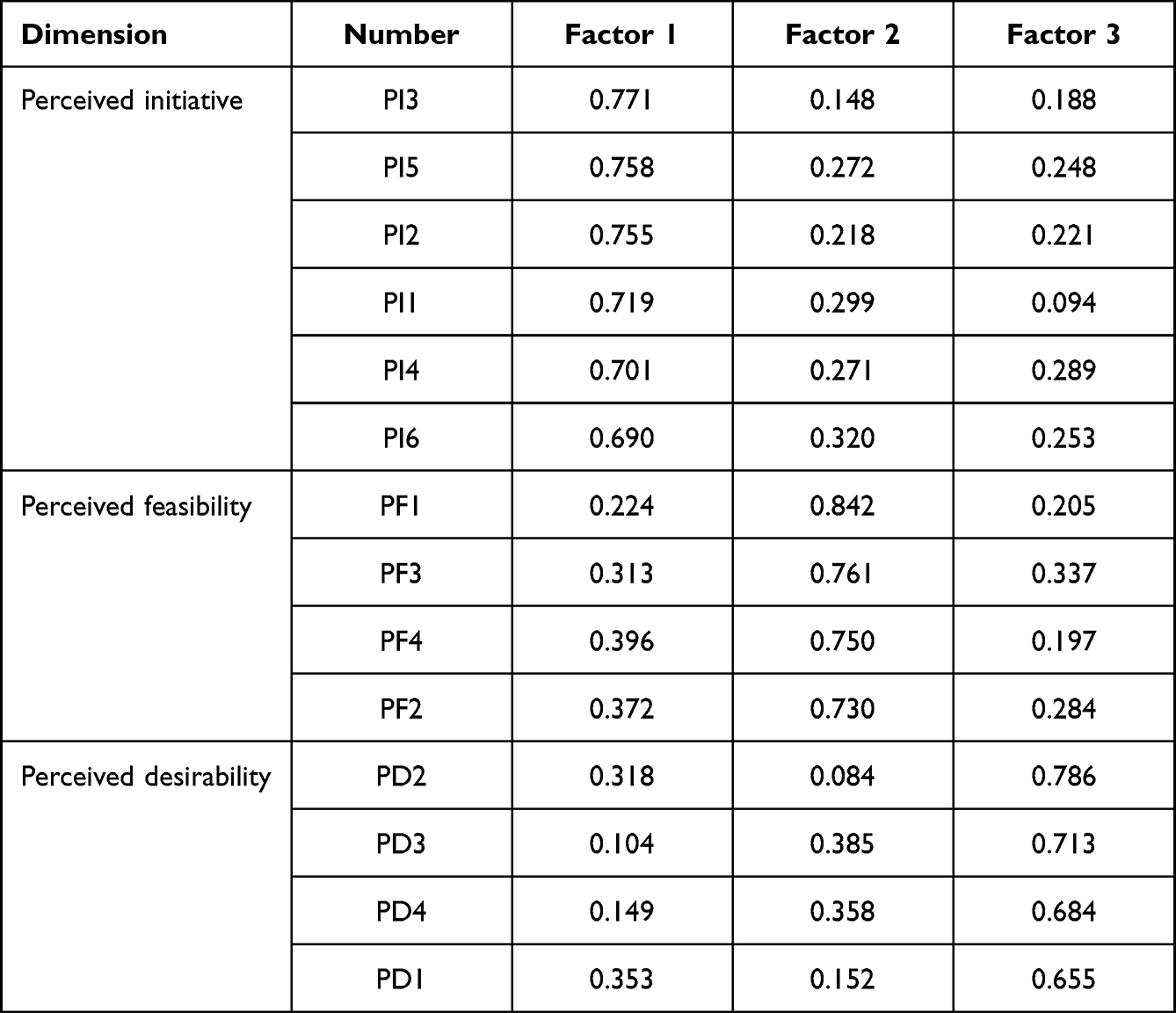 |
Table 4 The Results of Exploratory Factor Analysis |
Formal Study and Scale Testing
Questionnaire Collection and Sample Recruitment
Through item purification and exploratory factor analysis, this study identified a three-factor structure and 14 practical measurement items for willingness to utilize family doctor contracting services. The second survey was conducted to collect data for confirmatory factor analysis using a Likert scale questionnaire. The first part contained demographic information, including gender, age, education level, monthly income, chronic disease status, and family doctor service contract status. The second part consisted of measurement items for willingness to utilize family doctor contracting services, including four items for the feasibility perception dimension, four for the hope perception dimension, and six for the initiative perception dimension. The survey targeted community residents aged 18 or older (with local household registration or residence time of more than six months). In October 2022, electronic questionnaires were randomly distributed through the “Wenjuanxing” platform using a random sampling method. The design of the online questionnaire was optimized based on the characteristics of mobile devices to facilitate respondents’ reading and answering. A prize survey method was used to improve the respondents’ seriousness in answering the questionnaire. At the same time, IP address restriction was used to avoid repeated questionnaire filling. A total of 310 questionnaires were collected, and after screening out questionnaires that did not meet the survey inclusion criteria, those with excessively short or long response times, those with all items selected as the same option, and those with options showing apparent regularity, a total of 278 valid sample data were obtained for confirmatory factor analysis of residents’ willingness to use family doctor contracting services. The effective response rate was 89.7%, and the valid samples were from Jiangsu, Zhejiang, Shanghai, Guangdong, Beijing, Shandong, Jilin, Chongqing and other regions.
Confirmatory Factor Analysis
This study employed AMOS 26 to conduct confirmatory factor analysis on 278 valid samples, aiming to test the three-factor structural equation model of willingness to utilize family doctor contracting services. Single-factor, two-factor, and three-factor nested models were constructed for comparison, with the single-factor model loading all 14 items on only one common factor, the two-factor model loading all 14 items on two common factors, and the three-factor model loading all 14 items on three common factors.
As shown in Table 5, the fit indices of the single-factor and two-factor models were poor, with most indicators failing to reach empirical standards. The fit indices of the three-factor model were superior to those of other competing models. Specifically, the absolute fit index χ2/df of the three-factor model was 1.344, which was less than the empirical value of 3; the approximate error root mean square deviation RMSEA was 0.049, which was much smaller than the critical value of 0.08; the GFI was 0.940, reaching the ideal level of above 0.90; other related indices, including NFI (0.934), TLI (0.966), and CFI (0.972), were all higher than 0.90; and the PGFI was 0.663, which was greater than the standard value of 0.5, indicating good model parsimony.
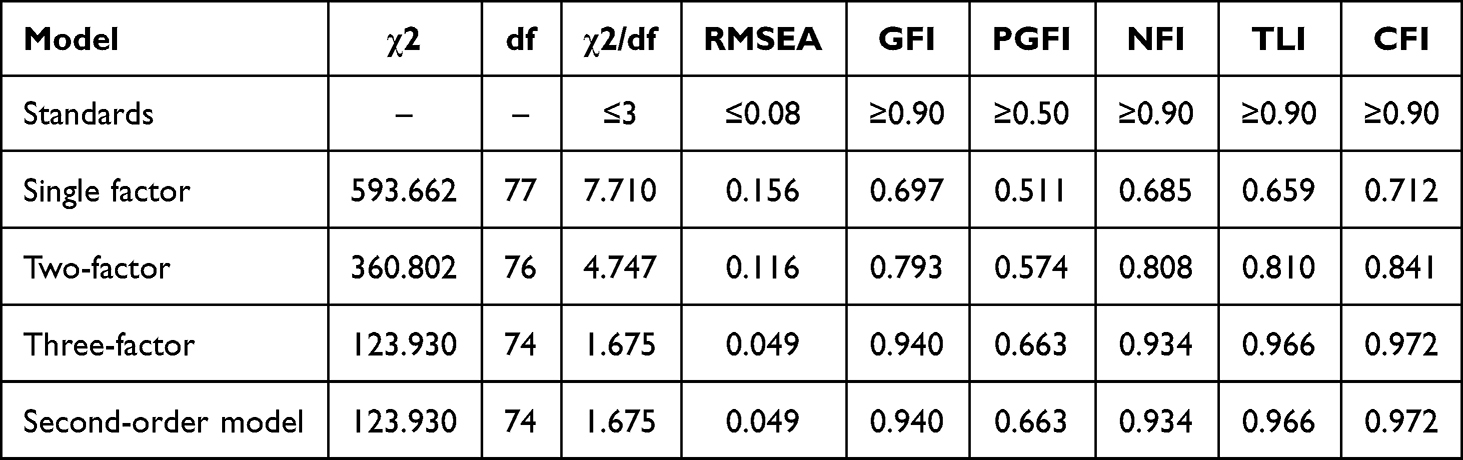 |
Table 5 The Results of the Fit Indicators for the Confirmatory Factor Analysis |
In summary, the first-order three-factor competing model of willingness to use primary medical services under contract has achieved ideal fit indices, indicating that the perceived feasibility dimension, perceived desirability dimension, and perceived initiative dimension have good discriminant validity. In the three-factor model, the standardized factor loading values of the 14 measurement items corresponding to the perceived feasibility dimension, perceived desirability dimension and perceived initiative dimension were all higher than the standard value of 0.5 (see Figure 1), indicating good convergent validity of the scale and further validating the rationality of the conceptual model.
As the correlation coefficients between the three dimensions of perceived feasibility, perceived desirability, and perceived initiative are between 0.52 and 0.63, they have a high correlation. Higher-order constructs may influence each factor when there is a high correlation between factors in a first-order confirmatory factor analysis model. Therefore, this study conducted a second-order confirmatory factor analysis on the scale. The second-order factor analysis treats the actual latent variables as measurement variables in the structural model, which can better reflect higher-level latent factors. The second-order model can test the convergent validity through the standardized path coefficients linking the second-order and first-order factors.
As shown in Table 5, the fit results of the second-order confirmatory factor model are the same as those of the first-order three-factor model, both reaching the ideal level, indicating that the two models are equivalent. The path coefficients of perceived feasibility, perceived desirability, and perceived initiative are all higher than the critical value of 0.7, indicating that willingness to use family doctor contracting services as a higher-order variable can explain these three first-order variables.
Testing Reliability and Validity
Reliability and validity tests were conducted on 278 valid samples from formal surveys to test the willingness to use the family doctor contracting services measurement scale. The Cronbach’s α coefficient was calculated for each dimension to test the reliability of the final three-dimensional model. With Cronbach’s α coefficient of 0.7 as the standard, the model is considered reliable when the measured value is higher than the standard value.
As shown in Table 6, Chronba ch’s α coefficient of the perceived feasibility dimension was 0.850, the perceived desirability dimension was 0.854, the perceived initiative dimension was 0.858, and the total Chronbach’s α coefficient of the scale was 0.898. The reliability coefficients of each dimension and the total scale were all higher than the empirical standard of 0.7, indicating that the reliability of the willingness to use the family doctor contracting services measurement scale developed in this study is promising.
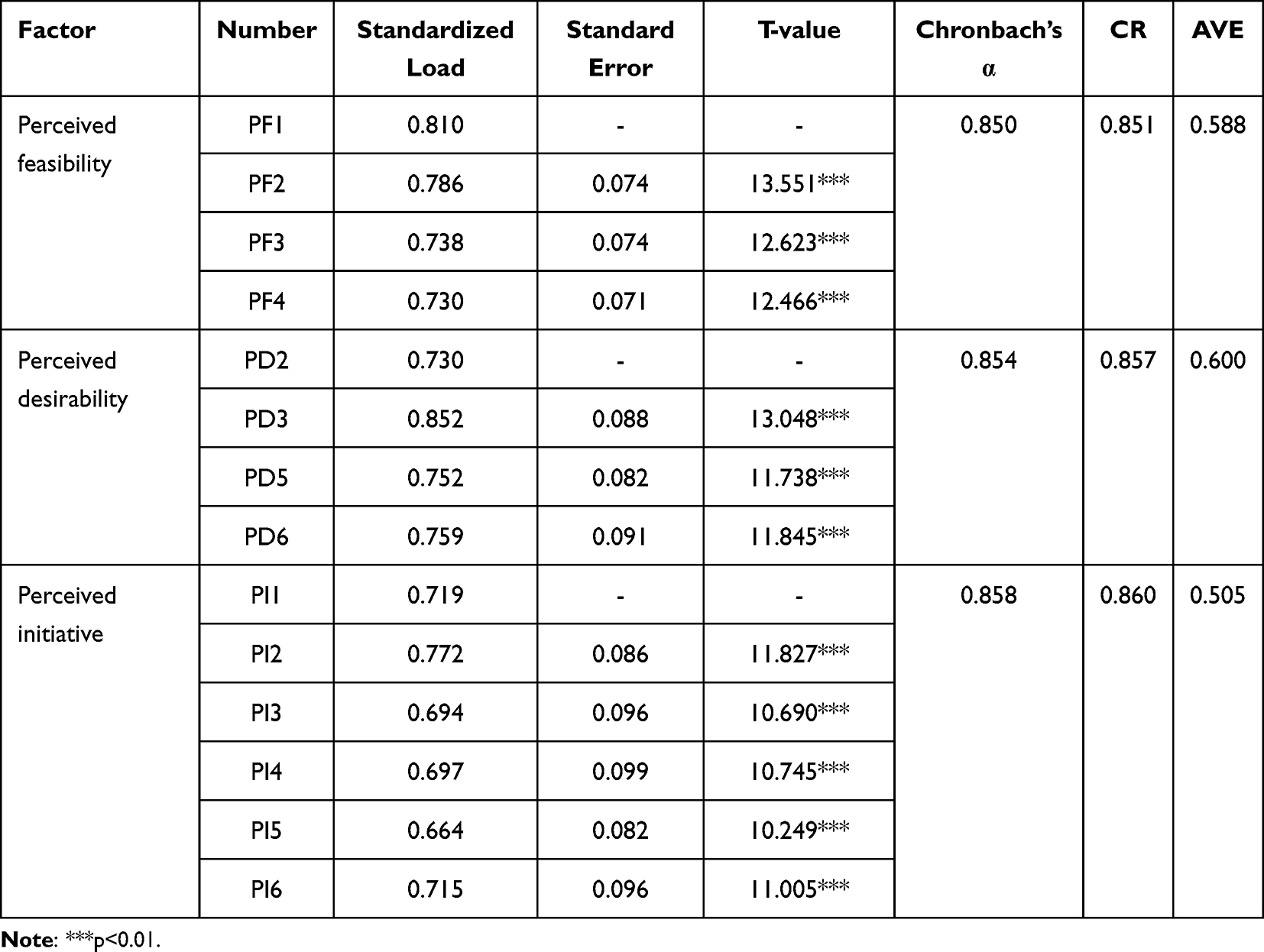 |
Table 6 The Results of Reliability and Validity Tests of Scale |
Structural validity includes convergent validity and discriminant validity. Convergent validity refers to the consistency of results obtained by measuring the same construct using different methods. It is usually measured by two indicators: average variance extracted (AVE) and composite reliability (CR). The standardized loading coefficients of the three factors and 14 items in the willingness to use family doctor contracting services measurement scale were all greater than 0.5 and reached a significant level. As shown in Table 6, the AVE value of the feasibility perception dimension was 0.588, and the CR value was 0.851; that of the hope perception dimension was 0.600, and the CR value was 0.857; that of the initiative perception dimension was 0.505, and the CR value was 0.860. The AVE values of all three dimensions exceeded the critical value of 0.5, and CR values were higher than the critical value of 0.7. In conclusion, the three-dimensional structure of willingness to use family doctor contracting services has good convergent validity.
The judgment criteria for discriminant validity mainly include whether there is a high correlation coefficient between each dimension and whether the square root value of AVE is greater than the utterly standardized correlation coefficient between dimensions. If the former is less, it indicates sufficient discriminant validity between dimensions. The correlation coefficients between the three dimensions of perceived feasibility, perceived desirability, and perceived initiative in willingness to use family doctor contracting services was 0.627, 0.522, and 0.580, respectively, all less than the empirical standard of 0.85, indicating that there was no severe multicollinearity between dimensions. Meanwhile, the square root values of AVE for perceived feasibility, perceived desirability, and perceived initiative were 0.767, 0.775, and 0.711, respectively, all higher than the correlation coefficients between dimensions. Therefore, the three-dimensional structure of willingness to use family doctor contracting services has good discriminant validity.
Discussion
Theoretical Implications
Firstly, through in-depth interviews, this study explored the connotation of willingness to use family doctor contracting services and constructed a conceptual model using the programmatic grounded theory method, making a significant theoretical contribution. In previous studies, scholars focused on service demanders’ acceptance or willingness to pay for a single medical service project when studying medical service demand, medical behavior, and willingness to use primary medical services. They generally used simple standards such as willing or unwilling for measurement,29 ignoring the process and internal structure of willingness to use medical services. In many countries, the hierarchical diagnosis and treatment system operates orderly under policy guarantees. Researchers are not concerned about the willingness to use primary medical services but rather about decision-making issues facing multiple types of primary care service providers.47 The willingness to use concept model constructed in this study explains the internal structure of service demanders’ willingness to use specific medical service products in a relatively free medical environment, improves the theoretical framework of medical service utilization and utilization behavior, helps to expand the research scope of willingness to use medical services, and lays a foundation for research on primary medical service utilization behavior.
Secondly, this study developed a measurement scale for willingness to use family doctor contracting services following scientific procedures. This scale is applicable to urban community residents who have access to family doctor services or similar primary healthcare services. Previous medical service willingness measurement tools emphasized the results of willingness.25,48 However, the scale developed in this study focuses on how the service demander’s willingness to use is generated and reinforced and constructs three dimensions of willingness, providing a more in-depth and comprehensive interpretation of willingness. Based on this, a family doctor contracting services utilization willingness scale was compiled, which can effectively measure the service demander’s willingness to use medical services. Furthermore, it can be utilized as a measurement tool in empirical research on healthcare services in the future. Overall, this study has made a significant theoretical contribution.
Practical Implications
In a healthcare environment where the hierarchical referral system still needs to be well-established, the utilization willingness of residents towards primary care services serves as a prerequisite for actual utilization behavior. The poor utilization behavior of primary care services signifies a lack of motivation among residents, possibly due to the mismatch between primary care services and residents’ needs. Therefore, accurately grasping the connotation of residents’ utilization willingness and providing primary care services that align with their healthcare needs are essential pathways to promote the utilization behavior of primary care services.
At the same time, even in countries where the hierarchical referral system operates smoothly, it does not guarantee that residents are delighted with primary care services. There is always room for optimizing the efficiency and quality of primary care services. The utilization willingness of residents undoubtedly serves as an essential reference for primary care service providers to improve service quality and enhance competitiveness.
Limitations and Future Research Directions
The conceptual model for the willingness to utilize family doctor contracting services developed in this study is based on research conducted within the context of China’s primary healthcare system. Therefore, at present, this model can only represent the utilization willingness of Chinese residents toward primary care services. When applying the measurement scale developed based on this model to residents in other countries or in underdeveloped regions with primary healthcare services, limitations may arise.
Due to workforce, time, and resource limitations, most of this study’s interviewees and survey respondents were urban residents. They did not cover remote provinces, cities, and rural areas where residents may have unique medical habits due to objective conditions. In future research, the scope of the investigation can be expanded to improve the universality of the research. This study has contributed to the willingness to use primary medical services. However, there is still much work to be done in understanding the complexity of this structure and its influencing factors. In future research, the goal should be to enhance understanding of residents’ utilization willingness, optimize the primary medical service system, and support residents to use medical resources more efficiently.
Ethics Statement
We declare that all participants in this study volunteered to participate and were free to withdraw at any time. In conducting this research, we adhered to the Helsinki Declaration, ensuring that all participants remained anonymous and their privacy was protected. The Institutional Review Board at Jiangsu University approved all aspects of this study.
Funding
This work was funded by the National Natural Science Foundation of China (71974082).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu Y, Kong Q, Yuan S, van de Klundert J, Ciccozzi M. Factors influencing choice of health system access level in China: a systematic review. PLoS One. 2018;13(8):e0201887. doi:10.1371/journal.pone.0201887
2. Notice on Issuing the Guiding Opinions on Promoting Family Doctor Contract Services. Available from: http://www.gov.cn/gongbao/content/2016/content_5124373.htm.
3. Zhang Y, Su T, Chai Q, et al. Analysis of the status quo of policies on contracted family doctor services in Taiyuan based on in-depth interview. Chin General Pract. 2020;23(4):468–472. doi:10.12114/j.issn.1007-9572.2020.00.053
4. National Medical Service Status from January to November; 2022. Available from: http://www.nhc.gov.cn/mohwsbwstjxxzx/s7967/202304/60a495626bec4ec58cd7467b4f6d4eab.shtml.
5. Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: an Introduction to Theory and Research. Philosop Rhetoric. 1977;10(2):130–132.
6. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
7. Fishbein M, Ajzen I. Theory-based behavior change interventions: comments on Hobbis and Sutton. J Health Psychol. 2005;10(1):
8. Eagly A, Chaiken S. The Advantages of an Inclusive Definition of Attitude. Soc Cogn. 2007;25(5):582–602. doi:10.1521/soco.2007.25.5.582
9. Bell DR, Bucklin RE. The Role of Internal Reference Points in the Category Purchase Decision. J Consumer Res. 1999;26(2):128–143. doi:10.1086/209555
10. Fishbein M, Manrfedo MJ. A theory of behavior change in influencing human behavior: theory and application in recreation. Tour Nature Resources Manag. 1992;11:29–50.
11. Yang K, Li Y, Qi H. Determinants of and Willingness to Use and Pay for Digital Health Technologies Among the Urban Elderly in Hangzhou, China. RMHP. 2023;16:463–478. doi:10.2147/RMHP.S393767
12. Saadatfar N, Jadidfard MP. An overview of the methodological aspects and policy implications of willingness-to-pay studies in oral health: a scoping review of existing literature. BMC Oral Health. 2020;20(1):323. doi:10.1186/s12903-020-01303-3
13. Mussio I, Brandt S, Hanemann M. Parental beliefs and willingness to pay for reduction in their child’s asthma symptoms: a joint estimation approach. Health Econ. 2021;30 Suppl 1(Suppl 1):30. doi:10.1002/hec.4181
14. Contoli B, Minardi V, Possenti V, Lana S, Luzi P, Masocco M. The willingness to be vaccinated against SARS-CoV-2 in the Italian population. Eur J Public Health. 2021;31(Supplement_3):
15. Yu X, Bao H, Shi J, et al. Preferences for healthcare services among hypertension patients in China: a discrete choice experiment. BMJ Open. 2021;11(12):e053270. doi:10.1136/bmjopen-2021-053270
16. Wen T, Chen M, Du Q. Investigation on township residents’ cognition and demand to family doctor’ s contract service in Foshan City. Med Soc. 2019;32(1):93–95, 112. doi:10.13723/j.yxysh.2019.01.022
17. Qiu B, Huang J, Liang M, et al. A comparative study on the health services utilization and satisfaction of the family doctor service. Chin J Health Policy. 2016;9(8):31–36. doi:10.3969/j.issn.1674-2982.2016.08.006
18. Hu C, Huang X. Analysis of the awareness and utilization of family doctor service among elderly people in N city. J Nanjing Med Univ. 2019;19(5):384–387. doi:10.7655/NYDXBSS20190510
19. Sun J, Zhao Y, Jia C, Zhang C, Liu R, Peng M. Study on the status and service utilization of family doctors in a community in Beijing city. Chin Hosp Manage. 2019;39(7):74–75.
20. Chen Y, Jiang P, Liu S, Liang L, Zhao J. Study on the willingness and influencing factors of patients on primary treatment. Health Econom Res. 2021;38(9):13–17. doi:10.14055/j.cnki.33-1056/f.2021.09.003
21. Zhao X, Xiao J, Chen H, et al. Patient preferences and attitudes towards first choice medical services in Shenzhen, China: a cross-sectional study. BMJ Open. 2022;12(5):e057280. doi:10.1136/bmjopen-2021-057280
22. Hu X, Hou L, Zhou C, et al. Research on policy awareness and service utilization of family doctor contract services—based on a survey of residents in Hangzhou. Health Econom Res. 2020;37(1):52–55. doi:10.14055/j.cnki.33-1056/f.2020.01.016
23. Liu Z, Tan Y, Liang H, et al. Factors influencing residents’ willingness to contract with general practitioners in Guangzhou, China, during the GP policy trial phase: a cross-sectional study based on Andersen’s behavioral model of health services use. INQUIRY. 2019;56:004695801984548. doi:10.1177/0046958019845484
24. Liu J, Qiao Y, Gan Y, et al. Evaluation of family doctor services and intention of renewing the contract with the family doctor among contracted residents in Shenzhen. Chin General Pract. 2020;23(1):
25. Wang C, Yan S, Jiang H, et al. Residents’ Willingness to Maintain Contracts with Family Doctors: a Cross-sectional Study in China. J GEN INTERN MED. 2021;36(3):622–631. doi:10.1007/s11606-020-06306-y
26. Li W, Li J, Fu P, et al. Family characteristics associated with rural households’ willingness to renew the family doctor contract services: a cross-sectional study in Shandong, China. BMC Public Health. 2021;21(1):1282. doi:10.1186/s12889-021-11048-5
27. Zeithaml VA. Consumer Perceptions of Price, Quality, and Value: a Means-End Model and Synthesis of Evidence. J Mark. 1988;52(3):2–22. doi:10.1177/002224298805200302
28. Gümüş R. Role of Marketing Mix Perception and Participation on Repurchase Intention of Health Consumers. J Health Manag. 2022;24(4):525–538. doi:10.1177/09720634221128395
29. Pan Y, Qu H. Influence of cross-border e-commerce web quality on clothing purchase intention. J Donghua Univ. 2019;45(1):128–134. doi:10.3969/j.issn.1671-0444.2019.01.020
30. Wang Y, Wang W, Liu Z. An empirical study on the influence of online negative reviews on potential consumers’ purchasing intention. Inform Sci. 2018;36(10):156–163. doi:10.13833/j.issn.1007-7634.2018.10.028
31. Zhao Y, Yao X, Leng W, Lv C. Analysis on influencing factors of community health services utilization willingness of the residents in Karamay city, Xinjiang. Med Soc. 2016;29(6):39–41, 47. doi:10.13723/j.yxysh.2016.06.012
32. Alsulaiman JW, Mazin M, Al-Shatanawi TN, Kheirallah KA, Allouh MZ. Parental Willingness to Vaccinate Their Children Against SARS-CoV-2 in Jordan: an Explanatory Cross-Sectional Study. RMHP. 2022;15:955–967. doi:10.2147/RMHP.S360838
33. Wang L, Ge M, Jiang P, et al. Community residents’ awareness and willingness towards contractual services from family doctors. Chin General Pract. 2018;21(4):401–406. doi:10.3969/j.issn.1007-9572.2018.04.006
34. Xu L, Wang Y, Zhang Y, et al. Survey on the willingness to sign a contract of family physician service and its influencing factors among university community residents. Health Med Res Pract. 2018;15(1):45–48. doi:10.11986/j.issn.1673-873X.2018.01.008
35. Charmaz K, Thornberg R. The pursuit of quality in grounded theory. Qual Res Psychol. 2021;18(3):305–327. doi:10.1080/14780887.2020.1780357
36. Wan W, Song X, Zhao Y, Zhu Q. A Probe into the Influencing Factors of Online Health Information Substituting Search Behavior: based on Grounded Theory. Inform Document Serv. 2020;41(6):88–94.
37. Zhou Q, Wu T, Yang W, et al. Research on mode of enterprise technical standards alliance for the “Belt and Road” initiative based on proceduralised grounded theory. Manage Rev. 2021;2:108–119. doi:10.14120/j.cnki.cn11-5057/f.2023.05.014
38. Chen L, Jin M. Research on the relationship between policy marketing, individual willingness to acquire policy and evaluation of policy effectiveness—mediating effect based on policy awareness. Chin Public Admin. 2020;2:117–122. doi:10.19735/j.issn.1006-0863.2020.02.15
39. Bhattacherjee A. Understanding Information Systems Continuance: an Expectation-Confirmation Model. MIS Quart. 2001;25(3):351–370. doi:10.2307/3250921
40. Wang X, Yu C, Wei Y. Social Media Peer Communication and Impacts on Purchase Intentions: a Consumer Socialization Framework. J Interact Market. 2012;26(4):198–208. doi:10.1016/j.intmar.2011.11.004
41. Johnson MD, Herrmann A, Huber F. The Evolution of Loyalty Intentions. J Mark. 2006;70(2):122–132. doi:10.1509/jmkg.70.2.122
42. Zhang C, Li Z, Peng X, You H. Study on the formation mechanism of community patients’ willingness to use online medical services. Chin Health Resources. 2022;25(1):106–113. doi:10.13688/j.cnki.chr.2022.210262
43. Lam CLK, Yu EYT, Lo YYC, et al. Having a Family Doctor is Associated with Some Better Patient-Reported Outcomes of Primary Care Consultations. Front Med. 2014:1. doi:10.3389/fmed.2014.00029
44. Taylor S, Todd PA. Understanding Information Technology Usage: a Test of Competing Models. Inform Syst Res. 1995;5:91–108.
45. Armitage CJ, Conner M. Efficacy of the Theory of Planned Behaviour: a meta-analytic review. Br J Soc Psychol. 2001;40(Pt 4):471–499. doi:10.1348/014466601164939
46. Churchill G. A Paradigm for Developing Better Measures of Marketing Constructs. J Market Stud. 1979;16:12–27. doi:10.1177/002224377901600110
47. Gabrani J, Schindler C, Wyss K. Factors associated with the utilisation of primary care services: a cross-sectional study in public and private facilities in Albania. BMJ Open. 2020;10(12):e040398. doi:10.1136/bmjopen-2020-040398
48. Li X, Zhang L, Li Z, Tang W. Patient Choice and Willingness Toward Gatekeepers as First-Contact Medical Institutions in Chinese Tiered Healthcare Delivery System: a Cross-Sectional Study. Front Public Health. 2021;9:665282. doi:10.3389/fpubh.2021.665282
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Concept Construction and Scale Development of Employee Zhengchong Behaviour in Family Firms in Jiangsu Province of China
Ma Z, Fan M, Ouyang C, Su J, Wu M
Psychology Research and Behavior Management 2022, 15:2717-2734
Published Date: 22 September 2022
Research on Employee Voice Intention: Conceptualization, Scale Development, and Validation Among Enterprises in China
Ouyang C, Ma Z, Ma Z, Su J
Psychology Research and Behavior Management 2023, 16:2137-2156
Published Date: 12 June 2023