Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Constructing a Management Evaluation Index System Based on Hierarchical Analysis in the Interventional Therapy of Hematological Surgery in Hospitals
Authors Fu L, Wang Y, Gao Z, Zhao W, Wang M, Yu H
Received 17 May 2025
Accepted for publication 27 August 2025
Published 18 September 2025 Volume 2025:18 Pages 5935—5947
DOI https://doi.org/10.2147/JMDH.S541171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Lingxue Fu, Yiying Wang, Zimian Gao, Weiwei Zhao, Miaomiao Wang, Huiqian Yu
Department of Vascular Surgery, The Second Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, 325000, People’s Republic of China
Correspondence: Huiqian Yu, Email [email protected]
Purpose: To construct a set of comprehensive, practical, scientific and reasonable management evaluation index system to provide strong theoretical support and practical guidance for improving the management level of interventional therapy of hematology surgery in hospitals.
Methods: A research team was set up at an early stage and a large amount of literature was consulted to construct a preliminary evaluation index system for the management of interventional therapy in the Department of Hematologic Surgery, which was modified and improved with two rounds of Delphi expert correspondence; at the same time, the weighting of the index system was analyzed by using the hierarchical analysis method. The reliability of the questionnaire was evaluated by using the Cronbach’s alpha coefficient, a measure of correlation and internal consistency, on 100 patients receiving interventional therapy.
Results: The final evaluation index system of interventional therapy management in hematologic surgery includes 5 first-level indexes, 18 second-level indexes, and 41 third-level indexes; the Cronbach’s α of all the first-level indexes is > 0.7.
Conclusion: The scientific, reliable, and practicality of the index system of interventional therapy management in hematologic surgery is high, and it provides a relevant basis for the continuous improvement of interventional therapy in hematologic surgery in the future. It provides a relevant basis for the continuous improvement of hematology surgery interventional therapy in the future.
Keywords: hierarchical analysis, hematologic surgery, interventional therapy, indicator construction
Introduction
Interventional therapy is a minimally invasive and highly effective therapeutic means, which is increasingly widely used in the clinical treatment of various blood diseases.1 It has brought new hope to many patients by virtue of its precise localization, small trauma, and relatively short recovery period, significantly improving patients’ quality of life and increasing the survival rate.2 However, the complexity of interventional therapy and the high demands on the professional competence of the medical team, equipment resources, and management of the treatment process make it a key challenge for hospitals to ensure the safety and effectiveness of the treatment process and to improve the overall management level.3
Evaluating the management quality of interventional therapy scientifically and reasonably can help identify potential risks in the treatment process, optimize the allocation of resources, improve the efficiency of medical staff, and enhance the hospital’s ability to serve patients.4 At present, the evaluation system for interventional treatment management in hematology surgery often focuses on a single dimension and lacks integrated evaluation of medical resource utilization and team collaboration; Part of the system relies on subjective scoring, with insufficient quantification.5–7 Although hospitals are investing more and more in the hardware facilities and technical applications of interventional therapy, there are still many deficiencies in the construction of the management evaluation system, and there is a lack of a comprehensive, systematic, and targeted evaluation index system to accurately measure the effectiveness of management. As a multi-criteria decision-making method that combines qualitative and quantitative analysis, the Analytic Hierarchy Process (AHP) is able to effectively deal with the judgment of the relative importance of factors in complex problems.8 By constructing a hierarchical model, a complex management problem is decomposed into constituent factors at different levels, and the weights of the factors are determined by two-by-two comparison, thus providing a scientific basis for decision-making.9
In view of this, this study aims to use hierarchical analysis to deeply analyze the key links in the management of interventional therapy of hematology surgery in hospitals, and to construct a set of comprehensive, practical and scientifically reasonable management evaluation index system, with a view to providing strong theoretical support and practical guidance for improving the management level of interventional therapy of hematology surgery in hospitals.
Methods and Data
Establishment of the Research Team
The survey invited 18 experts in related disciplines to construct the indicators, including 4 hematological surgeons, 4 surgeons, 8 experts in nursing management, and 2 postgraduate students in hematological surgery. The average working experience of the experts was 13.15±6.12 years. In the initial stage, the research team participated in the formulation of the management evaluation index system in hematologic surgical interventions in combination with clinical experience, and mainly referred to the Proposed diagnostic criteria for classical chronic myelomonocytic leukemia (CMML), CMML variants and pre-CMML conditions.,10 “Leukopenie - ein diagnostischer Leitfaden für die Praxis [Leukopenia - A Diagnostic Guideline for the Clinical Routine]”,11 “Practical approach to the management of catheter-related bloodstream infection”,12 and “Interventional Radiology. Indications and Best Practices”13 to refine and score the index system. Meanwhile, at the reference and scoring stage, suggestions can be provided for changing the elements to further improve the whole index system.
Literature Search Strategy
Computerized searches of PubMed, Web of Science, the Cochrane, Library, EMbase, China Knowledge Network, Wanfang Database, China Biomedical Literature Database and guidelines websites such as Medical Pulse, National Institute for Health and Care Excellence (NICE), the Guidelines International Network (GIN) and other guideline websites. The search terms were: Hematologic Surgery/Hematologic/Interventional Therapy/Evaluation/Systems/Evaluation/Systems Vascular Interventions/Non-Vascular Interventions/Management/Hospital Management. A literature search was conducted using a combination of subject terms and free words with a timeframe of building the library until April 8, 2025. The research team used the retrieved literature to initially formulate a system of indicators for evaluating management in hematologic surgical interventions.
Expert Correspondence
The extracted indicators were summarized and organized, and a preliminary system of management evaluation indicators in hematological surgery interventions was formulated, and an expert correspondence questionnaire was developed. The questionnaire consists of three parts: 1) a preamble; 2) a questionnaire for experts to assess the necessity, importance, achievability, and comprehensibility of each element of the survey using the Linkert 5-point scale (1=strongly disagree, 2=disagree, 3=undecided, 4=agree, and 5=strongly agree); and 3) a questionnaire on the situation of the experts. Purposive sampling method was used to select correspondence experts nationwide. Inclusion criteria for correspondence experts: undergraduate education or above; intermediate or above title; more than 10 years of experience in surgery in a tertiary hospital; more than 3 years of experience in direct care or management of hematological surgery patients; voluntary participation in the study, and the ability to complete the correspondence questionnaire within a specified period of time. The experts were invited by telephone before the questionnaire was distributed, and after the experts agreed, the researcher sent the questionnaire by e-mail. After each round of correspondence, the researcher conducted statistics and discussions on the results of the correspondence, using the mean value ≥ 4.0 points and coefficient of variation (CV) and lt; 0.25 as the criteria for the screening of indicators, and then the research team focused on the discussion of expert opinions after the collation of experts’ opinions, and the correspondence was terminated when the experts’ opinions were basically the same. A total of 2 rounds of expert correspondence were conducted in this study.
Study Subjects
Convenience sampling method was used to investigate 100 patients who received interventional therapy from April 2024 to April 2025 in the Department of Hematological Surgery of the Second Affiliated Hospital of Wenzhou Medical University. The data collection stage adopts a single blind method: the evaluator is unaware of the patient’s clinical information and only scores based on objective indicators; During the expert consultation stage, anonymous scoring of indicator weights is used to avoid group bias. This study has been reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (Wenzhou, Zhejiang Province, China), Patients or family members were informed and agreed.(Approval No.:).
Inclusion criteria: (1) reference to the literature “The main progresses and hot spots of hematological diseases in the past decade”14 patients were diagnosed with blood diseases by clinical symptoms, laboratory tests and imaging examinations; (2) according to the patient’s condition, it was clearly required to receive interventional therapy by the hematological surgery department and related departments. (2) According to the patient’s condition, after consultation and evaluation by experts from the Department of Hematology and related departments, it is clear that the patient needs to receive interventional therapy as the main treatment or part of the comprehensive treatment; (3) It is the first time to receive interventional therapy of hematological surgery, and has not received similar interventional therapy programs for this disease; (4) The patient and his/her family members have signed an informed consent form. Exclusion criteria: (1) the existence of vital organ function problems; (2) the combination of psychiatric diseases; (3) communication barriers, unable to understand the meaning of the indicators. The patients and their families were aware of and agreed to the general information in Table 1.
 |
Table 1 General Information |
Statistical Methods
SPSS 27.0 and R4.4.2 were used for data processing. The coefficient of variation (CV) and Kendall’s coefficient of concordance (KW) were used to measure the level of agreement between expert opinions. The coefficient of expert authority (Cr) was calculated as the average of the coefficient of judgmental basis (Ca) and the coefficient of familiarity (Cs), and a hierarchical analysis was performed using the R language psych package; the Cronbach’s alpha coefficient was used to evaluate the credibility of the indicator system. Counts were expressed by their frequencies and percentages, while quantitative data were expressed by mean ± standard deviation, with P < 0.05 indicating significant differences.
Results
Results of Expert Correspondence
A total of 28 experts, aged 35.34 ± 6.78 years, with 10.65 ± 6.76 years of working experience, from 19 tertiary hospitals and above across China were included in this study. Among them, 8 were doctoral students, 14 were master’s students, and 6 were undergraduates. 31 questionnaires were distributed in both rounds of correspondence, and 28 valid questionnaires were recovered, with the effective recovery rate of both questionnaires being 90.32%. In the first round of correspondence, 15 experts (53.57%) put forward modification opinions, and in the second round of correspondence, 5 experts (17.86%) put forward modification opinions, which shows that the degree of authority of the experts is high. The coefficient of authority of experts in the first round of correspondence is 0.8289, and the coefficient of authority of experts in the second round of correspondence is 0.9039, so the results are credible. Meanwhile, the Kendall’s coefficient of the first round is 0.560, and the Kendall’s coefficient of the second round is 0.536, with P<0.001, the Kendall’s harmonization coefficient is good, and the credibility is high.
Experts’ Modification Opinions
Results of the first round of expert consultation: After the first round of expert consultation, 15 experts proposed modification opinions, and after discussion by the research group, the third-level indicator “Comparison of the cure rate with the average level of the same industry in China” was added to the second-level indicator “Cure rate”. The secondary indicator “recurrence rate” is subdivided into “short-term recurrence rate”, “medium-term recurrence rate” and “long-term recurrence rate”. The secondary indicator “recurrence rate” is subdivided into “short-term recurrence rate”, “medium-term recurrence rate”, and “long-term recurrence rate”; the secondary indicator “stock turnover of medicines” is added under the primary indicator “medical resources”, and subdivided into the tertiary indicators “commonly used” and “high-value”. “High-value”. Results of the second round of expert consultation: After the second round of expert consultation, a total of 5 experts proposed modifications. Based on the experts’ opinions and group discussions, the indicators were modified as follows: “Incidence of postoperative infections” was modified to “Incidence of interventional infections”.
Constructing the Indicator System
The final indicator system includes 5 first-level indicators, 18 second-level indicators and 41 third-level indicators for the evaluation of the management of interventional therapy in hematological surgery, and the distribution and weights of the specific indicators are shown in Table 2.
 |
Table 2 Evaluation Index System for Management of Haematological Surgical Interventions |
Importance Scores
The importance scores and coefficients of variation of the evaluation system of haematological surgical interventional therapy management are shown in Table 3.
 |
Table 3 Importance Score of the Evaluation System of Haematological Surgical Intervention Management |
Correlation Analysis
The management evaluation index system in haematological surgical interventions was implemented in 100 patients and the correlation of patient scores is shown in Figure 1.
 |
Figure 1 Heat map of correlation between patient scores in the management evaluation index system of hematological surgical interventional therapy. The x-axis is labeled “Evaluation Indicators”, the y-axis is labeled “Correlation Coefficient”, specifying that “Red gradient indicates positive correlation (0 to 1), and blue gradient indicates negative correlation (−1 to 0)”. |
Reliability Analysis
The Cronbach’α coefficient was used to indicate the reliability of the index system of patients’ evaluation of management in haematological surgical interventions, and the Cronbach’α of all the level 1 indexes were > 0.7, indicating that the index system had high reliability (P < 0.05), see Table 4.
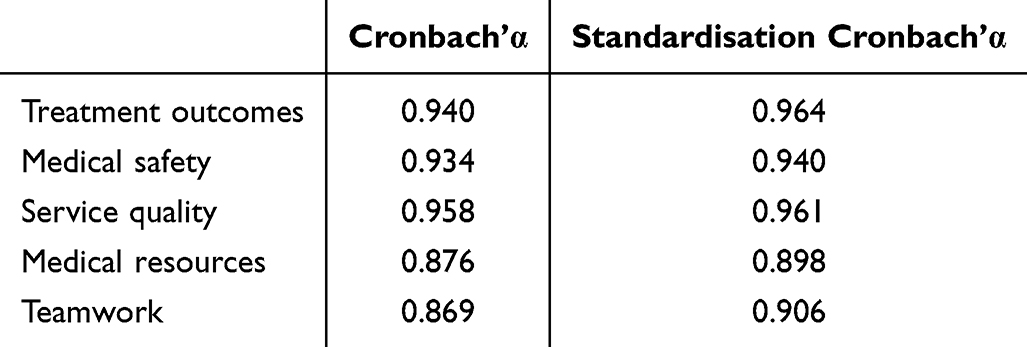 |
Table 4 Reliability Analysis |
Actual Cases
The Second Hospital Affiliated to Wenzhou Medical University is a comprehensive tertiary hospital, whose haematological surgery department has a high reputation in the region and carries out a large number of haematological surgical interventions every year. Before the management evaluation index system in haematological surgical interventions, there were some management problems in the hospital’s haematological surgical interventions. The original evaluation system in our hospital focused on efficacy indicators, and the Cronbach’s α of this system was 0.869–0.958, which was significantly higher than that of the original system (0.682–0.824). The results of the patient satisfaction survey showed that patients had more complaints about the long waiting time, insufficiently detailed communication between doctors and nurses, and insufficient postoperative rehabilitation guidance, with an overall satisfaction rate of only 65%. In terms of medical quality, the incidence of surgical complications was about 8%, and some of the surgical procedures were not standardised enough, which affected the treatment effect. In terms of medical resource utilisation, the equipment utilisation rate was about 60%, with a certain degree of idleness, low bed turnover rate, and longer average hospitalisation days for patients. After one year of implementing the indicator system, patient satisfaction has significantly improved to 85%. Further analysis of patient feedback revealed that patients highly valued the professionalism and service attitude of the medical and nursing staff. At the same time, the incidence of surgical complications was reduced to 4%, reaching the advanced level of the industry; the equipment utilisation rate was raised to 90%. By monitoring the equipment utilisation indicators, the hospital rationally arranged the surgical plan and avoided the waste of idle equipment. According to the volume of surgery and patient demand, the maintenance and repair plan of the equipment is optimised to ensure that the equipment is always in good operating condition. The turnover rate of beds has significantly improved, and the average number of patient days in hospital has been shortened by 1 day. Through real-time monitoring and analysis of bed usage, the hospital rationally allocates bed resources, reduces patients’ waiting time for beds, and at the same time optimises the treatment process and improves patients’ treatment efficiency Table 5.
 |
Table 5 Comparison Before and After Implementation of the Indicator System |
Discussion
As an emerging minimally invasive discipline integrating diagnostic imaging and clinical treatment, interventional therapy in hematologic surgery has been developing rapidly.15 At the technical level, endoluminal intervention technology continues to innovate, aortic endoluminal repair, peripheral arterial endoluminal angioplasty and stenting are widely used, transcatheter thrombolysis, vascular embolization technology in the treatment of bleeding disorders and tumors with remarkable results in clinical practice, the treatment of minimally invasive, safe, efficient and so on, for many patients to bring new hope,16 such as part of the hospitals with the help of interventional embolization therapy to deal with a variety of bleeding disorders, significantly reducing complications. For example, some hospitals have successfully dealt with a variety of bleeding conditions with the help of interventional embolization therapy, which significantly reduces complications and improves patients’ quality of life.17 However, there is a big gap between the management level of different regions and hospitals, and the lack of equipment, technology, and talents in primary medical institutions makes it difficult to practice advanced management models. Moreover, the degree of informatization of interventional therapy management is low, and data integration and analysis are insufficient, which affects the control and study of treatment effects and complications.18 Based on this, this study constructed an evaluation index system for the management of interventional therapy in hematologic surgery, with a view to providing guidance for the management of hospitals.
This study conducted an in-depth literature research on the basis of interventional therapy, and established a preliminary index system to ensure the extensiveness of the management evaluation index system of haematological surgical interventions, and the index system was repeatedly revised through the form of experts’ correspondence and interviews. The authority coefficient of the first round of correspondence was 0.8289, and after adjusting the system according to the experts’ opinions, the authority coefficient of the second round of experts’ correspondence was increased to 0.9039. The 28 interviewed experts who participated in this study came from various provinces and cities in China, including medical professionals, nursing professionals, and haematological surgeons, who are representative and authoritative in their respective fields, which provided solid professional support for the study and ensured that the management of haematological surgery interventional therapy was not only a good choice, but also an effective way to evaluate the management of haematological surgery. At the same time, the implementation of this index system requires an investment of approximately 50,000 yuan for staff training and data system upgrades. However, with the improvement in resource utilization, the investment can be recovered within 6 months.
In the stage of hierarchical analysis, this study demonstrates and improves the evaluation index system of haematological surgery interventional therapy management, and increases the credibility of the weights of the indexes by quantitatively calculating and dealing with the subjective ratings of the experts. After the construction of the index system was completed, this study chose 100 patients treated in haematological surgery to conduct a survey to ensure the good readability and authenticity of the index system and at the same time, the Cronbach’α coefficient was used to indicate the reliability of the index system of haematological surgery interventional therapy management. In addition, the content of the evaluation index system of haematological surgery interventional therapy management is closely related to the clinic, the index elements are complete, and it is practical and operable by simply collecting data.
The management evaluation index system constructed in this study covers four first-level indicators, namely, medical safety, medical service quality, medical resource utilisation and teamwork, which provides a comprehensive and detailed assessment framework for the clinical management and care of haematological surgical intervention. In clinical practice, these indicators show remarkable features, which strongly promote the optimisation and upgrading of medical services.
Level 1 indicators control the key areas of haematosurgical interventional therapy management at a macro level. Medical safety focuses on surgical safety, infection prevention and control, adverse event management and emergency equipment and drug protection, providing a solid foundation for treatment;19 medical service quality focuses on patient satisfaction, pre-operative and post-operative communication, and complaint handling, improving patients’ experience in all aspects;20 medical resource utilisation aims to rationally deploy equipment, beds, manpower and materials, improving operational efficiency;21 teamwork emphasises multidisciplinary consultation, information transfer, medical and nursing cooperation and inter-departmental project promotion, which is the key to the optimisation and upgrading of medical services. Teamwork emphasises multidisciplinary consultation, information transfer, medical and nursing care, and inter-departmental project promotion to enhance team cohesion and collaboration.22
As a subdivision of the first-level indicators, the second-level indicators play a key role in clinical management and nursing care. Indicators such as surgical error rate, infection incidence rate, timely reporting of adverse events, and completion rate of emergency equipment help to accurately manage medical safety; patient satisfaction, preoperative communication adequacy, completion rate of postoperative follow-up, and timely handling of complaints provide a clear direction for the improvement of healthcare service quality; equipment usage rate, bed turnover rate, medical and nursing workload rate, and turnover rate of drug and consumable stocks guide the efficient allocation of medical resources; multidisciplinary meetings and conferences are also used to enhance the effectiveness of medical care and nursing care, as well as to improve the quality of medical care. Equipment utilisation rate, bed turnover rate, workload rate of medical and nursing staff, drug and consumable inventory turnover rate, guiding the efficient allocation of medical resources; Timeliness of multidisciplinary consultation, accuracy of inter-departmental information transfer, satisfaction of teamwork, completion rate of inter-departmental collaborative projects, facilitating the efficient development of teamwork.
The three-level indicators penetrate into clinical practice and provide an accurate basis for management evaluation. In terms of medical safety, we assess the effectiveness of treatment to optimize the plan by comparing the cure rate of different disease types and age groups with the average cure rate of the same industry in China; we monitor the treatment process with the help of the changes of symptoms, haematology and imaging indexes in the short-, medium- and long-term as well as in the perioperative period; and we strictly control the deviation of key operations and plan execution to prevent the infection of surgical incisions and instruments and ensure the safety of equipment and medication. In terms of the quality of medical services, we assess the service experience in terms of the satisfaction of patients and medical staff, the satisfaction of the consultation environment, refine the information on surgical risks and the answers to patients’ questions, and improve the quality of follow-up visits by the response and resolution of telephone and online follow-up visits. In the dimension of medical resource utilisation, we have improved the efficiency of core equipment and interventional devices, shortened the average length of stay of patients, accelerated the turnover of patients in the recovery period, reasonably arranged doctors’ consultations and nurses’ working hours, and optimised the turnover rate of stock of commonly used and high-value consumables. In the field of teamwork, we have strengthened the smoothness of communication between doctors and nurses and the degree of cooperation on problems, ensured timely and effective emergency and routine consultations, promoted the timely completion of interdepartmental projects, and improved the success rate of joint treatment for complex cases.
Conclusion
The multi-dimensional evaluation system constructed in this study is scientific and reliable. After implementation, it has significantly improved treatment outcomes and resource utilization efficiency, providing a standardized tool for the management of interventional therapy in hematologic surgery., The sample of this study was only from a single hospital, and regional differences in medical resources may affect the generalizability of the results; additionally, the index system does not incorporate special needs of patients with rare diseases. In the future, we will expand the sample size to include multi-center data and supplement relevant indicators to enhance applicability; with the rapid development of medical technology, such as the application of new interventional devices, the promotion of telemedicine in the Department of Hematologic Surgery and so on, the demand for new management indexes may arise. In conclusion, the index system effectively provides strong support for the management of hematology surgery and effectively promotes the improvement of the management level of the department. In the future, we will verify the universality of the system through multi-center studies involving hospitals in different regions and with varying resource allocations. Additionally, we plan to integrate artificial intelligence technology to develop a real-time evaluation module, enabling dynamic updates of indicator weights—for example, incorporating management indicators for new interventional devices as they emerge. These efforts aim to enhance the adaptability and timeliness of the index system, providing more targeted support for the management of hematological surgical interventional therapy.
Data Sharing Statement
The datas used and/or analyzed during the current study are available from the corresponding author.
Ethics Statement
This study was approved by the Human Ethics Committee of The Second Affiliated Hospital of Wenzhou Medical University (Ethics Approval Number: 2024-K-048-02). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Consent to Publish Declaration
All participants agreed to publish.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no fund support from any institution or individual for this research.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kärkkäinen JM, Pather K, Tenorio ER, et al. Should endovascular approach be considered as the first option for thoraco-abdominal aortic aneurysms? J Cardiovasc Surg. 2019;60(3):298–312. doi:10.23736/S0021-9509.19.10905-6
2. Clough RE, Martin-Gonzalez T, Van Calster K, et al. Endovascular repair of thoracoabdominal and arch aneurysms in patients with connective tissue disease using branched and fenestrated devices. Ann Vasc Surg. 2017;44:158–163. doi:10.1016/j.avsg.2017.05.013
3. Tian Z, Vollmer Barbosa C, Lang H, et al. Efficacy of pharmacological and interventional treatment for resistant hypertension: a network meta-analysis. Cardiovasc Res. 2024;120(1):108–119. doi:10.1093/cvr/cvad165
4. Zhang J, Fang J, Xu Y, et al. How AI and robotics will advance interventional radiology: narrative review and future perspectives. Diagnostics. 2024;14(13):1393. doi:10.3390/diagnostics14131393
5. Anderson DR, Morgano GP, Bennett C, et al. American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019;3(23):3898–3944. doi:10.1182/bloodadvances.2019000975
6. Kasper CK, Boylen AL, Ewing NP, Luck JV, Dietrich SL. Hematologic management of hemophilia A for surgery. JAMA. 1985;253(9):1279–1283. doi:10.1001/jama.1985.03350330077026
7. Chacon GE, Ugalde CM. Perioperative management of the patient with hematologic disorders. Oral Maxillofac Surg Clin. 2006;18(2):161–171. doi:10.1016/j.coms.2005.12.010
8. Saini V, Li J, Yang Y, et al. Evaluating environmental quality in Rujigou coalfield, China, using analytic hierarchy process. Environ Sci Pollut Res Int. 2023;30(1):1841–1853. doi:10.1007/s11356-022-22340-1
9. Park S, Kim HK, Lee M. An analytic hierarchy process analysis for reinforcing doctor-patient communication. BMC Prim Care. 2023;24(1):24. doi:10.1186/s12875-023-01972-3
10. Valent P, Orazi A, Savona MR, et al. Proposed diagnostic criteria for classical chronic myelomonocytic leukemia (CMML), CMML variants and pre-CMML conditions. Haematologica. 2019;104(10):1935–1949. doi:10.3324/haematol.2019.222059
11. Christen D, Brümmendorf TH, Panse J. [Leukopenia - a diagnostic guideline for the clinical routine]. Dtsch Med Wochenschr. 2017;142(23):1744–1749. German. doi:10.1055/s-0043-113123
12. Cantón-Bulnes ML, Garnacho-Montero J. Practical approach to the management of catheter-related bloodstream infection. Rev Esp Quimioter. 2019;32(Suppl 2):38–41. doi:10.1016/j.medin.2017.09.012
13. Arnold MJ, Keung JJ, McCarragher B. Interventional Radiology: indications and Best Practices. Am Fam Physician. 2019;99(9):547–556.
14. Tang FF, Huang XJ. [The main progresses and hot spots of hematological diseases in the past decade]. Zhonghua Nei Ke Za Zhi. 2024;63(4):321–327. Polish. doi:10.3760/cma.j.cn112138-20231222-00397
15. Pepe M, Peruzzi M, Biondi-Zoccai G, et al. Antithrombotic Therapy for Vascular Disease and Intervention: the Best Is Yet to Come? J Cardiovasc Pharmacol. 2021;78(3):334–335. doi:10.1097/FJC.0000000000001092
16. Duan W, Akinyemi T, Du W, et al. Technical and clinical progress on robot-assisted endovascular interventions: a review. Micromachines. 2023;14(1):197. doi:10.3390/mi14010197
17. Lengyel BC, Chinnadurai P, Corr SJ, et al. Robot-assisted vascular surgery: literature review, clinical applications, and future perspectives. J Robot Surg. 2024;18(1):328. doi:10.1007/s11701-024-02087-2
18. Gupta A, Thulasidasan N, Mak SM, et al. Contemporary interventional management of pulmonary embolism. Clin Radiol. 2023;78(5):315–322. doi:10.1016/j.crad.2023.01.005
19. Tidswell EC. A nontrivial analysis of patient safety risk from parenteral drug- and medical device-borne endotoxin. Drugs R D. 2023;23(1):65–76. doi:10.1007/s40268-023-00412-y
20. Valença-Feitosa F, Carvalho GAC, Alcantara TS, et al. Identifying health outcomes of pharmaceutical clinical services in patients with cancer: a systematic review. Res Social Adm Pharm. 2023;19(4):591–598. doi:10.1016/j.sapharm.2022.12.009
21. Feuerstadt P, Stong L, Dahdal DN, et al. Healthcare resource utilization and direct medical costs associated with index and recurrent Clostridioides difficile infection: a real-world data analysis. J Med Econ. 2020;23(6):603–609. doi:10.1080/13696998.2020.1724117
22. Williams ME, Pearson DA, Capal JK, et al. Impacting development in infants with tuberous sclerosis complex: multidisciplinary research collaboration. Am Psychol. 2019;74(3):356–367. doi:10.1037/amp0000436
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.