Back to Journals » Clinical Ophthalmology » Volume 18
Consistency in Standalone Canaloplasty Outcomes Using the iTrack Microcatheter
Authors Khaimi MA ![]() , Koerber N, Ondrejka S, Gallardo MJ
, Koerber N, Ondrejka S, Gallardo MJ ![]()
Received 19 September 2023
Accepted for publication 5 January 2024
Published 16 January 2024 Volume 2024:18 Pages 173—183
DOI https://doi.org/10.2147/OPTH.S441113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract of “Standalone canaloplasty outcomes using iTrack microcatheter” [441113].
Views: 1446
Mahmoud A Khaimi,1 Norbert Koerber,2 Simon Ondrejka,2 Mark J Gallardo3
1Dean McGee Eye Institute – Oklahoma Health Center, Oklahoma City, OK, USA; 2Augencentrum Köln, Köln, Germany; 3El Paso Eye Surgeons, PA, El Paso, TX, USA
Correspondence: Mahmoud A Khaimi, Dean McGee Eye Institute – Oklahoma Health Center, 608 Stanton L Young Blvd, Oklahoma City, OK, 73104, USA, Tel +1 405-271-6060, Email [email protected]
Purpose: To study the consistency in outcomes of standalone canaloplasty performed via an ab-interno surgical technique in reducing intraocular pressure (IOP) and number of medications in uncontrolled open-angle glaucoma (OAG) eyes over a 12-month period.
Methods: This retrospective multicenter case series included patients who underwent standalone canaloplasty via an ab-interno surgical technique using the iTrack microcatheter (Nova Eye, Inc., Fremont, USA) and had preoperative uncontrolled OAG (IOP≥ 18mmHg) along with no previous glaucoma surgery. The iTrack microcatheter is used to circumnavigate 360° and viscodilate Schlemm’s canal. Consistency of IOP and medications reduction on an eye-by-eye basis were evaluated to understand the outcomes in each single eye.
Results: Sixty-four eyes of 60 patients (age 71.5± 13.4 years) were included. Six eyes (9%) that underwent additional glaucoma surgery were considered a failure and were subsequently excluded from analysis. At 12 months, IOP was reduced in 57 of the 58 (89%) remaining eyes; one eye had the same IOP with a reduced number of medications. Of the 57/58 eyes with a reduced IOP: 44 eyes (69%) required fewer medications; 12 eyes (19%) required the same number of medications. Of these 58 eyes, 78% of eyes had a ≥ 20% reduction in IOP compared to baseline; 69% eyes had a postoperative IOP ≤ 15 mmHg, and 86% eyes ≤ 18 mmHg at 12 months. Forty percent of the eyes were medication-free at 12 months compared to none at baseline.
Conclusion: Canaloplasty performed via an ab-interno surgical technique as a standalone procedure consistently reduced IOP and glaucoma medications in almost all eyes.
Keywords: canaloplasty, iTrack, microcatheter, viscodilation, intraocular pressure, open-angle glaucoma
Introduction
Glaucoma has been identified as the leading cause of irreversible but preventable blindness in the world, with the number of cases expected to rise to 112 million by 2040, exerting a huge pressure on healthcare systems worldwide.1,2
Intraocular pressure (IOP) is known to be the only known modifiable risk factor in glaucoma.3 According to the Early Manifest Glaucoma Trial, every 1 mmHg decrease in IOP can reduce the progression of glaucoma by almost 10%.4,5
Introduced to bridge the gap between topical antiglaucoma treatment and invasive filtration surgery, minimally invasive glaucoma surgery (MIGS) has demonstrated utility in lowering IOP in a safe and significant manner. However, the results are usually reported as a mean outcome of a cohort and, still today, little is known regarding how consistent MIGS procedures are on an eye-by-eye basis.
Several MIGS devices are currently available, differing mostly in their mechanism of action and target location, acting on either the trabecular/conventional outflow, the suprachoroidal area, or the subconjunctival area.6 The majority of MIGS are focal in their approach, i.e the iStent Trabecular Micro-Bypass Stent System (Glaukos Corporation, San Clemente, CA) and Hydrus Microstent (Ivantis, Inc, Irvine, CA). With focal-based MIGS, the clinical outcomes may vary depending on the placement of the stent and whether this correlates with the point(s) of outflow resistance. Consequently, results may therefore fluctuate among eyes, with some eyes experiencing a large IOP reduction and other eyes with no IOP reduction at all:7 with this perspective, the mean IOP reduction of a cohort may not help predictability on an individual basis.
Since the variety of MIGS devices and procedures enables surgeons to take a more nuanced treatment approach that is better tailored to the needs of each patient, their effectiveness should also be evaluated with respect to each individual patient rather than relying only on mean outcomes.
The authors decided to investigate whether canaloplasty would yield a consistent eye-by-eye reduction in IOP. Canaloplasty performed via an ab-interno surgical technique is a type of implant-free MIGS that targets all aspects of the complete 360° of the conventional outflow pathway (trabecular meshwork, Schlemm’s canal, and the distal collector channels), offering a comprehensive approach to lower IOP, unlike other MIGS that are mainly focal in their approach. This understanding of the disease pathology may be further translated into a consistent reduction in IOP in all patients of primary open-angle glaucoma (POAG).8,9 The authors decided to investigate its efficacy when performed as a standalone procedure in excluding the confounding effect of phacoemulsification in reducing IOP.10,11
This study assesses the consistency of results (the IOP lowering effect on each single eye) obtained with standalone canaloplasty via an ab-interno surgical technique in reducing IOP and number of medications in uncontrolled open-angle glaucoma patients over a 12-month period using the iTrack canaloplasty device (Nova Eye, Inc., Fremont, California).
Materials and Methods
Study Design
This study was a multicenter, multi-surgeon, retrospective review of a consecutive case series of eyes treated with canaloplasty as a standalone procedure. This study was conducted according to the tenets of the Declaration of Helsinki, and written consent was obtained from patients. Data meeting inclusion criteria (below) was extracted and collated from three cohorts whose overall results are already published and available in the scientific literature and had received Institutional Review Board (IRB) approval or waiver.12–14
Patient Selection
Inclusion criteria included adult POAG patients (18 years of age or older) with a diagnosis of mild–moderate or severe glaucoma, as per the Hodapp–Parrish–Anderson classification system, uncontrolled IOP with medications (defined as baseline IOP≥18mmHg), as well as healthy angle structures on gonioscopy with a homogenously pigmented trabecular meshwork without variegation or excessive pigmentation. Disease severity was determined based on mean deviation (MD) from Humphrey visual field (HVF) testing: MD less than −6dB (mild), −6db to −12dB (moderate), and greater than 12dB (severe).
Patients with peripheral anterior synechiae, goniosynechiae, or angle recession, were excluded from the study. Patients with neovascular disease, uveitis, peripheral anterior synechiae, and developmental or other forms of secondary glaucoma, such as steroid- induced glaucoma, were also excluded.
The authors (MK, NK, SO, MG) have collated three different cohorts of eyes with open-angle glaucoma that was uncontrolled by medications at baseline (IOP≥18mmHg), underwent canaloplasty as a standalone procedure (not concomitant with cataract surgery), reached at least the 12-month follow-up, and did not undergo any additional glaucoma surgery. The outcomes of the entire cohort of eyes (ie, including the eyes treated with other glaucoma surgery and that were controlled at baseline) were previously published in the literature (Gallardo 2022,12 Khaimi 2021,13 Koerber et al 202215).
Endpoints
Success was defined either as a reduction in IOP and number of medications, or a reduction in IOP with the same number of medications. An ambiguous outcome was defined as when either the IOP decreased but the number of medications also increased, when IOP and number medications did not change, or when IOP increased and number of medications decreased. Failure was assigned when eyes underwent additional glaucoma surgery and when IOP remained the same or increased and the number of medications increased or remained the same. Success was also reported according to the Guidelines on Design & Reporting Glaucoma Trials.16
Surgical Technique
A small 1–2 mm incision is made in the trabecular meshwork, and the microcatheter is inserted into Schlemm’s canal, circumnavigating the entire 360°. If an obstruction to the passage of the microcatheter is encountered, the microcatheter is withdrawn and re-inserted into the canal in the opposite direction. After the microcatheter completes 360° catheterization of the canal, it is slowly withdrawn. Simultaneously, precisely regulated microquantities of high-molecular-weight hyaluronic acid (HA)-based ophthalmic viscosurgical device (OVD) is delivered into Schlemm’s canal, with a mean of 36 clicks per procedure, resulting in an average of 100μL delivered over the entirety of Schlemm’s canal.
The postoperative care included a topical steroid like Loteprednol, and a fourth-generation fluoroquinolone. Anti-glaucoma medications were stopped postoperatively.
A description of the surgical steps is described in the literature.12,13,15
Device
All patients underwent canaloplasty performed with the same device: iTrack (Nova Eye, Inc., Fremont, USA). The iTrack is a 200-micron microcatheter with an illuminated fiber optic tip that provides continuous location while performing surgery in the eye, designed for canaloplasty. It performs 360° catheterization and pressurized viscodilation of Schlemm’s canal.
Statistical Analysis
The comparisons between changes in IOP and number of medications between two time points were analyzed using a commercially available software (Excel, Microsoft) with, where applicable, non-parametric tests (Wilcoxon) (Jamovi). Descriptive statistics (mean, standard deviation, and range) were calculated for IOP and number of medications at each visit. A p-value of <0.05 was required for a value to be considered as statistically significant and p-values are indicated where applicable. Graphs were produced according to the Guidelines on Design & Reporting Glaucoma Trials.16
Results
Demographics
In total, the entire canaloplasty cohort of uncontrolled OAG eyes included 85 eyes. Of those, several eyes were excluded from the analysis for the following reasons: 1 eye was administered Avastin prior to the 6-month follow-up; 6 eyes were lost at follow-up before 12 months. Fourteen additional eyes that were excluded had a preoperative IOP below 18 mmHg.
The remaining 64 eyes met the inclusion criteria (standalone canaloplasty, uncontrolled glaucoma) and were enrolled in the study. Thirty-eight percent of eyes had mild glaucoma, 27% had moderate, and 27% had severe glaucoma, while 9% of the eyes were not classified. Table 1 presents patient demographics while Table 2 shows preoperative measurements and postoperative outcomes at 12 months.
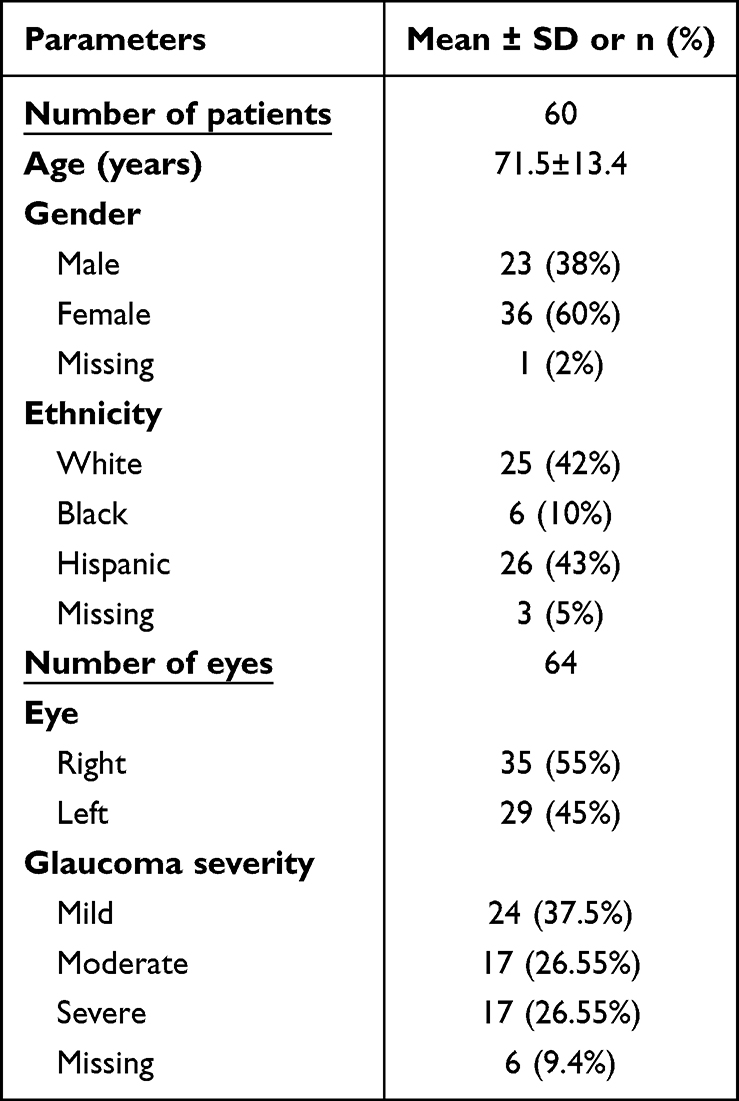 |
Table 1 Patient Demographics |
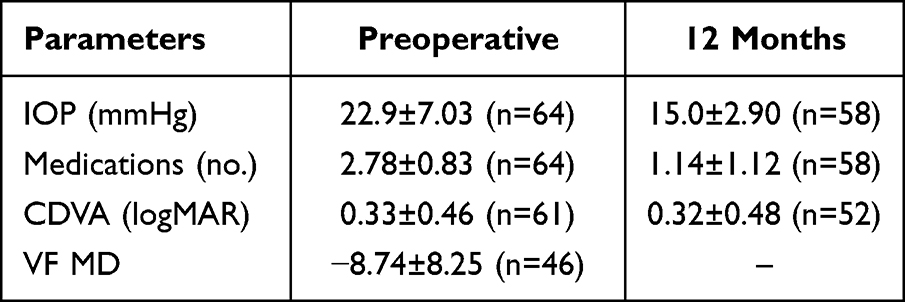 |
Table 2 Preoperative Mean Measurements and Postoperative Mean Outcomes |
Six eyes (9%) that underwent additional glaucoma surgery prior to the 12-month follow-up (5 Express shunts, Alcon, and 1 cyclophotocoagulation) were categorized as complete failures and were not included in the data analysis.
Mean IOP and Medications
Mean reductions in IOP and number of medications were statistically significant (p<0.001) in the remaining cohort that was analyzed (58 eyes; 91% of the entire cohort): mean IOP decreased from 22.94±7.03 mmHg (median:20; range: 18, 58) at baseline to 15.03±2.9 mmHg (median: 15; range: 9, 26) at 12 months postop and mean number of medications decreased from 2.74±0.8 (median: 3; range: 1, 4) to 1.14±1.1 (median: 1; range: 1, 3) at the 12-months postoperative time point. Figure 1 shows a bar diagram of the number of medications at baseline and 12 months.
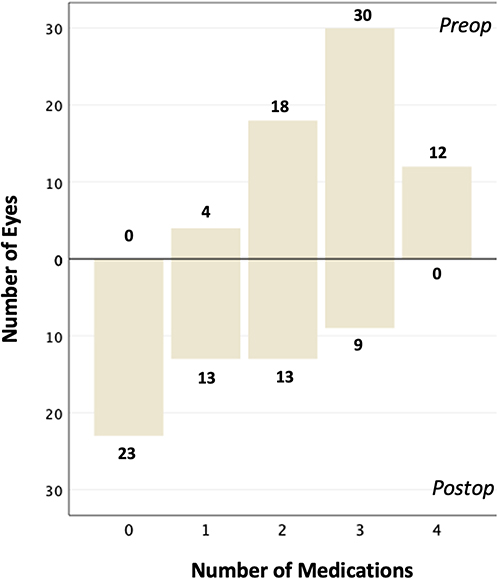 |
Figure 1 Bar diagram showing number of eyes with medications at preop and postop (12 months). |
IOP and Medications Reduction on an Eye-by-Eye Basis (Baseline Vs 12 Months)
Success and Failures
Figure 2 shows a scatterplot of the 58 eyes that reached the 12-month follow-up with canaloplasty alone. Each point represents an eye’s outcomes at preop and postop. Notably, the reduction in IOP was consistent, with no increase in IOP observed.
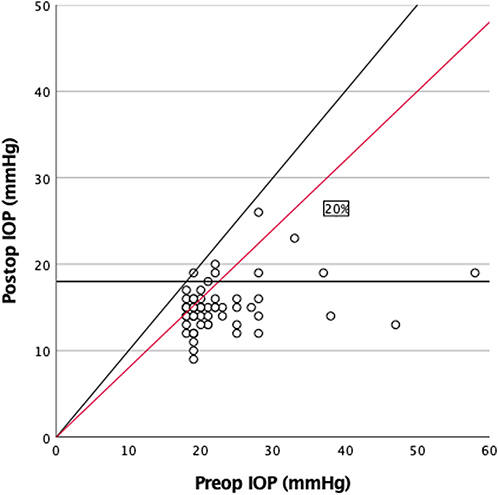 |
Figure 2 Scatterplot of intraocular pressure (IOP) outcomes at preop and postop (12 months). Points on the diagonal line indicate eyes with no change in IOP; points to the right of the red line indicate eyes with at least 20% reduction in IOP. Horizontal line indicates IOP of 18 mmHg. |
Fifty-seven (57) out of those 58 eyes (89% of the entire cohort) demonstrated a reduced IOP at 12 months postop, while one eye had no change in IOP. Of the 57/58 eyes that noted a reduced IOP, 44 eyes (69%) also had a reduced medication burden, while in 12 eyes (19%) the number of medications remained the same. As such, 56 eyes (88%) were categorized as success and 2 eyes (3%) as ambiguous. Six eyes (9%) were categorized as complete failure because they underwent additional glaucoma surgery (Table 3).
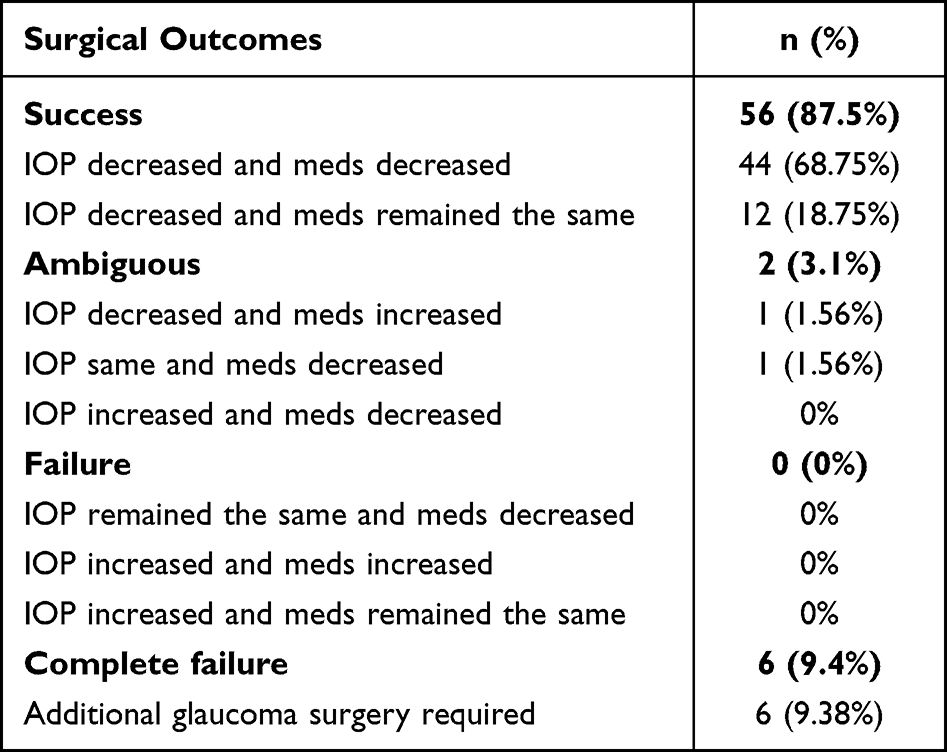 |
Table 3 Number and Percentage of Eyes That Succeeded, Failed, or Had Ambiguous IOP and Medication Outcomes (Baseline Vs 12 Months Data) as per Methods Section |
When using the Guidelines on Design & Reporting of Glaucoma Surgical Trials (World Glaucoma Association),16 87.5% of the eyes were either a complete or qualified success and 12.5% were failures (Table 4).
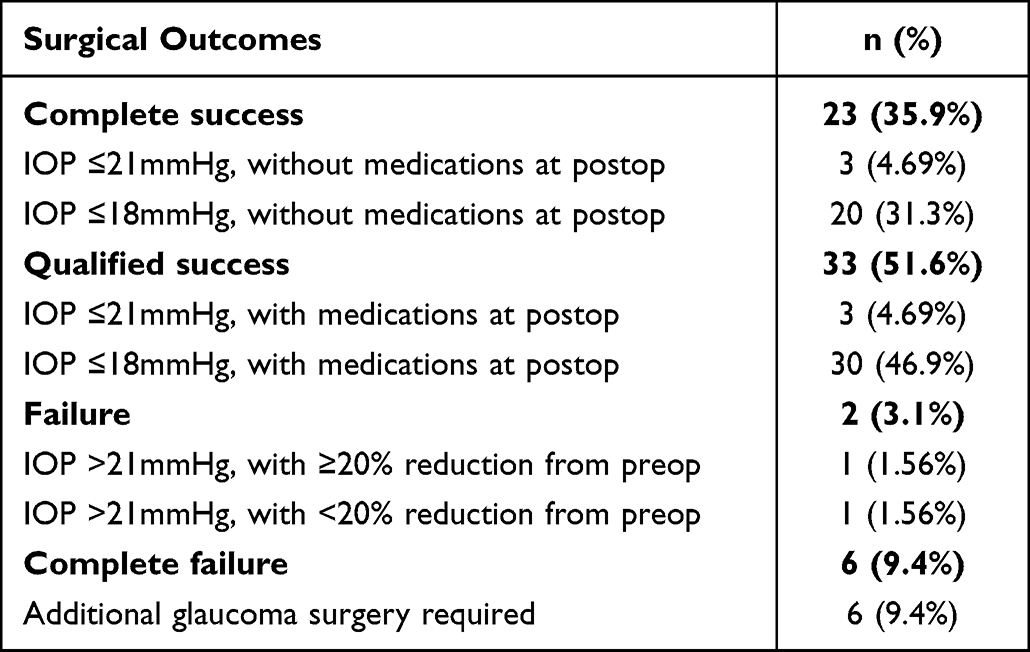 |
Table 4 Surgical Outcomes (Baseline Vs 12 Months). Success Range Reported as per the Guidelines on Design and Reporting of Glaucoma Surgical Trials (World Glaucoma Association) |
Stratification of IOP Reduction
Out of the 58 eyes that were analyzed, 28 eyes (48%) had an IOP reduction of ≥7 mmHg and 25 eyes (43%) had an IOP reduction between 3 and 6 mmHg. Only 5 eyes (9%) had an IOP reduction between 0 and 3 mmHg (Figure 3). Forty-five eyes (77.6%) of eyes had a ≥20% reduction in IOP compared to baseline; 69% eyes had a postoperative IOP ≤15 mmHg compared to none at preop, and 86.2% eyes had an IOP ≤18 mmHg at 12 months, compared to 17.2% at preop (10 eyes had an IOP=18mmHg at baseline).
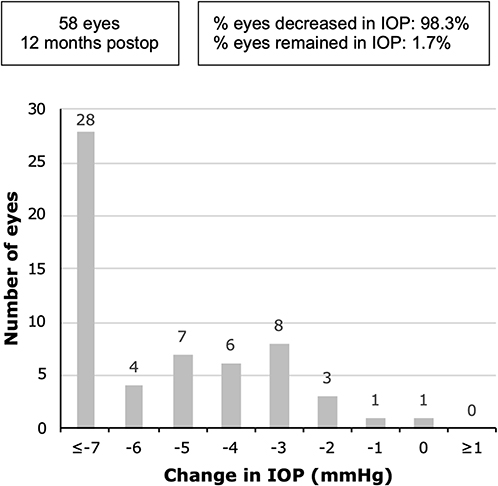 |
Figure 3 Changes in intraocular pressure outcomes of 58 eyes (baseline vs 12 months). |
Forty percent of the eyes were medication-free at 12 months compared to zero at baseline (Table 5). Thirty-four percent of the eyes had a postoperative IOP ≤18 mmHg without any medications, compared to zero at baseline.
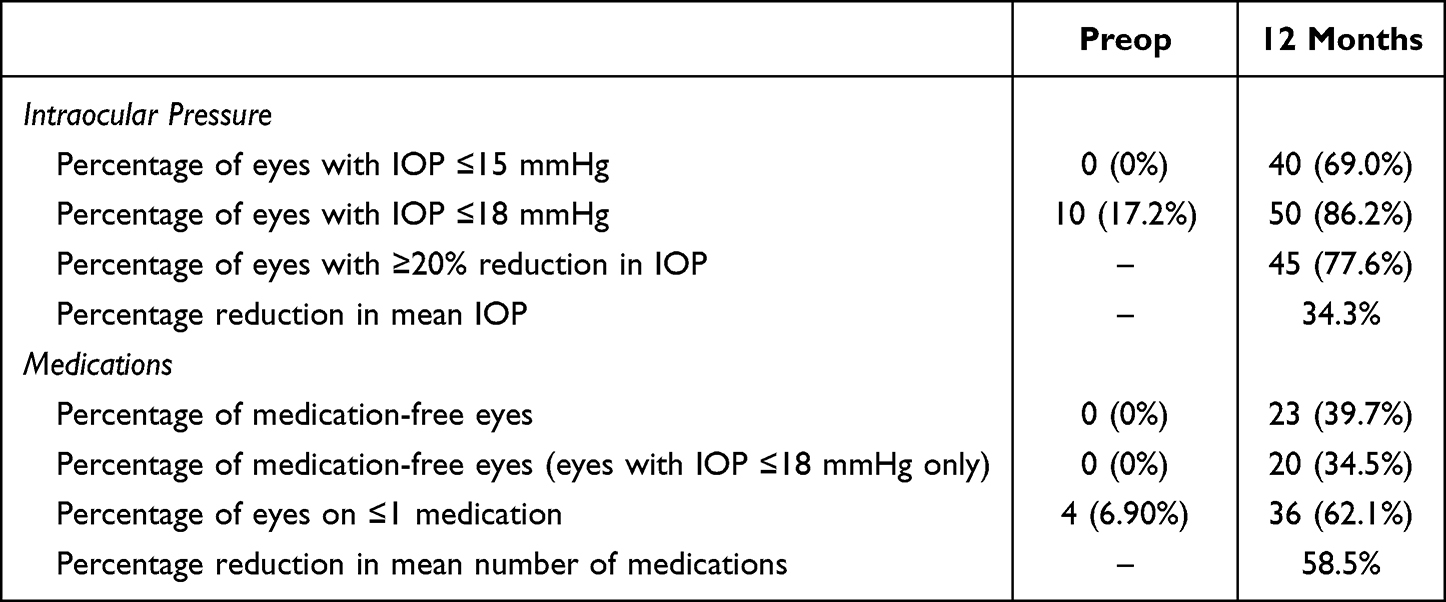 |
Table 5 IOP and Medications Outcomes (Baseline Vs 12 Months) of the 58 Eyes Reaching the 12-Month Follow-Up with Canaloplasty Alone |
Figure 4 shows the mean pre- and postoperative outcomes and the range of the IOP distribution of the 58 eyes, being distributed widely at baseline (range 18–58 mmHg; median 20 mmHg) while much narrower at 12 months postoperatively (range 9–26 mmHg; median 15 mmHg).
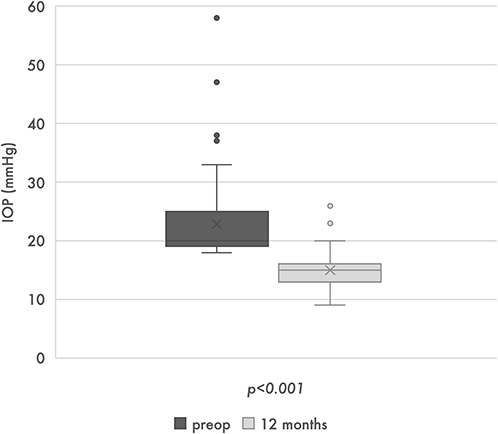 |
Figure 4 Mean preoperative and postoperative intraocular pressure outcomes of 58 eyes. |
Preoperatively, 17% of the eyes were ≤18 mmHg and 45% ≤21 mmHg; postoperatively they were 86% and 10% respectively, with only 4% above 21 mmHg.
Excluded Eyes Due to Additional Glaucoma Surgery
Six eyes were excluded because they received additional glaucoma surgery for a various of reasons and the IOP and medication outcomes could not be evaluated with canaloplasty only at 12 months. The eyes (glaucoma stage mild n=3; moderate n=2; severe n=1) had a mean preoperative IOP of 23.5 mmHg and were on 3.2 medications.
One of the 6 eyes was excluded because it underwent cyclophotocoagulation at 6 months: this eye belonged to a 90-year-old patient with very low visual acuity (0.10 logMAR) and while this eye IOP was under control, it was not possible to reduce the medications. One eye registered an IOP reduction of 20% which was not enough to bring the glaucoma under control (from 25mmHg to 20mmHg). IOP did not reduce in the remaining 4 eyes (6% of the entire cohort; 2 mild, 1 moderate, 1 severe).
Safety
There were no serious complications recorded. Postoperative micro-hyphema and cells, as well as flare, were observed in some patients, but they were transient and resolved without sequelae. Vision on the logMAR chart remained stable (Table 2).
Discussion
The literature published by the authors in 2021/2022 has supported the safety and effectiveness of canaloplasty via an ab-interno surgical technique for POAG in lowering mean IOP and reducing the mean number of medications12,13,15,17 and several other studies have also confirmed these findings.18–21 Riaz et al22 showed that the tissue-sparing, minimally invasive nature of canaloplasty, which aims to works with patient physiology, can also effectively and safely reduce IOP in post-keratoplasty glaucoma eyes, where topical hypotensives may pose a risk factor for corneal graft failure and further filtration glaucoma surgery may be too invasive for such fragile corneas.23 The mean IOP and medication reduction of canaloplasty are proven in this study and in the literature.
However, the purpose of this study was not to investigate the mean IOP reduction but the consistency of IOP reduction in each individual eye. It was observed that almost all eyes that reached the 12-month follow-up (57/58 eyes) with canaloplasty alone (and no other glaucoma surgery) have obtained an IOP reduction that, in most cases, was associated with a reduction in the number of medications. It is not possible to compare the results of this cohort in the literature given that, to our knowledge, this is the first study to investigate this kind of eye-by-eye outcome, either employing canaloplasty or other MIGS procedures.
The reason that canaloplasty appears to be, to varying degrees, effective in most eyes (91% of the cohort) may be related to its comprehensive approach. Canaloplasty improves outflow facility via a combination of mechanical, hydrostatic, and biophysical mechanisms: the 360° catheterization of Schlemm’s canal mechanically breaks adhesions within the canal while pushing herniations of the trabecular meshwork out of the collector channel ostia, thus improving outflow facility. The hydrostatic pressure caused by the delivery of OVD stretches the trabecular meshwork, possibly creating microperforations into the anterior chamber, while also dilating Schlemm’s canal and the collector channels.24,25 These obstructions within the trabecular meshwork may account for up to 75% of the total outflow resistance in cases of POAG, and herniations of the trabecular meshwork into the collector channels are a significant contributor to outflow resistance.9,26 Research by Gong et al has shown that up to 90% of the collector channels in POAG eyes are blocked by herniations of the trabecular meshwork27 and thus represents another important cause of outflow resistance, in addition to Schlemm’s canal, which is significantly shorter, narrower, and often collapsed in POAG eyes.28,29 This can be attributed to a better understanding of the disease pathology along with the fact that, since outflow obstruction can reside across all levels of the conventional outflow pathway, including the trabecular meshwork, Schlemm’s canal, and the collector channels, glaucoma treatments which employ a more comprehensive approach may offer more significant utility with respect to treatments that are focal in their approach.24,25,30
Indeed, other MIGS such as Trabectome (NeoMedix Corporation, Tustin, USA), the iStent, and the Hydrus Microstent, target the trabecular meshwork in isolation.31,32 The Trabectome ablates the trabecular meshwork and inner wall of Schlemm’s canal using an electrosurgical pulse while the iStent works as a trabecular microbypass from the anterior chamber into Schlemm’s canal.33 The Hydrus is inserted into Schlemm’s canal to improve outflow from the anterior chamber to Schlemm’s canal.34
A retrospective study conducted by Arnljots et al on patients undergoing iStent implantation versus Kahook Dual Blade (KDB) goniotomy found that standalone iStent implantation could reduce IOP to <19 mmHg in 57% of cases (8/14), while the KDB goniotomy successfully reduced IOP to <19 mmHg in 77% of cases (10/13).7 In the COMPARE study, 64.4% of eyes were implanted with the Hydrus device (Ivantis) and 57.3% of the eyes implanted with 2 iStent (Glaukos) were ≤18mmHg postoperatively (41.3% and 44.2% respectively preoperatively).35 In the current study, 78% of eyes (50/64) which underwent canaloplasty had a postoperative IOP ≤18 mmHg at 12 months with canaloplasty alone – compared to 16% preoperatively. Furthermore, in this study, canaloplasty achieved a ≥20% reduction in IOP in 78% of eyes that reached the 12-month follow-up (45/58). In the COMPARE study, at 12 months, the percentage of eyes ≤18 mmHg without medications was 30.1% in the Hydrus group and 9.3% in the iStent group:35 in this study with canaloplasty 34% of eyes had IOP of ≤18 mmHg without medications.
This suggests that canaloplasty can return consistent results and that its postoperative IOP outcomes are grouped in a more homogenous manner—below the “safe” limit of 18mmHg and regardless of the mean IOP reduction of the cohort.
Theoretically, the reason may lie in the design of the procedure: a focal-based MIGS procedure such as an iStent, which bypasses the trabecular meshwork, will be effective in overcoming outflow resistance localized in the trabecular meshwork.33 In those patients where outflow resistance is located distally to the trabecular meshwork, either in Schlemm’s canal or the collector channels, stenting the eye may not be effectual. As stated earlier, the outflow obstruction in glaucoma occurs at all levels in the proximal as well as distal outflow pathway24,25,30 and bypassing only the trabecular meshwork may lead to inconsistent results despite a successful procedure on the surgical table.
In addition, common postoperative complications of stent mispositioning or stent occlusion may hinder the effectiveness of stent-based MIGS on a per patient basis. According to a 2019 meta-analysis, the reported rate of further surgical intervention was in the range of 4.5–11.3% of study subjects.36 Another meta-analysis reported that 22.5% of the eyes that received iStent implantation experienced adverse events, of which the most common were IOP elevation or spikes, stent blockage, obstruction, and malpositioning.37 Comparatively, in this study, 6 eyes (6/64; 9%) were excluded from the analysis because they received additional glaucoma surgery: although some of them achieved an IOP reduction, the overall diagnosis recommended further glaucoma surgery.
This is not to suggest that stents are not effective in reducing IOP, because they are and there is a solid foundation of literature that proves significant and sustained IOP reduction in the long term, but that their effectiveness may vary greatly from eye to eye due to the multi-level nature of the outflow obstruction in glaucomatous eyes, which can occur at the trabecular meshwork, Schlemm’s canal, and the collector channels.
A comparison of study results regarding stents35,38–47 shows a similar trend, with a consistent reduction in mean IOP being observed in all studies while the standard deviation in postoperative IOP indicates a wide degree of variability, ranging from as low as ±1.8 to as high as ±5.2, while in the present cohort a postoperative standard deviation of ±2.9 was observed. A higher standard deviation points to the fact that reduction in IOP is not consistent in all patients, leading to variability in outcomes. This also shows that mean IOP reduction may not be a reliable approach to measure repeatability and reliability in treatment outcomes, especially when it comes to IOP control.
Every MIGS has its place in the glaucoma paradigm and the true value of MIGS is that it enables the surgeon to tailor a procedure that is best suited to each individual patient. Regarding canaloplasty for instance, this is not always preferable, namely when the trabecular meshwork is too fibrotic, or when the surgeon expects complicated cataract surgery.
The major limitation of this study is in the retrospective design and selection bias, as well as the lack of randomization. Another limitation is the lack of a control group to compare the results.
In conclusion, glaucoma is a multifactorial disease that requires a comprehensive treatment approach. Canaloplasty performed via an ab-interno surgical technique offers a minimally invasive procedure that targets and treats the complete outflow pathway and across the full 360 degrees, rather than treating an isolated point of the outflow pathway. This allows for results that are more predictable and consistent across all stages and categories of POAG patients.
Data Sharing Statement
All data generated or analysed for this study are included in the article. Further enquiries can be directed to the corresponding author.
Acknowledgments
Assistance in medical writing was provided by GP Communications, funded by Nova Eye Medical.
Funding
No funding has been gathered for this study.
Disclosure
The authors have no financial or proprietary interest in any material or method mentioned. Dr Khaimi is Nova Eye Medical Chief Medical Consultant for the iTrack. Prof. Koerber is the Principal Investigator for the CATALYST clinical study which uses the product mentioned in this article (iTrack, Nova Eye Medical). Dr Ondrejka is an investigator for the CATALYST study. Dr Gallardo is a consultant of Nova Eye Medical and Sight Science.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
2. Tham YCC, Li X, Wong TY, Quigley HA, Aung T, Cheng CYY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Goldmann H, Schmidt T. Über Applanationstonometrie [Applanation tonometry]. Ophthalmologica. 1957;134(4):221–242. doi:10.1159/000303213
4. Heijl A, Leske MC, Bengtsson B, Hyman L, Bengtsson B, Hussein M. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Archives of Ophthalmology. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
5. European Glaucoma Society. European glaucoma society terminology and guidelines for glaucoma, 4th edition - Chapter 2: classification and terminology supported by the EGS foundation: part 1: foreword; introduction; glossary; Chapter 2 classification and terminology. Br J Ophthalmol. 2017;101(5):73–127. doi:10.1136/bjophthalmol-2016-EGSguideline.002
6. Pillunat LE, Erb C, Jünemann AG, Kimmich F. Micro-invasive glaucoma surgery (MIGS): a review of surgical procedures using stents. Clin Ophthalmol. 2017;11:1583–1600. doi:10.2147/OPTH.S135316
7. Arnljots TS, Economou MA. Kahook dual blade goniotomy vs istent inject: long-term results in patients with open-angle glaucoma. Clin Ophthalmol. 2021;15:541–550. doi:10.2147/OPTH.S284687
8. Francis BA, Singh K, Lin SC, et al. Novel glaucoma procedures: a report by the American Academy of ophthalmology. Ophthalmology. 2011;118(7):1466–1480. doi:10.1016/j.ophtha.2011.03.028
9. Goel M, Picciani RG, Lee RK, Bhattacharya SK. Aqueous humor dynamics: a review. Open Ophthalmol J. 2010;4(1):52–59. doi:10.2174/1874364101004010052
10. Mathalone N, Hyams M, Neiman S, Buckman G, Hod Y, Geyer O. Long-term intraocular pressure control after clear corneal phacoemulsification in glaucoma patients. J Cataract Refract Surg. 2005;31(3):479–483. doi:10.1016/j.jcrs.2004.06.046
11. Shingleton BJ, Pasternack JJ, Hung JW, O’Donoghue MW. Three and five year changes in intraocular pressures after clear corneal phacoemulsification in open angle glaucoma patients, glaucoma suspects, and normal patients. J Glaucoma. 2006;15(6):494–498. doi:10.1097/01.ijg.0000212294.31411.92
12. Gallardo MJ. 36-month effectiveness of ab-interno canaloplasty standalone versus combined with cataract surgery for the treatment of open-angle glaucoma. Ophthalmol Glaucoma. 2022;5(5):476–482. doi:10.1016/j.ogla.2022.02.007
13. Khaimi MA. Long-term medication reduction in controlled glaucoma with iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery. Ther Adv Ophthalmol. 2021;13:251584142110457. doi:10.1177/25158414211045751
14. Koerber N, Ondrejka S. 6-year efficacy and safety of iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery in primary open-angle and pseudoexfoliative glaucoma. J Glaucoma. 2023. doi:10.1097/IJG.0000000000002311
15. Koerber NJ, Ondrejka S. 4-year efficacy and safety of iTrack ab-interno canaloplasty as a standalone procedure and combined with cataract surgery in open-angle glaucoma. Klin Monbl Augenheilkd. 2022;2022:1
16. Shaarawy TM, Sherwood MB, Grehn F. Guidelines on Design and Reporting of Surgical Trials. World Glaucoma Association; 2009.
17. Ondrejka S, Koerber N, Dhamdhere K. Long term effect of canaloplasty on IOP and use of IOP-lowering medications in patients with open angle glaucoma. J Cataract Refract Surg. 2022;48(12):1388–1393. doi:10.1097/j.jcrs.0000000000001000
18. Kazerounian S, Zimbelmann M, Lörtscher M, Hommayda S, Tsirkinidou I, Müller M. Canaloplasty ab interno (AbiC) – 2-year-results of a novel Minimally Invasive Glaucoma Surgery (MIGS) technique. Klin Monbl Augenheilkd. 2020;238(10):1113–1119. doi:10.1055/a-1250-8431
19. Lewis RA, Von Wolff K, Tetz M, et al. Canaloplasty: three-year results of circumferential viscodilation and tensioning of Schlemm canal using a microcatheter to treat open-angle glaucoma. J Cataract Refract Surg. 2011;37(4):682–690. doi:10.1016/j.jcrs.2010.10.055
20. Gillmann K, Aref A, Niegowski LJ, Baumgartner JM. Combined Ab interno viscocanaloplasty (ABiC) in open-angle glaucoma: 12-month outcomes. Int Ophthalmol. 2021;41(10):3295–3301. doi:10.1007/s10792-021-01891-1
21. Davids AMM, Pahlitzsch M, Boeker A, Winterhalter S, Maier-Wenzel AKK, Klamann M. Ab interno canaloplasty (ABiC)—12-month results of a new minimally invasive glaucoma surgery (MIGS). Graefes Arch Clin Exp Ophthalmol. 2019;257(9):1947–1953. doi:10.1007/s00417-019-04366-3
22. Riaz KM, Gill MS, Murphy DA, Ding K, Khaimi MA. Surgical management of intraocular pressure with ab interno canaloplasty inPostkeratoplasty patients: 12-month results. Cornea. 2022;42(1):52–59. doi:10.1097/ICO.0000000000003009
23. Price MO, Thompson RW, Price FW. Risk factors for various causes of failure in initial corneal grafts. Arch Ophthalmol. 2003;121(8):1087–1092. doi:10.1001/archopht.121.8.1087
24. Gong H, Gorantla V, Zhang Y, Freddo TF, Swain D Morphological changes in the distal outflow pathway of primary open angle glaucoma. In:
25. Wang K, Read AT, Sulchek T, Ethier CR. Trabecular meshwork stiffness in glaucoma. Exp Eye Res. 2017;158:3–12. doi:10.1016/j.exer.2016.07.011
26. Swaminathan SS, Oh DJ, Kang MH, Rhee DJ. Aqueous outflow: segmental and distal flow. J Cataract Refract Surg. 2014;40(8):1263–1272. doi:10.1016/j.jcrs.2014.06.020
27. Cha EDK, Xu J, Gong L, Gong H. Variations in active outflow along the trabecular outflow pathway. Exp Eye Res. 2016;146:354–360. doi:10.1016/j.exer.2016.01.008
28. Allingham RR, de KATER AW, Ethier CR, Ethier RC. Schlemm’s canal and primary open angle glaucoma: correlation between Schlemm’s canal dimensions and outflow facility. Exp Eye Res. 1996;62(1):101–110. doi:10.1006/exer.1996.0012
29. Hann CR, Vercnocke AJ, Bentley MD, Jorgensen SM, Fautsch MP. Anatomic changes in Schlemm’s canal and collector channels in normal and primary open-angle glaucoma eyes using low and high perfusion pressures. Invest Ophthalmol Vis Sci. 2014;55(9):5834–5841. doi:10.1167/iovs.14-14128
30. Tripathi RC. Aqueous outflow pathway in normal and glaucomatous eyes. Br J Ophthalmol. 1972;56(3):157–174. doi:10.1136/bjo.56.3.157
31. Craven ER, Katz LJ, Wells JM, Giamporcaro JE. Cataract surgery with trabecular micro-bypass stent implantation in patients with mild-to-moderate open-angle glaucoma and cataract: two-year follow-up. J Cataract Refract Surg. 2012;38(8):1339–1345. doi:10.1016/j.jcrs.2012.03.025
32. Pfeiffer N, Garcia-Feijoo J, Martinez-De-La-Casa JM, et al. A randomized trial of a schlemm’s canal microstent with phacoemulsification for reducing intraocular pressure in open-angle glaucoma. Ophthalmology. 2015;122(7):1283–1293. doi:10.1016/j.ophtha.2015.03.031
33. Saheb H, Le K. iStent trabecular micro-bypass stent for open-angle glaucoma. Clin Ophthalmol. 2014;8:1937. doi:10.2147/OPTH.S45920
34. Brandão LM, Grieshaber MC. Update on Minimally Invasive Glaucoma Surgery (MIGS) and new implants. J Ophthalmol. 2013;2013:1–12. doi:10.1155/2013/705915
35. Ahmed IIK, Fea A, Au L, et al. A prospective randomized trial comparing Hydrus and istent microinvasive glaucoma surgery implants for standalone treatment of open-angle glaucoma. Ophthalmology. 2020;127(1):52–61. doi:10.1016/j.ophtha.2019.04.034
36. Wellik SR, Dale EA. A review of the iStent® trabecular micro-bypass stent: safety and efficacy. Clin Ophthalmol. 2015;9:677. doi:10.2147/OPTH.S57217
37. Popovic M, Campos-Moller X, Saheb H, Ahmed IIK. Efficacy and adverse event profile of the istent and istent inject trabecular micro-bypass for open-angle glaucoma: a meta-analysis. J Curr Glaucoma Pract. 2018;12(2):67. doi:10.5005/JP-JOURNALS-10008-1248
38. Shalaby WS, Lam S, Arbabi A, et al. iStent versus iStent inject implantation combined with phacoemulsification in open angle glaucoma. Indian J Ophthalmol. 2021;69(9):2488. doi:10.4103/ijo.IJO_308_21
39. Ziaei H, Au L. Manchester iStent study: long-term 7-year outcomes. Eye. 2021;35(8):2277–2282. doi:10.1038/s41433-020-01255-6
40. Guedes RAP, Gravina DM, Lake JC, Guedes VMP, Chaoubah A. One-year comparative evaluation of istent or istent inject implantation combined with cataract surgery in a single center. Adv Ther. 2019;36(10):2797–2810. doi:10.1007/s12325-019-01067-5
41. Manning D. Real-world case series of iStent or iStent inject trabecular micro-bypass stents combined with cataract surgery. Ophthalmol Ther. 2019;8(4):549–561. doi:10.1007/s40123-019-00208-x
42. Nitta K, Yamada Y, Morokado S, Sugiyama K. Istent trabecular micro-bypass stent implantation with cataract surgery in a Japanese glaucoma population. Clin Ophthalmol. 2020;14:3381–3391. doi:10.2147/OPTH.S274281
43. Kozera M, Konopińska J, Mariak Z, Rękas M. Effectiveness of iStent trabecular micro-bypass system combined with phacoemulsification vs. phacoemulsification alone in patients with glaucoma and cataract depending on the initial intraocular pressure. Ophthalmic Res. 2020;64(2):327–336. doi:10.1159/000511456
44. Samuelson TW, Chang DF, Marquis R, et al. A schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: the HORIZON study. Ophthalmology. 2019;126(1):29–37. doi:10.1016/j.ophtha.2018.05.012
45. Holmes DP, Clement CI, Nguyen V, et al. Comparative study of 2‐year outcomes for Hydrus or iStent inject microinvasive glaucoma surgery implants with cataract surgery. Clin Exp Ophthalmol. 2022;50(3):303–311. doi:10.1111/ceo.14048
46. Hengerer FH, Auffarth GU, Conrad-Hengerer I. iStent inject trabecular micro-bypass with or without cataract surgery yields sustained 5-year glaucoma control. Adv Ther. 2022;39(3):1417–1431. doi:10.1007/s12325-021-02039-4
47. Salimi A, Watt H, Harasymowycz P. Long-term outcomes of two first-generation trabecular micro-bypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results. Eye Vis. 2021;8(1):43. doi:10.1186/s40662-021-00263-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Canaloplasty and Trabeculotomy Combined with Phacoemulsification for Glaucoma: 12-Month Results of the GEMINI Study
Gallardo MJ, Pyfer MF, Vold SD, Sarkisian SR Jr, Campbell A, Singh IP, Flowers B, Dhamdhere K
Clinical Ophthalmology 2022, 16:1225-1234
Published Date: 21 April 2022
Open-Label Extension Study Comparing Latanoprost 0.005% Without vs With Benzalkonium Chloride in Open-Angle Glaucoma or Ocular Hypertension
Shen Lee B, Malhotra R, Sall K, Mitchell B, Peace J
Clinical Ophthalmology 2022, 16:2285-2293
Published Date: 19 July 2022
A Multicenter 12-Month Retrospective Evaluation of Canaloplasty and Trabeculotomy in Patients with Open-Angle Glaucoma: The ROMEO 2 Study
Murphy III JT, Terveen DC, Aminlari AE, Dhamdhere K, Dickerson Jr JE
Clinical Ophthalmology 2022, 16:3043-3052
Published Date: 14 September 2022
Long-Term Effectiveness of XEN 45 Gel-Stent in Open-Angle Glaucoma Patients
Marcos-Parra MT, Salinas-López JA, Mateos-Marcos C, Moreno-Castro L, Mendoza-Moreira AL, Pérez-Santonja JJ
Clinical Ophthalmology 2023, 17:1223-1232
Published Date: 26 April 2023
Maximum Tolerated Medical Therapy for Glaucoma: Fixed-Dose Combinations of Timolol, Dorzolamide, Brimonidine with Latanoprost Versus Timolol, Dorzolamide with Latanoprost
Olvera-Montaño O, Mejia-Morales C, Jauregui-Franco RO, Gomez-Mendez SC, Muñoz-Villegas P
Clinical Ophthalmology 2025, 19:2913-2925
Published Date: 22 August 2025