")
Back to Journals » Psychology Research and Behavior Management » Volume 12
Confidence is the plant of slow growth: a moderated mediation model for predicting voice behavior among power distance orientation and team-based self-esteem in Taiwanese nurses
Authors Chang WY , Hsu CT , Yu PY
Received 25 March 2019
Accepted for publication 11 July 2019
Published 5 August 2019 Volume 2019:12 Pages 609—617
DOI https://doi.org/10.2147/PRBM.S209931
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Wen Ying Chang,1,2 Chin-Tien Hsu,1 Pei Yun Yu1,3
1Department of Counseling and Industrial-Organizational Psychology, Ming Chuan University, Taoyuan District, Taiwan; 2Taipei Veterans General Hospital, Taoyuan Branch Registered Nurse, Taoyuan District, Taiwan; 3Tri-Service General Hospital Nurse Anesthetist, Taipei, Taiwan
Background: According to the social identity theory and Chinese cultural influences, power distance orientation may play an important role in this relationship, and thus the examined model investigates the mediating role of team-based self-esteem relations between voice behavior and team trust.
Purpose: This study explores how voice behavior in the nursing workplace correlates to changes in team-based self-esteem and trust. We also examine the power distance orientation level in this process to test for any moderated mediation in these linkages.
Patients and methods: Employing convenient sampling of 247 registered nurses from a medical center in northern Taiwan. Nurses received envelopes including self-report questionnaires from the researchers, which were immediately sealed after interviews.
Results: Structural equation modeling indicates all model fits are acceptable, suggesting that team-based self-esteem has partial mediation between team trust and voice behavior. Power distance orientation also moderates the indirect effect of team trust upon self-esteem, such that the relationship is stronger among those who have a high power distance orientation.
Conclusion: This study highlights the usefulness of continued research into how nurses display promoting behavior through team-based self-esteem with a distinct level of power distance orientation under differing sources of team trust from peers, managers, and organizations, as well as how nurses, especially fresh graduates and those who underwent a job transfer, shape their social identity through psychological factors in the sense-making process.
Keywords: nurses, power distance orientation, team trust, team-based self-esteem, voice behavior
Introduction
Voice refers to the expression of a constructive challenge intended to improve a situation. Through such a promotive behavior, employees can propose innovative suggestions for change and adjusting the original procedure even when others oppose them.1 In general, voice behavior can be promotive, in which employees express a new idea or method for how to do things better, and prohibitive, in which they prevent existing or imbedding incidents, practices, and behaviors that are harmful to the group.2 In a work setting, voice behavior represents the motivation to express work-related issues, ideas, information, and opinions.3
Forming a profession with a skill for caring, medical knowledge, and emotion intelligence for collaboration, nurses not only take care of patients’ physical and psychological problems, but also need to pay attention to co-workers’ perception, such as those of doctors and their peers.4,5 Nurses mostly contribute voices toward the avoidance of negative outcomes, such as patient safety and error action.6 In fact, over two-thirds of doctors or nurses indicate having observed broken rules or medical errors, but almost always choose to not share their concerns to colleagues due to feelings of incompetence and poor teamwork.7 Thus, team-based self-esteem from a team or from one’s self plays an important role at enhancing communication, patients’ safety, and facilitating problem-solving.8,9
What drives this psychological process to promote voice behavior? Many research studies have identified the relationship between teamwork and trust that originates from a safe and stable requirement of human’s instinct, especially in females.10,11 Trust provides people with a mental resource to challenge unfavorable situations, maintain self-evaluation, and most importantly lead to individuals feeling good.12,13 However, there are some traditional values in Taiwan, like hierarchical relationships, collectivism, and Confucianism, making interpersonal relationships become more complex and highlighting the worth of group harmony, status difference, and collective capability in a work setting.14,15 The tendency toward power distance orientation, such as status difference and hierarchical relationships, may break up collaboration in such a profession that demands teamwork and should be considered as a research topic. Therefore, we propose our model for clarifying the trust-voice relationship in Figure 1.
 |
Figure 1 Hypothesized model in the present study. |
Theoretical background and hypotheses
The literature has conceptualized and operationalized the social identity theory in a wide variety of ways. There is a consensus about its overarching focus, which is how individuals make sense of themselves and other people in a social environment, such as an organization or company.16,17,18 The more individuals feel like members in such a group, the more likely for them to exhibit an attitude and behavior of belonging to that group.19 In a hospital, the professional identity of health care professionals may lead to breaking the trust between different departments, whether intra-group or inter-group, if it is stronger than organizational identity.20 This crack of trust causes competition, inter- or intra-group polarization, lower job satisfaction, or difficulties at improving patient care.21
To prove nurses’ organizational identity, voice behavior as a powerful predictor of belonging had been reported in a workplace with a high degree of teamwork demand.22 Voice behavior as a “seed corn” challenges the status quo with constructive suggestions or opinions for one’s own benefits, even in a dissenting situation.23,24 However, its potential importance, which has been verified as being related to teamwork and job performance,9,25 in the closed nursing profession has so far received little empirical attention.
Team trust and voice behavior
Team trust refers to “positive expectations about the intent and behaviors between among individual, other members and organization”.26 Greenwood and Van Buren III27 also suggested that trust in an organization should contain three components: predictability, benevolence, and integrity. Team trust explains the essence of employee engagement, including environment, perception, and the interactive process between individuals and organization.28 This is important to the nursing profession, because trust is crucial in the confidence of internal perceptions and external expectations about colleagues’ abilities and behaviors, which can increase nurses’ working state and promote teamwork.26,29 Thus, we suggest that experiencing a more trustful environment with co-workers, supervisors, or even organizations tends to improve individuals’ voice behavior and propose the following.
Hypothesis 1: Team trust is positively related to voice behavior.
Team-based self-esteem as a mediator
Having a social identity satisfies individuals’ simultaneous needs for inclusion and differentiation. In other words, people need to simultaneously fill the need to belong to a social group while maintaining their distinction from another group (p. 554).30 The above content means that the relationship between employees and organization is a give-and-take process between each other. Employees accept something (eg, organizational support) from the company and internalize what they feel or perceive that can be integrated or fused into self-esteem.31 Similarly, employees with a satisfying self-esteem show a low level of turnover intention.32
Self-esteem is “a term that reflects a person’s overall evaluation or appraisal of her or his own worth” (p. 21).33 According to the social identity theory, organizational-based self-esteem comprises one side of the identification process between individuals and an organization that allows employees to feel their contribution as being valued and can perceive satisfaction from their job.34,35 In contrast, employees who have a low level of team-based self-esteem are expected to have less motivation to perform voice behavior.15 This is why our research argues that team-based self-esteem mediates between team trust and voice behavior though the interaction of the giving process and proposes the following.
Hypothesis 2: Team-based self-esteem mediates the relationship between team trust and voice behavior.
Power distance orientation as a moderated mediator
We further propose that higher power distance orientation will strengthen the positive impact of team trust on voice behavior via team-based self-esteem. Power distance reflects that authority in institutions and organizations is distributed unequally, especially in the relationship between employees and their supervisor in a Chinese culture, which is collectivistic.36,37 Moreover, power distance orientation emphasizes a personal tendency to highlight capability, individual differences, hierarchical gap, a low-level relationship, and team support.38 We expect that power distance orientation moderates the relationship between team trust and team-based self-esteem (stage 1) as well as moderates the relationship between team-based self-esteem and voice behavior (stage 2).
Team trust leads individuals to perform organizational citizenship behavior,39 to generate more positive behaviors and fewer deviant behaviors 40 and to recognize the impact of these behaviors on others.41,42 Having high power distance orientation is particularly important, because team trust sensitizes individuals to team affirmation and provides a sense of belonging.43 Those who have a high level of power distance orientation find it difficult to develop close relationships with their leaders. Moreover, team trust more greatly affects their responses in such areas as satisfaction, a desire to stay with the team, as well as their team-based self-esteem. Taken together, we argue that team trust is associated with higher levels of team-based self-esteem when power distance orientation is high (stage 1). Consistent with what we predict about the relationship between team trust and team-based self-esteem, we also suggest a direct effect of team-based self-esteem on voice behavior.44 The social identity theory suggests that employees desire to maintain any identity that they highly value45,46 – that is to say, employees are motivated to present voice behavior if they want to maintain their self-esteem within the organization.47 Therefore, we argue that the relationship between team-based self-esteem and voice behavior is stronger under high levels of power distance orientation than under low levels (stage 2).
To complete our theoretical model, we further predict that team-based self-esteem mediates the relationship between the interactive effect of team trust and power distance orientation on voice behavior. We suggest that power distance orientation moderates the indirect effect of team trust on voice behavior through team-based self-esteem. In other words, we expect that the indirect effect of team trust on voice behavior via team-based self-esteem will be stronger when power distance orientation is high versus when it is low.
Hypothesis 3: Power distance orientation moderates the indirect effect of team trust on voice behavior via team-based self-esteem, such that the indirect effect is stronger among nurses who tend to exhibit higher power distance orientation and weaker or even non-existent among those who display lower power distance orientation.
Methods
Participants and procedures
This study is conducted under IRB Protocol #201806ES024 at National Taiwan University (Project Title: “Why do nurses leave? Moderated mediation model of career adaptability explores what medical institution can do to retain them?”). Before data collection, written informed consent was obtained from the participants, who took part in the study voluntarily. All employees who participated were ensured that their responses would be anonymous and confidential. In total, 258 Taiwanese registered nurses working in anesthesiology (41%), acute wards (25%), operating room (23%), and other departments were recruited via convenient sampling from a medical center in northern Taiwan. Nurses received envelopes including self-report questionnaires from the researchers, which were immediately sealed after interviews.
In the final sample (n=247; total response rate of 96%), the nurses were mostly female (96%), unmarried (58%), and university graduates (72%), with an average age of 35.57 years (standard deviation=9.37). On average, respondents reported having over 6 years of experience as a nurse, and they had also been in their current job beyond 6 years. Table 1 lists the descriptive statistics of these sociological variables.
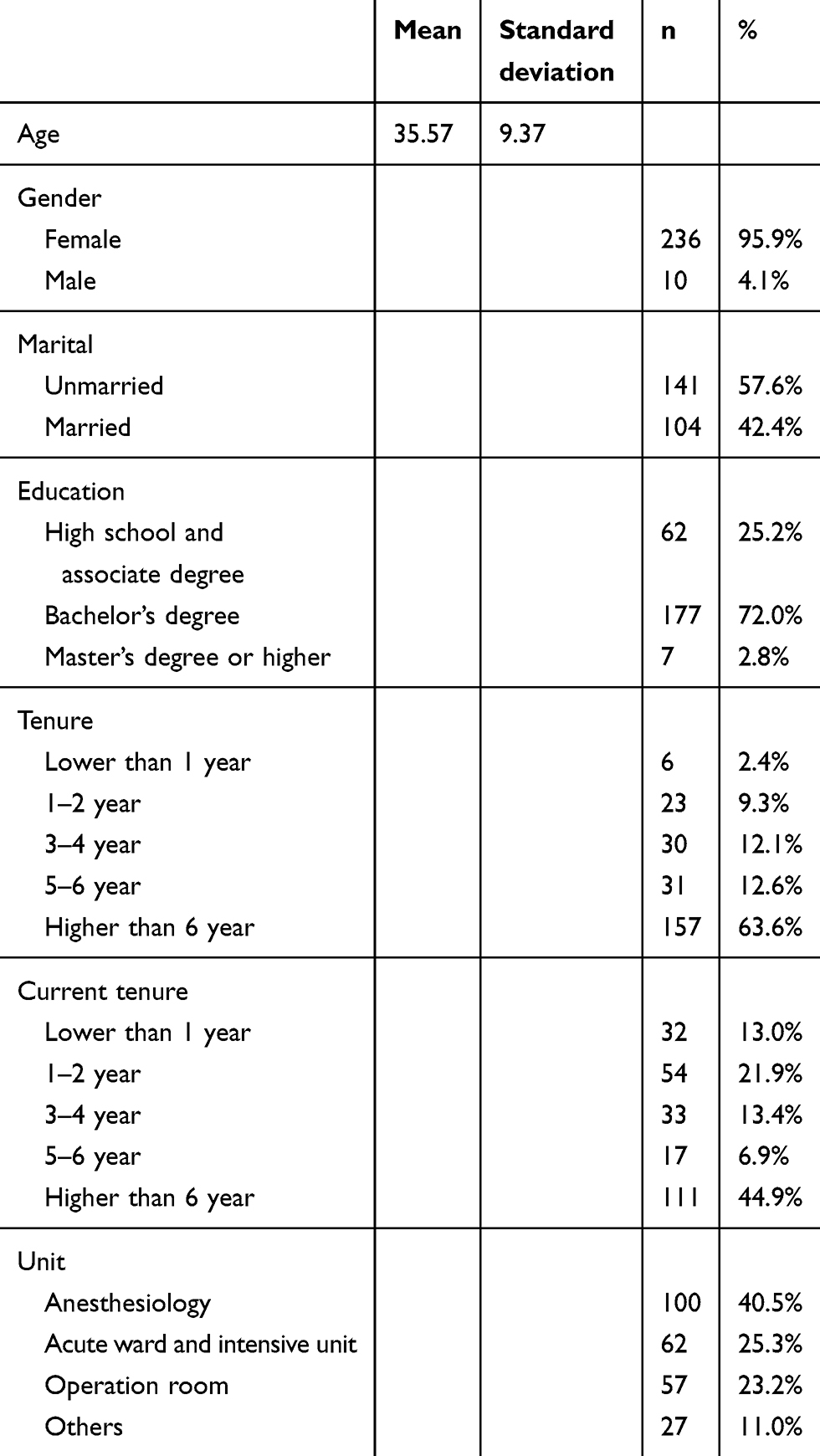 |
Table 1 Descriptive statistic of sociological variables |
Measures
The Chinese versions of scales were established for all measures following the commonly used translation–back-translation procedure.48 All measures have the same response scale, ranging from 1 (strongly disagree) to 6 (strongly agree). The measures presented in the following sections are the focus of this study’s research question and its associated analyses.
Team-based self-esteem
The Organizational-based Self-esteem Scale was assessed via a ten-item form of measurement developed by Pierce, Gardner, Cummings, and Dunham.49 The sample items include “I am important around here” and “There is faith in me around here.” Cronbach’s alpha for the scale is 0.91.
Team trust
The Team Trust Scale was assessed with a 12-item form of measurement developed by McAllister.50 One item is reversed scored in the analysis to indicate low scores equal high trust. The sample items include “Management can be trusted to make sensible decisions for the firm’s future” and “I can trust the people I work with to lend me a hand if I need it.” Cronbach’s alpha for the scale is 0.93.
Voice behavior
The Voice Behavior Scale was assessed with a six-item form of measurement developed by Linn and LePine.1 The sample items include “I develop and make recommendations to my supervisor concerning issues that affect my work” and “I keep well informed about issues at work where my opinion can be useful.” Cronbach’s alpha for the scale is 0.92.
Power orientation distance
The Power Orientation Distance Scale was assessed with a six-item form of measurement developed by Dorfman and Howell.51 The sample items include “Managers should make most decisions without consulting subordinates” and “Managers should avoid off-the-job social contacts with employees.” Cronbach’s alpha for the scale is 0.81.
Data analyses
To test confirmatory factor analysis on our hypothesized measurement model with four factors (ie, team-based self-esteem, team trust, voice behavior, and power orientation distance), we use structural equation modeling (SEM) and bootstrap in Mplus 8.052 to assess the direct, indirect, and moderating effects, because SEM is found to be superior to regression analysis.53 Factor loadings mean the correlation between an observed indicator and a target latent variable (eg, the relationship among a sample item like “Management can be trusted to make sensible decisions for the firm’s future” to the independent variable of “Team Trust”). Generally, factor loadings should be higher than 0.4 and can be used to estimate reliability, validity, model fit, and other coefficients in SEM.54 Following the procedures recommended by Fornell and Larcker,55 we take composite reliability to assess internal consistency reliability and the average of variance extracted to evaluate convergent validity. A commonly acceptable value for composite reliability is 0.7 or more, and for the average of variance extracted it is 0.5 or more.55,56 To support discriminant validity between each latent variable, the square root of the average of variance extracted estimates should be greater than the square of the correlations.54 In addition, Preacher and Hayes57 suggested that bootstrap results for indirect effects of independent variable on dependent variable through proposed mediator and accompanying percentile and bias-corrected 95% confidence intervals, and the estimate of an indirect effect is significantly by containing zero.
Results
Measurement model
Table 2 presents convergent validity, discriminant validity, and intercorrelations from the study. The four psychological variables (team trust, team-based self-esteem, voice behavior, and power distance orientation) are all significantto each other (all p<0.05), except for power distance orientation with team-based self-esteem (r=0.12, p=0.07). The range for the average of variance extracted estimates of psychological variables is between 0.52 and 0.72, providing support to convergent validity. The square root of the average of variance extracted estimates (voice behavior=0.85, team-based self-esteem=0.82, team trust=0.79, power distance orientation=0.72) is greater than the square of the correlations between voice behavior and team-based self-esteem (r2=0.54), between voice behavior and team trust (r2=0.59), between voice behavior and power distance orientation (r2=0.18), between team-based self-esteem and team trust (r2=0.48), between team-based self-esteem and power distance orientation (r2=0.11), and between team trust and power distance orientation (r2=0.16), providing support for discriminant validity of these measures. The range of standardized factor loadings for the indicators onto the latent variables is between 0.69 and 0.95, and all values are p<0.01. These results show that the four variables are distinct from each other.
 |
Table 2 Convergent validity, discriminant validity, and intercorrelations of psychological variables |
Structural model
The moderated mediation SEM includes an additional interaction term to the measurement model, power distance orientation×team trust, and results in an acceptable fit to the data:58 χ2 (147)=819.08 (p<0.01), χ2/df=2.79, CFI=0.88, TLI=0.87, RMSEA=0.08, SRMR=0.08, GFI=0.90, AGFI=0.79, and NFI 0.83.
Following the recommendations of Grace and Bollen,59 Table 3 presents the unstandardized regression coefficients. In support of Hypotheses 1 and 2, the results show that voice behavior is associated with team trust (β=0.66, p<0.01, CI [0.350, 0.994], with bias-correct CI [0.252, 0.624]); and the indirect effect of voice behavior on team trust via team-based self-esteem is significant (β=0.25, p<0.01, CI [0.106, 0.476], with bias-correct CI [0.079, 0.305]). In support of Hypothesis 3, the results show that power distance orientation moderates the indirect effect of the relationship in stage 1 (β=0.33, p=0.04), but not in stage 2 (β=0.03, p=0.73) – that is, as shown in Figure 2, the relationship between team-based self-esteem and team trust is stronger under high levels of power distance than under low levels.
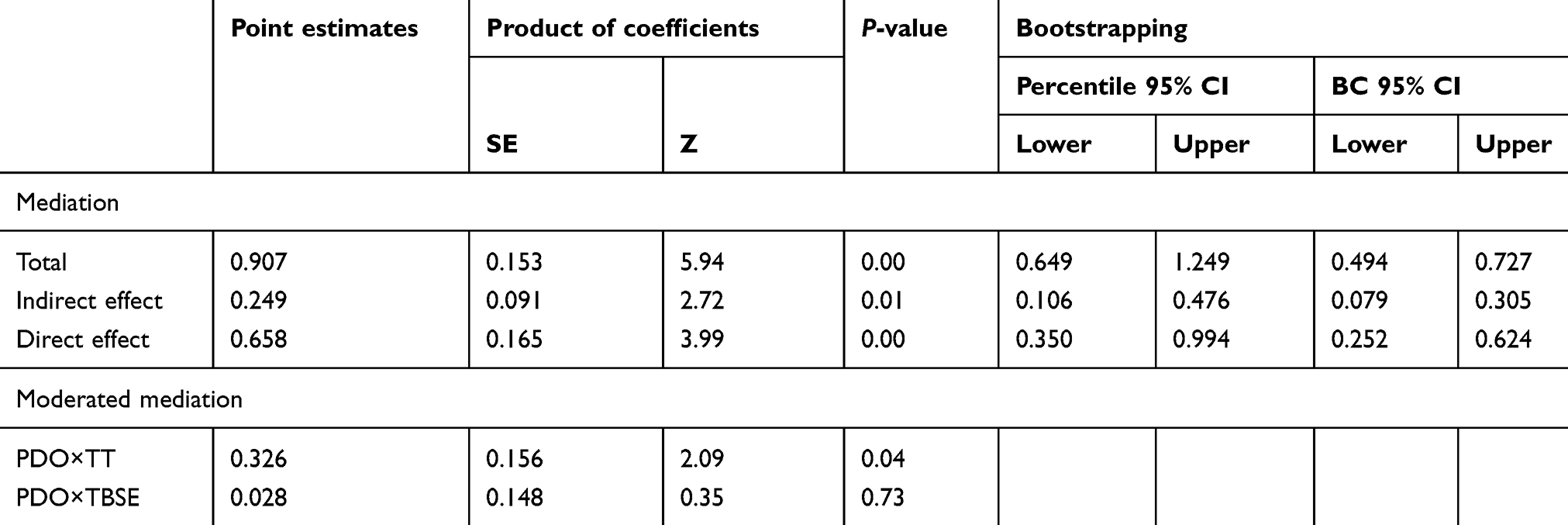 |
Table 3 Mediation of indirect effect of team-based self-esteem between voice behavior on team trust, and moderated mediation of power distance orientation |
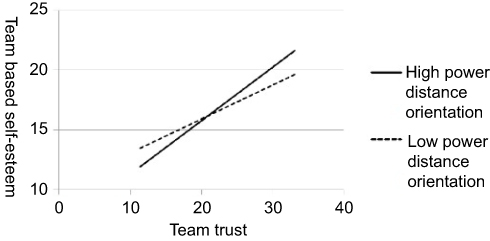 |
Figure 2 Moderation. |
Discussion
Theoretical and practical implications
The present study makes two contributions to the literature about what psychological mechanism works in the relationship between team trust and voice behavior. First, team-based self-esteem provides nurses with a mental resource for exchanging or expressing voice behavior to peers, managers, and organizations. Greenwald and Banaji60 pointed out some proofs of the features about self-esteem like automatic, intuitive process, unconscious, implicit, and affective. In other words, employees, especially nurses, take note of either a friendly or aggressive attitude or behavior from other colleagues and provide feedback to them through self-esteem.61 In the process of shaping self-esteem, social identity plays an important role to weaken the negative effect of peers or a manager’s aggressive attitude and behaviors, workplace phenomenon, and even organizational culture.62
Second, when employees experience either positive or negative feelings about job context and personal role in the workplace, motivation appears and various cognitive strategies, such as imitation, personal experience, self-regulation, and self-efficacy, push employees to adjust their behavior or belief toward fitting into their job environment.63,64 As such, because of the features of neglected interpersonal trust, attentive status difference, and focusing on self, nurses with vigorous power distance orientation can better confront cognitive dissonance in a profession that requires teamwork.65,66 While nurses must regulate their mentalities to suit the working ambience, the role of power distance orientation as moderator between social/interpersonal support (eg, perceived organization support, leader–member exchange) and work outcomes (eg, job performance, voice) is uncertain, due to past studies presenting differing results.67,68 We suggest that the path of power distance orientation must be clarified in future research due to its significance in Chinese culture.
Third, in a previous article, we neglect the effect from guanxi in the Taiwanese samples. Guanxi, known as a trust-based interpersonal relationship, takes on a traditional Chinese role and values trust, favors, dependence, and adaptation.69,70 Role-based guanxi, one of the guanxi’s rules, means that a relationship is built upon different positions or levels of power, such as supervisor and subordinate.15,71 In other words, when Taiwanese nurses have a higher level of power distance orientation, they may get more team-based identity from team trust. Nurses who have a higher level of power distance orientation are also more willing to depend on senior staff than nurses who have lower levels of power distance orientation. Dependence increases the whole quality of the group relationship, especially in a teamwork profession.72
Finally, the current study also extends the team trust literature into the domain of predicting voice behavior in more nuanced ways. Previous research has largely focused on the simple positive73 or negative74 association between team trust and voice behavior. Our results not only provide evidence of when team trust may translate into more voice behavior, but also show in certain situations (eg, higher power distance orientation) that team trust can be translated into more voice behavior via team-based self-esteem. Specifically, the results of our studies indicate that when power distance orientation is high, the indirect effect of team trust on voice behavior via team-based self-esteem is stronger. As such, we contribute to the literature by highlighting the complexity of this relationship.
In summary, this study suggests that managers can increase promoting behavior, such as voice behavior, to facilitate healthy team development by promoting nurses’ team identification. To grow this identification, managers can provide experience that focuses on the team and profession, like regular social gatherings and professional training sessions, emphasizing on the cooperative context of the job and building a reasonable reciprocity institution or rules on the job. Particularly, elevating team trust may be a greater influence factor of team-based self-esteem than a personal factor, such as personality trait and professional ability in such a cooperation-needed medical profession. We further find that power distance orientation, which may be sculpted from an ethnic culture of collectivism, career culture, and family, does not impair the identical process of team-based self-esteem on trust, but rather strengthens it. Overall, we infer that personal tendency and ability are not far more important than team factors in Chinese samples, such as team trust and social identity, and suggest that the variable of guanxi should be controlled in future research.
Limitations
This study has several limitations. First, we use a cross-sectional design to examine the relationship among research variables herein. Because the process of identification may be dynamic, we cannot certainly discriminate that power distance orientation is a personality trait or a state affected through the environment and must explore the change effect of the present model over time, especially in the sample of nurses who are fresh graduates or underwent a job transfer. Second, we use convenience sampling to collect participants from just one medical center in northern Taiwan. The results may not represent all Taiwanese nurses, but rather perhaps just those in that medical center. In light of this, future researchers should replicate this study with different groups using hierarchical linear modeling to clearly understand the relationship between these psychological variables. Third, the simplified model provides a clear, obvious, and evident construct, which makes it easier to conduct the research, but restricts further cognition with the present model, such that team trust can be composed of affect-based trust and cognition-based trust from peers, managers, and organizations.50 Fourth, we conduct this study in Taiwan, and because of its national health insurance system, medical personnel may present a cultural effect – for example, working values, professional identity, management styles, etc. Finally, by neglecting the guanxi literature in this article, the effect of power distance orientation is still unclear. Moreover, the interaction between power distance orientation and guanxi can be considered in Chinese samples through future studies.
Conclusion
Our results indicate when nurses increase their own team-based self-esteem that a predictor perceives more team trust, which improves their motivation or confidence to engage in voice behavior that could be risky behavior in their group. This association is stronger when the nurses have higher power distance orientation. Our study thus highlights the usefulness of continued research into how nurses display promoting behavior through team-based self-esteem with a distinct level of power distance orientation under differing sources of team trust from peers, managers, and organizations, as well as how nurses, especially fresh graduates and those who underwent a job transfer, shape their social identity through psychological factors in the sense-making process.
Acknowledgments
The authors would like to thank all nurses in Tri-Service General Hospital, National Taiwan University Hospital, Shin Kong Wu Ho-Su Memorial Hospital, and Chang Gung Memorial Hospital for their support in data collection. Financial support from the Ministry of Science and Technology (MOST 107-2410-H-130-054 -SSS) is greatly appreciated.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Linn VD, LePine JA. Helping and voice extra-role behaviors: evidence of construct and predictive validity. Acad Manage J. 1998;41(1):108–119.
2. Liang J, Farh CIC, Farh J. Psychological antecedents of promotive and prohibitive voice: a two-wave examination. Acad Manage J. 2012;55(1):71–92. doi:10.5465/amj.2010.0176
3. Linn VD, Ang S, Botero IC. Conceptualizing employee silence and employee voice as multidimensional constructs. J Manage Stud. 2003;40(6):1359–1392. doi:10.1111/1467-6486.00384
4. Curtin LL. One nurse, two nurse … red nurse, blue nurse. Nurs Manage. 1998;29(4):5–6.
5. Gardner JK, Thomas-Hawkins C, Fogg L, Latham CE. The relationships between nurses’ perceptions of the hemodialysis unit work environment and nurse turnover, patient satisfaction, and hospitalizations. Nephrol Nurs J. 2007;34(3):
6. Carney BT, West P, Neily J, Mills PD, Bagian JP. Differences in nurse and surgeon perceptions of teamwork: implications for use of a briefing checklist in the OR. Aorn J. 2010;91(6):722–729. doi:10.1016/j.aorn.2009.11.066
7. Maxfield D, Grenny J, McMillan R, Patterson K, Switzler A. Silence Kills: The Seven Crucial Conversations for Healthcare. Alisa Viejo, CA: Vital Smarts and American Association of Critical-Care Nurses; 2007.
8. Breitbach AP, Reeves S, Fletcher SN. Health care as a team sport?-Studying athletics to improve interprofessional collaboration. Sports. 2017;5(3):62. doi:10.3390/sports5030062
9. Eppich W. “Speaking up” for patient safety in the pediatric emergency department. Clin Pediatr Emerg Med. 2015;16(2):83–89. doi:10.1016/j.cpem.2015.04.010
10. Wrzesniewski A, Dutton J, Debebe G. Interpersonal sensemaking and the meaning of work. Res Organizational Behav. 2003;25:93–135. doi:10.1016/S0191-3085(03)25003-6
11. Krueger L, Ernstmeyer K, Kirking E. Impact of interprofessional simulation on nursing students’ attitudes toward teamwork and collaboration. J Nurs Educ. 2017;56(6):321–327. doi:10.3928/01484834-20170518-02
12. Aly NAEM, El-Shanawany S. Nurses’ organizational trust: its impacts on nurses’ attitudes towards change in critical care and toxicology units. Int J Inf Bus Manage. 2016;8(4):205–223.
13. Critchley D, Edwards C, Fallon R. The importance of good teamwork. Nurs Manage. 2007;14(7):8–12. doi:10.7748/nm.14.7.8.s12
14. Kang H, Chang B. Examining culture’s impact on the learning behaviors of international students from Confucius culture studying in western online learning context. J Int Students. 2016;6(3):779–797.
15. Gong B, He X, Hsu H. Guanxi and trust in strategic alliances. J Manage Hist. 2013;19(3):362–376. doi:10.1108/JMH-08-2012-0054
16. Joshi V, Goyal KA. An empirical case study on employees’ satisfaction after merger in selected bank. Productivity. 2015;55(4):327–337.
17. Schmidts T, Shepherd D. Social identity and family business: exploring family social capital. J Family Bus Manage. 2015;5(2):157–181. doi:10.1108/JFBM-04-2015-0018
18. Karakaya F, Yannopoulos P, Kefalaki M. Factors impacting the decision to attend soccer games: an exploratory study. Sport Bus Manage. 2016;6(3):320–340. doi:10.1108/SBM-05-2014-0024
19. Daan VK, Els C M van S. Foci and correlates of organizational identification. J Occup Organ Psychol. 2000;73:137–147. doi:10.1348/096317900166949
20. van Os A, de Gilder D, van Dyck C, Groenewegen P. Responses to professional identity threat. J Health Organ Manag. 2015;29(7):1011–1028. doi:10.1108/JHOM-12-2013-0273
21. Topa G, Guglielmi D, Depolo M. Mentoring and group identification as antecedents of satisfaction and health among nurses: what role do bullying experiences play? Nurse Educ Today. 2014;34(4):507–512. doi:10.1016/j.nedt.2013.07.006
22. Schwappach DLB, Gehring K. Trade-offs between voice and silence: a qualitative exploration of oncology staff’s decisions to speak up about safety concerns. BMC Health Serv Res. 2014;14:303. doi:10.1186/1472-6963-14-303
23. Wu W, Tang F, Dong X, Liu C. Different identifications cause different types of voice: a role identity approach to the relations between organizational socialization and voice. Asia Pac J Manage. 2015;32(1):251–287. doi:10.1007/s10490-014-9384-x
24. Fuller JB, Barnett T, Hester K, Relyea C, Frey L. An exploratory examination of voice behavior from an impression management perspective. J Managerial Issues. 2007;19(1):
25. Shih H, Wijaya NHS. Team-member exchange, voice behavior, and creative work involvement. Int J Manpow. 2017;38(3):417–431. doi:10.1108/IJM-09-2015-0139
26. Huff L, Lane K. Levels of organizational trust in individualist versus collectivist societies: a seven-nation study. Organization Sc. 2003;14(1):81–90. doi:10.1287/orsc.14.1.81.12807
27. Greenwood M, Van Buren HJ
28. Hough C, Green K, Plumlee G. Impact of ethics environment and organizational trust on employee engagement. J Legal Ethical Regul Issues. 2015;18(3):45–62.
29. Altuntas S, Baykal U. Relationship between nurses’ organizational trust levels and their organizational citizenship behaviors. J Nurs Scholarship. 2010;42(2):186–194. doi:10.1111/j.1547-5069.2010.01347.x
30. Shinnar RS. Coping with negative social identity: the case of mexican immigrants. J Soc Psychol. 2008;148(5):553–575. doi:10.3200/SOCP.148.5.553-576
31. Ghosh SK. Linking perceived organizational support to organizational identification: role of organization based self-esteem. Contemp Manage Res. 2016;12(2):225–244. doi:10.7903/cmr.15765
32. Norman SM, Gardner DG, Pierce JL. Leader Roles, Organization-Based Self-Esteem, and Employee Outcomes. Leadership & Organization Development Journal. 2015;36(3):253–270.
33. Sharma S, Agarwala S. Self-esteem and collective self-esteem as predictors of depression. J Behav Sci. 2014;24(1):21–28.
34. Hunter JA. Self-esteem and in-group bias among members of a religious social category. J Soc Psychol. 2001;141(3):401–411. doi:10.1080/00224540109600561
35. Khattak K, Inderyas S, Hassan Z, Raza AA. Relationship between perceived organization support and affective commitment of hospital nurses in Pakistan: a meditational model. Int J Innovation Appl Stud. 2014;7(4):1465–1474.
36. Polsa P, Fuxiang W, Sääksjärvi M, Shuyuan P. Cultural values and health service quality in china. Int J Health Care Qual Assur. 2013;26(1):55–73. doi:10.1108/09526861311288640
37. Zhao C, Liu Y, Gao Z. An identification perspective of servant leadership’s effects. J Managerial Psychol. 2016;31(5):898–913. doi:10.1108/JMP-08-2014-0250
38. Hon AHY, Yang J, Lu L. A cross-level study of procedural justice perceptions. J Managerial Psychol. 2011;26(8):700–715. doi:10.1108/02683941111181789
39. Li A, Thatcher SMB. Understanding the effects of self and teammate OCB congruence and incongruence. J Bus Psychol. 2015;30(4):641–655. doi:10.1007/s10869-014-9387-0
40. Kim M, Beehr Terry A. Organization-based self-esteem and meaningful work mediate effects of empowering leadership on employee behaviors and well-being. J Leadersh Organizational Stud. 2018;25(4):385–398. doi:10.1177/1548051818762337
41. Ogungbamila B. Positive employee behaviors and occupational burnout in healthcare workers: moderating roles of work engagement. Indian J Positive Psychol. 2018;9(3):404–412.
42. Haider S, Carmen de PH, Munir A. A three-wave time-lagged study of mediation between positive feedback and organizational citizenship behavior: the role of organization-based self-esteem. Psychol Res Behav Manag. 2019;12:241–253. doi:10.2147/PRBM.S192515
43. Pietri ES, Hennes EP, Dovidio JF, et al. Addressing unintended consequences of gender diversity interventions on Women’s sense of belonging in STEM. Sex Roles. 2019;80(9–10):527–547. doi:10.1007/s11199-018-0952-2
44. Wang L, Huang J, Chu X, Wang X. A multilevel study on antecedents of manager voice in chinese context. Chin Manage Stud. 2010;4(3):212–230. doi:10.1108/17506141011074110
45. Stryker S, Burke PJ. The past, present, and future of an identity theory. Soc Psychol Q. 2000;63:284–297. doi:10.2307/2695840
46. Stets JE, Burke PJ. Identity theory and social identity theory. Soc Psychol Q. 2000;63:224–237. doi:10.2307/2695870
47. Duan J, Bao C, Huang C, Brinsfield CT. Authoritarian leadership and employee silence in china. J Manage Organ. 2018;24(1):62–80. doi:10.1017/jmo.2016.61
48. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1:185–216. doi:10.1177/135910457000100301
49. Pierce JL, Gardner DG, Cummings LL, Dunham RB. Organization-based self-esteem: Construct definition, measu. Academy of Management Journal. 1989;32(3):622–648.
50. McAllister DJ. Affect- and cognition-based trust as foundations for interpe. Acad Manage J. 1995;38(1):24–59.
51. Dorfman PW, Howell JP. Dimensions of national culture and effective leadership in patterns: hofstede revisited. In: McGoun EG, editor. Advances in International Comparative Management. Greenwich, CT: JAI Press; 1988:127–150.
52. Muthen LK, Muthen BO, editors. MPlus user’s guide. 4th ed. Los Angeles, CA: Muthen and Muthen; 2017.
53. Hayes A. Beyond Baron and Kenny: statistical mediation analysis in the new millennium. Commun Monogr. 2009;76:408–420. doi:10.1080/03637750903310360
54. Hair JF, Black WC, Babin BJ, Anderson RE, Tatham RL. Multivariate Data Analysis.
55. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Marketing Res. 1981;18(1):39–50. doi:10.1177/002224378101800104
56. Bagozzi R, Yi Y. On the evaluation of structural equation models. J Acad Marketing Sci. 1988;16(1):74–94. doi:10.1007/BF02723327
57. Preacher AJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40:879–891.
58. Hooper D, Coughlan J, Mullen MR. Structural Equation Modelling: Guidelines for Determining Model Fit. The Electronic Journal of Business Research Methods. 2008;6:53–60.
59. Grace JB, Bollen KA. Interpreting the results from multiple regression and structural equation models. Bull Ecol Soc Am. 2005;86:283–295. doi:10.1890/0012-9623(2005)86[283:ITRFMR]2.0.CO;2
60. Greenwald AG, Banaji MR. Implicit social cognition: attitudes, self-esteem, and stereotypes. Psychol Rev. 1995;102(1):4–27.
61. Kundu SC, Rani S. Human resources’ self-esteem across gender and categories: a study. Ind Manage Data Sys. 2007;107(9):1366–1390. doi:10.1108/02635570710834018
62. Kim E, Glomb TM. Victimization of high performers: the roles of envy and work group identification. J Appl Psychol. 2014;99(4):619–634. doi:10.1037/a0035789
63. Vito AG, Schafer BP, Higgins GE, Marcum CD, Ricketts ML. Juvenile hallucinogen use: what do multiple theories say about it? Am J Criminal Justice. 2015;40(1):116–128. doi:10.1007/s12103-013-9233-3
64. George JM, Brief AP. Motivational agendas in the workplace: the effects of feelings on focus of attention and work motivation. Res Organizational Behav. 1996;18:75–110.
65. Pronovost PJ, Berenholtz SM, Goeschel C, et al. Improving patient safety in intensive care units in michigan. J Crit Care. 2008;23(2):207–221. doi:10.1016/j.jcrc.2007.09.002
66. Havyer RD, Wingo MT, Comfere NI, Nelson DR, Halvorsen AJ, Reed DA. Teamwork assessment in internal medicine: a systematic review of validity evidence and outcomes. J Gen Intern Med. 2014;29(6):894–910. doi:10.1007/s11606-013-2686-8
67. Farh J, Hackett RD, Liang J. Individual-level cultural values as moderators of perceived organizational support-employee outcome relationships in China: comparing the effects of power distance and traditionality. Acad Manage J. 2007;50(3):715–729. doi:10.5465/amj.2007.25530866
68. Costigan RD, Instinga RC, Berman JJ, Kranas G, Kureshov VA. A cross-cultural study of coworker trust. Int J Commerce Manage. 2011;21(2):103–121. doi:10.1108/10569211111144328
69. Crombie B. Is Guanxi social capital? ISM J Int Bus. 2011;1:2–25.
70. Wang C. Guanxi vs. relationship marketing: exploring underlying differences. Ind Marketing Manage. 2007;36(1):81–86. doi:10.1016/j.indmarman.2005.08.002
71. Jiang D, Cheng B. Affect- and role-based loyalty to supervisors in chinese organizations. Asian J Social Psychol. 2008;11(3):214–221. doi:10.1111/ajsp.2008.11.issue-3
72. Wong YH. The dynamics of guanxi in China. Singapore Manage Rev. 1998;20(2):25–42.
73. Allen JA, Yoerger MA, Lehmann-Willenbrock N, Jones J. Would you please stop that!?: the relationship between counterproductive meeting behaviors, employee voice, and trust. J Manage Dev. 2015;34(10):1272–1287. doi:10.1108/JMD-02-2015-0032
74. Qamar B, Bashir M, Saleem S, Saqib S. How bad can voice aversion be? An empirical investigation of the joint influences of own and coworkers’ experience of voice aversion: a moderation mediation model. Pak J Social Issues. 2016;7:122–141.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.