Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Concurrent Steatotic Liver Disease and Prognosis After Curative Resection of Hepatocellular Carcinoma
Authors Liu YW ![]() , Wang CC, Liu YW, Li WF, Yen YH, Kuo YH
, Wang CC, Liu YW, Li WF, Yen YH, Kuo YH ![]() , Wang HM, Tsai MC
, Wang HM, Tsai MC
Received 29 October 2025
Accepted for publication 22 January 2026
Published 10 February 2026 Volume 2026:13 577506
DOI https://doi.org/10.2147/JHC.S577506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Imam Waked
Yan-Wen Liu,1 Chih-Chi Wang,2 Yueh-Wei Liu,2 Wei-Feng Li,2 Yi-Hao Yen,1 Yuan-Hung Kuo,1 Hsin-Ming Wang,3 Ming-Chao Tsai1,3,4
1Division of Hepato-Gastroenterology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 2Division of General Surgery, Department of Surgery, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan; 3Kaohsiung Municipal Fong Shan Hospital - Under the Management of Chang Gung Medical Foundation, Kaohsiung, Taiwan; 4School of Medicine, College of Medicine, National Sun Yat-Sen University, Kaohsiung, Taiwan
Correspondence: Ming-Chao Tsai, Kaohsiung Municipal Fong Shan Hospital - Under the management of Chang Gung Medical Foundation, 42, 42-1, Jingwu Road, Fongshan District, Kaohsiung City, Taiwan, Tel +886-7-741-8151, ext. 3356, Fax +886-7-732-2402, Email [email protected]
Purpose: Steatotic liver disease (SLD), linked to obesity and metabolic disorders, is a growing health burden. While implicated in hepatocarcinogenesis, its prognostic role in resectable hepatocellular carcinoma (HCC) is unclear, with conflicting reports and uncertain interaction with viral hepatitis. We aimed to evaluate the impact of concurrent SLD on recurrence-free (RFS) and overall survival (OS) in HCC, and to explore differences across etiologic subgroups.
Patients and methods: In this retrospective cohort study, we analyzed 2123 HCC patients who underwent curative hepatic resection between 2009 and 2023. Patients were stratified by histologically defined SLD (≥ 5% steatosis in non-tumorous liver). Primary outcomes were RFS and OS. Subgroup analyses were performed by HCC etiology.
Results: SLD was present in 52.2% of patients and associated with favorable metabolic and tumor profiles. While RFS did not differ between groups (P = 0.942), patients with SLD had significantly improved OS (P = 0.001). On multivariate analysis, SLD remained an independent protective factor for mortality (HR 0.76, P = 0.005). The survival benefit was most evident in chronic hepatitis B (CHB) patients (HR 0.71, P = 0.011), and SLD was associated with significantly lower risks of both liver-related mortality (P=0.006) and non–liver-related mortality (P=0.001).
Conclusion: Concurrent SLD was associated with improved overall survival after curative resection for HCC, particularly among patients with CHB. These findings suggest that SLD may represent a clinically relevant prognostic factor in resectable HCC; however, the observed association should be regarded as hypothesis-generating and requires prospective validation.
Keywords: hepatocellular carcinoma, steatotic liver disease, overall survival, hepatic resection, chronic hepatitis
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer and remains a leading cause of cancer-related death globally.1,2 While chronic infections with hepatitis B (CHB) and C (CHC) have historically been the main causes, other risk factors such as heavy alcohol intake, obesity, diabetes, and smoking are also implicated.2 Despite the predominance of viral etiologies, a growing proportion of HCC cases occur in patients seronegative for both HBV and HCV, referred to as non-B, non-C (NBNC) hepatitis. With the success of HBV vaccination and antiviral therapy, virus-related HCC is declining, whereas non-viral cases, particularly NBNC-HCC, are on the rise.3–5 In this context, steatotic liver disease (SLD) has emerged as a key contributor to hepatocarcinogenesis, driven by the global increase in metabolic disorders such as obesity and type 2 diabetes.4,6
In parallel, the global burden of SLD has markedly increased, affecting an estimated 1.27 billion people in 2021,7 largely due to rising rates of obesity and diabetes.8 Reflecting this shift, the term metabolic dysfunction-associated steatotic liver disease (MASLD) was proposed in 2023 to replace NAFLD, highlighting its association with cardiometabolic disease.9 Increasing evidence links SLD not only to liver fibrosis and cirrhosis but also to HCC development.10,11 Importantly, recent data suggest that SLD may also impact clinical outcomes in patients with HCC, warranting its inclusion in prognostic assessments.12
The prognostic significance of concurrent SLD in HCC patients undergoing curative hepatectomy remains controversial. Some studies have reported that patients with NAFLD-related HCC may exhibit favorable long-term survival despite higher surgical morbidity and metabolic comorbidities.13 In contrast, others have found that hepatic steatosis in the background liver is independently associated with poorer overall survival after resection, particularly in non-cirrhotic patients.14 These discrepant findings likely reflect differences in patient selection, disease stage, and histological definitions of steatosis. In addition, heterogeneity in underlying liver disease etiology, including the prevalence of viral hepatitis (HBV/HCV), access to antiviral therapy, and the burden of metabolic comorbidities such as diabetes and hypertension, may further contribute to the inconsistent prognostic effects reported across studies.
Given these potential sources of heterogeneity, it remains important to determine whether the prognostic impact of SLD varies according to the underlying liver disease etiology, including viral and non-viral causes. However, few studies have systematically examined this issue with respect to long-term outcomes. Therefore, in this study, we investigated the association between concurrent SLD and oncologic outcomes, including recurrence-free survival (RFS) and overall survival (OS), in HCC patients undergoing curative surgical resection. We further conducted etiology-stratified analyses to assess whether the prognostic relevance of SLD differs between viral- and non-viral–related HCC.
Methods
Study Design and Ethics
This retrospective cohort study was conducted at Kaohsiung Chang Gung Memorial Hospital (KCGMH), a medical center in Southern Taiwan. The study protocol was approved by the Institutional Review Board (IRB) of KCGMH (approval number: 202500957B0). All patients who underwent curative hepatic resection for hepatocellular carcinoma between January 2009 and December 2023 were included. Given the retrospective design and use of de-identified data, the requirement for informed consent was waived by the IRB.
Study Population
We retrospectively identified patients who underwent hepatic resection for HCC between January 2009 and December 2023. The inclusion criteria for this study were: (1) histologically confirmed HCC; (2) curative hepatic resection (R0) with no evidence of macrovascular invasion or extrahepatic metastasis. The exclusion criteria for this study were: (1) received any treatment prior to surgery; (2) underwent liver transplantation; (3) lacked pathological assessment of hepatic steatosis; (4) had less than 3 months of postoperative follow-up. A flowchart illustrating the process of patient selection is shown in Figure 1.
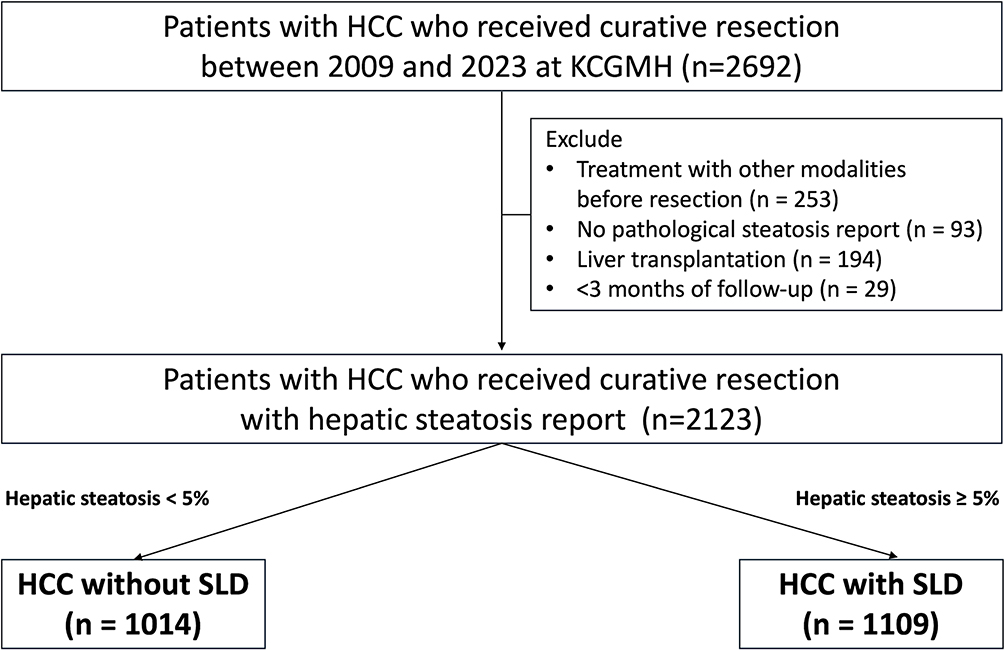 |
Figure 1 Patient selection flow diagram of the study cohort. Among 2123 patients who underwent curative hepatic resection for hepatocellular carcinoma (HCC) between 2009 and 2023, 1109 (52.2%) had concurrent steatotic liver disease (SLD). Numbers shown in bold represent the number and proportion of patients at each step of the selection process. |
Definition of Steatotic Liver Disease
Patients were categorized into two groups based on the presence or absence of concurrent SLD. SLD was defined histologically as hepatic steatosis involving ≥5% of hepatocytes in the non-tumorous portion of the resected liver specimen.15,16 The presence and degree of steatosis were determined based on formal pathological reports from our institution’s Department of Pathology. These assessments were performed using routine hematoxylin and eosin (H&E) staining by board-certified pathologists as part of a standardized clinical protocol. Importantly, these pathological evaluations were conducted at the time of surgery, effectively blinding the pathologists to the patients’ long-term postoperative survival and recurrence outcomes.
Clinical and Pathological Variables
Baseline data included age, sex, body mass index (BMI), diabetes mellitus, hypertension, and alcohol consumption. Viral etiology was classified as CHB, CHC, or NBNC. Liver function was assessed using aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, serum albumin, platelet count, Albumin–Bilirubin (ALBI) grade, and Child–Pugh score. Due to the retrospective nature and the long-term inclusion period of this cohort, quantitative virological data such as baseline HBV DNA levels and detailed longitudinal antiviral treatment records were not available for all patients and were thus not included in the multivariate models. Renal function was evaluated by estimated glomerular filtration rate (eGFR) and serum creatinine. Tumor characteristics included alpha-fetoprotein (AFP) level, tumor size, number, histological grade, presence of microvascular invasion (MVI), satellite nodules, and Barcelona Clinic Liver Cancer (BCLC) stage. Pathological evaluation of the non-tumorous liver included the Ishak fibrosis score and presence of cirrhosis. All patients underwent curative hepatic resection and were followed regularly for recurrence and survival outcomes based on institutional surveillance protocols.
Outcomes and Statistical Analysis
Study Outcomes
The primary outcomes were recurrence-free survival (RFS) and overall survival (OS). RFS was defined as the interval from the date of hepatic resection to the first radiologically or pathologically confirmed recurrence of HCC, whereas OS was defined as the time from surgery to death from any cause. Secondary outcomes included liver-related and non–liver-related mortality, OS according to the severity of hepatic steatosis (HS), and subgroup analyses of RFS and OS based on HCC etiology, including CHB, CHC, and NBNC infection. Liver-related mortality was defined as death attributable to HCC progression or complications of chronic liver disease (eg, hepatic failure or variceal bleeding), whereas non–liver-related mortality referred to deaths from other causes, such as cardiovascular events, infections, or extrahepatic malignancies. Classification was based on the proximate cause of death, regardless of underlying metabolic comorbidities.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics software (version 30; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means with standard deviations and compared using the Student’s t-test or the Mann–Whitney U-test, depending on distribution. Categorical variables were analyzed using the chi-square test. Survival curves for RFS and OS were generated using the Kaplan–Meier method and compared with the Log rank test. Prognostic factors were assessed using Cox proportional hazards regression models. To minimize potential confounding, we included all significant factors from the univariate analysis along with clinically established prognostic variables (eg, age, cirrhosis, and tumor stage) as covariates. Variables with a p-value < 0.01 in univariate analysis were included in the multivariate analysis. A two-sided p-value < 0.05 was considered statistically significant.
Results
Patient Enrollment and Baseline Characteristics
Between January 2009 and December 2023, a total of 2123 patients with hepatocellular carcinoma who underwent curative hepatic resection at KCGMH were included after applying the exclusion criteria (shown Figure 1). Among them, 1109 (52.2%) had concurrent SLD. Compared with those without SLD, patients with SLD were generally younger and had higher body mass index and a greater prevalence of metabolic comorbidities. Chronic hepatitis B and non-B, non-C etiologies were more common in the SLD group, whereas chronic hepatitis C was less frequent. In terms of liver function and tumor burden, the SLD group exhibited more favorable profiles, including better hepatic function, smaller tumor size, and lower rates of microvascular invasion. A detailed comparison of baseline characteristics is shown in Table 1.
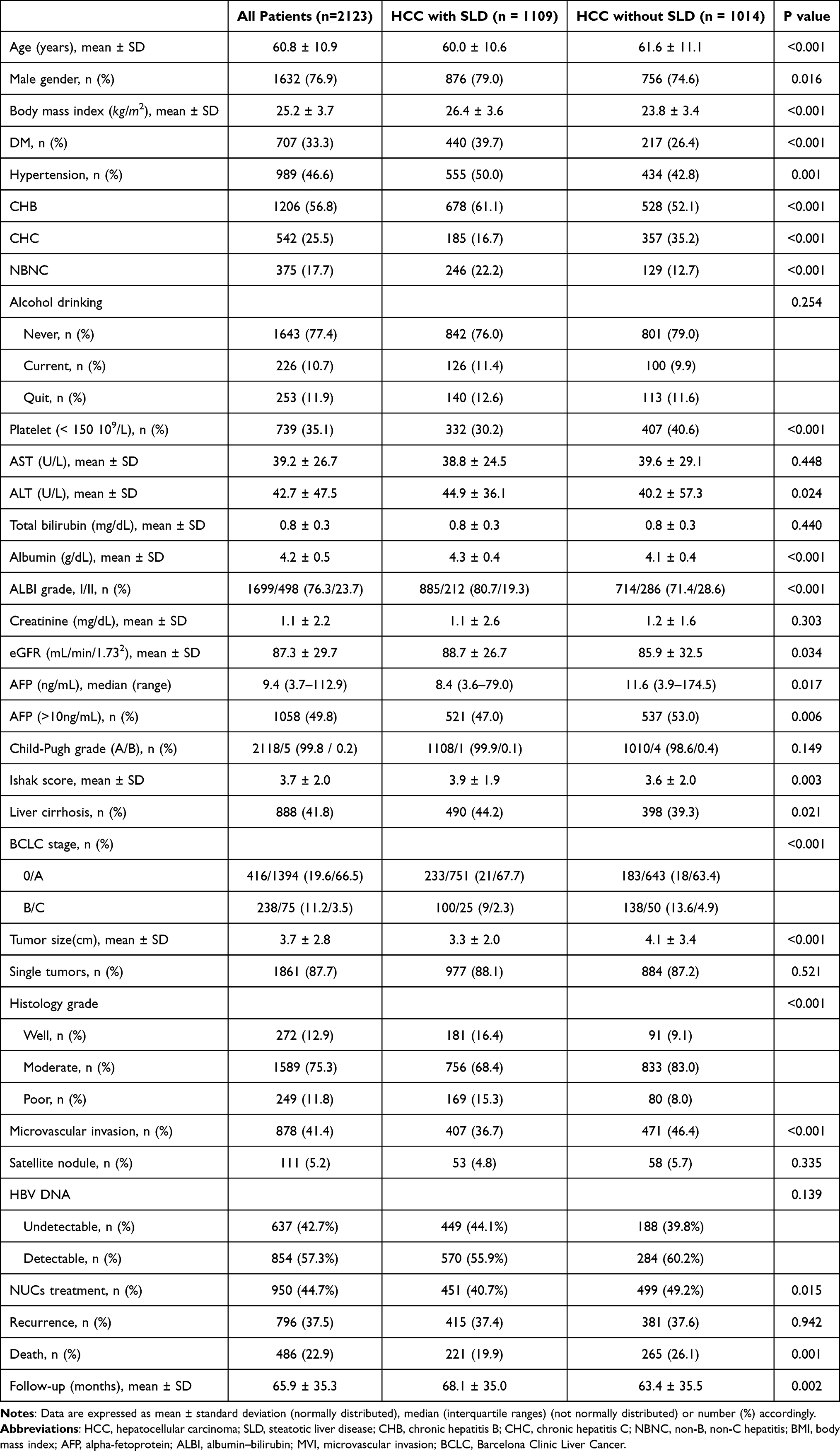 |
Table 1 Characteristics of the 2123 HCC with or without SLD Who Underwent Curative Resection |
Impact of Concurrent Steatotic Liver Disease on Recurrence-Free and Overall Survival
During a median follow-up period of 66 months, a total of 796 patients (37.5%) developed HCC recurrence, and 486 patients (22.9%) died. Patients with concurrent SLD exhibited significantly lower all-cause mortality compared with those without SLD (19.9% vs 26.1%, P = 0.001), whereas the recurrence rate was comparable between groups (37.4% vs 37.6%, P = 0.942). Kaplan–Meier analysis revealed that SLD was associated with significantly improved overall survival (P = 0.001, shown in Figure 2B), but no significant difference in recurrence-free survival (P = 0.218, shown in Figure 2A).
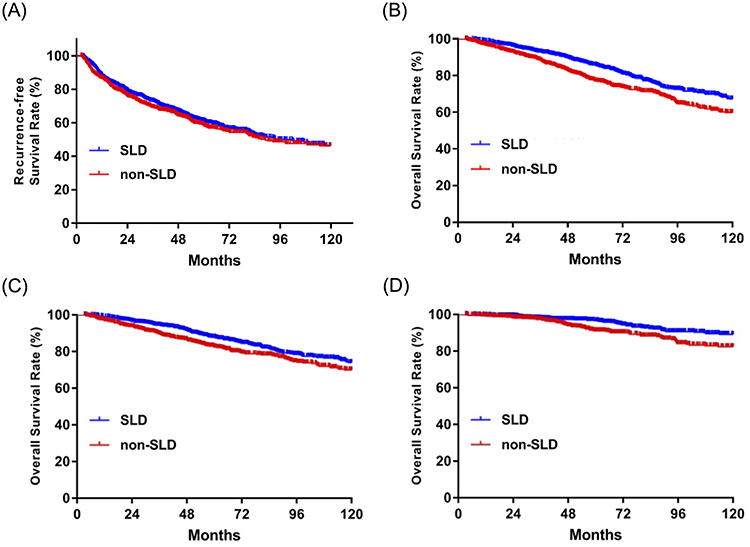 |
Figure 2 Kaplan–Meier curves comparing patients with and without SLD. (A) Recurrence-free survival (RFS) (n=1109 for SLD group and n=1014 for non-SLD group; P=0.218), (B) overall survival (OS) (P<0.001), (C) liver-related mortality (P=0.006), and (D) non–liver-related mortality (P=0.001). Abbreviations: SLD, steatotic liver disease; RFS, recurrence-free survival; OS, overall survival. |
In terms of cause-specific mortality, patients with SLD demonstrated significantly lower rates of both liver-related mortality (P = 0.006, shown in Figure 2C) and non–liver-related mortality (P = 0.001, shown in Figure 2D) compared to those without SLD.
Survival Analysis Stratified by Hepatic Steatosis Severity
Analysis based on hepatic steatosis severity further revealed that patients with 5–30% and >30% hepatic steatosis had similar overall survival, and both groups exhibited significantly better outcomes than those with steatosis <5% (shown in Figure 3).
 |
Figure 3 Overall survival according to severity of hepatic steatosis (HS). Patients were categorized into three groups: HS <5% (n=1011), HS 5–30% (n=800), and HS >30% (n=258). Analysis revealed that patients with 5–30% and >30% HS had similar overall survival, and both groups exhibited significantly better outcomes than those with HS <5% (P<0.001). Abbreviation: HS, hepatic steatosis |
Factors Associated with HCC Recurrence
In univariate Cox regression analysis, several clinical and tumor-related factors were significantly associated with increased risk of HCC recurrence. These included age ≥65 years, diabetes mellitus, thrombocytopenia (platelet <150 ×109/L), ALBI grade II, AFP ≥10 ng/mL, presence of liver cirrhosis, BCLC stage B or C, tumor size ≥3 cm, multiple tumors, moderate to poor tumor differentiation, presence of MVI, and satellite nodules (all P < 0.01). The presence of SLD was not significantly associated with recurrence risk (P = 0.218).
Variables with P < 0.01 in univariate analysis were included in the multivariate model (shown in Table 2). Independent predictors of recurrence included age ≥65 years (HR 1.32, 95% CI: 1.14–1.53, P < 0.001), platelet <150 ×109/L (HR 1.18, 95% CI: 1.01–1.38, P = 0.043), ALBI grade II (HR 1.33, 95% CI: 1.14–1.56, P < 0.001), AFP ≥10 ng/mL (HR 1.23, 95% CI: 1.06–1.42, P = 0.006), liver cirrhosis (HR 1.59, 95% CI: 1.36–1.86, P < 0.001), BCLC stage B or C (HR 1.52, 95% CI: 1.22–1.89, P < 0.001), tumor size ≥3 cm (HR 1.32, 95% CI: 1.01–1.51, P = 0.043), MVI (HR 1.55, 95% CI: 1.33–1.80, P < 0.001), and satellite nodules (HR 1.18, 95% CI: 1.51–2.58, P < 0.001).
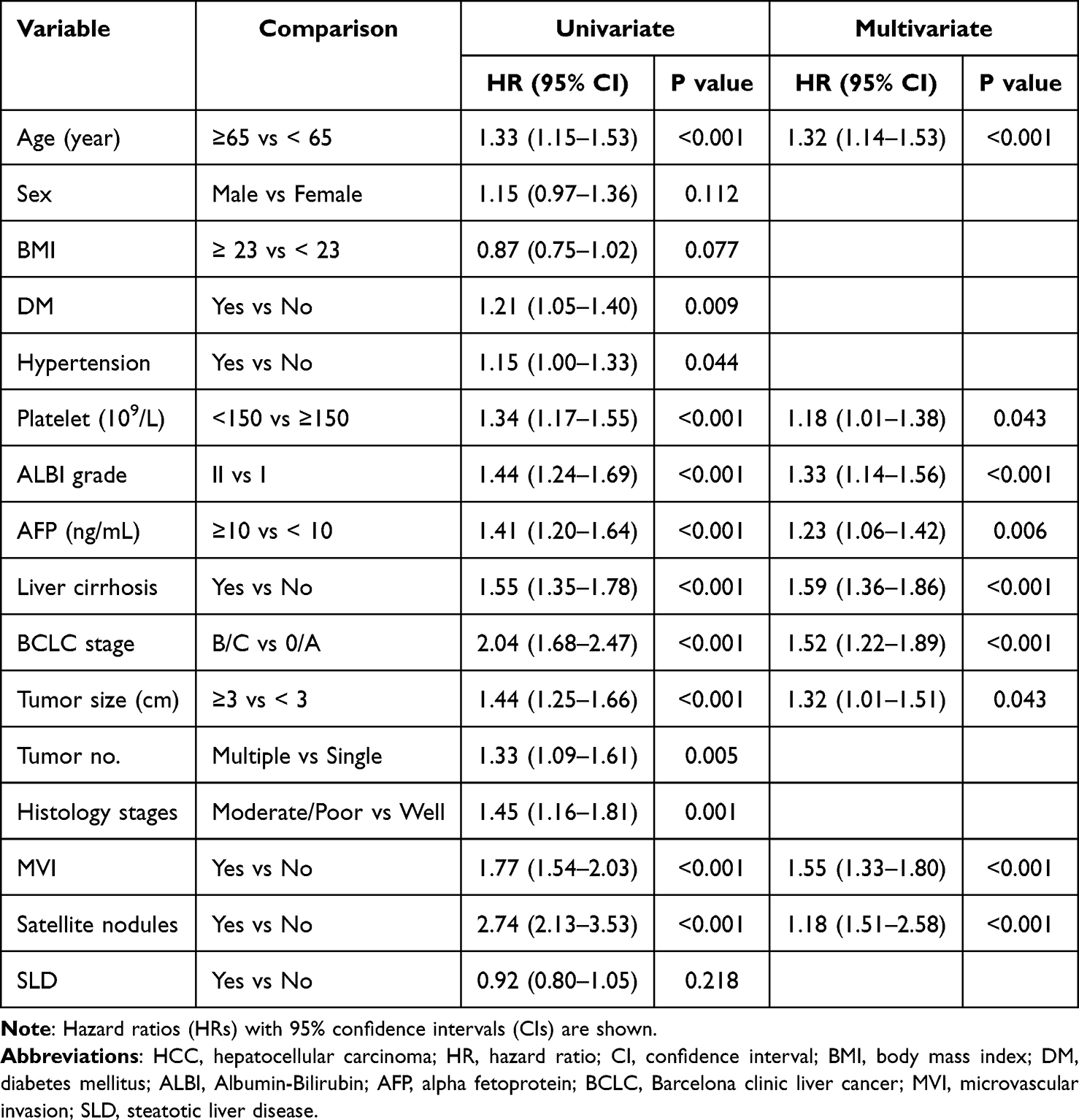 |
Table 2 Univariate and Multivariate Analyses of Prognostic Factors Associated with HCC Recurrence Following Curative Resection |
Factors Associated with Overall Survival
In univariate Cox regression analysis, several clinical and tumor-related variables were significantly associated with increased all-cause mortality, including age ≥65 years, diabetes mellitus, hypertension, platelet count <150 ×109/L, ALBI grade II, AFP ≥10 ng/mL, liver cirrhosis, BCLC stage B or C, tumor size ≥3 cm, presence of microvascular invasion (MVI), satellite nodules, and moderately to poorly differentiated tumor histology (all P < 0.01). Antiviral treatment status for HBV or HCV infection was evaluated in univariate analyses but was not significantly associated with overall survival and was therefore not included in the multivariable models. Conversely, the presence of steatotic liver disease (SLD) was significantly associated with a reduced risk of mortality (HR 0.70, 95% CI: 0.59–0.84, P < 0.001).
In multivariate analysis (shown in Table 3), independent predictors of increased all-cause mortality included age ≥65 years (HR 1.48, 95% CI: 1.22–1.79, P < 0.001), diabetes mellitus (HR 1.31, 95% CI: 1.08–1.59, P = 0.007), hypertension (HR 1.26, 95% CI: 1.04–1.53, P = 0.019), ALBI grade II (HR 1.83, 95% CI: 1.51–2.21, P < 0.001), AFP ≥10 ng/mL (HR 1.32, 95% CI: 1.09–1.59, P = 0.004), liver cirrhosis (HR 1.53, 95% CI: 1.27–1.85, P < 0.001), BCLC stage B or C (HR 2.10, 95% CI: 1.60–2.76, P < 0.001), tumor size ≥3 cm (HR 1.50, 95% CI: 1.23–1.84, P < 0.001), MVI (HR 1.65, 95% CI: 1.36–2.00, P < 0.001), and satellite nodules (HR 2.04, 95% CI: 1.48–2.81, P < 0.001). Notably, the presence of SLD remained an independent protective factor against all-cause mortality (HR 0.76, 95% CI: 0.63–0.92, P = 0.005).
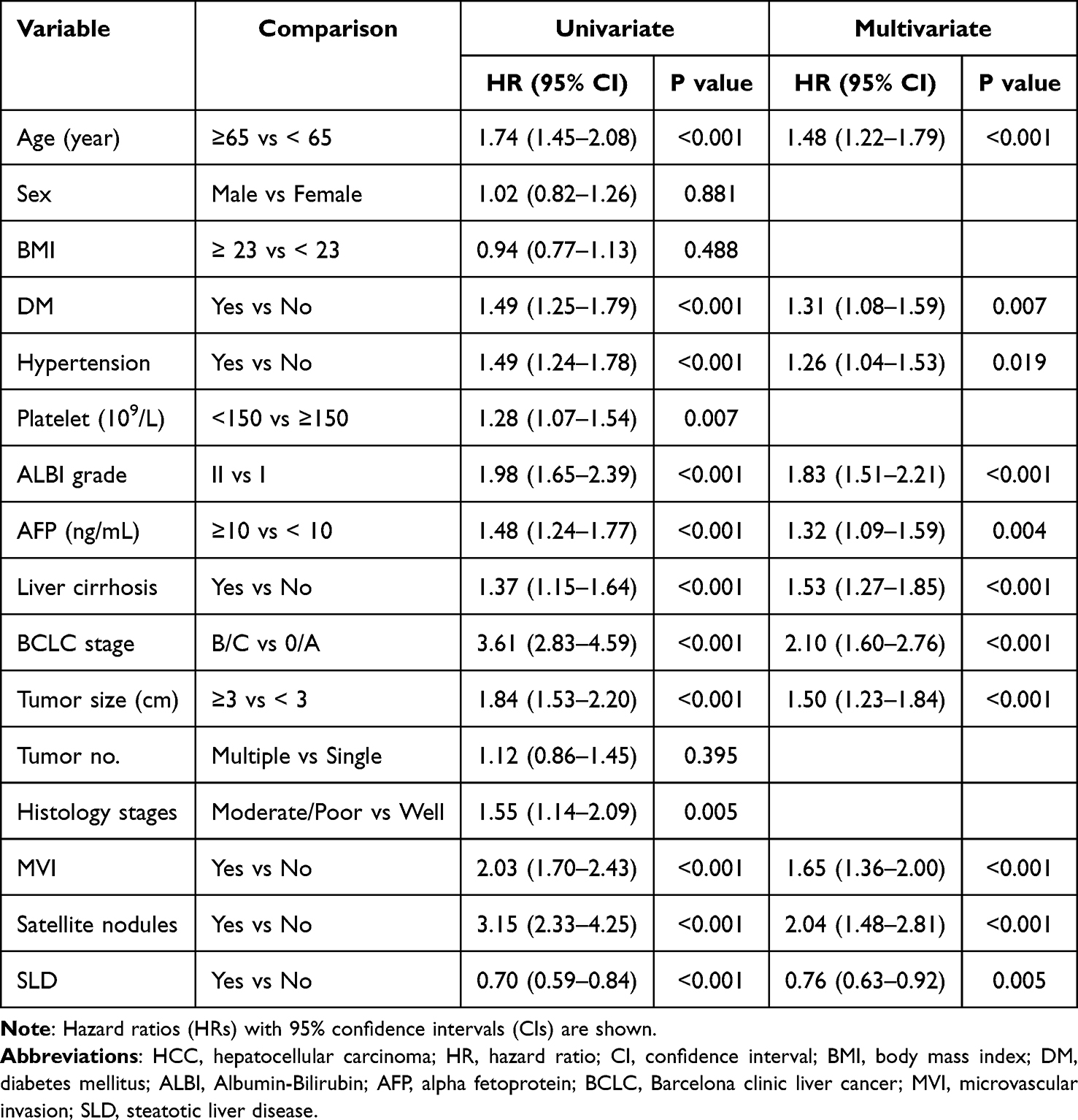 |
Table 3 Univariate and Multivariate Analyses of Prognostic Factors Associated with All-Cause Mortality in Patients with HCC Undergoing Curative Resection |
Subgroup Analysis of Survival by Clinical Characteristics
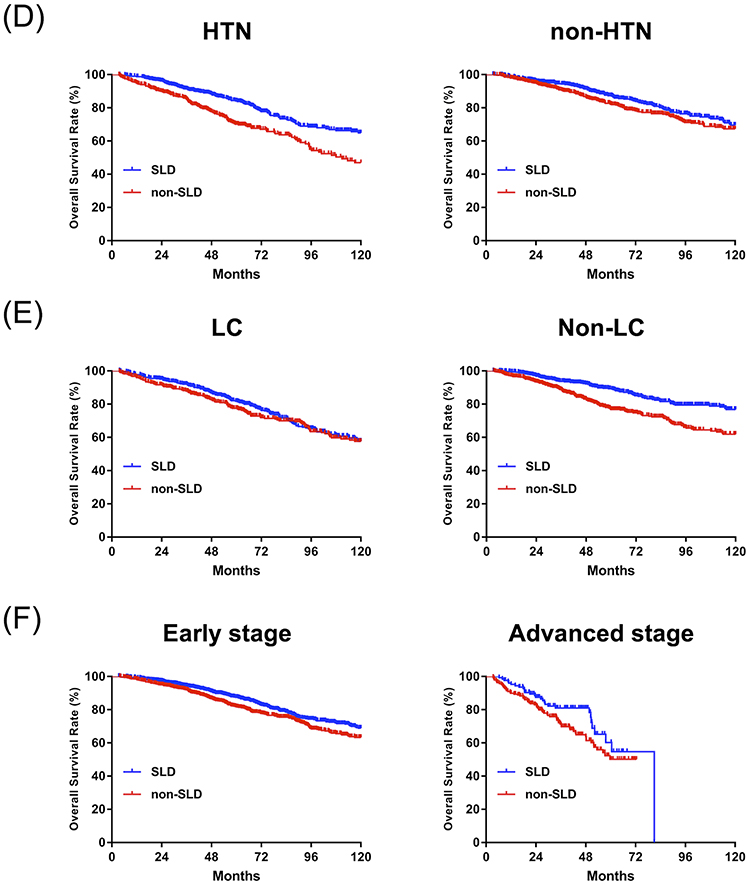
As shown in Figure 4, the survival benefit of SLD was more pronounced in male patients (Figure 4A), those with higher BMI (Figure 4B), diabetes (Figure 4C), hypertension (Figure 4D), absence of cirrhosis (Figure 4E), and early-stage HCC (Figure 4F). In contrast, no significant benefit was observed in female patients, those with lower BMI, cirrhosis, or advanced-stage disease. Overall, despite some heterogeneity, the presence of SLD was consistently associated with improved survival in several clinically relevant subgroups.
Figure 4 continued. Figure 4 Overall survival curves comparing patients with and without SLD, stratified by clinical characteristics. (A) Gender: men (n=876/756, P<0.001) and women (n=233/258, P=0.768); (B) body mass index (BMI): BMI ≥ 23 (n=946/584, P<0.001) and BMI < 23 (n=161/425, P=0.474); (C) diabetes mellitus (DM): DM (n=440/267, P=0.003) and non-DM (n=669/746, P<0.001); (D) hypertension (HTN): HTN (n=555/434, P<0.001) and non-HTN (n=554/580, P=0.109); (E) liver cirrhosis (LC): LC (n=490/398, P=0.384) and Non-LC (n=619/616, P<0.001); and (F) hepatocellular carcinoma (HCC) stage: early stage (n=984/826, P=0.010) and advanced stage (n=125/188, P=0.059). Abbreviations: SLD, steatotic liver disease; BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; LC, liver cirrhosis; HCC, hepatocellular carcinoma.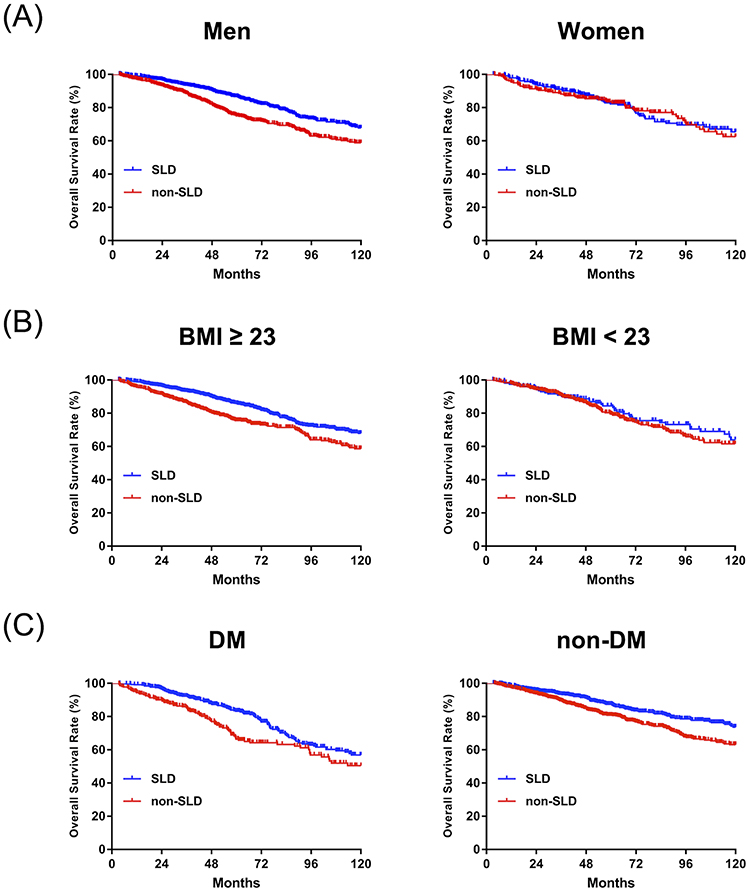
Subgroup Analysis of Survival by Viral and Non-Viral HCC Etiology
When stratified by HCC etiology, significant differences were observed (Figure 5). Kaplan–Meier analysis showed that the presence of SLD was associated with better overall survival in patients with CHB-related HCC (Figure 5A; P = 0.006) and NBNC-related HCC (Figure 5C; P = 0.007), whereas no significant difference was noted in patients with CHC-related HCC (Figure 5B). However, after adjustment for potential confounders in multivariate analysis (shown in Table 4), the survival benefit of SLD remained statistically significant only in the CHB subgroup (HR 0.71, 95% CI: 0.54–0.93, P = 0.011), while the associations observed in the CHC and NBNC groups were no longer significant.
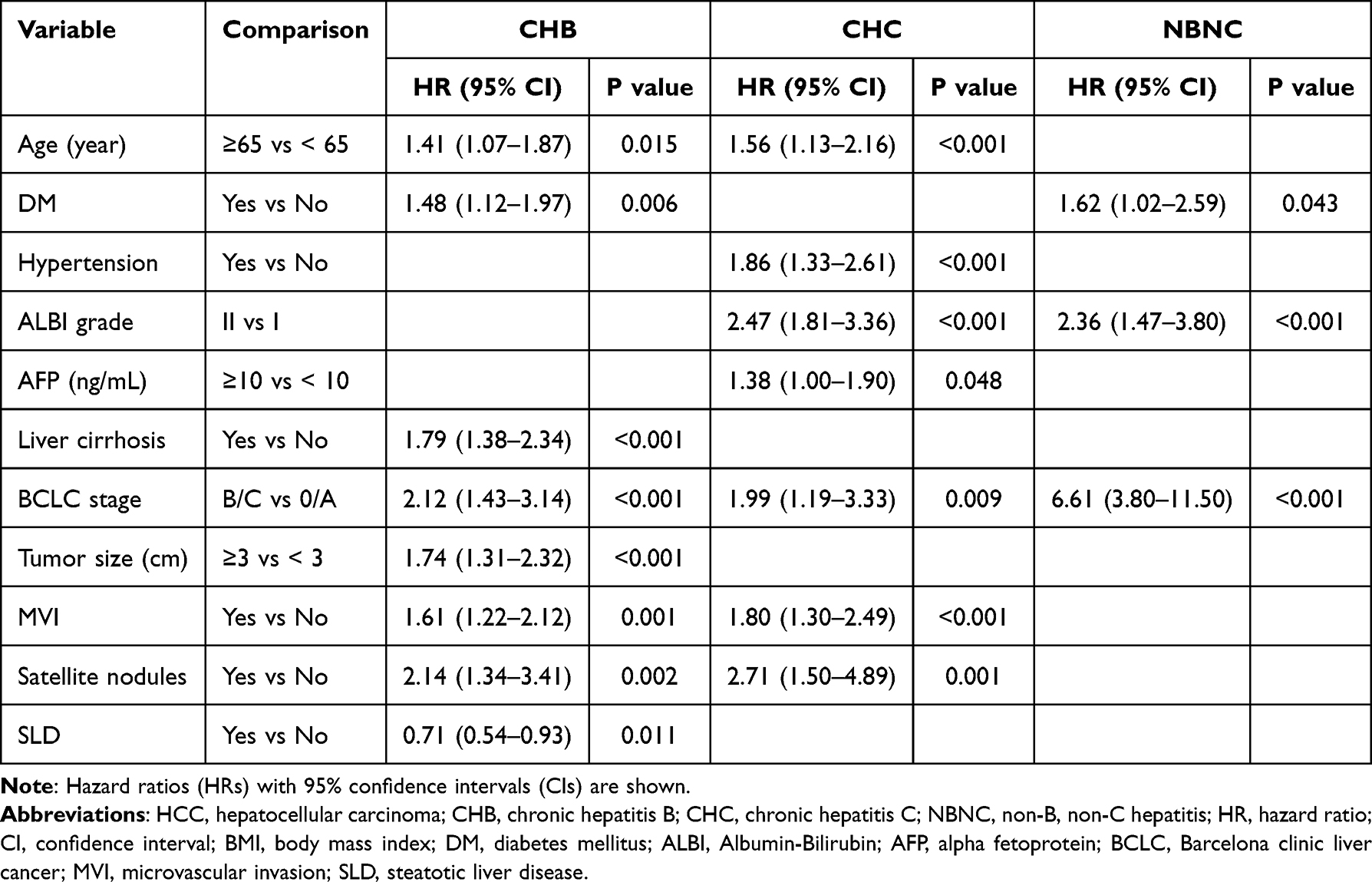 |
Table 4 Multivariate Analysis of All-Cause Mortality Stratified by Etiology of Hepatocellular Carcinoma (HCC): Chronic Hepatitis B (CHB), Chronic Hepatitis C (CHC), and Non-B, Non-C (NBNC) Hepatitis |
 |
Figure 5 Recurrence-free survival (RFS) and overall survival (OS) in patients with HCC stratified by etiology. (A) Chronic hepatitis B (CHB) (RFS: n=678/528, P=0.964; OS: n=678/528, P=0.006); (B) chronic hepatitis C (CHC) (RFS: n=185/357, P=0.459; OS: n=185/357, P=0.793); and (C) non-B, non-C (NBNC) hepatitis (RFS: n=246/129, P=0.030; OS: n=246/129, P=0.007). Abbreviations: SLD, steatotic liver disease; HCC, hepatocellular carcinoma; RFS, recurrence-free survival; OS, overall survival; CHB, chronic hepatitis B; CHC, chronic hepatitis C; NBNC, non-B, non-C. |
Discussion
In this large retrospective cohort, we demonstrated that concurrent SLD is independently associated with improved OS following curative resection for HCC, despite no significant impact on RFS. This divergence—a central finding of our study—suggests that the observed survival benefit is likely driven by factors beyond enhanced oncological control. To our knowledge, this is the first large-scale study to identify SLD as a positive prognostic indicator in resectable HCC, particularly among patients with CHB. These findings challenge the conventional paradigm of hepatic steatosis as a uniformly detrimental feature, suggesting instead that its prognostic significance is highly context dependent. Notably, while SLD remained significantly associated with improved OS after multivariable adjustment, this finding should not be interpreted as biological independence from metabolic comorbidities, such as diabetes or hypertension, which remain critical determinants of mortality.
In our cohort, patients with SLD exhibited more favorable tumor and hepatic characteristics—including smaller tumor size, lower microvascular invasion rates, earlier BCLC stage, and better-preserved liver function (eg, higher albumin levels and lower ALBI grade)—all of which are established predictors of improved postoperative survival. These results are in line with prior studies by Su et al and Liu et al, who observed similar OS benefits in NAFLD- or MAFLD-related HCC cohorts.17,18 Beyond clinical parameters, recent studies suggest that NAFLD-associated HCC may represent a biologically distinct subtype. Compared with viral-related HCC, NASH-HCC is less frequently associated with vascular invasion and poor differentiation.19 Notably, steatohepatitic HCC—a histologic subtype commonly seen in NAFLD—is generally not associated with β-catenin activation, a pathway known to promote immune exclusion and resistance to immunotherapy. Collectively, these observations raise the possibility that hepatocellular carcinoma arising in the setting of SLD may be associated with a relatively more immunogenic tumor microenvironment and less aggressive biological features.20 While these features may explain the observed OS advantage, residual confounding must be acknowledged. Patients with SLD often present with metabolic comorbidities that lead to more intensive surveillance and earlier detection, along with increased opportunity for curative or salvage therapies. Prospective studies are needed to confirm whether this relationship is truly causal and to better understand the underlying mechanisms.
Subgroup analyses revealed that the survival benefit of SLD was most pronounced in patients without cirrhosis or diabetes, those with hypertension, BMI ≥23 kg/m2, early-stage HCC, and male sex. While Huynh et al reported greater benefit in females,21 our data suggest that sex-specific effects may vary by population. Interestingly, we found no significant difference in survival between patients with moderate versus severe steatosis, implying that the prognostic impact of SLD may follow a threshold effect rather than a dose-response relationship.
The survival benefit of SLD was most evident in patients with CHB-related HCC, who exhibited a significantly lower risk of all-cause mortality compared with those without SLD (adjusted HR 0.71). This finding is consistent with a recent US cohort showing that hepatic steatosis was associated with reduced mortality and a lower incidence of HCC among patients with CHB.22 Importantly, however, the present study lacked longitudinal HBV DNA and HBsAg data and therefore cannot directly assess viral activity or antiviral treatment response.
Prior studies have suggested that hepatic steatosis may be associated with attenuation of HBV replication through a range of immunometabolic pathways, including altered innate immune signaling, metabolic stress–related modulation of viral transcription, and changes in hepatocellular secretory processes.23 These mechanisms are derived from experimental or external clinical studies and should be regarded as biologically plausible but speculative hypotheses rather than causal explanations for our findings. In the context of our results—particularly the dissociation between improved overall survival and unchanged recurrence-free survival—the observed survival advantage in CHB patients with concurrent SLD is more likely to reflect a favorable host or hepatic milieu. Supporting this interpretation, patients with steatosis may exhibit preserved functional reserve and milder fibrosis rather than a direct antiviral effect. A multicenter biopsy-based study demonstrated that CHB patients with NAFLD had lower rates of significant fibrosis, advanced fibrosis, and cirrhosis compared with those without NAFLD.24 Consistent with this concept, a recent cohort also reported higher rates of HBsAg seroclearance and seroconversion in CHB patients with MASLD.25 Taken together, these observations suggest that the survival benefit associated with SLD in CHB-related HCC may arise from an overall more favorable hepatic environment and non-oncologic factors, rather than from viral suppression alone.
In contrast, steatosis in CHC has been strongly linked to inflammatory activity and fibrosis progression. A meta-analysis of over 3000 CHC patients showed that hepatic steatosis was independently associated with both inflammation and advanced fibrosis.26 As for NBNC, the prognostic impact of SLD may be less apparent due to the heterogeneous nature of its underlying etiologies. These observations suggest that the prognostic role of SLD may differ by viral etiology—potentially beneficial in CHB but detrimental in CHC. Such divergence may reflect underlying pathophysiologic differences as well as treatment context. In Taiwan, CHB patients have long had access to reimbursed nucleos(t)ide analogs, enabling stable viral suppression and possibly amplifying the protective effects of SLD. By contrast, direct-acting antivirals for HCV only became broadly available in recent years, and their limited uptake in earlier cohorts may have attenuated the impact of SLD in CHC-related HCC. Collectively, these findings underscore that the prognostic implications of SLD are highly context-dependent and cannot be generalized across different viral etiologies.
The observed dissociation between significantly improved overall survival and unchanged recurrence-free survival suggests that the survival advantage in patients with SLD is not primarily driven by enhanced oncological control. Instead, our finding of significantly lower rates of both liver-related and non–liver-related mortality in the SLD group points toward non-oncologic contributors (shown in Figure 2C and D), such as superior physiological reserve or enhanced treatment tolerance. This pattern—improved OS without corresponding gains in RFS—aligns with previous reports by Huynh et al and Benhammou et al in MASLD- or NAFLD-related HCC cohorts.21,27 Collectively, these findings underscore that recurrence alone may be an insufficient prognostic metric for this population, as overall survival appears to be heavily influenced by the patient’s underlying metabolic status and physiological resilience.
Several limitations of this study should be acknowledged. First, its retrospective nature precludes the establishment of causality and may involve surveillance bias, as younger patients with SLD often undergo more frequent clinical monitoring. Second, SLD was defined histologically from resected non-tumorous tissue, which may not represent the entire liver parenchyma; furthermore, the retrospective design precluded a formal assessment of inter-observer variability. Third, steatosis is dynamic and may regress with metabolic control, introducing temporal variability that a single-point pathological assessment cannot capture. Fourth, given the long inclusion period of this cohort, antiviral treatment strategies—particularly for chronic hepatitis C—evolved substantially over time, encompassing both interferon-based and direct-acting antiviral regimens. Detailed longitudinal data on lifetime antiviral exposure, treatment adherence, and virological response were not uniformly available, limiting our ability to fully characterize the potential impact of antiviral therapy and virological activity on long-term outcomes. Fifth, the lack of comprehensive longitudinal metabolic indices (e.g., HOMA-IR, lipid profiles), together with incomplete virological data, restricts our ability to evaluate the complex interplay between metabolic status, viral factors, and survival, and residual confounding cannot be entirely excluded. Finally, the generalizability of our results to non-Asian or advanced-stage populations is limited, and subgroup analyses for CHC and NBNC were constrained by sample size and etiologic heterogeneity. To overcome these limitations, future prospective studies are needed to validate our findings and evaluate histologic subtypes, metabolic markers, and fibrosis severity. Non-invasive imaging modalities such as MRI-PDFF or AI-assisted ultrasound may enable preoperative identification of SLD and facilitate its incorporation into risk prediction tools and staging systems.
In conclusion, concurrent SLD is independently associated with superior overall survival following curative resection for HCC, a benefit particularly pronounced among patients with CHB. Our findings identify SLD as a clinically significant prognostic modifier, challenging the conventional paradigm of hepatic steatosis as a uniformly detrimental feature. These results suggest that SLD may warrant consideration in the prognostic assessment of resectable HCC; however, they should be regarded as hypothesis-generating and underscore the need for prospective validation in well-designed, longitudinal cohorts. Ultimately, incorporating SLD status into future prognostic models could refine individualized risk stratification and optimize postoperative surveillance strategies in this population.
Ethical Statement
The study protocol was approved by the IRB of Kaohsiung Chang Gung Memorial Hospital (approval number: 202500957B0). All procedures performed in this study involving human participants were conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments or comparable ethical standards. Due to the retrospective nature of the study and the use of de-identified data, the requirement for informed consent was waived by the IRB.
Acknowledgments
The authors would like to thank the clinical and research staff of Kaohsiung Chang Gung Memorial Hospital for their assistance in data collection and patient care. We thank the service provided by the Cancer Registration of Cancer Center Department, Kaohsiung Chang Gung Memorial Hospital. This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declare that they have no conflicts of interest. No author has any commercial association, such as consultancies, stock ownership, equity interests, or patent-licensing arrangements, that could be perceived as a potential conflict of interest.
References
1. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. The Lancet. 2012;379(9822):1245–15. doi:10.1016/S0140-6736(11)61347-0
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Chen TC, Hsiao SW, Chen YY, et al. Increased prevalence but decreased survival of nonviral hepatocellular carcinoma compared to viral hepatocellular carcinoma in recent ten years. Sci Rep. 2024;14(1):9068. doi:10.1038/s41598-024-59668-2
4. Huang DQ, El-Serag HB, Loomba R. Global epidemiology of NAFLD-related HCC: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2021;18(4):223–238. doi:10.1038/s41575-020-00381-6
5. Lin Y-P, Wang P-M, Chuang C-H, et al. Metabolic risks are increasing in non-B Non-C early-stage hepatocellular carcinoma: a 10-year follow-up study. Front Oncol. 2022. 10.3389/fonc.2022.816472.
6. Myers S, Neyroud-Caspar I, Spahr L, et al. NAFLD and MAFLD as emerging causes of HCC: a populational study. JHEP Rep. 2021;3(2):100231. doi:10.1016/j.jhepr.2021.100231
7. Kan C, Zhang K, Wang Y, et al. Global burden and future trends of metabolic dysfunction-associated Steatotic liver disease: 1990-2021 to 2045. Ann Hepatol. 2025;30(2):101898. doi:10.1016/j.aohep.2025.101898
8. Hailemichael D, Renata F, David H, et al. Prevention and control of risk factors in metabolic and alcohol-associated steatotic liver disease. Metab Target Organ Damage. 2024;4(3):25. doi:10.20517/mtod.2024.30
9. Tacke F, Horn P, Wai-Sun Wong V, et al. EASL–EASD–EASO Clinical Practice Guidelines on the management of metabolic dysfunction-associated steatotic liver disease (MASLD). J Hepatol. 2024;81(3):492–542. doi:10.1016/j.jhep.2024.04.031
10. White DL, Kanwal F, El-Serag HB. Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review. Clin Gastroenterol Hepatol. 2012;10(12):1342–1359.e2. doi:10.1016/j.cgh.2012.10.001
11. Chen YT, Chen TI, Yang TH, et al. Long-term risks of cirrhosis and hepatocellular carcinoma across steatotic liver disease subtypes. Am J Gastroenterol. 2024;119(11):2241–2250. doi:10.14309/ajg.0000000000002778
12. Tsai FP, Su TH, Huang SC, et al. Outcomes of radiofrequency ablation for hepatocellular carcinoma with concurrent steatotic liver disease. Cancer. 2025;131(1):e35541. doi:10.1002/cncr.35541
13. Koh YX, Tan HJ, Liew YX, et al. Liver resection for nonalcoholic fatty liver disease-associated hepatocellular carcinoma. J Am Coll Surg. 2019;229(5):467–478.e1. doi:10.1016/j.jamcollsurg.2019.07.012
14. Su CW, Chau GY, Hung HH, et al. Impact of steatosis on prognosis of patients with early-stage hepatocellular carcinoma after hepatic resection. Ann Surg Oncol. 2015;22(7):2253–2261. doi:10.1245/s10434-014-4221-5
15. Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023;77(5):1797–1835. doi:10.1097/hep.0000000000000323
16. van Keulen A-M, Olthof PB, Buettner S, et al. The influence of hepatic steatosis and fibrosis on postoperative outcomes after major liver resection of perihilar cholangiocarcinoma. Annals Surg Oncol. 2024;31(1):133–141. doi:10.1245/s10434-023-14419-x
17. Su JY, Deng ZJ, Teng YX, et al. Prognosis after hepatic resection of patients with hepatocellular carcinoma related to non-alcoholic fatty liver disease: meta-analysis. BJS Open. 2023;7(1). doi:10.1093/bjsopen/zrac167
18. Liu L, Xie S, Teng Y-X, et al. Outcomes of liver resection for metabolic dysfunction-associated fatty liver disease or chronic Hepatitis B-Related HCC. Front Oncol. 2022:11–2021. 10.3389/fonc.2021.783339.
19. Hernandez-Alejandro R, Croome KP, Drage M, et al. A comparison of survival and pathologic features of non-alcoholic steatohepatitis and hepatitis C virus patients with hepatocellular carcinoma. World J Gastroenterol. 2012;18(31):4145–4149. doi:10.3748/wjg.v18.i31.4145
20. Fujiwara N, Nakagawa H. Clinico-histological and molecular features of hepatocellular carcinoma from nonalcoholic fatty liver disease. Cancer Sci. 2023;114(10):3825–3833. doi:10.1111/cas.15925
21. Huynh CN, Tsai YC, Tsai MJ, et al. Impact of concurrent MASLD on early-stage HCC following curative resection in chronic hepatitis B. Am J Cancer Res. 2024;14(9):4567–4579. doi:10.62347/ljrg3048
22. Yendewa GA, Elangovan A, Olasehinde T, et al. Impact of hepatic steatosis on mortality, hepatocellular carcinoma, end-stage liver disease and HBsAg seroclearance in chronic hepatitis B: a United States cohort study. Front Immunol. 2025;16:1566925. doi:10.3389/fimmu.2025.1566925
23. Zhang S, Mak LY, Yuen MF, Seto WK. Mechanisms of hepatocellular carcinoma and cirrhosis development in concurrent steatotic liver disease and chronic hepatitis B. Clin Mol Hepatol. 2025;31(Suppl):S182–s195. doi:10.3350/cmh.2024.0837
24. Yao R, Lu S, Xue R, et al. NAFLD is associated with less severe liver fibrosis in chronic hepatitis B: a multi-center, retrospective study. Ann Hepatol. 2024;29(1):101155. doi:10.1016/j.aohep.2023.101155
25. Huang SC, Su TH, Tseng TC, et al. Metabolic dysfunction-associated steatotic liver disease facilitates hepatitis b surface antigen seroclearance and seroconversion. Clin Gastroenterol Hepatol. 2024;22(3):581–590.e6. doi:10.1016/j.cgh.2023.09.040
26. Leandro G, Mangia A, Hui J, et al. Relationship between steatosis, inflammation, and fibrosis in chronic hepatitis C: a meta-analysis of individual patient data. Gastroenterology. 2006;130(6):1636–1642. doi:10.1053/j.gastro.2006.03.014
27. Benhammou JN, Aby ES, Shirvanian G, Manansala K, Hussain SK, Tong MJ. Improved survival after treatments of patients with nonalcoholic fatty liver disease associated hepatocellular carcinoma. Sci Rep. 2020;10(1):9902. doi:10.1038/s41598-020-66507-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.