Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Concurrent Nasal Sebaceous Carcinoma and Right-Hand Squamous Cell Carcinoma: A Case Report and Literature Review
Authors Yang Y ![]()
Received 3 December 2025
Accepted for publication 26 February 2026
Published 2 March 2026 Volume 2026:19 583728
DOI https://doi.org/10.2147/CCID.S583728
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Ying Yang
Department of Dermatology, Zigong Fourth People’s Hospital, Zigong, People’s Republic of China
Correspondence: Ying Yang, Department of Dermatology, Zigong Fourth People’s Hospital, Zigong, People’s Republic of China, Email [email protected]
Abstract: Cutaneous squamous cell carcinoma (cSCC) is the second most common nonmelanoma skin cancer with an increasing incidence. Sebaceous carcinoma (SC) is a rare, highly aggressive malignant tumor of cutaneous appendage origin, mainly occurring in the head and neck region (most commonly in the ocular area), and extremely rare in the nasal region. A literature review showed that only 3 cases of collision tumors composed of SC and squamous cell carcinoma (SCC) have been reported previously, and there is no report of concurrent SC and cSCC in different sites of the same patient. Combined with a literature review, this paper reports an 84-year-old female patient with progressive ulcerative skin lesions on the right hand and nose for 5 years. Initial biopsy suggested cSCC of the hand and sebaceous adenoma of the nose. After surgical excision, postoperative pathology and immunohistochemistry confirmed well-differentiated cSCC of the right hand and SC of the nose. Oncology consultation recommended adjuvant radiotherapy for nasal SC after surgery, which was refused by the patient’s family due to her advanced age; no recurrence or metastasis was observed in either of the two lesions during the 5-month postoperative follow-up period. By analyzing this rare case of multicentric primary cutaneous malignant tumors combined with relevant literature, we emphasize that elderly patients with long-standing chronic skin lesions require comprehensive screening to avoid missed diagnosis. Accurate diagnosis relies on pathology and immunohistochemistry, surgical resection is the main treatment, and long-term follow-up is crucial. This case enriches the clinical data on concurrent SC and cSCC, providing references for their diagnosis and treatment.
Keywords: cutaneous squamous cell carcinoma, sebaceous carcinoma, case report, treatment
Introduction
Cutaneous squamous cell carcinoma (cSCC) is the second most common nonmelanoma skin cancer (keratinocyte carcinoma), with an increasing incidence trend.1,2 Currently, confirmed risk factors for cSCC consist of ultraviolet radiation, advanced age, fair skin, immunosuppression, chemical exposure, and chronic inflammation.3–7 While most cSCC cases can be successfully cured through surgical resection, a subset carries a higher risk of recurrence, metastasis, and mortality—studies have shown that patients diagnosed with cSCC face a 3.7% risk of metastasis and a 2.1% risk of disease-specific mortality.8 Early identification of cSCC is therefore crucial.
Sebaceous carcinoma (SC) is a rare malignant tumor of cutaneous appendage origin, which is divided into periocular sebaceous carcinoma (PSC) and extraocular sebaceous carcinoma (ESC).9 Compared with cSCC, SC is a far rarer but highly aggressive malignant tumor. An epidemiological study on the US population showed that the overall incidence rate of SC is 2.63 per million person-years.10 The etiology and pathogenesis of SC have not been fully elucidated. UV radiation damage, advanced age, genetic predisposition (particularly in Muir-Torre syndrome [MTS]), and immunosuppression are recognized as risk factors for SC development.11–14 SC rarely develops local regional or distant metastasis and is associated with a favorable overall survival. Age, gender, tumor size, tumor grade, and tumor stage are all prognostic factors for this disease, while the impact of ethnicity, primary tumor site, and urban-rural differences on prognosis remains controversial.15–17
Clinically, SC is predominantly found in the head and neck region, with the ocular area being the most common site, while SC arising in the nasal region is extremely rare.9,10,15 The metastasis rate of extraocular SC is 1.8%, and that of periocular SC is 12.5%.9 The 3- to 5-year disease-specific mortality rate is 18% for the extraocular type and 25.6% for the periocular type.9 Most of the reported nasal SCs occur in elderly male patients, which is consistent with the epidemiology of SC (Table 1).18–28 Only one patient in the reports had metastasis indicated by CT examination, while the rest had no metastasis and all achieved a good prognosis after surgical treatment.18–28
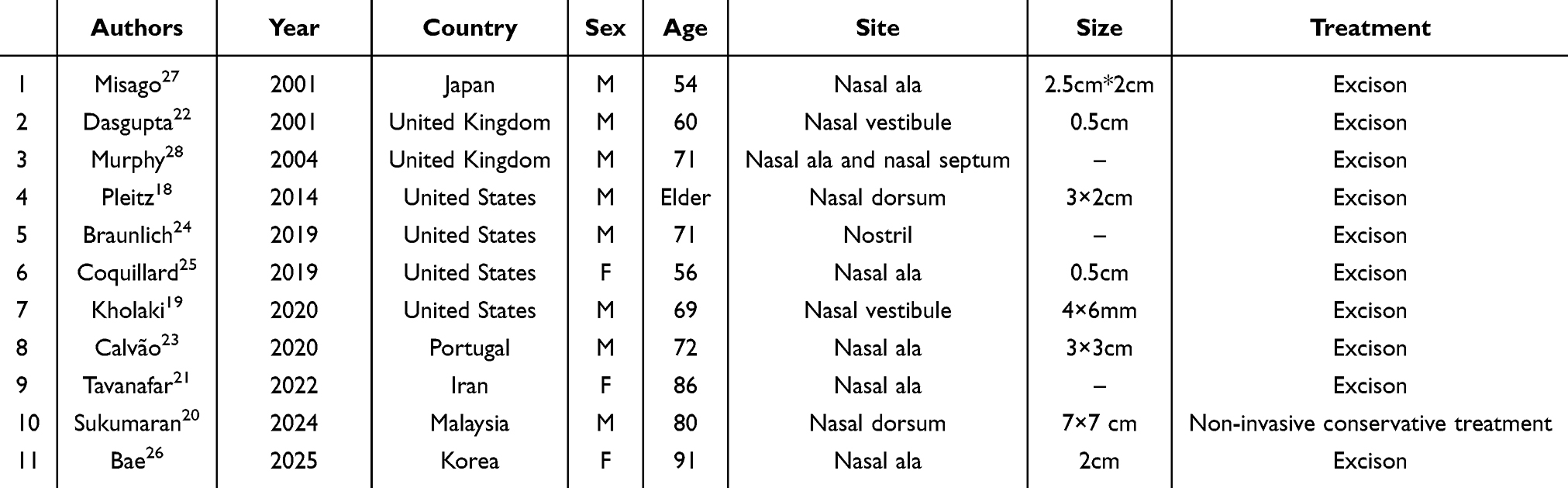 |
Table 1 Reported Cases of Nasal Sebaceous Carcinoma in the Literature |
Herein, we describe a rare case of concurrent SC of the nose and cSCC of the hand. Only 3 cases of collision tumors composed of SC and squamous cell carcinoma (SCC) have been reported in the existing literature, and the simultaneous occurrence of SC and SCC in different sites of the same patient is reported for the first time in the literature with this case.29–31Given the rarity and misdiagnosis risk of these two concurrent cutaneous malignancies, this case underscores the urgency of proactive clinical screening and accurate differential diagnosis.
Case Presentation
We admitted an 84-year-old female patient who complained of local ulceration on the ring finger of her right hand after wearing a ring more than 5 years ago, accompanied by mild pain and discomfort. She had received topical treatment with fusidic acid cream, Kangfuxin Liquid and mupirocin ointment after the onset of the disease, but all showed poor efficacy. The skin lesion on her right hand gradually enlarged, proliferated and elevated, with an ulcer forming in the center of the lesion, and the pain also gradually worsened. Meanwhile, we noticed a skin tumor on her nose. Further inquiry about the patient’s medical history revealed that this tumor had also been present for more than 5 years without any subjective symptoms. After the nasal neoplasm appeared, the patient self-administered topical iodophor for treatment with no improvement, and the skin lesion gradually enlarged over time.
The patient had a history of Meniere’s disease, cholelithiasis and sleep disorder, and had been taking alprazolam tablets orally for a long time to aid sleep. She had no other significant past medical history or history of facial or hand trauma. There was no family history of cancer either. She had an unremarkable personal and social history with no smoking or drinking habits.
Clinical examination revealed a tender, firm, fixed nodule measuring approximately 2 cm × 1 cm at the base of the right ring finger. The lesion was pale red with well-defined borders and showed central ulceration (Figure 1). In addition, a firm, fixed non-tender nodule measuring about 1.5 cm × 1 cm was present on the nasal tip, with regular borders and central ulceration (Figure 2). No similar lesions were identified elsewhere on the body. The initial clinical diagnoses were cSCC and basal cell carcinoma (BCC).
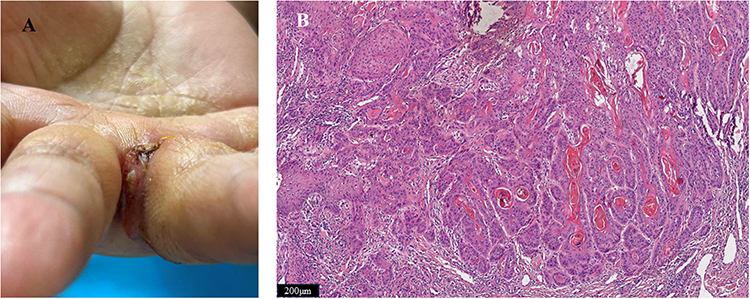 |
Figure 1 (A) Photograph showing mass of the right hand. (B) Hematoxylin and eosin-stained section showing well-differentiated squamous cell carcinoma (original magnificationⅹ10). |
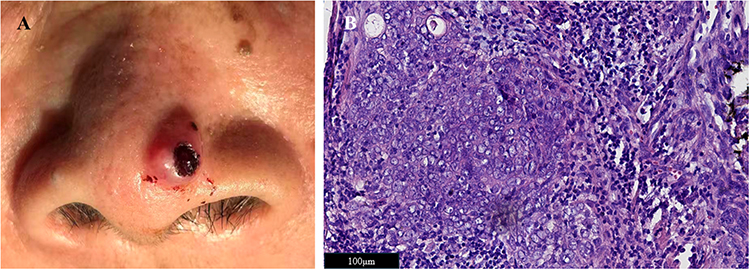 |
Figure 2 (A) Photograph showing mass of the nose. (B) Hematoxylin and eosin-stained section showing sebaceous carcinoma (original magnificationⅹ40). |
We performed biopsies on both masses. Pathological examination results showed that the morphological features of the right-hand mass were consistent with cSCC, while those of the nasal mass were consistent with sebaceous adenoma. Meanwhile, we conducted clinical and radiological screenings for the patient, and no abnormal lesions or distant metastases were detected. After excluding surgical contraindications, the patient subsequently underwent local excision of the nasal mass and local excision of the right-hand mass. Intraoperative frozen section examination of the right-hand mass indicated negative surgical margins (including the surrounding and basal edges), and postoperative pathological examination confirmed it as well-differentiated SCC. The patient refused intraoperative frozen section examination for the nasal mass. Postoperatively, pathological examination and immunohistochemical testing were performed, with the immunohistochemical results showing CKpan (+), EMA (+), P40 (+), P63 (+), AR (+), BER-EP4 (-), S-100 (-), and Ki-67 (+, approximately 30%) (Figure 3). Combining the morphological features of hematoxylin-eosin (HE)-stained sections and the immunohistochemical staining results, the final diagnosis was confirmed as SC.
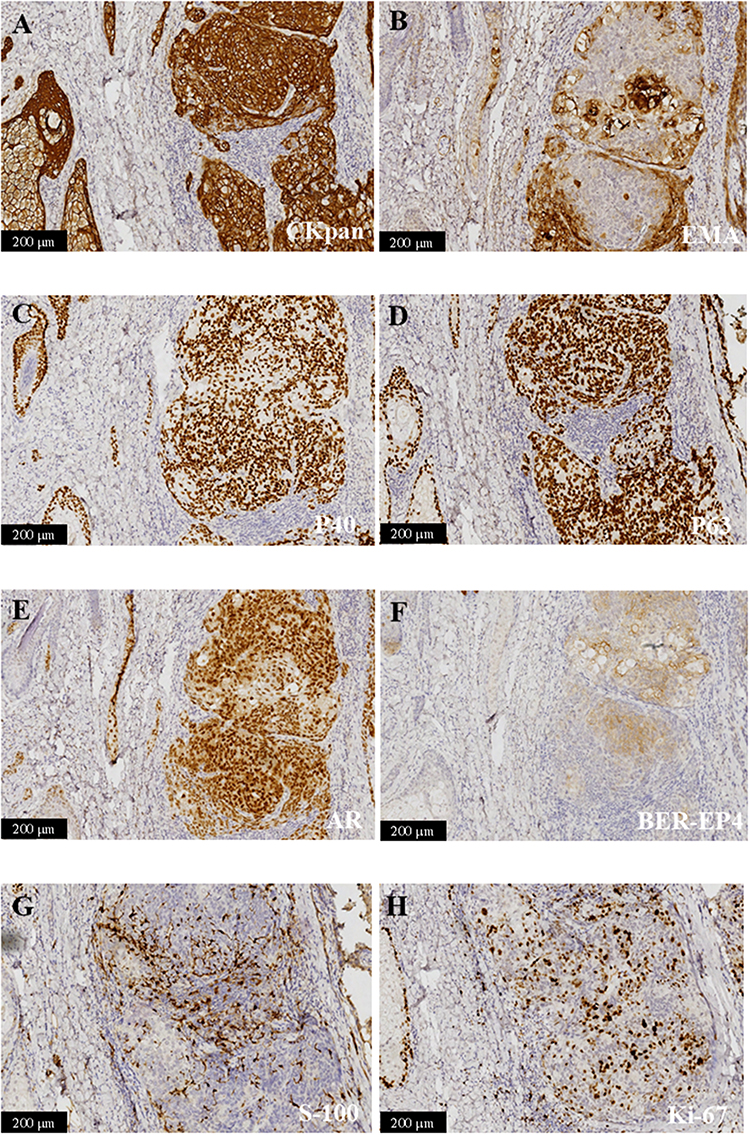 |
Figure 3 (A) The neoplastic cells are positive for CKpan (ⅹ20); (B) Neoplastic cells are positive for EMA (ⅹ20); (C) Neoplastic cells are positive for P40 (ⅹ20); (D) Neoplastic cells are positive for P63 (ⅹ20); (E) Neoplastic cells are positive for AR (ⅹ20); (F) Neoplastic cells are negative for BER-EP4 (ⅹ20); (G) Neoplastic cells are negative for S-100 (ⅹ20); (H) Neoplastic cells are partially positive for Ki-67 (×25). |
Given the high recurrence risk of SC, oncology consultation recommended adjuvant radiotherapy (RT) for the patient 4 weeks after surgical resection of the nasal malignant tumor. The patient recovered uneventfully after the operation with no complications. During subsequent follow-up, the patient’s family declined the recommended adjuvant radiotherapy due to her advanced age. To date, the patient has been followed up for more than 5 months postoperatively, with no recurrence of the skin tumors at either site, and continues to undergo regular follow-up.
Discussion
CSCC is the second most common nonmelanoma skin cancer with increasing incidence.1,2 SC is a rare, highly aggressive cutaneous appendage malignancy, mostly occurring in the head and neck (predominantly ocular) and extremely rarely in the nose.9,10,15 A literature review revealed only 3 previously reported collision tumors of SC and SCC, with no reports of concurrent SC and cSCC in different sites of the same patient.29–31 Combined with a literature review, we report an 84-year-old female with 5-year progressive ulcerative lesions on the right ring finger and nasal tip.
The concurrent occurrence of nasal SC and cSCC of the right hand in an elderly female is extremely rare clinically, and its pathogenesis is presumed to be closely related to systemic and local risk factors. The right-hand cSCC is considered to be associated with her advanced age and local chronic irritation caused by long-term ring wearing, which is consistent with the conclusion in previous studies that “advanced age and local chronic inflammation are risk factors for cSCC”.3–7 The nasal SC is presumed to be associated with ultraviolet radiation and advanced age, both of which are major risk factors for SC.11–14 As a systemic risk factor, advanced age (84 years) can induce natural skin aging and impaired immune function of the body, leading to senescent cells evading immune surveillance and abnormally accumulating in tissues to form a tumor-promoting microenvironment, thereby significantly increasing the susceptibility to cutaneous carcinogenesis.32 Meanwhile, photoaging induced by excessive ultraviolet exposure is also an important predisposing factor for the development of cutaneous malignant tumors.33 Integrating clinical, pathological, and immunohistochemical findings, both tumors are confirmed as independent primary malignant neoplasms (not metastatic lesions), supporting the diagnosis of multicentric primary cutaneous malignancies. Their pathogenesis is presumably associated with the synergistic interaction between systemic age-related factors and local site-specific stimuli.
Clinically, cSCC, SC, and BCC often require differentiation from one another. The clinical diagnosis of cutaneous tumors is challenging. In most cases, histopathological examination can assist in confirming the diagnosis. When histopathological findings are inconclusive, immunohistochemical (IHC) testing is typically used to validate the diagnosis. EMA, adipophilin, androgen receptor, BerEP4, and CK7 staining are recommended to differentiate SCC, SC, and BCC.34,35 In the present case, preoperative biopsy initially suggested a sebaceous adenoma; however, a definitive diagnosis of SC was established only after comprehensive histological and IHC evaluations following complete surgical resection. This scenario exemplifies a common clinical conundrum: the overlapping clinicopathological features between SC and benign sebaceous tumors often render differentiation based on clinical presentation and routine pathological assessment unreliable. Recent molecular research has identified several distinguishing features between SC and sebaceous adenomas, including reduced cholesterol biosynthesis, elevated TP53 mutation frequencies, specific copy number gains (predominantly on chromosomes 6, 8q, and/or 18), and a high tumor mutation burden (TMB > 10 mutations per megabase).36 These molecular alterations show promise as potential biomarkers for distinguishing malignant from benign sebaceous neoplasms.
Regarding treatment choices, the selection of therapeutic strategies for both tumors in this case was based on current clinical guidelines and the patient’s individual condition. For SC, whether PSC or ESC, complete micrographically controlled surgery (MCS) of the primary tumor remains the standard of care, with adjuvant or therapeutic radiotherapy as a supplementary option to reduce recurrence risk.37 Currently, there is no established standard treatment protocol for advanced, inoperable, or metastatic SC, and options such as local treatments and systemic therapies (including chemotherapy and immunotherapy) may be taken into account.37
For cSCC, surgical treatment is the first priority; for low-risk lesions where surgery is not feasible or advisable, non-surgical modalities such as radiotherapy, photodynamic therapy, and cryosurgery can be adopted.38 For patients with advanced cSCC who are not amenable to curative surgery or radiation therapy, immune checkpoint inhibitors have recently been approved for clinical use.39,40 Both lesions in this patient were surgically excised. However, postoperative pathological examination of the nasal lesion revealed residual tumor at the basal margin. After consultation with the Department of Oncology, adjuvant radiotherapy was recommended for the nasal SC to reduce the risk of local recurrence, but this was declined by the patient’s family owing to the patient’s advanced age.
In terms of prognosis, the 5-month postoperative follow-up showed no recurrence or metastasis in this patient. For SC patients, post-treatment clinical follow-up should be performed every six months, with a minimum duration of three years.9 For cSCC patients, regular follow-up is mandatory, with intervals based on risk stratification: once yearly for low-risk cases, every 3–6 months for the initial 2 years in high-risk cases, and every 3 months for the first 2 years in advanced patients.41 This patient will continue to undergo regular follow-up to monitor for long-term recurrence and metastasis.
Despite the clinical insights provided by this case, several gaps remain in the management of concurrent SC and cSCC, highlighting the need for future research directions to establish standardized treatment guidelines. First, large-scale retrospective or prospective studies are needed to collect more clinical data on multicentric primary cutaneous malignancies involving SC and cSCC, to clarify their epidemiological characteristics, pathogenesis, and prognostic factors. Second, further research on molecular biomarkers (such as TP53 mutations and specific copy number gains) is required to validate their clinical value in the differential diagnosis of SC and benign sebaceous tumors, and to explore their potential role in guiding treatment selection and prognosis prediction. Third, standardized treatment protocols for advanced, inoperable, or metastatic SC need to be established through multi-center clinical trials, evaluating the efficacy and safety of systemic therapies such as immunotherapy and chemotherapy. Fourth, studies focusing on the optimal follow-up strategies for elderly patients with multiple primary cutaneous malignancies are necessary, considering their poor tolerance to adjuvant therapy and complex comorbidities. Finally, research on the prevention of such malignancies should be strengthened, especially for high-risk populations (such as the elderly and those with long-term local irritation or excessive ultraviolet exposure), to reduce the incidence of multicentric primary cutaneous malignancies. These research efforts will help fill the current clinical gaps and provide evidence for establishing standardized diagnosis and treatment guidelines, ultimately improving the clinical management and prognosis of patients with such rare diseases.
Conclusion
This article reports a rare case of concurrent nasal SC and hand SCC. Both tumors were resected surgically. This case provides several important clinical insights. First, local chronic irritation is a modifiable risk factor for cSCC, and avoiding long-term mechanical irritation (such as improper jewelry wearing) may reduce the risk of skin cancer in susceptible populations. Second, elderly patients with chronic skin lesions require comprehensive systemic screening to avoid missed diagnosis of multiple primary cancers, especially asymptomatic lesions. Third, immunohistochemical staining is indispensable for the differential diagnosis of SC from other cutaneous malignant tumors, and accurate histological typing directly guides treatment decisions.
In view of the clinical value of this case and the existing gaps in the management of concurrent SC and cSCC, several forward-looking research implications should be emphasized. Further studies should focus on collecting more cases of concurrent SC and cSCC through multi-center collaboration, to clarify the epidemiological characteristics and potential pathogenic mechanisms of such multicentric primary cutaneous malignancies. Further studies should also verify the effectiveness of targeted interventions for modifiable risk factors (such as avoiding long-term local irritation) in reducing the incidence of cSCC in high-risk populations, so as to formulate more targeted prevention strategies. In addition, further studies should explore the optimization of preoperative diagnostic protocols for SC, especially the clinical application of molecular biomarkers (such as TP53 mutations), to improve the accuracy of preoperative differentiation between SC and benign sebaceous tumors and reduce misdiagnosis. Finally, further studies should focus on establishing standardized treatment and follow-up guidelines for elderly patients with multiple primary cutaneous malignancies, combining their tolerance to adjuvant therapy and comorbidity status, to achieve individualized management and improve long-term prognosis. These research efforts will help translate the clinical insights from this case into practical clinical guidance, and provide more evidence for the diagnosis, treatment and prevention of such rare diseases.
Ethics Approval and Consent for Publication
The case report adhered to the ethical principles outlined in the Declaration of Helsinki. A written informed consent was obtained from the patient’s family for publication of this study and any accompanying image. Institutional ethical approval was not required to publish this case details.
Acknowledgments
We thank the patient and physicians for participating in our study.
Funding
No funding was received for this study.
Disclosure
The author reports no potential conflicts of interest in this work.
References
1. Muzic JG, Schmitt AR, Wright AC, et al. Incidence and trends of basal cell carcinoma and cutaneous squamous cell carcinoma: a population-based study in Olmsted County, Minnesota, 2000 to 2010. Mayo Clin Proc. 2017;92(6):890–8. doi:10.1016/j.mayocp.2017.02.015
2. Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol. 2012;166(5):1069–1080. doi:10.1111/j.1365-2133.2012.10830.x
3. Xiang F, Lucas R, Hales S, Neale R. Incidence of nonmelanoma skin cancer in relation to ambient UV radiation in white populations, 1978-2012: empirical relationships. JAMA Dermatol. 2014;150(10):1063–1071. doi:10.1001/jamadermatol.2014.762
4. Gallagher RP, Bajdik CD, Fincham S, et al. Chemical exposures, medical history, and risk of squamous and basal cell carcinoma of the skin. Cancer Epidemiol Biomarkers Prev. 1996;5(6):419–424.
5. Sun Y, Liu N, Guan X, Wu H, Sun Z, Zeng H. Immunosuppression induced by chronic inflammation and the progression to oral squamous cell carcinoma. Mediators Inflammation. 2016;2016:5715719. doi:10.1155/2016/5715719
6. Schmitt J, Seidler A, Diepgen TL, Bauer A. Occupational ultraviolet light exposure increases the risk for the development of cutaneous squamous cell carcinoma: a systematic review and meta-analysis. Br J Dermatology. 2011;164(2):291–307. doi:10.1111/j.1365-2133.2010.10118.x
7. Omland SH, Gniadecki R, Hædersdal M, Helweg-Larsen J, Omland LH. Skin cancer risk in hematopoietic stem-cell transplant recipients compared with background population and renal transplant recipients: a population-based cohort study. JAMA Dermatol. 2016;152(2):177–183. doi:10.1001/jamadermatol.2015.3902
8. Schmults CD, Karia PS, Carter JB, Han J, Qureshi AA. Factors predictive of recurrence and death from cutaneous squamous cell carcinoma: a 10-year, single-institution cohort study. JAMA Dermatol. 2013;149(5):541–547. doi:10.1001/jamadermatol.2013.2139
9. Owen JL, Kibbi N, Worley B, et al. Sebaceous carcinoma: evidence-based clinical practice guidelines. Lancet Oncol. 2019;20(12):e699–e714. doi:10.1016/S1470-2045(19)30673-4
10. Joshi TP, Ranario JS. Epidemiology of Sebaceous Carcinoma in the United States: analysis of SEER data from 2000-2022. J Am Acad Dermatol. 2025. doi:10.1016/j.jaad.2025.09.051
11. Cook S, Pethick J, Kibbi N, et al. Sebaceous carcinoma epidemiology, associated malignancies and Lynch/Muir-Torre syndrome screening in England from 2008 to 2018. J Am Acad Dermatol. 2023;89(6):1129–1135. doi:10.1016/j.jaad.2023.03.046
12. Sargen MR, Cahoon EK, Lynch CF, Tucker MA, Goldstein AM, Engels EA. Sebaceous carcinoma incidence and survival among solid organ transplant recipients in the United States, 1987-2017. JAMA Dermatol. 2020;156(12):1307–1314. doi:10.1001/jamadermatol.2020.3111
13. Sargen MR, Starrett GJ, Engels EA, Cahoon EK, Tucker MA, Goldstein AM. Sebaceous carcinoma epidemiology and genetics: emerging concepts and clinical implications for screening, prevention, and treatment. Clin Cancer Res. 2021;27(2):389–393. doi:10.1158/1078-0432.CCR-20-2473
14. Sargen MR, Mai ZM, Engels EA, et al. Ambient ultraviolet radiation and sebaceous carcinoma incidence in the United States, 2000-2016. JNCI Cancer Spectrum. 2020;4(2):pkaa020. doi:10.1093/jncics/pkaa020
15. Tripathi R, Chen Z, Li L, Bordeaux JS. Incidence and survival of sebaceous carcinoma in the United States. J Am Acad Dermatol. 2016;75(6):1210–1215. doi:10.1016/j.jaad.2016.07.046
16. Chang RC, Brunsgaard EK, Reid DC. Rural-urban differences in management and Survival of Sebaceous carcinoma: a National Cancer Database Analysis. J Am Acad Dermatol. 2025. doi:10.1016/j.jaad.2025.09.040
17. Patel A, Pawar O, Bordeaux JS. Factors associated with time to treatment for definitive surgery for sebaceous carcinoma. J Am Acad Dermatol. 2025;93(1):289–291. doi:10.1016/j.jaad.2025.03.061
18. Pleitz JL, Patel AB, Spires SE, Anderson FL, Aouad RK. A mass on the nasal dorsum. Sebaceous carcinoma (SC) of the nose. JAMA Otolaryngol Head Neck Surg. 2014;140(3):267–268. doi:10.1001/jamaoto.2013.6189
19. Kholaki O, Chang D, Kim RY. Nasal Sebaceous carcinoma: a case report and review of the literature. J Oral Maxillofacial Surg. 2020;78(1):82–86. doi:10.1016/j.joms.2019.08.011
20. Sukumaran Y, Lynn JCS, Baba FB, Dam V. Nasal Sebaceous Carcinoma - A Rare Presentation. Indian J Otolaryngol Head Neck Surg. 2024;76(2):2151–2154. doi:10.1007/s12070-023-04439-0
21. Tavanafar S, Gheibollahi H, Mousavi SS, Dehghanian A. Nasal sebaceous carcinoma: a rare case. National J Maxillofacial Surg. 2022;13(Suppl 1):S176–s178. doi:10.4103/njms.NJMS_245_20
22. Dasgupta S, Scott A, Skinner DW, Prichard AJ, Green NJ. Sebaceous carcinoma of the nasal vestibule. J Laryngology Otol. 2001;115(12):1010–1011. doi:10.1258/0022215011909620
23. Calvão J, Cardoso JC, Pinho A, Brinca A, Vieira R. Sebaceous carcinoma of the nose: for a difficult diagnosis, a challenging reconstruction. Dermatol Ther. 2020;33(6):e13841. doi:10.1111/dth.13841
24. Braunlich K, Wanner B, Miller R. Sebaceous carcinoma of the nose: a rare presentation of an uncommon tumor. Eplasty. 2019;19:ic11. doi:10.1258/002221504323086598
25. Coquillard C, Boustany A, DeCoster RC, Vasconez HC. Muir-Torre syndrome presenting as a Sebaceous carcinoma of the nasal ala. Am Surgeon. 2019;85(3):e115–e117. doi:10.1177/000313481908500301
26. Bae TH, Kim WJ, Woo SH, Kang SH, Kim HK. Sebaceous carcinoma of the nose reconstructed with a superiorly based folded nasolabial flap. J Craniofacial Surg. 2025;36:e1042–e1043. doi:10.1097/SCS.0000000000011663
27. Misago N, Narisawa Y. Sebaceous carcinoma with apocrine differentiation. Am J Dermatopathol. 2001;23(1):50–57. doi:10.1097/00000372-200102000-00009
28. Murphy J, Bleach NR, Thyveetil M. Sebaceous carcinoma of the nose: multi-focal presentation? J Laryngology Otol. 2004;118(5):374–376.
29. Kogame T, Ohe S, Yamazaki F, Okamoto H, Kiyohara T. Extraocular sebaceous carcinoma accompanied by invasive squamous cell carcinoma: the first case report and consideration of histogenesis. J Dermatol. 2018;45(4):501–504. doi:10.1111/1346-8138.14196
30. Wang JJ, Lee KF, Chen CY. Collision tumor of sebaceous carcinoma and squamous cell carcinoma of the eyelid: case report. Eur J Ophthalmol. 2022;32(5):Np55–np59. doi:10.1177/11206721211020649
31. Benedict KC, Al Hmada Y, Gordon C, Hoppe I. Squamous cell carcinoma admixed with sebaceous carcinoma of upper lip in a 7-year-old female. Pediatric Hematol Oncol J. 2022;7(4):126–129. doi:10.1016/j.phoj.2022.08.002
32. Zhang M, Lin Y, Han Z, et al. Exploring mechanisms of skin aging: insights for clinical treatment. Front Immunol. 2024;15:1421858. doi:10.3389/fimmu.2024.1421858
33. Rigel DS. Cutaneous ultraviolet exposure and its relationship to the development of skin cancer. J Am Acad Dermatol. 2008;58(5 Suppl 2):S129–132. doi:10.1016/j.jaad.2007.04.034
34. Plaza JA, Mackinnon A, Carrillo L, Prieto VG, Sangueza M, Suster S. Role of immunohistochemistry in the diagnosis of sebaceous carcinoma: a clinicopathologic and immunohistochemical study. Am J Dermatopathol. 2015;37(11):809–821. doi:10.1097/DAD.0000000000000255
35. Iacobelli J, Harvey NT, Wood BA. Sebaceous lesions of the skin. Pathology. 2017;49(7):688–697. doi:10.1016/j.pathol.2017.08.012
36. Starrett GJ, Baikie BC, Stoff BK, et al. Multiomics profiling distinguishes Sebaceous carcinoma from benign sebaceous neoplasms and provides insight into the genetic evolution of sebaceous carcinogenesis. Clin Cancer Res. 2024;30(21):4887–4899. doi:10.1158/1078-0432.CCR-24-1327
37. Utikal J, Nagel P, Müller V, et al. S1-guideline Sebaceous carcinoma. Journal der Deutschen Dermatologischen Gesellschaft. 2024;22(5):730–747.
38. Kim JYS, Kozlow JH, Mittal B, Moyer J, Olenecki T, Rodgers P. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78(3):560–578. doi:10.1016/j.jaad.2017.10.007
39. Rischin D, Migden MR, Lim AM, et al. Phase 2 study of cemiplimab in patients with metastatic cutaneous squamous cell carcinoma: primary analysis of fixed-dosing, long-term outcome of weight-based dosing. J Immunother Cancer. 2020;8(1):e000775. doi:10.1136/jitc-2020-000775
40. Maubec E, Boubaya M, Petrow P, et al. Phase II Study of Pembrolizumab as first-line, single-drug therapy for patients with unresectable cutaneous squamous cell carcinomas. J Clin Oncol. 2020;38(26):3051–3061. doi:10.1200/JCO.19.03357
41. Stratigos AJ, Garbe C, Dessinioti C, et al. European consensus-based interdisciplinary guideline for invasive cutaneous squamous cell carcinoma: Part 2. Treatment-update 2023. Eur J Cancer. 2023;193:113252. doi:10.1016/j.ejca.2023.113252
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Infantile Eosinophilic Pustular Folliculitis in a Child Aged 7 Years: A Case Report
Shi W, Lu Y, Zhou F, He H, Jiang J, Xue X
Clinical, Cosmetic and Investigational Dermatology 2023, 16:717-720
Published Date: 22 March 2023
Primary Sebaceous Carcinoma of the Eyebrow: A Case Report
Ye J, Li Q
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1715-1720
Published Date: 29 June 2023
Lymphocytic Thrombophilic Arteritis: A Case Report with a History of 67 Years
He Y, Feng S, Yao L, Zhang G
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2557-2559
Published Date: 19 September 2023
Type 1 Gaucher’s Disease. A Rare Genetic Lipid Metabolic Disorder Whose Diagnosis Was Concealed by Recurrent Malaria Infections in a 12-Year-Old Girl
Mitala Y, Birungi A, Mushabe B, Manzi J, Ssenkumba B, Atwine R, Ankunda S
Journal of Blood Medicine 2024, 15:1-7
Published Date: 20 January 2024
Metastatic Fibrolamellar Hepatocellular Carcinoma in a Young Adult: A Case Report and Narrative Review
El Darzi R, Ashy C, Khrayzat A, Chahine S, Tawil A, Temraz S
Journal of Hepatocellular Carcinoma 2026, 13:597439
Published Date: 6 May 2026