Back to Journals » Lung Cancer: Targets and Therapy » Volume 16
Comprehensive Survey of AACR GENIE Database of Tumor Mutation Burden (TMB) Among All Three Classes (I, II, III) of BRAF Mutated (BRAF+) NSCLC
Authors Arter ZL ![]() , Shieh K, Nagasaka M
, Shieh K, Nagasaka M ![]() , Ou SHI
, Ou SHI ![]()
Received 18 September 2024
Accepted for publication 6 February 2025
Published 19 February 2025 Volume 2025:16 Pages 1—9
DOI https://doi.org/10.2147/LCTT.S493835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Fengying Wu
Zhaohui Liao Arter,1,2 Kevin Shieh,1,2 Misako Nagasaka,1,2 Sai-Hong Ignatius Ou1,2
1Division of Hematology-Oncology, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA
Correspondence: Sai-Hong Ignatius Ou, Division of Hematology-Oncology, University of California Irvine School of Medicine, Orange, CA, USA, Tel +1 714-456-5153, Fax +1 714-456-2242, Email [email protected]
Background: BRAF mutations are generally divided into three classes based on the different altered mechanism of activation.
Methods: We queried the public AACR GENIE database (version 13.1), which includes tumor mutation burden (TMB) data, to explore potential molecular differences among the three classes of non-small cell lung cancer (NSCLC).
Results: Out of 20,713 unique NSCLC patients, 324 (1.6%) were BRAF mutations positive (BRAF+) class I, 260 (1.3%) class II, and 236 (1.1%) class III. The distribution of patient characteristics, including sex, age, and race, remains uniform across the three classes. The median TMB (mt/MB) was 6.5, 9.5, and 10.3 for class I, II, and III, respectively. The mean TMB was 61.5 ± 366.1 for class I, 40.5 ± 156.2 for class II, and 129.4 ± 914.8 for class III. About 30.5% of BRAF V600E+ patients had TMB ≥ 10; 47.7% of class II had TMB ≥ 10; and 52.5% of class III had TMB ≥ 10. For those patients with TMB ≥ 10, the median TMB was 45, 28.9, 18.4 for class I, II, and III, respectively. For TMB ≥ 10 patients, TP53 mutation was the most common co-alterations across all 3 classes.
Conclusion: A substantial proportion of BRAF+ NSCLC patients exhibited a TMB ≥ 10, among all three classes of BRAF mutation classification, including BRAF V600E+ NSCLC. Class III mutations appeared to have the highest median TMB, followed by class II, and then class I.
Keywords: target therapy, immunocheck point inhibitor (ICI), BRAF mutation, tumor mutation burden (TMB), class I, II, III mutations, NSCLC
Introduction
The landscape of actionable driver mutation in NSCLC is continuously evolving.1 Among the various actionable driver mutations that have US Food and Drug Administration (FDA) approved treatment, BRAF (v-Raf murine sarcoma viral oncogene homolog B1) V600E is one of these validated targets.
BRAF is an integral part of the RAS-RAF-MEK-ERK signaling cascade, a pathway central to cell differentiation, growth, and survival.2–5 Mutations in BRAF disrupt this tightly regulated pathway, fostering unchecked cell proliferation and tumorigenesis.6 BRAF mutations are observed in approximately 2–5% of NSCLCs.1,4,7 Importantly, BRAF mutations are categorically stratified into three classes, based on their signaling mechanisms from their underlying mutations.8–10 Class I is distinguished by its robust kinase activity that directly stimulates the MEK-ERK signaling cascade. Notably, this category encompasses the BRAF V600 mutation, recognized as a significant oncogenic driver in NSCLC. Class II are BRAF non-V600E mutations while still possessing kinase activity, they require dimerization with other RAF proteins to effectively transmit signals through the MEK-ERK pathway.11 Class III are also BRAF non-V600E mutations that are characterized by impaired kinase activity. They act as scaffolds to facilitate the activation of CRAF, another member of the RAF kinase family, thereby indirectly activating the downstream MEK-ERK signaling pathway.11 Those with BRAF V600 mutations seems to be more likely to be found in light or never-smokers compared with those with non-V600 mutations (42 versus 11%), and the prognosis was significantly better compared with non-V600 mutations (three-year survival rate, 24 versus 0%).12
Immune checkpoint inhibitors (ICIs), targeting the Programmed Death-1 (PD-1)/Programmed Death-Ligand 1 (PD-L1) axis, are the standard first-line therapy for most NSCLC patients without actionable mutations, either as monotherapy for high PD-L1 expression or combined with chemotherapy. While their efficacy in NSCLC with oncogenic alterations, including BRAF V600E mutations, is still under investigation, emerging evidence suggests potential activity in this subset.13 Tumor Mutation Burden (TMB) is an important biomarker for the selection of the use of ICIs in solid tumors.14–17 TMB expressed as the number of mutations per megabase (mut/Mb) of the genome examined offers a quantitative measure of the number of mutations within a tumor’s DNA. The higher the TMB the higher the genomic complexity of the tumor and in lung cancer usually represents previous smoking exposure.18 In the LC-SCRUM-Asia study, Sakai et al examined the TMB in 82 BRAF-mutated NSCLC samples and revealed that Class III BRAF mutations were associated with a higher median TMB compared to Class I (8.9 vs 3.7, p<0.01),19 highlighting a potential distinct molecular profile and pathogenesis among these three classes of BRAF mutations.
Currently, only BRAF V600E+ NSCLC has the FDA approved treatment - a combination regimen of a BRAF inhibitor and MEK inhibitor (dabrafenib + trametinib and encorafenib + binimetinib respectively). The other two classes (II and III) and within the class I BRAF mutations, the non-BRAF V600E mutants have no approved targeted treatment. We investigated TMB in BRAF mutations positive (BRAF+) NSCLC patients to assess the percentage of high TMB (≥10) BRAF+ NSCLC patients who could then potentially benefit from treatment with ICI.
Methods
Data Source and Extraction
The American Association for Cancer Research (AACR) Project Genomics Evidence Neoplasia Information Exchange (GENIE) (https://genie.cbioportal.org) is an ongoing international pan-cancer registry that has accumulated data from more than 110,000 tumors by April 2024 making it the largest repository of publicly accessible, clinically annotated genomic data. We accessed the GENIE version 13.1’s patient data, which included 148,222 patients and 167,358 samples.20 It was publicly released in June 2023 and was accessed in August 2023. In accordance with 45 CFR 46, it was determined that the present study was exempt from institutional review board review and the requirement for informed consent because it utilized publicly available deidentified data. This report follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for retrospective cross-sectional studies.
The database was queried for NSCLC patients exhibiting the three BRAF mutation classes. Class I: V600D/E/M/K/R; Class II: K601E/N/T, L597Q/V, G469A/V/R, G464V/E; Class III: D287H, V459L, G466A/E/V, S467L, G469E, N581S/I, D594A/G/H/N, F595L, G596D/R.21,22 We extracted variables of interest from the database, including demographic data (age at sequencing, sex, and race), data sources, and tumor characteristics.
TMB
TMB is not publicly listed but obtained from the AACR GENIE database statistician. The methods of how AACR GENIC generated TMB has been previously reported.23
Statistical Analysis
Data organization and analysis were conducted using Microsoft Excel (version 2306) and R Project (version 4.3.3). For continuous variable group comparisons, the Wilcoxon rank-sum test was used. Two-sided P < 0.05 was considered statistically significant.
Results
Distribution of the BRAF Mutations
Of the 20,713 NSCLC patients, we identified 1173 (5.8%) BRAF+ NSCLC patients: 324 patients (1.6%) with class I BRAF mutations, 260 patients (1.3%) with class II mutations, and 236 patients (1.1%) with class III mutations. Among the BRAF+ NSCLC, 25.8% were class I, 20.7% class II, 18.8% class III and 34.7% non-class I–III. The distribution of the BRAF mutations in all three classes is shown in Table 1 and Figure 1A–D. All class I to class III BRAF mutations are missense mutations. While the majority of non-class I–III BRAF mutations are also missense mutations (64.9%), they include other types of alterations such as fusions (9.9%), splice region mutations (4.8%), in-frame deletions (4.5%), nonsense mutations (4.2%), in-frame insertions (3.7%), splice site mutations (3.1%), frameshift insertions (2.8%), and frameshift deletions (2%).
 |
Table 1 Classification of BRAF Mutations |
 |
Figure 1 Pie chart on the frequency of class I, II, and III BRAF mutations. (A) Percentage of the 3 classes of BRAF mutations. (B) Frequency of individual class I BRAF mutations. (C) Frequency of individual class II BRAF mutations. (D) Frequency of individual class III BRAF mutations. |
Among 324 patients with class I mutations, predominantly were V600E (321 cases), with V600K and V600D found in 2 and 1 cases, respectively (Figure 1B). The class II group comprised 260 patients, including G469A (N = 114), K601E (N=50), G469V (N = 43), G464V (N = 24), K601N (N = 11), G469R (N = 11), L597Q (N = 6), and G464E (N = 2) (Figure 1C). Class III mutations were observed in 236 patients, including G466V (N = 66), N581S (N = 34), D594N (N = 34), D594G (N = 25), G596R (N = 20), G466A (N = 16), N581I (N = 14), G466E (N = 10), D594H (N = 6), G469E (N = 4), D594A (N = 3), V459L (N = 2), D287H (N = 1), S467L (N = 1), and F595L (N = 1) (Figure 1D).
Sex and Ethnicity Distribution
There were 190 female (58.6%) and 134 male (41.5%) in class I, with an average age of 67.4 ± 10.5. There were 147 female (56.5%) and 113 male (43.5%) in class II, with an average age of 69.0 ± 8.9. There were 117 female (49.6%), and 119 male (50.4%) in class III, with an average age of 67.6 ± 9.6 (Table 2). Smoking status was not captured in the database.
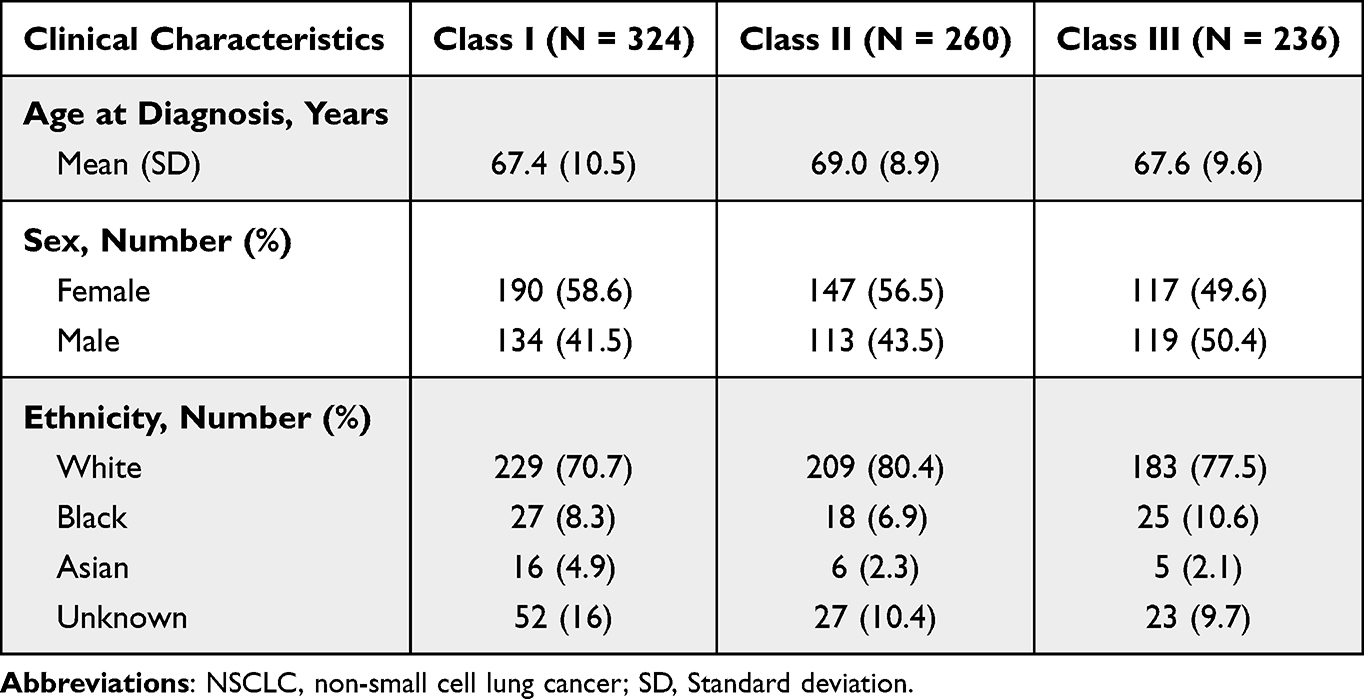 |
Table 2 Clinical Characteristics of Patients With BRAF-Mutant NSCLC by Mutation Class |
TMB Analysis
The median TMB (mt/MB) were 6.5, 9.5, and 10.3 for class I, II, and III BRAF+ NSCLC, respectively (Figure 2). Significant differences per Wilcoxon testing were observed between class I and II (p<0.001) in addition to class I and class III (p<0.001). The mean TMB was 61.5 ± 366.1 for class I, 40.5 ± 156.2 for class II, and 129.4 ± 914.8 for class III. About 30.5% of BRAF V600E had TMB ≥ 10; 47.7% of class II had TMB ≥ 10; and 52.5% of class III had TMB ≥ 10. For those patients with TMB ≥ 10, the median TMB was 45, 28.9, 18.4 for class I, II, and III, respectively.
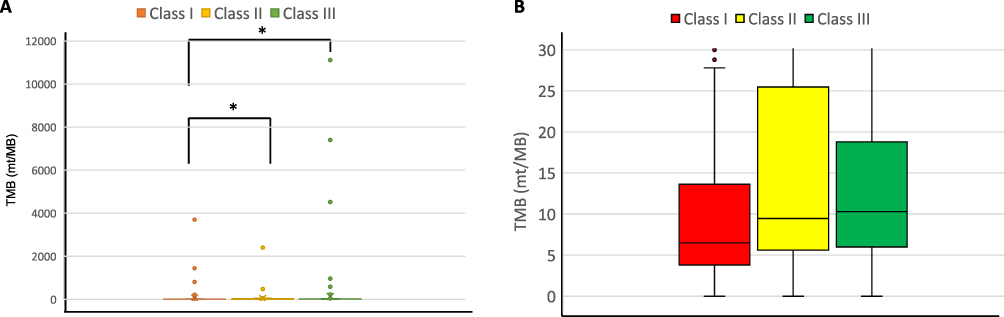 |
Figure 2 Box and whiskers plot of tumor mutation burden (TMB) in BRAF+ NSCLC by mutation class. (A) Median TMB (mut/Mb) values were 6.5, 9.5, and 10.3 for class I, II, and III BRAF+ NSCLC, respectively. Significant differences were observed between class I and class II (p = 2.092e-05) as well as class I and class III (p = 2.604e-07) based on Wilcoxon testing. (B) Zoomed-in view of the TMB range (0–30 mut/Mb) from (A), providing a detailed visualization of the data distribution within this range. Asterisk represents significant difference between classes. Abbreviations: NSCLC, non-small cell lung cancer; TMB, tumor mutation burden. |
The median TMB for TP53 mutations positive (TP53-mut)/BRAF+ class I NSCLC patients was 7.15, compared to a median of 6 for TP53 mutations negative (TP53-wt) class I NSCLC patients (P=0.009). In class II, the median TMB for TP53-mut was 12.7, compared to a median of 7.65 for TP53-wt patients (P=0.002). In class III, the median TMB for TP53-mut was 12.6, compared to a median of 7.9 for TP53-wt patients (P=0.007) (Figure 3). Among TP53-mut patients, both class II and class III demonstrated significantly higher median TMB compared to class I (P < 0.05).
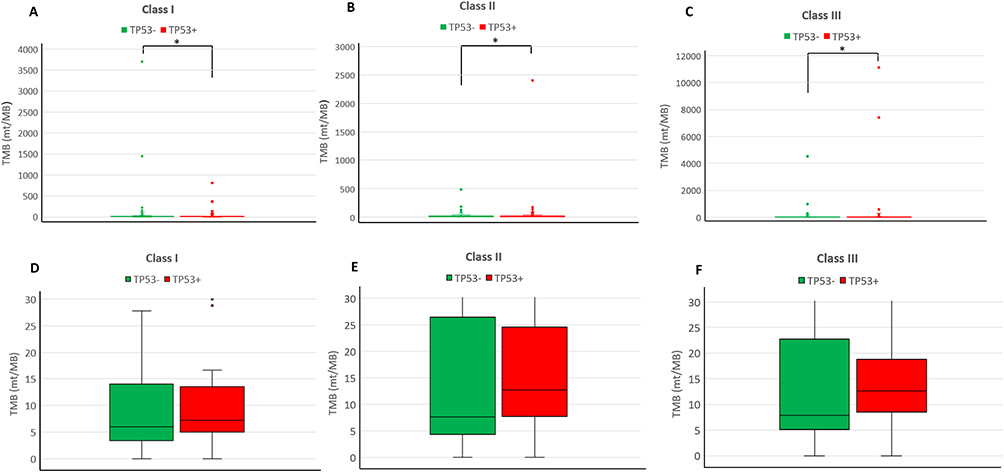 |
Figure 3 Box and whiskers plot of tumor mutation burden (TMB) in BRAF-mutant NSCLC by TP53 mutation status. (A) In Class I, the median TMB for TP53-mut patients was 7.15, compared to a median of 6 for TP53-wt patients. Significant differences were observed (P = 0.009, Wilcoxon test). (B) In Class II, the median TMB for TP53-mut was 12.7, compared to 7.65 for TP53-wt patients. Significant differences were observed (P = 0.002, Wilcoxon test). (C) In Class III, the median TMB for TP53-mut was 12.6, compared to 7.9 for TP53-wt patients. Significant differences were observed (P = 0.007, Wilcoxon test). (D–F) Detailed view of the TMB range (0–30 mut/Mb) as zoomed-in sections from (A–C) respectively. Asterisk represents significant difference between classes. Abbreviations: NSCLC, non-small cell lung cancer; TMB, tumor mutation burden; TP53-mut, TP53 mutations positive; TP53-wt, TP53 wild-type. |
Major Genomic Alteration Associated With High TMB in BRAF Class I-III mutations
The most common co-currence mutation with BRAF+ NSCLC was TP53 (49.4%), KRAS (17.7%) and STK11 (17.4%). In patients with a TMB≥ 10 within BRAF class I, the predominant concurrent alteration was observed in TP53 (42.6%), followed by SETD2 (13.8%). Among BRAF class II with a TMB ≥10, the most common co-alteration was TP53 (62.6%), followed by STK11 (20%) and EPHA3 (17.4%). For TMB ≥10 BRAF class III patients, the most common co-alteration was TP53 (71.2%), followed by KEAP1 (22.9%) and STK11 (20.3%) (Figure 4). The percentage of TP53 co-mutations increased progressively across the classes, from 42.6% in class I to 62.6% in class II, and 71.2% in class III.
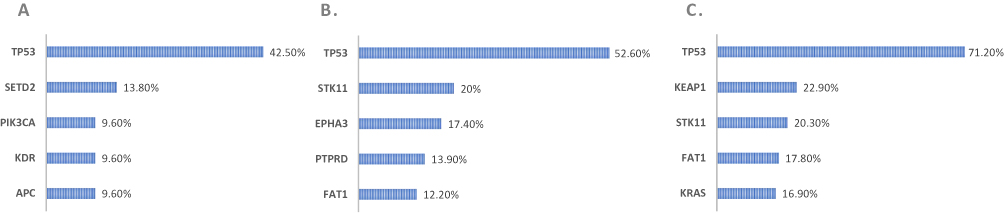 |
Figure 4 Common co-alterations in BRAF+ NSCLC by mutation class. (A) Common co-alterations in Class I. (B) Common co-alterations in Class II. (C) Common co-alterations in Class III. Abbreviation: NSCLC, non-small cell lung cancer. |
Discussion
Our exploration into the TMB across the three classes of BRAF+ NSCLC unveils genomic complexity unique to each class of BRAF mutations. The median TMB values for all three classes were relatively low, which aligns with findings from previous research.19 However, a significant proportion of BRAF+ NSCLC across all classes harboring a TMB of 10 or higher underscores TMBs as a biomarker for additional treatment with ICIs. High TMB is linked to increased neoantigen load, rendering tumors more recognizable to the immune system, and enhances the effectiveness of ICIs, as they work by unleashing the immune system’s ability to target and destroy cancer cells.15 Clinical studies have demonstrated that patients with high TMB (≥10) solid tumors experience better response rates and improved survival outcomes when treated with ICIs compared to those with lower TMB.24 This practical implication of these results is that many BRAF+ NSCLC patients could benefit from ICI. Our observation could potentially elucidate why BRAF+ NSCLC (both V600 and non-V600) demonstrates a more favorable response to immunotherapy than most driver oncogene NSCLC.13 While there were no differences in the progression free survival (PFS) for immunotherapy among the three subgroups,19,25,26 Bracht et al reported that treatment with chemotherapy plus immunotherapy resulted in lower PFS in class I BRAF+ NSCLC (median 1.8 months, N=3) compared to class II (6.1 months, N=3) and class III (5.0 months, N=3; one patient received osimertinib).27
The divergent TMB profiles across classes emphasize that a “one-size-fits-all” approach may be inadequate. The elevated TMB in class III, in particular, hints at underlying genomic instability or increased mutagenic processes and potentially a different underlying pathogenic pathways. Interestingly, our study also highlighted the significant variability within each class, particularly in class III, as evidenced by the high standard deviation in mean TMB. This suggests that even within each class, there is substantial molecular heterogeneity that could impact disease behavior and treatment responses. The use of next-generation sequencing is important not just to diagnose BRAF mutations but to determine the TMB.
Recent research has aimed at developing therapies for tumors with BRAF non-V600E mutations.28 A small retrospective series including patients with class II or III BRAF+ NSCLC found limited response to monotherapy with BRAF inhibitors, consistent with preclinical studies suggesting that these inhibitors are less effective against dimer-promoting BRAF variants. This observation is supported by clinical reports in melanoma where resistance to BRAF inhibitors has been linked to genetic alterations that promote RAF dimerization.29 Another study involving 3 patients with NSCLC harboring Class III BRAF mutations found that treatment with MEK inhibitors led to progressive disease in 2 patients, with only 1 patient achieving short-term disease stabilization.29 This underscores the complexity of these mutations and the imperative need for larger, prospective studies to evaluate the potential of MAPK-directed therapies and other novel treatment strategies for these specific molecular subsets. Hence, it is even more important to assay for TMB to provide potentially more than half of these patients with ICIs.
TP53, a gene commonly associated with tumor suppression, appears as the top co-alteration across all BRAF classes, with its prevalence increasing from class I to class III. The presence of TP53 mutations in a significant majority may potentially negatively modulate the response to targeted therapy and warrants further investigation. For class II, the co-alteration in STK11 (20%) may influence response to immunotherapy, as STK11 mutations have been associated with resistance to ICIs in lung cancer.30,31 BRAF class III harbors the highest percentage of TP53 co-mutations (71.2%), indicating a potential for a more aggressive tumor profile. KRAS mutations (16.9%) in this group could imply a subset of tumors that may not respond to standard therapies targeting BRAF alone due to the involvement of KRAS in alternate proliferative signaling pathways.
Within each class of BRAF mutations, TP53 positivity exhibited a higher median TMB than those with TP53 negativity. Especially in class II and III BRAF mutations, where the median TMB of TP53 positivity was greater than 10, a threshold for use of ICIs. This may suggest that TP53 mutations are linked to an increased TMB, as reported in the previous study32 or potential a positive smoking history which was not systemically captured in the AACR GENIE database.
Limitations
First, TMB was calculated from different sequencing platforms used by the reporting institutions which may explain the large range of TMB reported. Second, the smoking history was not captured as this is important etiology and prognostic factor in NSCLC. High TMB and/or TP53-mut may refelct a smoking history which would add further confidence in the anticipated efficacy of ICIs. Third, the lack of treatment outcome data limited further insight into how TMB and the three classes of mutations interact. Finally, the study is constrained by the lack of reported PD-L1 expression levels within the GENIE dataset, which is another predictive factor for the efficacy of ICIs.
Conclusion
Our analysis of the AACR GENIE database reveals a complex and heterogeneous molecular landscape of BRAF + NSCLC. A large proportion of BRAF+ NSCLC harbored a high TMB (≥10) regardless of the classification of the mutations. Class I BRAF+ NSCLC may benefit from additional ICI if the TMB ≥10. For class II and III BRAF+ NSCLC, given the lack of approved targeted therapies, ICIs are likely the standard of care. However, future targeted therapies, such as a pan-RAS inhibitor, may potentially be combined with ICIs.
Abbreviations
AACR, American Association for Cancer Research; BRAF, V-Raf Murine Sarcoma Viral Oncogene Homolog B; BRAF+, BRAF mutations positive; FDA, Food and Drug Administration; GENIE, Genomics Evidence Neoplasia Information Exchange; ICI, Immunocheck Point Inhibitor; MSI/MMR, Microsatellite Instability/Mismatch Repair; NSCLC, Non-Small Cell Lung Cancer; PD-L1, Programmed Death-Ligand 1; PFS, Progression Free Survival; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; TMB, Tumor Mutation Burden; TP53-mut, TP53 mutations positive; TP53-wt, TP53 wild-type.
Data Sharing Statement
The data utilized in this research is publicly available except for the tumor mutation burden (TMB) which was obtained from the AACR GENIE database statistician.
Ethics Approval and Consent to Participate
In accordance with 45 CFR 46, it was determined that the present study was exempt from institutional review board review and the requirement for informed consent because it utilized publicly available deidentified data. This report follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for retrospective cross-sectional studies.
Consent for Publication
This is an observational study involving analysis of secondary data only. All data were deidentified. There was no direct interaction with human subjects for this study.
Acknowledgments
We wish to express our sincere appreciation to Ms. Jennifer Hoppe and the AACR Genie team for their indispensable assistance and support in providing access to, and guidance with, the Tumor Mutational Burden (TMB) data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
Dr. Ou has received speaker bureau honoraria from Pfizer, Janssen/JNJ, DAVA Oncology LLP, and OncLive. He also holds advisory board roles with AnHeart Therapeutics, Pfizer, Janssen/JNJ, Daiichi Sankyo, BMS, and Elevation Oncology, for which he receives honoraria. Additionally, he serves on the scientific advisory boards for Elevation Oncology and AnHeart Therapeutics and has ownership in MBrace Therapeutics, Nuvalent, Nuvation, and BlossomHill Therapeutics. Dr Nagasaka has received consulting fees from Caris Life Sciences, honoraria from AstraZeneca, Daiichi Sankyo, Novartis, Lilly, Pfizer, EMD Serono, Genentech, Regeneron and BMS. She is a speaker for Mirati, Takeda, Janssen, and Blueprint Medicine and has received travel support from AnHeart Therapeutics. The authors report no other conflicts of interest in this work.
The abstract of this paper was presented at the ESMO Asia Conference 2023 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Annals of Oncology, Annals of Oncology, Volume 34, S1687–S1688, as “559P Comprehensive survey of AACR GENIE database revealed a wide range of TMB distribution among all three classes (I, II, III) of BRAF mutated NSCLC”.
References
1. Harada G, Yang SR, Cocco E, Drilon A. Rare molecular subtypes of lung cancer. Nat Rev Clin Oncol. 2023;20(4):229–249. doi:10.1038/s41571-023-00733-6
2. Luk PP, Yu B, Ng CC, et al. BRAF mutations in non-small cell lung cancer. Transl Lung Cancer Res. 2015;4:142–148.
3. Holderfield M, Deuker MM, McCormick F, McMahon M. Targeting RAF kinases for cancer therapy: BRAF-mutated melanoma and beyond. Nat Rev Cancer. 2014;14:455–441467. doi:10.1038/nrc3760
4. Marchetti A, Felicioni L, Malatesta S, et al. Clinical features and outcome of patients with non-small-cell lung cancer harboring BRAF mutations. J Clin Oncol. 2011;29:3574–3579. doi:10.1200/JCO.2011.35.9638
5. Paik PK, Arcila ME, Fara M, et al. Clinical characteristics of patients with lung 446 adenocarcinomas harboring BRAF mutations. J Clin Oncol. 2011;29:2046–2051. doi:10.1200/JCO.2010.33.1280
6. Owsley J, Stein MK, Porter J, et al. Prevalence of class I–III BRAF mutations among 114,662 cancer patients in a large genomic database. Exp Biol Med. 2021;246:31–39. doi:10.1177/1535370220959657
7. Villaruz LC, Socinski MA, Abberbock S, et al. Clinicopathologic features and outcomes of patients with lung adenocarcinomas harboring BRAF mutations in the lung cancer mutation consortium: BRAF mutations in lung adenocarcinomas. Cancer. 2015;121:448–456. doi:10.1002/cncr.29042
8. Yao Z, Yaeger R, Rodrik-Outmezguine VS, et al. Tumours with class 3 BRAF mutants are sensitive to the inhibition of activated RAS. Nature. 2017;548:234–238. doi:10.1038/nature23291
9. Wan PT, Garnett MJ, Roe SM, et al. Mechanism of activation of the RAF-ERK signaling pathway by oncogenic mutations of B-RAF. Cell. 2004;116:855–867. doi:10.1016/S0092-8674(04)00215-6
10. Yao Z, Torres NM, Tao A, et al. BRAF mutants evade ERK-dependent feedback by different mechanisms that determine their sensitivity to pharmacologic inhibition. Cancer Cell. 2015;28:370–383. doi:10.1016/j.ccell.2015.08.001
11. Johnson B, Kopetz S. Applying precision to the management of BRAF-mutant metastatic colorectal cancer. Target Oncol. 2020;15(5):567–577. doi:10.1007/s11523-020-00747-5
12. Litvak AM, Paik PK, Woo KM, et al. Clinical characteristics and course of 63 patients with BRAF mutant lung cancers. J Thorac Oncol. 2014;9(11):1669. doi:10.1097/JTO.0000000000000344
13. Mazieres J, Drilon AE, Mhanna L, et al. Efficacy of immune-checkpoint inhibitors (ICI) in non-small cell lung cancer (NSCLC) patients harboring activating molecular alterations (ImmunoTarget). Ann Oncol. 2019;30(8):1321–1328. doi:10.1093/annonc/mdz167
14. Goodman A, Kato S, Bazhenova L, et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. mol Cancer Ther. 2017;16(11):2598–2608. doi:10.1158/1535-7163.MCT-17-0386
15. Samstein R, Lee C, Shoushtari A, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet. 2019;51(2):202–206. doi:10.1038/s41588-018-0312-8
16. Rizvi N, Hellmann M, Snyder A, et al. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015;348(6230):124–128. doi:10.1126/science.aaa1348
17. Hellmann M, Nathanson T, Rizvi H, et al. Genomic features of response to combination immunotherapy in patients with advanced non-small-cell lung cancer. Cancer Cell. 2018;33(5):843–852.e4. doi:10.1016/j.ccell.2018.03.018
18. Chalmers Z, Connelly C, Fabrizio D, et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017;9(1):34. doi:10.1186/s13073-017-0424-2
19. Sakai T, Matsumoto S, Ueda Y, et al. Clinicogenomic features and targetable mutations in NSCLCs harboring BRAF non-V600E mutations: a multi-institutional genomic screening study (LC-SCRUM-Asia). J Thorac Oncol. 2023;18(11):1538–1549. doi:10.1016/j.jtho.2023.07.024
20. Gouda MA, Nelson BE, Buschhorn L, Wahida A, Subbiah V. Tumor-agnostic precision medicine from the AACR GENIE database: clinical implications. Clin Cancer Res. 2023;29:2753–2760. doi:10.1158/1078-0432.CCR-23-0090
21. Śmiech M, Leszczyński P, Kono H, Wardell C, Taniguchi H. Emerging BRAF mutations in cancer progression and their possible effects on transcriptional networks. Genes. 2020;11(11):1342. doi:10.3390/genes11111342
22. Dankner M, Rose A, Rajkumar S, Siegel P, Watson L. Classifying BRAF alterations in cancer: new rational therapeutic strategies for actionable mutations. Oncogene. 2018;37(24):3183–3199. doi:10.1038/s41388-018-0171-x
23. Anaya J, Sidhom JW, Cummings CA, Baras AS; AACR Project GENIE Consortium. Probabilistic mixture models improve calibration of panel-derived tumor mutational burden in the context of both tumor-normal and tumor-only sequencing. Cancer Res Commun. 2023;3(3):501–509. doi:10.1158/2767-9764.CRC-22-0339
24. Aggarwal C, Ben R, Gao Y, et al. Assessment of tumor mutational burden and outcomes in patients with diverse advanced cancers treated with immunotherapy. JAMA Netw Open. 2023;6(5):e2311181. doi:10.1001/jamanetworkopen.2023.11181
25. Murciano-Goroff YR, Pak T, Mondaca S, et al. Immune biomarkers and response to checkpoint inhibition of BRAF(V600) and BRAF non-V600 altered lung cancers. Br J Cancer. 2022;126:889–898. doi:10.1038/s41416-021-01679-1
26. Guisier F, Dubos-Arvis C, Viñas F, et al. Efficacy and safety of anti-PD-1 immunotherapy in patients with advanced NSCLC with BRAF, HER2, or MET490 mutations or RET translocation: GFPC 01-2018. J Thorac Oncol. 2020;15:628–636. doi:10.1016/j.jtho.2019.12.129
27. Bracht J, Karachaliou N, Bivona T, et al. BRAF mutations classes I, II, and III in NSCLC patients included in the SLLIP trial: the need for a NewPre-clinical treatment rationale. Cancers. 2019;11(9):1381. doi:10.3390/cancers11091381
28. Dankner M, Lajoie M, Moldoveanu D, et al. Dual MAPK inhibition is an effective therapeutic strategy for a subset of class II BRAF mutant melanomas. Clin Cancer Res. 2018;24:6483–6494. doi:10.1158/1078-0432.CCR-17-3384
29. Dagogo-Kack I, Award M, Shaw A. RAF mutation class and clinical outcomes-response. Clin Cancer Res. 2019;25(10):3189. doi:10.1158/1078-0432.CCR-19-0422
30. Pons-Tostivint E, Lugat A, Fontenau JF, Denis MG, Bennouna J. STK11/LKB1 modulation of the immune response in lung cancer: from biology to therapeutic impact. Cells. 2021;10(11):3129. doi:10.3390/cells10113129
31. Skoulidis F, Goldberg ME, Greenawalt DM, et al. STK11/LKB1 mutations and PD-1 inhibitor resistance in KRAS-mutant lung adenocarcinoma. Cancer Discov. 2018;8(7):822–835. doi:10.1158/2159-8290.CD-18-0099
32. Li H, Yang L, Wang Y, et al. Integrative analysis of TP53 mutations in lung adenocarcinoma for immunotherapies and prognosis. BMC Bioinf. 2023;24(1):155. doi:10.1186/s12859-023-05268-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.