Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Comprehensive Geriatric Assessment and Geriatric Interdisciplinary Team Care Model: An Integrated Model for Older Adults
Authors Wu Y ![]() , Yang L, Sha Y, An Y, Li W, Hu X, Yang G, Chen X
, Yang L, Sha Y, An Y, Li W, Hu X, Yang G, Chen X
Received 16 April 2026
Accepted for publication 4 June 2026
Published 17 June 2026 Volume 2026:19 612972
DOI https://doi.org/10.2147/JMDH.S612972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Yinrun Wu, Lei Yang, Yanmei Sha, Yangxin An, Weijuan Li, Xueqin Hu, Gangyu Yang, Xiaoyun Chen
Department of Geriatrics, Dali Bai Autonomous Prefecture People’s Hospital, Dali, Yunnan, People’s Republic of China
Correspondence: Xiaoyun Chen, Department of Geriatrics, Dali Bai Autonomous Prefecture People’s Hospital, Dali, Yunnan, People’s Republic of China, Email [email protected]
Abstract: Accelerated global population aging has been accompanied by multimorbidity, progressive decline in organ function, and complex psychosocial conditions among older adults, which collectively place substantial pressure on conventional single-disease–oriented care models. Comprehensive Geriatric Assessment (CGA), defined as a multidimensional and interdisciplinary diagnostic process, in combination with a Geriatric Interdisciplinary Team (GIT) structured around patient-centered care, represents a principal strategy to address these challenges. This narrative review synthesized literature from PubMed, Web of Science, and CNKI (up to December 2025) using keywords including “comprehensive geriatric assessment”, “multidisciplinary team”, and “integrated care”. This review synthesizes the theoretical framework, key components, and implementation pathways of this integrated care model. The underlying conceptual foundations and core principles are examined, with particular attention to critical steps and operational approaches during implementation. Evidence regarding clinical outcomes is evaluated alongside current limitations and future directions. This work aims to provide a conceptual basis and practical reference for the development of efficient and sustainable geriatric integrated care systems.
Keywords: comprehensive geriatric assessment, multidisciplinary team, integrated care, older adults, China
Introduction
With ongoing demographic aging worldwide, the complexity of healthcare delivery for older populations continues to increase. Comprehensive Geriatric Assessment (CGA) is a structured, interdisciplinary diagnostic approach. It focuses on the systematic identification of functional capacity and latent problems in older individuals. These problems span four key domains: physical, functional, psychological, and social.1 CGA transcends the mere aggregation of clinical data; instead, it functions as the cornerstone for formulating holistic management protocols. By leveraging CGA, clinicians can effectively devise and execute care pathways that are both synchronized and seamlessly integrated.2 Among older patients presenting to emergency settings, frailty is highly prevalent and typically manifests as geriatric syndromes such as falls, delirium, fatigue, and restricted mobility. In this context, CGA provides an effective framework for evaluating and managing the overall condition of frail individuals.3 Evidence from community and outpatient settings indicates that implementation of CGA is associated with improved maintenance of independent living and reduced hospitalization rates.1 Beyond clinical benefits, CGA aligns with evolving healthcare demands.1
The Geriatric Interdisciplinary Team (GIT) constitutes another essential component in addressing the complexity of geriatric care.4 Through collaboration among professionals from diverse disciplines, GIT enables the development and execution of individualized care plans. The value of this collaborative approach is evident across multiple clinical settings. In geriatric oncology, international recommendations advocate multidisciplinary assessment to refine treatment strategies and align interventions with heterogeneous aging trajectories.5 Evidence indicates that CGA contributes to improved therapeutic effectiveness, supports individualized care planning, and enhances quality of life as well as functional outcomes.6 In specific domains such as gastrointestinal malignancies, integration of geriatric assessment has been associated with improved treatment tolerance, reduced complications, and alignment of therapeutic goals with patient preferences.6 In the management of osteoporotic fragility fractures, fracture liaison services involving multidisciplinary teams incorporate comprehensive evaluation of fracture risk factors together with multidimensional geriatric assessment, These methods have improved efficiency in osteoporosis management, anti-fracture therapy, and supplementation with vitamin D and calcium.7 These findings underscore the central role of interdisciplinary collaboration in managing multimorbidity and complex health conditions in older populations.
Systematic integration of CGA with GIT-based care represents a necessary direction for improving healthcare quality, enhancing patient outcomes, and optimizing resource allocation in geriatric medicine. Within this integrated care model, comprehensive assessment findings inform the development of targeted intervention strategies, generating synergistic effects across disciplines. Among community-dwelling older adults at high risk of frailty, CGA has been associated with reduced risk of unplanned hospitalization.2 In emergency care settings, transitional care models such as ED PLUS, led by physiotherapists, initiate CGA at the point of emergency contact and extend care through multidisciplinary follow-up, thereby facilitating care transition between emergency and community settings and improving patient’s quality of life.8 For older trauma patients, early intervention, intensive care management, appropriate triage, and age-adapted assessment are essential components of care, highlighting the importance of interdisciplinary strategies in optimizing trauma management and resource utilization.9
Healthy aging extends beyond clinical outcomes to encompass quality of life, emotional well-being, and social participation.10 The health of older adults is closely intertwined with that of their informal caregivers, as caring for individuals with dementia is associated with a decline in caregivers’ cognitive and physical health.11 Physical exercise programs incorporating cognitive tasks can improve patient–caregiver outcomes and reduce caregiver burden.12
Comprehensive Geriatric Assessment (CGA) is specifically designed to assess these multidimensional aspects of aging and caregiving. As a structured, interdisciplinary approach, CGA systematically evaluates physical, functional, psychological, and social domains, thereby directly aligning with the determinants of quality of life and healthy aging. The Geriatric Interdisciplinary Team (GIT) then translates these assessments into patient-centered interventions that address both patient and caregiver needs. Together, the integrated CGA-GIT model operationalizes healthy aging principles by addressing the full spectrum of older adults’ needs, from disease management to social participation and caregiver support.
Despite the recognized value of CGA and GIT individually, a systematic theoretical framework that integrates both into a coherent, implementable model remains lacking. Specifically, three key gaps persist: (1) the absence of standardized implementation pathways for CGA-MDT integration across diverse healthcare settings; (2) limited evidence on comprehensive outcome measures that capture both clinical and health-system impacts; and (3) a lack of strategies for scaling integrated models from high-resource to routine practice settings. This review aims to address these gaps by proposing a conceptual framework for CGA-GIT integration, delineating practical implementation pathways, and identifying future research priorities.
Theoretical Framework and Core Principles of the Integrated Care Model
Conceptual Foundations and Assessment Domains of CGA
CGA represents a structured approach that extends beyond the conventional biomedical paradigm and is grounded in core principles of geriatric medicine. Its conceptual basis lies in the identification and management of conditions such as geriatric syndromes, frailty, and functional impairment, with emphasis placed on a global understanding of health status rather than a disease-specific focus.3 As a standardized, multidimensional, and interdisciplinary approach, CGA supports early detection of geriatric syndromes, including frailty, and informs the development of individualized care plans.1,13 The scope of assessment encompasses multiple domains, including physical health (eg., comorbidities and polypharmacy), functional capacity (eg., activities of daily living (ADL), instrumental activities of daily living (IADL), gait, and balance), cognitive and psychological status (eg., cognitive function, depression, anxiety), as well as social and environmental conditions (eg., social support, financial resources, living environment), together with quality of life (QoL).1 International consensusfurther supports the central role of CGA in geriatric practice. The European Geriatric Medicine Society (EuGMS) has formally endorsed CGA as the cornerstone of geriatric care, recommending its use for frailty assessment, clinical decision-making, and rehabilitation planning across both geriatric and non-geriatric settings.14 Similarly, the American Geriatrics Society (AGS) guidelines advocate for CGA as the standard for multidimensional health status evaluation in older adults.15 Among older individuals with chronic kidney disease, application of CGA enables identification of depression and malnutrition as factors associated with increased mortality risk, thereby contributing to more refined risk stratification.16
Theoretical Basis and Team Structure of the GIT
GIT is conceptually derived from systems theory, team science, and the framework of patient-centered care. It relies on coordinated interaction and complementarity among professionals from diverse disciplines, generating a synergistic effect that addresses the complex and multidimensional healthcare needs of older adults.4 Within geriatric oncology, such collaboration is considered essential for optimizing treatment strategies and aligning clinical decisions with individualized care pathways.5 The core team typically includes geriatricians, nurses, clinical pharmacists, rehabilitation therapists, dietitians, social workers, and mental health professionals. Clearly defined roles, responsibilities, and communication mechanisms are fundamental to effective team performance. For instance, in fracture liaison service models for fragility hip fractures, interdisciplinary teams conduct comprehensive evaluations to identify risk factors for subsequent fractures and assess multidimensional geriatric syndromes, including muscle status, which informs anti-fracture treatment strategies and structured follow-up.7 Effective team function depends on shared objectives, regular structured meetings, transparent decision-making processes, and a culture characterized by mutual respect and trust. This collaborative environment provides the organizational foundation for the operation of the integrated care model.
Core Concepts and Operational Mechanisms of the Integrated Care Model
Within the integrated care model, CGA functions as the driving mechanism for problem identification, whereas GIT serves as the operational framework for problem resolution, enabling seamless linkage between assessment and intervention within a continuous care cycle. CGA extends beyond assessment alone; it informs comprehensive care planning and directs implementation of targeted interventions.2 Operationally, CGA findings initiate GIT involvement, while a designated coordinator—typically a geriatric nurse or case manager—oversees implementation, follow-up, and reassessment to maintain continuity of care, care coordination, and individualization. This mechanism is essential for addressing the dynamic and evolving needs of older patients. Qualitative evidence further indicates that CGA in community and outpatient settings represents an integrated assessment process in which evaluation of the home environment enhances overall effectiveness, and collaborative care approaches support its implementation.17 A CGA-driven and GIT-executed framework therefore constitutes the central mechanism for delivering individualized and continuous geriatric care.
Practical Pathways and Key Components of the Integrated Care Model
Initiation of Assessment and Information Integration Processes
Implementation of the integrated care model begins with systematic identification of older individuals at high risk. Across diverse care settings, including emergency departments, outpatient clinics, and inpatient units, the application of efficient screening tools constitutes the initial step toward comprehensive assessment. In emergency settings, frailty is frequently encountered and is associated with increased risk of adverse events, often presenting as geriatric syndromes such as falls, delirium, and restricted mobility; early identification and stratification are therefore essential for subsequent management.3 Once individuals requiring further evaluation are identified, standardized CGA is conducted as the central component of the process. Ensuring the effectiveness of assessment and continuity of information transfer requires structured documentation systems together with an information integration platform. Standardized electronic CGA templates, combined with shared EHRs, support effective dissemination of assessment findings across GIT members and form the basis of integrated care delivery.1 Establishment of clearly defined referral criteria and pathways enables seamless exchange of assessment information across multiple care settings, including hospitals, community services, and long-term care institutions, thereby reducing redundant assessments, minimizing data silos, and maintaining continuity of care. Evidence from community and outpatient settings indicates that CGA incorporating home environment evaluation and collaborative care approaches improves comprehensiveness of assessment while increasing patient satisfaction and access to healthcare services.17
Multidisciplinary Team Meetings and Development of Individualized Care Plans
Regular GIT meetings represent a central operational component of the integrated care model, serving as the primary interface through which assessment findings are translated into actionable strategies. These meetings follow a structured agenda. The coordinator typically presents key CGA findings at the outset, after which team members—including geriatricians, nurses, rehabilitation therapists, dietitians, clinical pharmacists, and social workers—contribute discipline-specific perspectives, refine assessments, and raise relevant clinical considerations.5 This structured format supports comprehensive information exchange and enables multidimensional characterization of patient status. Based on this collective evaluation, the team defines a prioritized list of clinical issues and, through collaborative deliberation, establishes a unified, feasible, and goal-oriented individualized care plan. The plan encompasses multiple domains, including optimization of clinical management (eg., comorbidity management and medication review), functional rehabilitation, nutritional support, social support, and broader care planning strategies.2 Alignment with patient values requires active engagement of both patients and their families; clear communication ensures understanding and agreement regarding the proposed care plan. This step is fundamental to patient-centered care and contributes directly to improved adherence and satisfaction. Evidence from qualitative synthesis in community and outpatient CGA settings indicates that meaningful involvement of older individuals and their caregivers during the CGA process is associated with enhanced care experience and improved outcomes.17
Execution, Coordination, and Iterative Reassessment
Effective execution of the care plan requires clearly defined responsibilities and specified timelines. Within this process, the coordinator assumes a central role, monitoring implementation, coordinating across service providers—including hospitals, community rehabilitation services, and home care—and acting as the principal liaison between patients and the GIT.8 Robust communication and feedback mechanisms are essential to maintain continuity of care. Approaches such as shared task lists, scheduled telephone follow-up, and home visits enable early identification of barriers and support timely resolution, ensuring that planned interventions are carried out as intended. The integrated care model operates as a dynamic process rather than a single intervention. Ongoing reassessment, guided by clinical status and response to interventions, is required to maintain effectiveness. Among community-dwelling older individuals at high risk of frailty, CGA-based reassessment may be conducted at intervals of 3–6 months, with subsequent modification of the care plan according to updated findings, thereby sustaining an iterative cycle of assessment, intervention, and reassessment.2 For older patients discharged from emergency care, initiation of CGA combined with multidisciplinary follow-up supports care transition across settings and contributes to improved post-discharge outcomes.8,18 Reassessment extends beyond clinical indicators to include evaluation of healthcare utilization, particularly unplanned readmission rates, which serve as key indicators of long-term effectiveness of the integrated care model.19
Based on the theoretical foundation outlined above and the analysis of practical implementation considerations, we propose an integrated operational framework for CGA-GIT (Comprehensive Geriatric Assessment-Geriatric Interdisciplinary Team). The integrated CGA-GIT care pathway is illustrated in Figure 1.
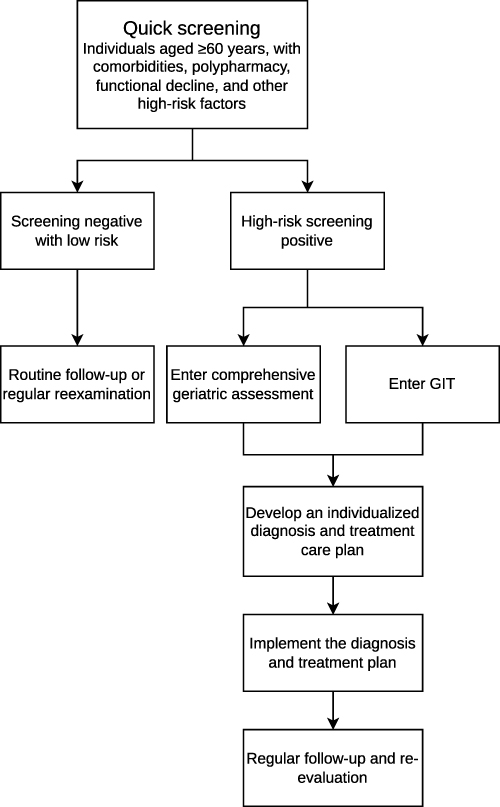 |
Figure 1 Integrated CGA-GIT care model pathway for older adults. The pathway consists of five sequential steps: Screening (Step 1) for rapid identification of high-risk older adults using validated tools (e.g., FRAIL, ICOPE); Comprehensive Geriatric Assessment (Step 2) for multidimensional evaluation of medical, functional, cognitive, nutritional, and psychosocial domains; And Geriatric Interdisciplinary Team diagnosis and treatment; Develop an individualized diagnosis and treatment care plan (Step 3); and Implementation (Step 4) and follow-up (Step5) for executing the care plan with regular reassessment and adjustment. |
Outcomes Evaluation, Challenges, and Future Directions
Clinical Outcomes and Health Economic Evaluation of the Integrated Care Model
Accumulating evidence indicates that integration of CGA with GIT-based care is associated with measurable improvements in clinical outcomes, more efficient healthcare utilization, and enhanced cost-effectiveness in older populations. In terms of clinical outcomes, the integrated care model is linked to reductions in mortality and unplanned readmission rates.19 A systematic review focusing on community-dwelling older individuals at high risk of frailty reported that CGA-based interventions may reduce the risk of unplanned hospitalization.2 The landmark meta-analysis by Stuck et al including 28 controlled trials and nearly 10,000 participants demonstrated that CGA programmes with strong long-term management improve survival and functional outcomes in older persons (OR for living at home at follow-up: 1.68 for geriatric evaluation and management units.20 Limited evidence from single-center studies suggests potential benefits of CGA in outpatient settings, though findings remain preliminary.21 Improvements have also been observed in the management of geriatric syndromes, including frailty, falls, and delirium, particularly in acute care environments where early identification and proactive management are essential.3 It has been proposed that integrating CGA with GIT improves care coordination, although robust data from large-scale trials are currently lacking.22 From the perspective of patient-reported outcomes (PROs), comprehensive and coordinated care planning contributes to increased quality of life and higher levels of patient satisfaction.17 With regard to healthcare utilization, delivery of the integrated care model is associated with reduced consumption of medical resources. Economic evaluations further indicate that CGA demonstrates alignment with evolving healthcare demands while maintaining clinical benefit.1 Nevertheless, evidence regarding effectiveness across inpatient, outpatient, and diverse cultural settings remains limited, highlighting the need for high-quality studies with extended follow-up. Future evaluations should incorporate multidimensional outcome measures, including clinical outcomes, PROs, healthcare utilization metrics, and cost-effectiveness analyses, to enable comprehensive assessment of the value of the integrated care model.
Major Challenges and Barriers to Implementation of the Integrated Care Model
The major challenges and barriers to implementation of the integrated care model are summarized in Table 1, spanning system-level, organizational-level, and professional/cultural-level domains.
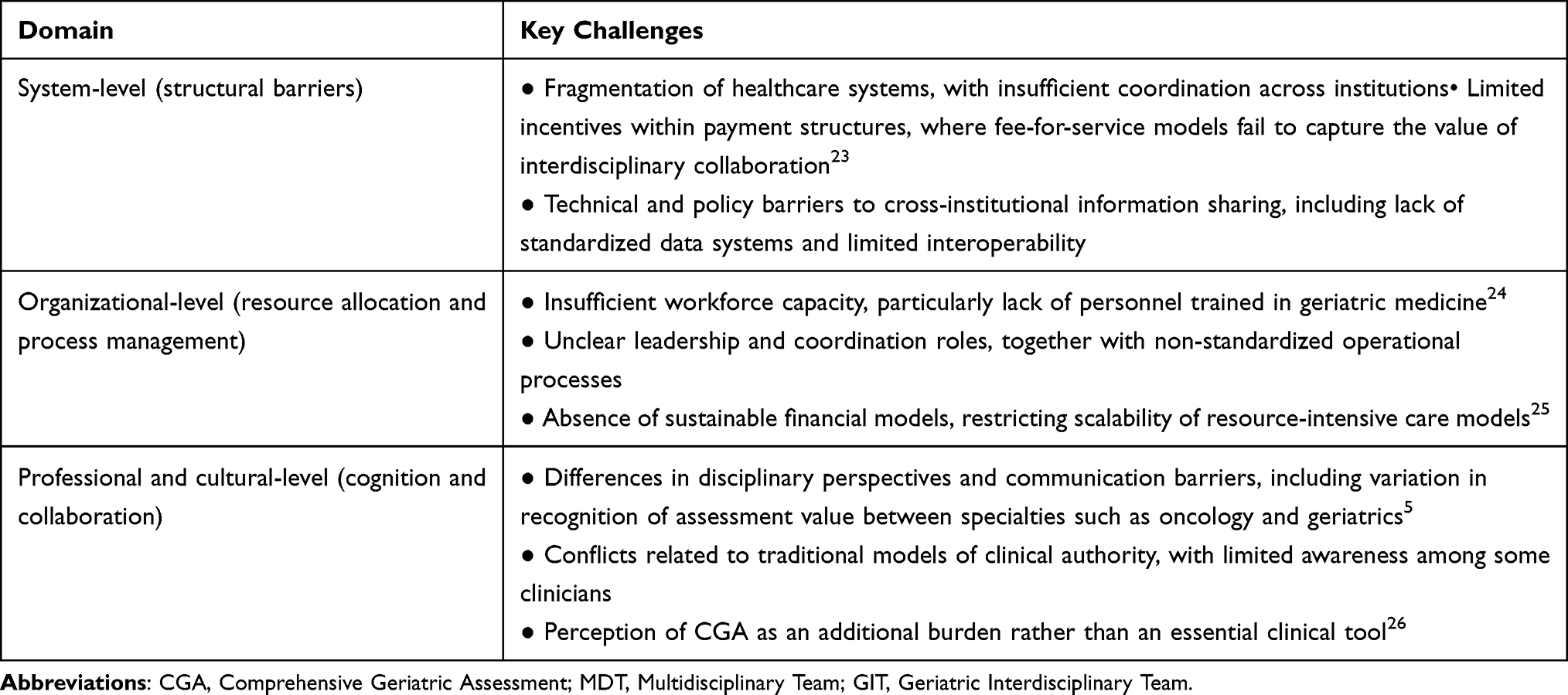 |
Table 1 Major Challenges in the Implementation of the Integrated Care Model Based on CGA and GIT |
Future Optimization and Development Directions
The mode Advancement from conceptual frameworks to routine clinical practice requires focused efforts in several key domains, as summarized in Table 2:
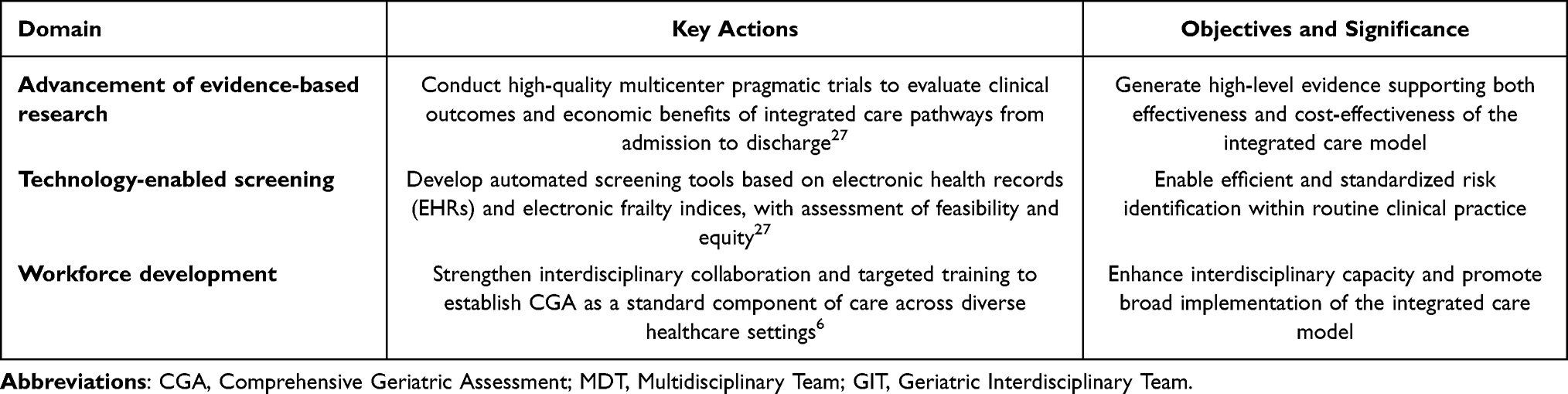 |
Table 2 Future Directions of the Integrated Care Model Based on CGA and GIT |
Further advancement of the integrated care model based on CGA and GIT requires coordinated efforts across three domains: theoretical refinement, practice-oriented innovation, and policy support. From a theoretical perspective, development of conceptual models applicable to diverse care settings—including emergency departments, outpatient clinics, inpatient units, and community-based services—as well as different cultural contexts, remains necessary. Contemporary models of integrated care emphasize the importance of connectivity across broader healthcare ecosystems and inter-organizational networks.25 Exploration of advanced technologies, including artificial intelligence and large-scale data analytics, in the interpretation of CGA data and risk prediction should be expanded. Artificial intelligence–driven clinical decision support systems demonstrate strong performance in risk prediction and treatment optimization; in older populations with diabetes, such approaches are associated with improved diagnostic accuracy and reduced hospitalization rates.26 These approaches support more precise decision-making within GIT and contribute to individualized care delivery. From the perspective of practical innovation, development of telemedicine-based “virtual GIT” models is warranted to expand service accessibility, particularly in resource-limited or remote settings.28 Integration of the care model with emerging service frameworks, including enhanced recovery units and chronic disease management units, should be further examined. For example, implementation of CGA within emergency departments, combined with multidisciplinary follow-up as exemplified by the ED PLUS model, supports care transition between emergency and community settings.8 Strengthening the coordinating role of primary healthcare institutions within integrated care is also required. Through targeted training and system-level support, these institutions can undertake key functions, including initial assessment, coordination of referrals, and long-term follow-up.29 At the policy level, reform of payment mechanisms is essential. Incentive structures based on value, bundled payments, or capitation models should replace fee-for-service approaches that fail to reflect the benefits of integrated care, thereby promoting preventive management and interdisciplinary collaboration.30 Development of national guidelines and quality standards for geriatric integrated care would provide a unified framework for service delivery, workforce training, and outcome evaluation, ensuring consistency and comparability of care.27 Expansion of training programs in geriatric medicine and interdisciplinary collaboration is required to strengthen workforce capacity in managing complex care needs among older populations.24 Coordinated advancement across theoretical, practical, and policy domains is required to support large-scale implementation and optimization of the integrated care model, ultimately improving quality and efficiency of geriatric care.
Conclusion
The integration of Comprehensive Geriatric Assessment (CGA) with Geriatric Interdisciplinary Team (GIT) care represents a paradigm shift from disease-focused to person-centered geriatric practice. Accumulating evidence indicates this model improves functional outcomes, quality of life, and care coordination.
However, translating this model into routine practice encounters persistent barriers, including workforce shortages, fragmented coordination, misaligned incentives, and specialty-centered traditions. Moreover, robust evidence regarding the integrated model specifically—distinct from CGA or GIT alone—remains limited, with most data derived from single-center or observational studies.
Future priorities include rigorous study designs, standardized implementation protocols, context-specific frameworks, digital tools for standardized assessment, and payment reforms rewarding value over volume. These efforts are essential to facilitate the transition of the integrated model from pilot programs to sustainable practice for aging populations.
Funding
Dali Prefecture Science and Technology Bureau Key Research and Development Program (20232903B030003); Medical Science Research Record Project of Dali Bai Autonomous Prefecture (ZB2025WJ009).
Disclosure
The authors declare no competing interests.
References
1. Mentens A, Panait C, Vaucher Y, et al. Prescribed autonomy: outpatient comprehensive geriatric assessment. Rev Med Suisse. 2025;21(937):1922–8. doi:10.53738/REVMED.2025.21.937.47973
2. Briggs R, Mcdonough A, Ellis G, et al. Comprehensive geriatric assessment for community-dwelling, high-risk, frail, older people. Cochrane Database Syst Rev. 2022;5(5):CD012705. doi:10.1002/14651858.CD012705.pub2
3. Baxter CT, Offord NJ. Frailty on the acute medical take. Clin Med. 2022;22(4):298–301. doi:10.7861/clinmed.2022-0312
4. Gao C, Yu P. Progress in the working model of geriatric interdisciplinary teams. Chinese J Geriatrics. 2020;39(2):238–240. doi:10.3760/cma.j.issn.0254-9026.2020.02.026
5. Barrault-Couchouron M, Micheli N, Soubeyran P. Exploring determinants of interdisciplinary collaboration within a geriatric oncology setting: a mixed-method study. Cancers. 2022;14(6):1386. doi:10.3390/cancers14061386
6. Vidra R, Alexander PV, Liposits G. Practical guide to integrating geriatric assessment in gastrointestinal oncology in a resource-limited setting. J Clin Med. 2025;14(23):8448. doi:10.3390/jcm14238448
7. Arcidiacono GP, Ceolin C, Sella S, et al. Taking care of inpatients with fragility Hip fractures: the hip-Padua osteosarcopenia (Hip-POS) fracture liaison service model. J Endocrinol Invest. 2025;48(1):99–108. doi:10.1007/s40618-024-02425-z
8. Holmes A, Fitzgerald C, Conneely M, et al. A multi-stakeholder qualitative evaluation of ed plus: a physiotherapy-led transition to home intervention for older adults following emergency department discharge. Clin Interventions Aging. 2025;20:147–159. doi:10.2147/CIA.S469933
9. Tu HR, Lin TH, Hsu LM, et al. High mortality and medical costs in geriatric trauma patients: surgical treatment and risk factors from a retrospective cohort study at a level i trauma center. Ann Geriatric Med Res. 2025;29(4):430–439. doi:10.4235/agmr.25.0124
10. Beard JR, Officer A, De Carvalho IA, et al. The world report on ageing and health: a policy framework for healthy ageing. Lancet. 2016;387(10033):2145–2154. doi:10.1016/S0140-6736(15)00516-4
11. Sanchís-Soler G, Parra-Rizo MA, Camacho PB, et al. Ejercicio físico, autonomía en personas con Alzheimer y sobrecarga del cuidador: una revisión sistemática. Retos. 2026;80:95–113. doi:10.47197/retos.v80.118676
12. Rodríguez CÁ, Carcausto-Calla W, Ríos AR, et al. Beneficios del entrenamiento multicomponente en el aprendizaje motor y cognitivo de los adultos mayores. Vive Revista de Salud. 2023;6(18):920–933. doi:10.33996/revistavive.v6i18.274
13. Lina W, Chunyan J, Chunyan WL. Advances in clinical application of comprehensive geriatric assessment. Chin J Gen Pract. 2019;22(9):999. doi:10.12114/j.issn.1007-9572.2018.00.271
14. Pilotto A, Custodero C, Palmer K, et al. A multidimensional approach to older patients during COVID-19 pandemic: a position paper of the special interest group on comprehensive geriatric assessment of the European Geriatric Medicine Society (EuGMS). Eur Geriatric Med. 2023;14(1):33–41. doi:10.1007/s41999-022-00740-3
15. Parks RM, Hall L, Tang SW, et al. The potential value of comprehensive geriatric assessment in evaluating older women with primary operable breast cancer undergoing surgery or non-operative treatment--a pilot study. J Geriatric Oncol. 2015;6(1):46–51. doi:10.1016/j.jgo.2014.09.180
16. Nastasa A, Hussien H, Apetrii M, et al. Revisiting risk prediction tools for death and end-stage renal disease in older patients with advanced chronic kidney disease: a prospective study. Int Urol Nephrol. 2022;54(8):1969–1976. doi:10.1007/s11255-021-03082-4
17. Hayes C, Fitzgerald C, O’shaughnessy Í, et al. Exploring stakeholders’ experiences of comprehensive geriatric assessment in the community and out-patient settings: a qualitative evidence synthesis. BMC Primary Care. 2023;24(1):274. doi:10.1186/s12875-023-02222-2
18. Ying Y, Liang Y. Progress in the application of comprehensive assessment in emergency visits of elderly patients. Chinese J Emerge Criti Care Nurs. 2023;4(6):568.
19. Gregersen M, Hansen TK, Jørgensen BB, et al. Frailty is associated with hospital readmission in geriatric patients: a prognostic study. Eur Geriatric Med. 2020;11(5):783–792. doi:10.1007/s41999-020-00335-w
20. Stuck AE, Siu AL, Wieland GD, et al. Comprehensive geriatric assessment: a meta-analysis of controlled trials. Lancet. 1993;342(8878):1032–1036. doi:10.1016/0140-6736(93)92884-v
21. Safitri ED, Ranakusuma W, Siagian NKP, et al. The effectiveness of comprehensive geriatric assessment intervention for older people in outpatient setting: a systematic review/ meta-analysis. BMC Geriatr. 2025;25(1):418. doi:10.1186/s12877-025-06048-8
22. Choi JY, Rajaguru V, Shin J, et al. Comprehensive geriatric assessment and multidisciplinary team interventions for hospitalized older adults: a scoping review. Arch Gerontol Geriatrics. 2023;104:104831. doi:10.1016/j.archger.2022.104831
23. Theodorakis N, Kollia Z, Christodoulou M, et al. Barriers to implementing effective healthcare practices for the aging population: approaches to identification and management. Cureus. 2025;17(2):e79590. doi:10.7759/cureus.79590
24. Ferretti-Rebustini RE, Souza-Talarico JN, Fhon JR, et al. The role of assessment in competence-based gerontological advanced practice nursing. Revista Da Escola De Enfermagem Da U S P. 2022;56(spe):e20220072. doi:10.1590/1980-220X-REEUSP-2022-0072en
25. M MMN, Z N, H K, et al. The renewed development model for integrated care: a systematic review and model update. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-12610-2
26. Hu J, Ren L, Wang T, et al. Artificial intelligence-assisted clinical decision-making: a perspective on advancing personalized precision medicine for elderly diabetes patients. J Multidisciplin Healthcare. 2025;18:4643–4651. doi:10.2147/JMDH.S529190
27. Ma YN, Karako K, Xia Y, et al. International landscape of guidelines for perioperative frailty assessment and barriers to clinical translation. Biosci Trends. 2026;20:149–159. doi:10.5582/bst.2025.01389
28. Yutong T, Yan Z, Qingyun C, et al. Information and communication technology based integrated care for older adults: a scoping review. Int J Integrated Care. 2023;23(2):2. doi:10.5334/ijic.6979
29. Inacio MC, Harrison S, Schwabe J, et al. Models of care across settings supporting ageing in place: a narrative review. Med J Austr. 2025;223(4):218–225. doi:10.5694/mja2.70003
30. Seghers PAL, Alibhai SMH, Battisti NML, et al. Geriatric assessment for older people with cancer: policy recommendations. Global Health Res Policy. 2023;8(1):37. doi:10.1186/s41256-023-00323-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Models of Integrated Acute Care for Older Adult Inpatients That Incorporate Integrative Health: An Integrative Review
Bonvin E, Perruchoud E, Tacchini-Jacquier N, Perrenoud J, Melly P, Celik S, Jean M, Verloo H
Journal of Multidisciplinary Healthcare 2025, 18:759-786
Published Date: 12 February 2025