Back to Journals » International Journal of Women's Health » Volume 18
Complications Following Late Second-Trimester Dilatation and Evacuation: A Retrospective Cohort Comparison of Missed and Induced Abortions
Authors Farhadian Y, Friedman M ![]() , Tarashandegan D, Mor L, Cohen I, Gluck O, Kerner R, Keidar R, Weiner E, Sagiv R
, Tarashandegan D, Mor L, Cohen I, Gluck O, Kerner R, Keidar R, Weiner E, Sagiv R
Received 20 August 2025
Accepted for publication 14 January 2026
Published 29 January 2026 Volume 2026:18 561941
DOI https://doi.org/10.2147/IJWH.S561941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Yasmin Farhadian,1,2,* Matan Friedman,1,2,* Danit Tarashandegan,3 Liat Mor,1,2 Ido Cohen,2,4 Ohad Gluck,1,2 Ram Kerner,1,2 Ran Keidar,1,2 Eran Weiner,1,2 Ron Sagiv1,2
1Department of Obstetrics and Gynecology, E. Wolfson Medical Center, Holon, Israel; 2Gray Faculty of Medical and Health Sciences, Tel Aviv University, Tel Aviv, Israel; 3Department of Obstetrics and Gynecology, Hillel Yaffe Medical Center, Hadera, Israel; 4Department of Medicine E, Sheba Medical Center Tel-Hashomer, Ramat Gan, Israel
*These authors contributed equally to this work
Correspondence: Matan Friedman, Department of Obstetrics and Gynecology, E. Wolfson Medical Center, Holon, Israel, Email [email protected]
Objective: Second-trimester D&E is generally safe, but whether pregnancy viability (missed vs induced abortion) alters complication risk remains unclear as comparative data remain limited. We compared complication rates following second-trimester dilatation and evacuation (D&E) for missed abortion (MA) versus induced abortion (IA) and assess potential contributing factors to increased morbidity in MA cases.
Methods: This retrospective cohort study included all consecutive second-trimester (13– 20 weeks) D&E procedures performed for MA and IA at a single tertiary medical center between 2002 and 2023. Patients were divided into two groups based on fetal viability at the time of the procedure. Data were extracted from electronic medical records and validated by trained clinical research associates. The primary outcome was maternal complications, including hemorrhage, uterine atony, disseminated intravascular coagulation (DIC), infection, cervical or vaginal lacerations, uterine perforation, hysterectomy, and bladder or ureteral injury.
Results: A total of 974 women underwent second-trimester D&E, including 202 (20.7%) in the MA group and 772 (79.3%) in the IA group. Women in the MA group were significantly older (32.1± 6.1 vs 29.1± 7.2 years, p < 0.01) and had higher parity (1.54± 1.46 vs 1.12± 1.32, p < 0.01). Compared to IA, MA was associated with a significantly higher incidence of hemorrhage (10.4% vs 1.3%, p < 0.01), blood transfusions (7.4% vs 0.9%, p < 0.01), DIC (0% vs 1.5%, p=0.007), and uterine atony (2.5% vs 0.1%, p < 0.01). Missed abortion was independently associated with complications (aOR 5.70, 95% CI 3.02– 10.74, p < 0.01). Notably, cervical preparation was required in only 19% of MA cases compared to 79% of IA cases (p < 0.01).
Conclusion: MA is associated with an increased risk of hemorrhagic and infectious complications following second-trimester D&E compared to IA. Differences in inflammatory response, coagulation status, and cervical preparation protocols may contribute. These findings highlight the need for risk stratification, pre-procedural cervical preparation, and closer post-procedural monitoring for patients undergoing D&E for MA.
Plain Language Summary: A retrospective study revealed a significantly higher incidence of hemorrhagic complications, uterine atony, and blood transfusion, in patients undergoing Dilation and Evacuation (D&E) for missed abortion over induced abortion. This emphasizes the need for perioperative strategies and individualized patient management.
Keywords: missed abortion, induced abortion, dilatation and evacuation, second-trimester abortion, complications, hemorrhage
Introduction
Late second-trimester surgical abortion is commonly used to describe uterine evacuation procedures performed between 13 and 20 weeks’ gestation, representing an essential aspect of reproductive healthcare, although terminology and gestational cutoffs vary across settings and remain debated as discussed by Jacobson et al.1 It encompasses two distinct clinical scenarios: missed abortion (MA)2 which involves the loss of a non-viable pregnancy still in-utero, also including induced abortion (IA) for viable pregnancies.3 While Dilatation and Evacuation (D&E) is the standard and generally considered a safe procedure for pregnancy termination in the second trimester, it is not without risks. As with any surgical procedure, D&E is associated with a range of complications, including retained products of conception, uterine atony, hemorrhage, disseminated intravascular coagulation (DIC), infections, cervical or vaginal lacerations, uterine perforation, hysterectomy, and injuries to adjacent structures such as the bladder or ureters.4–7
International data from high-resource settings consistently demonstrate that second-trimester D&E is associated with low overall complication rates, typically ranging between 1% and 5%, with severe morbidity remaining rare when procedures are performed by trained providers with appropriate cervical preparation. WHO reports and multi-country analyses similarly emphasize that procedural safety is primarily influenced by access to timely, standardized care rather than by the abortion procedure itself. The overall complication rates observed in our induced abortion cohort are consistent with these international reports, whereas the higher rates observed in missed abortion cases appear to reflect differences in the underlying clinical context rather than deviation from global procedural safety benchmarks.8 While MA and IA share procedural similarities, fundamental physiological differences, such as cervical integrity, placental characteristics, and uterine contractility,9–11may influence the type and incidence of complications. However, existing literature lacks comprehensive analysis directly comparing these two clinical entities, leaving a critical gap in our understanding of how pregnancy viability affects surgical outcomes.
Globally, complication rates following second-trimester uterine evacuation vary widely depending on access to standardized care, provider expertise, and institutional protocols. Studies from high-resource settings consistently report low complication rates for D&E, whereas data from low-resource environments often reflect higher risks driven by delays in care and inconsistent cervical preparation. Understanding these contextual factors is essential for interpreting differences in safety profiles between missed and induced abortions.12–14
Addressing this knowledge gap is essential, as a better understanding of the relationship between pregnancy status (viable vs non-viable) and post-procedural complications could lead to improved risk assessment, procedural modifications, and tailored patient counseling. Because missed and induced abortions are managed within the same standardized healthcare framework at our institution, this setting offers an opportunity to examine the impact of pregnancy viability on complication risk while minimizing health-system–related confounding.
This study aimed to compare complication rates following second-trimester D&E for missed versus induced abortions and to identify factors associated with increased morbidity. By identifying potential disparities in outcomes, this research seeks to provide clinicians with data-driven insights that can refine surgical approaches, enhance patient safety, and ultimately optimize reproductive healthcare.15
Materials and Methods
This was a retrospective observational cohort study between 2002 and 2023 conducted in a single, university-affiliated tertiary medical center, with a dedicated second-trimester D&E service staffed by experienced attending gynecologists, including all consecutive cases of women who underwent second-trimester (weeks 13–20) D&E due to one of two medical indications: (1) Missed Abortion or (2) termination of pregnancy for a viable fetus.
Ethical Approval
The research protocol was approved by The E. Wolfson Medical Center Institutional Review Board (decision number 0199-18-WOMC) on December 24th, 2018. Furthermore, the board also waived the need for informed consent. All methods were carried out in accordance with relevant declaration of Helsinki guidelines and regulations.
Dilation and Evacuation Procedure
D&E is performed in the operating room under general anesthesia, and continuous ultrasound guidance by experienced senior gynecologists is performed all through the procedure, consistent with established second-trimester D&E protocols.3 Cervical preparation was performed using laminaria (osmotic dilators) and/or misoprostol according to gestational age. The protocols used were as follows:
- For pregnancies <17 weeks: a single set of laminaria with or without 800 μg vaginal misoprostol administered 6–8 hours prior was used.
- For pregnancies ≥17 weeks, laminaria were inserted twice at 6- and 12-hour intervals.
- In selected cases, cervical preparation consisted solely of misoprostol.
All D&E procedures were performed under general anesthesia with continuous ultrasound guidance by senior attending gynecologists.
Inclusion criteria were singleton pregnancy, ages between 18 and 45 undergoing second-trimester D&E for the aforementioned indications. Exclusion criteria included cases with incomplete operative or postoperative documentation, missing key outcomes (hemorrhage, transfusion, infection), or unavailable gestational age data, and not all relevant medical data could be extracted. Maternal comorbidities, including hypertension, diabetes, or other chronic medical conditions, were not used as exclusion criteria.
Cases were divided into two groups based on pregnancy viability at the time of the procedure: the MA group (missed abortion, non-viable pregnancy) and the IA group (induced abortion, viable pregnancy).
Data collection was performed through a systematic review of medical charts, utilizing the hospital’s electronic medical record system searching cases by ICD9 and ICD10 codes. Trained clinical research associates were responsible for data extraction and validation from operative notes and post-up documentation to ensure accuracy and completeness. Collected variables included patients’ demographic characteristics, obstetric history, and relevant medical background. Maternal comorbidities and preoperative coagulation profiles were not consistently available in the medical records and therefore could not be incorporated into the analysis; this is acknowledged as a study limitation. Additionally, although the study spans more than 20 years, institutional protocols for D&E, including surgical technique, cervical preparation options, and operator training, remained largely consistent throughout this period, allowing for aggregation of data across years. The extended study period reflects the relatively low frequency of second-trimester Dilation and Evacuation Procedures for missed abortion, necessitating long-term data collection to ensure adequate statistical power. The study’s primary outcome was maternal complications, which were identified using operative reports, anesthesia records, and postoperative notes documented in the electronic medical record. ICD-9 and ICD-10 coding system was used as well to insure all cases were identified; all complications were validated manually by trained research staff (as can be seen in Supplementary Table 1). Complications were defined as the occurrence of one or more of the following adverse events: retained products of conception, uterine atony, hemorrhage as defined by the need for blood transfusion (DINDO Classification 2 and above),16–18 DIC, infections, cervical/vaginal laceration, uterine perforation, hysterectomy, and bladder or ureteral injury documented during the index hospitalization or subsequent clinical follow-up. Given the long study period, potential temporal variability was assessed descriptively by confirming that core procedural protocols and provider staffing patterns remained stable across years.
Statistical Analysis
Statistical analyses were conducted using SPSS software (IBM SPSS Statistics, version 27, 2020; IBM Corp., Armonk, NY, USA). Distribution of continuous variables was assessed for normality prior to analysis, and parametric or nonparametric tests were applied accordingly. Normally distributed continuous variables were compared using the independent-samples t-test, and non-normally distributed variables using the Mann–Whitney U-test. Categorical variables were analyzed using the chi-square test or Fisher’s exact test when expected cell counts were <5. All statistical tests were two-sided, with a significance level set at p < 0.05. Both statistical significance and clinical relevance were considered when interpreting effect sizes, with attention to whether confidence interval width reflected meaningful differences between groups.
Covariates included in the multivariable logistic regression model were maternal age, gestational age, and parity, selected based on clinical relevance and data completeness. Variables such as cervical preparation, prior cesarean delivery, provider identity, and maternal comorbidities were not consistently documented across the full 21-year study period, these variables could not be reliably incorporated into adjusted analyses. For the same reason, a sensitivity analysis (including propensity-score modeling) could not be performed. This represents a potential source of unmeasured confounding.
Results
As can be seen in Table 1. A total of 974 women underwent late surgical abortion procedures in the allocated timeframe. The Missed abortions group included 202 patients (20.73%), while the induced abortions group included 772 patients (79.26%).
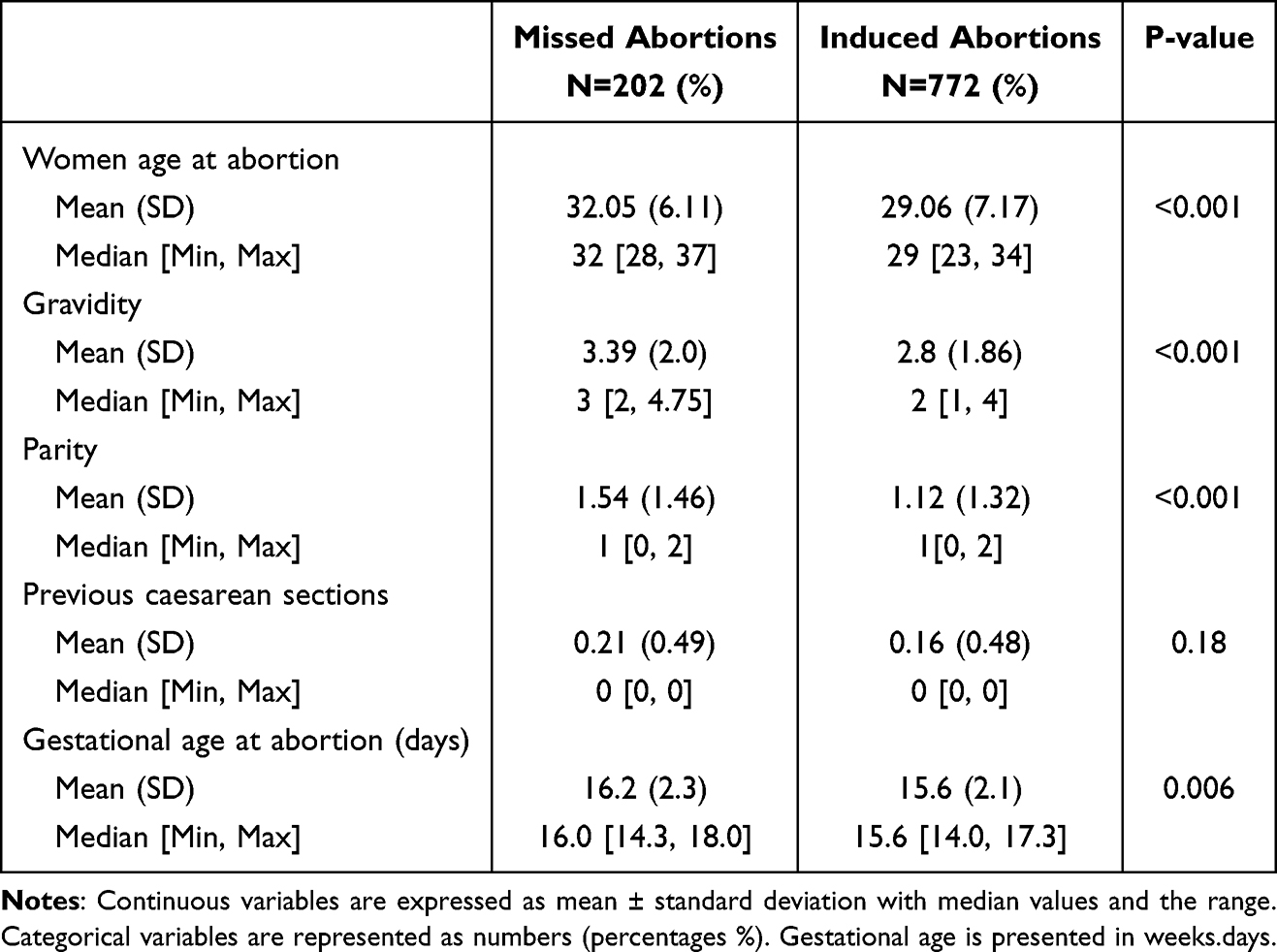 |
Table 1 Baseline Characteristic |
Notably, a subtle yet statistically significant demographic differences between these groups was observed: women in the missed abortion cohort were, on average, slightly older than their counterparts (32.05±6.13 years vs 29.06±7.2 years, p < 0.01). Additionally, they exhibited a higher degree of reproductive history, as evidenced by a greater number of previous pregnancies (3.39±2 vs 2.8±1.86, p < 0.01) and deliveries (1.54±1.46 vs 1.12±1.32, p < 0.01).
The median gestational age at the time of the abortion differed statistically between groups (p = 0.006), although the absolute difference was small and unlikely to be clinically significant. Sixteen weeks and 2 days [14 week and 3 days, 18 weeks] days for missed abortion vs 15 weeks and 6 days [14 weeks, 17 weeks, and 3 days] days for induced abortion.
Among the overall complications assessed in our study, there was an increased risk in the missed pregnancy group with a substantially elevated incidence of complications rate compared to their counterparts undergoing IAs as clearly described in Table 2. When comparing pre-procedural preparation, another statistically different observation was made. While the majority of patients in the MA group did not need cervical preparation prior to the procedure (81%), the majority of patients undergoing the same procedure for IA (79%) was performed following cervical preparation. This large imbalance in cervical preparation (81% in MA vs 79% in IA) represents a clinically significant difference that may partially account for the higher hemorrhage and laceration rates observed in the MA group.
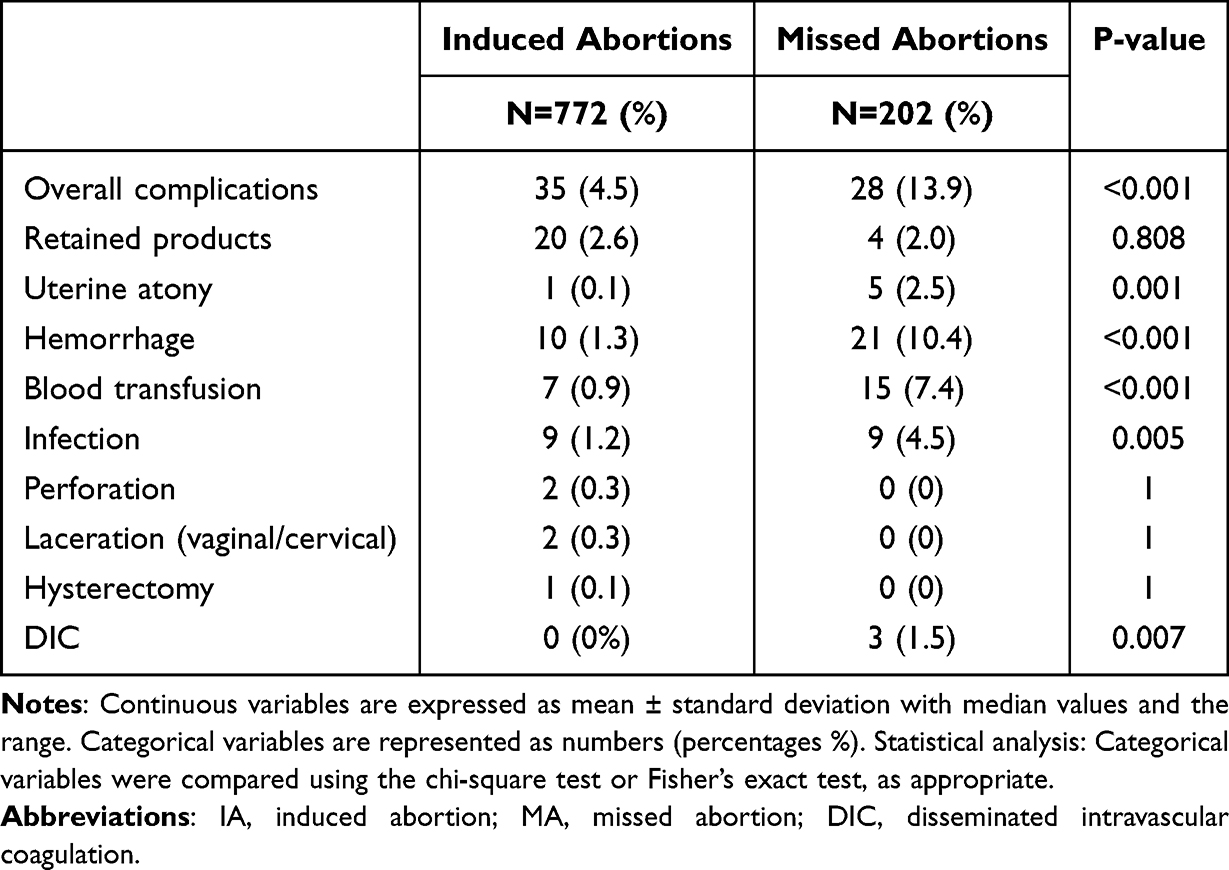 |
Table 2 Procedure Outcomes and Complications |
A logistic regression analysis (Table 3) has shown that comparing D&E preformed for MA was associated with a higher rate of adverse outcomes (including infections and hemorrhage) (aOR 5.7, CI 3.02–10.74, p < 0.01). The magnitude of the adjusted odds ratio (aOR 5.70) indicates a markedly increased risk, well beyond the threshold of statistical significance, and the relatively narrow confidence interval (3.02–10.74) supports the clinical relevance of this association. That being said, cervical preparation or providers experience was not included in the regression model due to incomplete or inconsistent documentation over the 20-year study period, and this must be considered a potential confounder.
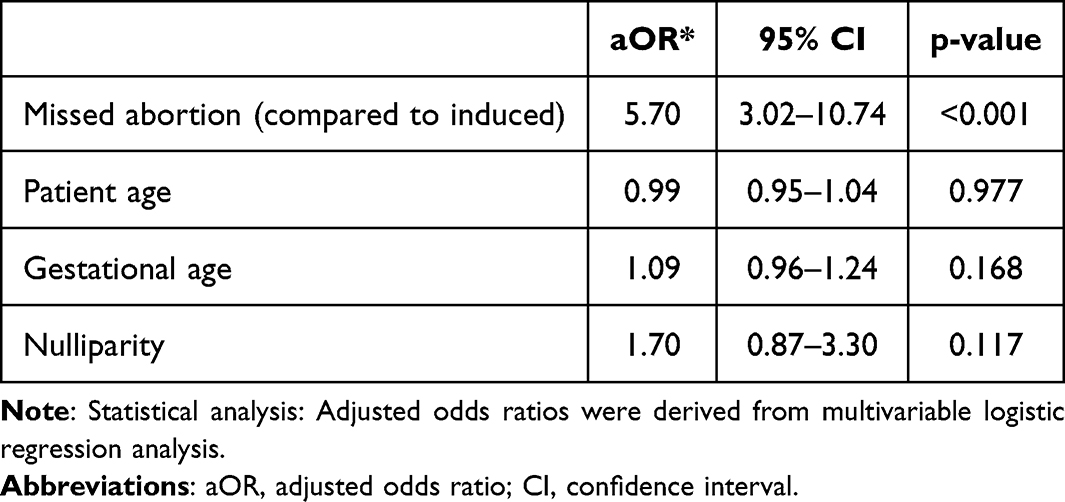 |
Table 3 Logistic Regression Analysis Examining the Associations Linked to a Composite of Adverse Outcomes During Dilation and Evacuation |
Discussion
In this retrospective cohort study, substantial differences in complication rates were observed between late surgical abortions performed for MA and IA. This new evidence offers critical insights into current clinical practice and the management of second-trimester D&E procedures. Most notably, a significantly elevated incidence of complications, particularly hemorrhage and the need for blood transfusions, was observed in the MA group compared to the IA group. A similar increase was noted for DIC and uterine atony. This association remained significant in multivariable logistic regression.
These findings also provide important context for public perceptions of abortion safety. The markedly lower complication rates observed in induced abortions compared with procedures following fetal demise suggest that risk is driven less by the evacuation procedure itself and more by the underlying clinical condition prompting it. As such, the process of framing “abortion” as intrinsically dangerous conflates procedure with circumstance; safety appears to largely depend untimely access to care, standardized cervical preparation, and management of coagulopathy or inflammation when one is present.
When considering potential contributing factors to the increased complication rates in late MA cases, multiple physiological and clinical elements must be examined. These may include factors intrinsic to the pregnancy itself, such as fetal viability status, as well as maternal characteristics and systemic responses. Similar trends have been reported in previous studies, highlighting the need for further investigation into how viability status influences surgical outcomes.19–21
One possible explanation for the heightened complication rates in MA cases is the differential inflammatory response associated with prolonged retention of non-viable fetal tissue. Research has shown that MA triggers a more pronounced immune reaction compared to viable pregnancies, leading to increased tissue damage within the uterus.22 Retained tissue fragments can act as a stimulus for both local and systemic inflammatory responses, potentially exacerbating coagulopathy and increasing the risk of hemorrhagic complications, such as post-abortion hemorrhage and uterine atony.6,23 These mechanisms align with the findings of historical observations of intrauterine fetal demise (IUFD), which have linked prolonged fetal retention to coagulopathic complications.22,24–27 Another plausible explanation lies in the potential for bacterial colonization and infection in cases of MA.28,29 Unlike IA, where the pregnancy is electively terminated and fetal tissue is promptly removed, MAs involve a period of fetal demise before uterine evacuation, during which retained products of conception may create an environment conducive to bacterial overgrowth. This prolonged exposure could increase the risk of subclinical or overt infections, leading to inflammatory responses that further contribute to uterine atony and hemorrhage. Even if infections remain undetected before the procedure, the surgical intervention itself could exacerbate underlying inflammatory changes, intensifying the risk of post-procedural complications.30–32
These mechanisms may be further amplified by prolonged retention of non-viable tissue, which has been associated with cytokine activation, endothelial dysfunction, and early consumption of clotting factors. Recent studies using advanced immunologic profiling support these pathways, demonstrating distinct inflammatory signatures in missed abortion tissue compared with viable pregnancies.22,33
The substantial difference in cervical preparation protocols between groups likely contributes to the disparity in complication rates. Cervical ripening reduces the degree of mechanical dilatation required and has been associated with decreased rates of cervical laceration, hemorrhage, and uterine trauma. Because most MA patients in our cohort underwent D&E without prior cervical preparation, this variable may act as both a confounder and a mediator, amplifying the observed risk associated with MA independent of inflammatory or coagulative mechanisms. From a clinical perspective, these findings support the consideration of routine pre-procedural cervical preparation in second-trimester D&E for missed abortion, even in cases where spontaneous cervical dilatation is present. Development of standardized perioperative protocols or safety checklists for MA cases may further reduce preventable hemorrhagic and mechanical complications.
Additionally, an important consideration is whether the underlying cause of fetal demise itself may be contributing to increased complication rates. Unrecognized maternal conditions, such as thrombophilias, autoimmune disorders, or placental pathologies—may not only lead to pregnancy loss but also predispose patients to post-procedural morbidity.6,7 In our study, patients in the MA cohort were found to have slightly higher maternal age and parity compared to the IA cohort. These demographic variations may indicate distinct baseline risk factors that could influence surgical outcomes.
While previous studies have explored the safety of surgical abortions in cases of MA versus IA, the available evidence remains inconsistent, and no prior research has specifically addressed second-trimester procedures. One study examining first-trimester surgical abortions found higher rates of complications in MAs, mirroring our findings.34 Maru et al reported that patients undergoing MA had significantly increased rates of hemorrhage, anemia, hypovolemic shock, and fever compared to those undergoing IA, although their study included both medical and surgical methods of uterine evacuation.35 In contrast, Hortence et al found higher complication rates in IA cases, particularly for infectious complications such as sepsis, pelvic peritonitis, and septic shock, as well as mechanical injuries like uterine perforation and intestinal lesions.36 However, a crucial distinction in their study was that many IAs were performed in clandestine settings, where aseptic measures were suboptimal. The authors themselves acknowledged that the overall complication rates in their study were higher than those reported in the broader literature for both MA and IA groups. Similar findings have been documented in regions where access to safe abortion services is restricted.37
It is also important to recognize that many previous studies on this topic were conducted in developing countries or in nations where IA was only recently legalized. While legalization and improved accessibility to IA have led to better patient outcomes in these regions, studies indicate that IA patients in such settings often seek medical care later and in poorer physical condition compared to MA patients (18). In contrast, Israel provides a legal, accessible, and widely accepted framework for abortion care, minimizing the risk of delays in treatment and ensuring a more standardized approach to both MA and IA cases. This uniform care environment allows differences in complication rates between missed and induced abortions to be interpreted as reflecting underlying clinical context rather than disparities in access, provider expertise, or procedural standards.
Methodologically, this study differs from many previously published reports by drawing on a long-term, single-center cohort in which both missed and induced abortions were managed under consistent institutional protocols, with uniform inclusion criteria and standardized surgical techniques. Such long-duration, single-center datasets are uncommon in this field, yet they offer an important advantage by minimizing inter-institutional variability and allowing outcomes to be interpreted within a stable clinical framework. This strengthens the internal validity of our findings and supports the attribution of observed differences in complication rates to underlying clinical context rather than procedural heterogeneity. That said, formal sensitivity analyses comparing early versus later study periods were not performed due to inconsistent documentation of key variables across years.
These differences across healthcare systems highlight that complication rates are not intrinsic to the D&E procedure itself but are instead closely tied to system-level factors such as access to timely care, legal status of abortion services, and availability of cervical preparation.
Beyond demographic and systemic factors, differences in procedural protocols between MA and IA cases must also be considered. Although the surgical technique for uterine evacuation is largely similar, the clinical context differs significantly. Because IA is an electively planned procedure, patients routinely undergo cervical preparation prior to D&E, facilitating safer dilatation and potentially reducing the risk of cervical trauma. In contrast, MA cases are often unpredictable, and many patients in this group do not receive adequate cervical preparation before the procedure. This lack of preoperative cervical dilatation may contribute to a higher incidence of mechanical trauma, increasing the likelihood of complications such as hemorrhage and cervical lacerations.
Importantly, these results reflect outcomes from second-trimester D&E performed in a well-resourced, legally regulated setting. They cannot be generalized to first-trimester procedures, medical abortions, or contexts where access to trained providers and cervical preparation is limited. In countries where abortion care is restricted or delayed, complication rates may be driven by system-level barriers rather than intrinsic procedural risk.
While the demographic variations and differences in procedural preparation make direct comparisons between MA and IA imperfect, this study provides critical insights into real-world clinical scenarios. The findings highlight the distinct risk profiles associated with each indication for second-trimester surgical abortion and underscore the need for tailored perioperative management strategies as they may suggest that risk is driven less by the evacuation procedure itself and more by the underlying physiologic and clinical context. Factors such as delayed presentation, inflammation or coagulopathy related to fetal demise, and differences in cervical preparation and perioperative management appear to play a central role. Accordingly, public and clinical discourse that frames “abortion” as intrinsically dangerous may conflate procedure with circumstance; safety is more accurately determined by timely access to care, standardized preparation, and evidence-based clinical pathways.
Beyond its local setting, these findings are relevant to global reproductive health contexts where access to safe surgical abortion, standardized cervical preparation, and post-procedural monitoring varies. The observed risk differential between missed and induced abortion underscores the importance of context-specific procedural protocols and trained clinical teams to mitigate preventable complications.
Ultimately, this research contributes valuable knowledge to the field of reproductive healthcare, helping providers enhance risk assessment, optimize procedural planning, and improve patient counseling. By recognizing the heightened complication risks associated with MA and identifying potential underlying mechanisms, clinicians can implement more targeted interventions to mitigate risks and enhance patient outcomes.
A comparison with the alternative clinical pathway, continued retention of fetal demise, is clinically relevant. Prolonged retention of an IUFD is associated with increasing risks of DIC, hemorrhage, and infection, which escalate with time. Thus, even though D&E for missed abortion is associated with higher complication rates than elective termination, timely evacuation remains the safer option compared with expectant management, particularly in the presence of coagulation or inflammatory changes.
This study has several limitations. It is a retrospective design, with data collected in a single tertiary center over a long-time span with incomplete data such as missing comorbidities. Additionally complication ascertainment partly relied on administrative ICD coding across a long study period; although all events were manually validated, coding practices and code availability may have changed over time, which could have affected case capture for some outcomes. Another limitation of this study is the substantial imbalance in cervical preparation between groups, with most MA cases undergoing D&E without prior cervical ripening. Because cervical preparation is known to reduce procedural trauma and hemorrhage, this discrepancy may have acted as an unmeasured confounder, potentially amplifying the observed difference in complication rates. Adding to the above, we must acknowledge that although procedural practices at our institution have been stable, the extended timeframe of data collection raises the possibility of unmeasured temporal variation, such as subtle evolutions in documentation, surgical instruments, or perioperative protocols. Additionally, the absence of follow-up information limited the ability to assess long-term complications such as intrauterine adhesions, delayed infection, or later reproductive sequelae. Moreover, although sensitivity or propensity-score analyses may further reduce residual confounding, these approaches were not feasible in the present study due to inconsistent documentation of key covariates across the study timeframe. This limitation may contribute to residual confounding and should be considered when interpreting the findings.
Conclusion
Our study identifies a higher incidence of hemorrhagic and infectious complications in second-trimester D&E for MA compared to IA, highlighting the need for tailored perioperative management and closer monitoring in MA cases. Adding to the above, based on these findings, routine pre-procedural cervical preparation and the use of tailored perioperative protocols for missed abortion cases should be considered to reduce complication rates and improve safety during second-trimester D&E.
Further research should explore underlying mechanisms, including inflammatory response, coagulation disturbances, and cervical preparation, to refine risk-reduction strategies. Using prospective research, implementing targeted interventions such as pre-procedural cervical preparation and enhanced hemostatic measures may improve outcomes.
Abbreviations
aOR, Adjusted odds ratio; CI, confidence interval; D&E, dilatation and evacuation; DIC, disseminated intravascular coagulation; IA, induced abortion; IUFD, intrauterine fetal demise; MA, missed abortion; SD, standard deviation; SPSS, Statistical Package for the Social Sciences; TOP, termination of pregnancy.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors did not report any potential conflicts of interest in this work.
References
1. Jacobson LE, Darney BG, Johnston HB, Ganatra B. A global scoping review of the circumstances of care seeking for abortion later in pregnancy. PLOS Glob Public Health. 2024;4(12):e0003965. doi:10.1371/journal.pgph.0003965
2. Gabbe SG, Niebyl JR, Simpson JL, et al. Obstetrics: Normal and Problem Pregnancies E-Book. Elsevier Health Sciences; 2016.
3. American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 135: second-trimester abortion. Obstet Gynecol. 2013;121(6):1394–10. doi:10.1097/01.AOG.0000431056.79334.cc
4. Kapp N, Lohr PA. Modern methods to induce abortion: safety, efficacy and choice. Best Pract Res Clin Obstet Gynaecol. 2020;63:37–44. doi:10.1016/j.bpobgyn.2019.11.008
5. Jacques L, Heinlein M, Ralph J, et al. Complication rates of dilation and evacuation and labor induction in second-trimester abortion for fetal indications: a retrospective cohort study. Contraception. 2020;102(2):83–86. doi:10.1016/j.contraception.2020.04.018
6. Kerns JL, Ti A, Aksel S, Lederle L, Sokoloff A, Steinauer J. Disseminated intravascular coagulation and hemorrhage after dilation and evacuation abortion for fetal death. Obstet Gynecol. 2019;134(4):708–713. doi:10.1097/aog.0000000000003460
7. Potter LA, Ly SH, Pei X, Ponzini MD, Wilson MD, Hou MY. Characteristics and outcomes of patients undergoing second-trimester dilation and evacuation for intrauterine fetal demise vs induced abortion. Contraception. 2023;126:110118. doi:10.1016/j.contraception.2023.110118
8. Burke KL, Potter JE. Meeting preferences for specific contraceptive methods: an overdue indicator. Stud Fam Plann. 2023;54(1):281–300. doi:10.1111/sifp.12218
9. Chandra M, Paray AA. Natural physiological changes during pregnancy. Yale J Biol Med. 2024;97(1):85–92. doi:10.59249/jtiv4138
10. Davis EP, Narayan AJ. Pregnancy as a period of risk, adaptation, and resilience for mothers and infants. Dev Psychopathol. 2020;32(5):1625–1639. doi:10.1017/s0954579420001121
11. Zhang Y, Ding W, Wu T, et al. Pregnancy with multiple high-risk factors: a systematic review and meta-analysis. J Glob Health. 2025;15:04027. doi:10.7189/jogh.15.04027
12. Farrington E, Huguenin A, Moore P, Neel A. Second-trimester surgical abortion is safe: audit of complication rates at an australian tertiary hospital. Aust N Z J Obstet Gynaecol. 2025. doi:10.1111/ajo.70062
13. Ganatra B, Gerdts C, Rossier C, et al. Global, regional, and subregional classification of abortions by safety, 2010–14: estimates from a Bayesian hierarchical model. Lancet. 2017;390(10110):2372–2381. doi:10.1016/s0140-6736(17)31794-4
14. Tufa TH, Prager S, Wondafrash M, Mohammed S, Byl N, Bell J. Comparison of surgical versus medical termination of pregnancy between 13–20 weeks of gestation in Ethiopia: a quasi-experimental study. PLoS One. 2021;16(4):e0249529. doi:10.1371/journal.pone.0249529
15. Edlow AG, Hou MY, Maurer R, Benson C, Delli-Bovi L, Goldberg AB. Uterine evacuation for second-trimester fetal death and maternal morbidity. Obstet Gynecol. 2011;117(2 Pt 1):307–316. doi:10.1097/AOG.0b013e3182051519
16. Alliende RI, Carrasco ÁM, Levancini M, Kovoor E, Guzmán-Rojas RA, Miranda-Mendoza I. 5,926 hysterectomies: complications described by Clavien–Dindo classification. J Obstet Gynaecol. 2021;41(7):1102–1106. doi:10.1080/01443615.2020.1835843
17. Clavien PA, Barkun J, De Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
18. Dindo D. The Clavien–Dindo classification of surgical complications. In: Treatment of Postoperative Complications After Digestive Surgery. Springer; 2014:13–17.
19. Nyarko SH, Greenberg LT, Phibbs CS, et al. Association between stillbirth and severe maternal morbidity. Am J Obstet Gynecol. 2024;230(3):
20. Tempfer CB, Brunner A, Bentz EK, Langer M, Reinthaller A, Hefler LA. Intrauterine fetal death and delivery complications associated with coagulopathy: a retrospective analysis of 104 cases. J Womens Health. 2009;18(4):469–474. doi:10.1089/jwh.2008.0938
21. Wall-Wieler E, Carmichael SL, Gibbs RS, et al. Severe maternal morbidity among stillbirth and live birth deliveries in California. Obstet Gynecol. 2019;134(2):310–317. doi:10.1097/aog.0000000000003370
22. Hou R, Huang R, Zhou Y, et al. Single-cell profiling of the microenvironment in decidual tissue from women with missed abortions. Fertil Steril. 2023;119(3):492–503. doi:10.1016/j.fertnstert.2022.12.016
23. Jain D, Oda T, Kohmura-Kobayashi Y, et al. Acute inflammation in the uterine isthmus coincides with postpartum acute myometritis in the uterine body involving refractory postpartum hemorrhage of unknown etiology after cesarean delivery. J Reprod Immunol. 2020;139:103116. doi:10.1016/j.jri.2020.103116
24. Goldstein DP, Reid DE. Circulating fibrinolytic activity—a precursor of hypofibrinogenemia following fetal death in utero. Obstetrics Gynecol. 1963;22(2):174–180.
25. Pritchard JA. Fetal death in utero. Obstet Gynecol. 1959;14:573–580.
26. Weiner AE, Reid DE, Roby CC, Diamond LK. Coagulation defects with intrauterine death from Rh isosensitization. Am J Obstet Gynecol. 1950;60(5):1015–1022. doi:10.1016/0002-9378(50)90507-2
27. Kwiatek M, Gęca T, Kwaśniewska A. Pro- and anti-inflammatory cytokines in the first trimester-comparison of missed miscarriage and normal pregnancy. Int J Environ Res Public Health. 2021;18(16):8538. doi:10.3390/ijerph18168538
28. Liu P, Chen G, Zhao S, Kong L, Liao X, Cheng M. The alteration of uterine microbiota participated in the activation of the decidual inflammatory response in early spontaneous abortion. PLoS One. 2025;20(2):e0317595. doi:10.1371/journal.pone.0317595
29. Sun D, Zhao X, Pan Q, et al. The association between vaginal microbiota disorders and early missed abortion: a prospective study. Acta Obstet Gynecol Scand. 2022;101(9):960–971. doi:10.1111/aogs.14410
30. Contini C, Rotondo JC, Magagnoli F, et al. Investigation on silent bacterial infections in specimens from pregnant women affected by spontaneous miscarriage. J Cell Physiol. 2018;234(1):100–107. doi:10.1002/jcp.26952
31. Orimoloye HT, He D, Li T, et al. Alpha-1 antitrypsin deficiency and pregnancy complications and birth outcomes: a population-based cohort study in Denmark. PLoS One. 2024;19(1):e0296434. doi:10.1371/journal.pone.0296434
32. Rotondo JC, Oton-Gonzalez L, Selvatici R, et al. SERPINA1 gene promoter is differentially methylated in peripheral blood mononuclear cells of pregnant women. Front Cell Dev Biol. 2020;8:550543. doi:10.3389/fcell.2020.550543
33. Gogesch P, Ortega Iannazzo S, Rupp N, et al. Immune cells play a critical role in cytokine- and endotoxin-mediated endothelial permeability. PLoS One. 2025;20(8):e0329700. doi:10.1371/journal.pone.0329700
34. Yasser AR, Aboutalib Y, Ragab RR, Nawara M. Complications associated with first-trimester surgical abortion at ain-shams maternity hospital over the period from January 1, 2016 to December 31, 2017. Evid Based Womens Health J. 2020;10(3):239–245. doi:10.21608/ebwhj.2020.26278.1085
35. Maru L, Verma M, Khan T. Reinforcing the vast difference between the outcomes of spontaneous versus induced miscarriages. Int J Reprod Contracept Obstet Gynecol. 2016;5(11):4031–4036. doi:10.18203/2320-1770.ijrcog20163884
36. Fouedjio JH. The early complications of induced abortion compared to those of spontaneous abortion in Yaoundé-Cameroon: a Cohort Study. Ethiop J Reprod Health. 2022;14(4):10. doi:10.69614/ejrh.v14i4.518
37. Goyaux N, Alihonou E, Diadhiou F, Leke R, Thonneau PF. Complications of induced abortion and miscarriage in three African countries: a hospital-based study among WHO collaborating centers. Acta Obstet Gynecol Scand. 2001;80(6):568–573.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.