Back to Journals » Risk Management and Healthcare Policy » Volume 15
Complexity of Decision-Making!: Case Studies of Cadaveric Organ Donations in Ahmedabad, India
Authors Saxena D ![]() , Yasobant S
, Yasobant S ![]() , Trivedi P, Bhavsar P
, Trivedi P, Bhavsar P ![]()
Received 10 June 2022
Accepted for publication 10 November 2022
Published 21 November 2022 Volume 2022:15 Pages 2147—2154
DOI https://doi.org/10.2147/RMHP.S376879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Deepak Saxena,1,2 Sandul Yasobant,1,2 Poonam Trivedi,1 Priya Bhavsar1
1Department of Public Health Science, Indian Institute of Public Health Gandhinagar (IIPHG), Gandhinagar, Gujarat, 382042, India; 2School of Epidemiology and Public Health, Datta Meghe Institute of Medical Sciences (DMIMS), Wardha, Maharashtra, 442004, India
Correspondence: Deepak Saxena, Indian Institute of Public Health Gandhinagar (IIPHG), Opp. Air Force Head Quarters, Nr. Lekawada, Gandhinagar, Gujarat, 382042, India, Email [email protected]
Background: The disequilibrium in the demand-supply nexus of organ donation prevails an urgent need for understanding the process and cascade of the donation. There is a lack of evidence in organ donation literature within India that focuses on factors influencing familial consent, the decision-making process, and psychosocial factors that can predict successful organ donation. Such evidence can assist in designing interventions and policy dialogue focusing on the discussion on enhancing donation decisions with relatives. Thus, the present study is an effort to document the decision-making complexity systematically among successful cadaveric organ donation cases.
Methods: A qualitative exploratory, including the network assessment was implemented between October 2021 and February 2022 in one of the western states of India, Gujarat. A semi-structured interview guide that was comprised of thematic, open-ended questions focused on understanding the network for the decision-making process was prepared, and trained interviewers conducted the interview at the suitable place of the donor’s relative.
Results: The 10 interviews among the closest relatives of the deceased were conducted and the decision-making process indicated the involvement of multiple actors. The social network analysis reveals a minimum node of 2 to 7, with the highest ties of 22. The maximal degree was 3.6, and the density of 1 of these networks. Out of 10, in most cases, the ties were more than 2, with a maximum of 22 ties, which shows that more people communicated to each other before the final decision-making.
Conclusion: The analysis indicates that the decision-making for deceased organ donation is a complex process as in most cases, multiple family members were involved and interaction happened before the final decision-making. The study explains the decision-making during the cadaveric organ donation process by exploring families’ experiences. Further research is recommended to generate evidence on the factors and the family dynamics, including the complexity of successful organ donation.
Keywords: organ donation, decision-making, social network, India
Introduction
Globally, there is an insistent inequity between organ donation and transplantation.1,2 Although there is widespread recognition of organ donation globally, there is an enormous gap between demand and supply in countries like India.3 In India, there is a need for 258,000 organs/year, which accounts for 185,000 kidneys, 33,000 livers and 50,000 hearts, whereas only 6000 kidneys, 1200 livers and 15 hearts are transplanted annually.4 India has a well-developed tissue donation and transplant program, but deceased organ donation has received minimal attention at the policy level. About eight people’s lives could be saved just by one organ donor, according to the Organ procurement of Transplant Network.5 Unfortunately, India’s deceased organ donation rate is dreadfully low at 0.34 per million population (PMP) compared to a country like Spain, with a donation rate of 36 PMP.3,6 This resulted in organ donation scarcity in India, which can be addressed even if only 5–10% of the persons involved in fatal accidents serve as organ donors.3
In India, the Transplantation of Human Organs Act (THOA) was passed in 1994; as per the act, one can pledge to donate one’s organs after death. The 2014 rules also enable the public to pledge to donate various tissues. Although there is an opt-in system in place, an individual can make his/her wish to donate on their own and the decision to donate or not in the event of brain stem death of an individual rests with the family and their decisions.7 Hence, the family plays a major role in deceased organ donation as they must decide if they want to donate the organs of their loved one to save others’ life or not. Evidence indicates that most relatives remained in a dilemma because of a conflict of values, which is influenced by the disparity between general willingness and actual decisions.8 Further, research has reported that there are differential reasons for denial, such as non-willingness to involve in the donation process, lack of decision-making capacity, and overwhelming emotions.9–11 Among other reasons, desires to reduce the suffering of another or to act according to religious beliefs, social pressures or perceived norms are some of the contributing factors toward the denial.3,12 Evidence indicates two different decision-making approaches, such as “moral decision-making” (influence of one’s decision by the action of others by accepting the social norms) and “rational decision-making” (collecting relevant information with all possible alternatives).8,13
There is a lack of evidence in organ donation literature within India that focuses on factors influencing familial consent, including attitudes to brain death or demographic and psychosocial factors that can predict successful organ donation. Such evidence can assist in designing interventions and policy dialogue focusing on enhancing donation decisions with relatives. However, the household members’ organ donation attitudes and intentions are essential to document to enhance knowledge about how donation rates can be increased. Therefore, we have adapted the conceptual framework in the line of Molina-Pérez et al14 and attempted to understand the complexity of decision-making among the family members and their role in deceased organ donation. The present study aims to systematically document case series on successful cadaveric organ donation and to understand the decision-making process in Gujarat in the year 2021–2022.
Materials and Methods
Study Type
A qualitative exploratory, including the network study, was designed to fulfil the above-mentioned objective of the study, which was implemented between October 2021 and February 2022 in one of the western states of India, Gujarat.
Study Setting
The present study was conducted in the Western part of India in Ahmedabad, located in Gujarat. Ahmedabad is one of the largest heritage cities with a higher density in the population (seven in national ranking) in Gujarat state.15 The Sabarmati River crosses this highly populated city with a population of 8.2 million.16
Study Sample and Sampling
The city documented 29 voluntary organ donations in the year 2021. Initially, the list of donors was procured retrospectively from the daily newspaper, and the index list was consequently compiled and then the geographical information were verified with the register at the Institute of Kidney Disease and Research Centre (IKDRC). It is a recognized organ retrieval, harvesting, and transplantation centre in Ahmedabad, also recognized as the institute of national importance by the Department of Science and Technology, Government of India.
The relatives of donors (cadaveric transplants) who donated their organs during the year 2021 and provided consent to be part of the study were included and interviewed in person. Participants from both upper and low socio-economic backgrounds were included in the study. A total of 29 cases were requested to be part of the study; however, only 10 provided consent for the interview.
Study Data Collection and Analysis
An in-depth qualitative interview (IDI) was planned to undertake the social network analysis to understand the social dynamics and the key actor beyond doctors who was instrumental in decision-making and, ultimately, the successful donation. The interviews were conducted at the date and time convenient to the relatives of the donors after obtaining written informed consent. The IDI of the closest household member who was present during the entire event and part of the discussion on organ donation was conducted. It was decided to personally visit the homes of the deceased and make an initial connection, which eased the IDI later. The IDI was undertaken by two researchers trained to be socially conscious, empathetic and aware of cadaveric organ donation basics. A semi-structured interview guide with open-ended questions was developed for face-to-face interviews. The broader topics of the interview were derived from the literature review, such as details of the event, what are the barriers and facilitators in the decision-making process and what can be done to improve organ donation in India. After obtaining the consent, the audio recording was conducted during the interview, and verbatim notes were taken. Transcripts and the network data based on the cascade of the decision-making were prepared on the same day based on the verbatim notes of the interview, and findings were reported.17
The social network analysis is used to understand a community by mapping the relationships that connect them as a network, then trying to draw out key individuals, groups within the network (“components”), and/or associations between them. The network analysis consists of nodes (sometimes also referred to as actors) connected via some types of relations called ties (also known as links, or edges). Nodes are the people in the network, while ties are the social connections/relationship between individuals in the network (nodes).19 Usually, the social network analysis data could be gathered in a survey; however, similar information through a quantitative survey is difficult while investigating the sensitive topics like organ donation. Thus, a qualitative method was adopted to have the qualitative network analysis of the decision-making process.20,21 The details for network analysis were extracted from the qualitative study, e.g., number of persons involved in decision-making, the relationship with the donor and the decision-making process. The UCINET version 6.723 was used to do the social network analysis.18
Ethics
The study has obtained the Institutional Ethical Committee (IEC) clearance from the Indian Institute of Public Health Gandhinagar, India letter no. TRC/2020-21/28. All the details were kept confidential and complies with the Declaration of Helsinki. Written consent was sought for being part of the interview and recording was done as per the consent of the participant. There was a provision for note taking by two researchers in case permission for audio recording was not given.
Results
The General Characteristics of Donors
Out of 29 cadaveric organ donors, 18 organ donors were residents of the urban municipal corporation area. Overall, 28 organs were donated by these 10 donors. As presented in Table 1, all the donors were male except 1. The age of the donors’ ranges from 32 to 78 years. All donors had completed primary or secondary education except 1 illiterate. Out of 10 donors, 3 were retired, 2 were occupied in private jobs, 2 were labourers, 2 were self-employed, and 1 female donor was a housewife.
 |
Table 1 Basic Profile of Selected 10 Cases of Successful Organ Donation in Ahmedabad, India, During 2021 |
The relation to the deceased person varies from immediate blood relatives like wife, son, daughter, sisters, or brother to extended cousins, nephews, and other family members (Table 1). It was documented that all 10 of the index cases (referred to as cadaveric organ donors) were hospitalized at the government-run Civil Hospital when declared brain dead. A majority (7 out of 10) were shifted to a civil hospital from a private hospital. The referral duration was 3–7 days after being at the private hospital. The respondent’s reason was the high cost of treatment at a private hospital and the probability of longish stay at the hospital. It was observed that the duration of hospitalization and number of hospitals (out of seven who visited more than one hospital) before being declared brain dead took less time in deviance towards organ donation. It was documented that the time between information about the index being declared brain dead and successful organ donation ranged from 12 hrs to 48 hrs. Although it was qualitatively measured, the expressed decision time depended on the number of members involved in decision-making.
Social Network Analysis
The nodes here presented are the individuals who have been part of the decision-making and ties mean the connection between the individuals involved in decision-making. As presented in Table 2, the minimum number of nodes was 2 and the maximum number of nodes was 7, where seven people were involved in decision-making. Out of 10, in most cases, the ties were more than 2, with a maximum of 22 ties, which shows that more people communicated to each other before the final decision-making.
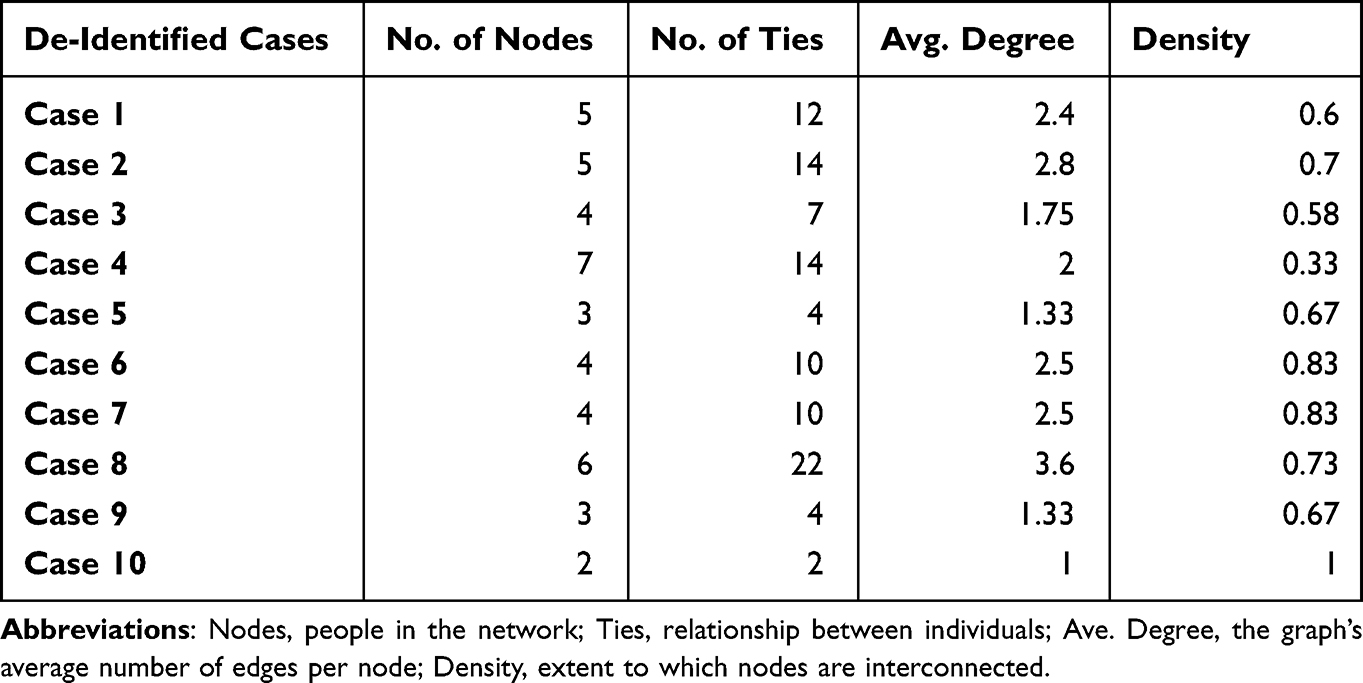 |
Table 2 Key Social Network Analysis Indicators Across the Selected 10 Cases Indicate the Individuals Involved in Decision-Making During Organ Donation in Ahmedabad, India |
Another important indicator is the average degree, which is the graph’s average number of edges per node. The highest average degree was the case with higher ties. This proportionately indicates that the higher the average degree more communication happened among the individuals for the final decision-making.
The density means the extent to which nodes are interconnected, e.g., lower density networks have fewer links between nodes. This density measure helped us understand how connected the network is compared to how connected it might be. Comparing two networks with the same number of nodes and the same type of relationships informed us how the networks differ. For example, the first two cases have an equal number of nodes as 5, with varying densities of 0.6 and 0.7. In an ideal case, if the density is 1, such as in case 10, all possible connections were established by the individuals involved in the decision-making process.
In this study, a bi-directional flow of information was extracted through the transcripts from the participating family members. In Figure 1, individuals with a relationship to the deceased person are mentioned as nodes. The two-headed arrow shows the mutual relationship between both the nodes. The arrows indicate the relationship (ties) with other individuals. The higher the attribute of the node bigger the size. Whereas the single-headed arrow pointing toward one person shows that this person has interacted with the other person, whereas the reverse is true for an arrow pointing away from the other person.
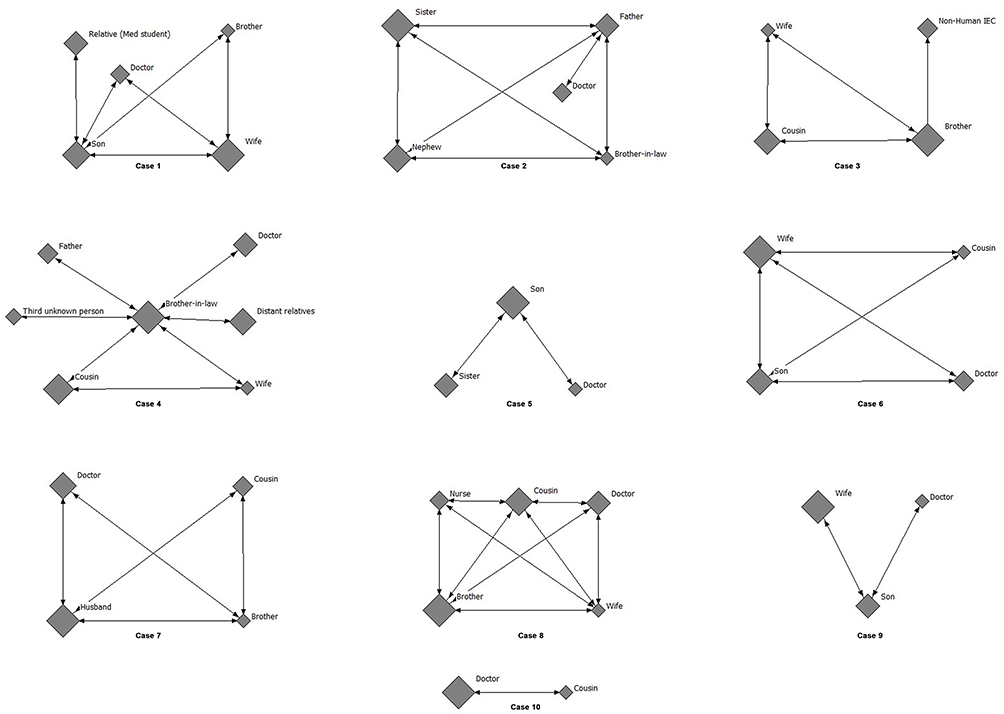 |
Figure 1 Social network diagram of the selected 10 cases of the organ donation and their complexity in decision-making process in Ahmedabad, India, during 2021. |
Case 10 had 2 nodes only, which shows that only two people, i.e., a doctor and one of the family members, were involved in the decision-making process. Contrasting to this, in case 4, there was a maximum number of 7 individuals involved (highest node) with 14 ties (two-way headed arrow) for the decision-making. While in case 8, there are 22 ties, having only 6 individuals involved in the decision-making process.
Discussion
The present social network analysis of 10 cases indicates that the decision-making for deceased organ donation is a complex process. In most cases, multiple family members were involved and interaction happened before the final decision-making. The analysis reveals that the bigger the network size, the longer the decision-making process duration. Global evidence indicates that multiple factors, such as the involvement of different decision-makers concerning the time involved, resulted in the organ donation process’s complexity.22 Further, factors like death circumstances, the coherence of the family members, their socio-economic culture, and their awareness level about the donation might add value to this complexity.22 Additionally, the number of healthcare staff involved in communicating with the deceased family also contribute to the decision-making duration. The decision-making network captured in this study is diverse, with simpler two-way communication to the multi-individual decision-maker. Firstly, the difficulties in the conclusive decision (involvement of multiple family members) were the prime reason documented in this study, which is also confirmed by other research.11 Secondly, some decision-making processes where the network has higher nodes and ties reflect that it might be related to religious beliefs, which require further research. Some studies emphasize religious reasons and that the practice of the religion does not coincide with organ donation, for example, protecting the body for life after death or specific burial rituals.23,24 Thirdly, there was sorrow and extreme sadness due to losing their family member (as per the field notes), which was observed during the interview process and this might be the potential reason for difficulties in decision-making.
In India, there is a long waiting time for organ transplantation due to the inequality in supply and demand. These rates are expected to increase further, leading to potential adverse outcomes for those on the waiting list for organs. The poor awareness about deceased organ donation and the problems of converting eligible donors into actual donors are some of the important reasons for such an organ shortage. The conversion rate from the anticipated donor to the real donor is further depreciated by the decision-making process of the involved actors. Similar observations are seen even in developed countries like the USA, where less than half (among the approached family members) agreed to donate concerning the original decisions.25,26
There is an immense possibility to improve the willingness for cadaveric donations amongst the deceased family member. However, it requires an intensive social network analysis to understand social actors and household members who can be influenced for successful donations in various parts of the globe as per the differential contexts. While physicians have the liberty to educate patients about donation and discuss this, efforts must be made with an active engagement with immediate relatives and other household members to develop shared decision-making for a successful donation. This will require a systematic effort to identify the key decision-maker within the household so that efforts can be included in promoting awareness about organ donation at the policy level.
To help boost organ donation rates, many western countries have resorted to the use of presumed consent, which assumes that an individual is agreeable to donating their organs after death.27 While presumed consent is thought to increase transplant rates, its true impact on increasing organ donation rates is questionable.28 In contrast, a study from an Asian country like Singapore which is a diverse and multi-ethnic society reported that the organ donation rates remain low, albeit presumed consent legislation, due to patient-level barriers, including but not limited to knowledge gaps, cultural values, religious backgrounds, and emotional impact at relatives’ death.28 This finding is consistent with the present study findings.
We assume that this is one of the first studies focusing on social network analysis of the household members for successful cadaveric organ donation from India. The present study highlights that the decision for cadaveric organ donation is a complex process involving many family members, and exploring the barriers in decision-making helps result in a successful donation. Although the decision-making process happens at emergence, the present study revealed that such a social network assists in understanding the complexity of the shared decision-making process. Recent initiatives like the National Organ & Tissue Transplant Organisation (NOTTO) and its adoption by State Organ & Tissue Transplant Organisation (SOTTO) are envisaged to enhance successful organ donation. There are many reasons for cadaveric organ donation; however, lack of organ donation awareness, misperceptions of organ procurement, and negative perceptions of organ donation need to be addressed. Many of these factors can be addressed by effective and sensitive discussions by immediate household members; hence, targeted interventions like awareness campaigns at the community level, wide dissemination of successful stories, and inclusion of organ donation in the school curriculum should be done.
This study has several limitations; first, the social networks were captured through an in-depth interview of only immediate relatives present at the time of donation. Thus, the nodes were collected based on ego-centric network information. It might have been better to understand the complete network analysis by interviewing all the individuals in the decision-making process for a successful organ donation which set the grounds for future, broader studies on this issue. Interviewing all the involved family members in the decision-making is practically a challenge in the studied context. Because most of the deceased person’s relatives were living distantly from the study setting, thus the closest family member was interviewed. Second, the study participants were not stratified based on their education, socio-economic status, and geographical location. It might have been good to explore these networks based on the differences across those socio-demographic variables.
Conclusion
A multi-faceted process includes socio-cultural and diverse “actors” involved in the decision-making process of organ donation. Further, mutual influence from the different involved actors has a major contributing role to the decision-making process. This study highlights the importance of understanding the networks and their influences, including the time taken for a successful organ donation. It recommends the urgent need to streamline organ donation to balance the supply–demand nexus of organ donation in India. The study also reflects a need for a more comprehensive awareness campaign to address the issue of misconceptions and mistrust of the organ donation system. The challenges of tradition can be addressed by involving religious leaders in the awareness generation process.
Acknowledgments
The authors would like to thank the Aangdaan charitable trust and IKDRC for the facilitation of the present work. We would like to thank all the participants for their support and contribution. We wish to thank the experts of IIPHG who contributed their valuable input and feedback to the final draft of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jawoniyi O, Gormley K, McGleenan E, Noble HR. Organ donation and transplantation: awareness and roles of healthcare professionals—a systematic literature review. J Clin Nurs. 2018;27(5–6):e726–e738. doi:10.1111/JOCN.14154
2. Knox K, Parkinson J, Pang B, Fujihira H, David P, Rundle-Thiele S. A systematic literature review and research agenda for organ donation decision communication. Prog Transplant. 2017;27(3):309–320. doi:10.1177/1526924817715459
3. Srivastava A, Mani A. Deceased organ donation and transplantation in India: promises and challenges. Neurol India. 2018;66(2):316–322. doi:10.4103/0028-3886.227259
4. MoHFW-GoI. Under the Aegis of NOTP, Directorate General of Health Services. MoHFW, Govt. of India; NOTTO: National Organ & Tissue Transplant Organisation. 2018.
5. Mohan L, Thanga T, Selvam P. Perspective on organ donation in India: a comprehensive review. J Community Heal Manag. 2020;7(3):73–76. doi:10.18231/J.JCHM.2020.017
6. Chowdhury S, Chakraborty P. Universal health coverage ‑ There is more to it than meets the eye. J Fam Med Prim Care. 2017;6(2):169–170. doi:10.4103/jfmpc.jfmpc
7. Navin SS. Current state of acceptance of brain stem death and organ donation in India. Amrita J Med. 2022;18(2):65–67. doi:10.4103/AMJM.AMJM
8. De Groot J, Van Hoek M, Hoedemaekers C, et al. Decision making on organ donation: the dilemmas of relatives of potential brain dead donors ethics in clinical practice. BMC Med Ethics. 2015;16(1):1–11. doi:10.1186/S12910-015-0057-1/TABLES/3
9. Den Dries SO, Annema C, Den Berg APV, Ranchor AV, Porte RJ. Shared decision making in transplantation: how patients see their role in the decision process of accepting a donor liver. Liver Transpl. 2014;20(9):1072–1080. doi:10.1002/LT.23921
10. Ross LF, Zenios S, Thistlethwaite JR. Shared decision making in deceased-donor transplantation. Lancet. 2006;368(9532):333–337. doi:10.1016/S0140-6736(06)69078-8
11. Siminoff L, Mercer MB, Graham G, Burant C. The reasons families donate organs for transplantation: implications for policy and practice. J Trauma. 2007;62(4):969–978. doi:10.1097/01.TA.0000205220.24003.51
12. Beyar R. Challenges in organ transplantation. Rambam Maimonides Med J. 2011;2(2). doi:10.5041/RMMJ.10049
13. Liu CW, Chen LN, Anwar A, et al. Comparing organ donation decisions for next-of-kin versus the self: results of a national survey. BMJ Open. 2021;11(11):e051273. doi:10.1136/BMJOPEN-2021-051273
14. Molina-Pérez A, Delgado J, Frunza M, et al. Should the family have a role in deceased organ donation decision-making? A systematic review of public knowledge and attitudes towards organ procurement policies in Europe. Transplant Rev. 2022;36(1):100673. doi:10.1016/j.trre.2021.100673
15. Ahmedabad Municipal Corporation. Ahmedabad city: Ahmedabad Municipal Corporation. About Ahmedabad City. 2005.
16. Ministry of Home Affairs. Office of the Registrar General & Census Commissioner, India. Indian Census; 2011.
17. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
18. Borgatti SP, Everett MG, Freeman L. Ucinet for windows: software for social network analysis. 2002.
19. Home Office. Social network analysis: ‘how to guide’; 2016:13. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/491572/socnet_howto.pdf%0Ahttps://www.gov.uk/government/uploads/system/uploads/attachment_data/file/491572/socnet_howto.pdf.
20. Ahrens P. Qualitative network analysis: a useful tool for investigating policy networks in transnational settings? Methodol Innov. 2018;11(1). doi:10.1177/2059799118769816
21. Kelman I, Luthe T, Wyss R, et al. Social network analysis and qualitative interviews for assessing geographic characteristics of tourism business networks. PLoS One. 2016;11(6):1–14. doi:10.1371/journal.pone.0156028
22. López JS, Soria-Oliver M, Aramayona B, García-Sánchez R, Martínez JM, Martín MJ. An integrated psychosocial model of relatives’ decision about deceased organ donation (IMROD): joining pieces of the puzzle. Front Psychol. 2018;9:408. doi:10.3389/FPSYG.2018.00408/BIBTEX
23. Svensson L. The role of relatives in decision making on organ donation: an ethical analysis. 2020.
24. Can F, Hovardaoglu S. Organ donation: a comparison of donating and nondonating families in Turkey. Transplant Proc. 2017;49(9):1969–1974. doi:10.1016/J.TRANSPROCEED.2017.09.032
25. Siminoff LA, Arnold RM, Caplan AL, Virnig BA, Seltzer DL. Public policy governing organ and tissue procurement in the United States. Results from the National Organ and Tissue Procurement Study. Ann Intern Med. 1995;123(1):10–17. doi:10.7326/0003-4819-123-1-199507010-00037
26. Siminoff LA, Arnold RM, Hewlett J. The process of organ donation and its effect on consent. Clin Transplant. 2001;15(1):39–47. doi:10.1034/J.1399-0012.2001.150107.X
27. Bird SM, Harris J. Time to move to presumed consent for organ donation. BMJ. 2010;340(7754):1010–1012. doi:10.1136/bmj.c2188
28. Muthiah MD, Sin M, Chua H, Griva K, Low I. A multiethnic asian perspective of presumed consent for organ donation: a population-based perception study. Front Public Health. 2021;9:1–11. doi:10.3389/fpubh.2021.712584
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.