Back to Journals » Journal of Pain Research » Volume 14
Complex Regional Pain Syndrome: A Comprehensive Qualitative Research Study on Unmet Needs in the “Patient Journey”
Authors Raja SN, Buvanendran A ![]() , Marcondes L
, Marcondes L
Received 26 April 2021
Accepted for publication 15 July 2021
Published 10 August 2021 Volume 2021:14 Pages 2391—2401
DOI https://doi.org/10.2147/JPR.S317648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Srinivasa N Raja,1 Asokumar Buvanendran,2 Lizandra Marcondes3
1Anesthesiology & Critical Care Medicine, Division of Pain Medicine, Johns Hopkins University, Baltimore, MD, USA; 2William Gottschalk, Endowed Chair of Anesthesiology, Rush University Medical Center, Chicago, IL, USA; 3Medical Affairs, Averitas Pharma, Morristown, NJ, USA
Correspondence: Lizandra Marcondes
Medical Affairs, Averitas Pharma, 360 Mt. Kemble Ave, 3rd FL, Suite 3, Morristown, NJ, 07960, USA
Email [email protected]
Purpose: This qualitative research study aimed to characterize the “patient journey” for patients with complex regional pain syndrome (CRPS) and identify the unmet needs related to the management and treatment of the condition for healthcare providers (HCPs), patients, and their caregivers.
Materials and Methods: Multifaceted, dynamic methodology, iteratively gathering cognitive, emotional and social insights, was used to support and conduct in-depth, immersion interviews across the USA with 59 HCPs in-office and in roundtable discussions, and 20 patient-support partner dyads in-home.
Results: Patients were aged > 18 years, primarily female, and all were diagnosed with CRPS (limited to type 1 in this patient cohort). Results show that the current state of CRPS treatment may fall short in multiple key areas. In some cases, poor awareness of CRPS causes delayed diagnoses impacting the opportunity for early treatment, resulting in long-term poor health outcomes. Consequently, the CRPS “patient journey” may be characterized by clinical frustration of physicians and disappointment for some patients. The poor treatment experiences and outcomes for some patients and HCPs may build the perception of a non-collaborative relationship. HCPs and patients agree that an effective treatment would be one that addresses CRPS rather than its symptoms, and the availability of such an option would transform the treatment experience.
Conclusion: CRPS leads to cognitive, social and emotional burdens for patients and their caregivers. There is an unmet need for improved CRPS disease awareness and successful therapeutic options to aid in earlier diagnoses, effective treatment and better outcomes for HCPs, patients, and their caregivers.
Keywords: complex regional pain syndrome, CRPS, pain, patient journey, qualitative
Introduction
Complex regional pain syndrome (CRPS) is a debilitating chronic pain condition characterized by severe pain along with sensory, autonomic, motor and trophic impairment that is seemingly disproportionate in time or degree to the usual course of any known trauma or other disease.1,2 The most common early clinical findings of CRPS are characterized by a “warm” presentation of one or more extremities, including swollen, red, and decreased movement of the extremities. Between 6- and 12-months post onset, the “warm” presentation decreases, and the affected limbs become “cold” as the condition evolves. Although the exact cause of CRPS is unknown, precipitating factors in most cases include trauma or surgery. CRPS is not caused by psychological factors, yet the constant pain and reduced health-related quality of life (QoL) impair activities of daily living and have been known to be associated with psychological co-morbidities.3,4 Income status is not related to the risk of CRPS.
As CRPS remains a diagnosis primarily based on clinical features, internationally recognized diagnostic and research criteria, the Budapest Criteria, were developed by an expert panel to improve recognition of this syndrome.2,5,6 Treatments recommended include physical therapy, pharmacological therapy, psychological treatments including cognitive behavioral therapy (CBT), nerve blocks, and neuromodulation.6,7 The success of these therapies is variable and often unsatisfactory, especially if the diagnosis and treatment are delayed.8 Healthcare providers (HCPs) currently use a variety of drugs to treat CRPS, including antidepressants, anti-inflammatory agents, cyclooxygenase inhibitors, bisphosphonates, gamma-aminobutyric acid analogs, ketamine, N-methyl-D-aspartate receptor antagonists, and opioids.6,9,10 However, although there is a strong evidence base for some drugs (eg, bisphosphonates), there is a general lack of scientific evidence supporting the use of many drugs used to reduce pain and improve functional status in CRPS.11,12 Treatment choices may be influenced by the type of CRPS. CRPS Type 1, formerly known as Reflex Sympathetic Dystrophy (RSD), is a syndrome that usually develops after a noxious or traumatic event (ie, fracture or surgery) resulting in pain which is disproportionate to the event. Complications include tissue atrophy and muscle contracture accompanied by unremitting pain. CRPS, in the absence of nerve injury, is commonly referred to in medical literature as Type I as the vast majority of patients diagnosed with the condition have this type of CRPS.2 It has an incidence rate of 5.46 per 100,000 person-years.13 CRPS Type II, formerly known as causalgia, has symptoms similar to those of CRPS Type 1. However, Type II also has evidence of nerve damage (typically resulting from injury to a peripheral nerve). Additionally, Type II CRPS tends to feature the more painful (usually burning pain) and difficult-to-control symptoms of CRPS;2 it has an incidence rate of 0.82 per 100,000 person years.13 CRPS not otherwise specified is the type that partially meets CRPS criteria and is not better explained by any other condition.2
The combination of impaired social and occupational function, poor QoL, and high rates of depression, has motivated appeals for a greater understanding and further research to address the unmet medical needs of patients with CRPS. Furthermore, the US Food and Drug Administration has declared CRPS a rare disease, which is a strong catalyst for the development of novel and effective therapies.
The patient journey is a multi-stage journey with many different channels and touchpoints along the way, generally describing phases such as: awareness (eg, What’s wrong with me? What’s going to happen to me? What support do I need along the way?), help/information (eg, What can I expect from my friends and family, professionals, and support organizations?), care (eg, How will I cope?), treatment, behavioral/lifestyle change (eg, losing independence, dealing with changing relationships and social roles), and ongoing care/proactive health.14,15 In recognition of the aging global population and the consequent increase in the incidence of chronic conditions, documenting the patient journey has become increasingly important to capture how it feels to face a difficult diagnosis and the impact such a diagnosis has on relationships and QoL.15 Crucially, raising awareness of patient journeys should highlight the need to treat patients, rather than diseases, and to understand the impact that an individual’s journey can have on their carers and families.15 Fundamentally, patient journeys should inform HCPs what really matters to patients and the support that patients need to make the most of their lives.
This qualitative research study, completed in 2016, aimed to characterize the “patient journey” for patients with CRPS and to identify the unmet needs related to the management and treatment of the condition for HCPs, patients, and their caregivers. The key objectives of this study were to understand the impact of CRPS on patients and what triggered the disease; explore the role and impact of CRPS on caregivers; establish the current steps for HCPs related to improving and standardizing diagnosis and treatment; for all stakeholders: define current treatment(s) and explore knowledge level and satisfaction of those treatments, understand awareness of alternative and future treatment options, and assess what additional support is needed for CRPS patients.
Materials and Methods
The qualitative research program was conducted by Insight Consulting Group (ICG, Chicago, IL, USA). Research stimuli were identified through secondary research (including scholarly peer-reviewed articles and clinical guidelines2,5,6,16) and a data audit. Secondary research consisted of web-based browsing/research on topics related to the disease state and current treatment options, and ICG also reviewed previously conducted primary research to help narrow down the questions that would be asked in this patient journey work (to avoid redundancies and to ensure the most critical questions were prioritized/included).
Multifaceted methodology was utilized to support and conduct individual in-depth, 1-hour in-office immersion interviews and 2-hour roundtable discussions with HCPs were conducted at the marker research center to assess treatment challenges, current paradigms and treatment gaps (Figure 1). Interviews were semi-structured with the facilitator using general open-ended probes. The methodology was also dynamic; in addition to being a mixed-target/mixed methodology, the phases of the research were executed iteratively, enabling ICG to adapt and evolve the interviews as more knowledge and points of comparison were obtained. Responses and behaviors were also assessed to understand the cognitive, social and emotional aspects involved in treating CRPS patients. For patients and their support partners, 1-hour individual phone or in-home interviews assessed the impact of CRPS on both parties including the cognitive, emotional and social consequences of the disease (Figure 1). Individuals performing interviews were members of a fully trained market research team with degrees in psychology and experienced in applicable research methodologies.
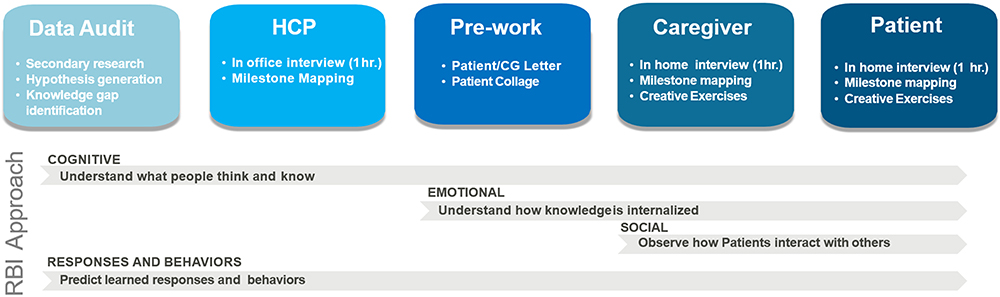 |
Figure 1 Multifaceted, dynamic methodology used to support and conduct in-depth, immersion interviews with healthcare providers, support partners and patients. *The term `Creative Exercises’ refers to collage techniques utilized for the focus groups as a projective technique. Participants’ selection of images act as an instrument to express needs and feelings that they may not otherwise be able to articulate. |
Written informed consent was attained. Patients were recruited via a large patient sample (restricted to several major cities with academic centers) utilizing a patient screening tool (Supplemental File 1). For inclusion in the study, patients had to be aged >18 years, diagnosed with Type I CRPS, with no experience of improvement in their pain management with current medication. Caregivers (aged >18 years) had to be an immediate or extended family member, friend, or professional caregiver of a patient diagnosed with CRPS, with responsibility for supporting and assisting the patient in their disease management, medication management and everyday life accommodations (eg, picking up prescriptions, transporting/accompanying the patient to doctor’s appointments, administering medications) (Supplemental File 2). HCPs, recruited using a Market Research call center via academic centers using an HCP screening tool (Supplemental File 3), had to be currently treating, or have treated in the past year, a patient diagnosed with CRPS symptoms in relevant settings (eg, office, hospital, clinic), and to be aware of primary existing treatments and new treatment developments (assessed by reaction to research stimulus questions, both open-ended and additional reactive probes). HCPs, patients, and caregivers were reimbursed in accordance with appropriate market research practices.
Patients (with support partners) and HCPs were interviewed in-person or virtually across the USA, determined by the location of Centers of Excellence related to CRPS (academic and non-academic hospitals and office-based practice). Patients expressed their journey in a series of stages defined by common cognitive turning points and shaped by shared clinical experiences that impact them physically, emotionally and socially. When allowed by respondents, audio recordings of interviews and discussion groups were made but not full transcription. Thematic analyses were conducted primarily by two members of the ICG research team using thematic analysis, with discussion between the researchers to determine themes; to ensure that evaluation of the data was thorough and unbiased, consensus was obtained with the research team.
Sample size determination was based on the following considerations: (a) the size of the CRPS patient population; (b) accessibility/viability of connecting with target individuals. Because the incidence of CRPS patients is low, HCPs were oversampled to provide a broad representation of patient cases/types by proxy. Additionally, a broad mix of HCP specialties was desired, resulting in a larger sample size. Sample size determinations followed general best practices for strong, directional qualitative data in a low-incidence category.
Unless specified otherwise as “a few” or “some”, reported outcomes represent the majority of participants. Additionally, HCP reported information represents a non-specific quantity of patients.
This qualitative market research study was conducted according to the ISPOR Code of Ethics.17 Clinical Research Ethics Committee or IRB approval for this type of qualitative market research is not required.
Results
In total, 20 patients (with support partners) with disease durations of <2 to >5 years, and 59 HCPs, were interviewed. Patients were aged >18 years, primarily female, and all were diagnosed with Type I CRPS (Table 1). HCPs varied in specialty, thereby providing different perspectives of treating CRPS (Table 1).
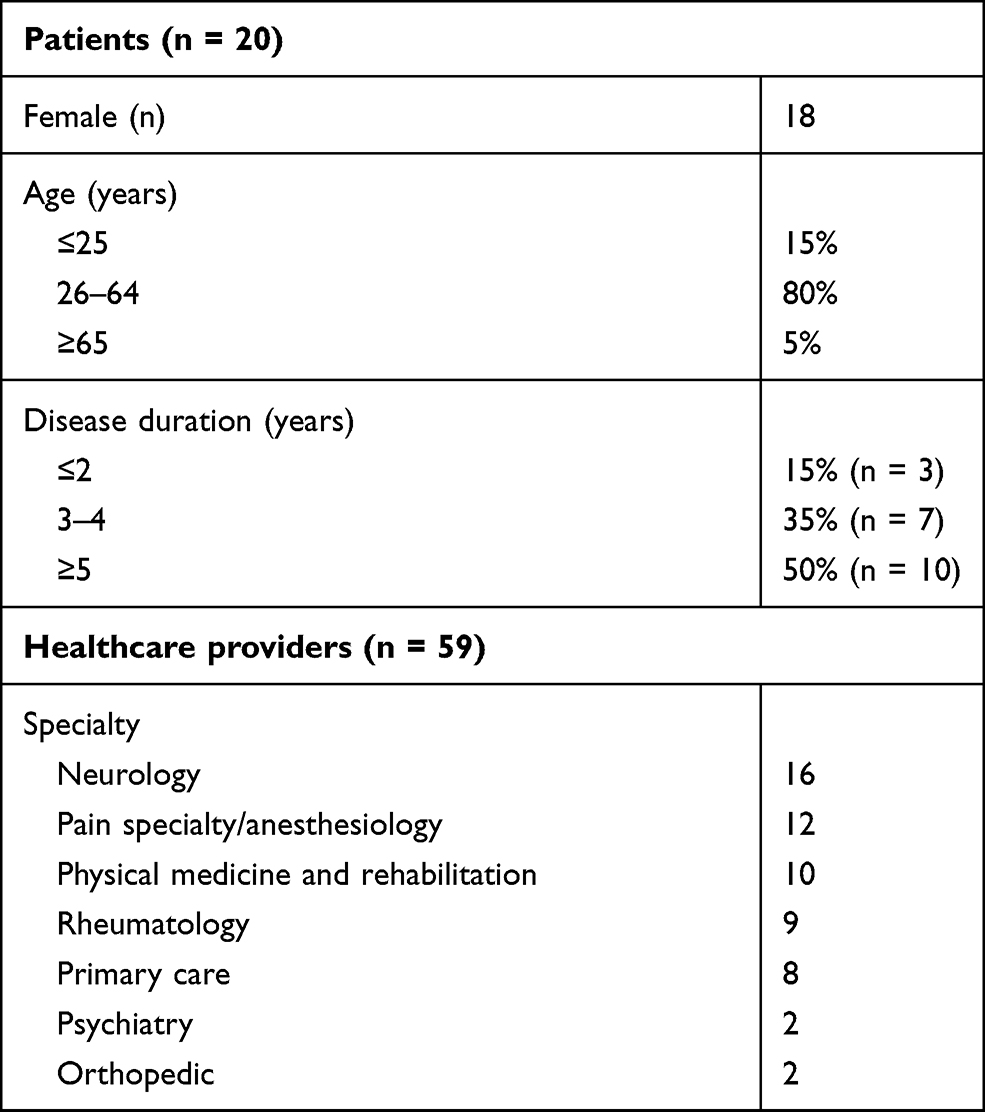 |
Table 1 Characteristics of Patients and Healthcare Providers |
The Impact of CRPS on Patients
Patients with CRPS described their patient journey as being defined by difficult and disappointing clinical progression and levels of personal loss that accompany their debilitating, chronic condition. Patients’ physical experience of CRPS, ie, constant pain and functional decline, force difficult changes in their lives that are made up of five generalizable levels of loss: loss of individuality, loss of identity, loss of independence, loss of intimacy and loss of integrity. These range from slightly more superfluous elements of their self-concept (eg, hobbies) to crucial building blocks of basic humanity (eg, ability to take care of one’s self), with the depth and breadth of loss that patients experience being vast and variable. Patients’ perception of their disease (most importantly their understanding of, and expectations for, treatment) shapes the way in which they view their personal losses – as being increasingly dire, as options are exhausted, and relief is not gained. Figure 2 summarizes the clinical and personal impact of CRPS on each stage of the patient’s journey.
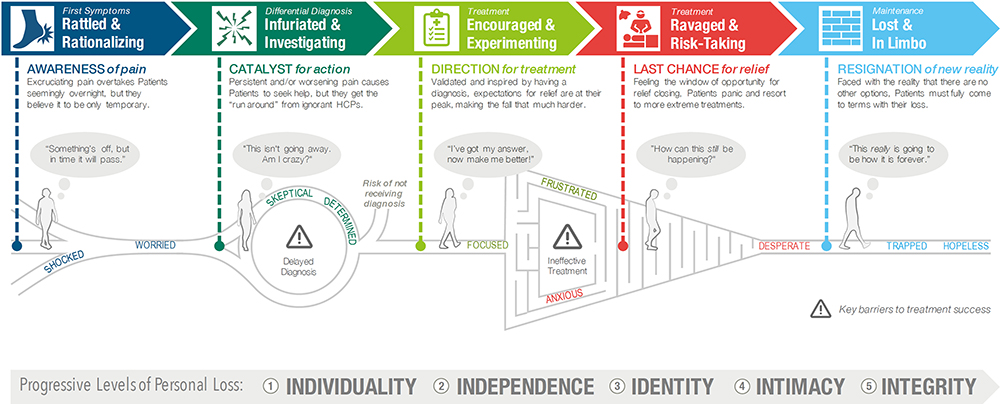 |
Figure 2 The clinical and personal impact of CRPS on patients at each stage of the patient’s journey. |
Based on aggregated interview outcomes from patients and their support partners, CRPS patients report horrific pain that impacts all aspects of their lives. The chronic nature and poor treatment outcomes leave patients disheartened as they face a future of limited functionality due to excruciating pain. As CRPS progresses, patients and their partners experience isolation and depression exacerbated by loss of employment and insurance battles. Before CRPS, patients describe themselves as ambitious and productive, living an active and satisfied life, relating to others easily, enjoying social interactions, free and in control. However, after the disease, they state that they became despondent, a burden on others (as they are unable to accomplish basic goals, eg, cooking consistently), static and sentimental (as they are unable to participate in activities which they previously took for granted), aggressive, self-involved, trapped and dependent.
While all CRPS patients desire relief from their agonizing pain, in this study four generalizable “mindsets” (characterized by personal values) were also noted. These perspectives may provide additional insights into the patient attitudes in the broader CRPS population, affording a more holistic understanding of the CRPS patient experience and affective aspects which may impact treatment approaches. The first type (9 of 20 patients) was those committed to not yielding to CRPS. They attempt to appear unaffected to everyone around them except for their primary support partner. The second type (4 of 20 patients) was represented by those fueled by a sense of purpose. Their self-worth is/was tied to their ability to excel and maintain job stability even if that means suffering through pain. The third type (3 of 20 patients) was driven by family well-being. They pride themselves on maintaining a well-run household and feeling needed versus dependent upon family members (especially their children). The fourth type (4 of 20 patients) was focused primarily on comfort and stability, often leading patients to remain heavily medicated for pain relief resulting in unwanted sedation and other side effects.
Impact of CRPS on Support Partners
Support partners of patients with CRPS also struggle to accept their new life and role amidst the quick succession of changes. Considered to have “second-hand CRPS”, they grapple with major shifts in expectations, responsibilities and way of life, which alters the dynamic of their relationship and threatens its viability. As patients’ CRPS-related needs increase, they find their own (emotional) needs overlooked. In addition, the debilitating effect of CRPS forces financial and domestic responsibilities onto them. As a result, they have to give up on hobbies and plans, and neglect work, which in turn leads to stress and resentment. Over time, the extreme changes and demands of CRPS (physical, financial and emotional) can have a negative impact on relationships, with marital strife being a common result of the major shift in dynamic. For example, due to the physical impact of the condition as well as the emotional strain of the disease on both individuals, relationships between spouses were described as transitioning from romantic (emotionally, physical intimacy) to caretaker/child (lacking intimacy). Support partners and patients described replacing a more transformational relationship (having experiences together, hobbies and activities) with a more transactional relationship (prioritizing necessities like financial planning). Although they are often present at medical appointments, support partners tend to stay out of treatment decisions; because of the abstract nature of CRPS they feel ill-equipped to assist. Desperate to gain control over the situation, they are initially in denial that there is no cure or effective treatment and become convinced of medical incompetence.
The Impact of CRPS on Healthcare Providers
A lack of in-depth knowledge and fragmented care characterizes the CRPS clinical environment. The need for greater awareness of CRPS is at the root of most patient and HCP challenges, and clinical missteps exacerbate patients’ functional decline and emotional fragility. Once the perceived critical window for diagnosis has passed, HCPs describe their ability to make progress in patients’ functionality and pain as significantly compromised, creating frustration and a sense of helplessness felt by all parties involved. In theory, they believe an interdisciplinary, collaborative approach to CRPS is ideal; however, in reality, this level of investment is infrequent. Ultimately, this puts a burden on patients to coordinate and manage their care.
Awareness of CRPS may come from an introduction during residency for some, providing HCPs with context to spot future cases. However, pain management training is often quite limited, creating a void in understanding. Those willing to take on CRPS cases expand their knowledge through first-hand experience and may somewhat inadvertently become “experts.” Bona fide pain management physicians are the most qualified to treat these CRPS patients due to a pain focus in residency, fellowship, and board certification. However, there are a limited number of these pain specialists nationwide which may limit patient access. Early and aggressive treatment is believed to be crucial for positive outcomes in CRPS and to maintain functionality and a normal life. Most HCPs hesitate to solicit advice about CRPS from others because of a poor understanding of the disease and out of respect for how others approach treatment. Because of the past negative clinical experiences of patients, HCPs struggle to gain their trust, and find the lack of effective treatment options disheartening. They agree that the greatest need is a therapy that addresses the root cause of CRPS and provides long-term relief for patients.
Based upon aggregated interview outcomes, HCPs interviewed during the study could be generalized into four different intervention approaches. These styles drove their treatment decisions, the understanding of and experiences with CRPS management, the level of interaction with patients and the knowledge of treatment advancements. Understanding these perspectives provides context about how HCPs may perceive a novel treatment. The four types of HCP intervention approaches are:
- HCPs driven by patient accountability, ie, those who are typically intolerant of the use of opioids, which they associate with “giving up” and believe make the pain worse. These HCPs take a “tough-it-out” approach and believe that success is possible if the patient is prepared to commit to rigorous physical therapy. They are open to, and stay abreast of, new therapies but anything that seems a “quick fix” is viewed with skepticism. A novel treatment for them would provide an alternative to opioids to assist patients in continuing physical therapy.
- HCPs driven by personal relationships, ie, those who prioritize patients’ sense of well-being. They are willing to spend as much time as is needed with the patient and are a source of positivity. These HCPs are often open-minded regarding treatment, are up to date on advances in therapy and encourage patients to be honest about how medications are working in order to help find the right treatment. A novel treatment for them would be an exciting addition to the treatment options for CRPS.
- HCPs focused on expert care, ie, those who are perhaps more aware of CRPS than most but admit to their lack of expertise. To ensure the best possible care for their patients, these HCPs will refer more complex CRPS cases to specialists, such as pain specialists. They believe that treatment should be administered by experts and, therefore, spend minimal effort in familiarizing themselves with new treatment options. A novel treatment would be a consideration for them if it is simple and relatively low risk.
- HCPs focused on relieving pain, ie, who view CRPS as a chronic condition with no cure and ineffective treatment options. They view providing pain relief as their primary role. They recommend opioids as a remedy to mask the pain and, as they are set in their understanding and treatment philosophy, they do not search for new treatment options. A novel therapy for them would be a better option for reducing pain, but only if it is really effective.
Current Diagnoses and Treatment Options
The CRPS diagnosis process is frustrating and tedious for HCPs and patients alike. In many cases, diagnoses took from months to years, due to misdiagnoses being common. Despite the availability of the Budapest Criteria for CRPS,2,3 there is limited awareness among HCPs of an algorithm or specific diagnostic tool to confirm the condition. Consequently, HCPs consider the vagueness of the process as a key reason for the misunderstanding of CRPS, resulting in high instances of misdiagnosis and mistreatment. In an effort to avoid this, HCPs place heavy emphasis on history and physical examination to help rule out conditions that have similar signs and symptoms, such as post-traumatic neuropathic pain, lupus, fibromyalgia and rheumatoid arthritis.
While HCPs vary in exactly how they treat CRPS, they typically follow a similar course, starting first with the least expensive and least invasive options. Nearly all HCPs agree on the importance of physical therapy; thus, the goal of treatment becomes relieving pain to the point where patients can participate in such activities. While more successful if started early, current options do not yield impressive results, with an average of only 30% of patients experiencing substantial relief from pain. As a result, a novel treatment option has an opportunity to play a key role in improving outcomes.
The CRPS treatment paradigm of the HCPs in this research study is summarized in Figure 3. While these HCPs may vary in exactly how they treat, they typically follow a similar course, starting with the least invasive and expensive options first. Specific treatment decisions are made on an individual basis and focused on avoiding intolerable side effects, invasive procedures, risky treatments and high costs. First-line treatments are used to jumpstart patients into physical therapy. While the treatment selection varies depending on HCPs familiarity and comfort level, all agree that physical therapy is crucial throughout treatment – aiding in desensitization and mobility. Physical therapy also provides the emotional benefit of a more intimate treatment. The earlier it is started, the easier it is to continue physical therapy; however, HCPs have to deal with issues that may arise with insurance coverage.
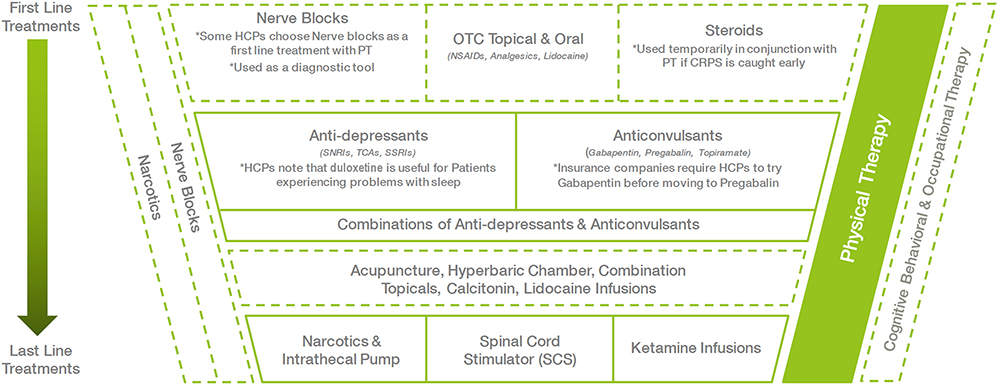 |
Figure 3 Current CRPS treatment paradigm based upon the HCPs in this study. |
As HCPs move into second- and third-line treatments, side effects, such as weight gain, sleep disturbances, gastrointestinal issues, become a bigger concern. Medications are combined and substituted until a balance between efficacy and tolerable side effects is achieved. If the patient has a history of depression or anxiety, HCPs may prescribe duloxetine or another anti-depressant early during treatment and may consult with a psychiatrist to help with management.
When second-line treatments fail to relieve pain, HCPs may try alternative, non-traditional treatments. These are often suggested by patients, vary greatly between cases and are guided by patients’ financial means, ability to travel and hesitation to resort to more extreme measures. Opioids, though rarely considered an effective treatment for CRPS, may be considered as last-line treatments, once all other options have been exhausted. Spinal cord stimulators and ketamine are considered the most risky and costly options. A psychological evaluation must be performed to authorize a spinal cord stimulator, and because of the emotional impact of living with CRPS, many patients do not pass the evaluation. Unfortunately, once patients reach this point, adherence to physical therapy is more likely to suffer.
Unmet Treatment Needs
HCPs express multiple unmet needs from a treatment, support and educational perspective. The current treatment options available are considered generally ineffective and unidimensional, treating only part of the disease. One of the greatest challenges for HCPs is the subjectivity of use of existing diagnostic tools, and they need more effective tools to expedite differential diagnosis and eliminate misdiagnoses. There is also a lack of effective treatment options for CRPS and a need for targeted, evidence-based treatment with proven efficacy in improving the standard of care and delivering desired results. HCPs also identified the need for open communication between specialists to ease patient transition, and greater access to pain psychologists to provide critical specialized mental care that other psychologists are not qualified to provide.
In terms of support, HCPs need opportunities to connect with CRPS experts, collaborate with a multidisciplinary team to treat patients in a holistic manner, easy access to updates regarding CRPS to maintain expertise and ensure delivery of cutting-edge treatment, and assistance in dealing with insurance companies to reduce the burden on patients. From an educational perspective, HCPs need greater awareness in the medical community to improve the quality of CRPS care and increase resources at the HCPs disposal, patient-oriented information for use at diagnosis, a definitive treatment algorithm for confident decision-making and a resource outlining the spectrum of CRPS that provides suggestions and implications for treatment. It is expected that better diagnostic tools and CRPS therapy would decrease complexity of treatment, improve outcomes and ultimately support a better patient-HCP dynamic.
Patient and Support Partner Challenges and Unmet Needs
Patients and support partners also convey an abundance of unmet needs from a treatment, support and educational perspective. Within each stage of the patient’s journey, unmet needs offer insight into the types of resources that would most benefit patients, support partners and HCPs (Figure 4). The CRPS journey is so rife with challenges and barriers that patients tend to lean heavily on those willing and around them to make it through. Because of this reliance and partnership, both parties describe their unmet needs similarly – a need for clinical improvements, bolstered support and greater education/awareness of CRPS.
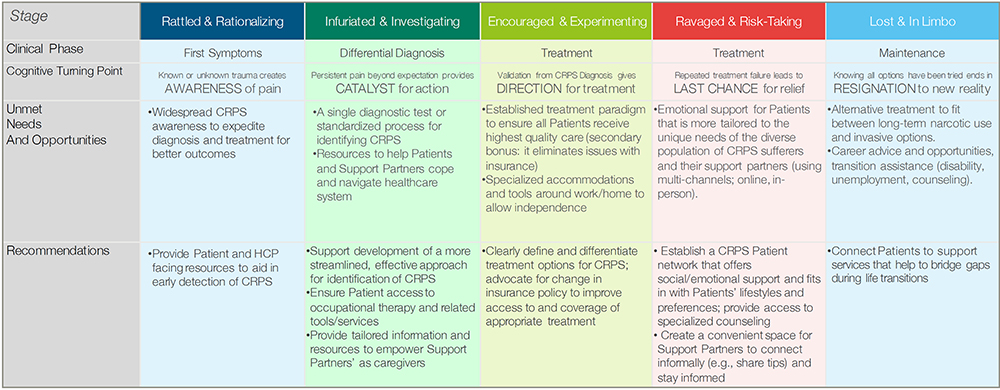 |
Figure 4 Unmet needs in each stage of the patient’s journey and recommended actions to improve the treatment experience. |
One of the greatest challenges patients and support partners face is finding an HCP who will listen and empathize. They desire longer and more holistic sessions with HCPs to discuss the complicated multifaceted aspects of CRPS, open-mindedness and empathy. They would like a treatment that targets the origin of disease rather than managing the symptoms, access to experts with in-depth knowledge of the condition and coordination of care via a multidisciplinary team to ease the burden of disease.
As lack of positivity is a major challenge faced by patients and support partners, they would like a support group with a positive tone. They desire improved manufacturer support (eg, free samples) to improve feasibility of long-term therapy; financial, logistical and transitional support to ease the strain while switching to new careers/living situations; support at work to prolong employment; and access to specialized pain counselling. Other major challenges and unmet needs for patients and support partners include a lack of understanding in their family and a lack of awareness and advocacy in the medical community. There is also a need for a consolidated up-to-date website/resource that would help to set expectations for disease progression and management, more information regarding CRPS and mental comorbidities, and a caregiver-oriented resource. In addition, support partners desire assurance of research and advancement of treatment, an easily accessible support system to receive caretaking tips/emotional support and an easy way to stay updated regarding the condition.
Discussion
This qualitative study shows that the current state of CRPS management falls short in multiple key areas. Poor awareness of CRPS results in delayed diagnoses, treatment limitations and poor health outcomes. These findings support previously published literature, particularly relating to the fact that constant pain and reduced health-related QoL impair activities of daily living in patients with CRPS.3,4 Consequently, our results show that the CRPS “patient journey” is characterized by clinical frustration of physicians and substantial loss for patients. The poor treatment experiences and outcomes for patients and HCPs build the perception of a non-collaborative relationship. Patients stated that major challenges include: (1) Finding an HCP who will listen and empathize, (2) A lack of awareness and advocacy in the medical community, (3) A lack of positivity in support groups, and (4) Feeling misunderstood by others. Our study shows that HCPs and patients agree that an effective treatment would be one that addresses the disease mechanisms of CRPS rather than its symptoms, and the availability of such an option would transform the treatment experience.
Unmet needs at each stage of the patient journey offer insight into the types of resources that would be beneficial for the key stakeholders. Currently, symptoms of CRPS are often not recognized by HCPs or patients until it is too late. Indeed, the early use of appropriate pharmacotherapeutic options, particularly for nociceptive pain, may prevent some of the significant functional limitation, psychological distress, and social and economic consequences associated with CRPS.12 Widespread awareness of the major indicators of CRPS (ie, pain descriptors, physical manifestation, patient history) will allow for quicker diagnosis and better treatment outcomes. A lack of consensus amongst parties who influence care limits the ability to treat CRPS. Thus, widespread knowledge related to the treatment of CRPS in the medical community should help to increase the likelihood of success and reduce conflict with insurance companies, thereby ensuring that precious time is not wasted.
Patient engagement is currently limited because of a depressing outlook on life and adjusting to life with CRPS is made difficult by a lack of specialized resources. An inspirational community environment and a larger CRPS presence online with a positive attitude towards the disease will foster connection amongst the broader CRPS patient population and bolster awareness by word-of-mouth. In addition, a comprehensive support network that ensures access to resources that address the needs of all CRPS-affected personnel (in the clinical, personal, work environments) will provide the holistic support that patients desire. In the US, the RSD Syndrome Association (RSDSA) is one of the organizations that provides patient support, education, advocacy, and financial assistance;16 however, there is a need for increased awareness of such resources.
As a post-study observation, patients with CRPS during the COVID-19 pandemic cannot undergo physical therapy at designated centers, especially in the case of quarantine, nor can they be seen by their physicians and treated.18 All treatment modalities (including psychological) are delayed, and these patients are left to worsen. These observations are echoed in recent international consensus recommendations on caring for patients with pain during the COVID-19 pandemic.19,20
Key limitations of the study are the qualitative nature of the findings, which limit the findings to be directional rather than generalizable, and the small sample size (59 HCPs and 20 patients and support partners). HCP results are limited to the medical field and no allied health, psychology, exercise science, or nutritional/dietary specialists were included. Moreover, the findings are limited to individuals with CRPS for whom medical intervention has not helped, and this may not provide a coherent picture of the experiences of all individuals who have had CRPS. While a key objective of our research study was to inform the unmet treatment needs of CRPS patients, by not sampling people with CRPS who have benefitted, we potentially missed out on identifying key strategies that can result in positive outcomes. A quantitative research study would be useful to confirm the findings of our qualitative research. Although the research tools were not validated, they were standardized in the sense that the same research questionnaire/materials were used for all interviews; however, because of the qualitative nature of the research (executed by a moderator), the questions were personalized and not read verbatim in each interview (and/or the order of questions may have varied with each interview), so some variability still existed. However, the multifaceted, dynamic (iterative) methodology used to conduct the in-depth interviews with HCPs, patients and support partners provides a good understanding of the cognitive, emotional and social consequences of the disease, thereby helping to predict the responses and behaviors of all affected personnel. Moreover, while acknowledging that this research only focused on medical specialties, the varied specialties of the HCPs interviewed across several nationwide markets provide a broad understanding of the current state of disease management. As noted above, no allied health practitioners were sampled in the current study and, despite the important treatment roles of allied health, further work, including a focus on communication between medical specialties and allied health, is needed in that area.
Conclusion
In summary, this qualitative study highlighted the complex and cumbersome journey of CRPS patients. It found that CRPS leads to cognitive, social and emotional burdens for patients and their caregivers. HCPs struggle to diagnose the condition and are frustrated by the generally ineffective treatment options currently available. To aid in early diagnoses, effective treatment and better outcomes, there is a need for improved CRPS disease awareness and successful therapeutic options for patients with CRPS.
Acknowledgments
Medical writing support, under the guidance of the authors, was provided by Sohita Dhillon PhD and David P. Figgitt PhD, ISMPP CMPP™, Content Ed Net, with funding from Grünenthal.
Funding
This qualitative research study was funded by Grünenthal.
Disclosure
Srinivasa Raja is a co-investigator in a research grant from Medtronic and is a recipient of a grant from the National Institute of Health (NIH, NS-26363). He has served as a consultant for Allergan, Aptinyx Inc., Grünenthal, Insys Therapeutics, and Lexicon Pharmaceuticals, Inc. Dr. Raja engaged in the research as a private consultant/advisor and not in his capacity as a Johns Hopkins faculty member. Asokumar Buvanendran is the recipient of a National Institutes of Health grant. Lizandra Marcondes is an employee of Averitas Pharma (Grünenthal).
References
1. Merskey H, Bogduk N. Classification of Chronic Pain: Description of Chronic Pain Syndromes and Definitions of Pain Terms. Seattle: IASP Press; 1994.
2. Harden RN, Oaklander AL, Burton AW, et al. Reflex sympathetic dystrophy syndrome association. Complex regional pain syndrome: practical diagnostic and treatment guidelines, 4th edition. Pain Med. 2013;14(2):180–229. doi:10.1111/pme.12033
3. Iolascon G, de Sire A, Moretti A, Gimigliano F. Complex regional pain syndrome (CRPS) type I: historical perspective and critical issues. Clin Cases Miner Bone Metab. 2015;12(Suppl 1):4. doi:10.11138/ccmbm/2015.12.3s.004
4. de Sire A, Paoletta M, Moretti A, et al. Complex regional pain syndrome: facts on causes, diagnosis and therapy. Clin Cases Miner Bone Metab. 2018;15(2):166–172.
5. Harden RN, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for complex regional pain syndrome. Pain. 2010;150(2):268–274. doi:10.1016/j.pain.2010.04.030
6. Shim H, Rose J, Halle S, et al. Complex regional pain syndrome: a narrative review for the practising clinician. Br J Anaesth. 2019;123(2):e424–e433. doi:10.1016/j.bja.2019.03.030
7. Lim JA, Choi SH, Lee WJ, et al. Cognitive-behavioral therapy for patients with chronic pain: implications of gender differences in empathy. Medicine. 2018;97(23):e10867. doi:10.1097/MD.0000000000010867
8. Bussa M, Guttilla D, Lucia M, et al. Complex regional pain syndrome type I: a comprehensive review. Acta Anaesthesiol Scand. 2015;59(6):685–697. doi:10.1111/aas.12489
9. Giusti A, Bianchi G. Treatment of complex regional pain syndrome type I with bisphosphonates. RMD Open. 2015;1(Suppl 1):e000056. doi:10.1136/rmdopen-2015-000056
10. Zhao J, Wang Y, Wang D. The effect of ketamine infusion in the treatment of complex regional pain syndrome: a systemic review and meta-analysis. Curr Pain Headache Rep. 2018;22(2):12. doi:10.1007/s11916-018-0664-x
11. Resmini G, Ratti C, Canton G, et al. Treatment of complex regional pain syndrome. Clin Cases Miner Bone Metab. 2015;12(Suppl 1):26–30. doi:10.11138/ccmbm/2015.12.3s.026
12. Iolascon G, Moretti A. Pharmacotherapeutic options for complex regional pain syndrome. Expert Opin Pharmacother. 2019;20(11):1377–1386. doi:10.1080/14656566.2019.1612367
13. Goh EL, Chidambaram S, Ma D. Complex regional pain syndrome: a recent update. Burns Trauma. 2017;5:2. doi:10.1186/s41038-016-0066-4
14. What is the patient engagement journey and why is it important?. Available from: https://www.evariant.com/blog/why-is-patient-engagement-journey-important.
15. Lapsley P, Groves T. The patient’s journey: travelling through life with a chronic illness. BMJ. 2004;329(7466):582–583. doi:10.1136/bmj.329.7466.582
16. Reflex sympathetic dystrophy syndrome association (RSDSA) foundation. Available from: www.rsdsa.org.
17. Santos J, Palumbo F, Molsen-David E, et al. ISPOR code of ethics 2017 (4th edition) - appendix 3. Value Health. 2017;20(10):1227–1242. doi:10.1016/j.jval.2017.10.018
18. Coronavirus (COVID-19) and CRPS. March 10, 2020. Available from: https://www.burningnightscrps.org/novel-coronavirus-covid-19-and-crps/.
19. Shanthanna H, Strand NH, Provenzano DA, et al. Caring for patients with pain during the COVID-19 pandemic: consensus recommendations from an international expert panel. Anaesthesia. 2020;75(7):935–944. doi:10.1111/anae.15076
20. Shanthanna H, Cohen SP, Strand N, et al. Recommendations on chronic pain during the COVID-19 pandemic. A joint statement by American society of regional anesthesia and pain medicine (ASRA) and European society of regional anesthesia and pain therapy (ESRA). Available from: https://www.asra.com/content/documents/asra_esra_covid-19_and_chronic_pain.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.