")
Back to Journals » International Medical Case Reports Journal » Volume 17
Complete Congenital Absence of the Left Pericardium in Elderly Patient: A Case Report
Authors Mekonnen S , Farris H , Azmeraw D
Received 14 December 2023
Accepted for publication 9 April 2024
Published 16 April 2024 Volume 2024:17 Pages 347—352
DOI https://doi.org/10.2147/IMCRJ.S454910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vinay Kumar
Sintayehu Mekonnen,1,2 Hawi Farris,3 Daniel Azmeraw1
1Department of Internal Medicine, All Africa Leprosy, Tuberculosis and Rehabilitation Training Center, Addis Ababa, Ethiopia; 2Department of Gastroenterology and Hepatology, Addis Ababa University College of Health Science, Addis Ababa, Ethiopia; 3Department of Radiology, Addis Ababa University College of Health Science, Addis Ababa, Ethiopia
Correspondence: Sintayehu Mekonnen, Email [email protected]
Abstract: Congenital pericardial absence is an uncommon heart condition that is usually undiagnosed due to a lack of symptoms and awareness. In this case study, we present a 72-year-old patient who initially presented for medical evaluation due to unexplained weight loss, a displaced cardiac apex, and poor echocardiographic windows. An extracardiac tumor was suspected at first, but it was later determined that the patient had a congenital complete absence of the left pericardium. This case illustrates the possibility for benign pathology to present abnormally and details the clinical features, imaging findings, and management of congenital absence of the pericardium.
Keywords: pericardium, congenital defect, echocardiography
Introduction
The pericardium is a fibrous sac that surrounds the heart, providing support and protection for the organ. Congenital absence of the pericardium (CAP) is an uncommon cardiac anomaly and the actual prevalence is unclear due to asymptomatic cases, while autopsy and surgical case studies have shown incidences of less than 1 in 10,000 and 0.04%, respectively.1,2 It results from a defect in the formation of the pleuropericardial membrane and might manifest as a partial or complete absence. In 30% of cases, other cardiac syndromes such as Tetralogy of Fallot, patent ductus arteriosus, atrial septal defects, mitral valve disease, sinus venosus defects, and partial anomalous pulmonary venous drainage will be identified.2,3
Due to its rarity, the majority of clinicians will not be familiar with this disorder and might overlook it during thoracic or cardiac examinations, leading to misdiagnosis. Patients are mostly asymptomatic, which makes diagnosis challenging, although occasionally patients will present a variety of clinical signs and symptoms that include chest pain, dyspnea, palpitation with shifting of apical impulse, and systolic ejection murmur.3–7 Partial defects can result in sudden cardiac death from herniation,8 but complete defects are typically benign, and depending on the type of defect and the existence of symptoms, surgical intervention may be necessary.9
This case illustrates an elderly patient initially presumed to have an extracardiac tumor who was later found to have a congenitally absent left pericardium. It aims to increase attention to the disorder and to detail the clinical and imaging findings as well as the management implications.
Case Presentation
This is a 72-year-old male patient, known to have hypertension and has been taking 25 mg of hydrochlorothiazide daily for the past year, comes for a medical exam due to chronic weight loss. He had no chest pain, edema, breathing difficulty, or any other complaints. He is not an alcoholic and never smoked. He had never been assessed from a cardiac perspective and had no personal history of diabetes, or other chronic illnesses. On physical examination, pulse rate was 65 beats per minute, blood pressure 110/70 mm/hg, and temperature 36.6°C. Apical impulse was displaced and the heart sounds well heard no murmur or gallop, the chest is clear on auscultation. Baseline workup including complete blood count, blood glucose, serum albumin, lipid profile, lactate dehydrogenase, erythrocyte sedimentation rate, C reactive protein, thyroid function test, fecal occult blood test, liver and renal function test were normal. Electrocardiography (ECG) showed sinus rhythm, extreme right axis deviation, absent R wave progression, and low voltage on limb leads (Figure 1). Due to the abnormal ECG; echocardiography was ordered and showed a leftward-displaced heart and poor echocardiographic window (Figure 2). Furthermore, except for mild aortic regurgitation, the sizes of the main pulmonary artery, aortic root, and cardiac chambers were normal with an estimated ejection fraction of 64%, and the interatrial and interventricular septum looked intact. Considering the patient’s complaint, a computed tomography (CT) scan including the chest and abdomen was ordered looking for possible extra cardiac tumor. The CT scan’s scout film showed a loss of the right cardiac border as well as a snoopy sign, which is characterized by an elongated and straightened left heart border and displacement of the heart to the left and posterior (Figure 3). Axial CT scan images demonstrated a levopositioned hearthaving a posteriorly directed cardiac apex with an absent left side of the pericardium completely (Figure 4) and an interposition of the lung tissue between the pulmonary artery and aorta (Figure 5). The abdominal CT scan was normal except for a simple liver cyst. The patient was finally determined to have a congenital absence of complete left pericardium based on the chest CT scan finding. Despite a thorough examination, no apparent causes for the patient’s weight loss were found. The patient was reassured, and given advice to maintain good oral hygiene, take a multivitamin supplement, and continue following up.
 |
Figure 1 Twelve lead electrocardiography showing sinus rhythm with first-degree AV block, low voltage limb leads, extreme right axis deviation, and absent R wave progression. |
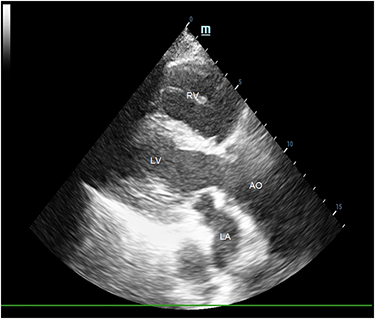 |
Figure 2 Parasternal long-axis view of transthoracic echocardiography, which was taken from an unusual window at the fourth intercostal space along the mid-axillary line. Abbreviations: AO, aortic outflow; LA, left atrium; LV, left ventricle; RV, right ventricle. |
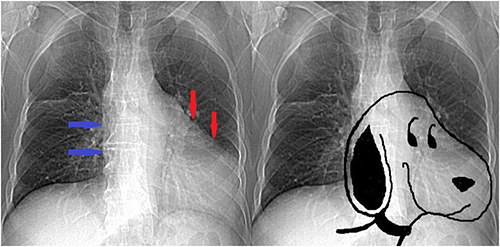 |
Figure 3 The scout film of CT exhibiting the snoopy sign, which is characterized by a leftward and posterior displacement of the heart as well as an elongation and straightening of the left heart border (red arrows). The right cardiac border is also absent (blue arrows). |
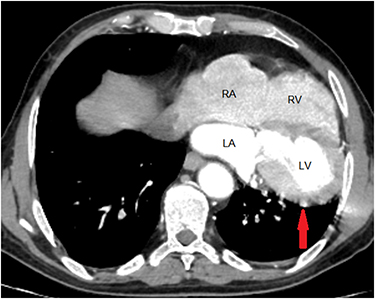 |
Figure 4 An axial CT scan image demonstrates the heart’s displacement into the left hemithorax and the total lack of pericardium along the left ventricular border (red arrow). Abbreviations: LV, left ventricle; LA, left atrium; RV, right ventricle; RA, right atrium. |
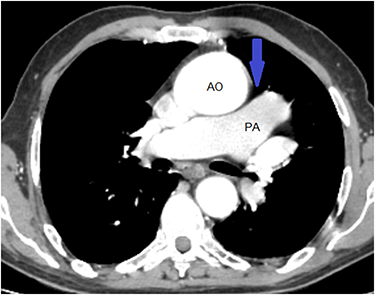 |
Figure 5 Axial CT scan image revealing lung tissue between the aorta and the main pulmonary artery (blue arrow). Abbreviations: AO, aorta; PA, pulmonary artery. |
Discussions
Congenital absence of the pericardium is an unusual disorder that is frequently seen in males and it can be associated with other congenital cardiac abnormalities.2,10 There are six different types of pericardial defects: left (complete and partial), right (complete and partial), complete bilateral, and diaphragmatic absence. Compared to the other types (right side, complete bilateral, and diaphragmatic absence), left-side pericardial absence is more prevalent.3 The proposed etiologic cause for the left pericardial defect is the premature left common cardinal vein atrophy, also called the left duct of Cuvier, between weeks five and six of embryonic development. This atrophy limits the blood supply to the left pleuropericardial fold and prevents it from closing normally.3,9
Although most of the cases show no symptoms and are usually discovered accidentally, a small number of patients may present with chest pain, palpitations, and dizziness.11,12 Signs and symptoms may also resemble acute coronary syndromes, hilar lymphadenopathy, lung, and cardiac tumors.2 A significantly misplaced apical impulse and systolic ejection murmurs likely from excessive heart motion can be detected during the physical examination.4,13 In our patient, weight loss and displaced apical impulses with a poor echocardiographic window were mistakenly considered as an extracardiac tumor. Therefore, it is essential to incorporate CAP while formulating a differential diagnosis for shifted apical impulses.
The ECG features vary depending on the type and size of the defect; small defects may show no abnormalities at all. However, right bundle branch block, low voltage limb lead, right axis deviation, and poor R-wave propagation due to the clockwise rotation are typical findings in left complete pericardial defects.4,11,12 In line with these findings, our case also showed extreme right axis deviation, low voltage limb lead, and poor R wave progression, which are expected from left complete defects. Occasionally, coronary artery kinking from compression might cause abnormalities in the ST segment and T wave.14
A variety of imaging modalities can be helpful for the evaluation and diagnosis of CAP. Loss of the right heart border, a leftward shift and straightening of the left cardiac border (Snoopy sign), and lung tissue between the left hemi diaphragm and the base of the heart as well as between the aortic knob and main pulmonary artery are typical chest x-ray findings, particularly for a left complete pericardial defect.6,13,15 Comparably, the scout film from the CT scan in our case showed loss of the right cardiac contour and straightening and elongation of the left heart border, even though an x-ray was not performed. Poor window is a common observation on echocardiograms, as it was in our case and other characteristic features include cardiac hypermobility, heart swinging, and abnormal ventricular septal motion.16,17 However, echocardiography lacks specificity, and the pericardium cannot be seen directly unless it has thickened.
For confirmation of the diagnosis and characterization of the defect through direct visualization of the pericardium, a CT or cardiac magnetic resonance (CMR) is necessary; nevertheless, because of its higher contrast tissue resolution than a CT scan, CMR is regarded as the gold standard.2,18 As demonstrated in our case, extreme levopositioning of the heart is a feature of left complete pericardial absence, and the interposition of pulmonary tissue where the pericardium should be is a specific indirect appearance that can be observed on a CT scan or CMR.3,5
Owing to the rarity of the condition, patient care and treatment are usually based on observational case studies and it depends on the type, extent of the defect, and the patient’s symptoms. Enlarging the defect, patch sealing the defect, pericardiectomy, and pericardioplasty are among the treatment options that often demand a multidisciplinary team effort. Generally, treatment is not necessary for asymptomatic patients with a complete unilateral or bilateral pericardial defect, as there is a low risk of complications and an excellent prognosis.2,9 But symptomatic patients who underwent surgery to close a complete left-sided lesion reported benefits in terms of symptom resolution in most case reports,7,13 although there is a report in which the symptoms persisted after surgery for an unknown reason.11 Close follow-up is an option for those with mild symptoms4 and symptom resolution without high-risk features.6 In case of partial defects, patients with symptoms or those without symptoms but with imaging-diagnosed herniation signs require surgery to fix the defects.7 It is debatable whether to monitor or do prophylactic surgery on asymptomatic individuals with partial defects to prevent complications from herniation; nonetheless, it is advised to educate the patient about the possible outcomes and opt for observation rather than preventive surgery.2 Treatment was deemed unnecessary and our patient was reassured because there were no symptoms and the left pericardium was completely absent.
Conclusion
Congenital absence of the pericardium is a rare heart disorder, yet it might be misinterpreted as an extracardiac mass lesion. Clinicians need to understand the imaging findings and recognize CAP as a differential diagnosis in older patients with nonspecific symptoms, displaced cardiac apex, and inadequate echocardiographic windows, particularly in those with normal baseline biochemical and metabolic blood workups. Management of pericardial agenesis in the elderly requires multidisciplinary team involvement but in case of left complete absence, the course is benign and life expectancy is not affected.
Data Sharing Statement
The data was included in the report.
Ethical Approval
Ethical approval was not required for a single case report.
Consent for Publication
The patient provided written consent.
Funding
There is no funding to report.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Van Son JAM, Danielson GK, Schaff HV, Mullany CJ, Julsrud PR, Breen JF. Congenital partial and complete absence of the pericardium. Mayo Clin Proc. 1993;68(8):743–747. doi:10.1016/S0025-6196(12)60630-2
2. Shah AB, Kronzon I. Congenital defects of the pericardium: a review. Eur Heart J Cardiovasc Imaging. 2015;16(8):821–827. doi:10.1093/ehjci/jev119
3. Verde F, Johnson PT, Jha S, Fishman EK, Zimmerman SL. Congenital absence of the pericardium and its mimics. J Cardiovasc Comput Tomogr. 2013;7(1):11–17. doi:10.1016/j.jcct.2013.01.003
4. Abbas AE, Appleton CP, Liu PT, Sweeney JP. Congenital absence of the pericardium: case presentation and review of literature. Int J Cardiol. 2005;98(1):21–25. doi:10.1016/j.ijcard.2003.10.021
5. Sergio P, Bertella E, Muri M, et al. Congenital absence of pericardium: two cases and a comprehensive review of the literature. BJR. 2019;5(3):20180117.
6. Ignaszewski M, Baturin B, Waldman B, Peters P. Cardiac eclipse: congenital absence of the pericardium manifesting as atypical chest pain. Case. 2020;4(2):59–62. doi:10.1016/j.case.2019.07.005
7. Gatzoulis MA, Munk MD, Merchant N, Van Arsdell GS, McCrindle BW, Webb GD. Isolated congenital absence of the pericardium: clinical presentation, diagnosis, and management. Ann Thorac Surg. 2000;69(4):1209–1215. doi:10.1016/S0003-4975(99)01552-0
8. Scheuermann-Freestone M, Orchard E, Francis J, et al. Partial congenital absence of the pericardium. Circulation. 2007;116(6):126–129. doi:10.1161/CIRCULATIONAHA.107.701599
9. Xu B, Betancor J, Asher C, Rosario A, Klein A. Congenital absence of the pericardium: a systematic approach to diagnosis and management. Cardiology. 2017;136(4):270–278. doi:10.1159/000452441
10. Bernardinello V, Cipriani A, Perazzolo Marra M, Motta R, Barchitta A. Congenital pericardial agenesis in asymptomatic individuals: tips for the diagnosis. Circulation. 2020;13(5):1–3.
11. Garnier F, Eicher JC, Philip JL, et al. Congenital complete absence of the left pericardium: a rare cause of chest pain or pseudo-right heart overload. Clin Cardiol. 2010;33(2):52–57. doi:10.1002/clc.20607
12. Li XY, Jiang Y, Li HW, Liu YK, Bai J. Congenital absence of the left pericardium: a case report. BMC Cardiovasc Disord. 2023;23(1):1–4. doi:10.1186/s12872-023-03262-3
13. Bouchard M, Hoschtitzky A, Gatzoulis M. Diagnosis and management of congenital absence of pericardium: a case report. Eur Heart J Case Rep. 2019;3(4):1–5. doi:10.1093/ehjcr/ytz223
14. Wilson SR, Kronzon I, Machnicki SC, Ruiz CE. A constrained heart: a case of sudden onset unrelenting chest pain. Circulation. 2014;130(18):1625–1631. doi:10.1161/CIRCULATIONAHA.114.011410
15. Kalekar T, Reddy LP, Koganti D, Soman N. Pericardial agenesis - The wandering heart. Egypt Heart J. 2023;75(1). doi:10.1186/s43044-023-00405-x
16. Connolly HM, Click RL, Schattenberg TT, Seward JB, Tajik AJ. Congenital absence of the pericardium: echocardiography as a diagnostic tool. J Am Soc Echocardiogr. 1995;8(1):87–92. doi:10.1016/S0894-7317(05)80362-1
17. Klein AL, Abbara S, Agler DA, et al. American society of echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the society for cardiovascular magnetic resonance and society of cardiovascular computed tomography. J Am Soc Echocardiogr. 2013;26(9):965–1012.e15. doi:10.1016/j.echo.2013.06.023
18. Cuccuini M, Lisi F, Consoli A, et al. Congenital defects of pericardium: case reports and review of literature. Italian J Anat Embryol. 2013;118(1):136–150.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.