Back to Journals » Nature and Science of Sleep » Volume 18

Complementary Feeding Frequency and Maternal Health: Reducing Anxiety and Improving Sleep Through Biobehavioral Pathways
Authors Shi Y, Zeng P, Fan X, Wang L, He C, Zhou Z, Deng W, Guo J, Zhang Y, Luo Y, Zhao Y ![]() , Wang N
, Wang N
Received 17 October 2025
Accepted for publication 13 January 2026
Published 19 February 2026 Volume 2026:18 571703
DOI https://doi.org/10.2147/NSS.S571703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Ya Shi,1– 4 Peng Zeng,5– 8 Xin Fan,1– 4 Li Wang,1– 4 Chunyan He,1– 4 Ziqi Zhou,1– 4 Wanli Deng,1– 4 Jiaxin Guo,5– 8 Yu Zhang,5– 8 Yaocheng Luo,5– 8 Yong Zhao,5– 8 Nianrong Wang1– 4
1Department of Children Healthcare, Women and Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Children Healthcare, Chongqing Health Center for Women and Children, Chongqing, People’s Republic of China; 3Chongqing Research Center for Prevention & Control of Maternal and Child Diseases and Public Health, Chongqing, People’s Republic of China; 4NHC Key Laboratory of Birth Defects and Reproductive Health, Chongqing, People’s Republic of China; 5School of Public Health, Chongqing Medical University, Chongqing, People’s Republic of China; 6Research Center for Medicine and Social Development, Chongqing Medical University, Chongqing, People’s Republic of China; 7Research Center for Public Health Security, Chongqing Medical University, Chongqing, People’s Republic of China; 8Nutrition Innovation Platform-Sichuan and Chongqing, School of Public Health, Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Nianrong Wang, Department of Children Healthcare, Women and Children’s Hospital of Chongqing Medical University, Chongqing, 401147, People’s Republic of China, Tel +86-139-9616-1120, Email [email protected]
Background: Maternal caregivers of infants frequently experience anxiety and sleep disturbances. Complementary feeding may influence maternal mental health through biobehavioral pathways, yet these mechanisms remain insufficiently explored. This study examined these associations and the moderating role of infant age.
Methods: We recruited 543 mother–child pairs with children aged 6– 23 months from a maternal-child health center in southwestern China. Five WHO-recommended IYCF-CF indicators were assessed: Minimum Dietary Diversity, Minimum Meal Frequency, Minimum Acceptable Diet, Egg and/or Flesh Food Consumption, and Zero Fruit/Vegetable Consumption. Maternal sleep quality and anxiety were measured using the Pittsburgh Sleep Quality Index and Generalized Anxiety Disorder Scale, respectively. Binary and ordinal logistic regression models were used to examine associations and interaction effects with infant age.
Results: Maternal sleep disturbances and anxiety were reported in 27.1% and 18.6% of participants, respectively. The prevalence of complementary feeding indicators ranged from 30– 60%, while Minimum Acceptable Diet remained lowest at 12.5%. In adjusted regression models, mothers of children achieving Minimum Meal Frequency had significantly lower odds of poor sleep quality (OR = 0.67; 95% CI: 0.45– 0.99) and reduced anxiety risk (OR = 0.53; 95% CI: 0.31– 0.91). In minimally adjusted models, Minimum Meal Frequency, Minimum Dietary Diversity, and Zero Fruit/Vegetable intake were inversely associated with several PSQI components, including daytime dysfunction, sleep latency, and subjective sleep quality; however, these associations were attenuated and lost statistical significance after adjustment for infant age. Interaction analyses indicated that infant age moderated the associations of Minimum Meal Frequency and Zero Fruit/Vegetable with maternal sleep outcomes (p < 0.05).
Conclusion: Meeting Minimum Meal Frequency was linked to lower maternal anxiety and fewer sleep disturbances, potentially through reduced caregiving stress, improved infant sleep continuity, and stress- and circadian-related physiological regulation. Integrating sleep-focused guidance into IYCF counseling may support both infant feeding goals and maternal sleep health.
Keywords: maternal sleep disturbance, maternal anxiety, complementary feeding, IYCF, PSQI, GAD-7
Introduction
Maternal anxiety and sleep disturbance are two major health risks in the first 1–2 years after childbirth. Mothers, serving as primary caregivers, experience prolonged reductions in sleep quality lasting up to six years postpartum.1,2 Maternal anxiety is associated with worsening sleep quality and insomnia during pregnancy, and has been closely associated with both sleep disturbances and children’s future growth and developmental outcomes.3 Evidence from the Italian cohort study indicates that maternal anxiety and sleep disturbance significantly increase Attention Deficit Hyperactivity Disorder scores in children.4 Moreover, maternal anxiety is linked to poor child nutrition, particularly a higher risk of underweight in low-income areas of Dhaka.5 A previous study has shown That Sleep disturbances in infants are linked to maternal sleep quality and mental health.6 Moreover, the close association between maternal mental health and infant feeding behaviors reflects the inherently strong bond between mothers and their infants.7 Building on our team’s previous finding from 15 Chongqing districts that proper complementary feeding supports caregiver sleep,8 this hospital-based study in the urban core employs validated maternal sleep scales to provide more specific and actionable evidence.
Breastfeeding and complementary feeding make up most of the nutrition in early life.9 Complementary feeding (CF) is defined as semisolid, soft, or solid foods other than breast, formula, or animal milk.10 According to the World Health Organization (WHO), fewer than 25% of infants aged 6–23 months achieved age-appropriate standards for dietary diversity and meal frequency.11 Failure to achieve age-appropriate dietary diversity and meal frequency increases the risk of infant malnutrition and heightens susceptibility to common infections and mortality during early life.12 The WHO has issued global recommendations on complementary feeding for children aged 6–23 months, aiming to promote optimal growth and development. Guidelines include 17 standardized indicators covering both breastfeeding and complementary feeding practices.13 This study focuses on the complementary feeding status of children aged 6–23 months, particularly examining key indicators such as Minimum Dietary Diversity (MDD) and Minimum Acceptable Diet (MAD).14
Previous studies have shown that maternal anxiety levels have been shown to influence both the timing and approach to complementary feeding in infants.15 Such phenomena are common among postpartum mothers, who tend to place high importance on their child’s caregiving environment and overall health. Among mothers with Major Depressive Disorder, more intensive early feeding patterns have been associated with poorer sleep efficiency and increased psychological distress.16 The cognitive-behavioral model of health anxiety suggests that emotional responses to health-related information result from individuals’ interpretations or appraisals of the situation.17 Specifically, mothers’ heightened concern for their child may lead to maladaptive assumptions about the child’s health, causing them to interpret health-related information in a particularly threatening way, which in turn triggers elevated levels of anxiety.18 Moreover, policy research from Sri Lanka indicates that strengthening healthcare workers’ support for IYCF caregiving education can reduce maternal parenting stress and, in turn, maternal anxiety.19 Fluctuations in mothers’ stress and anxiety are accompanied by shifts in key hormones, and the dynamic interactions among cortisol, oxytocin, progesterone, and estrogen may mediate these associations.20 Melatonin, in particular, shows pronounced circadian rhythmicity and regulates transcriptional pathways essential for daily sleep-wake patterns, making it particularly important for understanding sleep-related difficulties.21,22 Mothers, who often assume a larger share of infant caregiving across socioeconomic contexts, may experience elevated caregiving demands that place them at risk of hormonal dysregulation and reduced secretion of sleep-supporting melatonin and lactational oxytocin.23,24 Additionally, nighttime infant care frequently occurs under artificial light, which disrupts melatonin’s physiological functions and impairs normal circadian entrainment, further intensifying sleep disturbances associated with infant night waking.21,25 These findings highlight the need to examine complementary feeding in the context of maternal dual health challenges.
Current research pays insufficient attention to complementary feeding practices within the In IYCF framework, with particularly limited exploration of how these practices influence maternal anxiety and sleep quality. Infants aged 6–23 months were selected for this study, as this age range aligns with the recommended application period of the IYCF complementary feeding indicators. This study hypothesizes that adherence to appropriate IYCF practices may serve a protective role against sleep disturbances and anxiety in mothers during the complementary feeding stage. Focusing on the southwestern region of China, this research aims to provide new insights into how complementary feeding may address the dual burden of maternal sleep disruptions and anxiety.
Methods
Sample and Design
Participant data were collected from the electronic health records of the Chongqing Health Center for Women and Children, a large academic medical center in the Southwestern CN. The study employed a convenience sampling strategy. Trained physician-investigators, who underwent standardized protocol training, conducted one-to-one interviews with eligible mothers to ensure consistent and reliable data collection. Data were collected for the period from December 1, 2024, to January 31, 2025. This study has been approved by the Institutional Review Board of Chongqing Maternal and Child Health Hospital (REC reference no.2024–083), and written informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Inclusion criteria for this study were i) Mothers who voluntarily participate in the study and provide written informed consent; ii) Mothers aged 18–59 years with children aged 6–23 months; iii) Mothers without severe complications or comorbidities during pregnancy; iv) Mothers able to communicate effectively to provide reliable questionnaire information. Exclusion Criteria for this study were i) Children with severe gastrointestinal diseases, such as active bleeding ulcers; ii) Cases where the mother or child does not meet the specified age requirements; iii) Cases in which communication barriers, as assessed by trained physician-investigators, prevented the collection of valid maternal responses.
Of the 646 mother/child pairs recruited, 2 infants were excluded due to incomplete IYCF feeding practice data, 2 mothers were excluded due to missing education level information, and 99 mother/child pairs were excluded due to incomplete sleep information.
Outcome
Maternal Sleep
Maternal sleep was assessed via the Pittsburgh Sleep Quality Index (PSQI) Chinese version, which is a validated tool for assessing sleep quality in the Chinese population.26 The PSQI combines assessment of seven component scores (subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction) into a global sleep quality score ranging from 0 to 21, a widely used tool for evaluating individual sleep quality.27 Mothers completed the PSQI under the guidance of a physician through face-to-face interviews. Internal consistency for PSQI overall Cronbach’s alpha was 0.76 and the KMO was 0.72. Besides, the reliability and validity coefficients for each dimension of the PSQI were above 0.70, indicating acceptable psychometric properties. Based on previous literature research, we defined a total PSQI score > 5 as indicative of sleep disturbance and a score ≤ 5 as indicative of good sleep quality.26
Maternal Anxiety
Maternal anxiety scores were assessed via the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7). Due to its diagnostic reliability, factorial, construct, and criterion validity, the GAD-7 is today among the most widely used anxiety measures, both in clinical practice and research.28 Mothers completed the GAD-7 scale through face-to-face interviews conducted under the guidance of a physician. The GAD-7 assesses how often individuals have experienced seven core symptoms of generalized anxiety disorder over the past two weeks, with response options including “not at all”, “on some days”, “on more than half of the days”, and “almost every day” (scored 0–3), yielding a total score ranging from 0 to 21.29 In this study, the internal consistency of the GAD-7 was acceptable, with a Cronbach’s alpha of 0.90, and the KMO measure of sampling adequacy was 0.91. Based on previous literature research, we defined a total GAD-7 score >5 as indicative of anxiety and a score ≤ 5 as indicative of no anxiety symptoms.30,31
Exposure
Mothers were asked to recall the types of food and drink and the number of times that their children consumed them in the past 24 h prior to the survey using a food frequency questionnaire.32 IYCF includes two parts, Breastfeeding and Complementary Feeding indicators. A total of 17 IYCF indicators recommended by WHO/ the United Nations agency for Children’s Fund (UNICEF).14 In this study, we focused on the Complementary Feeding indicators section of IYCF (IYCF-CF). We selected 5 indicators [including Minimum dietary diversity (MDD), Minimum meal frequency (MMF), Minimum acceptable diet (MAD), Egg and/or flesh food consumption 6–23 months, Zero-vegetable or fruit consumption 6–23 months (ZVF)] that assess IYCF practices for infants aged 6–23 months indicators based on the age characteristics of the study subjects. Definitions for each of the 5 selected IYCF indicators are provided in Appendix Table 1 from Infant and Young Child Feeding guidance by WHO/ UNICEF.13
Covariates
Relevant covariates were selected using Directed Acyclic Graphs (DAGs) of the proposed relationships between potential covariates, IYCF-CF and maternal sleep, and maternal anxiety based on subject matter knowledge. Selected covariates related to the infant, the mother, and the household were included in the statistical analysis. Infant characteristics included age in months and sex. Maternal characteristics included mother’s age, job, education level, family annual income level and family foster model, and marriage status.
Analyses
Continuous variables were reported as mean ± standard deviation (SD) for normally distributed data, and as median with interquartile range [M (Q1, Q3)] for non-normally distributed data. Categorical variables were presented as counts and percentages [n (%)]. Differences in demographic, socioeconomic, maternal PSQI and maternal anxiety scores parameters between infants’ age in months were assessed using the Chi-square test of association and the t-test, for categorical and continuous data, respectively. Binary Logistic regression analysis was conducted to assess the association between IYCF-CF practices and maternal sleep quality, anxiety scores. Additionally, ordinal logistic regression models were employed to examine the associations between IYCF-CF and each of the seven PSQI components.
Sensitivity analyses were conducted by fitting three models for each regression analysis. Variables included in the models were selected based on the DAGs framework and the results of LASSO regression. Model 1 was unadjusted. Model 2 was adjusted for key demographic variables, including maternal age, occupation, education level, annual household income, and family caregiving model. Model 3 further included infant age to explore the interaction between IYCF practice and infant age in months. All statistical analyses were conducted using STATA software (version 18; Stata Corp LLC, Cary, NC, USA), and the crude odds ratio (OR) or adjusted OR (AOR) with its respective 95% confidence intervals (CI) were reported. All p-values < 0.05 were considered statistically significant.
Results
Overall Characteristics of the Overall Sample
Of 543 mother/child pairs included in the study, 49.2% of children were girls. The majority of mothers (86.9%) were ≤ 35 years old and 98.0% in a state of marriage. Mothers were primarily identified as employees of enterprises (37.8%) or housewives (37.1%). Our sample was highly educated, 91.0% of mothers reported receiving a college degree or above. 35.7% of the family’s annual income at middle class. 72.0% of children were raised by a combination of parents and grandparents. 18.6% of mothers have anxiety status, 27.1% of mothers have sleep disturbance. The distribution of maternal sleep quality was different among infants of different ages (p<0.05). See Table 1 for full participant demographic information.
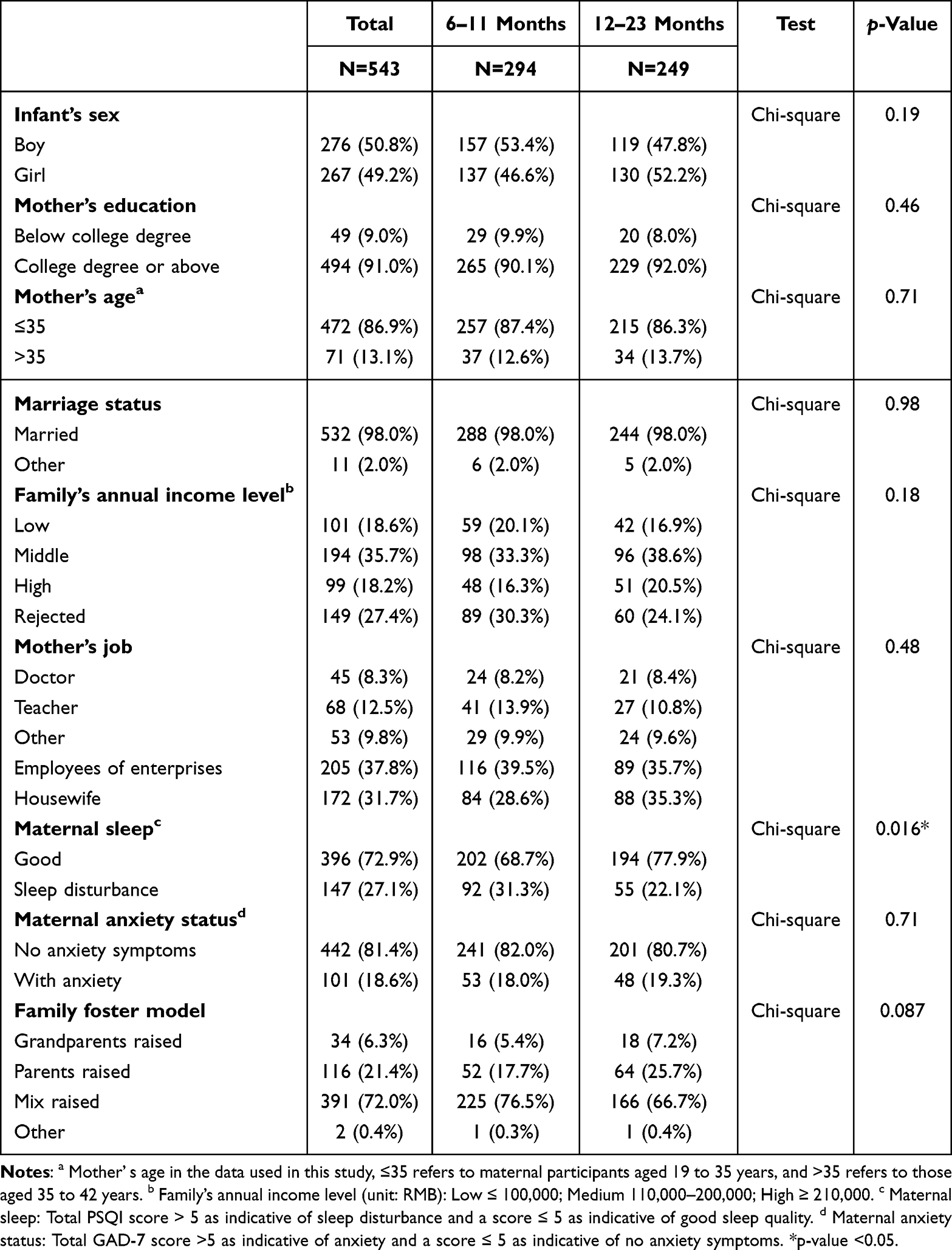 |
Table 1 Demographic Statistics by Infant Age |
Prevalence of IYCF-CF Practices Within Each Infant Age Group
Figure 1 shows that the overall prevalence of MDD, MMF, ZVF and EFF ranging from nearly 30 to 60%, yet the prevalence of MAD was lowest, ranging nearly 12%. The rates of achieving MDD, MMF, MAD and ZVF were higher in infants aged 12-23 months than in infants aged 6-11 months, while the rates of achieving EFF were opposite.
 |
Figure 1 Attainment of overall IYCF-CF practices (A) and by infant’s age in months (B). |
Prevalence of Practices of IYCF-CF by Maternal Status
As shown in Figure 2, the prevalence of MDD, MMF, ZVF and EFF ranged from nearly 24 to 65%, yet the prevalence of MAD was lowest, ranging from nearly 8 to 14%. In addition, mothers with sleep disturbance had higher rates of reaching targets for MAD, and EFF than those with good sleep quality, except for MDD, MMF and ZVF. Mothers with anxiety had higher rates of reaching targets for EFF than those with no anxiety symptoms, except for the other indicators.
 |
Figure 2 Attainment of IYCF-CF Practices by Maternal Sleep Status (A) and Maternal Anxiety Status (B). |
Relationships Between Infant Age and Maternal Sleep and Anxiety Status
As shown in Table 2, Mothers of infants aged 12–23 months had improved sleep compared with those of infants aged 6–11 months (Model 1: OR = 0.62, 95% CI: 0.42–0.92, p = 0.017; Model 2: OR = 0.61, 95% CI: 0.41–0.91, p = 0.016). No significant association was found between infant age (6–11 vs 12–23 months) and maternal anxiety in model 1 and model 2.
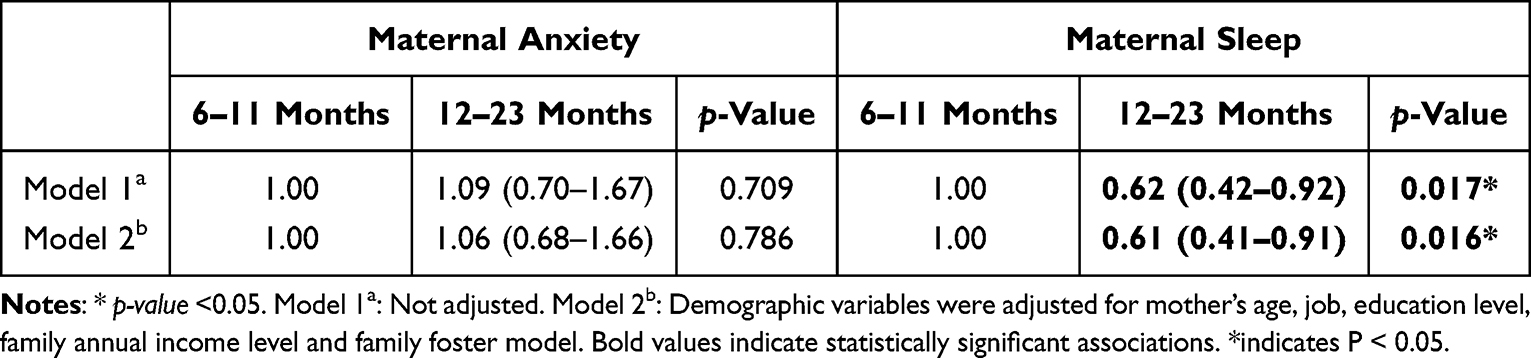 |
Table 2 Association Between Infant Age and Maternal Status |
Relationships Between IYCF-CF Practices and Maternal Sleep and Anxiety Status
Table 3 presents the results that, in both Model 1 and Model 2, Mothers of children achieving MMF had significantly lower PSQI scores (OR= 0.66, 95% CI: 0.45 to 0.96, p = 0.030; OR= 0.67, 95% CI: 0.45 to 0.99, p = 0.045, respectively). No associations were found between other IYCF-CF practices and maternal sleep (p > 0.05). In model 3, MMF was significantly associated with maternal anxiety (OR= 0.53, 95% CI: 0.31 to 0.91, p= 0.021). No associations were found between other IYCF-CF practices and maternal anxiety (p > 0.05).
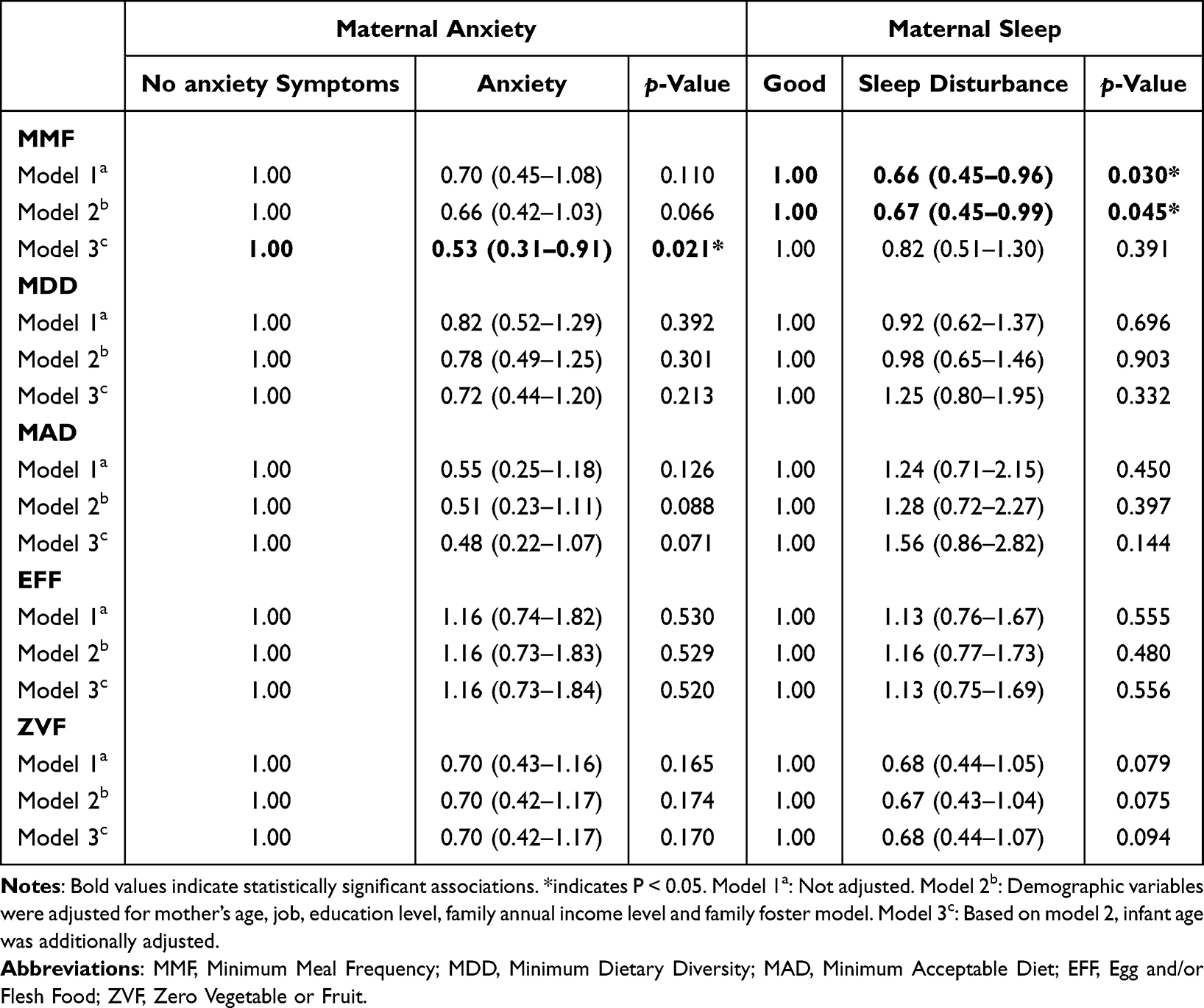 |
Table 3 Association Between IYCF-CF Indicators and Maternal PSQI and Anxiety Status |
Children who achieved MMF, ZVF, and MDD were negatively associated with maternal daytime dysfunction. In addition, MMF and MDD were significantly negatively correlated with maternal sleep latency, and MMF was significantly negatively correlated with maternal subjective sleep quality. However, after adjusting for the infant age, these associations were no longer statistically significant (see Appendix Table 2).
Stratified Analyses of Interaction Effects Between IYCF-CF Practices and Infant Age
As shown in Figures 3 and 4, compared to mothers of infants aged 6–11 months with suboptimal MMF or ZVF, mothers of infants aged 12–23 months exhibited significantly better sleep quality. However, no significant interactions were observed between other IYCF-CF practices and infant age. Furthermore, the combined effect of infant age and IYCF-CF practices did not significantly influence maternal anxiety levels.
 |
Figure 3 The joint effect of infant age and IYCF-CF practice on maternal sleep. Abbreviations: MMF, Minimum Meal Frequency; MDD, Minimum Dietary Diversity; MAD, Minimum Acceptable Diet; EFF, Egg and/or Flesh Food; ZVF, Zero Vegetable or Fruit. Notes: Demographic variables were adjusted for mother’s age, job, education level, family annual income level and family foster model. |
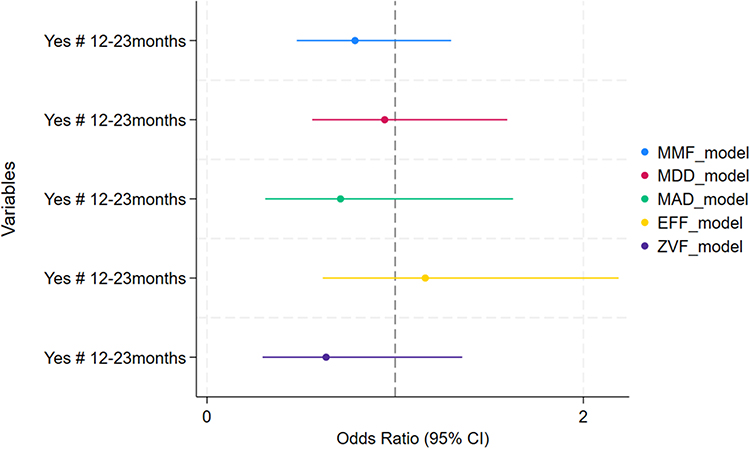 |
Figure 4 The joint effect of infant age and IYCF-CF practice on maternal anxiety. Abbreviations: MMF, Minimum Meal Frequency; MDD, Minimum Dietary Diversity; MAD, Minimum Acceptable Diet; EFF, Egg and/or Flesh Food; ZVF, Zero Vegetable or Fruit. Notes: Demographic variables were adjusted for mother’s age, job, education level, family annual income level and family foster model. |
Discussion
Maternal sleep disturbances and anxiety are common throughout the CF practices period and pose significant public health concerns.4,33 A meta-analysis covering 34 countries across six continents estimated the prevalence of perinatal anxiety at nearly 20%.34 Another review reported postpartum sleep disturbance rates as high as 67.2%, with anxiety prevalence ranging from 18.3% to 29.4%.35 Poor maternal sleep, particularly in late pregnancy, has been associated with adverse neuropsychological and behavioral outcomes in children36 and may increase the risk of psychological distress within young families.37
Our study, conducted in Chongqing major urban center in southwest China-found that 27.1% of mothers experienced postpartum sleep disturbances, while 18.6% reported anxiety symptoms. Sleep disturbances were more common among mothers of infants aged 6–11 months compared to those with children aged 12–23 months.
Compared to reports from lower-income regions such as parts of the Middle East, where maternal sleep disturbance rates can reach 72%,38 our findings suggest a relatively lower prevalence in Chongqing. This may be attributed to higher socioeconomic status (SES), with 53.7% of participating families reporting middle-to-upper income levels. Access to resources such as postpartum caregivers (eg, “yuesao”) may buffer sleep problems but may not mitigate psychological stress, as economic demands and societal expectations may contribute to anxiety.
Additionally, 72.6% of infants were cared for through mixed caregiving (parents and grandparents). While grandparental support can ease maternal workload, intergenerational caregiving conflicts may increase maternal stress. These findings underscore the need for targeted CF period mental health interventions that address both sleep and anxiety, particularly in rapidly urbanizing settings.
Breastfeeding and complementary feeding are key to early-life nutrition. Undernutrition contributes to 45% of infant deaths globally, with 2.7 million deaths annually in LMICs.9 Our study in Southwest China revealed suboptimal IYCF practices: MMF, MDD, ZVF, and EFF ranged from 30–60%, while MAD was as low as 12.5%, much lower than previous studies in urban or welfare-covered regions. In the study by other scholars in Chongqing, the proportion of non-vegetables at 7–9 months of age was close to 30%, and the proportion of egg intake was 40%.39 For example, in urban Chinese ECE centers, the prevalence of MDD, MMF, and MAD was 59.4%, 60.6%, and 39.2%,40 respectively; in rural Qinghai, these were 63.4%, 55.6%, and 39.3%.41 This may reflect that most mothers in our study were from nutrition-improvement areas not covered by national welfare (eg, Yingyangbao). Welfare support, such as WIC, is known to positively impact feeding behaviors, frequent feeding to reassure infants and young children is the mainstay.42 In addition, the qualified rates of MDD, MAD, and MMF were 69.2%, 68%, and 41.9%, respectively, which were significantly higher than those in other areas.43 Conversely, employment and higher maternal education may paradoxically reduce feeding quality due to time constraints and stress.44 This may also explain the low IYCF-CF compliance rate among our 68% of working women and 91.0% of those with post-college education. External factors-advertising, social norms-and cultural influences (eg, food aversions, parental overcontrol) further contribute.45 Precise feeding often limits dietary diversity and frequency.46 Evidence from the Sleep SAAF RP intervention47 shows that targeted support can improve practices, suggesting that enhancing hospital-based IYCF education is essential, particularly for mothers and primary caregivers.
Maternal perceptions of sleep disturbances and stressors vary cross‑culturally, yet concerns regarding infant health and behavior emerge as a key factor connecting caregiving stress to maternal sleep and anxiety. This pattern is supported by studies from Iran, Italy, and Jordan, where infant‑related worries were identified as a major source of parental stress.24,48,49 A qualitative study in the Congo found that maternal stress and perceived feeding concerns-such as weight loss, further exacerbated anxiety.33 Beyond anxiety, maternal sleep disorders also pose serious health threats. Feeding infants while fatigued-often leading to mothers falling asleep during breastfeeding common and heightens the risk of accidental harm. Our results indicate a clear behavioral distinction: meeting the MMF was directly associated with a lower likelihood of maternal sleep disturbances, whereas failing to meet MMF was associated with poorer sleep outcomes. However, the presence or absence of adequate complementary feeding practices, including MMF, did not correspond to meaningful differences in maternal anxiety levels. Prior research also found no strong association between feeding practices and maternal worry.50 From a mechanistic perspective, adherence to MMF may alleviate caregiving stress and enhance mothers’ confidence in their child’s nutritional status, thereby helping stabilize key hormonal pathways-particularly melatonin-, oxytocin-, and cortisol-related regulation-that support circadian alignment and sleep quality.20,24,49 In contrast, multiparous mothers, who carry greater cumulative caregiving demands, may find it more difficult to maintain MMF, a strain that can heighten stress and dysregulate cortisol secretion through the HPA axis, increasing vulnerability to anxiety.51 Studies show that half of mothers reported adding cereal to bottles,47 and fewer than 5% mentioned feeding eggs, meat, legumes, or nuts. In Chongqing, cereals were the most common first food (77.3%).39 Additionally, we observed an interaction between child age and feeding: among mothers of 12–23-month-olds, meeting MMF and ZVF standards significantly reduced the risk of sleep disturbances compared to mothers of younger infants. The observed reduction in sleep disturbances could stem from decreased infant gastrointestinal distress (due to restricted fermentable fibres) and enhanced calming effects of frequent feedings, collectively improving infant-parent sleep continuity.52,53 Moreover, increased infant age is generally considered a protective factor against maternal sleep disruption54 and maternal sleep self-regulation and improvement.55
While breastfeeding has been extensively studied for its impact on maternal health, research on the effects of IYCF-CF practices on postpartum maternal mental health remains limited. This study highlights a novel finding: adequate IYCF practices may help alleviate the dual burden of anxiety and poor sleep commonly experienced by mothers. A key strength of this study lies in its methodological advancements over prior research. We not only employed validated sleep scales to improve the measurement and comparability of sleep quality but also incorporated maternal anxiety to explore the effects of complementary feeding on maternal health from multiple dimensions. Moreover, the use of nationally standardized IYCF indicators to assess feeding practices ensures a consistent and objective benchmark. Our study offers a conceptual framework that may help explain how complementary feeding behaviors relate to maternal sleep. By considering caregiving demands, stress-response processes, and circadian regulation as potential pathways, these findings provide a plausible lens through which to interpret the observed associations between feeding practices and sleep outcomes. This perspective also has implications for IYCF programming: aligning feeding schedules with developmentally appropriate meal frequency may help stabilize infant routines and, in turn, support more predictable maternal sleep opportunities. Incorporating sleep-focused guidance into IYCF counselling and maternal-child health services could therefore enhance program relevance by addressing both nutritional practices and their potential spillover effects on maternal well-being. However, several limitations should be considered when interpreting these findings. First, the cross-sectional design restricts causal inference and limits understanding of the temporal dynamics linking complementary feeding behaviors with maternal sleep quality and anxiety. Longitudinal studies, ideally incorporating mechanistic approaches to clarify biological and behavioral pathways, are needed to establish directionality and capture changes across the complementary feeding period. Second, although validated instruments were employed, reliance on self-reported feeding practices and subjective sleep measures may introduce information bias. Future research should integrate objective sleep-monitoring tools (eg, actigraphy) and digital dietary tracking systems to enhance measurement accuracy. Third, 90.1% of participating mothers held a college degree or higher, representing a highly educated subgroup within the specific context of urban China. This limits the generalizability of findings to populations with different educational, socioeconomic, or cultural backgrounds-particularly in settings where infant‑feeding practices and maternal roles may be shaped by distinct cultural norms and family structures. Broader recruitment across more diverse maternal populations will be essential to strengthen external validity and advance understanding of behavioral mechanisms linking infant caregiving and maternal sleep health.
Conclusion
In this study from Chongqing, a major metropolis in Southwest China, we examined highly educated mothers of children aged 6–23 months. Despite this profile, maternal sleep disturbances (27.1%) and anxiety (~20%) remained common, and adherence to core IYCF practices-including MDD, MMF, MAD, and EFF-was lower than in comparable studies. Only 12.5% of children met MAD intake recommendations.
Improved adherence to MMF was linked with lower maternal anxiety and fewer sleep disturbances. Although causal inference is not possible in this cross-sectional design, these associations may reflect underlying biobehavioral pathways. More regular feeding routines may improve maternal sleep through multiple pathways. In addition to supporting hormonal regulation-particularly cortisol, melatonin, and oxytocin, which are involved in circadian alignment and stress buffering-adequate feeding practices may also promote infant satiety, reduce gastrointestinal discomfort, and enhance infant sleep continuity. These effects may be especially pronounced among older infants, for whom improved feeding regularity and maturation-related sleep consolidation jointly reduce nocturnal caregiving demands and support maternal sleep quality. Embedding brief maternal sleep support into IYCF counselling and postpartum services, following the global complementary food addition recommendation guidelines, may better address the interconnected nutritional and sleep needs of mothers and infants. Such integration could enhance caregiver well-being while strengthening the effectiveness of complementary feeding programs.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author N.W., upon reasonable request.
Author Contributions
All authors meet the ICMJE criteria for authorship and are accountable for all aspects of the study. Specific contributions are as follows: Ya Shi: writing-original draft, Investigation, Methodology, Formal analysis, Data curation, Conceptualization. Peng Zeng: Writing-review & editing, Investigation, Formal analysis. Xin Fan: Writing-review & editing, Investigation, Formal analysis. Li Wang: Writing-review & editing, Investigation, Data curation. Chunyan He: Writing-review & editing, Investigation, Data curation. Ziqi Zhou: Writing-review & editing, Investigation, Data curation. Wanli Deng: Writing-review & editing, Investigation, Data curation. Jiaxin Guo: Writing-review & editing, Investigation, Data curation. Yu Zhang: Writing-review & editing, Investigation, Data curation. Yaocheng Luo: Writing-review & editing, Investigation, Data curation. Yong Zhao: Writing-review & editing, Formal analysis, Supervision. Nianrong Wang: Writing - review & editing, Supervision, Methodology, Investigation, Conceptualization, Funding acquisition. All authors agreed on the journal to which the article will be submitted, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, agrees to take responsibility and be accountable for the contents of the article.
Funding
This study was supported by grants from Chongqing Municipal Education Commission (grant no. 233157) and the China Foundation for International Medical Exchange (PI) (grant no. 2022SQJ3034).
Disclosure
The authors completed the ICMJE Unified Competing Interest form and declare no conflicts of interest.
References
1. Richter D, Krämer MD, Tang NKY, Montgomery-Downs HE, Lemola S. Long-term effects of pregnancy and childbirth on sleep satisfaction and duration of first-time and experienced mothers and fathers. Sleep. 2019;42(4):zsz015. doi:10.1093/sleep/zsz015
2. Saxbe DE, Schetter CD, Guardino CM, et al. Sleep Quality Predicts Persistence of Parental Postpartum Depressive Symptoms and Transmission of Depressive Symptoms from Mothers to Fathers. Ann Behav Med Publ Soc Behav Med. 2016;50(6):862–13. doi:10.1007/s12160-016-9815-7
3. Zhang Y, Hu Y, Talarico R, et al. Prenatal Exposure to Ambient Air Pollution and Cerebral Palsy. JAMA Network Open. 2024;7(7):e2420717. doi:10.1001/jamanetworkopen.2024.20717
4. Vizzini L, Popovic M, Zugna D, et al. Maternal anxiety, depression and sleep disorders before and during pregnancy, and preschool ADHD symptoms in the NINFEA birth cohort study. Epidemiol Psychiatr Sci. 2018;28(5):521–531. doi:10.1017/S2045796018000185
5. Karim KMR, Islam MH, Tasnim T, Akter S. Child undernutrition is associated with maternal mental health and other sociodemographic factors in low-income settings in Dhaka, Bangladesh. PLoS One. 2025;20(5):e0322507. doi:10.1371/journal.pone.0322507
6. Andrade Correia LT, Coimbra DG, Gitaí DLG, Gitaí LLG, de Andrade TG. Associations between chronotype, sleep quality, maternal mental health, and child development in mother-infant dyads. Sleep Med. 2023;106:90–96. doi:10.1016/j.sleep.2023.03.023
7. McMahon C, Barnett B, Kowalenko N, Tennant C, Don N. Postnatal Depression, Anxiety and Unsettled Infant Behaviour. Aust N Z J Psychiatry. 2001;35(5):581–588. doi:10.1080/0004867010060505
8. Shi Y, Li S, Chen J, et al. Complementary Feeding and Caregiver Sleep: findings from a Representative Survey in Chongqing, China. Front Nutr. 2025:12. doi:10.3389/fnut.2025.1586206.
9. Lassi ZS, Rind F, Irfan O, Hadi R, Das JK, Bhutta ZA. Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: systematic Review. Nutrients. 2020;12(3):722. doi:10.3390/nu12030722
10. Embleton ND, Fewtrell M. Complementary feeding in preterm infants. Lancet Glob Health. 2017;5(5):e470–e471. doi:10.1016/S2214-109X(17)30151-1
11. WHO. Infant and young child feeding. Available from: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding.
12. Lassi ZS, Irfan O, Hadi R, Das JK, Bhutta ZA. PROTOCOL: effects of interventions for infant and young child feeding (IYCF) promotion on optimal IYCF practices, nutrition, growth and health in low‐ and middle‐income countries: a systematic review. Campbell Syst Rev. 2018;14(1):1–26. doi:10.1002/CL2.189
13. UNICEF Programming Guidance Complementary Feeding. Portrait FINAL PDF|PDF|Malnutrition|Foods. 2020. Available from: https://www.scribd.com/document/447224780/UNICEF-Programming-Guidance-Complementary-Feeding-2020-Portrait-FINAL-pdf?utm_source=chatgpt.com.
14. WHO. Indicators for assessing infant and young child feeding practices: definitions and measurement methods. Available from: https://www.who.int/publications/i/item/9789240018389.
15. Brown A. Differences in eating behaviour, well‐being and personality between mothers following baby‐led vs. traditional weaning styles. Matern Child Nutr. 2015;12(4):826–837. doi:10.1111/mcn.12172
16. Sharkey KM, Iko IN, Machan JT, Thompson-Westra J, Pearlstein TB. Infant Sleep and Feeding Patterns are Associated with Maternal Sleep, Stress, and Depressed Mood in Women with a History of Major Depressive Disorder. Arch Womens Ment Health. 2016;19(2):209–218. doi:10.1007/s00737-015-0557-5
17. Salkovskis PM, Clark DM. Panic disorder and hypochondriasis. Adv Behav Res Ther. 1993;15(1):23–48. doi:10.1016/0146-6402(93)90002-J
18. Rimes KA, Salkovskis PM. Prediction of psychological reactions to bone density screening for osteoporosis using a cognitive-behavioral model of health anxiety. Behav Res Ther. 2002;40(4):359–381. doi:10.1016/S0005-7967(01)00015-8
19. Godakandage SSP, Senarath U, Jayawickrama HS, et al. Policy and stakeholder analysis of infant and young child feeding programmes in Sri Lanka. BMC Public Health. 2017;17(Suppl 2):522. doi:10.1186/s12889-017-4342-4
20. Henshaw EJ. Breastfeeding and Postpartum Depression: a Review of Relationships and Potential Mechanisms. Curr Psychiatry Rep. 2023;25(12):803–808. doi:10.1007/s11920-023-01471-3
21. Bagci S, Wieduwilt A, Alsat EA, et al. Biodynamic lighting conditions preserve nocturnal melatonin production in pregnant women during hospitalization: a randomized prospective pilot study. Front Endocrinol. 2022;13:1043366. doi:10.3389/fendo.2022.1043366
22. Buniyaadi A, Prabhat A, Bhardwaj SK, Kumar V. Role of melatonin in physiological mitigation of sleep disruption in an unnatural temporal environment. J Neuroendocrinol. 2025;37(8):e70035. doi:10.1111/jne.70035
23. Arlinghaus KR, Laska MN. Parent Feeding Practices in the Context of Food Insecurity. Int J Environ Res Public Health. 2021;18(2):366. doi:10.3390/ijerph18020366
24. Al Maghaireh DF, Abdullah KL, Chong MC, Chua YP, Al Kawafha MM. Stress, Anxiety, Depression and Sleep Disturbance among Jordanian Mothers and Fathers of Infants Admitted to Neonatal Intensive Care Unit: a Preliminary Study. J Pediatr Nurs. 2017;36:132–140. doi:10.1016/j.pedn.2017.06.007
25. Schwarzkopf N, Rivas M, Peña F, et al. Maternal sleep during the first ten years of the child’s life. Sleep Med. 2026;138:108677. doi:10.1016/j.sleep.2025.108677
26. Wang C, Su K, Hu L, et al. The impact of short-term exposure to criteria air pollutants on sleep disturbance among young adults: a nationwide analysis in 261 Chinese cities. Environ Res. 2025;264:120316. doi:10.1016/j.envres.2024.120316
27. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
28. Toussaint A, Hüsing P, Gumz A, et al. Sensitivity to change and minimal clinically important difference of the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7). J Affect Disord. 2020;265:395–401. doi:10.1016/j.jad.2020.01.032
29. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
30. Zhang X, Cai Y, Zhu K, et al. Prevalence and risk factors of depression and anxiety among Chinese adults who received SARS-CoV-2 vaccine — a cross-sectional survey. J Affect Disord. 2023;324:53–60. doi:10.1016/j.jad.2022.12.077
31. Liang J, Zhao Y, Xi Y, et al. Association between Depression, Anxiety Symptoms and Gut Microbiota in Chinese Elderly with Functional Constipation. Nutrients. 2022;14(23):5013. doi:10.3390/nu14235013
32. Tan PY, Som SV, Nguyen SD, et al. The Role of Complementary Feeding Practices in Addressing the Double Burden of Malnutrition among Children Aged 6–23 Months: insight from the Vietnamese General Nutrition Survey 2020. Nutrients. 2024;16(19):3240. doi:10.3390/nu16193240
33. Emerson JA, Tol W, Caulfield LE, Doocy S. Maternal Psychological Distress and Perceived Impact on Child Feeding Practices in South Kivu, DR Congo. Food Nutr Bull. 2017;38(3):319–337. doi:10.1177/0379572117714385
34. Dennis CL, Falah-Hassani K, Shiri R. Prevalence of antenatal and postnatal anxiety: systematic review and meta-analysis. Br J Psychiatry. 2017;210(5):315–323. doi:10.1192/bjp.bp.116.187179
35. Yang Y, Li W, Ma TJ, et al. Prevalence of Poor Sleep Quality in Perinatal and Postnatal Women: a Comprehensive Meta-Analysis of Observational Studies. Front Psychiatry. 2020;11:161. doi:10.3389/fpsyt.2020.00161
36. Koutra K, Margetaki K, Kampouri M, et al. Maternal sleep disturbances during late pregnancy and child neuropsychological and behavioral development in early childhood. Eur Child Adolesc Psychiatry. 2023;32(11):2139–2150. doi:10.1007/s00787-022-02053-z
37. Juulia Paavonen E, Saarenpää-Heikkilä O, Pölkki P, Kylliäinen A, Porkka-Heiskanen T, Paunio T. Maternal and paternal sleep during pregnancy in the Child-sleep birth cohort. Sleep Med. 2017;29:47–56. doi:10.1016/j.sleep.2016.09.011
38. Mindell JA, Lee C, Sadeh A. Young child and maternal sleep in the Middle East. Sleep Med. 2017;32:75–82. doi:10.1016/j.sleep.2016.11.011
39. Ruiyi N. Investigation of 357 Cases of Infant Feeding and Feeding Skills[D]. Chongqing medical university; 2019.
40. Wu Q, Meng N, Wang X, et al. Complementary feeding practices for children aged 6–23 months in early childhood education institutions in urban China: a cross-sectional study. J Glob Health. 2024;14:04043. doi:10.7189/jogh.14.04043
41. Zhang J, Wu Q, Wang X, Zhang Y, Helena van Velthoven M. High response rate and low cost of WeChat-based data collection of infant and young child feeding data in rural Qinghai Province, China. J Glob Health. 2022;12:11011. doi:10.7189/jogh.12.11011
42. Leerkes EM, Bailes LG, Eagleton SG, Buehler C, Shriver LH, Wideman L. Maternal sleep problems, depression, and infant negative emotionality are associated with maternal feeding to soothe in early infancy. Appetite. 2022;176:106098. doi:10.1016/j.appet.2022.106098
43. Ou W, Lijuan W, Jian H, et al. Analysis of the influencing factors for anemia of infants and young children aged 6 to 23 months in Yingyanghao intervention areas. Chinese Journal of Child Health Care. 2019;27(11):1211–1215.
44. Baltagi BH, Yen YF. Welfare Reform and Children’s Health. Health Econ. 2016;25(3):277–291. doi:10.1002/hec.3139
45. Gao H, Wang Q, Hormann E, et al. Breastfeeding practices on postnatal wards in urban and rural areas of the Deyang region, Sichuan province of China. Int Breastfeed J. 2016;11(1):11. doi:10.1186/s13006-016-0070-0
46. Xingyu L. Analysis of Eating Behavior Problems and Dietary Nutritional Status of Children Aged 1-6 years in Chongqing[D]. Chongqing medical university; 2024; doi:10.27674/d.cnki.gcyku.2024.000778
47. Hernandez E, Lavner JA, Moore AM, et al. Sleep SAAF responsive parenting intervention improves mothers’ feeding practices: a randomized controlled trial among African American mother-infant dyads. Int J Behav Nutr Phys Act. 2022;19(1):129. doi:10.1186/s12966-022-01366-1
48. Mothers are not fathers: differences between parents in the reduction of stress levels after a parental intervention in a NICU – matricardi. Acta Paediatrica. 2013;2013:120258. doi:10.1111/apa.12058
49. Rouzafzoon M, Farnam F. Do behavioral mother-infant sleep interventions in the first six months affect maternal sleep, anxiety, and fatigue? A randomized controlled trial. Sleep Med. 2025;134:106675. doi:10.1016/j.sleep.2025.106675
50. Guyol GG, Kerr SM, Colson E, et al. The Impact of Maternal Worry on Infant Care Practices. Acad Pediatr. 2022;22(6):935–941. doi:10.1016/j.acap.2022.02.001
51. Dessì A, Pianese G, Mureddu P, Fanos V, Bosco A. From Breastfeeding to Support in Mothers’ Feeding Choices: a Key Role in the Prevention of Postpartum Depression? Nutrients. 2024;16(14):2285. doi:10.3390/nu16142285
52. Vandenplas Y, Hauser B, Salvatore S. Functional Gastrointestinal Disorders in Infancy: impact on the Health of the Infant and Family. Pediatr Gastroenterol Hepatol Nutr. 2019;22(3):207–216. doi:10.5223/pghn.2019.22.3.207
53. Heine RG, AlRefaee F, Bachina P, et al. Lactose intolerance and gastrointestinal cow’s milk allergy in infants and children - common misconceptions revisited. World Allergy Organ J. 2017;10(1):41. doi:10.1186/s40413-017-0173-0
54. da SKSR, Serra-Negra JM, Prado IM, Abreu LG, Reis TVD, Auad SM. Sleep disturbances are associated with feeding practices and age in preterm infants. Sleep Med. 2023;111:2–8. doi:10.1016/j.sleep.2023.08.030
55. Christian LM, Carroll JE, Teti DM, Hall MH. Maternal Sleep in Pregnancy and Postpartum Part I: mental, Physical, and Interpersonal Consequences. Curr Psychiatry Rep. 2019;21(3):20. doi:10.1007/s11920-019-0999-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.