Back to Journals » Cancer Management and Research » Volume 11
Competing risk analysis of primary tracheal carcinoma based on SEER database
Authors Gao HX ![]() , He X, Du JF, Yang SH, Wang Y, Zhang JW, Zhao CN
, He X, Du JF, Yang SH, Wang Y, Zhang JW, Zhao CN
Received 8 October 2018
Accepted for publication 17 December 2018
Published 24 January 2019 Volume 2019:11 Pages 1059—1065
DOI https://doi.org/10.2147/CMAR.S190124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Beicheng Sun
HongXiang Gao,1 Xuan He,1 JianFei Du,1 SanHu Yang,2 Yang Wang,1 JunWei Zhang,1 ChenNian Zhao1
1Department of Oncology, Chang’An Hospital, Xi’an, Shaanxi, China; 2Department of Thoracic Surgery, Tangdu Hospital, Xi’an, Shaanxi, China
Purpose: To analyze the prognostic factors of primary tracheal carcinoma.
Patients and methods: All patients of primary tracheal carcinoma were extracted from the Surveillance, Epidemiology, and End Results database during 1973–2015. The potential prognostic factors were analyzed by using the competing risk analysis of R statistical software.
Results: A total of 485 eligible patients were enrolled. The univariate analysis indicated that age, sex, diagnostic confirmation, extension, lymph node, metastasis, multiple primary tumors, primary site surgery, and lymph node dissection were statistically significant for the patients’ death due to tracheal tumor. The multivariate analysis indicated that age (P=0.0000, CI: 1.0255–1.0630), lymph node (P=0.0000, CI: 1.6031–3.4890), metastasis (P=0.0100, CI: 1.1342–2.5790), multiple primary tumors (P=0.0000, CI: 0.0276–0.1090), and primary site surgery (P=0.0001, CI: 0.3565–0.7110) were independent prognostic factors affecting survival, and there were significant differences in the stratification of each prognostic factors.
Conclusion: Age, lymph node, metastasis, multiple primary tumors, and primary site surgery were independent prognostic factors of primary tracheal carcinoma.
Keywords: primary tracheal carcinoma, SEER, prognostic factor, competing risk analysis
Introduction
Primary tracheal carcinoma is a rare tumor, accounting for only 0.1%–0.4% of all newly diagnosed tumors, with an incidence of 2.6 new cases per 1,000,000 people per year.1 The common pathological types are squamous cell carcinoma and adenoid cystic carcinoma. Surgery and postoperative adjuvant therapy can significantly prolong the survival time.2 But until now, there is a lack of accurate prognostic factors to guide clinical practice, which leads to inadequate or excessive treatment.
In the previous studies, prognostic factors were analyzed by the Cox proportional hazards model, and the outcome events by this model were classified into two categories, namely death or censored observation. However, during follow-up, patients often died from other causes, such as cardiovascular disease, car accidents, and other unexpected events, which lead to the failure to observe the tumor’s final outcome. In the Cox proportional hazards model, such patients were treated as censored observation or classified as death cases; the death-specific hazard function does not have a direct interpretation in terms of survival probability, which led to the wrong evaluation of survival. Competing risk3,4 refers to a situation where an individual is exposed to two or more causes of failure, and its eventual failure can be attributed exactly to only one. In this case, the occurrence of one type of event hinders the occurrence of any other event. In this study, failure events commonly studied are death due to tracheal tumor (DTT) and death due to other causes (DOC); the competing risk model of R statistical software was used to analyze the survival of patients with primary tracheal carcinoma, in order to obtain the accurate prognostic factors of death caused by tracheal tumor.
Patients and methods
Data source and selection
The data for this analysis were obtained from the Surveillance, Epidemiology, and End Results (SEER) database, a publicly available cancer registry maintained by the National Cancer Institute. The database we used was the Incidence – SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases, Nov 2017 Sub (1973–2015 varying). The end date of follow-up for this version of database was the end of 2015. According to ICD-0-3, there were 1,392 cases of tracheal tumor. Since no data related to tumor invasion were recorded before 2004, cases after 2004 were selected. The pathologically confirmed patients with malignant tracheal tumors were selected, and the secondary tumors and tumors of the lymphatic blood system were excluded. Finally, 485 cases were selected, as shown in Figure 1.
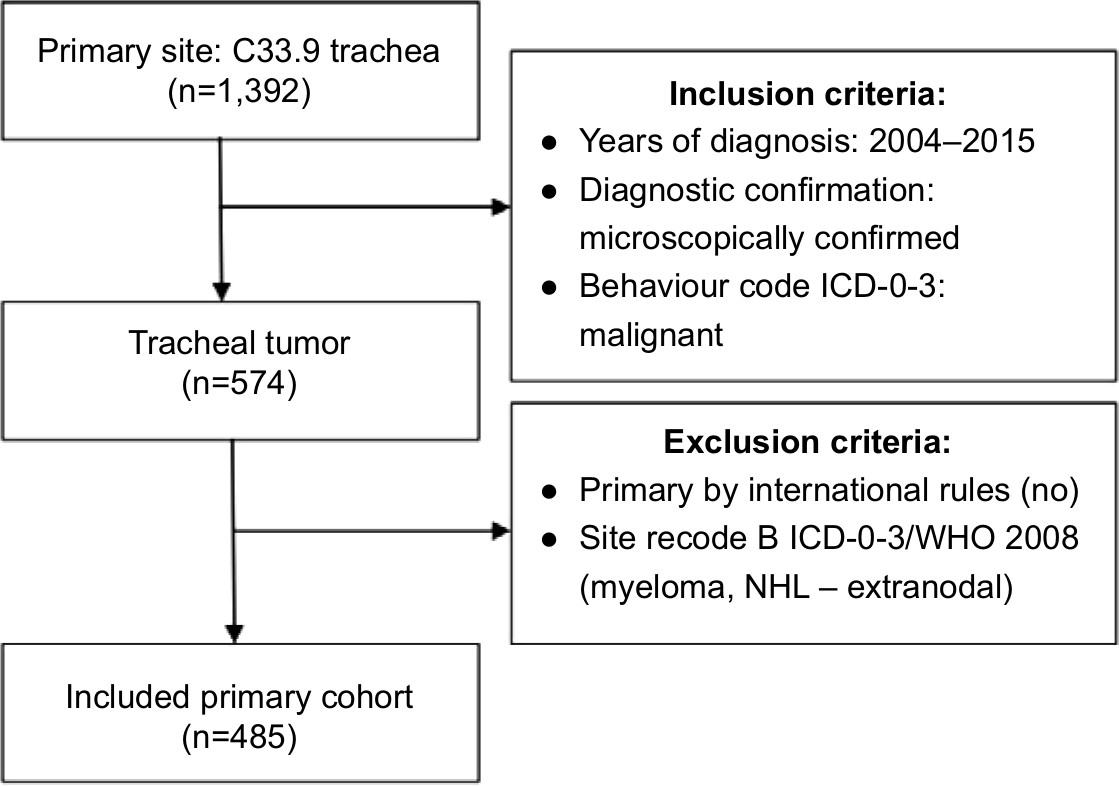 | Figure 1 Patient enrollment and exclusion process of in the SEER database. Abbreviation: SEER, Surveillance, Epidemiology, and End Results. |
Variables and outcomes
Twelve variables were selected from SEER database, including race, age, sex, diagnostic confirmation, histological type, pathology grade, extension, lymph node, metastasis, multiple primary tumors, primary site surgery, and lymph node dissection. Extension stratified two classes: localized refers to cases recorded in the SEER database as “Confined to trachea and Localized” and regional extension refers to “Adjacent connective tissue, Adjacent organs/structures, Further contiguous extension”. Multiple primary tumors were defined as cases in SEER database where “sequence number” was not recorded as “one primary tumor only”. Except age, which was a continuous variable, other variables were classified variables.
According to the “SEER cause-specific death classification” recorded in the database, the causes of death are divided into the following three situations: DTT, death due to other tumors (DOT), and DOC. In this study, a total of 294 patients died by the end of follow-up, and 159 patients died from DTT, accounting for 54% of the deaths and 33% of the total patients. One hundred patients died from DOT, accounting for 34% of deaths. Deaths due to other causes, such as heart disease and car accidents, accounted for 12% of all deaths.
Patients
The median age of the total patients was 64 years, ranging from 0 to 93 years. Only one case was younger than 1 year. The median age of patients who died from DTT was 67 years, ranging from 16 to 93 years. The distribution of sex was similar in the total patients and DTT group, with 292/193 and 105/54 in male and female, respectively. For the histological type, squamous cell carcinoma and adenoid cystic carcinoma account for 69% of total patients, of which squamous cell carcinoma accounts for 49%. For the diagnostic confirmation, positive histology accounts for 94.43% and 91.82% of the total patients and DTT group, respectively. The proportion of patients with multiple primary tumors was 5.66% in the DTT group and 39.38% in the total patients. In addition, about half of the 485 patients (237 patients, 48.87%) were treated with surgery, while less than one-third of the patients who died due to tracheal tumor were treated with surgery, as shown in Table 1.
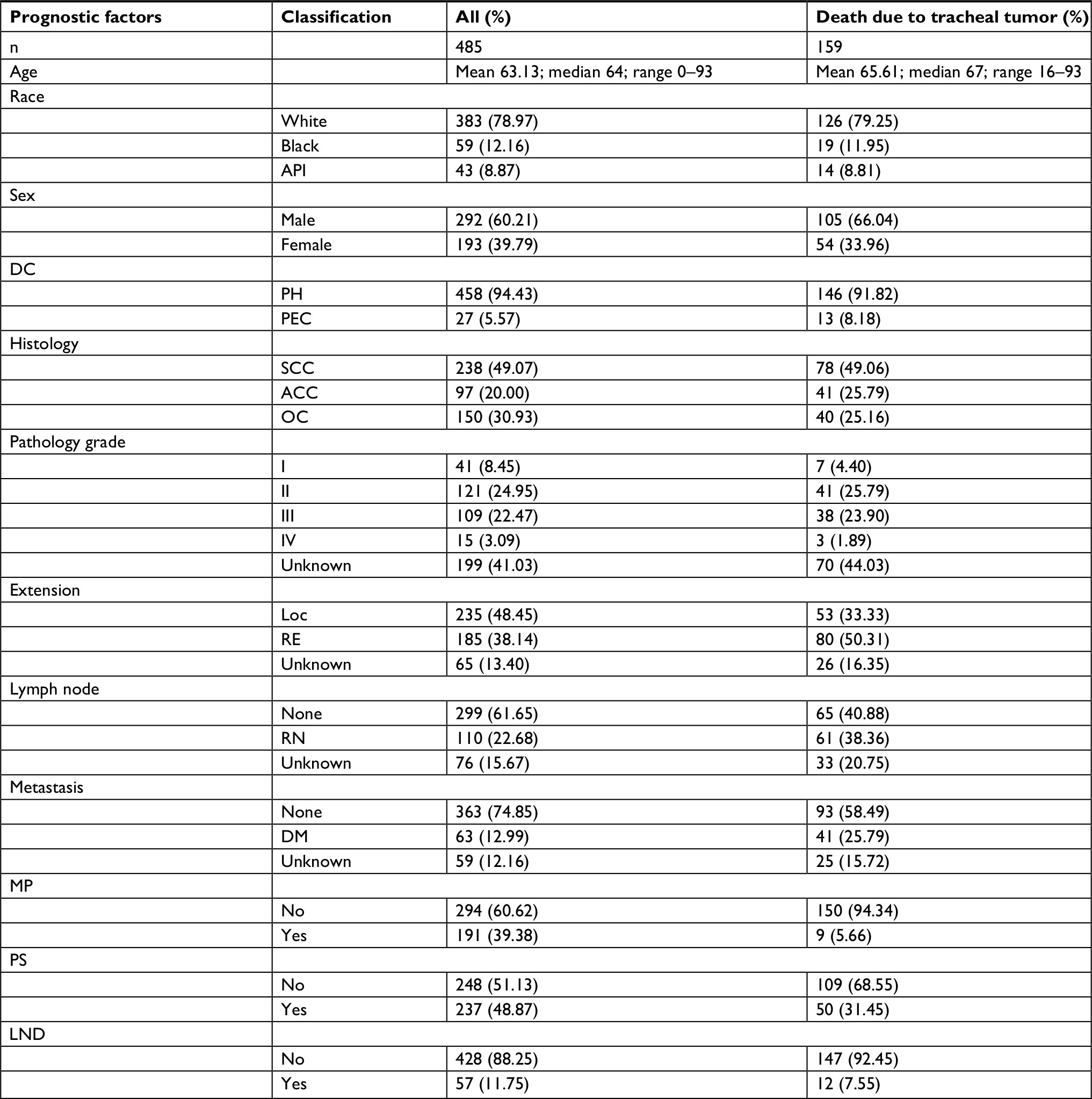 | Table 1 Characteristics and demographics of patients with primary tracheal carcinoma Abbreviations: ACC, adenoid cystic carcinoma; API, Asian or Pacific Islander; DC, diagnostic confirmation; DM, distant metastasis; LND, lymph node dissection; Loc, localized; MP, multiple primary tumors; OC, other carcinoma; PEC, positive exfoliative cytology, no positive histology; PH, positive histology; PS, primary site surgery; RE, regional extension; RN, regional lymph node; SCC, squamous carcinoma. |
Statistical method
The analysis was performed using the Cmprsk package for the R statistical software (version 3.5.1). The CumIncidence function was used for univariate analysis to analyze each potential prognostic factor, and the value of Gray’s test and the cumulative incidence rate at each time point were obtained. The Crr function was used for multivariate analysis, and independent prognostic factors were obtained. P<0.05 was considered statistically significant, and all tests were bilateral.
Results
A total of 485 eligible patients were enrolled. Twelve potential prognostic factors were univariate analyzed by Gray’s test, and the results showed that age, sex, diagnostic confirmation, extension, lymph node, metastasis, multiple primary tumors, primary site surgery, and lymph node dissection were statistically significant in the patients of DTT. Meanwhile, the cumulative incidence rate of 1, 2, and 5 years was calculated, as shown in Table 2.
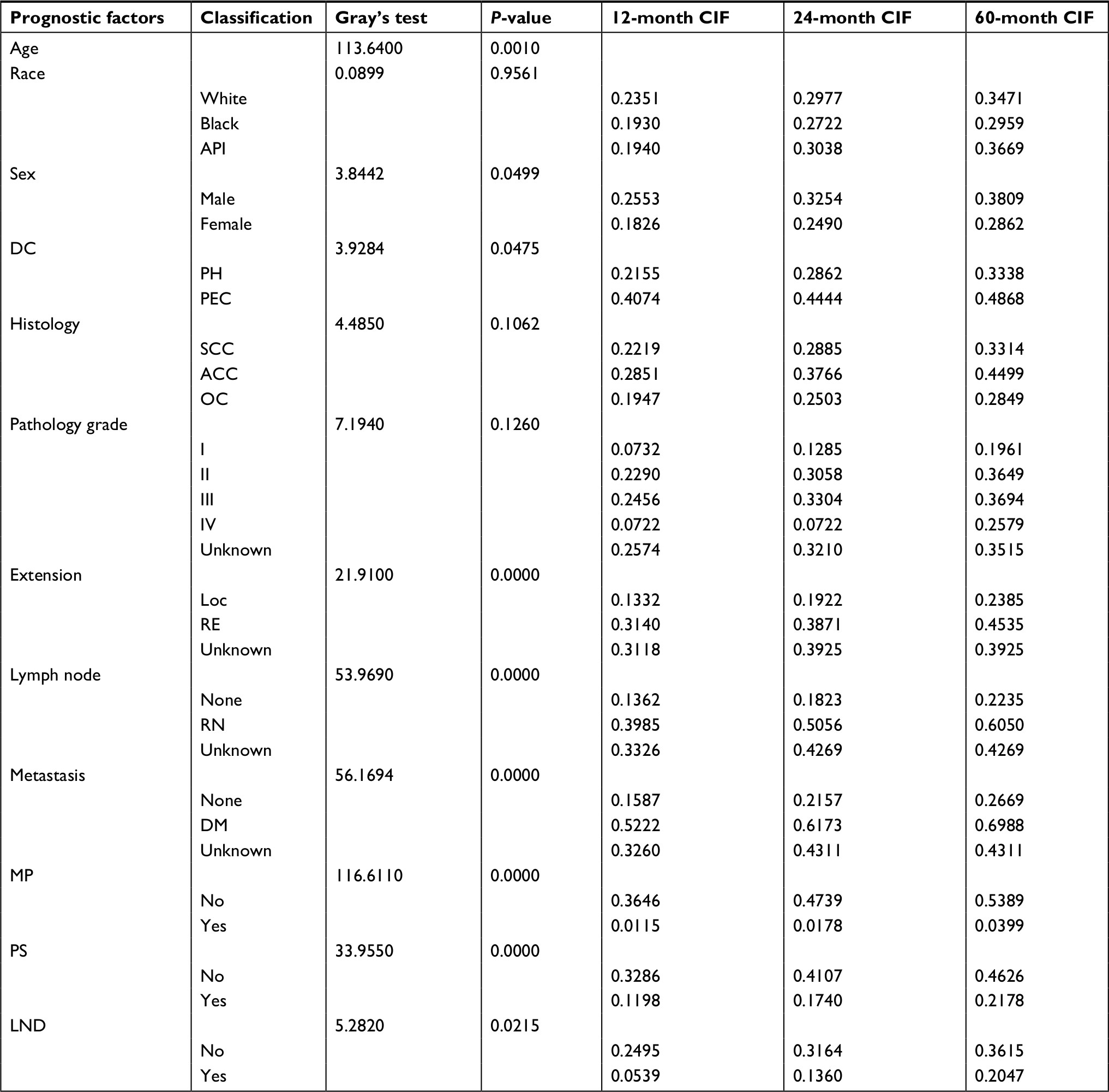 | Table 2 Univariate analysis of prognostic factors in patients with primary tracheal carcinoma Abbreviations: ACC, adenoid cystic carcinoma; API, Asian or Pacific Islander; CIF, cumulative incidence function; DC, diagnostic confirmation; DM, distant metastasis; LND, lymph node dissection; Loc, localized; MP, multiple primary tumors; OC, other carcinoma; PEC, positive exfoliative cytology, no positive histology; PH, positive histology; PS, primary site surgery; RE, regional extension; RN, regional lymph node; SCC, squamous carcinoma. |
The multivariate analysis indicated that age (P=0.0000, CI: 1.0255–1.0630), lymph node (P=0.0000, CI: 1.6031–3.4890), metastasis (P=0.0100, CI: 1.1342–2.5790), multiple primary tumors (P=0.0000, CI: 0.0276–0.1090), and primary site surgery (P=0.0001, CI: 0.3565–0.7110) were independent prognostic factors affecting survival, as shown in Figure 2. Moreover, significant differences were found in the stratification of each prognostic factors, and the statistical results were multiple primary tumors (χ2=69.2, P=0.0000), primary site surgery (χ2=15.2, P=0.0001), node (χ2=19.1, P=0.0001), and metastasis (χ2=6.6, P=0.037), respectively, as shown in Table 3. The risk probability of age changes with time, so age was analyzed in the competing risk model as time-varying covariates in this study. The results show that neither the linear (RR =0.9987, P=0.056) nor the quadratic (RR =1.00, P=0.14) term expressing the interaction of time with age is statistically significant. Results suggest that for each 1 year increase in age, the relative risk probability increases by 1.044 times (RR =1.044). The relative risk probability of multiple primary tumors was 20 times that of single primary tumor (RR =0.0548). The relative risk probability after surgical resection of the primary lesion was half that of the patients without surgery (RR =0.5033). For cases with regional lymph node metastasis, the relative risk increased more than twice (RR =2.3650). For cases with distant metastasis, the relative risk increased by 1.7 times (RR =1.7104).
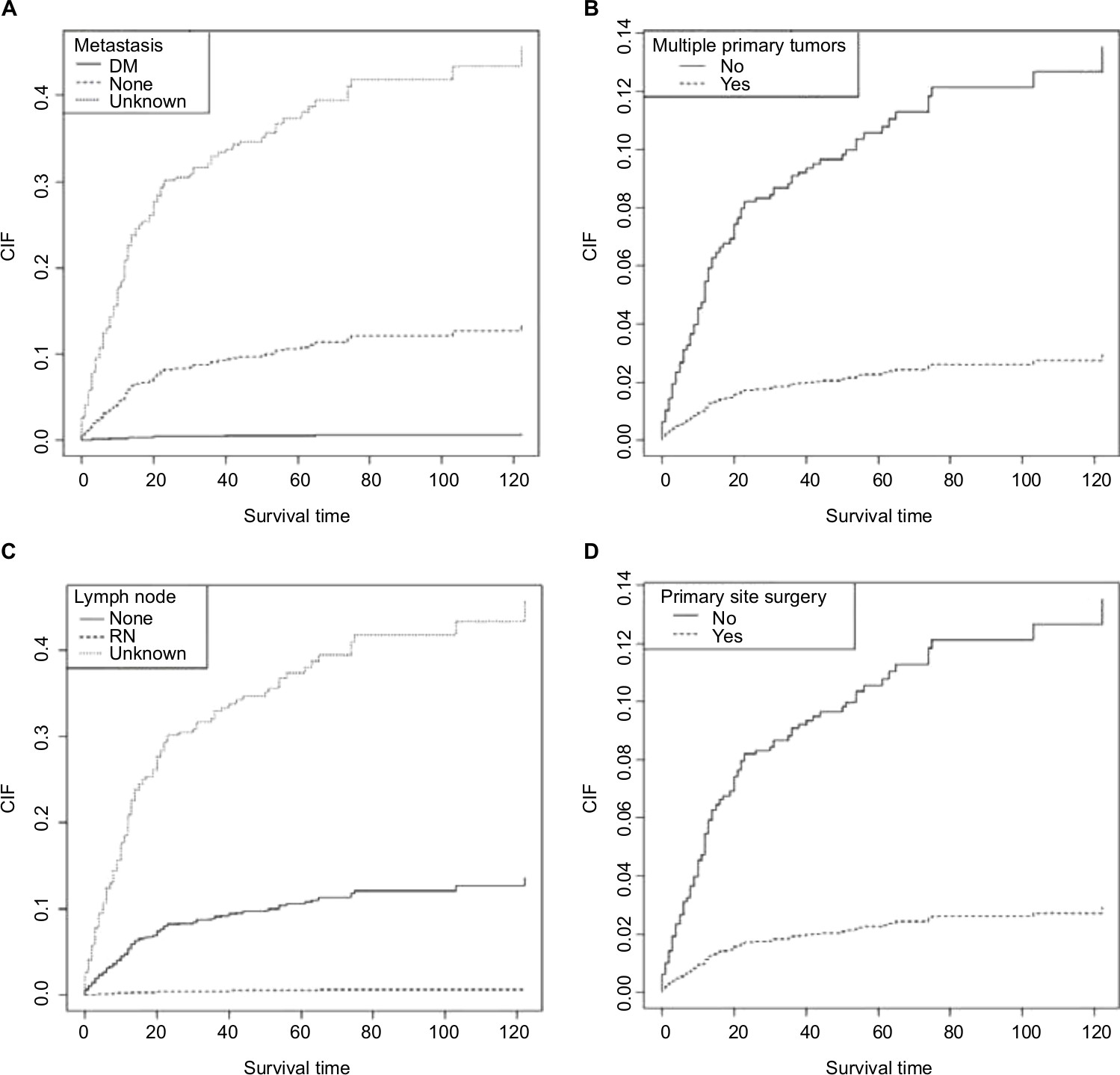 | Figure 2 Multivariate analysis for prognostic factors. Note: (A) Metastasis; (B) multiple primary tumors; (C) lymph node; and (D) primary site surgery. Abbreviations: CIF, cumulative incidence function; DM, distant metastasis; RN, regional lymph node. |
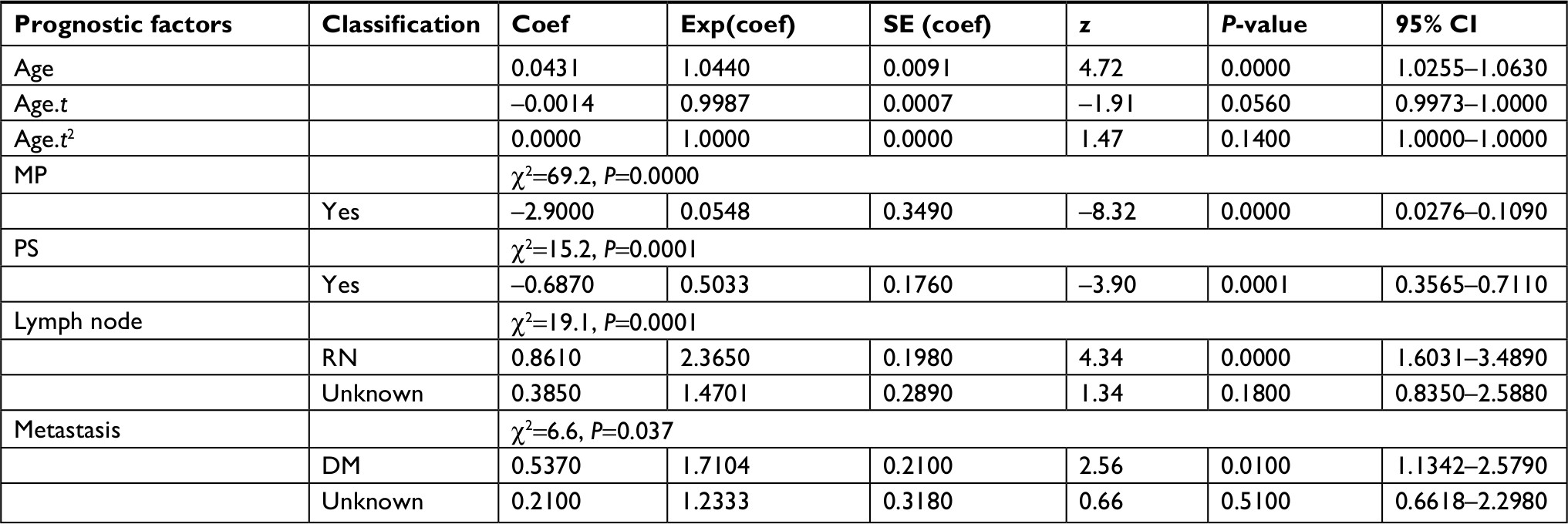 | Table 3 Multivariate analysis of prognostic factors in patients with primary tracheal carcinoma Abbreviations: DM, distant metastasis; MP, multiple primary tumors; PS, primary site surgery; RN, regional lymph node. |
Discussion
Primary tracheal carcinoma was infrequent in clinic, and the current understanding was derived from pooled population-based datasets or single institution series involving a variety of treatment regimens. The analysis of prognostic factors is disordered due to case selection bias and improper use of statistical methods. So far, no widely accepted clinical standard has been established to guide clinical practice. In our study, 294 patients died in the follow-up, but only 159 were related to tracheal tumors. That means that the proportion of patients with an interesting outcome in survival analysis was only one-third of the total patients. If the commonly used survival analysis method was adopted, two-thirds of the cases will be treated as censored data, resulting in excessive statistical error. And even worse, all 294 deaths will be attributed to the death of tracheal tumor, resulting in a wrong conclusion. These problems were solved by the competing risk model very well. For this reason, this study aimed to obtain accurate prognostic factors through appropriate case selection and appropriate application of statistical methods.
Age as a prognostic factor changed with time and caused variations in other prognostic factors. For example, squamous cell carcinoma was associated with smoking. With the increases of smoking time, the probability of occurrence increases, generally in 60 years of high incidence. Therefore, in this study, age was used as time-varying covariates for multivariate analysis, and the results showed that age was an independent prognostic factor affecting survival and did not change with time.
Whether regional lymph node metastasis affects survival has always been controversial. In two large studies setting staging criteria,5,6 regional lymph node metastasis was confirmed to be an important prognostic factor for survival. However, in another multicenter retrospective study,7 it was found that regional lymph node involvement did not seem to have a significant adverse effect on prognosis. In the univariate and multivariate analysis in this study, regional lymph node involvement showed strong statistical significance, with a difference of 2.36 times in survival, which was the most valuable predictive factor among all prognostic factors.
Distant metastasis of tracheal carcinoma was inferior to local lesions in survival time, and its predictive efficacy had been confirmed by database-based analysis.8 Distant metastasis includes distant organ metastasis and distant lymph node metastasis. In another database-based prognostic analysis study,9 distant metastasis was not taken as a prognostic factor alone, but as two prognostic factors – distant organ metastasis and distant lymph node metastasis, respectively. The results still suggest that both of them were independent prognostic factors. In this study, the “Trachea Mets at DX/Distant lymph node except or plus Distant metastasis” recorded in SEER database was taken as the prognostic factor of distant metastasis; the results showed that it was an independent prognostic factor, similar to the results of He’s.9 However, in the study of He, there were eleven patients of distant organ metastasis, accounting for only 4% of the total study patients, and six patients of distant lymph node metastasis, accounting for only 2% of the total. As a potential prognostic factor, too little sample size would lead to bias of the analysis results. In this paper, distant metastasis accounted for 13% of the total study patients and 26% of deaths due to tracheal tumor, so the analysis results were more accurate.
Surgery, as the main treatment measure for tracheal tumor, has been increasingly applied in recent years, bringing about the improvement of survival.10,11 The goal of surgery was to achieve R0 in total tumor resection, but there were also studies12 indicating that it did not affect survival. Agrawal10 conducted survival analysis for patients with tracheal tumor in SEER database from 1973 to 2011; the result indicated that those who did not have surgery were 2.50 times more likely to die of tracheal carcinoma than those who did have surgery. The results of this study also confirmed that for patients who died from tracheal tumor, surgery could increase survival time by nearly twice. However, whether lymph node dissection was necessary, this study suggested that only univariate analysis shows statistical differences, while multivariate analysis did not indicate that it could affect survival, which was consistent with the Gaissert12 and Regnard7 studies.
Multiple primary malignant tumors refer to two or more primary malignant tumors occurring simultaneously or successively in one or more organs of the same host. This was documented in detail in the SEER database. The statistical analysis of this study found that among the 485 patients studied, there were 191 patients with multiple primary tumors, 155 cases with two primary tumors, 26 cases with three primary tumors, 7 cases with four primary tumors, 3 cases with five primary tumors, and 154 cases with more than two malignant primary tumors. According to the statistical analysis of the causes of death, 117 patients with multiple primary tumors died at the end of follow-up, among which 9 patients died of tracheal tumor, accounting for 6% of the total number of deaths due to tracheal tumor. One hundred patients died from other tumors, accounting for 100% of the total deaths from other tumors. Eight patients died from other causes, accounting for 23% of all deaths from other causes. Few studies on multiple primary tumors, especially in the survival analysis of tracheal tumors, had not mentioned this prognostic factor. In this study, it was found that the mortality risk of patients with multiple primary tumors was two times higher than that of patients with single tumors, which was a strong independent prognostic factor.
In this study, a competing risk model was used to analyze the prognostic factors of specific outcome events, and the factors affecting the prognosis of primary tracheal carcinoma could be obtained more accurately. The inadequacy was that the survival time could not be predicted and could not be compared with previous literature. On the other hand, with the wide application of comprehensive treatment of tumor, postoperative adjuvant radiotherapy had been proved to improve survival,13 while SEER database did not have detailed records of other treatment measures such as radiotherapy, resulting in the incomplete selection of potential prognostic factors, leading to decreased reliability of the conclusion.
Conclusion
This study indicated that age, lymph node, metastasis, multiple primary tumors, and primary site surgery were independent prognostic factors of primary tracheal carcinoma. This study only analyzed the prognostic factors, but did not establish a clinical and practical prognostic model, which needs to be established in future research.
Disclosure
The authors report no conflicts of interest in this work.
References
Honings J, van Dijck JA, Verhagen AF, van der Heijden HF, Marres HA. Incidence and treatment of tracheal cancer: a nationwide study in the Netherlands. Ann Surg Oncol. 2007;14(2):968–976. | ||
Behringer D, Könemann S, Hecker E. Treatment approaches to primary tracheal cancer. Thorac Surg Clin. 2014;24(1):73–76. | ||
Scrucca L, Santucci A, Aversa F. Competing risk analysis using R: an easy guide for clinicians. Bone Marrow Transpl. 2007;40(4):381–387. | ||
Scrucca L, Santucci A, Aversa F. Regression modeling of competing risk using R: an in depth guide for clinicians. Bone Marrow Transpl. 2010;45(9):1388–1395. | ||
Bhattacharyya N. Contemporary staging and prognosis for primary tracheal malignancies: a population-based analysis. Otolaryngol Head Neck Surg. 2004;131(5):639–642. | ||
Webb BD, Walsh GL, Roberts DB, Sturgis EM. Primary tracheal malignant neoplasms: the University of Texas MD Anderson Cancer Center experience. J Am Coll Surg. 2006;202(2):237–246. | ||
Regnard JF, Fourquier P, Levasseur P. Results and prognostic factors in resections of primary tracheal tumors: a multicenter retrospective study. The French Society of Cardiovascular Surgery. J Thorac Cardiovasc Surg. 1996;111(4):808–813. | ||
Urdaneta AI, Yu JB, Wilson LD. Population based cancer registry analysis of primary tracheal carcinoma. Am J Clin Oncol. 2011;34(1):32–37. | ||
He J, Shen J, Huang J, et al. Prognosis of primary tracheal tumor: a population-based analysis. J Surg Oncol. 2017;115(8):1004–1010. | ||
Agrawal S, Jackson C, Celie KB, et al. Survival trends in patients with tracheal carcinoma from 1973 to 2011. Am J Otolaryngol. 2017;38(6):673–677. | ||
Nouraei SM, Middleton SE, Nouraei SA, et al. Management and prognosis of primary tracheal cancer: a national analysis. Laryngoscope. 2014;124(1):145–150. | ||
Gaissert HA, Grillo HC, Shadmehr MB, et al. Long-term survival after resection of primary adenoid cystic and squamous cell carcinoma of the trachea and carina. Ann Thorac Surg. 2004;78(6):1889–1897. | ||
Napieralska A, Miszczyk L, Blamek S. Tracheal cancer – treatment results, prognostic factors and incidence of other neoplasms. Radiol Oncol. 2016;50(4):409–417. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.