Back to Journals » Clinical Ophthalmology » Volume 17
Compensatory Corneal Epithelial Changes After Femtolaser - Assisted Intracorneal Rings Implantation in Early and Moderate Cases of Keratoconus
Authors Shaaban YM, Badran TA
Received 26 July 2023
Accepted for publication 7 November 2023
Published 22 November 2023 Volume 2023:17 Pages 3591—3599
DOI https://doi.org/10.2147/OPTH.S432446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yasmine Maher Shaaban,1,2,* Tamer Abdelfattah Badran1,3,*
1Department of Ophthalmology, Faculty of Medicine, Ain Shams University, Cairo, 1181, Egypt; 2Ain Shams University Hospitals and Ain Shams Specialized Hospital, Cairo, 11588, Egypt; 3The Eye Subspeciality Center (ESC), Cairo, 11402, Egypt
*These authors contributed equally to this work
Correspondence: Yasmine Maher Shaaban, Department of Ophthalmology, Faculty of Medicine, Ain Shams University, Cairo, 1181, Egypt, Tel +20 1227123242, Fax +20224346753 ; +20224346041, Email [email protected]
Purpose: To study the compensatory corneal epithelial changes after femtolaser-assisted intracorneal ring segment (ICRS) implantation in early and moderate cases of keratoconus (KC) using anterior segment optical coherence tomography (AS-OCT).
Patients and Methods: A prospective observational non-randomized study of 40 eyes with mild to moderate KC received femtolaser-assisted ICRS implantation. Ferrara ICRS with different arc lengths and thicknesses were used according to the patients’ tomographic pattern. Patients had a clear central cornea, keratometry reading < 60 diopters, and corneal thickness > 400 microns. AS-OCT was performed preoperatively and at 1, 3, and 6 months after surgery. Corneal epithelial thickness (CET) was measured over 17 points (2 mm central and 16 points on 2– 5 mm and 5– 7 mm annular zones) over the pupil center. All data were collected and analyzed.
Results: Comparing the preoperative and postoperative data, there was a statistically significant increase in the CET postoperatively throughout the 6-month follow-up period in all zones (p< 0.001). The epithelial thickness (ET) was noticed shortly around and central to the ring ridges by the first month (5– 7 mm zone). By the third month, the flattened central cornea (2 mm zone) and the 2– 5 mm zone showed a significant increase in ET up to the 6th month.
Conclusion: ICRS implantation in KC results in a thicker and more regular epithelium in the central corneal zone as a secondary response to the corneal stromal changes induced by the implants.
Keywords: keratoconus, Ferrara rings, epithelial thickness, AS-OCT
Introduction
Keratoconus (KC) is a progressive corneal disease characterized by thinning and steepening of the cornea, high myopia, irregular astigmatism, and decreased visual acuity.1 Treatment of KC includes rigid gas-permeable contact lenses, ICRS implantation, corneal surface ablation combined with corneal crosslinking (CXL), phakic toric intraocular lens implantation, and lamellar or penetrating keratoplasty.2–5 Corneal Allogenic Intrastromal Ring Segments (CAIRS), of a donor cornea were also used in patients with keratoconus.6
The ICRS was first introduced by Blevatskaya in 1966 to treat myopia and later used by Colin3 in 2000 to treat KC.
ICRS changes the corneal curvature, enhancing its refractive properties and improving vision. It has been proved that ICRS implantation decreases the keratometry readings, spherical equivalent, and cylinder, reduces high-order aberrations, and improves both the uncorrected and corrected visual acuity.7
ICRS works by flattening and reshaping the steep part of the keratoconic corneas. Ring segment implantation in the cornea’s periphery causes local separation of the corneal lamellae and shortens the corneal arc length. This flattening effect on the cornea reduces myopia by lowering its optical power. Another theory states that flattening of the cornea occurs when tissue is added to the corneal periphery or tissue is removed from the center of the cornea (thickness law).8 It has been proved that the flattening observed after ICRS implantation is directly proportional to the thickness of the implanted segment and inversely proportional to the corneal diameter of the implantation site, meaning that the thicker and the smaller the ICRS diameter, the higher the corneal flattening effect.9 Commercially available types of ICRS with variable thicknesses, geometries, and diameters for corneal stabilizing effect and restoring visual acuity in patients with KC are commercially available.10
Nomograms are clinical guidelines offered by ICRS companies to determine the important parameters for the procedures. Based on the pentacam corneal tomography, the patient data are entered into the online nomogram. The nomograms are based on patients’ data, not on mathematical calculations.
Materials and Methods
This study was carried out in Ain Shams University Hospitals and the Eye Subspeciality Center, Cairo, Egypt. The study is adherent to the Declaration of Helsinki involving human subjects and had approval from the Ain Shams University Faculty of Medicine Research Ethical Committee Review Board (FWA 000017585). Written informed consent was obtained from all patients.
The inclusive criteria included age > 18 years, early to moderate KC (Amsler Krumeich classification), contact lens intolerance, impaired vision with spectacle correction, average keratometry reading < 60 diopters, corneal pachymetry > 400 microns in the site of the corneal tunnel, and absence of significant central corneal scarring. One eye from each patient was included in the study.
The exclusion criteria included acute hydrops, progressive or advanced KC, keratitis, history of herpetic disease, corneal dystrophy, previous CXL, glaucoma, retinopathy, retinal detachment or degeneration, neuro-ophthalmic disease, systemic connective tissue or autoimmune diseases, severe dry eye, and pregnant women.
Medical and family histories were taken from all patients. Contact lens discontinuation 2 weeks before the examination was necessary for appropriate corneal measurements. Auto refractometer and C Landolt chart measuring the uncorrected and corrected distance visual acuity were done. A slit lamp examination was performed for the anterior segment, cornea, Fleischer ring, Vogts stria, and cornea lid relationship (Munson sign). Fundus examination was done through a dilated pupil using slit lamp bio-microscopy and indirect ophthalmoscope. Pentacam, Scheimpflug imaging (Oculus Optikgerate GmbH, Wetzlar, Germany) was used to detect early KC.
Anterior segment optical coherence tomography (AS-OCT, Zeiss Cirrus HD 5000; Carl Zeiss Meditec, Germany) was used to measure the corneal epithelium thickness (CET) preoperatively and postoperatively for all patients. The Ferrara ICRS (AJL Ophthalmic, Álava, Spain) with different arc lengths and thicknesses was used in the procedure.
The surgical procedure was performed in the operating room under complete aseptic conditions using topical anesthesia benoxinate hydrochloride 0.4% eye drops (Benox®, Epico, Inc., Cairo, Egypt).
ICRS was inserted into a previously performed corneal tunnel of deep corneal stroma using the 500-kHz VisuMax femtosecond laser (VisuMax®, Carl Zeiss Meditec AG, Jena, Germany). The data provided by the nomogram included the number of segment rings, their arc length, thickness, and the location of insertion. Single 160° ICRS, double 160° ICRS, 210° ICRS, and 320° ICRS were used. The femtosecond laser creates tunnels and incisions at a frequency of 500 kHz, and a wavelength of 1043 nm. The tunnel depth was selected to be 80% of the corneal thickness. The auto-centration and fixation using the contact glass and the suction pressure were done through the docking procedure. The tunnel numbers depended on the number of segments to be inserted. The patient was automatically released from the laser system contact glass when the incisions and tunnels were completed. The patency of the incisions and tunnels was tested before ring implantation. The ICRS was placed with special forceps through the dialing holes at the ends of the segments until it was completely buried within the tunnel. Postoperative treatment included topical antibiotics (moxifloxacin eye drops 0.5%, Alcon, Novartis, Geneva, Switzerland) and topical corticosteroids (prednisolone acetate eye drops 1%, Allergan, Irvine, California, USA). Eye drops were instilled three times daily for 2 weeks and tapered over the following 2 weeks. All patients were seen on day one and followed up after one week, one month, three months, and six months postoperatively. The AS-OCT was done postoperatively at one, three, and six months for each patient to measure the CET over the central 2 mm zone and the 16 points on 2–5 mm and 5–7mm annular zones. All data were collected and analyzed.
Statistical Analysis
Statistical Package for Social Sciences (SPSS) version 25 (IBM Corporation, Chicago, IL, USA) was used for the statistical analysis. Mean and standard deviations were used to present quantitative data for the analysis of the study. The two-way repeated measure ANOVA with time points (4 levels) and zone points (8 levels) was used to analyze the corneal epithelial thickness. If the interaction term between two factors proved to be statistically significant, the simple effects were tested using post-hoc Bonferroni correction to present and compare the outcome variable, ie, comparing the thickness in zone points across time points and comparing the thickness at each time point between zone points. In all tests, a p-value of ≤0.05 was considered statistically significant.
Results
This study included 40 eyes of 40 patients with a mean age of 24.5 ± 5.1 years, 22 females (55%), 18 males (45%), 20 right eyes (50%), and 20 left eyes (50%). No intraoperative or postoperative complications were encountered in this group of patients. Comparing the pre-and post-operative epithelial thickness (ET), there was a significant increase in CET in all three studied zones that occurred after ICRS implantation and continued throughout the 6 months follow-up period of the study. By the first postoperative month, there was a significant increase in thickness, especially in the areas close, around, and central to the ridge of the ring (the 5–7 mm zone). The mean preoperative CET at the 5–7 mm zone was 42.71 ± 2.23 μm. The mean postoperative CET at the 5–7 mm zone was 45.38 ± 2.17, 47.09 ± 1.85, and 47.72 ± 1.1.76 μm at one, three, and 6 months, respectively (Table 1).
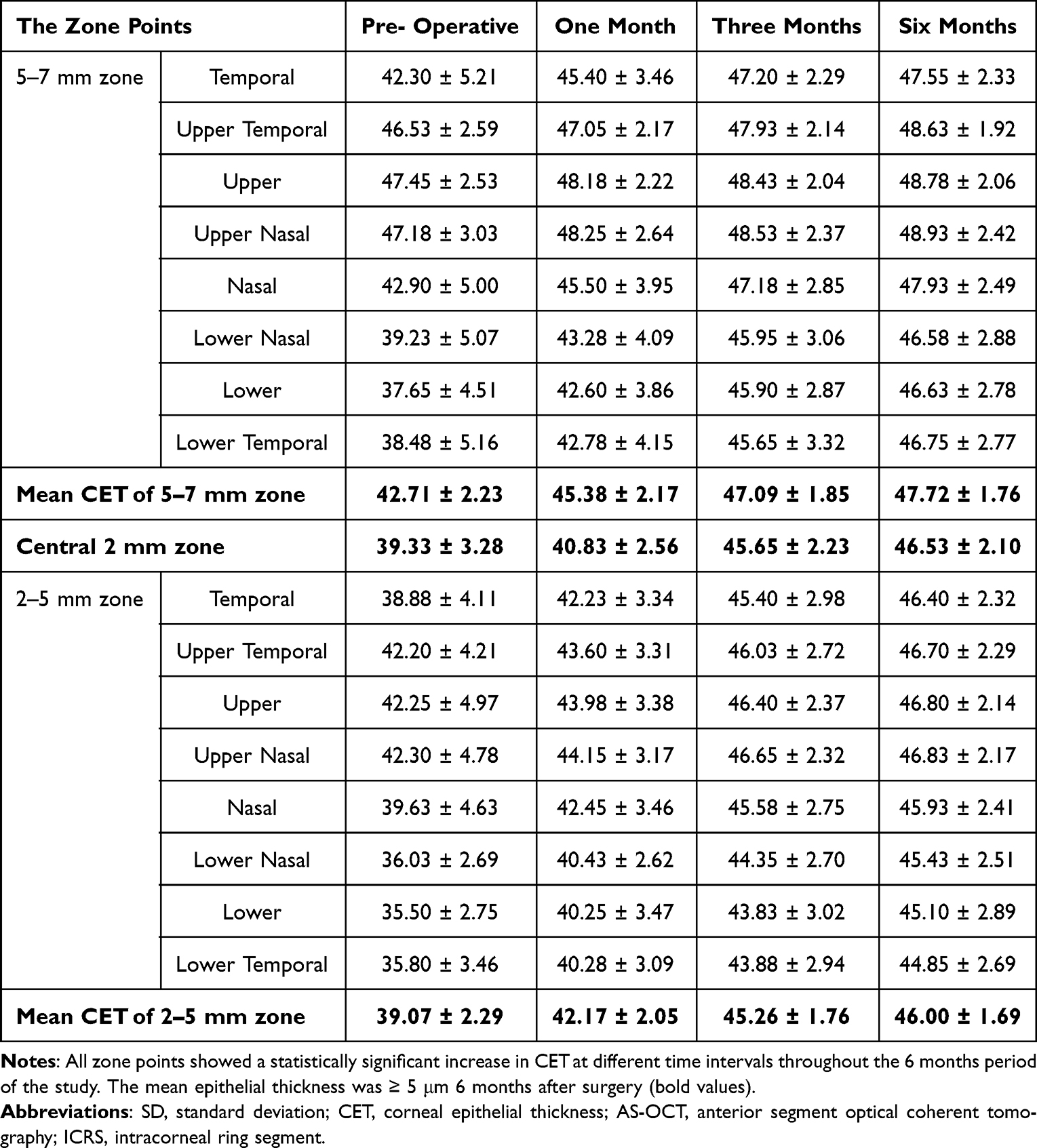 |
Table 1 Mean and SD of the CET (μm) Measured by as-OCT on 17 Points Over the Pupil Center at Different Time Intervals Through 6 Months After ICRS Implantation |
Thickness increased by the third month and tended to be stable by the 6th postoperative month. The CET at different points of the 5–7 mm zone at different time intervals is shown in (Figure 1).
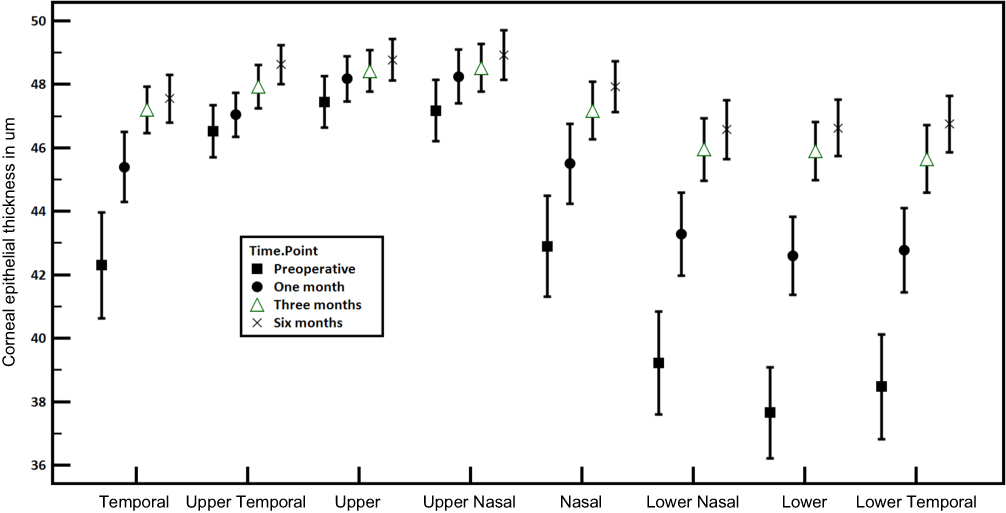 |
Figure 1 Mean and 95% confidence level of the corneal epithelial thickness in different points of the 5–7 mm zone at different points in time. Mauchly’s test for sphericity was statistically significant with p<0.001. Greenhouse-Geisser p values were statistically significant (<0.001) for the effects and the interaction between time points and zone points, comparing the thickness at zone points across the time points and comparing the thickness at each time point between the zone points. |
By the third postoperative month, the 2 mm central zone that was flattened by the mechanical effect of the ring showed a statistically significant increase in the CET at different time intervals, which continued to increase up to the 6th postoperative month. The mean preoperative CET at the 2 mm zone was 39.33 ± 3.28 μm. The mean postoperative CET at the 2 mm zone was 40.83 ± 2.56, 45.65 ± 2.23, and 46.53 ± 2.10 μm at one, three, and 6 months, respectively (Table 1).
The mean (ET) in the central 2 mm zone showed a statistically significant increase at different points in time throughout the study (Figure 2).
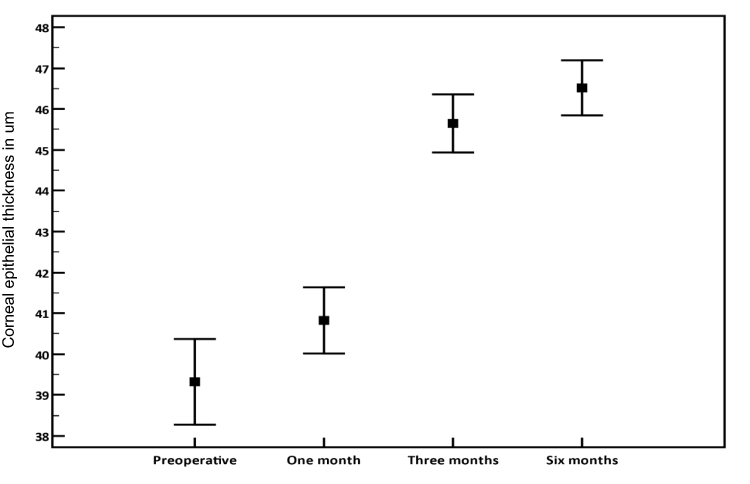 |
Figure 2 Mean and 95% confidence level of the central 2 mm zone of the cornea at different points in time. All pairwise comparisons of the mean epithelial thickness at the center showed a statistically significant difference. |
At about the same time, in the third month, the 2–5 mm zone showed a significant increase in the CET up to the 6th postoperative month. The mean preoperative CET at the 2–5mm zone was 39.07 ± 2.29 μm. The mean postoperative CET at the 2–5 mm zone was 42.17 ± 2.05, 45.65 ± 1.76, and 46.00 ± 1.169 μm at one, three, and 6 months, respectively (Table 1). The increase in CET at different points of the 2–5 mm zone at different points in time is shown in (Figure 3).
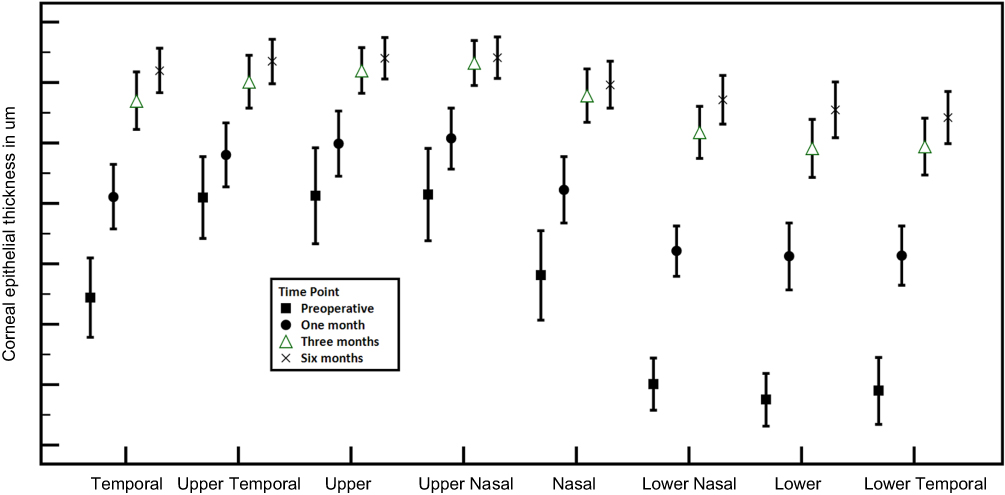 |
Figure 3 Mean and 95% confidence level of the corneal epithelial thickness in different points of the 2–5 mm zone at different points in time. Mauchly’s test for sphericity was statistically significant with p<0.001. Greenhouse-Geisser p values were statistically significant (<0.001) for the effects and the interaction between time points and zone points, comparing the thickness at zone points across the time points and comparing the thickness at each time point between the zone points. |
Figure 4 summarizes the pre-and post-operative CET in the three studied zones after ICRS implantation throughout the 6-month follow-up period.
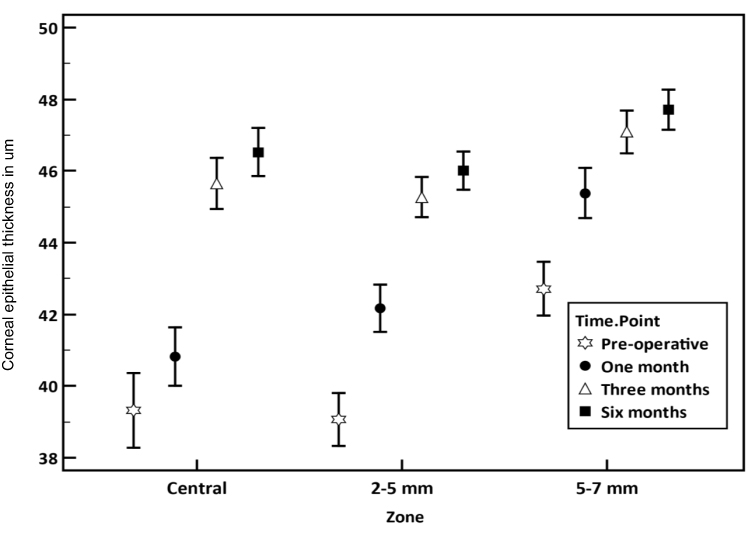 |
Figure 4 Mean and 95% confidence level of the corneal epithelial thickness in each zone at different points in time. |
The effect of time at different zone points in 2–5mm and 5–7 mm zones showed statistically significant increases throughout the 6-month study (p<0.001). However, some zone points did not show significant changes at certain time intervals at p ≥ 0.05 (Table 2)
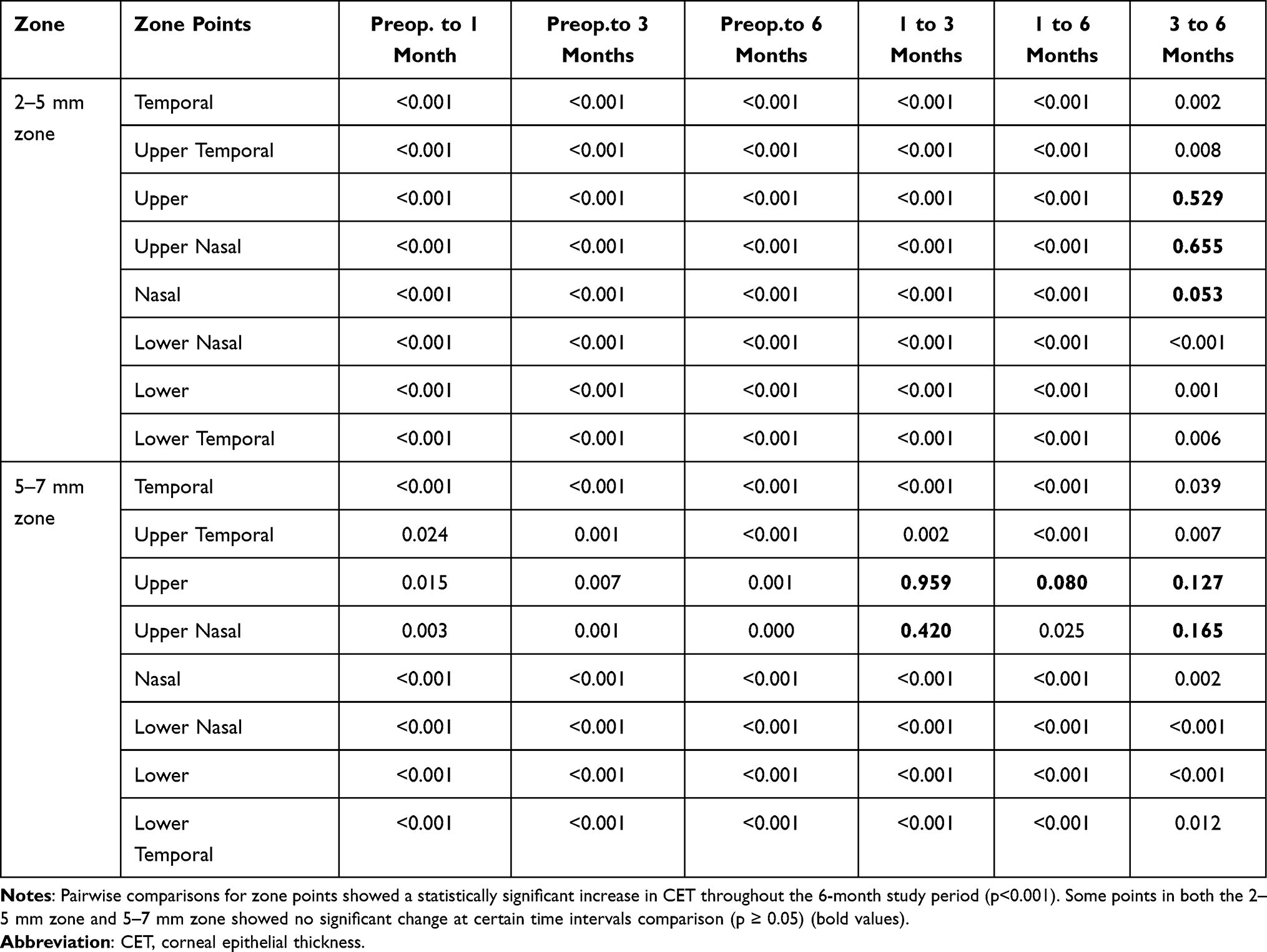 |
Table 2 Pairwise Comparisons for Zone Points 2–5mm and 5–7 Mm Throughout a 6-Month Study Showing the Effect of Time at Different Zone Points |
Comparing the differences in CET in each of the three studied zones at different time intervals throughout the study, there was a statistically significant difference at p <0.001(Table 3).
 |
Table 3 Mean and 95% CL of the Pairwise Differences in CET in Each Zone at Different Time Intervals |
Discussion
ICRS implantation can improve vision, and contact lens tolerance, and delay or prevent the need for keratoplasty.4,7 Femtosecond laser-assisted technique offers a high precision level, minimal direct manipulation, and efficiency with a low incidence of complications. AS-OCT has a valuable role in the early diagnosis of KC, and CET measurements, and in following up the ICRS procedures.11,12 Multiple studies13,14–19 have been done regarding AS-OCT, ICRS implantation, and KC. These studies concern the depth of the rings,13,17 position of the rings,15,16 corneal tomography,14 corneal curvature, corneal thickness,16 and corneal aberrations.18 A study done by Reinstein et al19 l described epithelial remodeling after Intacs ICRS implantation in five myopic patients using very high-frequency digital three-dimensional ultrasound scanning (VHF). Thickness maps of epithelium, stroma, and full cornea were done before and three months after Intacs insertion, and the induced thickness profile was studied. Epithelial compensation was noted with thickening adjacent to the ICRS. A similar compensatory epithelial response was encountered in this current study using the AS-OCT after ICRS implantation.
The literature is deficient in studying the CET in KC and ICRS implantation using AS-OCT and Femtolaser. A study was done by David et al,20 to assess epithelial corneal remodeling by AS-OCT in 68 keratoconic eyes implanted with Ferrara ICRS with different arc lengths, and thicknesses. In all cases, they reported significant epithelial changes that occurred a short time after ICRS implantation. A significantly increased ET was seen close to and around the ridge of the ring central to the ICRS. A maximum ET in the 6 mm zone of the central cornea was observed 6 months after surgery in all cases. This agrees with our study.
In the current study, all zones showed a statistically significant increase in the mean ET ≥ 5 μm 6 months after surgery. David et al20 reported a significant increase of ≥ 5 μm and a significant increase of < 5 μm in the 6 mm of CET with no changes in the thickness in some points in the 3–6 mm zone 6 months after surgery. We also encountered some points in the 2–5 mm and 5–7 mm zones, where there was no change in CET 6 months after surgery, a common finding in both studies.
David et al20 reported that the areas of epithelial thickening in response to ICRS differed according to the used ICRS arc. At 6 months after ICRS implantation, they reported a significant epithelial thickening at the apex of the cone in all patients but they reported no changes in the ET in the central 3.00 mm zone after surgery when using 2100 ICRS. In the current study, and contrary to this finding, it has been found that whatever the arc of ICRS used, there was a statistically significant increase in CET in the central 2.00-mm zone. This can be explained by the fact that since all types of ICRS have the same mechanical flattening effect on the center of the cornea, the compensatory epithelial effect and the subsequent increase in the CET in this zone would occur in all types of ICRS.
The significant increase in the thickness of the CET in the 2–5 mm zone in this study, could be a part of the compensatory epithelial response to the stromal rearrangement after ICRS implantation.
With the deficiency of such topics in the literature and with similarities and discrepancies in the few available studies, further investigations, including larger numbers of patients, different types of ICRS, and longer follow-up periods are required to evaluate this procedure.
Studying the CET time response to ICRS implantation in KC patients using AS-OCT may help in the further evolution of the ICRS and could be a helpful tool in assessing the success of ICRS implantation.
Conclusions
ICRS implantation creates an elevation on the stromal surface, thickening the epithelium on either side of the rings, and flattening in the corneal center. The subsequent stromal fiber re-arrangement, and epithelial cell compensation to adjust to the new stroma result in a thicker and more regular epithelium in the central area over the cone.
Abbreviations
KC, Keratoconus; AS-OCT, Anterior segment optical coherence tomography; ICRS, Intracorneal ring segments; CET, Corneal epithelial thickness; ET; Epithelial thickness; CXL, corneal crosslinking. CAIRS, Corneal Allogenic Intrastromal Ring Segments.
Acknowledgments
The authors thank Professor Dr. Mustafa El Hossini, Professor of Community and Public Health, Faculty of Medicine, Ain University, for helping with the statistics of this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297–319. doi:10.1016/S0039-6257(97)00119-7
2. Barnett M, Mannis MJ. Contact lenses in the management of keratoconus. Cornea. 2011;30(12):1510–1516. doi:10.1097/ICO.0b013e318211401f
3. Colin J, Cochener B, Savary G, et al. Correcting keratoconus with intracorneal rings. J Cataract Refract Surg. 2000;26(8):1117–1122. doi:10.1016/S0886-3350(00)00451-X
4. Vega-Estrada A, Alio JL. The use of intracorneal ring segments in keratoconus. Eye and Vision. 2016;3:8. doi:10.1186/s40662-016-0040
5. Balparda K, Vanegas-Ramírez CM, Herrera-Chalarca T, et al. Early results with the EyeCryl Phakic Toric intraocular lens I implantation in keratoconus patients. Rom J Ophthalmol. 2021;65(2):163–170. doi:10.22336/rjo.2021.32
6. Jacob S, Patel SR, Agarwal A, et al. Corneal Allogenic Intrastromal Ring Segments (CAIRS) Combined With Corneal Cross-linking for Keratoconus. J Refract Surg. 2018 May 1;34(5):296-303. doi: 10.3928/1081597X-20180223-01
7. Sakellaris D, Balidis M, Gorou O, et al. Intracorneal Ring Segment Implantation in the Management of Keratoconus: An Evidence-Based Approach. Ophthalmology and Therapy. 2019; 8(Suppl 1), 5-14. doi: org/10.1007/s40123-019-00211-2
8. Albertazzi R. Tratamiento del queratocono con segmentos intracorneales. In: Albertazzi R, editor. Queratocono: Pautas para su diagnóstico y tratamiento. Buenos Aires: Ediciones cientificas argentina para la keratoconussociety; 2010:205–268.
9. Burris TE, Baker PC, Ayer CT, et al. Flattening of central corneal curvature with intrastromal corneal rings of increasing thickness: an eye-bank eye study. J Cataract Refract Surg. 1993;19(Supplement 1):182–187. doi:10.1016/S0886-3350(13)80404-X
10. Alió JL, Shabayek MH, Artola A. Intracorneal ring segments for keratoconus correction: long-term follow-up. J Cataract Refract Surg. 2006;32(6):978–985. doi:10.1016/j.jcrs.2006.02.044
11. Ertan A, Colin J. Intracorneal rings for keratoconus and keratectasia. J Cataract Refract Surg. 2007;33(7):1303–1314. doi:10.1016/j.jcrs.2007.02.048
12. Yip H, Chan E. Optical coherence tomography imaging in keratoconus. Clin Exp Optom. 2019;102(3):218–223. doi:10.1111/cxo.12874
13. Lai MM, Tang M, Andrade EM, et al. Optical coherence tomography to assess intrastromal corneal ring segment depth in keratoconic eyes. J Cataract Refract Surg. 2006;32(11):1860–1865. doi:10.1016/j.jcrs.2006.05.030
14. Ortiz S, Pérez-Merino P, Alejandre N, et al. Quantitative OCT-based corneal topography in keratoconus with intracorneal ring segments. Biomed Opt Express. 2012;3(5):814–824. doi:10.1364/BOE.3.000814
15. Gorgun E, Kucumen RB, Yenerel NM, et al. Assessment of intrastromal corneal ring segment position with anterior segment optical coherence tomography. Ophthalmic Surg Lasers Imaging. 2012;43(3):214–221. doi:10.3928/15428877-20120301-01
16. Pérez-Merino P, Ortiz S, Alejandre N, et al. Quantitative OCT-based longitudinal evaluation of intracorneal ring segment implantation in keratoconus. Invest Ophthalmol Vis Sci. 2013;54(9):6040–6051. doi:10.1167/iovs.13-12401
17. Naftali M, Jabaly-Habib H. Depth of intrastromal corneal ring segments by OCT. Eur J Ophthalmol. 2013;23(2):171–176. doi:10.5301/ejo.5000212
18. Pérez-Merino P, Ortiz S, Alejandre N, et al. Ocular and optical coherence tomography-based corneal aberrometry in keratoconic eyes treated by intracorneal ring segments. Am J Ophthalmol. 2014;157(1):116–127. doi:10.1016/j.ajo.2013.08.017
19. Srivannaboon S. Epithelial and stromal changes induced by Intacs were examined by three-dimensional very high-frequency digital ultrasound. J Refract Surg. 2001;17(3):310–318. doi:10.3928/1081-597X-20010501-04
20. David C, Reinstein DZ, Archer TJ, et al. Postoperative Corneal Epithelial Remodeling After Intracorneal Ring Segment Procedures for Keratoconus: an Optical Coherence Tomography Study. J Refract Surg. 2021;37(6):404–413. doi:10.3928/1081597X-20210225-02
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Corneal Epithelium Asymmetry in Children With Atopy: The Effect of Hand Dominance
Loureiro T, Rodrigues-Barros S, Carreira AR, Gouveia-Moraes F, Carreira P, Vide Escada A, Campos P, Machado I, Campos N, Archer TJ, Reinstein DZ, Ambrósio R Jr
Clinical Ophthalmology 2022, 16:2453-2461
Published Date: 6 August 2022