Back to Journals » Drug Design, Development and Therapy » Volume 20
Compatibility and Stability Study of Butorphanol, Nicardipine, Urapidil, and Tirofiban During Multidrug Simultaneous Infusion
Authors Zhao X, Zhang L, Yu S, Fan L, An J ![]() , Dong Z
, Dong Z
Received 2 November 2025
Accepted for publication 25 February 2026
Published 4 March 2026 Volume 2026:20 578559
DOI https://doi.org/10.2147/DDDT.S578559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Xiaoyu Zhao,1,2,* Liting Zhang,1,2,* Siqi Yu,1,2 Liju Fan,1– 3 Jing An,1– 3 Zhanjun Dong1– 3
1School of Pharmacy, Hebei Medical University, Shijiazhuang, 050017, People’s Republic of China; 2Department of Pharmacy, Hebei General Hospital, Shijiazhuang, 050051, People’s Republic of China; 3Hebei Key Laboratory of Clinical Pharmacy, Shijiazhuang, 050051, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhanjun Dong, Department of Pharmacy, Hebei General Hospital, Shijiazhuang, 050051, People’s Republic of China, Email [email protected] Jing An, Department of Pharmacy, Hebei General Hospital, Shijiazhuang, 050051, People’s Republic of China, Email [email protected]
Purpose: This study aimed to assess the physicochemical stability and compatibility of butorphanol tartrate, nicardipine hydrochloride, urapidil, and tirofiban hydrochloride to support safe infusion practices in the ICU.
Patients and Methods: Compatibility systems involving four-, three-, and two-drug combinations were prepared in 0.9% sodium chloride injection under simulated clinical conditions at room temperature in the absence of light. Evaluations included appearance, pH, and insoluble particle counts at 0, 2, 4, 8, 12, and 24 hours. Quantitative analysis of drug concentrations was performed using high performance liquid chromatography (HPLC).
Results: All tested combinations retained physical stability within 24 hours, showing no measurable variation in appearance, pH, or particle. Nicardipine concentrations declined significantly, reaching 74.35% of baseline in the nicardipine–urapidil–tirofiban mixture at 24 hours, and decreasing to 76.29% at 12 hours and 71.46% at 24 hours in the nicardipine–tirofiban combination. The concentrations of active ingredients in the remaining mixtures remained stable, consistently exceeding 90% of initial values.
Conclusion: Butorphanol demonstrated compatibility with the other agents under the tested conditions. In clinical application, infusion of nicardipine combined with tirofiban should be restricted to less than 8 hours, and nicardipine combined with urapidil and tirofiban should not exceed 12 hours. Other mixtures can be administered for up to 24 hours with flexibility in infusion duration.
Keywords: compatibility, stability, butorphanol tartrate, nicardipine hydrochloride, HPLC
Introduction
Administration of multiple intravenous agents is frequently required in intensive care unit (ICU) patients to sustain vital functions and manage underlying conditions. Given the limitation of venous access, simultaneous delivery of several drugs through a single line using a Y-connector or three-way stopcock is commonly adopted. Nevertheless, co-infusion may induce physical or chemical incompatibilities, manifested as precipitation, discoloration, or reduced pharmacological activity, ultimately diminishing therapeutic effectiveness or provoking adverse events.1–3 A systematic assessment of the stability of widely used drug combinations is therefore essential to ensure safe pharmacotherapy in critically ill patients.
The management of critically ill patients with cardiovascular emergencies (acute coronary syndrome, refractory hypertensive crisis, aortic dissection, etc) in the ICU represents a therapeutic challenge due to the frequent coexistence of severe chest pain, hemodynamic instability, and heightened thrombotic risk. Addressing these conditions typically demands the concurrent administration of analgesics, antihypertensive agents, and antiplatelet therapies. In this context, the present study emphasizes four widely employed intravenous agents: the opioid analgesic butorphanol tartrate, the antihypertensives nicardipine hydrochloride and urapidil, and the antiplatelet agent tirofiban hydrochloride. A survey of ICU medication practices at our institution indicated that these drugs were frequently administered in various combinations to achieve hemodynamic stabilization, pain relief, and suppression of platelet activation. Despite their common “cocktail” co-administration in clinical settings—often through intravenous infusion pumps using three-way stopcocks, either in pairs or as multi-drug mixtures—systematic investigations into their physicochemical and pharmaceutical stability remain limited.4 Consequently, the evaluation of compatibility within such multi-drug regimens is essential to ensure both therapeutic effectiveness and patient safety.
Butorphanol tartrate, a mixed opioid receptor agonist–antagonist, constitutes an essential component of ICU analgesic protocols. Reports indicate broad compatibility with multiple agents, although incompatibilities with esketamine and sufentanil have been documented.5–8 Nicardipine, a dihydropyridine calcium channel blocker frequently employed in hypertensive emergencies, demonstrates compatibility with a range of intravenous solutions and drugs, while incompatibility occurs with alkaline solutions and certain antimicrobial agents.9–12 Urapidil, acting through both central and peripheral mechanisms to lower blood pressure, has been shown to remain stable in combination with several commonly administered solvents and medications.9,10 Tirofiban, a glycoprotein IIb/IIIa receptor antagonist used in acute coronary syndromes, retains compatibility with many cardiovascular drugs but demonstrates incompatibility with diazepam.13,14
Although extensive compatibility data exist for each agent individually, investigations into the simultaneous stability of the four agents under clinical mixing conditions remain absent. Considering the frequent clinical co-administration and associated safety concerns, this study systematically assessed the physicochemical stability and compatibility of butorphanol tartrate, nicardipine hydrochloride, urapidil, and tirofiban hydrochloride in various combined regimens, thereby establishing a theoretical basis for safe infusion practices. This study provided the first comprehensive evaluation of the compatibility of butorphanol, nicardipine, urapidil, and tirofiban in dual-, triple-, and quadruple-drug combinations for simultaneous infusion. The results provide robust scientific evidence to support rational and safe infusion strategies in the ICU.
Materials and Methods
Instruments
ACQUITY UPLC H-Class Ultra HPLC system (Waters, USA); AB204-S electronic analytical balance (Mettler-Toledo, Switzerland); adjustable pipettes (Eppendorf, Germany); FE20 laboratory pH meter (Mettler Toledo Instruments, Shanghai, China); GWF8JD particle size analyzer (Tianjin Tianhe Analytical Instrument Co., Ltd., China).
Drugs and Reagents
Butorphanol tartrate injection (1 mL: 1 mg; Jiangsu Hengrui Pharmaceuticals Co., Ltd.; batch number: 230424BP), nicardipine hydrochloride injection (10 mL: 10 mg; Chengdu Easton Biopharmaceuticals Co., Ltd.; batch number: H230701), urapidil injection (5 mL: 25 mg; Guangzhou Imvin Pharmaceutical Co., Ltd.; batch number: 22122601), and tirofiban hydrochloride sodium chloride injection (100 mL: 5 mg; Sichuan Meida Kangjiale Pharmaceutical Co., Ltd.; batch number: 22091911).
Reference standards included butorphanol tartrate (lot number: 171288-202202; purity: 99.7%), nicardipine hydrochloride (lot number: 100586-202203; purity: 99.8%), urapidil (lot number: 100626-202104; purity: 99.8%), and tirofiban hydrochloride (lot number: 100626-202104; purity: 96.1%), all obtained from the National Institutes for Food and Drug Control.
Additional reagents comprised potassium dihydrogen phosphate (Tianjin Damao Chemical Reagent Partnership Enterprise), chromatographic-grade acetonitrile (Thermo Fisher), and purified water (Wahaha, China).
Chromatographic Conditions
Analyses were conducted on an ACQUITY UPLC® BEH C18 column (2.1 × 100 mm, 1.7 μm). The mobile phase consisted of a 0.05 mol/L potassium dihydrogen phosphate aqueous solution and acetonitrile (71.5:28.5, v/v). The flow rate was maintained at 0.3 mL∙min−1. Detection wavelengths were set at 227 nm for butorphanol, nicardipine, and tirofiban, and at 288 nm for urapidil. The injection volume was 10 μL, and the column was operated at ambient temperature.
Solution Preparation
Reference Standard Stock Solution
Precisely 10 mg of butorphanol, 10.1 mg of nicardipine hydrochloride, 21.05 mg of urapidil, and 11.01 mg of tirofiban hydrochloride were weighed and individually dissolved in methanol. Each solution was then diluted to 10 mL with methanol to yield stock solutions at approximate concentrations of 1 mg∙mL−1, 1 mg∙mL−1, 2 mg∙mL−1, and 1 mg∙mL−1, respectively.
Mixed Reference Standard Stock Solutions
The 50 μL, 180 μL, 200 μL, and 30 μL of butorphanol, nicardipine hydrochloride, urapidil, and tirofiban hydrochloride stock solutions were precisely transferred into 1 mL volumetric flasks. Water was used to fill to the calibration line, followed by mixing thoroughly. The resulting mixed reference stock solutions contained the components at approximately 50 μg∙mL−1, 180 μg∙mL−1, 400 μg∙mL−1, and 30 μg∙mL−1, respectively.
Preparation of Test Solutions
Test solutions were prepared using 11 mixed infusion schemes (M1–M11). For each scheme, the corresponding mass or volume of the injection solutions specified in Table 1 was combined with 0.9% sodium chloride injection to reach a final volume of 100 mL, followed by thorough mixing to obtain the mixed solutions. The theoretical concentrations of each drug in these mixtures are listed in the column “Theoretical Concentrations of Each Component in Mixed Solution” in Table 1. Before administration, the infusion mixtures were aspirated from the infusion bags and diluted 2-fold or 4-fold as required to generate the test solutions.
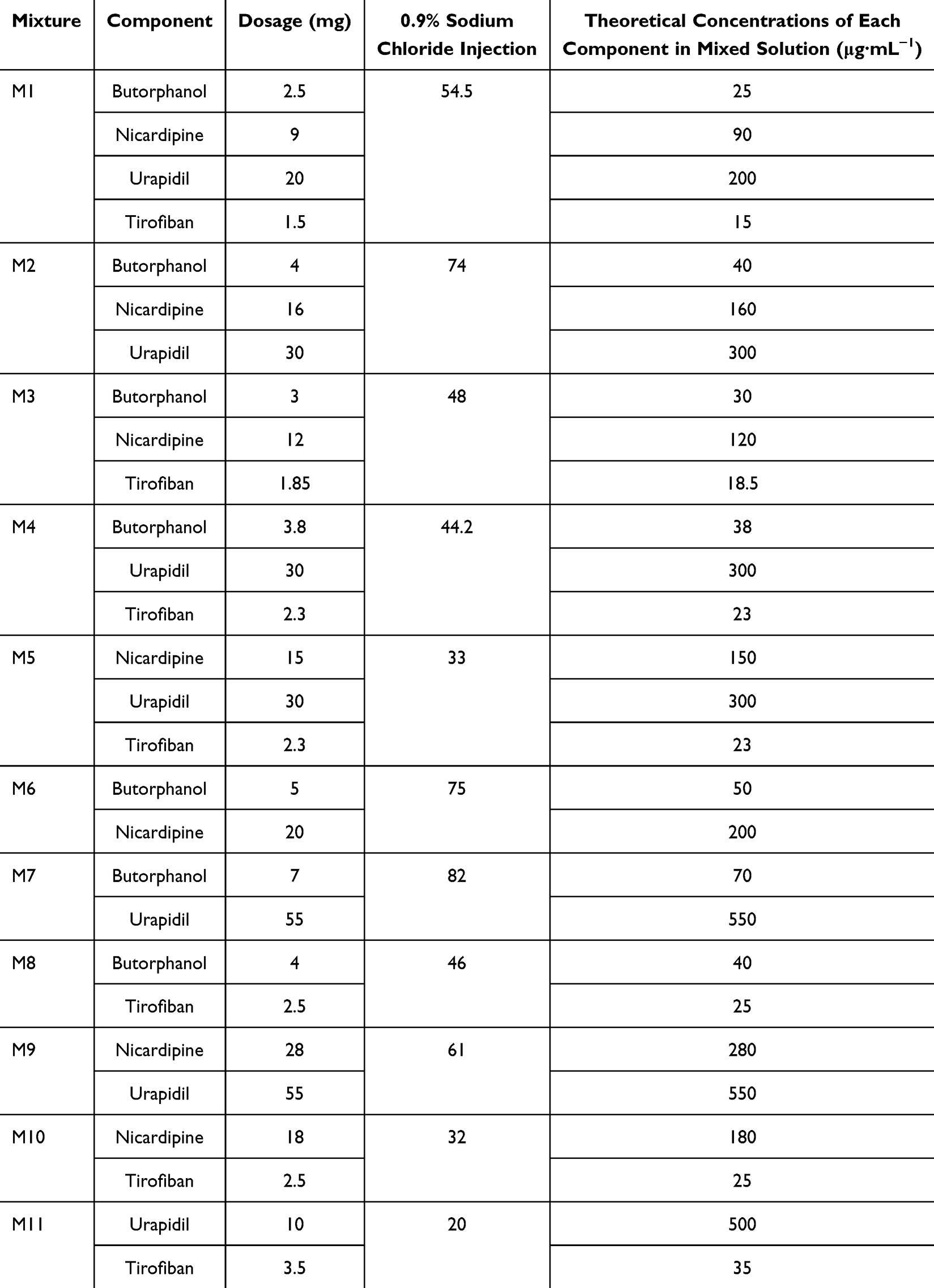 |
Table 1 Composition and Theoretical Concentration of 11 Mixed Infusion Schemes |
Methodological Validation Tests
Specificity Test
Under the chromatographic conditions described in Chromatographic Conditions, both 0.9% sodium chloride injection and the test solution were analyzed, and the chromatograms were recorded.
Range
Accurately measured volumes of the reference stock solutions were diluted with water to obtain calibration standards at the following concentrations: 12.5, 21.25, 25, 28.75, and 37.5 μg∙mL−1 for butorphanol; 45, 76.5, 90, 103.5, and 135 μg∙mL−1 for nicardipine; 100, 170, 200, 230, and 300 μg∙mL−1 for urapidil; and 7.5, 12.75, 15, 17.25, and 22.5 μg∙mL−1 for tirofiban. Each standard was injected under the conditions in Chromatographic Conditions, and chromatograms were recorded.
Repeatability
Six replicates of the test solution were prepared as described in Preparation of Test Solutions and analyzed under the validated chromatographic conditions. Peak areas of each target compound were determined, and the corresponding RSD values were calculated.
Accuracy
A 100 μL aliquot of the test solution from Preparation of Test Solutions was combined with 100 μL of the mixed reference solution at concentrations of 25, 90, 200, and 15 μg∙mL−1, followed by thorough mixing. Five replicates were prepared for chromatographic analysis, and peak areas were recorded to calculate recovery rates. Accuracy was expressed as spiked recovery, where recovery (%) = (amount found – original amount)/amount spiked × 100%. The recovery rates were then calculated.
Mixed Infusion Compatibility Assessment
In accordance with the procedure described in Preparation of Test Solutions, eleven drug mixtures were prepared. Each formulation was tested in triplicate and stored in light-protective black bags at room temperature. At 0, 2, 4, 6, 8, 12, and 24 hours, visual attributes (color, clarity, gas formation), pH, insoluble particle counts, and the concentrations of each constituent were systematically examined.
Criteria for compatibility assessment were defined as follows: the appearance of the solutions, including color, brightness, and clarity, was required to remain unchanged relative to baseline (0 h); a pH variation of 0.2–1.0 was considered acceptable for stability and compatibility.15 And the number of insoluble particles was expected to meet the limits established in the 2020 edition of the Chinese Pharmacopoeia, specifically ≤25 particles with a diameter ≥10 μm and ≤3 particles with a diameter ≥25 μm per milliliter of solution.16 Chemical stability was defined as the retention of at least 90% of the initial concentration of the principal component throughout the observation period.
Appearance
Visual assessment of the compatibility solutions was conducted against a white background.
pH
pH measurements were performed using a pH meter equipped with a glass electrode as the indicator and a saturated calomel electrode as the reference. The instrument was calibrated with standard buffer solutions prior to testing. During measurement, the electrode was rinsed thoroughly with purified water, carefully aspirated, and subsequently rinsed with the test solution until the reading stabilized within ±0.1 units for 1 minute.
Insoluble Particles
At ambient temperature, aliquots of each compatibility mixture were sampled, and particle counts were quantified using a particle analyzer with the light-obscuration method at predetermined intervals. Each sample was assessed in triplicate.
Relative Percentage Composition
For quantitative analysis, 10 μL of each compatibility mixture was injected under the chromatographic conditions described in Chromatographic Conditions. In the case of three-drug combinations, the samples were diluted twofold before injection. The concentrations of butorphanol, nicardipine, urapidil, and tirofiban were measured, and the values obtained at 0 h were defined as 100%. Subsequent relative concentrations were expressed as percentages of these initial values.
Results
Methodological Validation Tests
Specificity Test
The retention times for urapidil, tirofiban, butorphanol, and nicardipine were 1.0, 1.35, 1.8, and 12.8 min, respectively. No additional components in the injection interfered with the quantification of the target analytes, confirming that the method exhibited satisfactory selectivity (Figure 1).
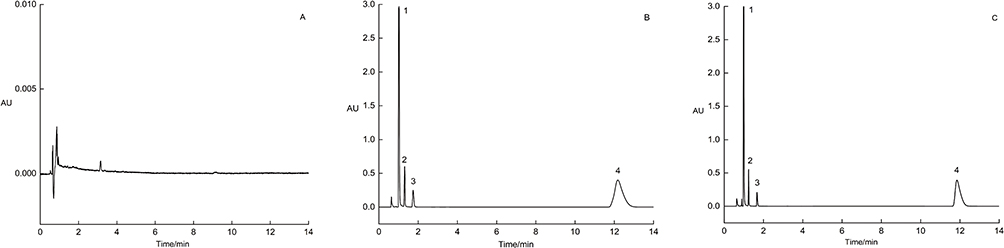 |
Figure 1 HPLC chromatogram (227 nm). Notes: (A) 0.9% sodium chloride injection; (B) test solution; (C) reference solution (1. urapidil; 2. tirofiban; 3. butorphanol; 4. nicardipine). |
Range
Linear regression analysis was conducted using peak area (Y) versus analyte concentration (X), yielding calibration equations with satisfactory linearity (Table 2).
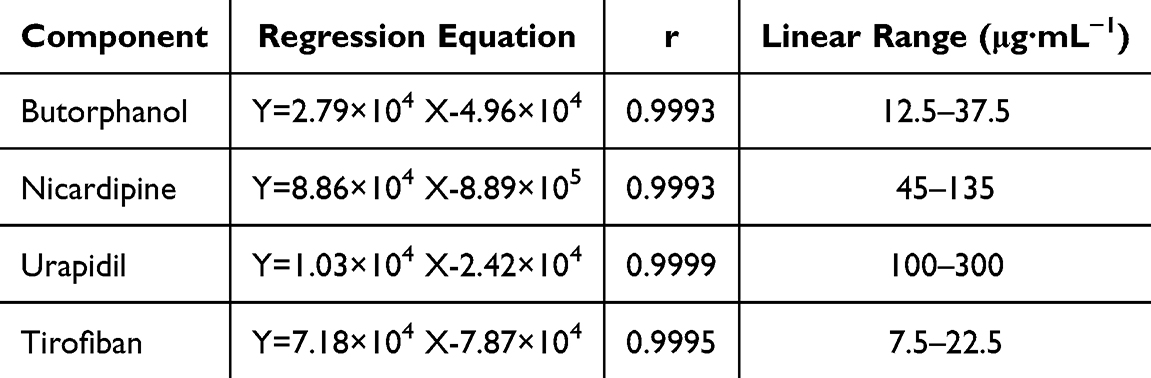 |
Table 2 Regression Equations, Correlation Coefficients, and Linear Ranges of the Four Components |
Repeatability
The RSD values for butorphanol, nicardipine, urapidil, and tirofiban were 0.08%, 0.08%, 0.43%, and 0.10%, respectively, all remaining below 2.0%, thereby confirming satisfactory repeatability of the method.
Accuracy
The average recoveries of butorphanol, nicardipine, urapidil, and tirofiban ranged from 95.86% to 99.56%, with all RSD values below 2% (Table 3).
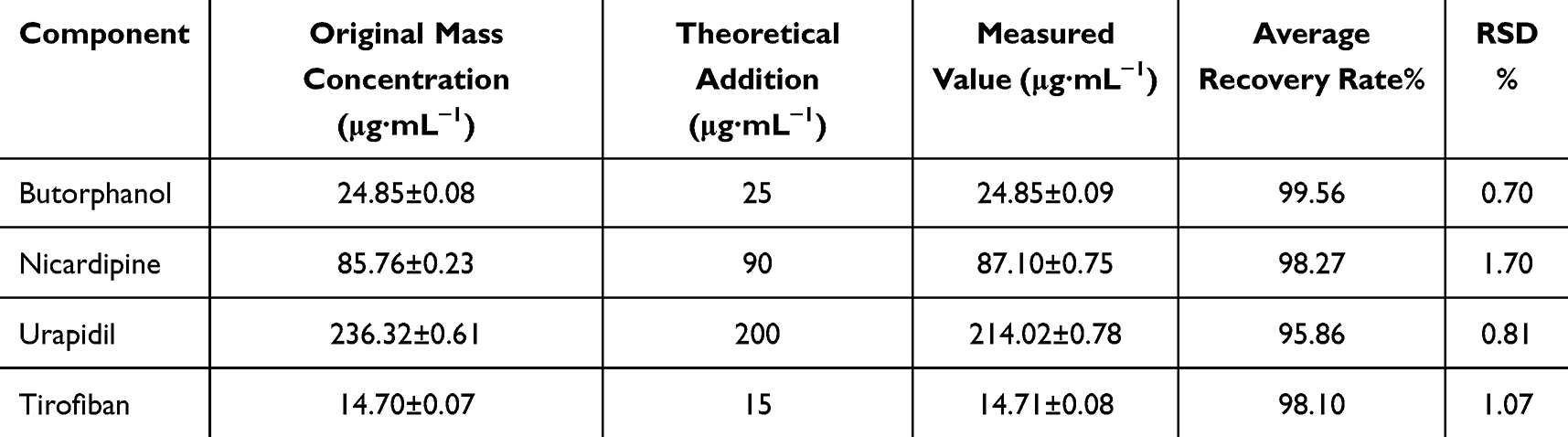 |
Table 3 Spike Recovery of Four Drugs (n=5) |
Mixed Infusion Compatibility Assessment
Appearance
At 0 h, the solutions were colorless, transparent, and free of gas formation. Subsequent evaluations revealed no alterations in color or the presence of gas, precipitates, or turbidity at any tested time point.
pH
Under light-protected conditions, the pH of all test groups remained stable after preparation, with fluctuations not exceeding 0.1 units. Detailed results are provided in Table 4.
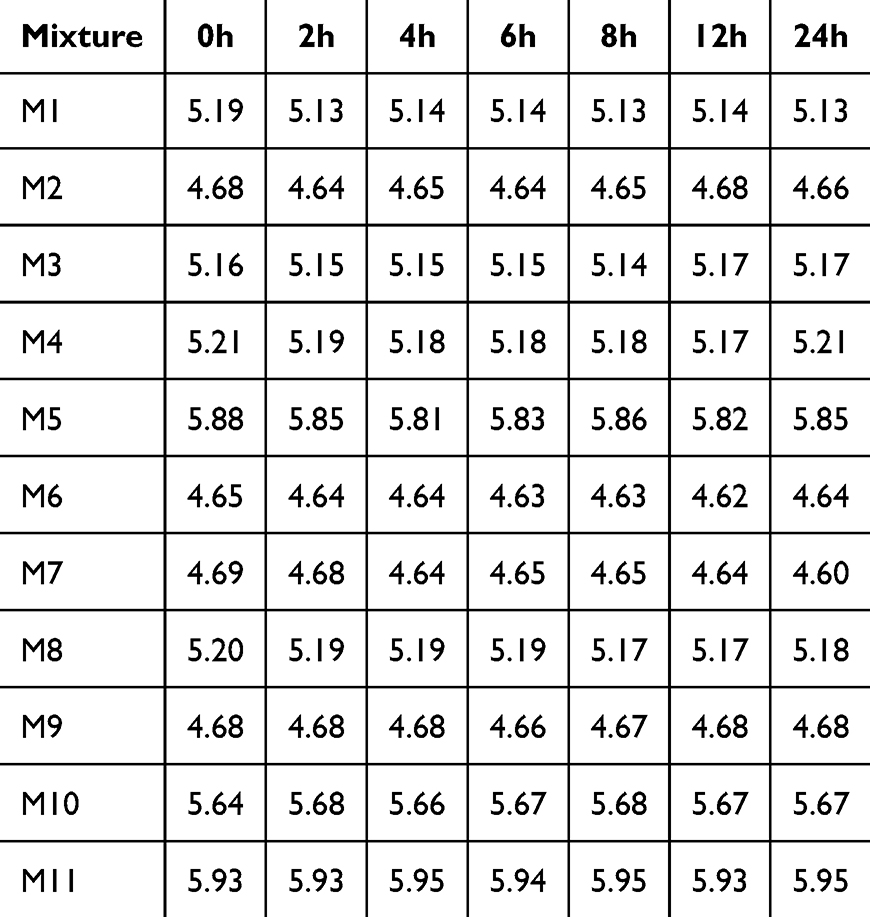 |
Table 4 Changes of pH of Different Compatibility Solutions Over Time |
Insoluble Particles
All preparations complied with the 2020 Chinese Pharmacopoeia criterion, as the number of particles within 24 h remained within the acceptable threshold (Figure 2).
 |
Figure 2 Changes in insoluble particle counts in different compatibility solutions over time. Notes: (A) diameter≥10 μm; (B) diameter≥25 μm. |
Relative Percentage Composition
Nicardipine levels in the nicardipine–urapidil–tirofiban mixture declined to 74.35% at 24 h, whereas in the nicardipine–tirofiban mixture they decreased to 76.29% at 12 h and 71.46% at 24 h. Concentrations of the other analytes remained consistent throughout the observation period, exceeding 90% of baseline values (Figure 3 and Table S1).
 |
Figure 3 Changes in the content of each component in different compatibility solutions over time. Notes: (A) Mixture of four drugs, (B) Mixture of three drugs, (C) Mixture of two drugs (B- Butorphanol; N-Nicardipine; U-Urapidil; T-Tirofiban). |
Discussion
Optimization of Chromatographic Conditions
In HPLC analysis, the mobile phase composition is a determinant of analyte retention, peak shape, and separation efficiency. The present study established optimized chromatographic conditions for a combined system of butorphanol, nicardipine, urapidil, and tirofiban through systematic evaluation of mobile phase compositions.
An initial mobile phase of potassium dihydrogen phosphate–acetonitrile–methanol yielded satisfactory peak shapes for urapidil (tR = 2.25 min), tirofiban (tR = 2.92 min), and butorphanol (tR = 3.76 min). The presence of polar substituents such as urea, sulfonamide, and tertiary amine groups promoted efficient elution in polar organic media via hydrogen bonding. In contrast, nicardipine exhibited markedly poor chromatographic performance under this system, with an extended retention time of 19 min and significant peak tailing. This behavior likely results from the hydrophobic benzene ring and ester functionalities in nicardipine, which interact strongly with the C18 stationary phase in methanol-containing systems. In addition, methanol, acting as a proton donor, readily forms hydrogen bonds with the ester group of nicardipine, enhancing peak tailing. Prolonged retention not only lengthens the analytical cycle but also introduces baseline noise from gradient drift, thereby reducing quantitative reliability. To address these limitations, the mobile phase was adjusted to potassium dihydrogen phosphate–acetonitrile. Under these optimized conditions, nicardipine retention time was reduced to 12.8 min, while retention time and peak shape of urapidil, tirofiban, and butorphanol remained unaffected. This optimized system achieved baseline separation of all four analytes under isocratic conditions, delivering robust and efficient chromatographic performance suitable for quantitative evaluation of mixed drug formulations.
Compatibility Study: Determination of Concentration and Clinical Rationale
Drug concentrations in the mixed infusion were established strictly according to routine clinical protocols, taking into account both prescribed concentrations and infusion rates. In practice, butorphanol tartrate injection, nicardipine hydrochloride injection, urapidil injection, and tirofiban hydrochloride sodium chloride injection are each prepared in 50 mL volumes and co-infused via a microsyringe pump (Figure 4).
 |
Figure 4 Schematic representation of the mixed infusion of four drugs. |
To define clinically representative dosing parameters, a dual approach was applied: retrospective review of medical records from patients who had received single or combined administrations of butorphanol, nicardipine, urapidil, and tirofiban, together with structured interviews of senior ICU nurses. From this process, the following infusion parameters were identified as standard practice: butorphanol 100 μg∙mL−1 at 5 mL∙h−1, nicardipine 400 μg∙mL−1 at 5 mL∙h−1, urapidil 2 mg∙mL−1 at 2 mL∙h−1, and tirofiban 50 μg∙mL−1 at 6 mL∙h−1.
The resulting infusion mixture followed a volumetric ratio of 5:5:2:6, corresponding to a cumulative flow rate of 18 mL∙h−1. From this ratio, theoretical concentrations of each component were derived and subsequently employed as the working levels for the compatibility assessment.
The calculated theoretical concentration corresponds to the drug’s state at the point of venous entry, preceding any dilution by circulating blood, and thus accurately mirrors the exposure encountered within the infusion pathway. Employing clinically relevant concentrations in stability assessments prevents distortion caused by unrealistically high or low levels, providing a sound experimental foundation and reinforcing the reliability of the study’s conclusions.
Rationality Analysis of Drug Combination
The simultaneous administration of multiple intravenous medications is required in critically ill ICU patients. However, limited vascular access or the urgent need to achieve synergistic goals such as blood pressure control, analgesia, and antiplatelet therapy within a short timeframe frequently necessitates multi-drug co-infusion through a single line. A survey of intravenous medication use in our ICU identified 32 commonly used intravenous drugs. Patients often received mixed infusions of 2 to 7 drugs, resulting in a total of 39 distinct combination regimens. The four drugs involved in this study are frequently employed in various combined regimens in clinical practice for stabilizing hemodynamics, alleviating pain, and inhibiting platelet aggregation.17
From the perspective of antihypertensive and hemodynamic management, nicardipine and urapidil are primarily used for arterial hypertension and hypertensive crises. Their combination can leverage complementary mechanisms of action, achieving synergistic, rapid, and stable blood pressure control while potentially reducing adverse effects associated with high doses of a single agent.18,19 Studies indicate that nicardipine achieves target blood pressure levels faster than urapidil.20 Compared to sodium nitroprusside, urapidil has a lesser impact on heart rate when treating hypertensive emergencies.21 In the management of blood pressure prior to intravenous thrombolysis for acute ischemic stroke, it is necessary to rapidly reduce systolic blood pressure to <180 mmHg and diastolic blood pressure to <100 mmHg, while avoiding a precipitous drop in pressure. Urapidil, with its rapid onset and minimal effect on heart rate, is suitable for most hypertensive patients. If its effect is insufficient, nicardipine can be added. Although sodium nitroprusside has a rapid onset and potent antihypertensive effect, a too-rapid dose increase may lead to a sharp decline in blood pressure, and long-term use carries a risk of toxicity; therefore, it is not recommended as the first choice prior to thrombolysis and should be used with caution. Regarding antiplatelet therapy, tirofiban, as a potent GP IIb/IIIa receptor antagonist, is particularly suitable for combination with the aforementioned antihypertensive drugs in patients with acute coronary syndrome complicated by hypertension or during the perioperative period of percutaneous coronary intervention, allowing for simultaneous management of thrombosis and blood pressure].22 Studies have confirmed that in patients with acute ischemic stroke, intravenous tirofiban administered prior to endovascular thrombectomy can facilitate the procedure, significantly improving the first-pass effect without increasing the risk of symptomatic intracranial hemorrhage.23 For analgesia, butorphanol, characterized by relatively low respiratory depression and a longer duration of action, serves as an option for analgesia in critically ill or postoperative patients. Its combination with antihypertensive drugs can help maintain hemodynamic stability while providing pain control.
The four-drug combination scheme is applicable for severe cases with multi-system dysfunction, such as complex scenarios involving severe cerebral hemorrhage complicated by coronary heart disease, refractory hypertension, and moderate-to-severe pain. However, simultaneous infusion of multiple drugs carries risks related to physical compatibility, drug-drug interactions, and the superimposition of adverse effects. These risks require heightened vigilance, particularly in elderly patients or those with hepatic or renal impairment. Therefore, clinical implementation necessitates rigorous monitoring of platelet counts, hemodynamic parameters, and adverse reactions. Furthermore, careful planning of administration sequence, infusion routes, and dose adjustment strategies is essential to ensure the safety and efficacy of the treatment.
Investigation into the Stability and Molecular Mechanisms of Drug Infusion Compatibility
This study showed that no visible precipitation or turbidity was observed in any of the compatibility solutions within 24 hours. When co-infused with tirofiban, nicardipine concentration declined to 76.29% after 12 h and further to 71.46% at 24 h. In the ternary combination of nicardipine, urapidil, and tirofiban, the content decreased to 74.35% within 24 h. Chromatographic analysis (Figure 5) revealed that although the main peak area of nicardipine continued to decrease, no prominent or distinct new chromatographic peaks appeared in its vicinity. These findings suggest that nicardipine exhibits limited stability under such conditions and raising concerns for clinical application.
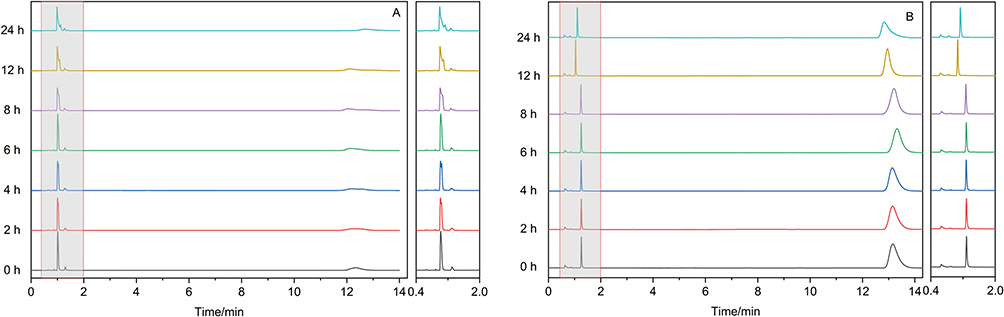 |
Figure 5 Chromatograms of the two combinations with content degradation ((A) Nicardipine-Urapidil-Tirofiban, (B) Nicardipine-Tirofiban). |
Despite the overall stability of pH across 0–24 h in all groups, notable variations were observed in the initial values among compatibility regimens. The pH in both the nicardipine–tirofiban and nicardipine–urapidil–tirofiban mixtures consistently exceeded 5.5, which is substantially higher than the recommended range for nicardipine injection (3.0–4.5). Studies have shown that an increase in pH can significantly accelerate the degradation rate of nicardipine, with optimal stability observed at pH 4.5.24 The alkaline environment may enhance the electron cloud density of the dihydropyridine ring in nicardipine, making it more susceptible to oxidation or nucleophilic attack. Under mildly alkaline conditions, the sulfonamide group in the tirofiban molecule exhibits increased nucleophilicity, potentially attacking the ester bonds at the C3 and C5 positions of nicardipine and accelerating hydrolysis. Additionally, this group can act as a weak ligand, altering the electron distribution of the dihydropyridine ring and promoting its oxidative aromatization, collectively contributing to accelerated degradation.
The degradation of nicardipine exhibits a multi-pathway, progressive pattern. As a dihydropyridine calcium channel blocker, nicardipine is prone to oxidative aromatization and hydrolysis of its ester bonds and dihydropyridine ring under alkaline conditions, leading to the formation of various polar degradation products. In reversed-phase chromatography, these products may elute earlier and present as dispersed peaks without forming distinct, isolated signals. Additionally, factors such as high temperature and light exposure may further induce nicardipine to undergo hydrolysis, ring‑opening, rearrangement, and decarboxylation reactions, resulting in unstable derivatives.24–28
The combination of multiple drugs may trigger complex drug – drug interactions, where degradation products can alter the local microenvironment and thereby affect the stability of co‑existing drugs. In the chromatogram of the nicardipine – urapidil – tirofiban mixture (Figure 5), the chromatographic peak of urapidil showed gradual splitting between 8 h and 24 h, indicating that its chemical stability had been compromised. It is hypothesized that carboxylic acid derivatives generated from nicardipine degradation progressively modify the local microenvironment, which may induce tautomerization or minor degradation of urapidil.
Additionally, in this study, butorphanol maintained high stability (content > 90%) across all compatibility combinations, which is closely related to its molecular structural characteristics. Butorphanol possesses a rigid fused‑ring skeleton and lacks susceptible functional groups prone to hydrolysis or oxidation (such as ester bonds or a dihydropyridine ring). Moreover, its tert‑butyl side chain provides steric hindrance, collectively conferring favorable chemical inertness and broad pH stability. As a result, butorphanol retains structural integrity even in complex multi‑drug environments (Figure 6).
 |
Figure 6 Chemical structures of the four drugs. |
Although no precipitation was observed in any of the compatibility solutions in this study, existing literature indicates that nicardipine rapidly precipitates in sodium bicarbonate injection.29 This suggests that under specific ionic strengths or higher pH conditions, degradation products of nicardipine may form microparticles. Therefore, for multi‑drug combination infusions, relying solely on solution clarity and changes in the main drug peak area is insufficient to fully evaluate compatibility safety. Close attention must also be paid to abnormal chromatographic behavior of co‑existing drugs. To ensure the efficacy of nicardipine and avoid unforeseen interactions, it is essential to strictly avoid long‑term co‑infusion with drugs that elevate pH in the same infusion line. Administration via a separate line or sequential infusion with adequate line flushing between drugs is recommended.
Limitations
The drug concentrations investigated in this study were restricted to ranges commonly applied in clinical settings and did not include all potential extremes or transitional levels. In addition, compatibility under conditions of high-dose administration or ultra-rapid infusion rate remains to be clarified through further research.
Conclusion
This study systematically assessed the physicochemical stability and compatibility of butorphanol, nicardipine, urapidil, and tirofiban in dual-, triple-, and quadruple-drug infusion systems, thereby establishing an experimental foundation for safe combination therapy in clinical practice. A validated HPLC method was developed and optimized for the simultaneous quantification of these drugs, enabling precise evaluation of mixture integrity across different time intervals.
The findings indicate that several drug combinations demonstrated favorable physical stability over 24 h. Based on the chemical instability observed, it is recommended that when nicardipine is co-administered with tirofiban, the infusion durations should be limited to 8 hours, whereas combinations of nicardipine, urapidil, and tirofiban should not exceed 12 hours. Other tested combinations maintained acceptable physical and chemical stability over a 24-hour period, permitting more flexible infusion strategies.
Overall, the study findings offer practical reference for rational compatibility of ICU medications, minimize risks associated with reduced efficacy or adverse reactions from instability, and contribute to ensuring both safety and therapeutic effectiveness in critically ill patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Medical Science Project of Hebei (No.20250307); Wu Jieping Medical Foundation Special Fund for Clinical Research (No. 320.6750.2024-6-60).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Négrier L, Martin Mena A, Lebuffe G, et al. Strategies to prevent drug incompatibility during simultaneous multi-drug infusion in intensive care units: a literature review. Eur J Clin Pharmacol. 2021;77(9):1309–13. doi:10.1007/s00228-021-03112-1
2. Sriram S, Aishwarya S, Moithu A, et al. Intravenous drug incompatibilities in the intensive care unit of a tertiary care hospital in India: are they preventable. J Res Pharm Pract. 2020;9(2):106–111. doi:10.4103/jrpp.JRPP_20_11
3. Wagner LAF, Neininger MP, Hensen J, et al. Avoiding incompatible drug pairs in central-venous catheters of patients receiving critical care: an algorithm-based analysis and a staff survey. Eur J Clin Pharmacol. 2023;79(8):1081–1089. doi:10.1007/s00228-023-03509-0
4. Marsilio NR, Silva D, Bueno D. Drug incompatibilities in the adult intensive care unit of a university hospital. Rev Bras Ter Intensiva. 2016;28(2):147–153. doi:10.5935/0103-507X.20160029
5. Chen FC, Shi XY, Li P, et al. Stability of butorphanol-tropisetron mixtures in 0.9% sodium chloride injection for patient-controlled analgesia use. Medicine. 2015;94(6):e432. doi:10.1097/MD.0000000000000432
6. Fang B, Wang L, Chen F, et al. A simple HPLC method for the determination of butorphanol tartrate and ondansetron hydrochloride in patient-controlled analgesia solution. Acta Chromatogr. 2018;30(1):43–46. doi:10.1556/1326.2016.00142
7. Chen F, Li P, Zhou B, et al. Stability of an epidural analgesic admixture containing butorphanol tartrate and ropivacaine hydrochloride. Eur J Hosp Pharm. 2015;22(1):7–11. doi:10.1136/ejhpharm-2014-000450
8. Fang B, Wang L, Gu J, et al. Physicochemical stability of ternary admixtures of butorphanol, ketamine, and droperidol in polyolefin bags for patient-controlled analgesia use. Drug Des Devel Ther. 2016:3873–3878. doi:10.2147/DDDT.S123411
9. Leeuwerik AF, van Merendonk LN, de Boer MA, et al. A new approach to drug intravenous compatibility research: the case of obstetric parenteral drugs. Eur J Hosp Pharm. 2024;31(5):455–460. doi:10.1136/ejhpharm-2022-003577
10. Peng S, Li X, Yang H, et al. Compatibility and safety of vancomycin combined with nicardipine, nimodipine, and urapidil in microinfusion pump systems for clinical subarachnoid hemorrhage treatment. J Pharm Sci. 2025;114:103968. doi:10.1016/j.xphs.2025.103968
11. Thabit AK, Hamada Y, Nicolau DP. Physical compatibility of ceftolozane-tazobactam with selected i.v. drugs during simulated Y-site administration. Am J Health Syst Pharm. 2017;74(1):e47–e54. doi:10.2146/ajhp150762
12. Correard F, Savry A, Gauthier-Villano L, et al. Visual compatibility of defibrotide with selected drugs during simulated Y-site administration. Am J Health Syst Pharm. 2014;71(15):1288–1291. doi:10.2146/ajhp130700
13. Patel K, Hursting MJ. Compatibility of argatroban with Abciximab, eptifibatide, or tirofiban during simulated Y-site administration. Am J Health Syst Pharm. 2005;62(13):1381–1384. doi:10.2146/ajhp040391
14. Garabito MJ, Jimenez L, Bautista FJ, et al. Stability of tirofiban hydrochloride in 0.9% sodium chloride injection for 30 days. Am J Health Syst Pharm. 2001;58(19):1850–1851. doi:10.1093/ajhp/58.19.1850
15. Koller AK, Krebs S, Dörje F. Medication safety in intravenous therapy: a compatibility study of clonidine with drugs frequently used in intensive care. Pharmaceutics. 2020;13(1):21. doi:10.3390/pharmaceutics13010021
16. Chinese Pharmacopoeia Commission. Chinese Pharmacopoeia (the Fourth Volume). Med Sci Technol Press China. 2020:125–126.
17. He XR, Fan LJ, Li X, et al. Literature analysis of compatible stability of commonly used intravenous drugs in ICU. China Pharm. 2023;34(6):752–757.
18. Ibarra F, Holzmann S, Shah S, et al. Utility of nicardipine in the management of hypertensive crises in adults with reduced ejection fractions. Am J Emerg Med. 2023;75:79–82. doi:10.1016/j.ajem.2023.10.041
19. Abdrakhmanov VR, Gaponova NI, Plavunov NF. Use of urapidil-antihypertensive drug with double action-new direction in treatment of hypertensive crises. Racional’naâ farmakoterapiâ v kardiologii. 2014;10(5):559–564. doi:10.20996/1819-6446-2014-10-5-559-564
20. Wu KS, Zhou JC, Li HY, et al. Antihypertensive therapy with nicardipine for patients with aortic disease is associated with more esmolol usage than urapidil. J Thorac Dis. 2014;6(12):1765–1771. doi:10.3978/j.issn.2072-1439.2014.12.22
21. Villarreal EG, Flores S, Kriz C, et al. Sodium nitroprusside versus nicardipine for hypertension management after surgery: a systematic review and meta-analysis. J Cardiac Surg. 2020;35(5):1021–1028. doi:10.1111/jocs.14513
22. Sun Z, Zeng J, Huang H. Intracoronary injection of tirofiban prevents microcirculation dysfunction during delayed percutaneous coronary intervention in patients with acute myocardial infarction. Int J Cardiol. 2016;208:137–140. doi:10.1016/j.ijcard.2016.01.204
23. Lin L, Liu F, Yi T, et al. Tirofiban on first-pass recanalization in acute stroke endovascular thrombectomy: the OPTIMISTIC Randomized Clinical Trial. JAMA Network Open. 2025;8(4):e255308. doi:10.1001/jamanetworkopen.2025.5308
24. Ibrahim K, Al-Ashban R, Babiker L. A selective high performance liquid chromatographic method to follow the hydrolytic degradation of nicardipine hydrochloride. E-J Chem. 2010;7(1):85–92. doi:10.1155/2010/625296
25. Shen GB, Gao SH, Jia YW, et al. Establishing the thermodynamic cards of dipine models’ oxidative metabolism on 21 potential elementary steps. Molecules. 2024;29(15):3706. doi:10.3390/molecules29153706
26. Al-Ghannam S, Al-Olayan A. Stability-indicating HPLC method for the determination of nicardipine in capsules and spiked human plasma. Identification of degradation products using HPLC/MS. Arabian J Chem. 2019;12(8):1983–1993. doi:10.1016/j.arabjc.2014.11.044
27. Vaghela B, Rao S. Identification and characterization of a novel potential degradant and development and validation of stability-indicating RP-LC method for nicardipine impurities in injectable dosage form. J Liquid Chromatogr Related Technol. 2013;36(15):2166–2181. doi:10.1080/10826076.2012.717056
28. Fuss D, Gondé H, Lamoureux F, et al. Stability study of a compounded oral solution of nicardipine for the treatment of hypertension in children. Eur J Pharm Sci. 2021;160:105738. doi:10.1016/j.ejps.2021.105738
29. Baaske DM, DeMay JF, Latona CA, et al. Stability of nicardipine hydrochloride in intravenous solutions. Am J Health Syst Pharm. 1996;53(14):1701–1705. doi:10.1093/ajhp/53.14.1701
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Compatibility and Stability of Ten Commonly Used Clinical Drugs in Pediatric Electrolyte Supplements Injection
Shen H, Fu Y, Chen Y, Xia W, Jia ZJ, Yu Q, Zhang L, Han L
Drug Design, Development and Therapy 2022, 16:1433-1440
Published Date: 12 May 2022