Back to Journals » Patient Preference and Adherence » Volume 17
Comparisons of Clients’ and Caregivers’ Satisfaction Across Conventional, Virtual, and Hybrid Speech-Language Therapy Services in Malaysia
Authors Hassan FH ![]() , Zakaria AS
, Zakaria AS ![]() , Ahmad Rusli Y, Haris SM, Mohd Azraai H
, Ahmad Rusli Y, Haris SM, Mohd Azraai H
Received 3 March 2023
Accepted for publication 28 June 2023
Published 19 July 2023 Volume 2023:17 Pages 1731—1740
DOI https://doi.org/10.2147/PPA.S407347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Fatimah Hani Hassan,* Anis Syazwani Zakaria,* Yazmin Ahmad Rusli, Siti Munirah Haris, Hafizah Mohd Azraai
Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
*These authors contributed equally to this work
Correspondence: Fatimah Hani Hassan, Speech Sciences Program, Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Temerloh, Kuala Lumpur, 53200, Malaysia, Tel +60392895014, Email [email protected]
Purpose: This study compared the satisfaction of recipients of conventional speech-language therapy (C-SLT), speech-language teletherapy (SLTT), and hybrid speech-language therapy (H-SLT), and determined sociodemographic factors that affect their satisfaction.
Patients and Methods: Participants were clients and caregivers of a speech-language clinic at a public university. Services were primarily provided by student clinicians, who were undergoing supervised clinical training. An online survey was distributed, which consisted of three sections: Background Information, Overall Satisfaction in SLT, and Satisfaction in SLTT. All participants completed the first two sections, while the third section was completed only by those who experienced SLTT or H-SLT.
Results: Most of the respondents were caregivers (89.7%), female (79.4%), of Malay ethnicity (80.9%), have received tertiary education (77.9%), within the low-income category (66.2%), held a job (76.5%), and resided in central West Malaysia (83.8%). Many participants experienced C-SLT (51%), followed by H-SLT (34%), and SLTT (15%). There were no significant differences in the overall satisfaction of the participants across three modes of services delivery (F[2,67] = 0.02, p = 0.95), and in the satisfaction with teletherapy between the H-SLT and SLTT groups (t = 0.90, p = 0.38). Income was the only sociodemographic factor that was correlated with the satisfaction level in teletherapy (r = 0.37, p = 0.04).
Keywords: communication disorders, patients’ experience, telerehabilitation, university training
Introduction
A high satisfaction level of healthcare recipients is one of the key indicators of effective person-centered healthcare services.1 Consumer satisfaction in healthcare services is associated with positive health outcomes, an increased number of patients pursuing care at specific healthcare institutions, and increased loyalty of their consumers.2 Satisfaction is a psychological outcome based on personal experiences that are matched with individuals’ perceived needs and expectations.3,4 Consumers’ satisfaction levels may be influenced by their backgrounds, such as gender, educational level, and economic status.5,6 Naunheim et al emphasized that the satisfaction level of healthcare consumers may indicate the suitability of treatment programs according to individuals’ sociocultural background that tends to be diverse across groups.1 In the field of speech-language therapy (SLT), high satisfaction among clients and caregivers of those who receive speech-language services has been reported.7,8 Multiple factors were found associated with the level of satisfaction with SLT, including perceived therapeutic progress, cost of treatment, clinicians’ rapport with the clients, and duration and frequency of treatment.7,8 More recently, researchers have demonstrated high satisfaction among SLT recipients who received treatments through virtual methods.8–12
Teletherapy is a method for delivering SLT services from a distance using communication technologies, including telephones, internet-based video conferences, and electronic messaging.9 Molini-Avejonas et al13 reported growth of speech-language teletherapy in the past decade, especially in high-income countries, such as the United States and Australia. Following the COVID-19 outbreak, telehealth gained significant attention from healthcare providers due to its credibility as an alternative to face-to-face care.14 Following suit, speech-language therapists have been adopting this method of service delivery to a larger extent.15 Teletherapy services were reported to be convenient in reducing travel costs and time, enabling service provision in environments that are familiar to the recipients, and allowing multi-professional involvement from various locations.16 However, there are some persisting challenges related to teletherapy, such as the adequacy of technological infrastructures and individual technological incompetence.10,11 In addition, a lack of shared physical presence contributes to ineffective communication between clinicians and clients who are younger or have cognitive disabilities.15
Despite high satisfaction in conventional face-to-face SLT and teletherapy, none of the studies to our knowledge have compared the satisfaction of service recipients between these two service delivery methods. Moreover, the satisfaction level is unknown for those who receive a combination of these two services, referred to as the hybrid service (where SLT consumers attend a face-to-face session and receive treatments via teletherapy on alternating therapy sessions). It is important to compare the satisfaction of SLT recipients according to different service delivery modes to determine any potential differences in the quality of services. Underlying factors that may contribute to such differences should be determined to help prepare for further improvement in service delivery. In this study, we compared the satisfaction of clients and caregivers who were receiving three types of SLT services: (a) conventional face-to-face speech-language therapy (C-SLT), speech-language teletherapy (SLTT), and hybrid speech-language therapy (H-SLT). We also identified aspects of teletherapy and personal background factors that might influence their satisfaction with those services. The study protocol complied the with the Declaration of Helsinki and was approved by the Universiti Kebangsaan Malaysia’s Research Ethics Committee (approval number: JEP-2022-101).
Materials and Methods
Participants
To address the study objectives, we surveyed individuals who met the following inclusion criteria: (a) a client or a caregiver of clients who received services at the study site, and (b) SLT services were received between January 2022 and June 2022. Participants were excluded if: (a) they did not meet a minimum reported age of 18 years, or (b) they received less than five therapy sessions via one of the SLT service delivery modes (C-SLT, H-SLT, or SLTT).
Research Tools and Materials
A self-administered questionnaire was developed based on existing surveys that have been used in other studies.17–20 The initial questionnaire which consisted of 47 total items was validated by five speech-language therapists (SLTs), who served as panel experts. All of the SLTs met the following criteria: (a) have experience providing SLT services through conventional and virtual methods, (b) have provided teletherapy for the past one year, and (c) have at least three years of working experience as an SLT. The questionnaire was revised according to their input on the content, sentence structure, and overall presentation. The revised version was forward and backward translated from English to Malay languages. Both English and Malay questionnaires were evaluated by a different group of panel experts, which consisted of six speech-language therapists and a linguist. The panel experts evaluated the comparability between English and Malay versions of the questionnaire using a five-point Likert scale from 5 (extremely comparable) to 0 (not comparable at all) on the wording and sentence structuring, and similarity of meanings. In general, the experts indicated that the English and Malay versions are highly comparable (mean,  = 4.70, standard deviation, s = 0.26). Both versions of the questionnaire were further revised based on the experts’ recommendations.
= 4.70, standard deviation, s = 0.26). Both versions of the questionnaire were further revised based on the experts’ recommendations.
For each language, the questionnaire was made available in a client version and a caregiver version. Each of the client and caregiver questionnaires was divided into three sections: (a) Background Information, (b) Overall Satisfaction in SLT, and (c) Satisfaction in SLTT. The first section (Background Information) consisted of items for gathering participants’ sociodemographic data (eg, gender, age, marital status, education level, and income). In the caregiver version, this section focused on the background of the caregiver. Four additional questions were added to gather information about the person under the caregiver’s care who was receiving SLT. Section 2 (Overall Satisfaction in SLT) consisted of 23 statement-based items related to clients’ and caregivers’ experience in speech-language therapy. All items were positively worded except for seven that were negatively worded. Each item was presented with a five-point Likert scale (strongly disagree, disagree, neutral, agree, and strongly agree). At the beginning of Section 3 (Satisfaction in SLTT), two questions were added to determine methods for accessing online speech-language therapy. Those questions were followed by 21 statement-based items presented with the five-point Likert scale (strongly disagree through strongly agree) to measure different aspects of teletherapy (ie, usefulness, ease of utilization and learning, application interface, interaction quality, and reliability). Two of the 21 items were negatively worded. Both client and caregiver versions consisted of the same satisfaction-related statements. All versions of the questionnaire were converted into Google Forms. The questionnaire was pretested with five caregivers and two clients who had previously participated in H-SLT to determine the duration for completing the questionnaire and to measure the internal consistency of items for measuring satisfaction. The clients and caregivers completed the questionnaire within 10–15 minutes. The questionnaire achieved a Cronbach’s alpha value of 0.96, which indicated high internal consistency.
Procedures
The online questionnaire was distributed to all clients and caregivers who were receiving treatment at a university clinic in Kuala Lumpur. This clinic primarily served as a training facility for student clinicians who are pursuing an academic qualification in SLT. Student clinicians at this facility provided standard SLT services under the supervision of qualified SLTs. In addition, SLT services were provided by qualified clinicians and clinical lecturers. During the study period, the clinic was the only facility in Malaysia offering the three types of services being studied: C-SLT, H-SLT, and SLTT (Ahmad Rusli et al, 2021).21 The link to the online questionnaire was distributed directly to the clients and caregivers by the student and practicing clinicians. Additionally, a QR code to access the online questionnaire was generated and displayed at the registration counter and clinic notice boards.
Before completing the questionnaire, participants were asked to verify their consent for taking part in the study. Participants were then required to indicate their involvement in SLT either as a client or a caregiver. Their responses automatically directed them to the corresponding questionnaire. All participants completed the first two sections (Background Information and Overall Satisfaction in SLT). At the end of the second section, a question was asked to determine the type of service that the participants received (C-SLT, H-SLT, or SLTT). Participants who selected C-SLT were directed to the Thank You page at the end of the questionnaire. The selection of H-SLT and SLTT directed participants to the third section of the questionnaire (Satisfaction in SLTT).
Data Analysis
Data from Google Forms were automatically compiled in Microsoft Excel format. Data were imported into IBM SPSS Statistics Version 25.0 for analysis. All data for negative items were recorded so that their values are parallel to the values of positive items. All categorical data were analyzed for frequencies and percentages, while all continuous data were analyzed for means and standard deviations. Overall satisfaction in SLT and satisfaction in SLTT were compared between client and caregiver groups. A one-way, between-group analysis of variance (ANOVA) was conducted to compare the level of satisfaction in C-SLT, H-SLT, and SLTT. An independent t-test was conducted to compare satisfaction in SLTT between H-SLT and SLTT groups. A series of Pearson’s correlation analyses were conducted to determine factors that may influence clients’ and caregivers’ satisfaction with SLT services.
Results
Complete responses were collated from 70 participants (43.8% of clients/caregivers who were receiving SLT services at the university clinic). Two participants were excluded for not meeting the inclusion/exclusion criteria. Out of 68 participants, seven participants were clients (10.3%) and 61 were caregivers (89.7%). The percentages of participants according to the types of received SLT services were shown in Figure 1. Participants mostly received C-SLT, followed by H-SLT and SLTT.
 |
Figure 1 Proportions of participants according to the types of SLT services received. |
The participants’ ages ranged between 20 and 75 years. For the client group, the mean age of the participants was 37.3 years with a standard deviation (s) of 9.3 (age range: 20–75 years), while for the caregiver group, the mean age of participants was 39.3 years (s = 14.6, 22–69 years). Other background information of the participants was summarized in Table 1.
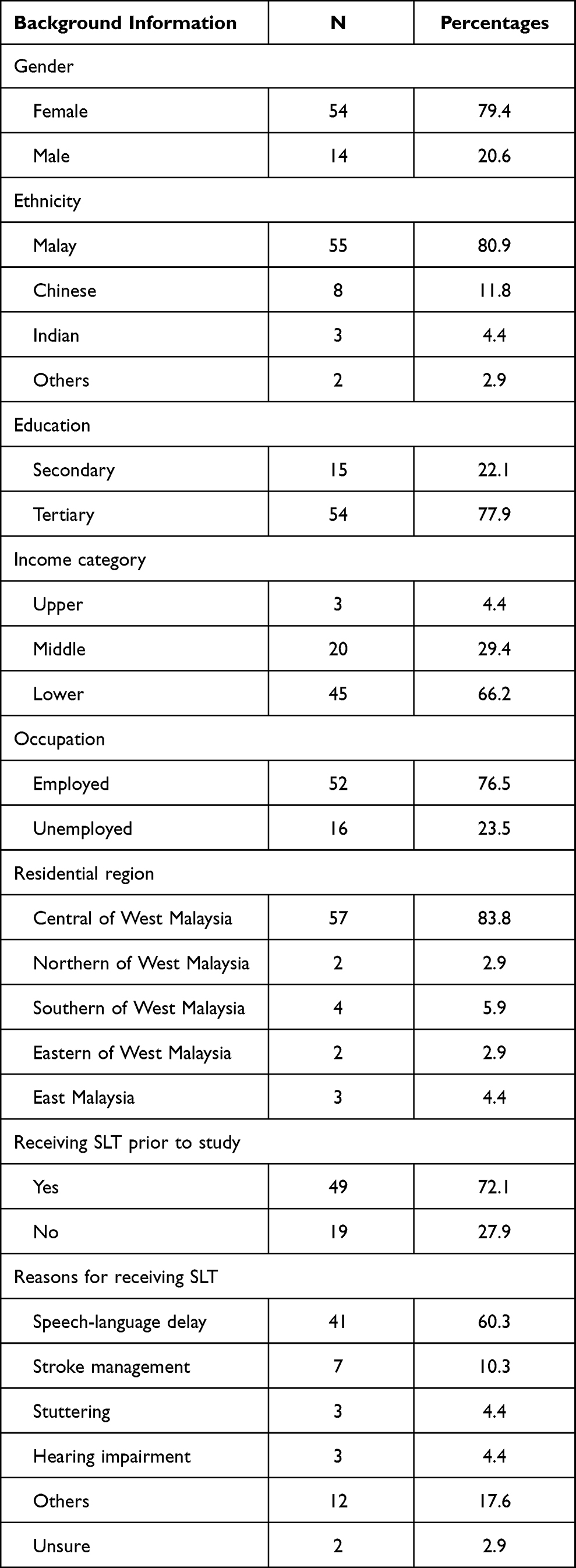 |
Table 1 Participants’ Demography |
Participants’ Overall Satisfaction with SLT Services
Based on data from Section 2: Overall Satisfaction in SLT, an average satisfaction level of 4.14 (s = 0.45). The independent samples t-test demonstrated non-significant differences (t=1.65 p=0.11) in the overall satisfaction between clients ( = 4.40, s = 0.41) and caregivers (
= 4.40, s = 0.41) and caregivers ( = 4.11, s = 0.45). In comparing participants’ satisfaction across different types of services (C-SLT, H-SLT, and SLTT)), no significant differences were found (F[2,67] = 0.02, p = 0.95). Mean values and standard deviations for different types of SLT services are specified in Table 2. Based on correlational analyses, none of the demographic variables (ie, gender, ethnicity, educational level, or income category) were found to be significantly related to the overall satisfaction with SLT services.
= 4.11, s = 0.45). In comparing participants’ satisfaction across different types of services (C-SLT, H-SLT, and SLTT)), no significant differences were found (F[2,67] = 0.02, p = 0.95). Mean values and standard deviations for different types of SLT services are specified in Table 2. Based on correlational analyses, none of the demographic variables (ie, gender, ethnicity, educational level, or income category) were found to be significantly related to the overall satisfaction with SLT services.
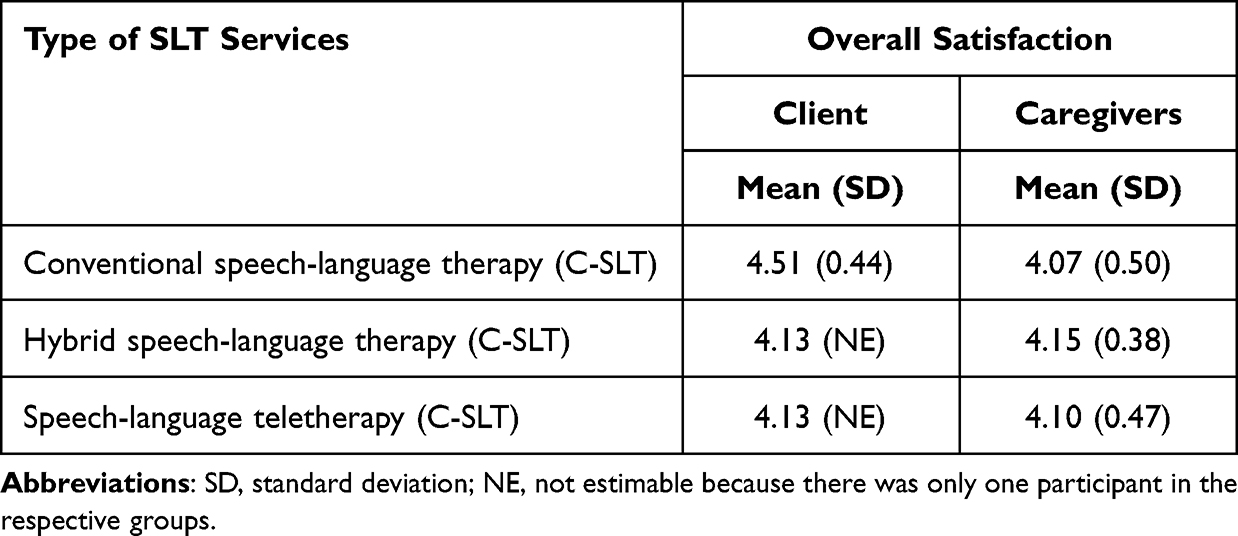 |
Table 2 Satisfaction Levels in Different Types of SLT Services |
Aspects of Teletherapy: Effects on Satisfaction Levels
Based on Section 3: Satisfaction in SLTT, participants who received H-SLT and SLTT as overall achieved an average satisfaction of 3.76 (s = 0.63]. There was no significant difference in satisfaction with teletherapy services, neither between the client ( = 4.00, s = 0.07) and caregiver groups (
= 4.00, s = 0.07) and caregiver groups ( = 3.75, s =0.65, t = 0.54 p = 0.59) nor between participants who were receiving H-SLT (
= 3.75, s =0.65, t = 0.54 p = 0.59) nor between participants who were receiving H-SLT ( = 3.70, s = 0.68) versus SLTT (
= 3.70, s = 0.68) versus SLTT ( = 3.91, s = 0.49, t = 0.90, p = 0.38). We found a significant correlation between the satisfaction level of participants in SLTT and their overall satisfaction with SLT services as measured in Section 2 (r = 0.53, p = 0.00). Overall satisfaction with SLT services was also found associated with all aspects of teletherapy (Table 3). As shown in Table 3, the mean value was highest for Item 2 (Teletherapy saves me time traveling to the clinic). The items with the lowest mean values was Item 19 (This teletherapy application clearly gave error messages and troubleshooting recommendations). In terms of factors related to participants’ satisfaction in teletherapy, income was found to be the only significant associated variable (r = 0.37, p = 0.04), where participants from the low-income category showed higher satisfaction in SLTT (
= 3.91, s = 0.49, t = 0.90, p = 0.38). We found a significant correlation between the satisfaction level of participants in SLTT and their overall satisfaction with SLT services as measured in Section 2 (r = 0.53, p = 0.00). Overall satisfaction with SLT services was also found associated with all aspects of teletherapy (Table 3). As shown in Table 3, the mean value was highest for Item 2 (Teletherapy saves me time traveling to the clinic). The items with the lowest mean values was Item 19 (This teletherapy application clearly gave error messages and troubleshooting recommendations). In terms of factors related to participants’ satisfaction in teletherapy, income was found to be the only significant associated variable (r = 0.37, p = 0.04), where participants from the low-income category showed higher satisfaction in SLTT ( =4.08, s = 0.60), as compared to those in the middle-income category (
=4.08, s = 0.60), as compared to those in the middle-income category ( = 3.63, s = 0.57) and the high-income category (
= 3.63, s = 0.57) and the high-income category ( = 2.76), the standard deviation was non-estimable because only one participant fit this category).
= 2.76), the standard deviation was non-estimable because only one participant fit this category).
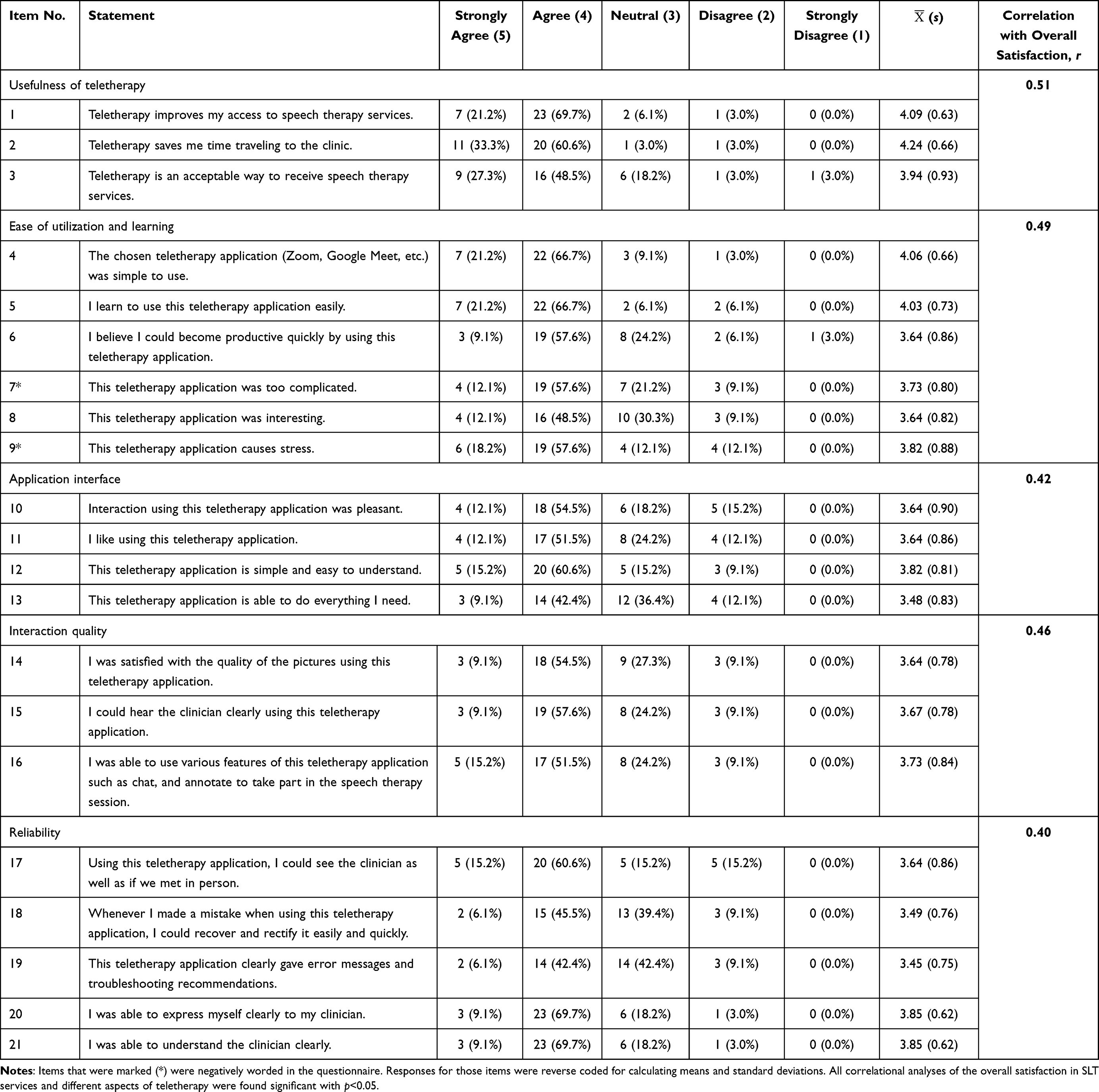 |
Table 3 Aspect of Satisfaction in Speech-Language Teletherapy |
Discussion
In addressing the study objectives, we found a lack of statistically significant differences in the satisfaction of clients and caregivers who received SLT services via different modes of service delivery (C-SLT, H-SLT, and SLTT) and a lack of differences in the level of satisfaction in teletherapy between H-SLT and SLTT groups. This may indicate that the participants were similarly satisfied with the services provided at the university clinic, regardless of the methods used for delivering SLT treatments. Similar satisfaction levels among the clients and caregivers may be due to positive treatment outcomes that were experienced by the service recipients. Regardless of service delivery modes, the needs and expectations of service recipients may have been adequately addressed. For example, Fridler et al17 found that home-based SLTT can produce comparable outcomes as compared to therapy provided in a clinical setting. This may indicate that telerehabilitation is a viable and dependable option for service delivery, and conventional, face-to-face healthcare services can readily be adapted to an online format to a certain extent.9
A high satisfaction level in teletherapy in the present study may be due to the service providers’ effort to ensure that all aspects of teletherapy were addressed. As described by Ahmad Rusli et al,21 teleservices at the university clinic where the current study was conducted were developed in multiple phases. After each trial phase, modifications of service delivery, clinical training and supervision, and administrative systems were made to further improve the online SLT services. However, it is important to note certain persisting limitations of telepractices. In the present study, participants continued to indicate lower satisfaction in a few teletherapy aspects, such as a lack of flexibility in troubleshooting problems and rectifying errors. Participants also indicated lower agreement with the statement that they can do everything with teletherapy. The hybrid mode, where clients and caregivers receive conventional therapy and teleservices alternatingly may be an option to encourage the strength of convention and teletherapy while minimizing the limitations of both service delivery options.22
The present study demonstrated a lack of influence of demographic factors, such as age, gender, education level, and income category on the overall satisfaction with SLT services across the three different modes. In terms of participants’ satisfaction in teleservices, income levels were found to influence the satisfaction level. In the present study, individuals with lower income showed higher satisfaction in teleservices as compared to those with higher income. Despite research evidence that demonstrated the effects of sociodemographic factors on patients’ satisfaction, such studies were lacking for delivery of SLT through virtual mode. Although there was an increase in the number of studies on the effectiveness of SLTT in managing a variety of disorders, Shahouzaie and Gholamiyan Arefi reported that less than 10 studies focused on patients’ satisfaction in virtual SLT services.23 None of those studies compared patients’ satisfaction between conventional SLT versus teletherapy services. Tenforde et al only associated patients’ satisfaction in SLTT with the ages of their participants and found no significant relationship.16 The present study provided a novel insight to the relationship between income and level of satisfaction in SLTT.
It is crucial to note several limitations of the present study. In this study, we did not measure or attempt to associate the satisfaction level with treatment effects. Therefore, we are unable to elucidate the suitability of SLT treatments according to service delivery modes. In addition, this study was conducted only in one clinic in Kuala Lumpur that primarily serves as a teaching facility. Satisfaction of clients and caregivers may be influenced by clinicians’ experience in providing teleservices and organizations where services were provided, including hospitals, nursing homes, rehabilitation centers, or personal homes.24 These limitations may direct the direction of similar studies in the future.
Conclusion
The present study demonstrated that the speech-language therapy services via three modes of delivery were well received by clients and caregivers. The satisfaction level was not influenced by the modes of service delivery. A similar satisfaction level was found following SLT services provided via conventional, hybrid, and virtual modes. Any of these modes may be adequate to meet the needs and expectations of SLT recipients. In addition, general satisfaction with SLT services is not influenced by sociodemographic factors. However, income level contributed to the satisfaction in SLT services that were delivered virtually. Teletherapy may serve as a viable alternative for clients to receive speech-language intervention alongside the conventional, face-to-face services that have always been considered a gold standard in the field of speech-language therapy. The application of teletherapy may also address some barriers that are associated with access to SLT services, such as distance between clients’ homes and clinics or hospitals, cost and time for traveling, and logistical challenges related to the mobility of people with disabilities. Government and non-government organizations and agencies should consider expanding their services to include teletherapy as an option to address those barriers.
Acknowledgments
We thank Prof. Dr. Poh Bee Koon, Dr. Shobha Sharma, and Dr. Badrulzaman Abdul Hamid for their suggestions for improving the quality of this manuscript. We extend our appreciation to the Faculty of Health Sciences and the Speech Sciences Program of Universiti Kebangsaan Malaysia for their support. We are grateful for the involvement of all participants in the study.
Funding
The authors did not receive any funding or grant for this project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Naunheim MR, Xu L, Zhou G, Agarwala A. Patient satisfaction with otolaryngology care: stratification by race, age, gender, income, and language. Otorynolaryngol Head Neck Surg. 2022;166:1055–1061. doi:10.1177/01945998221076797
2. Ariffin AA, Aziz NA, Zain NM, Menon BV. Antecedents and consequences of patient satisfaction in the context of private hospitalization services. WSEAS Trans Bus Econ. 2022;19:259–268. doi:10.37394/23207.2022.19.24
3. De Silva A. A framework for measuring responsiveness. Geneva: World Health Organization; 2000.
4. Sitzia J, Wood N. Patient satisfaction: a review of issues and concepts. Soc Sci Med. 1997;45:1829–1843. doi:10.1016/S0277-9536(97)00128-7.
5. Afrashtehfar KI, Assery MKA, Bryant SR. Patient satisfaction in medicine and dentistry. Int J Dent. 2020;6621848. doi:10.1155/2020/6621848
6. Ai Y, Rahman MK, Newaz MS, et al. Determinants of patients’ satisfaction and trust toward healthcare service environment in general practice clinics. Front Psychol. 2022;13:856750. doi:10.3389/fpsyg.2022.856750
7. Frizelle P, Ceroni A, Bateman L. Speech and language therapy services for people with down syndrome: the disparity between research and practice. J Policy Pract Intellect Disabil. 2021;19:171–182. doi:10.1111/jppi.12405
8. Eslami Jahromi M, Ahmadian L, Bahaadinbeigy K. The effect of tele-speech therapy on treatment of stuttering. Disabil Rehabil Assist Technol. 2022;17:34–39.
9. Chaudhary T, Kanodia A, Verma H, et al. A pilot study comparing teletherapy with the conventional face-to-face therapy for speech-language disorders. Indian J Otolaryngol Head Neck Surg. 2021;73:366–370. doi:10.1007/s12070-021-02647-0
10. Eslami Jahromi M, Farokhzadian J, Ahmadian L. Two-sided perspective on tele-speech therapy: experiences of stuttering patients, and their parents. Assist. Technol. 2021;24:1–8. doi:10.1080/10400435.2021.1937378
11. Lam JHY, Lee SMK, Tong X. Parents’ and students’ perceptions of telepractice services for speech-language therapy during the COVID-19 pandemic: survey study. JMIR Pediatr Parent. 2021;4:e25675. doi:10.2196/25675
12. Quinn R, Park S, Theodoros D, Hill AJ. Delivering group speech maintenance therapy via telerehabilitation to people with Parkinson’s disease: a pilot study. Int J Speech Lang Pathol. 2019;21:385–394. doi:10.1080/17549507.2018.1476918
13. Molini-Avejonas DR, Rondon-Melo S, De La Higuera Amato CA, Samelli AG. A systematic review of the use of telehealth in speech, language and hearing sciences. J Telemed Telecare. 2015;21:367–376. doi:10.1177/1357633X15583215
14. Camden C, Silva M. Pediatric telehealth: opportunities created by the COVID-19 and suggestions to sustain its use to support families of children with disabilities. Phys Occup Ther Pediatr. 2021;41:1–17. doi:10.1080/01942638.2020.1825032
15. Campbell DR, Goldstein H. Evolution of telehealth technology, evaluations, and therapy: effects of the COVID-19 pandemic on pediatric speech-language pathology services. Am J Speech Lang Pathol. 2022;31:271–286. doi:10.1044/2021_AJSLP-21-00069
16. Tenforde AS, Borgstrom H, Polich G, et al. Outpatient physical, occupational, and speech therapy synchronous telemedicine: a survey study of patient satisfaction with virtual visits during the COVID-19 pandemic. Am J Phys Med Rehabil. 2020;99:977–981. doi:10.1097/PHM.0000000000001571
17. Fridler N, Rosen K, Menahemi-Falkov M, Herzberg O, et al. Tele-rehabilitation therapy vs. face-to-face therapy for aphasic patients.
18. Meersman T, Mathieson K. Examining factors affecting parental satisfaction with speech therapy in children with Phelan-McDermid syndrome. Int J Dev Disab. 2020;66:304–316. doi:10.1080/20473869.2019.1582906
19. Parmanto B, Lewis AN, Kristin M, Bertolet MH. Development of Telehealth Usability Questionnaire (TUQ). Int J Telerehabil. 2016;8:3–10.
20. Sharma S, Ward EC, Burns C, Theodoros D, Russell T. Assessing dysphagia via telerehabilitation: patient perceptions and satisfaction. Int J Speech Lang Pathol. 2013;15:176–183. doi:10.3109/17549507.2012.689333
21. Ahmad Rusli Y, Hassan FH, Haris SM, Mohd Azraai H, Md Almi SN. We’re making it work! UKM’s Speech Sciences Program’s teleclinic experience in the time of COVID-19. Med J Malays. 2021;76:52–54.
22. Joginder Singh S, Kamarudin K. The implementation of telepractice by Malaysian speech-language pathologists during the COVID-19 pandemic. Commun Sci Disord. 2022;27(1):239–250. doi: 10.12963/csd.21848
23. Shahouzaie N, Gholamiyan Arefi M. Telehealth in speech and language therapy during the COVID-19 pandemic: a systematic review. Disabil Rehabil Assist Technol. 2022;20:1–8. doi: 10.1080/17483107.2022.2122605
24. Mani S, Sharma S, Singh DK. Concurrent validity and reliability of telerehabilitation-based physiotherapy assessment of cervical spine in adults with non-specific neck pain. J Telemed Telecare. 2021;27(2):88–97.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.