")
Back to Journals » Clinical Ophthalmology » Volume 15
Comparison of the Visual Outcomes of an Extended Depth-of-Focus Lens and a Trifocal Lens
Authors Moshirfar M, Ellis J, Beesley D , McCabe SE , Lewis A, West Jnr WB , Ronquillo Y , Hoopes Snr P
Received 25 May 2021
Accepted for publication 7 July 2021
Published 16 July 2021 Volume 2021:15 Pages 3051—3063
DOI https://doi.org/10.2147/OPTH.S321779
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Majid Moshirfar,1– 3 James Ellis,4 Daniel Beesley,5 Shannon E McCabe,1,6 Adam Lewis,7 William B West Jnr,4 Yasmyne Ronquillo,1 Phillip Hoopes Snr1
1Hoopes Vision Research Center, Hoopes Vision, Draper, UT, USA; 2John A. Moran Eye Center, Department of Ophthalmology and Visual Sciences, University of Utah, Salt Lake City, UT, USA; 3Utah Lions Eye Bank, Murray, UT, USA; 4University of Utah School of Medicine, Salt Lake City, UT, USA; 5Brigham Young University, Provo, UT, USA; 6Mission Hills Eye Center, Pleasant Hill, CA, USA; 7Kansas City University College of Osteopathic Medicine, Kansas City, MO, USA
Correspondence: Majid Moshirfar
Hoopes Vision Research Center, Hoopes Vision, Draper, UT, USA
Tel +1 801-568-0200
Fax +1 801-563-0200
Email [email protected]
Purpose: To compare the visual performance of the AcrySof IQ PanOptix trifocal intraocular lens and the TECNIS Symfony extended depth-of-focus lens at near and distance visual ranges.
Methods: A total of 146 patients (221 eyes) who underwent phacoemulsification and cataract extraction and received either a PanOptix or Symfony lens from January 2019 to July 2020 were included in the study (83 PanOptix non-toric, 30 PanOptix toric, 70 Symfony non-toric, and 38 Symfony toric). Uncorrected distance (UDVA), uncorrected near (UNVA), and corrected distance (CDVA) visual acuity were assessed at one-day, one-month, and three-months postoperatively. Averages of UDVA, UNVA, and CDVA were taken to evaluate which lens was superior at near and distance visual ranges. Secondary outcome measures including glare, halo, dryness, and problems with night vision were documented at each postoperative visit.
Results: At one month postoperatively, the average UNVA was 0.16 ± 0.14 logMAR in the PanOptix group and 0.21 ± 0.14 logMAR in the Symfony group (P=0.007); the average UDVA for the PanOptix group was 0.09 ± 0.13 logMAR compared to the Symfony group at 0.10 ± 0.14 logMAR (P=0.67); and the average CDVA was 0.02 ± 0.05 logMAR in the PanOptix group and 0.00 ± 0.04 logMAR in the Symfony group (P=0.11). At three months postoperatively, there were no statistically significant differences in UNVA, UDVA, or CDVA between the two groups (P=0.18, 0.79, 0.68 respectively). There was no statistically significant difference in secondary outcome measures at one- and three-months (P=0.49, 0.10 respectively).
Conclusion: The AcrySof IQ PanOptix trifocal intraocular lens appears to afford better UNVA compared to the TECNIS Symfony extended depth-of-focus intraocular lens at one-month postoperatively, though this difference was not seen at three months postoperatively. There is no statistically significant difference in UDVA and CDVA between the two groups at postoperative day one, one-month, and three-months.
Keywords: visual acuity, intraocular lens, trifocal lens, extended depth-of-focus lens
Introduction
Cataracts are the largest single contributor to reversible blindness worldwide, and cataract surgery is the only medically accepted method for treatment, making it one of the most commonly performed surgeries worldwide.1–3 In the past, most cataract surgeries involved implanting monofocal spherical intraocular lenses (IOLs), which have a single focal point. These resulted in good outcomes for either near or distance vision, depending on targeted distance, but with poor visual outcomes at intermediate visual distances and the non-targeted visual distance (near or far), leading to spectacle or contact lens dependence.4
Recently, alternatives to the monofocal IOLs have been developed to overcome the poor visual outcomes at non-targeted distances associated with a single focal point IOL.5 These alternatives include multifocal and extended depth-of-focus lenses. Multifocal and extended depth-of-focus IOLs contain rings inside the lens that allow for adequate focusing of light at near, intermediate, and distance zones. Studies performed on the effectiveness of multifocal IOLs suggest that patients who receive multifocal lenses have better uncorrected near vision, improved overall quality of vision, and increased spectacle independence than those who receive the monofocal IOLs.6,7 The defocus curve for conventional monofocal lenses shows optimal vision at a single point of focus, whereas multifocal and extended depth-of-focus lenses have defocus curves with high acuity across near, intermediate, and distance.8,9
The AcrySof IQ PanOptix Model trifocal IOL (henceforth referred to as PanOptix) was launched in 2015 by Alcon Laboratories (Fort Worth, Texas). The PanOptix IOL is made out of acrylate/methacrylate copolymer with 2 open-loop haptics. It uses a quadrifocal design with an inner diffractive zone, an outer refractive zone, and a central biconvex optic.10 The diffractive zone is non-apodized and allows for optimal light utilization across a wide spectrum of lighting conditions.10 The quadrifocal optic design includes three diffraction orders for near, intermediate, and distance, as well as an additional fourth order to improve acuity at distance.7 The spherical posterior lens surface and aspheric anterior lens surface divide the incoming light and create an intermediate power addition of +2.17 diopter (D) and near of +3.25 diopter (D). The PanOptix IOL, with its multiple focal points, is expected to provide superior overall visual outcomes at near and intermediate measures compared to the extended depth-of-focus IOLs.7
In 2016, the US approved the TECNIS Symfony extended depth-of-focus (EDOF) IOL (henceforth referred to as Symfony) made by Abbott Medical Optics (Santa Ana, California). This Symfony lens has an achromatic diffractive surface designed to improve the range of vision from distance through intermediate. The Symfony lens is a UV-blocking single piece hydrophobic-acrylic EDOF IOL that is biconvex with a +1.75 diopter (D) intermediate addition.10 While the design affords benefits in both near and distance vision, it is presumed that it may be inferior at near vision compared to the PanOptix.10 The Symfony lens increases acuity at near and distance, but compared to a multifocal IOL, the defocus curves demonstrate that PanOptix patients have significantly better near outcomes, with comparable acuity to Symfony patients at distance and intermediate vision.7,10
With the growing variety of commercially available IOL types and manufacturers, there is a need to obtain clinical data comparing them. The purpose of this study was to compare the effectiveness of the PanOptix and Symfony IOLs in primary and secondary visual outcomes in order to determine whether or not one lens provided superior outcomes over the other.
Materials and Methods
A retrospective comparative study was performed using patient data from a tertiary refractive surgical center. Data was collected from 146 patients (221 eyes) who underwent phacoemulsification cataract extraction with implantation of a PanOptix or Symfony intraocular lens between January 1st, 2019 and July 1st, 2020. Exclusion criteria included patients with congenital ocular abnormalities, use of ocular medications that may affect vision, previous retinal disease, glaucoma, previous corneal disease, history of trauma to the eye, previous cerebrovascular accidents affecting vision, perioperative or postoperative complications, degenerative eye disorders, and previous refractive surgery. This study was approved by the Hoopes Vision Ethics Committee and adhered to the tenets of the Declaration of Helsinki. This retrospective study involving de-identified data was approved by the Biomedical Research Alliance of New York (BRANY, Lake Success, NY). (# A20-12-547-823)
This study analyzed primary and secondary visual outcomes among treatment groups. The primary outcomes included the following: postoperative mean refractive spherical equivalent (MRSE), mean refractive cylinder (MRC), uncorrected near visual acuity (UNVA), uncorrected distance visual acuity (UDVA), and corrected distance visual acuity (CDVA). UNVA was measured at 40 cm on a Jaeger scale and converted to Snellen using a conversion chart. Primary outcome measures were documented at postoperative day one (POD1), one-month postoperatively, and three-months postoperatively. All Snellen units were converted to logMAR for statistical analysis and calculation of average visual acuity using a standard conversion formula.11 In the study, secondary outcomes included the following: glare, halo, dryness, and problems with night vision. Secondary outcome measures were reported by patients at one and three months postoperatively. Patients were divided into two study groups based on the type of IOL for the analysis of primary and secondary outcomes.
Summary descriptive statistics were calculated for all variables described above. For all continuous variables measured, statistical analysis was performed using one-way ANOVA F-test to determine unequal outcomes of variables and two-tailed hypothesis tests. A chi-square test was performed for all discrete variables. Statistical significance was evaluated and determined as a P value of less than 0.05.
Surgical Technique
After informed consent was obtained, cataract extraction procedures were done in the operating room under sterile conditions. A 2.4 mm temporal clear corneal incision was created with a keratome, and a 5.0–5.5 mm continuous curvilinear capsulorhexis was performed. Phacoemulsification was performed in a horizontal chop or divide-and-conquer fashion using the Infiniti Vision System (Alcon Laboratories, Inc. Fort Worth, Texas). All wounds were confirmed to be self-sealing, and no complications occurred. Patients were instructed to use third- or fourth-generation fluoroquinolone antibiotic eye drops four times daily for one month.
Patients were also started on a topical steroid medication four times daily and tapered weekly over one month.
Vector Analysis
Vector analysis was performed on all 68 eyes that had a toric IOL implanted. The indication for toric IOL placement was a total corneal astigmatism of greater than 0.8 D on preoperative measurements. Preoperative biometry measurements (flat keratometry, flat axis, steep keratometry, steep axis, aqueous chamber depth, axial length, lens thickness, and white-to-white) were performed before surgery using the Lenstar LS 900 (Haag Streit Switzerland). Incisional surgically induced astigmatism was 0.1 D for each patient. Incision location and IOL power were included in the data for analysis. Postoperative refraction was collected from patient charts at their one-month postoperative visit. Predicted postoperative refraction was obtained through the Barrett Toric Calculator provided by the American Society of Cataract and Refractive Surgery for both Symfony and PanOptix patients with a target of emmetropia. The Panoptix IOL power was chosen by selecting the lens predicted to yield a postoperative spherical equivalent of 0 to +0.25 D per the manufacturer recommendation. The Symfony IOL power was chosen by selecting the lens predicted to yield a postoperative spherical equivalent of −0.25 to 0 D per the manufacturer recommendation to optimize near vision. An A-constant of 119.1 was used for the PanOptix, and an A-constant of 119.17 was used for the Symfony.
All data required for the vector analysis was entered into the American Society of Cataract and Refractive Surgery astigmatism double-angle plot tool. Data was organized and presented according to the method proposed by Abulafia et al.12
Results
Patient Demographics
Data from 146 patients (221 eyes) were included in the study. Of those eyes, 83 received the PanOptix non-toric lens, 30 received the PanOptix toric lens, 70 received the Symfony non-toric lens, and 38 received the Symfony toric lens. The mean age at the time of surgery of the PanOptix and Symfony groups were 63.5 years ± 11.8 and 62.8 years ± 11.0, respectively. There was no statistically significant difference in preoperative biometry measures between groups, except in aqueous depth (P=0.03). (Table 1)
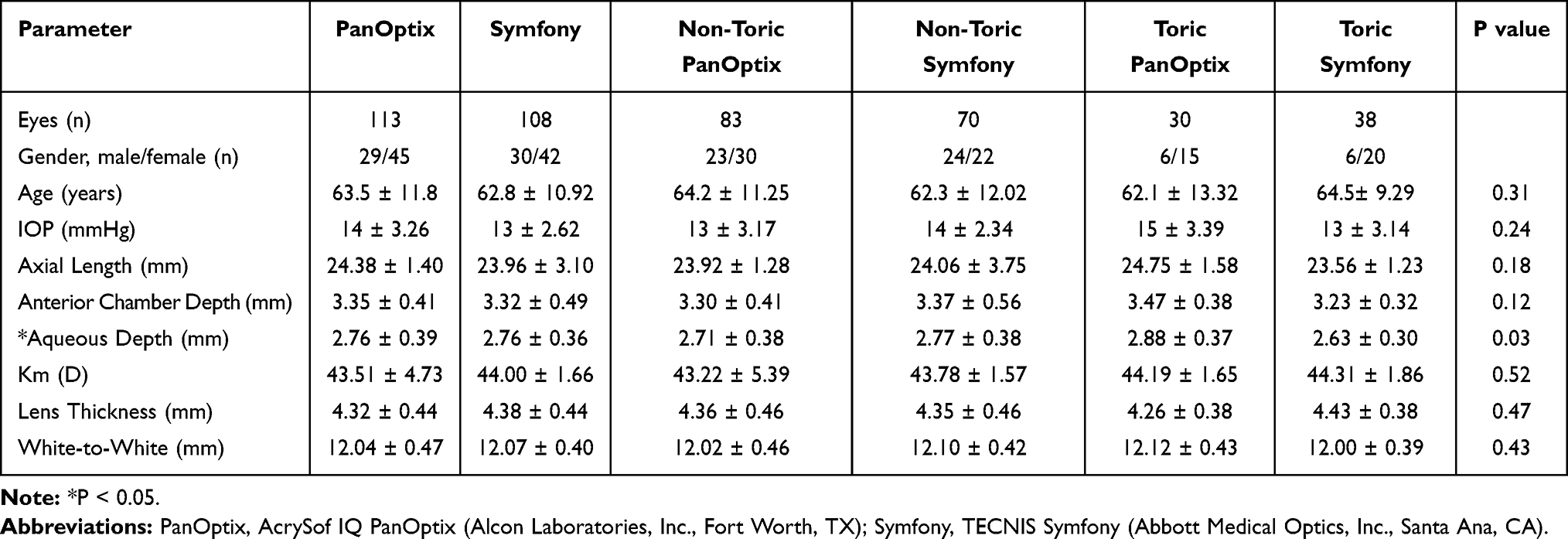 |
Table 1 Patient Demographics |
Visual Acuity Analysis
Refractive Outcomes
The manifest refractive spherical equivalent (MRSE) and manifest refractive cylinder (MRC) were collected at one-month postoperatively. The MRSE in the PanOptix group was −0.03 ± 0.39 D, 95% of individuals were within 0.50 D of target refraction. The MRSE in the Symfony group was −0.31 ± 0.50 D, 88% of individuals were within 0.50 D of target refraction. The difference in MRSE between the two groups was statistically significant (P<0.001). The MRC was −0.34 ± 0.33 D and −0.36 ± 0.40 D in the PanOptix and Symfony groups respectively. There was no statistically significant difference in MRC (P=0.61).
Uncorrected Near Visual Acuity
The UNVA was compared in both patient groups at POD1, one-month, and three-month visits. At POD1, the average UNVA was 0.32 ± 0.18 logMAR for the PanOptix group compared to 0.36 ± 0.24 logMAR for the Symfony group (P=0.16). At POD1, more patients achieved 20/20 or better in the PanOptix group (2%) compared to the Symfony group (1%) (Figure 1A). At one-month, the average UNVA was 0.16 ± 0.14 logMAR in the PanOptix group and 0.21 ± 0.14 logMAR in the Symfony group (P=0.007). More patients achieved 20/20 vision or better in the PanOptix group (19%) compared to the Symfony group (7%) (Figure 1B). At three-months, the average UNVA was 0.16 ± 0.12 logMAR in the PanOptix group compared to 0.21 ± 0.17 logMAR in the Symfony group (P=0.18). More eyes achieved 20/20 vision or better in the PanOptix group (23%) compared to the Symfony group (14%) (Figure 1C). The only statistically significant difference between the two groups for UNVA was at one month, which showed that the Panoptix group had superior near vision.
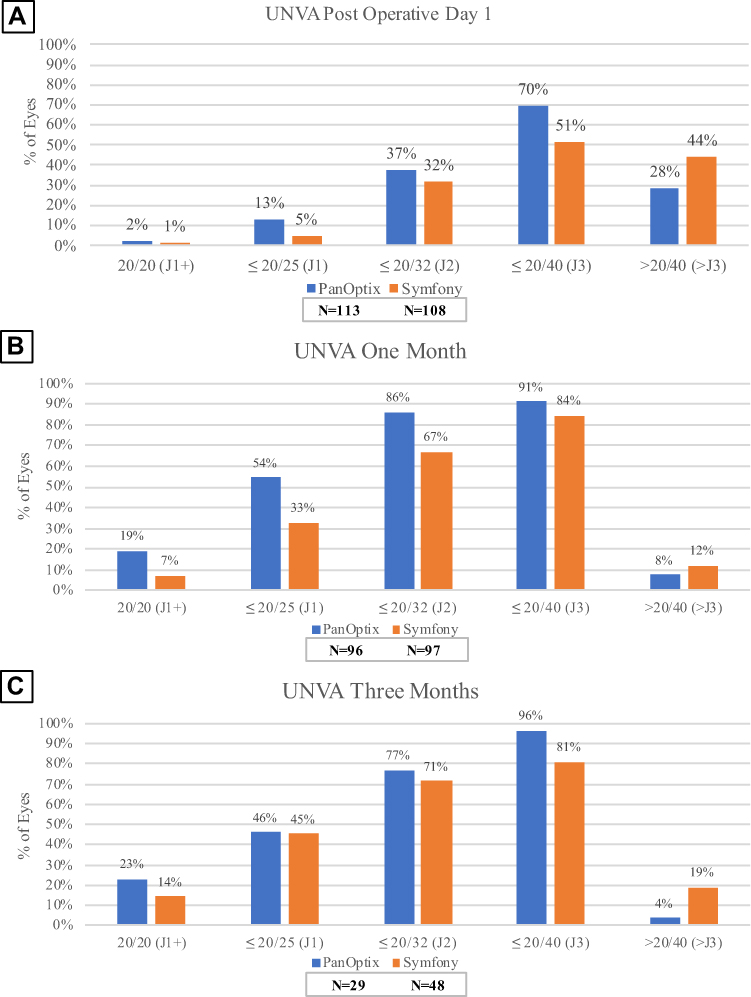 |
Figure 1 Distribution of uncorrected near visual acuity at postoperative day one (A), one-month (B), and three-months (C) in the AcrySof IQ PanOptix and TECNIS Symfony groups. |
Uncorrected Distance Visual Acuity
The UDVA was compared in both patient groups at POD1, one-month, and three-month visits. At POD1, the average UDVA for the PanOptix and Symfony groups were 0.20 ± 0.20 logMAR and 0.15 ± 0.16 logMAR, respectively (P=0.07). At POD1, fewer eyes achieved 20/20 vision or better in the PanOptix group (25%) compared to the Symfony group (31%) (Figure 2A). At one-month, the average UDVA for the PanOptix group was 0.09 ± 0.13 logMAR compared to the Symfony group at 0.10 ± 0.14 logMAR (P=0.67). More eyes achieved 20/20 vision or better in the PanOptix group (50%) than the Symfony group (48%) at one-month (Figure 2B). At three-months, the average UDVA for the PanOptix group was 0.12 ± 0.09 logMAR compared to 0.13 ± 0.17 logMAR in the Symfony group (P=0.79). At three-months, fewer eyes achieved 20/20 in the PanOptix group (21%) than the Symfony group (44%) (Figure 2C). There were no statistically significant differences in UDVA between the two groups.
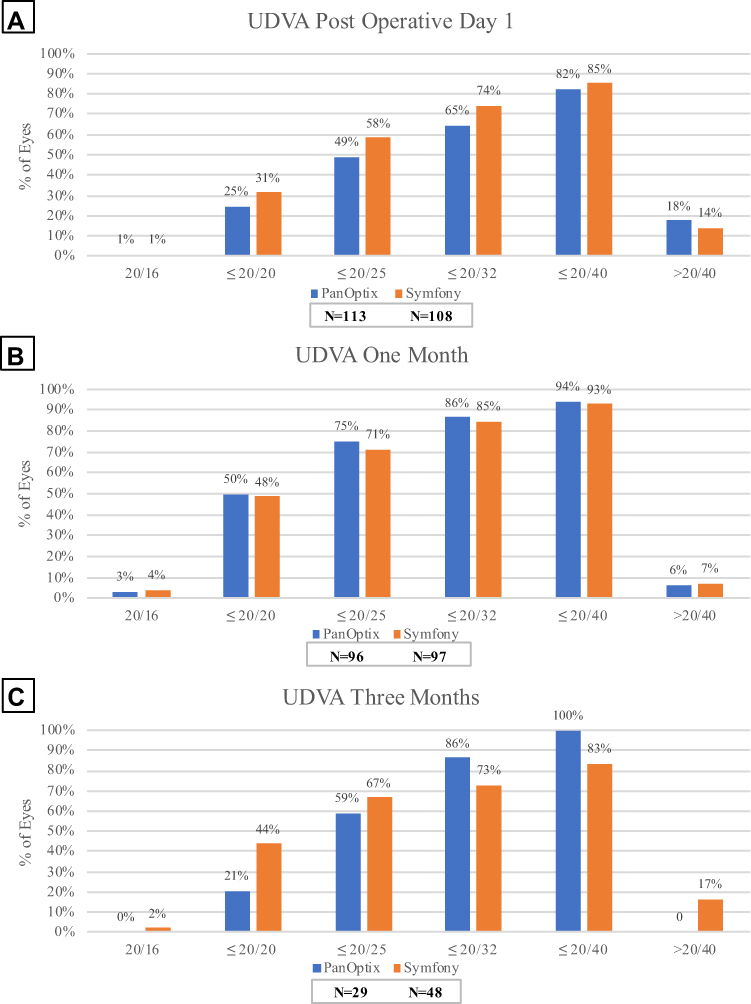 |
Figure 2 Distribution of uncorrected distal visual acuity at postoperative day one (A), one-month (B), and three-months (C) in the AcrySof IQ PanOptix and TECNIS Symfony groups. |
Corrected Distance Visual Acuity
The CDVA was compared in both patient groups at one-month and three-month visits. At one-month, the average CDVA was 0.02 ± 0.05 logMAR in the PanOptix group and 0.00 ± 0.04 logMAR in the Symfony group (P=0.11). Fewer patients achieved 20/20 vision or better in the PanOptix group (81%) compared to the Symfony group (92%) (Figure 3A). At three-months, the average CDVA was 0.02 ± 0.06 logMAR in the PanOptix group compared to 0.02 ± 0.05 logMAR in the Symfony group (P=0.68). More eyes achieved 20/20 vision or better in the PanOptix group (84%) compared to the Symfony group (83%) (Figure 3B). There were no statistically significant differences in CDVA between the two groups.
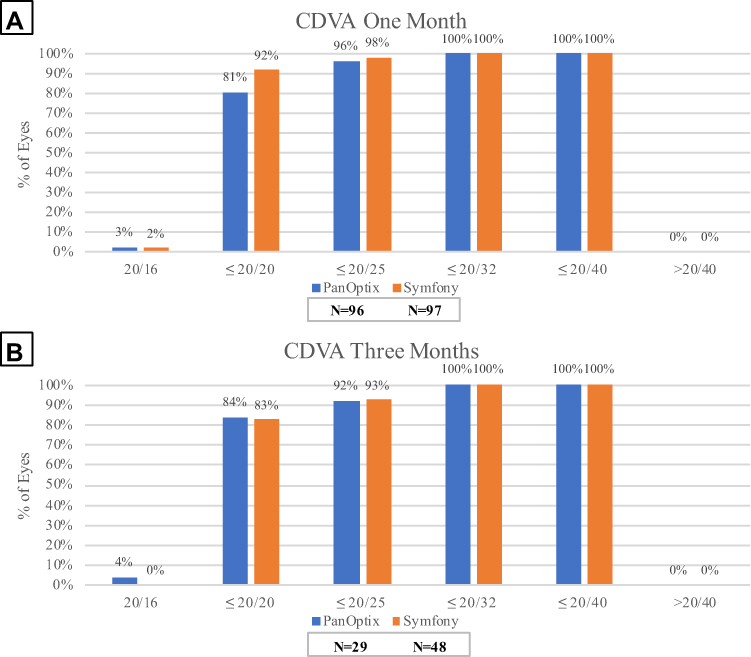 |
Figure 3 Distribution of corrected distal visual acuity at one-month (A) and three-months (B) in the AcrySof IQ PanOptix and TECNIS Symfony groups. |
Subjective Measures
Secondary outcome measurements for glare, halo, and photophobia were reported in less than 9% of eyes at their one-month visit and in less than 5% at their three-month postoperative visit in both the PanOptix and Symfony groups (P=0.49, 0.10 respectively). Dryness was reported in 14% and 8% of eyes in the PanOptix group and 16% and 4% of eyes in the Symfony group at one- and three-months, respectively (P=0.89, 0.09). The Symfony group demonstrated a higher incidence of night vision disturbance at one- and three-months compared to the PanOptix group (Figure 4A and B). There were no statistically significant differences in secondary outcome measures at one- and three-months.
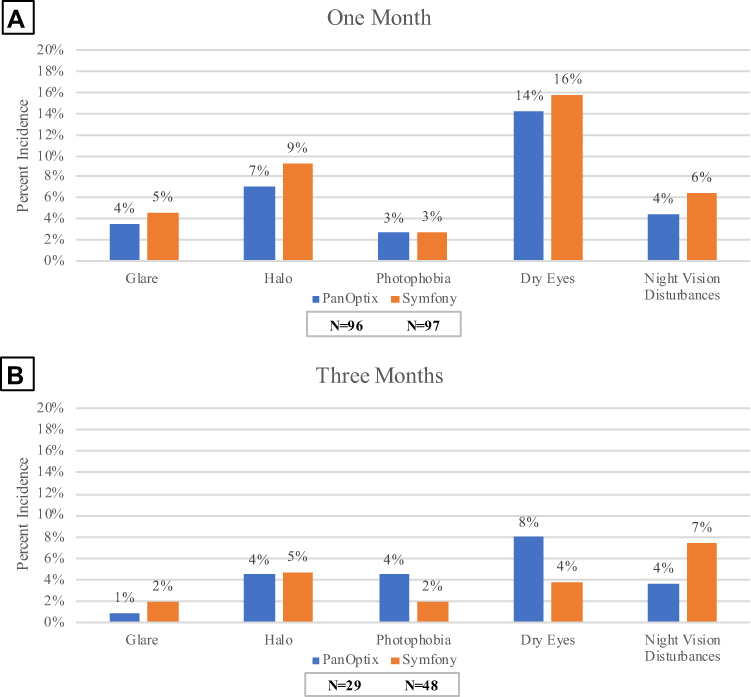 |
Figure 4 Distribution of secondary visual symptoms in the AcrySof IQ PanOptix and TECNIS Symfony groups at one-month (A) and three-months (B). |
Vector Analysis
The centroid represents the mean vector of astigmatism, and the ellipse represents one standard deviation around the centroid. Each ring on the graph represents 1.00 D. Figures 5A and 6A summarize preoperative and postoperative keratometric astigmatism in the PanOptix and Symfony groups, respectively.
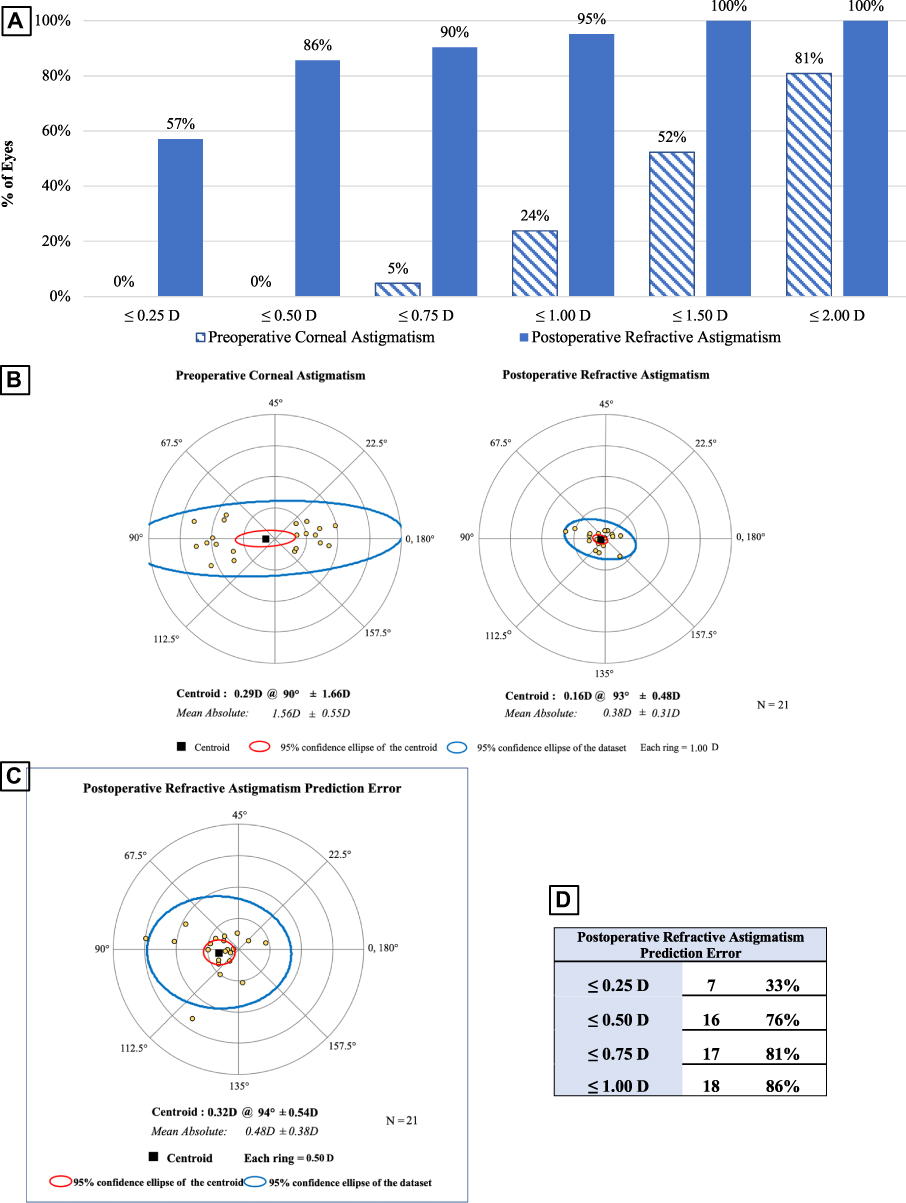 |
Figure 5 Vector analysis for the AcrySof IQ PanOptix group. (A) Cumulative histogram of the magnitude of the preoperative corneal astigmatism and postoperative refractive astigmatism. (B) Double-angle plots of the preoperative corneal astigmatism and postoperative refractive astigmatism. The centroid and standard deviation are shown. (C) Double-angle plot of postoperative refractive astigmatism prediction error. (D) Postoperative refractive astigmatism prediction error values. |
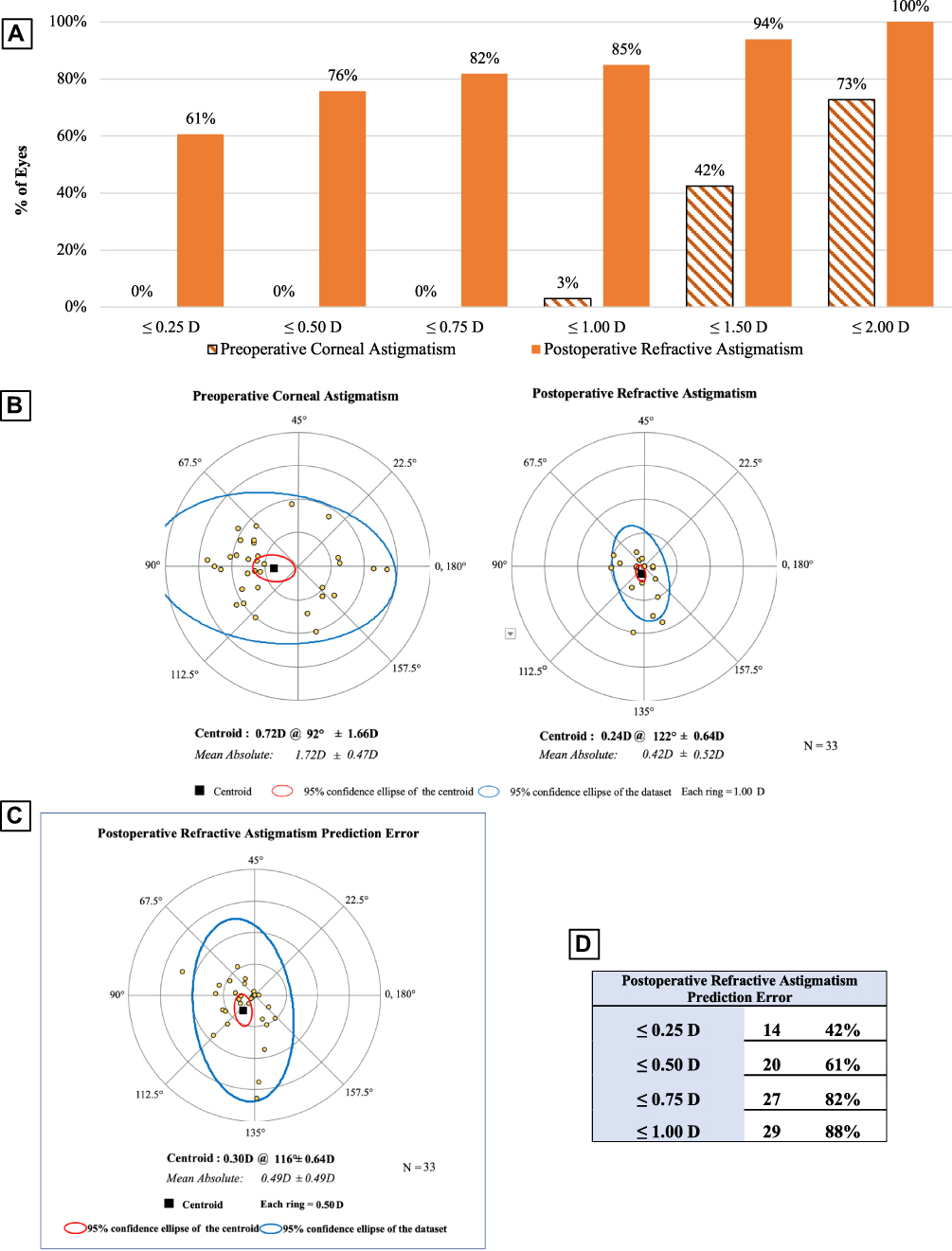 |
Figure 6 Vector analysis for the TECNIS Symfony group. (A) Cumulative histogram of the magnitude of the preoperative corneal astigmatism and postoperative refractive astigmatism. (B) Double-angle plots of the preoperative corneal astigmatism and postoperative refractive astigmatism. The centroid and standard deviation are shown. (C) Double-angle plot of postoperative refractive astigmatism prediction error. (D) Postoperative refractive astigmatism prediction error values. |
In the PanOptix group, the preoperative corneal astigmatism centroid was 0.29 D at 90 degrees ± 1.66 D. The centroid of postoperative refractive astigmatism was 0.16 D at 93 degrees ± 0.48 D (Figure 5B). The postoperative ellipse decreased in the postoperative corneal plane. These findings indicate an improvement in astigmatism following surgery.
In the Symfony group, the preoperative corneal astigmatism centroid was 0.72 D at 92 degrees ± 1.66 D. The centroid of postoperative refractive astigmatism was 0.24 D at 122 degrees ± 0.64 D (Figure 6B). The ellipse decreased from ~3.00 D to ~1.00 D in both the postoperative corneal spectacle plane and corneal plane, indicating an improvement in astigmatism following surgery.
In the PanOptix group, there was a predictive error ≤ 1.00 D in 86% of patients evaluated (Figure 5C and D). In the Symfony group, there was a predictive error ≤ 1.00 D in 88% of patients evaluated (Figure 6C and D). Data from the double-angle plot analysis for postoperative refractive astigmatism prediction error indicated effective prediction of the toric calculators used in both the PanOptix and Symfony groups.12
Discussion
Clinical outcomes following IOL surgery with the implantation of either a trifocal or an extended depth-of-focus IOL have historically produced superior results compared to the monofocal IOLs when considering overall visual outcomes.5 They have been shown repeatedly in the literature to produce improved visual outcomes at near without compromising distance vision. While monofocal lenses offer excellent results at their targeted distance, they have shown higher levels of spectacle dependence in patients due to poorer visual results at non-targeted distances. Both the PanOptix and Symfony IOLs offer satisfactory visual outcomes at both near and distance visual targets.
This study has the largest sample size of any study currently available in the literature that exclusively compares the PanOptix and Symfony IOLs. While other studies have compared multiple trifocal and EDOF IOLs, the total number of eyes studied that received either the PanOptix or the Symfony IOLs is larger than any other analysis currently found in the literature. The visual outcomes shown in this study demonstrated that in our cohort of 221 total eyes, those that received the PanOptix IOL had superior UNVA at one-month postoperatively compared to those that received a Symfony IOL. However, at three-months postoperatively, there was no statistically significant difference between the two groups (P=0.18). The postoperative MRSE was closer to emmetropia in the PanOptix patients compared to the Symfony group, with the Symfony group being slightly more myopic. The result of superior near vision in the PanOptix group is consistent with the conclusions of Cochener et al. Their study showed that in a group of 20 PanOptix patients compared to 20 Symfony patients, the PanOptix patients had superior UNVA at six months.13 Additional bench testing of the two lenses has consistently shown that the trifocal design produces superior near vision.7 Monaco et al demonstrated in their study of a small cohort of patients that even at earlier follow-up, patients that received the PanOptix lens had superior UNVA.8 The trifocal design of the PanOptix IOL should afford superior UNVA compared to the EDOF design of the Symfony IOL. The superior UNVA at one-month in the PanOptix group is consistent with predictions based upon the two designs. However, it is surprising that there was no statistically significant difference between the two groups at three-months in our study. A possible explanation for the lack of statistical significance in UNVA at three months is the decreased number of patient’s data collected at three-months follow-up compared to one month (Figure 1). It is also possible that the light-splitting design of the EDOF IOL requires greater time for retinal adjustment following implantation, explaining why there was a statistically significant difference between the PanOptix and Symfony groups at one-month and no statistically significant difference at three-months. The results were not anticipated and require additional follow-ups with patients for continued evaluation of UNVA beyond three months to identify any statistical differences between the two groups at later visits.
There was no statistically significant difference in UDVA between the two groups in our study at POD1, one-month, or three-months. Our results were consistent with the results of Farvardin et al and others.14,15 These outcomes reflect the theoretical benefits of the trifocal and extended depth-of-focus lenses, which both have a design meant to maintain distance vision.6,7 While a study by Escandon-Garcia concluded that the Symfony IOL produced superior outcomes for distance vision compared to their PanOptix group, it is important to note their limited sample size.16 Both the PanOptix and Symfony IOLs produce superior overall visual outcomes compared to the traditional monofocal IOLs, which have been shown to provide good visual acuity at their chosen distance but inferior overall visual outcomes comparatively.17 However, neither lens appears superior to the other when considering distance vision. Additionally, there were no statistically significant differences when comparing CDVA between the two IOL groups. The similarities in outcomes between UNVA, UDVA, and CDVA in our study can be reasonably explained by the different designs of the two lenses.
An issue that has been repeatedly reported in the literature regarding trifocal IOLs and EDOF IOLs is the increased incidence of photic phenomena compared to the traditional monofocal IOLs.18 Although both the trifocal and EDOF IOLs demonstrate increased photic phenomena, our data suggest that there is a difference in the frequency of patients experiencing visual phenomena between the two groups. While the incidence of visual phenomena was still low in both groups, we saw that at one-month, the Symfony group had a slightly higher frequency of patients complaining of halo and glare. At three-months, the percentage of patients experiencing glare or halo was nearly identical in both groups. In both the Symfony and PanOptix groups, fewer patients reported photic phenomena at three-months compared to one-month. This result is likely due to the recognized phenomenon of neuroadaptation, where patients adjust to retinal images within a particular period following IOL placement.19 However, neuroadaptation is a variable process that depends on the individual patient and may not be easily predicted.20 Previous studies have also shown that the designs of the two lenses are likely to produce a difference in the number of patients experiencing visual phenomena such as glare and halo.4,13,21 While trifocal and extended depth-of-focus IOLs tend to result in increased visual phenomena due to the transitions between the multiple foci compared to monofocal IOLs, our data did not show a statistically significant difference between the two groups at one- and three-months (P=0.49, 0.10 respectively).4 With the incidence of photic phenomena at three-months being low in both the PanOptix and Symfony groups, it is possible that with a larger sample size, a statistically significant difference could be seen between the two cohorts.
Visual outcomes in toric IOLs can be significantly affected by misalignment of the lens, which can result from preoperative target axis selection error, surgical misalignment, or postoperative rotation of the IOL. Malrotation of the toric IOL can negate the astigmatism correcting effect of the lens. It has been shown that for every ten degrees of toric IOL misalignment, one-third of the astigmatism-reducing effect is lost.22 In the event of residual postoperative astigmatism, surgical lens repositioning has been proven to be an effective technique for correction. The surgical repositioning rate of single-piece hydrophobic acrylic IOLs, like the Symfony lens, has been reported to be between 1–3%.23–25 Literature values for average Symfony postoperative lens rotation showed a mean toric IOL rotation of 4.49 ± 6.70 degrees.26 The literature is lacking current data describing the average postoperative toric IOL rotation or incidence of surgical repositioning in eyes that have had the PanOptix toric IOL implanted. However, studies on the AcrySof IQ ReSTOR Toric IOL (ReSTOR), which has a similar structure to the PanOptix IOL, have shown good rotational stability. Recent studies have demonstrated that at 30 days following surgery that the ReSTOR toric IOL had a mean rotation of 2.78 ± 5.83 degrees.27 While the ReSTOR toric IOL is not an exact representation of the PanOptix lens, the similar structure and design provide valuable information for comparison. In our study, there were no patients that required surgical repositioning in either the PanOptix or Symfony group. Based upon visual outcomes, vector analysis, and lack of eyes requiring surgical IOL repositioning, both IOLs appear to have demonstrated high rotational stability. Further investigation is needed in order to better compare the rotational stability of the Symfony or PanOptix toric IOLs and to identify advantages between the two IOLs in patients with astigmatism.
The limitations of this study include the retrospective collection of data. Additionally, although our sample size was significantly larger than other studies currently available in the literature, the limited sample size may increase the probability of obtaining results with a type I or II error. Additionally, an analysis of intermediate visual acuity was not included in the study, which has been shown to be different between PanOptix and Symfony groups in prospective studies.
Conclusion
Both the PanOptix and Symfony IOLs have been shown to provide satisfactory results in near and distance vision. The PanOptix demonstrates an initial superiority at near distances, but after three-months, the two IOLs have similar outcomes. While both IOLs have good visual outcomes with both near and far distances, it is important to counsel patients before surgery about the possible incidence of visual phenomena, including glare and halo. Although the lenses have different designs and different targeted spherical equivalents, they appear to be equally beneficial for patients who desire to preserve both near and distance vision without glasses (and intermediate distance from the literature, but this was not measured in our study).
Abbreviations
IOLs, intraocular lenses; EDOF, extended depth-of-focus; D, diopter; UNVA, uncorrected near visual acuity; UDVA, uncorrected distance visual acuity; CDVA, corrected distance visual acuity; POD1, postoperative day one; MRSE, mean refractive spherical equivalent; MRC, mean refractive cylinder.
Ethics Approval and Informed Consent
All patients were fully informed and consented to treatment. All methods and procedures followed the tenets of the Declaration of Helsinki and were approved by the Hoopes Vision Research Review Board. Biomedical Research Alliance of New York (Brany) Institutional Review Board (New York) approved this study.
Consent for Publication
We have not included any images, videos, recordings, etcetera requiring consent.
Consent
This retrospective study using de-identified data has been approved by the Hoopes Vision Ethics Board and BRANY IRB #20-12-547-823 (New York). The study conforms with the Helsinki Declaration of 1964, as revised in 2013, concerning human and animal rights. The patients signed informed consent.
Acknowledgments
Special thanks to Michael Bradley, MD, Benjamin Buckner, MD, and Phillip Hoopes Jr., MD for their assistance with surgical procedures, data acquisition, and management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by an unrestricted grant from Research to Prevent Blindness (RPB), 360 Lexington Avenue, 22nd Floor New York, NY 10017. No support was received for the publication of this article.
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Davis G. The evolution of cataract surgery. Mo Med. 2016;113(1):58–62. doi:10.1097/apo.0b013e31829df4bf
2. Rao GN, Khanna R, Payal A. The global burden of cataract. Curr Opin Ophthalmol. 2011;22(1):4–9. doi:10.1097/ICU.0b013e3283414fc8
3. Petrash JM. Aging and age-related diseases of the ocular lens and vitreous body. Investig Ophthalmol Vis Sci. 2013;54(14):ORSF54. doi:10.1167/iovs.13-12940
4. Khandelwal SS, Jun JJ, Mak S, Booth MS, Shekelle PG. Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis. Graefe’s Arch Clin Exp Ophthalmol. 2019;257(5):863–875. doi:10.1007/s00417-018-04218-6
5. de Medeiros AL, de Araújo Rolim AG, Motta AFP, et al. Comparison of visual outcomes after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of an extended depth of focus intraocular lens with a diffractive bifocal intraocular lens. Clin Ophthalmol. 2017;11:1911–1916. doi:10.2147/OPTH.S145945
6. Lee S, Choi M, Xu Z, Zhao Z, Alexander E, Liu Y. Optical bench performance of a novel trifocal intraocular lens compared with a multifocal intraocular lens. Clin Ophthalmol. 2016;10:1031. doi:10.2147/OPTH.S106646.
7. Son HS, Labuz G, Khoramnia R, Merz P, Yildirim TM, Auffarth GU. Ray propagation imaging and optical quality evaluation of different intraocular lens models. PLoS One. 2020;15:2. doi:10.1371/journal.pone.0228342
8. Monaco G, Gari M, Di Censo F, Poscia A, Ruggi G, Scialdone A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: trifocal versus extended range of vision. J Cataract Refract Surg. 2017;43:6. doi:10.1016/j.jcrs.2017.03.037
9. Yangzes S, Kamble N, Grewal S, Grewal SPS. Comparison of an aspheric monofocal intraocular lens with the new generation monofocal lens using defocus curve. Indian J Ophthalmol. 2020;68(12):3025–3029. doi:10.4103/ijo.IJO_985_20
10. Sudhir RR, Dey A, Bhattacharrya S, Bahulayan A. AcrySof IQ panoptix intraocular lens versus extended depth of focus intraocular lens and trifocal intraocular lens: a clinical overview. Asia-Pacific J Ophthalmol. 2019;8:4. doi:10.1097/APO.0000000000000253
11. Holladay JT. Proper method for calculating average visual acuity. J Refract Surg. 1997;13(4):388–391. doi:10.3928/1081-597X-19970701-16
12. Abulafia A, Koch DD, Holladay JT, Wang L, Hill W. Pursuing perfection in intraocular lens calculations: IV. Rethinking astigmatism analysis for intraocular lens-based surgery: suggested terminology, analysis, and standards for outcome reports. J Cataract Refract Surg. 2018;44(10):1169–1174. doi:10.1016/j.jcrs.2018.07.027
13. Cochener B, Boutillier G, Lamard M, Auberger-Zagnoli C. A comparative evaluation of a new generation of diffractive trifocal and extended depth of focus intraocular lenses. J Refract Surg. 2018;34:8. doi:10.3928/1081597X-20180530-02
14. Farvardin M, Johari M, Attarzade A, Rahat F, Farvardin R, Farvardin Z. Comparison between bilateral implantation of a trifocal intraocular lens (Alcon AcrySof IQ® PanOptix) and extended depth of focus lens (Tecnis® Symfony® ZXR00 lens). Int Ophthalmol. 2020. doi:10.1007/s10792-020-01608-w
15. Mencucci R, Favuzza E, Caporossi O, Savastano A, Rizzo S. Comparative analysis of visual outcomes, reading skills, contrast sensitivity, and patient satisfaction with two models of trifocal diffractive intraocular lenses and an extended range of vision intraocular lens. Graefe’s Arch Clin Exp Ophthalmol. 2018;256(10):1913–1922. doi:10.1007/s00417-018-4052-3
16. Escandón-García S, Ribeiro FJ, McAlinden C, Queirós A, González-Méijome JM. Through-focus vision performance and light disturbances of 3 new intraocular lenses for presbyopia correction. J Ophthalmol. 2018;2018:1–8. doi:10.1155/2018/6165493
17. Ruiz-Mesa R, Abengózar-Vela A, Ruiz-Santos M. A comparative study of the visual outcomes between a new trifocal and an extended depth of focus intraocular lens. Eur J Ophthalmol. 2018;28:2. doi:10.5301/ejo.5001029
18. Ferreira TB, Ribeiro FJ. Prospective comparison of clinical performance and subjective outcomes between two diffractive trifocal intraocular lenses in bilateral cataract surgery. J Refract Surg. 2019;35(7):418–425. doi:10.3928/1081597X-20190528-02
19. Makhotkina NY, Nijkamp MD, Berendschot TTJM, van den Borne B, Nuijts RMMA. Effect of active evaluation on the detection of negative dysphotopsia after sequential cataract surgery: discrepancy between incidences of unsolicited and solicited complaints. Acta Ophthalmol. 2018;96(1):81–87. doi:10.1111/aos.13508
20. Alio JL, Plaza-Puche AB, Férnandez-Buenaga R, Pikkel J, Maldonado M. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62(5):611–634. doi:10.1016/j.survophthal.2017.03.005
21. de Silva SR, Evans JR, Kirthi V, Ziaei M, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2016;2016:12. doi:10.1002/14651858.CD003169.pub4
22. Felipe A, Artigas JM, Díez-Ajenjo A, García-Domene C, Alcocer P. Residual astigmatism produced by toric intraocular lens rotation. J Cataract Refract Surg. 2011;37(10):1895–1901. doi:10.1016/j.jcrs.2011.04.036
23. Haripriya A, Gk S, Mani I, Chang DF. Comparison of surgical repositioning rates and outcomes for hydrophilic vs hydrophobic single-piece acrylic toric IOLs. J Cataract Refract Surg. 2021;47(2):178–183. doi:10.1097/j.jcrs.0000000000000415
24. Venkataraman A, Kalpana K. Visual outcome and rotational stability of open loop toric intraocular lens implantation in Indian eyes. Indian J Ophthalmol. 2013;61(11):626–629. doi:10.4103/0301-4738.123142
25. Lee BS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes. Ophthalmology. 2018;125(9):1325–1331. doi:10.1016/j.ophtha.2018.02.012
26. Lee BS, Onishi AC, Chang DF. Comparison of rotational stability and repositioning rates of two presbyopia-correcting and two monofocal toric intraocular lenses. J Cataract Refract Surg. 2020;47:5. doi:10.1097/j.jcrs.0000000000000497
27. Garzón N, Poyales F, De Zárate BO, Ruiz-García JL, Quiroga JA. Evaluation of rotation and visual outcomes after implantation of monofocal and multifocal toric intraocular lenses. J Refract Surg. 2015;31(2):90–97. doi:10.3928/1081597X-20150122-03
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.