")
Back to Journals » Clinical Ophthalmology » Volume 11
Comparison of the frequency of use of a pupil expansion device with and without an intracameral phenylephrine and ketorolac injection 1%/0.3% at the time of routine cataract surgery
Authors Bucci Jr FA, Michalek B, Fluet AT
Received 17 January 2017
Accepted for publication 23 March 2017
Published 1 June 2017 Volume 2017:11 Pages 1039—1043
DOI https://doi.org/10.2147/OPTH.S132552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Frank A Bucci Jr, Breanne Michalek, Angel T Fluet
Bucci Laser Vision Institute, Wilkes-Barre, PA, USA
Purpose: The objective of this study is to evaluate whether a phenylephrine and ketorolac injection 1%/0.3% (phenyl/keto injection) (Omidria®) prior to capsulotomy decreases the need for the Malyugin Ring® to manage small pupils.
Setting: Bucci Laser Vision Institute, Wilkes-Barre, PA, USA.
Design: Retrospective analysis of cataract surgeries performed by a single surgeon at a single center.
Methods: A historical control group of 1,004 consecutive cases (December 2013 to February 2015) did not receive a phenyl/keto intracameral injection prior to capsulotomy and were compared with 915 consecutive cases in the treatment group (June 2015 to April 2016) for the rate of use of the Malyugin Ring. Epinephrine injections were selectively used in the control group as per surgeon judgment. Use of the femtosecond laser was recorded for both groups. The incidence of alpha-1 blocker patients and the use of the femtosecond laser were recorded for both groups.
Results: In the 1,004 cases performed in the historical control group without a phenyl/keto injection, the surgeon chose to use the Malyugin Ring 79 times (7.87%). In the 915 cases performed in the treatment group, the surgeon chose to use the Malyugin Ring 27 times (2.95%). The surgeon selectively used intracameral injections of epinephrine in the control group 64 times (6.47%). There was no significant difference in the use of the femtosecond laser in the control group (15.04%) versus the treatment group (16.28%); however, 4 (2.65%) femtosecond patients in the control group required a Malyugin Ring, while zero patients needed the ring in the femtosecond treatment group. The incidence of Malyugin Ring use in alpha-1 blocker patients was 12/49 (24.49%) in the control group and 6/49 (12.74%) in the treatment group (P=0.05).
Conclusion: The frequency of use of the Malyugin Ring was significantly reduced (P<0.001) from 7.87% to 2.95% with this treatment. These results strongly suggest that the antimiotic/anti-inflammatory effects of this phenyl/keto injection reduced facility costs, surgical time, and other complexities related to the use of the Malyugin Ring during phacoemulsification.
Keywords: mydriasis, cataract, Malyugin Ring, Omidria, phenylephrine, ketorolac
Introduction
Maintaining adequate pupil dilation is crucial for successful surgical outcomes in cataract and intraocular lens replacement surgery. Intraoperative miosis can affect visualization of the surgical field; increase the risk of complications, inflammation, and postoperative pain; and reduce patient satisfaction.1 Failure to maintain an adequate pupil diameter can increase the difficulty of the procedure and increase the risk of intraoperative and postoperative complications.2 Intraoperative pupil constriction can make every step of a cataract procedure more challenging and problematic by limiting the size of the capsulorhexis, increasing the risk of iris injury, and reducing visualization for phacoemulsification and lens implantation.3 Maintenance of mydriasis throughout surgery to allow for better visualization of the surgical field and a greater working area within the pupil is crucial for successful surgical outcomes.4 Postoperative pain is associated with clinical outcomes and patient well-being, preventing or reducing postoperative pain can improve patient satisfaction.1,2 Reduction of postoperative pain is important because patient expectations are high in modern cataract surgery and ocular pain, and discomfort represents a common cause of patient dissatisfaction.5
Preoperative topical mydriatic drops are standard for pupil dilation in cataract surgery. The initial effect achieved by topical mydriatics, however, may not be sustained throughout the procedure.2 Even with the use of topical mydriatic drops, intraoperative miosis due to the release of prostaglandins in response to surgical trauma may still occur.6 The preoperative use of topical nonsteroidal anti-inflammatory drugs (NSAIDs) can improve maintenance of the intraoperative pupil diameter and reduce postoperative discomfort.6 Topical and intracameral NSAIDs can contribute to the maintenance of dilation by blocking the miotic effects of prostaglandins released during cataract surgery. However, topical drugs and their effects can be washed out of the anterior chamber by irrigating solutions.2,7
If dilation cannot be achieved and maintained with medications alone, pupil expansion devices, such as the Malyugin Ring (MicroSurgical Technology, Redmond, WA, USA), are available to maintain dilation. Pupil expansion devices provide good dilation and iris stabilization while minimizing pupil distortion and iris damage.8 Patients with Intraoperative Floppy Iris Syndrome (IFIS) may experience progressive pupillary constriction during surgery, and pupil expansion devices are a good option when treating small pupils due to IFIS.8 However, these devices add time, complexity, and cost to the surgical procedure and can traumatize the iris, which, in turn, increases postoperative inflammation.6
Intracameral mydriatics increase pupil dilation without causing measurable ocular side effects or influencing the phacoemulsification process negatively.1 They may also improve operating conditions in complicated cataract surgeries, including those with IFIS, by stabilizing the iris during surgery.1 The intracameral NSAID in the phenylephrine and ketorolac injection 1%/0.3% can reduce inflammation by decreasing prostaglandin production, thereby preventing intraoperative miosis and reducing postoperative pain.9
The phenylephrine and ketorolac injection 1%/0.3% (Omeros Corporation, Seattle, WA, USA) is a drug product added to the ophthalmic irrigation solution and indicated for maintaining pupillary dilation size by preventing intraoperative miosis and for reducing postoperative pain.9 Phenylephrine and ketorolac 1%/0.3% can be delivered by intracameral injection prior to performing the capsulotomy and by continuous irrigation throughout the procedure. The injection is prepared after dilution in the irrigation solution. The two active pharmaceutical ingredients, phenylephrine and ketorolac, act to maintain pupil size by preventing intraoperative miosis and by decreasing prostaglandin production.9 Phenylephrine HCl is an α1-adrenergic receptor agonist and, in the eye, acts as a mydriatic agent by contracting the radial muscle of the iris, resulting in pupil dilation.9 Ketorolac tromethamine is an NSAID that inhibits both cyclooxygenase enzymes (COX-1 and COX-2), resulting in a decrease in tissue concentrations of prostaglandin to reduce pain due to surgical trauma.9 Ketorolac, by inhibiting prostaglandin synthesis secondary to ocular surgical insult or direct mechanical stimulation of the iris, also prevents surgically induced miosis.9 The phenylephrine and ketorolac injection 1%/0.3% is delivered by either intracameral injection prior to performing the capsulotomy or as an anterior chamber irrigation throughout the surgical procedure. Intraocular tissues receive continuous exposure to the pharmacological effects of phenylephrine and ketorolac.2
The objective of this study was to evaluate whether the use of phenylephrine and ketorolac injection 0.01%/0.3% as a dilute intracameral injection, prior to application of a viscoelastic in preparation for the capsulotomy, decreases the need to use a Malyugin Ring for a small pupil during cataract surgery.
Methods
This study was a retrospective surgical chart review of 1,919 cataract surgeries over two time periods (December 2013 to February 2015 and June 2015 to April 2016) performed at a single center by one surgeon. The study was a purely retrospective analysis and did not require approval from an institutional review board, and the Declaration of Helsinki does not apply. All patient data were deidentified and kept confidential. No identifiable patient data were collected.
A chart review was performed on a historical control group of 1,004 consecutive cases who did not receive phenylephrine and ketorolac 1%/0.3% and on a treatment group of 915 consecutive cases who did receive phenylephrine and ketorolac 1%/0.3% as an intracameral injection. Intracameral injections of epinephrine were selectively used in control group cases with IFIS or poorly dilating pupils as determined by the judgment of the surgeon. Intracameral injections of epinephrine in the control group, and of phenylephrine and ketorolac 1%/0.3% in the treatment group, were performed just prior to use of a viscoelastic in preparation for the capsulotomy (just prior to the decision point regarding use of a Malyugin Ring). The number of times the Malyugin Ring was used during the control cases was recorded. In the treatment group, 4 mL of the phenylephrine and ketorolac injection 1%/0.3% was diluted in a 500 mL sterile balanced salt solution (BSS). Approximately 2 mL was drawn from the 500 mL bottle with phenylephrine and ketorolac 1%/0.3% to prepare the intracameral injection given just prior to adding the viscoelastic and performing the capsulotomy. The intracameral injections of epinephrine were not used in the treatment group. The number of times the Malyugin Ring was used during the treatment cases was recorded. Data were collected on how often the femtosecond laser was used in both groups. The frequency of the Malyugin Ring use for the femtosecond laser control and treatment groups was also recorded. The percentage of patients using an alpha-1 blocker and their incidence of Malyugin Ring use were compared between both groups.
Identical preoperative treatments for cataract surgery (antibiotic, NSAID, and steroid drops four times daily for 3 days prior to surgery) were used in both the control and treatment groups. In addition, patients received topical dilating drops (tropicamide 1%, cyclopentolate 1%, and phenylephrine HCl 2.5%) and topical anesthetic drops on the day of surgery. The same viscoelastic agent was used for all patients during surgery. All patients underwent surgery at the same facility by the same surgeon.
Statistical analysis
Data analysis was performed using Excel software (Microsoft Corp.). A one-tailed t-test with alpha =0.05 was used to perform statistical analysis of the differences in the frequency of use of the Malyugin Ring between the control and treatment groups. A P-value of <0.05 was considered statistically significant.
Results
Data from 1,919 cases performed during two different time periods were reviewed. Demographic characteristics were similar across all cases with no clinically meaningful differences between the control and treatment groups (Table 1). In the 1,004 consecutive historical control group cases performed between December 2013 and February 2015 without the use of the phenylephrine and ketorolac injection 1%/0.3%, the surgeon chose to use the Malyugin Ring 79 times (7.87%). The surgeon selectively used intracameral injections of epinephrine in the control group 64 times (6.47%). In 915 consecutive treatment group cases performed between June 2015 and April 2016 with the use of a phenylephrine and ketorolac injection 1%/0.3%, the surgeon chose to use the Malyugin Ring 27 times (2.95%). The frequency of use of the Malyugin Ring was significantly lower in the treatment group relative to the frequency in the control group (P<0.001) (Figure 1).
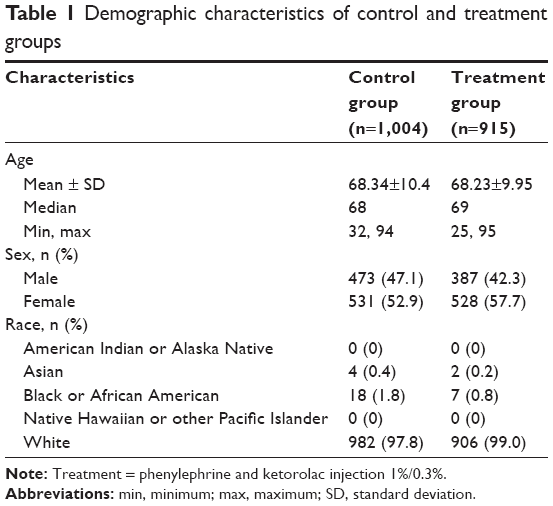 | Table 1 Demographic characteristics of control and treatment groups |
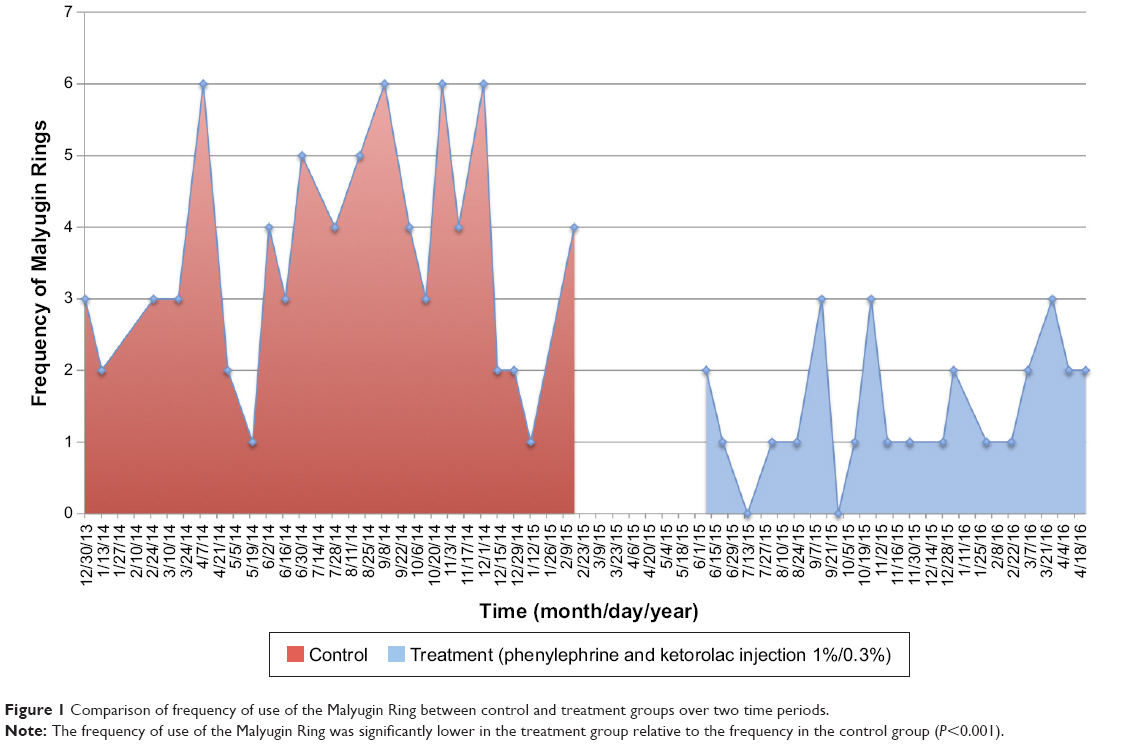 | Figure 1 Comparison of frequency of use of the Malyugin Ring between control and treatment groups over two time periods. |
There was no significant difference in the percentage of cases in which a femtosecond laser was used during the surgery (151 [15.04%] times in the control group versus 149 [16.28%] times in the treatment group). However, of the 151 femtosecond laser patients in the control group, 4 (2.65%) patients required the use of a Malyugin Ring versus none of the 149 patients in the treatment group. There were 49 patients in each group with a history of alpha-1 blocker use (4.88% in the control group and 5.67% in the treatment group). A statistically significant difference in Malyugin Ring use was detected (P=0.05) with 12 (24.49%) rings required in the control group and 6 (12.74%) rings used in the treatment group. The sex breakdown of Malyugin Ring use for each group was also not significantly different. In all, 48 males (60.76%) and 31 females (39.24%) required Malyugin Rings in the control group, while 17 males (62.96%) and 10 females (37.04%) needed a Malyugin Ring in the treatment group.
Discussion
Adequate mydriasis during cataract surgery is critical for preventing intraoperative complications and improving postoperative outcomes. An adequately dilated pupil facilitates visualization throughout the surgical procedure. To achieve mydriasis and control of inflammation during cataract surgery, topical and/or intracameral agents have been used to dilate the pupil and to control postoperative pain and inflammation.1 However, topical mydriatics, viscomydriasis, mechanical devices, and off-label intracameral injections have their limitations.10 When the phenylephrine and ketorolac injection 1%/0.3% is administered, ocular tissues are exposed to a constant concentration of the active ingredients, phenylephrine, and ketorolac.11 Use of the Malyugin Ring can increase the time, cost, and risks of cataract surgery. The results of this study suggested that the antimiotic and anti-inflammatory effects of the phenylephrine and ketorolac injection 1%/0.3% significantly reduced Malyugin Ring usage and associated facility costs. Although it could be argued that considerable cost savings are realized by decreasing complications and decreasing surgical time, it would be difficult to quantify objectively. However, it is clear that 52 fewer Malyugin Rings were used in the treatment group for a similar number of surgical cases. Malyugin Rings are sold for $125 per unit, thus a cost savings of $6,500 was realized from the decreased use of rings in the treatment group compared to the control group.
Analysis of the alpha-1 blocker and femtosecond patient subgroups further supports the benefits of the phenylephrine and ketorolac injection 1%/0.3% for inhibiting miosis and decreasing inflammation. In the alpha-1 blocker subgroup of control patients, the incidence of Malyugin Ring use is threefold greater (24.49%) than that in the entire control group. Consistent with the overall results of the study, we observed that the incidence of Malyugin Ring use in the alpha-1 blocker patients in the treatment group was reduced by half (12.74% vs 24.49%) compared to that in the control group. The femtosecond laser procedure at the time of cataract surgery has been shown to increase the release of prostaglandins, resulting in an increase in inflammation and miosis.12 Analysis of the femtosecond subgroup of patients also supports the overall findings of our investigation. Four patients of the 151 femtosecond patients in the control group required a Malyugin Ring, while none of the 149 patients in the treatment group needed a ring. The low incidence of Malyugin Ring use in femtosecond patients, in general, reflects the surgeon’s preference to avoid femtosecond laser treatment in patients with relatively poor preoperative dilation. Despite the overall lower incidence of Malyugin Ring use in the femtosecond patients, because of surgeon preference, the incidence of zero Malyugin Rings in the treatment group versus four rings (2.65%) in the control group strongly suggests a clinical benefit for femtosecond patients when receiving the phenylephrine and ketorolac injection 1%/0.3%.
Conclusion
The frequency of use of the Malyugin Ring was significantly reduced (P<0.001) from 7.87% to 2.95% with the phenelphrine and ketorolac 1%/0.3% treatment. These results strongly suggest that the antimiotic/anti-inflammatory effects of this phenyl/keto injection reduced facility costs, surgical time, and other complexities related to the use of the Malyugin Ring during phacoemulsification.
What was known
- Previous studies that did not include patients at risk for IFIS and did not include patients who underwent cataract surgery with the use of a femtosecond laser demonstrated that the phenylephrine and ketorolac injection 1%/0.3% was superior to placebo in maintaining pupil diameter, preventing pupil constriction, and reducing acute postoperative ocular pain.2
What this article adds
- Use of the intracameral phenylephrine and ketorolac injection 1%/0.3% in a broad range of patients undergoing cataract surgery significantly reduced the frequency of use of the Malyugin Ring to manage small pupils.
- Use of the phenylephrine and ketorolac injection 1%/0.3% also reduced facility costs related to Malyugin Ring use and associated patient risks of intraocular complications.
Acknowledgments
This study was funded by a grant from Omeros Corporation. The data was presented in part at the annual meeting of the Association for Research in Vision and Ophthalmology, Seattle, WA, USA, May 1–5, 2016.
Disclosure
The authors report no conflicts of interest in this work.
References
Grob SR, Gonzalez-Gonzales LA, Daly MK. Management of mydriasis and pain in cataract and intraocular lens surgery: review of current medications and future directions. Clin Ophthalmol. 2014;8:1281–1289. | ||
Lindstrom RL, Loden JC, Walters TR, et al. Intracameral phenylephrine and ketorolac injection (OMS302) for maintenance of intraoperative pupil diameter and reduction of postoperative pain in intraocular lens replacement with phacoemulsification. Clin Ophthalmol. 2014;8:1735–1744. | ||
Kent C, editor [webpage on the Internet]. Four new ways to manage small pupils. Rev Ophthalmol; 2015. Available from: http://www.reviewofophthalmology.com/content/d/technology_update/c/58155. Accessed March 22, 2016. | ||
Lawuyi LE, Gurbaxani A. The clinical utility of new combination phenylephrine/ketorolac injection in cataract surgery. Clin Ophthalmol. 2015;9:1249–1254. | ||
Donnenfeld ED. Current use of non-steroidal anti-inflammatory drugs in the treatment of ocular inflammation related to cataract surgery. Eur Ophthalmic Rev. 2012;6(3):173–177. | ||
Hovanesian JA, Sheppard JD, Trattler WB, et al. Intracameral phenylephrine and ketorolac (OMS302) during cataract surgery maintains intraoperative mydriasis and reduces postoperative ocular pain: integrated results from two pivotal phase 3 studies. J Cataract Refract Surg. 2015;41(10):2060–2068. | ||
Espandar L, Kim T [webpage on the Internet]. Pharmacologic approaches to the small pupil. Cataract Refract Surg Today; 2014. Available from: crstoday.com/2014/02/pharmacologic-approaches-to-the-small-pupil. Accessed March 28, 2016. | ||
Malyugin B [webpage on the Internet]. Maintaining small pupils: a step-wise approach. Ophthalmol Times; 2014. Available from: ophthalmologytimes.modernmedicine.com/ophthalmologytimes/content/tags/boris-malyugin-md-phd/managing-small-pupils-step-wise-approach?page=full. Accessed March 28, 2016. | ||
OMIDRIA® (phenylephrine and ketorolac injection) 1%/0.3% [package insert]. Seattle, WA: Omeros Corporation; 2015. | ||
Holland EJ, Donnenfeld ED, Henderson BA, Kim T. Case discussions in complicated cataract: miosis control and other surgical pearls. Symposium presented at: American Academy of Ophthalmology Annual Meeting; November 16, 2015; Las Vegas, NV. | ||
Osher RH, Ahmed IK, Demopulos GA. OMS302 (phenylephrine and ketorolac injection) 1%/0.3% to maintain intraoperative pupil size and to prevent postoperative ocular pain in cataract surgery with intraocular lens replacement. Expert Rev Ophthalmol. 2015;10(2):91–103. | ||
Schultz T, Joachim SC, Stellbogen M, Dick HB. Prostaglandin release during femtosecond laser-assisted cataract surgery: main inducer. J Refract Surg. 2015;31(2):78–81. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.